n770 poster handout - a community of learners improving ... · poster handout of supporting...
TRANSCRIPT

Comprehensive Pain Assessment – Best Practice 1
Documentation of Comprehensive Pain Assessment in Outpatient Medical Oncology –
Best Practice
Poster Handout of Supporting Material and References
N770 Scholarship Poster Presentation Session
March 26, 2013
Michelle K. H. Wald, MSN, RN, CNP

Comprehensive Pain Assessment – Best Practice 2
Needs Assessment - Chart Audit Tool
Clinic number Prior pain level o 0-10 o N/A
Gender o Female o Male
Pain score 1 – 3 o NSAID o Tylenol o Slow titration of short-acting opioid o No action
Age Opioid naïve: Pain score 4 – 6 o MSIR 5–15mg po o Oxycodone 5-10mg po o Dilaudid 2-4mg po o Other o No action
Type of visit o Initial consult o Follow-up
Opioid naïve: Pain score 7 – 10 o MSIR 5-15mg po o Oxycodone 5-10mg po o Dilaudid 2-4mg po o Other o No action
Date of visit Opioid tolerant: Pain score 4 – 6 … 10-20% of previous 24 hr dose?
o Yes o No o Other o No action
Primary site of cancer Opioid tolerant: Pain score 7 – 10 … 10-20% of previous 24 hr dose?
o Yes o No o Other o No action
Stage of disease o I / II o III o IV
Reassessment following change in therapy? o Yes o No o N/A
Care provider o Staff o Fellow o NP / PA
Bowel regimen addressed? o Yes o No o N/A
Documentation of pain score o Yes o No
Patient education documented? o Yes o No o N/A
Current pain level (0 – 10) Consistent w/ NCCN guidelines? o Yes o No o N/A

Comprehensive Pain Assessment – Best Practice 3
Needs Assessment – Provider Survey Tool
1) Who are you?
a. Consultant b. Fellow c. NP/PA
2) Number of years in practice?
a. Fellowship b. 0-5 years c. 6-10 years d. 11-15 years e. 16-20 years f. 20+ years
3) Pain management is an important component of oncologic practice …
a. Strongly agree b. Agree c. Neutral d. Disagree e. Strongly disagree
4) Pain is an issue in _______ of the patients I see …
a. None b. A few c. Some d. Most e. All
5) My knowledge of assessing and managing pain is based on …
a. Formal medical/nursing education (i.e. residency or fellowship training) b. Established clinical guidelines c. Self-directed (i.e. personal experience, advice from colleagues, or CME content) d. Pain consultation recommendations e. Other

Comprehensive Pain Assessment – Best Practice 4
6) Clinical vignette: 67-year old woman with non small cell lung cancer and metastatic disease to the bones presents c/o increasing pain in her left hip. She has been taking oxycodone 5mg/acetaminophen 325mg (Percocet) tablets … 16 tablets per day provide control of her pain. She is experiencing mild nausea and needs to take a pill during the middle of the night. The next appropriate step in drug therapy for this patient would be:
o Morphine (oral) 50mg = oxycodone 30mg = fentanyl (transdermal) 25mcg = 12.5mg po hydromorphone (Dilaudid)
a. Oxycontin 20mg po bid b. MS Contin 45mg po bid c. Transdermal fentanyl 100mcg/hr patch d. MS Contin 60mg po bid e. Oral hydromorphone 4mg po q 3hrs
7) Clinical vignette: 34-year old man with metastatic melanoma whose pain is controlled
with 8mg hydromorphone po q4h ATC. If the patient is late with a dose or awakened at night, he is in severe pain. He is experiencing nausea related to the opioid. You want to convert him to a long-acting pain medication and switch him to morphine to see if he will have less nausea. You check your equianalgesic table:
Opioid Oral Equivalent Parenteral Equivalent Hydromorphone Morphine Oxycodone
7.5mg 30mg 20mg
1.5mg 10mg
What would be an appropriate starting regimen when converting from hydrocodone to morphine (combination long-acting [SR] and short-acting [IR])?
a. MS Contin 30m po bid w/ morphine IR 15mg po q4h prn b. MS Contin 60mg po bid w/ morphine IR 15mg po q4h prn c. MS Contin 90mg po bid w/ morphine 30mg po q4h prn d. MS Contin 120mg po bid w/ morphine IR 30m po q4h prn
8) Clinical vignette: 53-year old woman with metastatic breast cancer, recently discharged
from the hospital on OxyContin 20m po bid. Her pain is well-controlled (3 out of 10 worst pain during the day) and she takes one dose of 5mg breakthrough per day. She is looking for a less expensive alternative and is willing to try morphine.
Opioid Oral Equivalent Parenteral Equivalent Hydromorphone Morphine Oxycodone
7.5mg 30mg 20mg
1.5mg 10mg

