n o t e - oilweb - corporate intranet portal standard...6 n o t e oisd publications are prepared for...
TRANSCRIPT
<< Back Home Next >>
6
N O T E
OISD publications are prepared for use in the oil and gas industry under the Ministry of Petroleum and Natural Gas. These are the properties of Ministry of Petroleum and Natural Gas and shall not be reproduced or copied or loaned or exhibited to others without written consent from OISD. Though every effort has been made to ensure the accuracy and reliability of the data contained in these documents, OISD hereby expressly disclaims any liability or responsibility for loss or damage resulting from their use. These documents are intended only to supplement and not to replace the prevailing statutory requirements.
7
F O R E W O R D Hydrocarbon processing and handling entails some risks arising out of potential hazards like fires, explosions, injuries/burns to the personnel etc. Most of such hazards are taken care, to a large extent, by better understanding, safer designs of the plants and other facilities and following safe operating practices. Oil Industry Safety Directorate (OISD), constituted by the Ministry of Petroleum and Natural Gas in 1986, have been bringing out Standards and Guidelines on various aspects of designing and operation of plants and facilities to improve safety standards in the oil industry. In the changed scenario of the economy, the oil industry too is becoming highly competitive and upgradation of technology is taking place around the world to achieve excellence. The successful application of a new technology depends greatly upon its successful adaptability. Such adaptability brings the "personnel". playing pivotal role in implementation of the technology, in the forefront. It is incontrovertible that personnel are most important resource of organisation and that maintaining their health is vital for productivity and effectiveness. As such, their health should be strongly emphasised in the organisation's strategic plan. Promotion of health of employees in the widest sense, should, therefore, be a high priority, both a goal and a challenge for the organisation. With a view to provide a structured programme to look after and promote the health of the vital "Human Resource" in the oil and gas industry, the present document "Guidelines for Occupational Health Monitoring in Oil and Gas Industry" has been prepared by the Functional Committee on Occupational Health Monitoring. It is hoped that these guidelines will help in establishing and practising an appropriate Occupational Health Monitoring programme for the employees of their industry. This document will be reviewed periodically for improvements based on the new experiences and better understanding. Suggestions from industry members may be addressed to :
The Coordinator Committee on Occupational Health Monitoring OIL INDUSTRY SAFETY DIRECTORATE
7TH FLOOR, NEW DELHI HOUSE 27, BARAKHAMBA ROAD
NEW DELHI - 110 001.

8
COMMITTEE ON OCCUPATIONAL HEALTH MONITORING ---------------------------------------------------------------------------------------------------------- NAME ORGANISATION ---------------------------------------------------------------------------------------------------------- LEADER Dr.V.Swaminathan Madras Refineries Limited, Chennai MEMBERS Dr. Hemant Kshirsagar Bharat Petroleum Corporn. Ltd., Mumbai Shri N Dasgupta Bharat Petroleum Corporn. Ltd., Mumbai Dr. P.K.Bhuyan Bongaigaon Refinery and Petrochemicals Limited, Bongaigaon Dr. John K John Cochin Refineries Limited, Cochin Dr. A. Biswas Gas Authority of India Limited, Vijaipur Shri K.K.Dixit Hindustan Petroleum Corporation Limited, Mumbai Shri A.A.Raichur Hindustan Petroleum Corporation Limited, Mumbai Dr. M.Ahmad Indian Oil Corporation Limited, Mathura Dr. A.K.Chakraborty Indian Oil Corporation Limited, Digboi Dr. R.P.Patel Indian Oil Corporation Limited, Vadodara [Alt:Dr.R.C.Saxena] Shri S. Kaul Indian Oil Corporation Limited, Vadodara Shri H.D.Bahadur Indian Oil Corporation Limited, Barauni Shri D.K.Kantak Lubrizol India Limited, New Mumbai Dr. A.K.Tomar Oil and Natural Gas Corporation Limited, Dehradun MEMBER-COORDINATOR Shri S.N.Mathur Oil Industry Safety Directorate, New Delhi ------------------------------------------------------------------------------------------------------ (In addition to the above, several other experts from the industry contributed in the preparation, review and finalisation of this document).
9
GUIDELINES FOR
OCCUPATIONAL HEALTH MONITORING IN OIL AND GAS INDUSTRY
I N D E X ------------------------------------------------------------------------------------------------------- SECTION CONTENT
------------------------------------------------------------------------------------------------------
1.0 INTRODUCTION
2.0 SCOPE 3.0 OCCUPATIONAL HEALTH MONITORING - OBJECTIVES 4.0 WORK ENVIRONMENTAL MONITORING - OCCUPATIONAL HYGIENE
4.1 THRESHOLD LIMIT VALUES
4.2 PHYSICAL HAZARDS 4.3 CHEMICAL HAZARDS 5.0 PRE-EMPLOYMENT/PRE- PLACEMENT MEDICALEXAMINATION 5.1 NORMS & STANDARDS FOR MEDICAL FITNESS 6.0 PERIODIC HEALTH EXAMINATION
6.1 BIOLOGICAL MONITORING 6.2 CLINICAL AND SCREENING LABORATORY TESTS 7.0 INFRASTRUCTURE FOR OCCUPATIONAL HEALTH MONITORING 8.0 REFERENCES -------------------------------------------------------------------------------------------------------
10
GUIDELINES FOR
OCCUPATIONAL HEALTH MONITORING
IN OIL AND GAS INDUSTRY
1.0 INTRODUCTION Technological advances while making the oil industry competitive, have also multiplied the hazards to the operating personnel in the form of complex processes and application of various hazardous chemicals. The enlightened management should consider that their duty is to preserve and promote the health of their employees and give them a good deal which in turn fosters better output and happiness in industry. Greater use of the assets of the work place - stability, long term relationships of trust and peer support can be advantageously utilised to make the work site as an effective and economical setting for various programmes designed to promote good health. The purpose of Occupational Health programme is to protect and promote the health of all employed persons. Occupational Health is not limited in scope only to diagnosis of specific occupational diseases and their treatment. It is necessary to consider not only the traditional specific hazards to health at work but also control of health problems of employees which are closely related to work conditions; are aggravated or influenced by work exposures; are susceptible to control or amelioration by interventions at work place. Occupational Health Monitoring will provide a scientific basis for decisions aimed at protection of human health from any possible adverse consequences of exposure to the hazards in the occupational environment.
2.0 SCOPE This document lays down minimum requirements for practising Occupational Health Monitoring in petroleum refineries, oil/gas production/processing plants, LPG bottling plants and other petroleum handling facilities/installations. This gives guidelines to establish Occupational Health Monitoring in the industry to provide specific level of occupational health and hygiene services to the employees and includes personal health of the individuals, the health of the occupational group, assessment of the employees' occupational environment and appraisal of the evidence linking job conditions and exposure to effect on health and course of the disease. Due to various reasons, if it is not possible to provide the required facilities of its own for the Occupational Health Monitoring at the petroleum handling facility / installation, the same should be arranged through outside agencies. 3.0 OCCUPATIONAL HEALTH
MONITORING OBJECTIVES Occupational Health Monitoring in the oil and gas industry should be viewed to meet the following objectives : (1) "Occupational Health Monitoring"
means a service established in or near to the place of employment for the purposes of -

7
(a) protecting the employees against any health hazard which may arise out of their work or the conditions in which it is carried on;
(b) contributing towards the
employees' physical and mental adjustment, in particular by the adaptation of the work to the employees and their assignment to jobs for which they are suited; and
(c) contributing to the establishment
and maintenance of the highest possible degree of physical and mental well-being of the employees.
(2) Occupational Health Monitoring
should be provided, as conditions require:-
(a) by virtue of laws or regulations; (b) by virtue of collective agreement
or as otherwise agreed upon by the employer and employees concerned; or
(c) in any other manner approved by
the competent authority after consultation with employers' and employees' organisations.
(3) Occupational Health Monitoring-
(a) should either be organised by the oil handling installations themselves or be attached to an outside body;
(b) should be organised -
(i) as a separate service within the
installation or
(ii) as a service common to a number of installations.
