national core indicators project lynnette henderson, phd ucedd associate director of community...
TRANSCRIPT

National Core Indicators Project
Lynnette Henderson, PhDUCEDD Associate Director of Community Services
Vanderbilt Kennedy Center
Jessie Baird, MEd Candidate

WHAT IS NATIONAL CORE INDICATORS (NCI)?
• Multi-state collaboration of state DD agencies • Measures performance of public systems for people with
intellectual and developmental disabilities• Assesses performance in several areas, including: employment,
community inclusion, choice, rights, and health and safety• Launched in 1997 in 13 participating states, now used in 39
states
• NASDDDS – HSRI Collaboration– National Association of State Directors of Developmental Disabilities
Services (NASDDDS) – Human Services Research Institute (HSRI).

CT
NCI State Participation 2013-14
HI
WA
AZOK
KY
AL
NC
PA
MA
TX
AR
GANM
NJ
MO
NH
OH*IL
LA
NY
Wash DC
FL
CA*
SDOR
MN
UTCO KS
MS
TNSC
WI
MI
IN
VA
DE
MD
State contract awarded in 2013-14 through AIDD fundingCA*- Includes 21 Regional CentersOH*- Also includes the Mid-East Ohio Regional Council
39 states, the District of Columbia and 22 sub-state regions
ME

National Sample
• Hewitt, A. S., Stancliffe, R. J., Johnson Sirek, A., Hall-Lande, J., Taub, S., Engler, J., Bershadsky, J., Fortune, J., & Moseley, C. (2011). Characteristics of adults with autism spectrum disorder who use adult developmental disability services: Results from 25 US states. Research in Autism Spectrum Disorders, 6(2), 741-751.
• Data from 2006––2008 from 25 states AL, AR, AZ, CT, DE, GA, HI, IN*, KY, LA, MO*, NC, NJ, NM, NY*, OK, PA*, RI, SC*, TX, VT, WV, and WY. CA (Orange County only), and WA– 12,382 people served by their states – (55.6%)men and (44.4%) women, – average age of 42.7 years (range 18–100).– 1002 individuals with an ASD diagnosis (8.1%).– percentage of members with ASD ranged from 3.7% to 27.4% . – TN 2013-2014 sample was at 11.9%


Age distribution of the 2013-2014 NCI Sample
N 436Mean 46.26Minimum 20Maximum 84Percentiles 25 34.00
50 47.0075 58.00

Nationally and in TN, Adults with ASD are younger than the larger NCI group.
F(1)=46.5, p=.000
m=48.1
m=34.30

Gender distribution of the 2013-2014 NCI Sample
GENDER Frequency PercentMale 265 60.8Female 171 39.2
60.8%39.2%

Substantial overrepresentation of males with an ASD diagnosis in National and TN samples
226
158
3913
χ2 (2) = 5.008, N = 436, p = .025

Level of Intellectual Disability within the 2013-2014 NCI Sample:
267
63.3%
109
25.8% 4610.9%

Intellectual Disability • National Studies found
there was an interesting bi-modal distribution of autism/ASD diagnosis by level of intellectual disability with higher proportions for people with no ID diagnosis or severe/profound ID.
• TN data did not support this finding, since only those with ID are eligible to receive DIDD services in TN
Mild-m
oderate
Severe-Profound
Unknow
n
χ2 (2) = 190, N = 436, p = .387
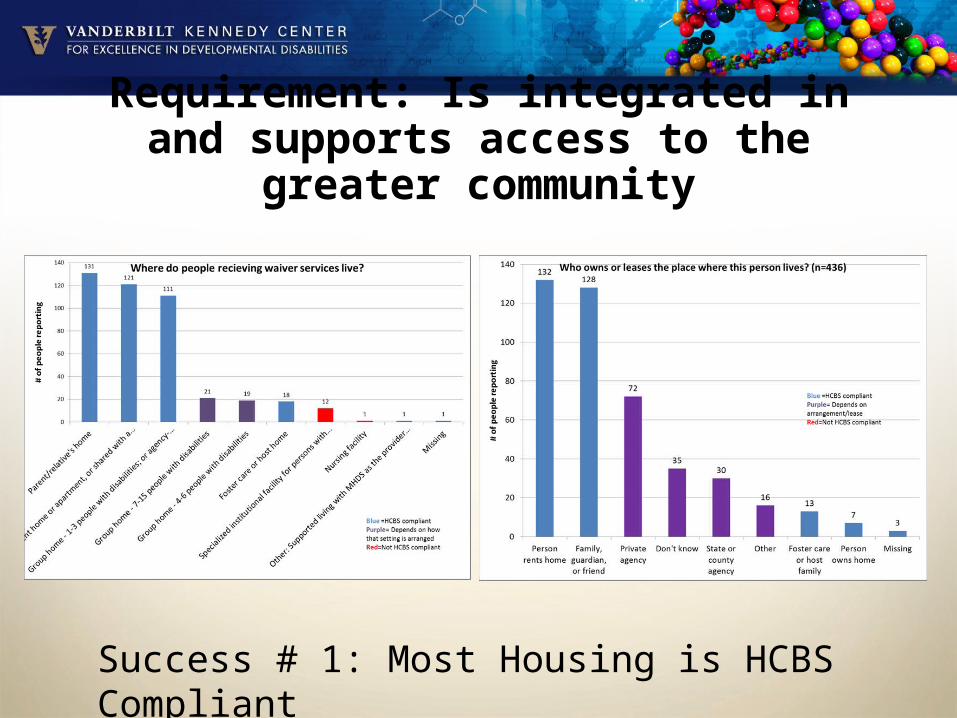
Requirement: Is integrated in and supports access to the greater community
Success # 1: Most Housing is HCBS Compliant