Comprehensive Pain Assessment – Best Practice 5
What is the correct dose of morphine to prescribe?
a. MS Contin 15mg po bid w/ morphine IR 10 mg po q4h prn b. MS Contin 30mg po bid w/ morphine IR 10mg po q4h prn c. MS Contin 45mg po bid w/ morphine IR 20mg po q4h prn d. MS Contin 60mg po bid w/ morphine 20mg o q4h prn
9) What prevents you from assessing your patient’s pain?
a. Lack of knowledge b. Lack of time c. “Not my job” d. Didn’t think of it e. Patient didn’t initiate conversation f. Other
10) What prevents you from documenting your patient’s pain?
a. Lack of knowledge b. Lack of time c. “Not my job” d. Didn’t think of it e. Other

Comprehensive Pain Assessment – Best Practice 6
Level of Effectiveness / Evidence Guides
* Level of Effectiveness
Effective: Research validates the effectiveness of the nursing activity or intervention, preferably with Level 1 or Level 2 evidence. Possibly Effective: There are some research studies that validate the effectiveness of the nursing activity or intervention, but with insufficient strength to recommend that nurses institute the activity or intervention at this time. Generally more research is needed. Not Effective: Research has shown that the nursing activity or intervention is not effective and generally should not be used. Possibly Harmful: There are some studies that show harm to clients when using the nursing activity or intervention and the nurse should evaluate carefully whether the activity is ever appropriate.
Ackley, B. J., Swan, B. A., Ladwig, G., & Tucker, S. (2008). Evidence-based nursing care
guidelines: Medical-surgical interventions. St. Louis, MO: Mosby Elsevier.
** Level of Evidence
Level I: Evidence from a systematic review or meta-analysis of all relevant randomized controlled trials (RCTs) or evidence-based clinical practice guidelines based on systematic reviews of RCTs or three or more RCTs of good quality that have similar results. Level II: Evidence obtained from at least one large (multi-site) well-designed RCT. Level III: Evidence obtained from well-designed controlled trials without randomization (i.e., quasi-experimental). Level IV: Evidence from well-designed case-control or cohort studies. Level V: Evidence from systematic reviews of descriptive and qualitative studies. Level VI: Evidence from a single descriptive or qualitative study. Level VII: Evidence from the opinion of authorities and/or reports of expert committees.
Ackley, B. J., Swan, B. A., Ladwig, G., & Tucker, S. (2008). Evidence-based nursing care
guidelines: Medical-surgical interventions. St. Louis, MO: Mosby Elsevier.

Comprehensive Pain Assessment – Best Practice 7
Stakeholders
o Chair Institutional Outpatient Clinical Practice Committee
o Medical Oncology Division Chair
• Medical Oncology Clinical Practice Committee Chair
o Supervisor – Nurse Practitioners (NPs) and Physician Assistants (PAs)
• Sarcoma / Head & Neck Clinic NP
o Nurse Administrator / Manager
• Registered Nurses (RNs)
o Supervisor – Clinical Assistants
• Clinical Assistants
o Supervisor – Medical Secretaries
• Assistant Supervisor – Medical Secretaries
o Medical Oncology Administrator
• Medical Oncology Operations Manager
• Systems and Procedures Staff