(4) Where the provision of
occupational health monitoring is not, for the time being, practicable for some reasons, the plant/installation should make arrangements with a physician or a local medical service for -
a) administering emergency
treatment; b) carrying out required medical
examinations ; c) to exercise monitoring over
hygiene conditions in the plant/installation.
(5) The role of occupational health
monitoring should essentially be preventive.
(6) Occupational health monitoring
should not be required to verify the justification of absence on grounds of sick-ness; they should not be precluded from ascertaining the conditions which may have led to an employee's absence on sick leave and obtaining information about the progress of the employee's illness, so that they will be better able to evaluate their preventive programme, discover occupational hazards and recommend the suitable placement of workers for rehabilitation purposes.
(7) The function of occupational health
monitoring should be progressively developed, in accordance with the

8
circumstances and having regard to the extent to which one or more of these functions are adequately discharged so that they will include in particular the following:
(a) Monitoring within the installation of all factors which
may affect the health of the employees through occupational hygiene monitoring, including periodic inspection and evaluation of workplaces to identify potential hazards, measure them when appropriate, suggest control measures as needed and advise in this respect to management and to employees or their representatives in the installation;
(b) job analysis or participation therein in the light of hygiene, physiological and psychological considerations and advice to management and employees on the best possible adaption of the job to the employee having regard to these considerations;
(c) participation, with the other
appropriate departments in the installation, in the prevention of accidents and occupational diseases and in the supervision of personal protective equipment and of its use, and advice to management and employees in this respect;
(d) monitoring of the hygiene of
sanitary installations and all other facilities for the welfare of the employees of the installation such as kitchens, canteens, day nurseries and rest homes and, as
necessary, monitoring of any dietetic arrangements made for the employees;
(e) pre-employment, periodic and
special medical examinations including, where necessary, biological, radiological examinations - considered advisable for preventive purposes by the industrial physician; such examinations should ensure particular monitoring over certain classes of employees, such as women employees exposed to special risks and handicapped persons;
(f) monitoring of the adaption of
jobs to employees, in particular handicapped employees, in accordance with their physical abilities, participation in the rehabilitation and retraining of such employees and advice in this respect;
(g) advice to management on the
occasion of the placing or re-assignment of employees;
(h) advice to individual employees at
their request regarding any disorder that may occur or be aggravated in the course of work;
(i) emergency treatment in case of
accident or indisposition, and also, in certain circumstances and in agreement with those concerned (including the employee's own physician), treatment for minor illness of employees who have not been absent from work or who have returned after absence ;

9
(j) Occupational Health Monitoring will play an important role of anticipating emergencies, of preparing policies for how to deal with them at the local level in collaboration with Safety, Fire and other services concerned and of having an input into disaster planning. In the event of fire, explosion, escape of toxic gases, chemicals etc., Occupational Health Monitoring will ensure the availability of the necessary infrastructure for emergency treatment to be administered.
(k) initial and regular subsequent
training of employees in first-aid and supervision and maintenance of first-aid equipment in co-operation, where appropriate, with other departments concerned;
(l) education of the personnel of the
installation in health and hygiene; (m) compilation and periodic review
of statistics concerning health conditions in the installation;
(n) research in occupational health or
participation in such research in association with specialised services or institutions.
(8) Occupational Health Monitoring
group should maintain close contact with the other departments in the installation concerned with issues of the employees' health, safety or welfare, and particularly the welfare department, the safety department, the personnel department, the trade union organisations in the installation,
safety and health committees and any other committee or any person in the installation dealing with health or welfare questions.
(9) Occupational Health Monitoring
Group should also maintain relations with external services and bodies dealing with issues of the health, safety, retraining, rehabilitation, reassignment and welfare of the employees.
(10) Occupational Health Monitoring
Group should open a confidential personal medical file at the time of an employee's pre-employment examination or first visit to occupational health centre and should keep the file up-to-date at each succeeding examination or visit.
Occupational Health Monitoring
Group should maintain appropriate records, so as to provide necessary information concerning the work of the services and the general state of health of the employees;
Occupational Health Group will
establish an efficient "Health Information System" through computerisation for storing and organising information on Occupational Hygiene ,medical records, exposure hazards of chemicals and locations of potential chemicals exposures.
(11) Occupational Health Monitoring
activities should be under the direction of a physician who will be directly responsible to the management for the same.
10
(12) The physicians in occupational Health Monitoring Group should enjoy full professional and moral independence of both the employer and the employees.
(13) The physician in charge of an
occupational health centre shall have special training in occupational health. He shall be familiar with industrial hygiene, special emergency treatment and occupational pathology, as well as with the laws and regulations governing the various duties of the service.
(14) The first-aid personnel should
a) consist exclusively of suitably
qualified persons ;
b) be readily available during working hours.
(15) The premises of occupational
Health Monitoring group should be adequately laid out.
(16) In order to efficiently perform
their functions, occupational health Monitoring group should -
(a) have free access to all work
places and to the ancillary installations ;
(b) inspect the work places at
appropriate intervals in co-operation, where necessary, with other services of the installation;
(c) have access to information
concerning the processes, performance standards and materials used or the use of which is contemplated;
(d) be authorised to undertake, or to request that approved technical bodies undertake-
i. surveys and investigations on
potential occupational health hazards, for example by the sampling and analysis of the atmosphere of work places, of the products and materials used, or of any other material suspected of being harmful;
ii. the assessment of harmful
physical agents;
(e) be authorised to request the competent authorities to ensure compliance with occupational health and safety standards.
(17) All persons attached to occupational Health Monitoring Group should be required to observe professional secrecy as regards both medical and technical information which may come to their knowledge in the exercise of the functions and activities as above.
(18) All employees and their
organisations should co-operate fully in attaining the objectives of occupational health services.
(19) The services provided by
occupational Health Monitoring Group in pursuance of these guidelines should not involve the employees any expense.

11
4.0 WORK ENVIRONMENTAL MONITORING-OCCUPATIONAL HYGIENE
Occupational hygiene is the science and art devoted to anticipation, identification, evaluation and control of environmental factors or stresses arising in or from the work place which may cause sickness, impaired health, significant discomfort or inefficiency among the employees. Occupational hygiene practice involves recognition of harmful exposure to hazards-heat, light, noise, radiation etc., chemicals-dust, fumes, gases etc. and to bring them under control, before the employees experience injury or evidence of any adverse signs or symptoms.
This will be done by measuring exposures, evaluating their probable effects by existing toxicological and hygienic standards and utilising sensitive biological examination of exposed persons to discover the entry of harmful materials into the human systems, in advance of any possible injury. The practice of occupational hygiene involves the qualitative and/or the quantitative evaluation of environmental agents which may pose health hazard at the work place.
The quantitative aspects of safe occupational exposures are expressed in the concepts of
Threshold Limit Values (TLV), a time weighted average exposure.
4.1 THRESHOLD LIMIT VALUES Threshold Limit Values refer to airborne concentrations of substances/levels of physical agents and represent conditions under which it is believed that nearly all the employees may be repeatedly exposed, day after day, without adverse effect. Because of wide variation in individual susceptibility, however, a small percentage of employees may experience discomfort from substances at concentrations at or below the TLV; a smaller percentage may be affected more seriously by aggravation of a pre-existing condition or by development of an occupational illness. Three categories of TLVs are specified as: 1. Threshold Limit Value -
Time Weighted Average (TLV-TWA) represents the time-weighted average concentration for a normal 8-hour workday and a 40 hour workweek, to which nearly all employees may be repeatedly exposed day after day without adverse effect.
2. Threshold Limit Value -
Short Term Exposure Limit (TLV-STEL) represents the concentration to which employees can be exposed continuously for a short period of time without suffering from

12
(1) irritation; (2) chronic or irreversible tissue change; (3) narcosis of sufficient degree to increase the likelihood of accidental injury, impair self rescue or materially reduce work efficiency and provided that the daily TLV-TWA also is not exceeded. A STEL is defined as a 15 minute time-weighted average exposure which should not be exceeded at anytime during a work day, even if the eight hour time weighted average is within the TLV. Exposures at the STEL should not be longer than 15 minutes and should not be repeated more than four times a day. There should be at least 60 minutes gap between successive exposures at the STEL.