Behavioral Challenges limit home choice for people with ASD in TN
β = -.887, t(433) = 2.42, p < .000

Requirement: Is integrated in and supports access to the greater community
Opportunity #1 and Opportunity #2 for more integration.

Requirement: Provides opportunities to seek employment and work in competitive integrated settings, engage in community
life, and control personal resources
Success #4 / Opportunity #1: Time and Money

People with ASD are less likely to have a paid job in the community
241
57 59
184
26 χ2 (2) = 36.16, N = 405, p = .000

Requirement: Ensures right to privacy, dignity and respect and freedom from coercion and restraint
Success #1: People feel good about their privacy.

Relationships with Staff are different for people with ASD
9
262
11
70
21 27
χ2 (3) = 27.73, N = 403, p = .000
AND complicated by
communication difficulties
β =.104, t(433) = 1.110, p = .000
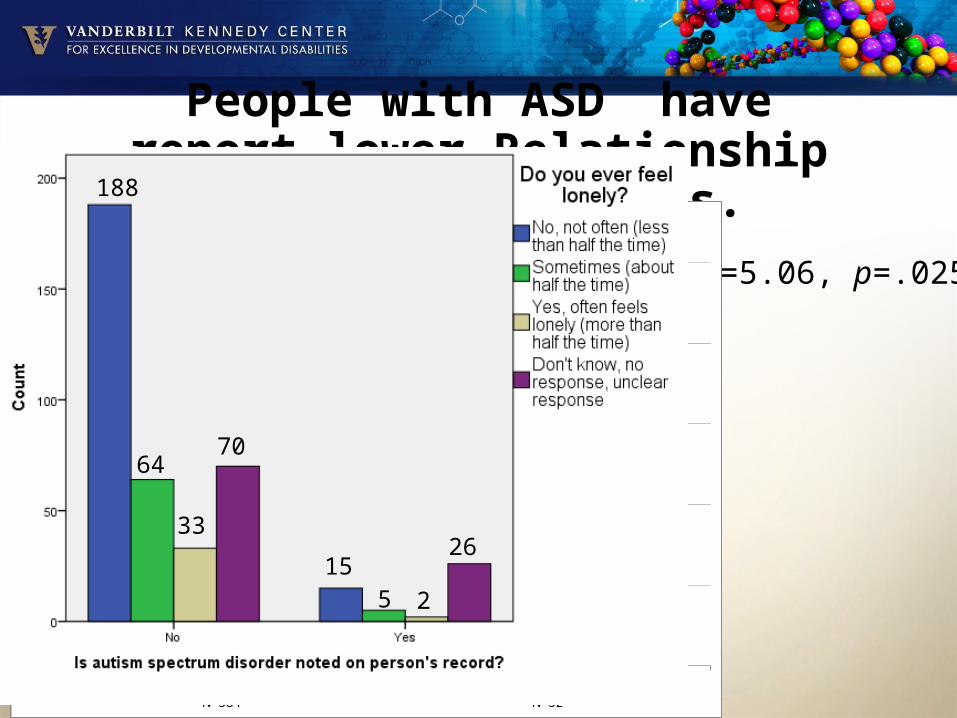
People with ASD have report lower Relationship Scores than others.
F(1)=5.06, p=.025
188
64
33
70
155 2
26

Requirement: Ensures right to privacy, dignity and respect and freedom from coercion and restraint
Opportunity #2: 22% can’t express whether they feel fear.