Comprehensive Pain Assessment – Best Practice 8
RN Tools
Pain Assessment Intake / Documentation Guide Based on NCCN guidelines (Swarm et al., 2010)
• Location
• Intensity (0-10)
• Interference with activities o Mood / Sleep / Appetite / General activity
• Timing
o Onset / Duration / Persistent / Intermittent
• Description / Quality o Aching / Stabbing / Throbbing / Pressure … somatic pain in skin, muscle, bone? o Gnawing / Cramping / Aching / Sharp … visceral pain in organs or viscera? o Sharp / Tingling / Ringing / Shooting … neuropathic pain?
• Aggravating / Alleviating factors
• Other current symptoms
• Current pain management plan (prescription, OTC, & non-pharmacologic) o What meds? o How much? o How often? o Who prescribes?
• Response to current therapy
o Relief / Adherence / Side effects … specific attention to constipation and nausea
• Prior pain therapies o Reason for / Length of use o Response o Why stopped?
• Special issues
o Beliefs / Patient goals & expectations
• Psychosocial o Family & other support o History of substance abuse o Risk for diversion
• Patient education needs

Comprehensive Pain Assessment – Best Practice 9
RN Tools
Constipation … Guide to Prophylaxis & Management Based on NCCN guidelines (Swarm et al., 2010)
Prevention: • Stimulant laxative +/- stool softener … such as senna +/- ducosate
o Senokot S, Peri-Colace are both examples of senna + ducosate 2 tabs orally (PO) every morning Max 8-12 tabs per day
• Increase dose of laxative when increasing dose of opioids • Maintain adequate fluid intake (8-10 glasses of clear liquid daily) • Maintain adequate dietary fiber intake
o Metamucil and like compounds are not recommended (risk of impaction) o Oral mineral oil is effective for hard stool, but should not be used for routine
prevention as it may interfere with absorption of some nutrients • Exercise (if feasible)
If Develops:
• Rule out (r/o) obstruction • r/o impaction • Increase stool softener / laxative as above
o Goal of one non-forced BM every 1-2 days If Persists:
• r/o obstruction • r/o impaction • Consider adding another agent:
o Magnesium hydroxide (Milk of Magnesia) 30-60 mls PO daily
o Bisacodyl (Correctol laxative, Dulcolax, Ex-lax Ultra) 2-3 tablets PO daily OR 1 rectal suppository daily
o Lactulose 30-60 mls PO daily
o Sorbitol 30 mls PO every 2 hrs x 3, then prn
o Magnesium citrate 8 oz PO daily
o Polyethelene glycol (MiraLAX, GoLYTELY) 1 capful in 8 oz water PO twice daily
• Fleet, saline, or tap water enema • Consider use of prokinetic
o Metoclopramide (Reglan) 10-20 mg PO every 6 hrs • In advanced disease, for opioid-induced constipation unresponsive to above, could
consider … o Methylnaltrexone (Relistor)
0.15 mg/kg SQ … max 1 dose / day