3. Threshold Limit Value - Ceiling (TLV-C) represents the concentration that should not be exceeded even instantaneously. For some substances, e.g. irritant gases, only TLV-C may be relevant. For other substances, either two or three categories may be relevant, depending upon their physiological action. It is important to observe that if any one of the three categories TLVs is exceeded, a potential hazard is presumed to exist.
4.2 PHYSICAL HAZARDS 4.2.1 Evaluation of heat stress
Wet Bulb Globe Temperature (WBGT) index is a technique adopted to measure environmental heat stress. Portable WBGT instrument consisting of three separate resistance thermometers - globe thermometer to measure radiant energy, a wet bulb thermometer to measure relative humidity and a dry bulb thermometer to measure ambient temperature is made use of. By means of a switch, each thermometer can be individually read on a scale. A fourth position of the switch integrates the outputs of the three thermometers into a single reading WBGT index which is read on a separate scale. The operation is from line power or batteries. Threshold Limit Values for heat exposure are given in the Table - 4.1.

21
TABLE - 4.1
Permissible heat exposure threshold limit values
[Values are given in deg.C and (deg.F) WBGT] ------------------------------------------------------------------------------------------------------- Work Load ------------------------------------------------- Work-Rest Regimen Light Moderate Heavy ------------------------------------------------------------------------------------------------------- Continuous work 30.0(86) 26.7(80) 25.0(77) 75% Work 25% Rest, each hour 30.6(87) 28.0(82) 25.9(78) 50% Work 50% Rest, each hour 31.4(89) 29.4(85) 27.9(82) 25% Work 75% Rest, each hour 32.2(90) 31.1(88) 30.0(86) ------------------------------------------------------------------------------------------------------ 4.2.2 Evaluation of exposure to noise
A wide range of equipment is available for measurement of sound. The basic general purpose sound level meter measures the sound levels in decibles. Portable single hand-held battery powered precision integrating sound level meters are made use of for all kinds of sound level measurements including Leq., frequency analysis using a filter
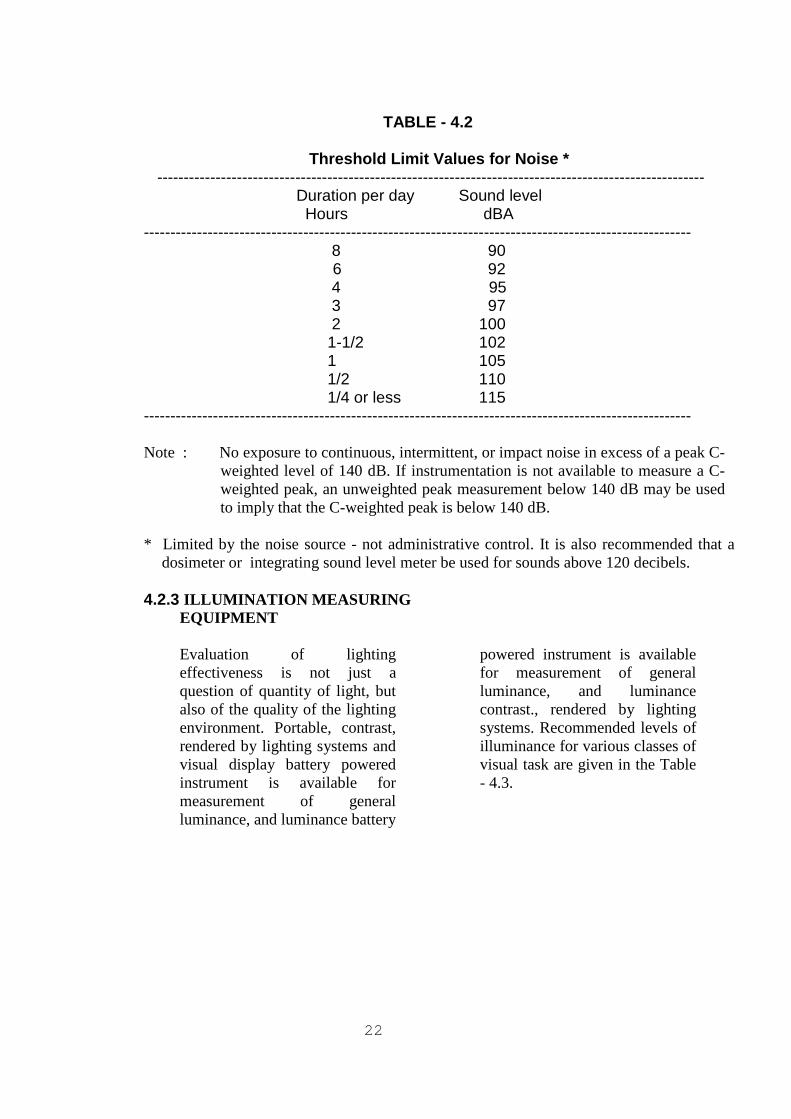
set. Personal noise dose meters worn by working personnel are made use of to get accurate assessment of the total noise dose the wearer has received throughout his working day. These instruments are easy to use, self contained pocket size units, battery powered with concealed or visible digital display for readout. Threshold Limit Values (TLVs) for Noise exposure are given in the Table 4.2.
22
TABLE - 4.2
Threshold Limit Values for Noise * ------------------------------------------------------------------------------------------------------- Duration per day Sound level Hours dBA ------------------------------------------------------------------------------------------------------- 8 90 6 92 4 95 3 97 2 100 1-1/2 102 1 105 1/2 110 1/4 or less 115 ------------------------------------------------------------------------------------------------------- Note : No exposure to continuous, intermittent, or impact noise in excess of a peak C-
weighted level of 140 dB. If instrumentation is not available to measure a C-weighted peak, an unweighted peak measurement below 140 dB may be used to imply that the C-weighted peak is below 140 dB.
* Limited by the noise source - not administrative control. It is also recommended that a
dosimeter or integrating sound level meter be used for sounds above 120 decibels.
4.2.3 ILLUMINATION MEASURING EQUIPMENT Evaluation of lighting effectiveness is not just a question of quantity of light, but also of the quality of the lighting environment. Portable, contrast, rendered by lighting systems and visual display battery powered instrument is available for measurement of general luminance, and luminance battery
powered instrument is available for measurement of general luminance, and luminance contrast., rendered by lighting systems. Recommended levels of illuminance for various classes of visual task are given in the Table - 4.3.

22
TABLE - 4.3 RECOMMENDED SERVICE ILLUMINANCE FOR VARIOUS CLASSES OF
VISUAL TASK -------------------------------------------------------------------------------------------------------- Class of Recommended Typical examples visual task illuminance(lx) -------------------------------------------------------------------------------------------------------- Exceptionally 2400 or more Inspection of minute work(e.g. difficult very small instruments) tasks Very difficult 1600 Extra-fine bench and machine
work, tool and die making (tolerances below 25 um); gauging and inspection of small or intricate parts.
1200 Inspection, examining and
handfinishing light goods. Difficult 800 Fine bench and machine work
(tolerances down to 25 um); inspection of fine work (e.g. calibrated scales, precision mechanisms and instruments).
Normal range 600 Office work with poor contrast of tasks and drawing offices-boards, fine workplaces painting, spraying and computer rooms-input and output terminals.
Moderately 400 Medium bench and machine difficult work (tolerances down to 125
mm); routine office work-typing, filing, reading, writing; inspection of medium work (e.g."Go" and "No Go" gauges, machine work; structural steel fabrication-marking off; enquiry desks
.
Ordinary 300 Training room, chalkboards and charts; pharmaceutical stores; kitchens - food preparation, cooking, washing up; staff canteens – counters.