C. New HCBS Person-Centered Service Plan Process RequirementsRequirement: Service planning process is driven by the individual
Success #1: People get the services they need.

People with ASD are less satisfied with their services than others in the sample.
F(1)=14.63, p=.000

Requirement: Facilitates choice of services and who provides them
Opportunity #1: Service coordinators are not viewed as partners.

People with ASD are less satisfied with their ISC and service planning than others in the sample.
• F(1)=40.18, p=.000•

Areas of Concern
Associated with
RegionalFindings
Areas of Concern Associated with Region of Tennessee
poorer outcomes better outcomes
Individual Outcomes
Work Living in East or West TN Living in Middle TN
Community Inclusion Living in East or West TN Living in Middle TN
Choice and Decision Making Living in West TN Living in Middle TN
Self Determination
Relationships Living in East or Middle TN Living in West TN
Health, Welfare and Rights
Health
Medications Living in Middle and East TN Living in West TN
Wellness
Respect/Rights /Safety Living in Middle and East TN Living in West TN
System Performance
Service Coordination Living in Middle TN Living in West and East TNs
Access

Areas of Concern
Associated with Level of
Demonstrated Communication
Areas of Concern Associated with Demonstrated Communication Level
poorer outcomes better outcomes
Individual Outcomes
Work Not having a functional communication system Communicating verbally
Community Inclusion Not having a functional communication system Communicating verbally
Choice and Decision Making Not having a functional communication system Communicating verbally
Self Determination
Relationships Not having a functional communication systemCommunicating verbally
Health, Welfare and Rights
Health
Medications
Wellness
Respect/Rights /Safety Not having a functional communication systemCommunicating verbally
System Performance
Service Coordination Not having a functional communication system Communicating verbally
Access Not having a functional communication system Communicating verbally

Areas of Concern Associated with
Conservator Status
Areas of Concern Associated with Conservatorship Status
poorer outcomes better outcomes
Individual Outcomes
Work Having a conservator Not having a conservator
Community Inclusion
Choice and Decision Making Having a conservator Not having a conservator
Self Determination
Relationships Having a conservator Not having a conservator
Health, Welfare and Rights
Health
Medications
Wellness
Respect/Rights /Safety Having a conservator Not having a conservator
System Performance
Service Coordination Having a conservator Not having a conservator
Access
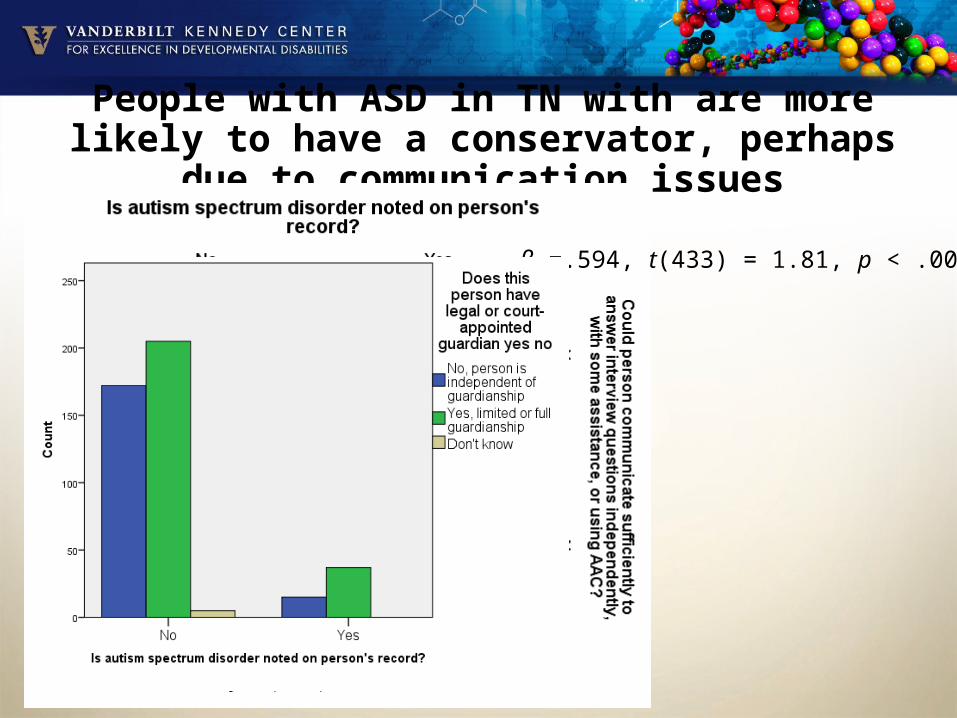
People with ASD in TN with are more likely to have a conservator, perhaps due to communication issues
β =.594, t(433) = 1.81, p < .000