Comprehensive Pain Assessment – Best Practice 10
RN Tools
Nausea … Guide to Prophylaxis & Management Based on NCCN guidelines (Swarm et al., 2010)
Prevention:
• For patients with a prior history of opioid-induced nausea, prophylactic treatment with antiemetic agents is highly recommended (see below)
If Develops:
• Assess for other causes o Constipation o CNS pathology o Chemotherapy o Radiation therapy o Hypercalcemia
• Consider: o Prochlorperazine (Compazine)
10 mg PO every 6 hrs as needed o Thiethylperazine (Torecan)
10 mg PO every 6 hrs as needed o Haloperidol (Haldol)
0.5-1 mg PO every 6-8 hrs o Metoclopramide (Reglan)
10-20 mg PO every 6 hrs as needed If Persists:
• Despite as needed regimen o Administer antiemetics ATC for 1 week, then change to as needed
• Consider adding a serotonin antagonist o Granisetron (Kytril)
2 mg PO daily o Ondansetron (Zofran)
8 mg PO three times daily o Dolasetron (Anzemet)
100-200 mg PO o Palonosetron (Aloxi)
300 mcg/kg IV Use with caution as constipation is a side effect
• Consider dexamethasone If Persists > 1 Week:
• Reassess cause and severity of nausea • Consider opioid rotation
Comprehensive Pain Assessment – Best Practice 11
RN Tools
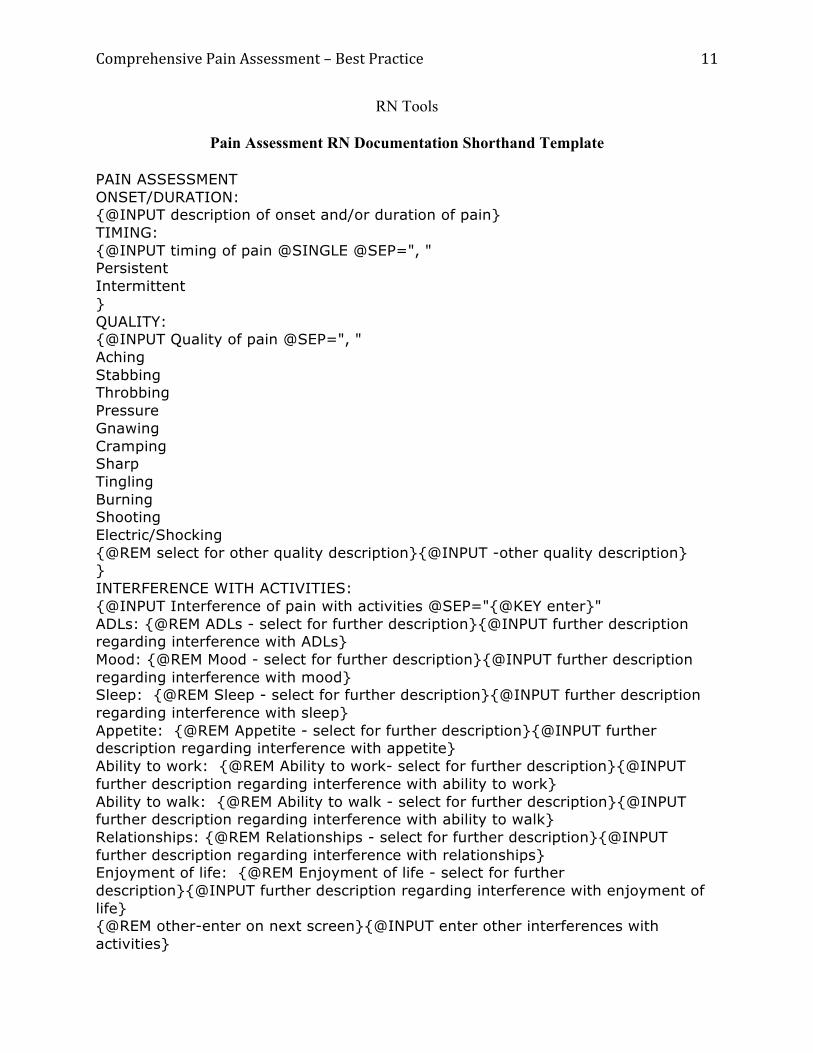
Pain Assessment RN Documentation Shorthand Template
PAIN ASSESSMENT ONSET/DURATION: {@INPUT description of onset and/or duration of pain} TIMING: {@INPUT timing of pain @SINGLE @SEP=", " Persistent Intermittent } QUALITY: {@INPUT Quality of pain @SEP=", " Aching Stabbing Throbbing Pressure Gnawing Cramping Sharp Tingling Burning Shooting Electric/Shocking {@REM select for other quality description}{@INPUT -other quality description} } INTERFERENCE WITH ACTIVITIES: {@INPUT Interference of pain with activities @SEP="{@KEY enter}" ADLs: {@REM ADLs - select for further description}{@INPUT further description regarding interference with ADLs} Mood: {@REM Mood - select for further description}{@INPUT further description regarding interference with mood} Sleep: {@REM Sleep - select for further description}{@INPUT further description regarding interference with sleep} Appetite: {@REM Appetite - select for further description}{@INPUT further description regarding interference with appetite} Ability to work: {@REM Ability to work- select for further description}{@INPUT further description regarding interference with ability to work} Ability to walk: {@REM Ability to walk - select for further description}{@INPUT further description regarding interference with ability to walk} Relationships: {@REM Relationships - select for further description}{@INPUT further description regarding interference with relationships} Enjoyment of life: {@REM Enjoyment of life - select for further description}{@INPUT further description regarding interference with enjoyment of life} {@REM other-enter on next screen}{@INPUT enter other interferences with activities}