Simple 200 Rough bench and machine work (tolerances above 750 um); rough visual inspection, counting, rough checking of stock parts; structural steel fabrication-general areas; entrance halls; waiting rooms; staff canteens-general.

23
-------------------------------------------------------------------------------------------------------- Class of Recommended Typical examples visual task illuminance(lx) ----------------------------------------------------------------------------------------------------- warehouses and bulk stores -
packing and despatch.
Rough inter- 100 Loading bays; office strong- mittent tasks rooms, staff change
rooms; locker rooms.
Movement and 50 Corridors with heavy traffic; orientation indoor carparks (lanes); walkways
and movement areas in industrial plant; stairs; rest rooms
20 Corridors with light traffic ---------------------------------------------------------------------------------------------------------- 4.2.4 Measurement of ionising radiation
There being no single instrument which performs acceptable under all conditions and requirements met with in practice; different types of instruments and detectors are used in various applications to obtain the monitoring characteristics required for different forms of radiation hazards. The radiation detection most widely used in survey instruments are isolation chambers, Geiger-Mueller counters,proportional counters and scintillation detectors. To assess the dose received by the individual, either film meters or Thermoluminescent dosimeters (TLD) or a combination of both are used for personal monitoring of exposure to external sources of radiation.
4.3 CHEMICAL HAZARDS
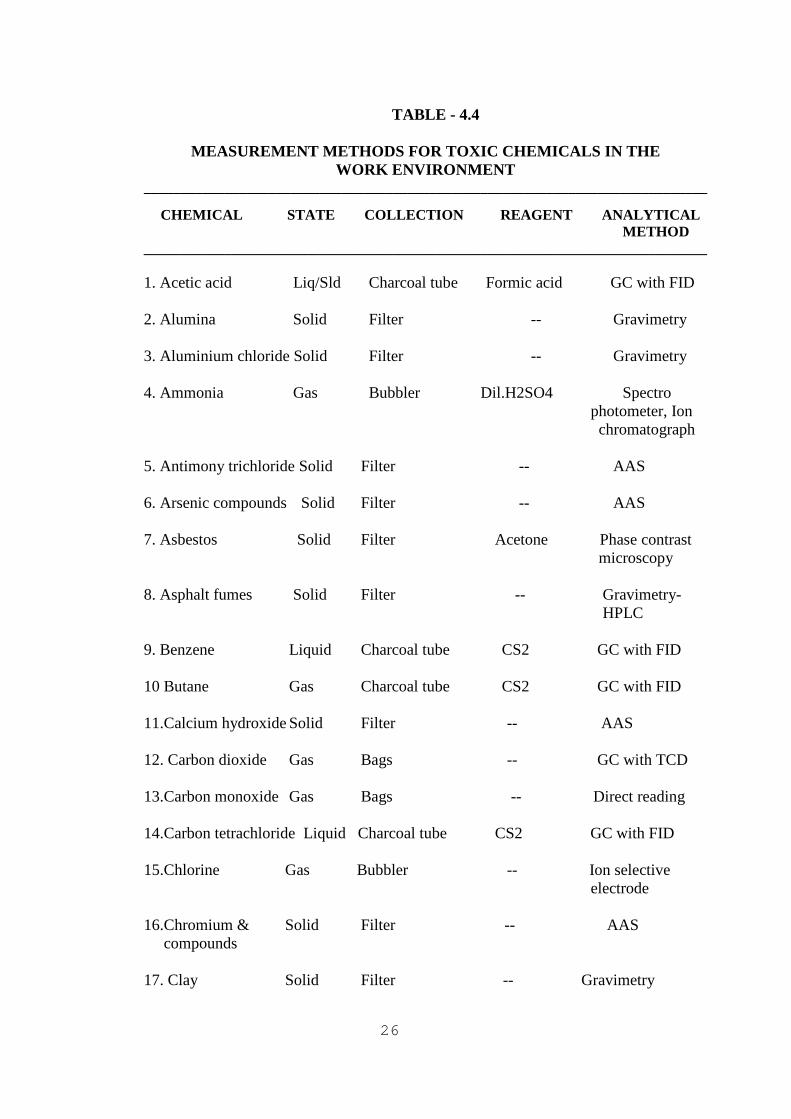
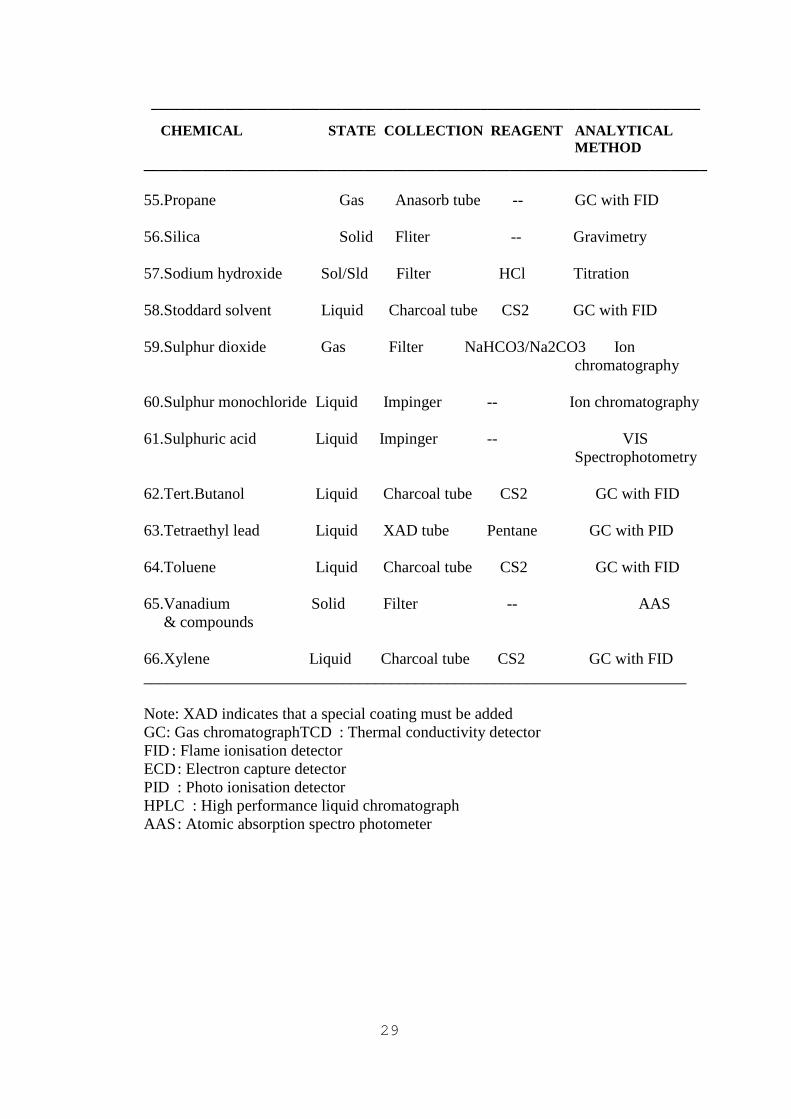
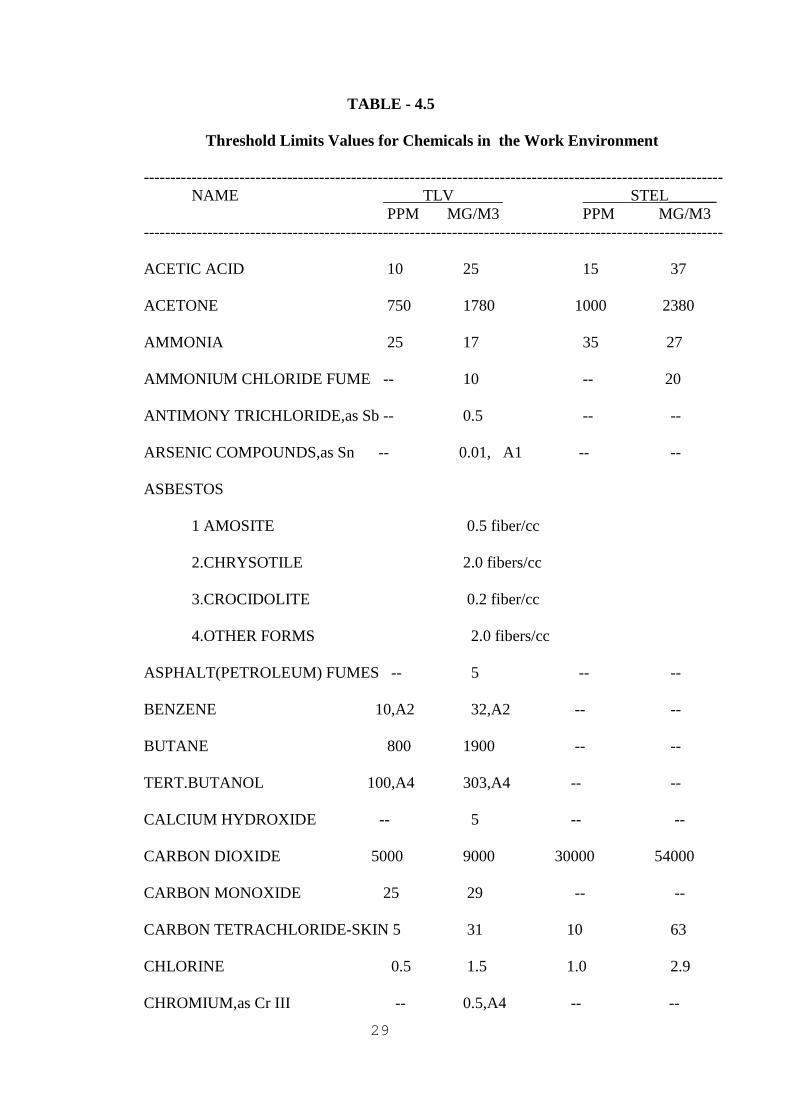
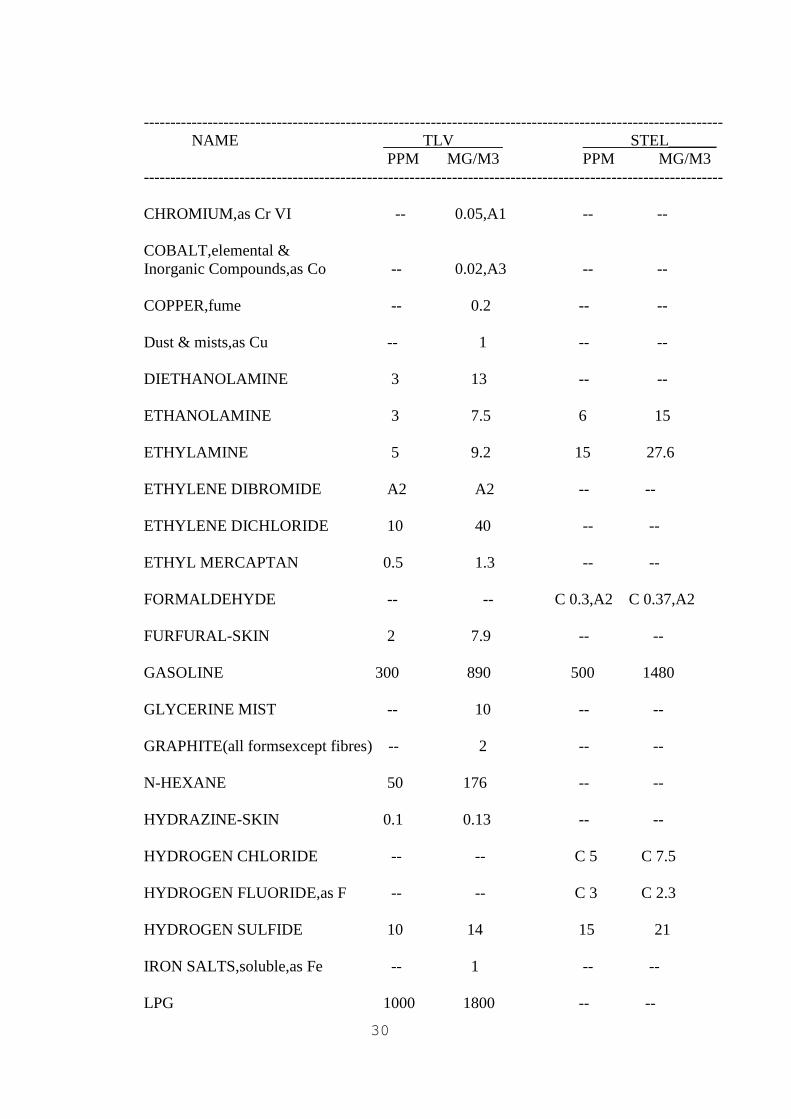
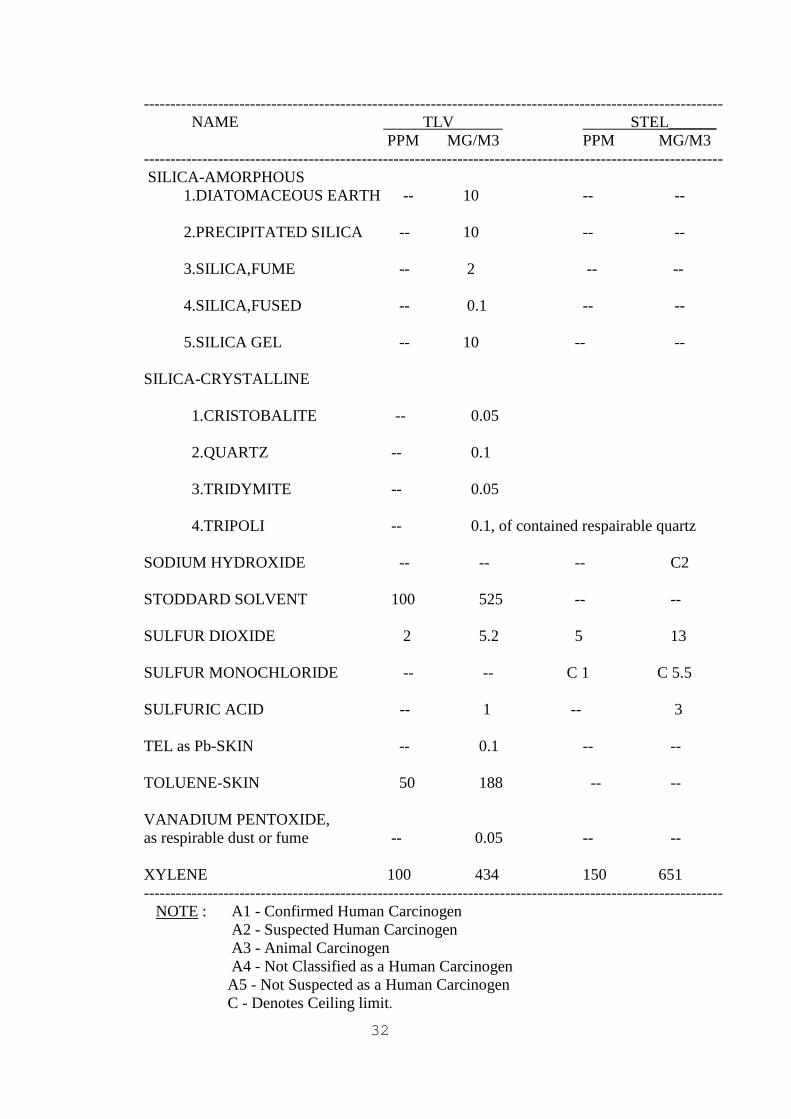
Hydrocarbon industry uses a variety of chemicals, organic and inorganic. These chemicals are used as absorbents, solvents, additives, catalysts, colouring agents, laboratory reagents etc. in the oil industry. All such chemicals, along with the petroleum, pose health hazards to the operating personnel. Chemicals have properties to cause personal injury due to contact with or entry into the body via inhalation, ingestion, skin contact or eye contact. Health hazard may result from repeated, chronic and long term exposure to low concentration of such chemicals. Measurement methods for toxic chemicals in the work environment are given in the Table - 4.4 and Threshold Limit Values for chemicals are given in the Table-4.5.