People with ASD receiving services in TN have fewer choices
F(1)=7.413, p=.007
β =.049, t(433) = 1.05, p = .050

Communication Differences found in the National and TN Sample
χ2 (1) = 26.442, N = 385, p = .000
283
59
21 22
293
69
6 10 5
28 221 1
χ2 (4) = 16.90, N = 435, p = .002

Communication Differences found in the National and TN Sample
χ2 (4) = 35.496, N = 402, p = .000
271
12
59
8 4 174
223 2

Co-morbidities
• In the Tennessee sample, persons with ASD were:– MORE likely to have a
psychiatric diagnosis– χ2 (5) = 13.886, N = 436, p = .016
– MORE likely to have a anxiety disorder diagnosis
– χ2 (1) = 3.715, N = 436, p = .041
– More likely to have noted behavioral challenges
– χ2 (1) = 10.918, N = 436, p = .001
• In the national sample persons with ASD were:– more likely to have a communication
disorder, – less likely to have a psychiatric
diagnosis, – less likely to have a vision problem, – less likely to have a physical disability , – less likely to have a hearing impairment, – less likely to have Down Syndrome, and – their was no relationship between ASD
and seizure disorder

Recommendations for using NCI Data for Quality Improvement
• Generate State-Specific Charts on the Website• Use the Data from this Report• Create Groups to Review the Data• Identify Areas for Improvement• Develop Change Strategies• Develop Benchmarks• Share the Data in an Accessible Format
• http://vkc.mc.vanderbilt.edu/vkc/nci/

“The Elephant in the Room”• DIDD was created in 2009, but its predecessor, DMHDD,
was established in 2000 after a title 33 revision• In 2014, individuals with developmental disabilities like
ASD without co-occurring intellectual disabilities are not being served by the department– Exception: Family Support program
• Waiting list for individuals with intellectual disabilities exceeds 7000; this is an underestimate of the need.

Waiver Programs for People with ASD
• The majority of states in the U.S. operate HCBS Section 1915(c) Medicaid waiver programs with related conditions or related disability clauses (Hall-Lande et al., 2011). These policies allow individuals with ASD to be eligible for HCBS that are available to people with DD or ID.
• Yet, at the time of the study only two states have implemented specific waiver programs for adults with ASD (IN and PA).
• “In the absence of specific eligibility criteria that do not require a diagnosis of ID, it is unlikely that people with Asperger disorder or high functioning autism will be served in the developmental disabilities system.”

Medicaid Waiver Background• Medicaid may vary eligibility from one state to another, so
too may states’ eligibility for HCBS waiver program ser vices and services funded by local state dollars.
• Medicaid eligibility require ments may be two-part: – income and other provisions such as the Tax Equity and
Fiscal Responsibility Act of 1982.– Needs institutional level of care criteria/ needs “active
treatment.”
“Clearly there is a need for IDD services nationally to be prepared to serve individuals with ASD, including those without
ID. It is worth asking the question whether or not individuals with ASD, particularly those who have ASD but not ID, are
appropriately served in traditional services for people with IDD or if there is a better option.”

New Waiver Proposals• TennCare and DIDD have developed new waiver proposals in an effort
to meet the needs of the DD population, including those with ASD. • Changes to three existing waivers Statewide Waiver,
Comprehensive, Aggregate Cap Waiver, and Self-Determination Waiver have been approved. They will be capped and services will be provided through managed care.
• TennCare and the Department of Intellectual & Developmental Disabilities (DIDD) have released a Concept Paper about the future of the state's Home and Community Based Services for people with intellectual and developmental disabilities. – For a summary of key points for people currently receiving waiver
services, click here. – For a summary of key points for people waiting for services,
click here. – To view the Consumer/Family presentation, click here. – To view the Provider/Advocate presentation, click here.

The TN Autism Plan - StructureWhile the plan is certainly “autism specific”, another key goal in designing the final report was to make sure that as much as possible, both the specific recommendations for action and the vision for new initiatives would dovetail as seamlessly as possible with existing disability community directions and values.

Policy Considerations• Historically, ASD has been a very expensive disability to
accommodate and states have been challenged to develop comprehensive, well-coordinated systems to sup port individuals with ASD.
• Furthermore, part of the challenge and expense may be that services are not always well-matched to the particular needs of the current popula tion of individuals with ASD.
• They may be using more costly services such as mental health services, emergency rooms, crisis placements or correctional facilities.
• Policy researchers may discover that less-costly community services addressing the long-term needs of people with higher functioning ASD could actually lower overall state costs.