Comprehensive Pain Assessment – Best Practice 12
No interference. } AGGRAVATING/ALLEVIATING FACTORS: {@INPUT factors that aggravate or alleviate pain} OTHER CURRENT SYMPTOMS: {@INPUT other current pain related symptoms} CURRENT PAIN MANAGEMENT PLAN: Pharmacologic: {@INPUT Pharmacologic @SEP="{@KEY enter}" Acetaminophen: {@REM Acetaminophen- select for dose, route, frequency}{@INPUT Acetaminophen dose, route, frequency} NSAIDs: {@REM NSAIDs- select for dose, route, frequency}{@INPUT NSAIDs dose, route, frequency} Morphine: {@REM Morphine - select for dose, route, frequency}{@INPUT Morphine dose, route, frequency} Hydromorphone: {@REM Hydromorphone - select for dose, route, frequency}{@INPUT Hydromorphone dose, route, frequency} Fentanyl: {@REM Fentanyl - select for dose, route, frequency}{@INPUT Fentanyl dose, route, frequency} Levorphanol: {@REM Levorphanol - select for dose, route, frequency}{@INPUT Levorphanol dose, route, frequency} Methadone: {@REM Methadone- select for dose, route, frequency}{@INPUT Methadone dose, route, frequency} Oxycodone:{@REM Oxycodone - select for dose, route, frequency} {@INPUT Oxycodone dose, route, frequency} Hydrocodone: {@REM Hydrocodone- select for dose, route, frequency}{@INPUT Hydrocodone dose, route, frequency} Oxymorphone:{@REM Oxymorphone - select for dose, route, frequency} {@INPUT Oxymorphone dose, route, frequency} Codeine: {@REM Codeine - select for dose, route, frequency}{@INPUT Codeine dose, route, frequency} Antidepressant: {@REM Antidepressant - select for dose, route, frequency}{@INPUT Antidepressant dose, route, frequency} Anticonvulsant: {@REM Anticonvulsant - select for dose, route, frequency}{@INPUT Anticonvulsant dose, route, frequency} Corticosteroid:{@REM Corticosteroid - select for dose, route, frequency} {@INPUT Corticosteroid dose, route, frequency} Topical agent:{@REM Topical agent - select for dose, route, frequency} {@INPUT Topical agent dose, route, frequency} {@REM Other-Enter med, dose, route, frequency on next screen}{@INPUT Enter med, dose, route, frequency} None. } Non-Pharmacologic: {@INPUT non-pharmacologic @SEP="{@KEY enter}" Ice: {@REM Ice}{@INPUT ice} Heat:{@REM Heat}{@INPUT heat} Massage: {@REM Massage}{@INPUT massage}