26
TABLE - 4.4
MEASUREMENT METHODS FOR TOXIC CHEMICALS IN THE WORK ENVIRONMENT
_____________________________________________________________________________
CHEMICAL STATE COLLECTION REAGENT ANALYTICAL METHOD _____________________________________________________________________________ 1. Acetic acid Liq/Sld Charcoal tube Formic acid GC with FID 2. Alumina Solid Filter -- Gravimetry 3. Aluminium chloride Solid Filter -- Gravimetry 4. Ammonia Gas Bubbler Dil.H2SO4 Spectro photometer, Ion chromatograph 5. Antimony trichloride Solid Filter -- AAS 6. Arsenic compounds Solid Filter -- AAS 7. Asbestos Solid Filter Acetone Phase contrast microscopy 8. Asphalt fumes Solid Filter -- Gravimetry- HPLC 9. Benzene Liquid Charcoal tube CS2 GC with FID 10 Butane Gas Charcoal tube CS2 GC with FID 11.Calcium hydroxide Solid Filter -- AAS 12. Carbon dioxide Gas Bags -- GC with TCD 13.Carbon monoxide Gas Bags -- Direct reading 14.Carbon tetrachloride Liquid Charcoal tube CS2 GC with FID 15.Chlorine Gas Bubbler -- Ion selective electrode 16.Chromium & Solid Filter -- AAS compounds 17. Clay Solid Filter -- Gravimetry

27
_____________________________________________________________________________
CHEMICAL STATE COLLECTION REAGENT ANALYTICAL METHOD _____________________________________________________________________________ 18. Cobalt & compounds Solid Filter -- AAS 19.Copper & compounds Solid Filter -- AAS 20.Diethanolamine Liquid Impinger -- Ion chromotography 21.Ethanolamine Liquid Silica gel tube -- GC with FID 22.Ethylamine Gas/Liq Silica gel tube H2SO4 GC with FID 23.Ethylene dibromide Liquid Charcoal tube CS2 GC with FID 24.Ethylene dichloride Liquid Silica gel tube CS2 GC with FID 25.Ethyl mercaptan Liquid Filter CS2 GC with ECD 26.Formalin Sol Filter/ Sodium VIS impinger bisulphide spectrophotometry 27.Furfural Liquid XAD tube Toluene GC with FID 28.Gasoline Liquid Charcoal tube CS2 GC with FID 29.Glycerin mist Liquid Filter -- Gravimetry 30.Graphite Solid Filter -- Gravimetry 31.Hexane Liquid Charcoal tube CS2 GC with FID 32.Hydrazine Liquid Bubbler HCl VIS Spectrophotometry 33.Hydrogen chloride Liquid Silica gel NaHCO3/Na2CO3 Ion chromatography 34.Hydrogen fluoride Liquid Filter -- Ion selective electrode 35.Hydrogen sulphide Gas Dry tube/mole- -- Thermal desorpt- cular sieve ion & GC with FID 36.Iron & compuonds Solid Filter -- AAS

28
_____________________________________________________________________________
CHEMICAL STATE COLLECTION REAGENT ANALYTICAL METHOD _____________________________________________________________________________ 37.LPG Gas Detector tube -- Direct reading instrument 38.Methanol Liquid Silica gel Water GC with FID 39.MEK Liquid Ambersorb CS2 GC with FID Tube 40.Methyl t-butyl Liquid Charcoaltube -- GC with FID ether 41.MIBK Liquid Charcoal tube Acetone GC with FID 42.Molybdenum Solid Filter -- AAS & compounds 43.Morpholine Liquid Silica gel tube H2SO4/NaOH GC with FID 44.Naphtha Liquid Charcoal tube CS2 GC with FID 45.Nickel & compounds Solid Fliter -- AAS 46.Nitric acid Liquid Silica gel tube -- Ion chromotography 47.Nitric oxide Gas Molecular seive -- Ion chromotography 48.Nitrogen dioxide Gas Molecular seive -- Ion chromotography 49.Oil mist Liquid Filter -- Gravimetry 50.Pentane Gas Charcoal tube CS2 GC with FID 51.Phenol Sol/Sld XAD tube Methanol HPLC 52.Phosgene Gas Impinger tube -- VIS spctrophotometry 53.Phosphoric acid Liquid Silica gel tube -- Ion chromotograph 54.Poly nuclear Liquid Filter -- GC with FID aromatic compound
29
___________________________________________________________________________
CHEMICAL STATE COLLECTION REAGENT ANALYTICAL METHOD _____________________________________________________________________________ 55.Propane Gas Anasorb tube -- GC with FID 56.Silica Solid Fliter -- Gravimetry 57.Sodium hydroxide Sol/Sld Filter HCl Titration 58.Stoddard solvent Liquid Charcoal tube CS2 GC with FID 59.Sulphur dioxide Gas Filter NaHCO3/Na2CO3 Ion chromatography 60.Sulphur monochloride Liquid Impinger -- Ion chromatography 61.Sulphuric acid Liquid Impinger -- VIS Spectrophotometry 62.Tert.Butanol Liquid Charcoal tube CS2 GC with FID 63.Tetraethyl lead Liquid XAD tube Pentane GC with PID 64.Toluene Liquid Charcoal tube CS2 GC with FID 65.Vanadium Solid Filter -- AAS & compounds 66.Xylene Liquid Charcoal tube CS2 GC with FID ____________________________________________________________________ Note: XAD indicates that a special coating must be added GC : Gas chromatographTCD : Thermal conductivity detector FID : Flame ionisation detector ECD : Electron capture detector PID : Photo ionisation detector HPLC : High performance liquid chromatograph AAS : Atomic absorption spectro photometer
29
TABLE - 4.5
Threshold Limits Values for Chemicals in the Work Environment
------------------------------------------------------------------------------------------------------------- NAME TLV STEL______ PPM MG/M3 PPM MG/M3 ------------------------------------------------------------------------------------------------------------- ACETIC ACID 10 25 15 37 ACETONE 750 1780 1000 2380 AMMONIA 25 17 35 27 AMMONIUM CHLORIDE FUME -- 10 -- 20 ANTIMONY TRICHLORIDE,as Sb -- 0.5 -- -- ARSENIC COMPOUNDS,as Sn -- 0.01, A1 -- -- ASBESTOS 1 AMOSITE 0.5 fiber/cc 2.CHRYSOTILE 2.0 fibers/cc 3.CROCIDOLITE 0.2 fiber/cc 4.OTHER FORMS 2.0 fibers/cc ASPHALT(PETROLEUM) FUMES -- 5 -- -- BENZENE 10,A2 32,A2 -- -- BUTANE 800 1900 -- -- TERT.BUTANOL 100,A4 303,A4 -- -- CALCIUM HYDROXIDE -- 5 -- -- CARBON DIOXIDE 5000 9000 30000 54000 CARBON MONOXIDE 25 29 -- -- CARBON TETRACHLORIDE-SKIN 5 31 10 63 CHLORINE 0.5 1.5 1.0 2.9 CHROMIUM,as Cr III -- 0.5,A4 -- --
30
------------------------------------------------------------------------------------------------------------- NAME TLV STEL______ PPM MG/M3 PPM MG/M3 ------------------------------------------------------------------------------------------------------------- CHROMIUM,as Cr VI -- 0.05,A1 -- -- COBALT,elemental & Inorganic Compounds,as Co -- 0.02,A3 -- -- COPPER,fume -- 0.2 -- -- Dust & mists,as Cu -- 1 -- -- DIETHANOLAMINE 3 13 -- -- ETHANOLAMINE 3 7.5 6 15 ETHYLAMINE 5 9.2 15 27.6 ETHYLENE DIBROMIDE A2 A2 -- -- ETHYLENE DICHLORIDE 10 40 -- -- ETHYL MERCAPTAN 0.5 1.3 -- -- FORMALDEHYDE -- -- C 0.3,A2 C 0.37,A2 FURFURAL-SKIN 2 7.9 -- -- GASOLINE 300 890 500 1480 GLYCERINE MIST -- 10 -- -- GRAPHITE(all formsexcept fibres) -- 2 -- -- N-HEXANE 50 176 -- -- HYDRAZINE-SKIN 0.1 0.13 -- -- HYDROGEN CHLORIDE -- -- C 5 C 7.5 HYDROGEN FLUORIDE,as F -- -- C 3 C 2.3 HYDROGEN SULFIDE 10 14 15 21 IRON SALTS,soluble,as Fe -- 1 -- -- LPG 1000 1800 -- --

31
------------------------------------------------------------------------------------------------------------- NAME TLV STEL______ PPM MG/M3 PPM MG/M3 ------------------------------------------------------------------------------------------------------------- METHANOL-SKIN 200 262 250 328 MEK 200 590 300 885 METHYL t-BUTYL ETHER 40,A3 144,A3 -- -- MIBK 50 205 75 307 MOLYBDENUM,as Mo Soluble compounds -- 5 -- -- Insoluble compounds -- 10 -- -- MORPHOLINE-SKIN 20 71 -- -- NAPHTHA 300 1370 -- -- NICKEL Metal -- 1 -- -- Insoluble compds.as Ni -- 1 -- -- Soluble compds. as Ni -- 0.1 -- -- NITRIC ACID 2 5.2 4 10 NITRIC OXIDE 25 31 -- -- NITROGEN DIOXIDE 3 5.6 5 9.4 OIL MIST,MINERAL -- 5 -- 10 PENTANE 600 1770 750 2210 PHENOL-SKIN 5 19 -- -- PHOSGENE 0.1 0.40 -- -- PHOSPHORIC ACID -- 1 -- 3 PROPANE (TWA-OSHA: 1000 ppm ; IDLH:20000 ppm)
32
------------------------------------------------------------------------------------------------------------- NAME TLV STEL______ PPM MG/M3 PPM MG/M3 ------------------------------------------------------------------------------------------------------------- SILICA-AMORPHOUS 1.DIATOMACEOUS EARTH -- 10 -- -- 2.PRECIPITATED SILICA -- 10 -- -- 3.SILICA,FUME -- 2 -- -- 4.SILICA,FUSED -- 0.1 -- -- 5.SILICA GEL -- 10 -- -- SILICA-CRYSTALLINE 1.CRISTOBALITE -- 0.05 2.QUARTZ -- 0.1 3.TRIDYMITE -- 0.05 4.TRIPOLI -- 0.1, of contained respairable quartz SODIUM HYDROXIDE -- -- -- C2 STODDARD SOLVENT 100 525 -- -- SULFUR DIOXIDE 2 5.2 5 13 SULFUR MONOCHLORIDE -- -- C 1 C 5.5 SULFURIC ACID -- 1 -- 3 TEL as Pb-SKIN -- 0.1 -- -- TOLUENE-SKIN 50 188 -- -- VANADIUM PENTOXIDE, as respirable dust or fume -- 0.05 -- -- XYLENE 100 434 150 651 ------------------------------------------------------------------------------------------------------------- NOTE : A1 - Confirmed Human Carcinogen A2 - Suspected Human Carcinogen A3 - Animal Carcinogen A4 - Not Classified as a Human Carcinogen
A5 - Not Suspected as a Human Carcinogen C - Denotes Ceiling limit.
33
5.0 PRE-EMPLOYMENT / PRE-PLACEMENT MEDICAL EXAMINATION
GUIDELINES FOR DETERMINING THE MEDICAL FITNESS OF A CANDIDATE CONSIDERED FOR PRE-EMPLOYMENT / PLACEMENT IN THE SERVICES OF THE COMPANY
(1) Every candidate shall be required to undergo medical examination to be eligible for appointment in the services of the company :
a) On a permanent or temporary
basis; b) As an apprentice/trainee; c) An employee in the services
of the company who is selected for alternative job on the basis of open recruitment or otherwise;
d) On deputation basis or
permanent from Central/State Governments/Public Sector Undertakings.
(2) Medical examination will be
conducted by the Company Medical Officer/Authorised Medical Officer who will be the authority to certify a candidate as medically fit/ unfit/ temporarily unfit in respect of all appointments in the company.
(3) It may become necessary to
refer the candidates to some outside hospitals/institutions for conducting some of the medical tests.
(4) The company medical authority
may,at his discretion,obtain the opinion of a Specialist that will
be duly recorded on the medical examination forms.
(5) The report of the company
medical authority is considered final.
(6) The company medical authority
will forward the medical fitness certificate to the Personnel department, declaring the candidate either "FIT", "UNFIT" or "TEMPORARILY UNFIT".
(7)Where a candidate has been
declared "Temporarily Unfit" by reasons of short term sickness, which is curable within a period of not more than thirty days, the candidate will be required to undergo a re-examination within thirty days from the date of his/her being declared "Temporarily Unfit". At the time of re-examination, he/she will be required to produce proof of treatment and certificate of cure from the Doctor who treated him/her. On satisfying himself that the short term sickness is cured, the Company Medical Authority will certify the candidate as medically fit.
(8) Where a candidate is declared
"Unfit", the result of the medical examination for unfitness will be communicated to him/her by the personnel department.
(9) Where a handicapped person is
selected, he/she may be declared "handicapped, but fit" if,
(a) Except for the handicap,he/she
otherwise satisfies all other physical standards as prescribed and
34
(b) Considering the nature of
duties and responsibilities of the job, location, hazard, strain and other factors, the handicap is not likely to interfere with the performance of duties of the post with reasonable efficiency and without possible deterioration of his/her health.
5.1 NORMS AND STANDARDS FOR
MEDICAL FITNESS
(1) Good mental and bodily health and a fit constitution.
(2) Free from physical defect or
abnormality, congenital or acquired, likely to interfere with the efficient performance of duties.
(3) No evidence of mal-development -
physical or mental. (4) Joints and locomotor functions are
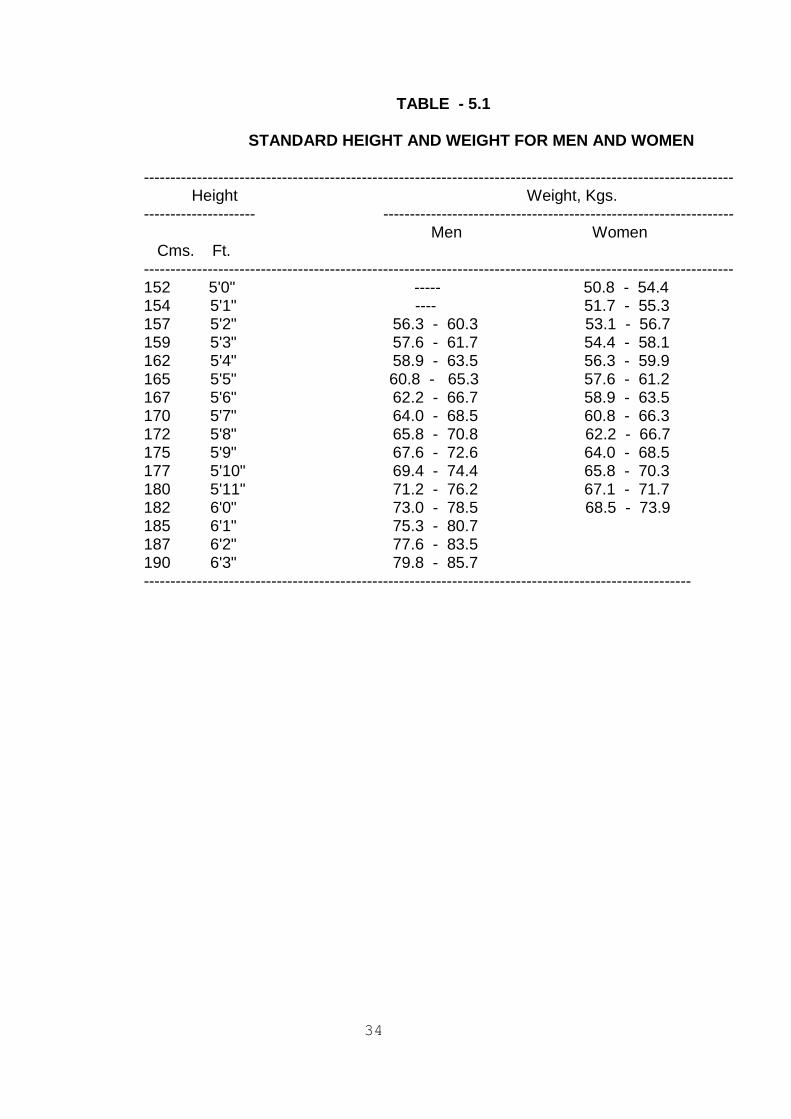
within normal limits. (5) HEIGHT AND WEIGHT Standard for height and weight
is given in the Table - 5.1.Weight will be recorded in kilograms and height measured will be in centimeters. The Company Medical Authority is empowered to relax the standards of height and weight, so long as such relaxation does not impede the performance of the job.