Comprehensive Pain Assessment – Best Practice 13
Acupuncture: {@REM Acupuncture}{@INPUT Acupuncture} TENS: {@REM TENS}{@INPUT TENS} Ultrasound:{@REM Ultrasound}{@INPUT ultrasound} Relaxation:{@REM Relaxation} {@INPUT relaxation} Guided imagery/hypnosis:{@REM Guided imagery/hypnosis} {@INPUT Guided imagery/hypnosis} None. {@REM select to type additional non-pharmacologic or further description on next screen}{@INPUT enter additional non-pharmacologic or further description} } RESPONSE TO CURRENT PAIN THERAPY: {@INPUT Response to current pain therapy @SEP="{@KEY enter}" Degree of pain relief: {@REM degree of pain relief-select to enter comments on next screen }{@INPUT enter degree of pain relief} Patient adherence: {@REM patient adherence- select to enter comments on next screen}{@INPUT enter comments regarding patient adherence} Pain medication adverse effects: {@REM Pain medication adverse effects}{@INPUTFILE adverse effects.txt} } PRIOR PAIN THERAPIES: {@INPUT enter prior pain therapies} SPECIAL ISSUES RELATED TO PAIN: {@INPUT special issues related pain @SEP="{@KEY enter}" History of substance abuse: {@INPUT further description of history of substance abuse} Risk for diversion: {@INPUT further description of risk for diversion} Psychosocial support: {@INPUT further description of psychosocial support} {@REM select for other special issues}{@INPUT enter other special issues} None. } PATIENT EDUCATION: {@INPUT Patient Education Pamphlet(s) @SEP="{@KEY enter}" Informational pamphlet(s) were provided and reviewed with the patient: Common Concerns About Medications for Cancer Pain (MC5236). Pain Control: A Guide for Those with Cancer and Their Loved Ones (ACS276845). Pain Control: Support For People with Cancer (NCI243542). Reinforced principles of pain medication administration and common side effect management. {@REM Free text regarding patient education}{@INPUT Free text regarding patient education} } {@REM Standard Patient Education Template}{@INPUT Standard Patient Education Template @SEP=", " {@REM Standard Patient Education Text}Ready to learn, no apparent learning barriers were identified; learning preferences include listening. Patient expressed understanding of the content. {@REM None} }
Comprehensive Pain Assessment – Best Practice 14
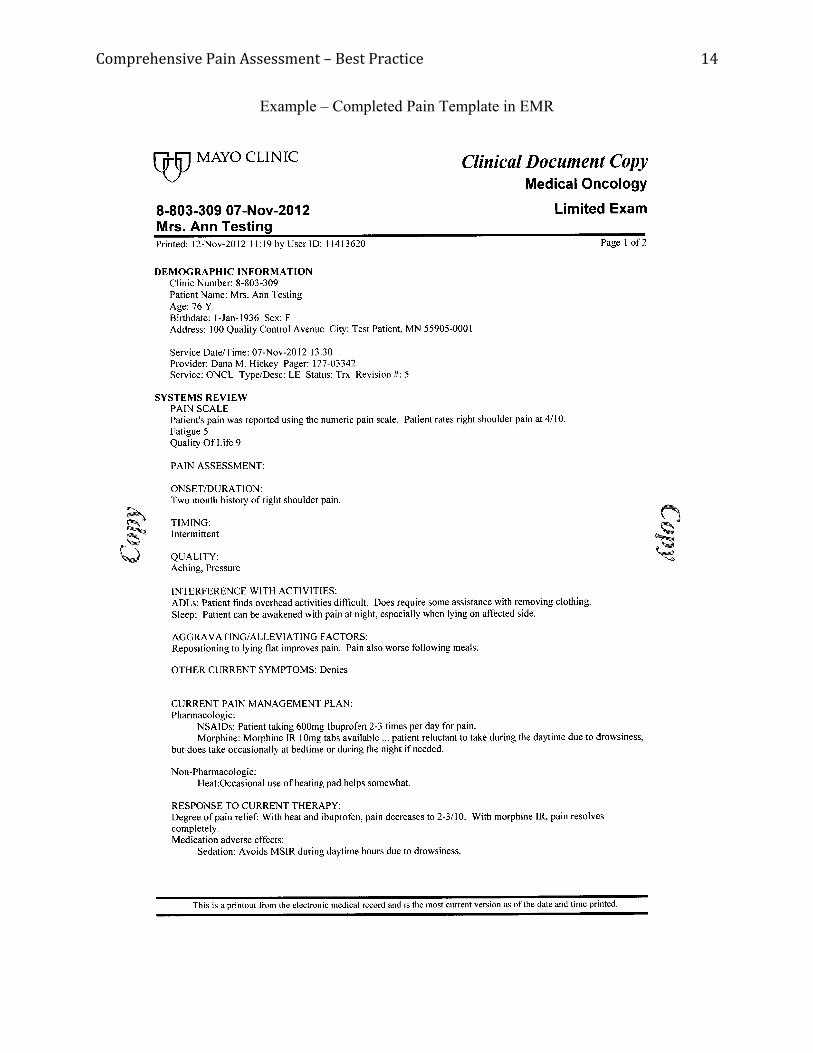
Example – Completed Pain Template in EMR

Comprehensive Pain Assessment – Best Practice 15

Comprehensive Pain Assessment – Best Practice 16
Outcome Evaluation – Chart Audit Tool
www.project-redcap.org
ConfidentialOutcome Evaluation Chart Audit - Pain Management MedOnc
Page 1 of 2
Outome Evaluation Chart Audit
Clinic Number __________________________________
Gender FemaleMale
Age __________________________________
Type of Visit Initial ConsultFollow-up
Date of Visit __________________________________
Primary Site of Cancer BreastGIHead & NeckLungSarcoma
Stage of Disease I / IIIIIIV
Care Provider StaffFellowNP/PA
RN Involved in Visit? YesNo
Docmentation of Pain Score YesNo
Current Pain Level 012345678910No pain score provided
Pain Assessment Documented YesNo
Assessment Documented By StaffFellowNP/PARN
Pain score consistent with provider note? YesNo
Is pain score reconciled in RN note? YesNo

Comprehensive Pain Assessment – Best Practice 17
www.project-redcap.org
ConfidentialPage 2 of 2
Prior Visit Pain Level 012345678910No pain score providedn/a (No prior visit)
Documentation of Treatment Plan YesNo
Treatment Plan Documented By ... StaffFellowNP/PARN
Reassessment Following Change in Therapy? YesNon/a
Bowel Regimen Addressed? YesNon/a
Bowel Regimen Addressed By ... StaffFellowNP/PARN
Patient Education Documented? YesNon/a (no needs identified, no change in rx, etc.)
Patient Education Documented By ... StaffFellowNP/PARN
Consistent with NCCN Guidelines? YesNo
Comments __________________________________

Comprehensive Pain Assessment – Best Practice 18
References
Abernethy, A. P., Samsa, G. P., & Matchar, D. B. (2003). A clinical decision and economic
analysis model of cancer pain management. American Journal of Managed Care, 9(10),
651-664.
AGREE Research Trust: Appraisal of Guidelines for Research & Evaluation II (AGREE II).
(2009). Retrieved from http://www.agreetrust.org/
Ackley, B. J., Swan, B. A., Ladwig, G. B., & Tucker, S. J. (2008). Evidence-based nursing care
guidelines: Medical-surgical interventions. St. Louis, MO: Mosby Elsevier.
Borneman, T., Koczywas, M., Sun, V., Piper, B. F., Smith-Idell, C., Laroya, B., . . . Ferrell, B.
(2011). Effectiveness of a clinical intervention to eliminate barriers to pain and fatigue
management in oncology. Journal of Palliative Medicine, 14(2), 197-205. doi:
10.1089/jpm.2010.0268
Borneman, T., Koczywas, M., Sun, V. C., Piper, B. F., Uman, G., & Ferrell, B. (2010). Reducing
patient barriers to pain and fatigue management. Journal of Pain and Symptom
Management, 39(3), 486-501. doi: 10.1016/j.jpainsymman.2009.08.007
Campbell, J. (2008). The effect of nurse champions on compliance with Keystone intensive care
unit sepsis-screening protocol. Critical Care Nursing Quarterly, 31(3), 251-269. doi:
10.1097/01.CNQ.0000325050.91473.0b
Deandrea, S., Montanari, M., Moja, L., & Apolone, G. (2008). Prevalence of undertreatment in
cancer pain: A review of published literature. Annals of Oncology, 19(12), 1985-1991.
doi: 10.1093/annonc/mdn419

Comprehensive Pain Assessment – Best Practice 19
DuBose, J. J., Nomoto, S., Higa, L., Paolim, R., Teixeira, P. G., Inaba, K., . . . Belzberg, H.
(2009). Nursing involvement improves compliance with tight blood glucose control in the
trauma ICU: A prospective observational study. Intensive and Critical Care Nursing,
25(2), 101-107. doi: 10.1016/j.iccn.2008.07.004
Duffy, M. E. (2005). Systematic reviews: Their role and contribution to evidence-based practice.
Clinical Nurse Specialist, 19(1), 15-17.
Dulko, D., Hertz, E., Julien, J., Beck, S., & Mooney, K. (2010). Implementation of cancer pain
guidelines by acute care nurse practitioners using an audit and feedback strategy. Journal
of the American Academy of Nurse Practitioners, 22(1), 45-55. doi: 10.1111/j.1745-
7599.2009.00469.x
Gracias, V. H., Sicoutris, C. P., Stawicki, S. P., Meredith, D. M., Horan, A. D., Gupta, R., . . .
Schwab, C. W. (2008). Critical care nurse practitioners improve compliance with clinical
practice guidelines in "semiclosed" surgical intensive care unit. Journal of Nursing Care
Quality, 23(4), 338-344. doi: 10.1097/01.NCQ.0000323286.56397.8c
Humphreys, J., Lee, K. A., Carrieri-Kohlman, V., Puntillo, K., Faucett, J., Janson, S., . . . Group,
U. S. o. N. S. M. F. (2008). Theory of Symptom Management. In M. J. Smith & P. R.
Liehr (Eds.), Middle range theory for nursing (2nd ed.) (pp. 145-158). New York, NY:
Springer Publishing Company.
Joint Commission. (2009). Comprehensive accreditation manual for hospitals: The official
handbook. Oakbrook Terrace, IL: Joint Commission Resources. Retrieved from
http://www.jointcommission.org/assets/1/18/pain_management.pdf

Comprehensive Pain Assessment – Best Practice 20
Lorenz, K. A., Dy, S. M., Naeim, A., Walling, A. M., Sanati, H., Smith, P., . . . Asch, S. M.
(2009). Quality measures for supportive cancer care: The Cancer Quality-ASSIST
Project. Journal of Pain and Symptom Management, 37(6), 943-964. doi:
10.1016/j.jpainsymman.2008.05.018
McNeill, J. A., Sherwood, G. D., & Starck, P. L. (2004). The hidden error of mismanaged pain:
A systems approach. Journal of Pain and Symptom Management, 28(1), 47-58. doi:
10.1016/j.jpainsymman.2003.11.005
Portenoy, R. K. (2000). Physical symptom management in the terminally ill. In H. M. C. W.
Breitbart (Ed.), Handbook of psychiatry in palliative medicine (pp. 99-129). New York,
NY: Oxford University Press.
Porter-O’Grady, T., & Malloch, K. (2011). Innovation Leadership. In T. Porter-O’Grady & K.
Malloch (Eds.), Quantum leadership: Advancing innovation, transforming health care
(3rd ed.) (pp. 143-164). Sudbury, MA: Jones and Bartlett.
Ripamonti, C. I., Bandieri, E., & Roila, F. (2011). Management of cancer pain: ESMO clinical
practice guidelines. Annals of Oncology, 22 Suppl 6, vi69-77. doi:
10.1093/annonc/mdr390
Sennfält, K., Carlsson, P., Sandblom, G., & Varenhorst, E. (2004). The estimated economic
value of the welfare loss due to prostate cancer pain in a defined population. Acta
Oncologica, 43(3), 290-296.
Swarm, R., Abernethy, A. P., Anghelescu, D. L., Benedetti, C., Blinderman, C. D., Boston, B., . .
. Weinstein, S. M. (2010). Adult cancer pain. Journal of the National Comprehensive
Cancer Network, 8(9), 1046-1086.

Comprehensive Pain Assessment – Best Practice 21
van den Beuken-van Everdingen, M. H., de Rijke, J. M., Kessels, A. G., Schouten, H. C., van
Kleef, M., & Patijn, J. (2007). Prevalence of pain in patients with cancer: A systematic
review of the past 40 years. Annals of Oncology, 18(9), 1437-1449. doi:
10.1093/annonc/mdm056
White, K. M., & Dudley-Brown, S. (Eds.). (2012). Translation of evidence into nursing and
health care practice. New York, NY: Springer Publishing Company.