34
TABLE - 5.1 STANDARD HEIGHT AND WEIGHT FOR MEN AND WOMEN --------------------------------------------------------------------------------------------------------------- Height Weight, Kgs. --------------------- ------------------------------------------------------------------ Men Women Cms. Ft. --------------------------------------------------------------------------------------------------------------- 152 5'0" ----- 50.8 - 54.4 154 5'1" ---- 51.7 - 55.3 157 5'2" 56.3 - 60.3 53.1 - 56.7 159 5'3" 57.6 - 61.7 54.4 - 58.1 162 5'4" 58.9 - 63.5 56.3 - 59.9 165 5'5" 60.8 - 65.3 57.6 - 61.2 167 5'6" 62.2 - 66.7 58.9 - 63.5 170 5'7" 64.0 - 68.5 60.8 - 66.3 172 5'8" 65.8 - 70.8 62.2 - 66.7 175 5'9" 67.6 - 72.6 64.0 - 68.5 177 5'10" 69.4 - 74.4 65.8 - 70.3 180 5'11" 71.2 - 76.2 67.1 - 71.7 182 6'0" 73.0 - 78.5 68.5 - 73.9 185 6'1" 75.3 - 80.7 187 6'2" 77.6 - 83.5 190 6'3" 79.8 - 85.7 -------------------------------------------------------------------------------------------------------

35
(6) CHEST Acceptable chest measurement at
full expiration will be 79 cms. (relaxable by 5 cms.) and minimum expansion of 5 cms. The range of expansion upto 4 cms. ( i.e. a deviation of 20%) will be acceptable. This is not applicable to female candidates and the state of physical development will be taken into account.
(7) EYE The candidate's eyes will be
tested and the result of the test recorded in accordance with the following rules:
(a) The candidate's eyes will be subjected to a general examination directed to detect any disease or abnormality. The candidate will be rejected if he/she suffers from morbid condition of eyes, eyelids or contiguous structures of such a nature as would render him/her unfit for service at the time of appointment or at a future date.
(b) If any candidate is suspected to
have any refractive error in either or both eyes, organic or progressive disease of any part of the eyes, a thorough ophthalmic checkup and report from the specialist in ophthalmology is essential.
(c) VISUAL ACUITY
Standard of visual acuity with or without glasses will be as follows:- ------------------------------------------------------------------------------------------------------------- Distance visual acuity Near visual acuity Age Better eye Worse eye Better eye Worse eye ----------------------------------------------------------------- --------------------------------------- Below 6/9 (20/30) 6/9 (20/30) 35 yrs or Sn 0.6 Sn 0.6 6/6 (20/13) 6/12 (20/40) (20/15) (20/17) (20/18) (20/20) 35 yrs. 6/12 (20/40) 6/12 (20/40) & above or Sn 0.8 Sn.0.8 6/9 (20/30) 6/18 (20/50) -------------------------------------------------------------------------------------------------------
Any organic disease or a progressive refractive error which is likely to result in lowering of the visual acuity will be considered as a disqualification.
(d) FUNDUS EXAMINATION (i) In case of myopia, fundus
examination should be carried out and the report from the specialist is essential. In the event of a pathological
34
condition being present, which is likely to be progressive and affect the efficiency of the candidate, he/she will be declared unfit.
The total amount of myopia
(including the cylinder) shall not exceed (-) 4.00 D. The total amount of hypermetropia (including the cylinder) shall not exceed (+) 4.00 D in each eye.
(ii) Fundus and media should be
healthy and within normal limits.
(iii) No degenerative signs of
vitreous or choriorentinitis to be present, suggesting progressive myopia.
(e) COLOUR VISION The testing of colour is essential
for all candidates. Colour vision will be tested with Ishihara's Isochromatic plates in good light.
COLOUR BLINDNESS
(i) PERMISSIBLE This will not be a
disqualification for such jobs wherein defective colour vision is not likely to interfere with his/her work or create risk for others working with him/her; for example, employment in Personnel, Finance, Administration, Training & HRD departments.
(ii) NOT PERMISSIBLE
Colour blindness is a
disqualification for the following jobs like employment
in Manufacturing, Maintenance, Technical Services, R & D, Projects, Medical departments; Refinery Operator, Refinery Technician, Operator, Chemist, Draughtsman, Crane Operator, Driver of all categories, Nurse, Nursing Assistants, Fireman, Security, Engineer, Doctor, Materials Management, etc., and jobs where perception of colours is considered essential.
(f) SQUINT For technical category where the
presence of binocular vision is essential, squint, even if the visual acuity is of prescribed standards, will be considered as a disqualification. For others, the presence of squint will not be considered as a disqualification if the visual acuity of each eye is of prescribed standard.
(g) ONE EYED PERSON For regular service, one eyed
individual will be considered as unfit except for ministerial and allied jobs where binocular vision is not considered essential. It will be ensured that the prognosis of the functioning eye is good and its vision is not likely to be endangered by the condition of the worse eye and the prescribed visual acuity standards are fully satisified.
(h) CONTACT LENSES Use of contact lenses for
correction will be accepted for employment only for such jobs as personnel, finance, administration, training & HRD, etc.
35
(i) NIGHT BLINDNESS No standard test for testing of
night blindness or dark adaptation is prescribed. The medical officer will record visual acuity with reduced illumination or by making the candidate recognize various objects in a dark room after he/she has been there for 20 to 30 minutes.
(8) EAR /NOSE/THROAT The candidate should be free
from signs or symptoms of ear diseases. Audiometric screening to measure the pure tone air conduction hearing threshold will be carried out. Impairment of hearing acuity in one or both ears, perforated ear drum, chronic ear discharge, etc., will be considered as disqualification. A report from the specialist in ENT is essential and should be duly recorded.
A candidate should be free from
any active disease of the nose. Throat, palate, gums, jaws,
temporomandibular joints and dentition should be within normal limits.
(9) BLOOD PRESSURE (B.P.) The normal limits of blood
pressure will be assessed as: Normotension < 140 SBP
and <90 DBP. Candidates diagnosed as a case of hypertension will be declared unfit.
(10) GLANDS There should not be generalised
enlargement of lymph glands.
Scars, if any, of the previous removal of tubercular glands should be normal and there must not have been any active disease.
(11) SKIN DISEASE Candidates suffering from
leprosy or chronic inveterate skin conditions will be declared unfit. Vitiligo cases are acceptable.
(12) VENEREAL DISEASES Candidates who have suffered or
are suffering from venereal diseases will not be declared fit unless detailed examination of urethral smear and serological test proves negative.
(13) FITS Candidates suffering from
epilepsy (seizure disorder) will be declared unfit.
(14) PREGNANCY If at the time of medical
examination a candidate is pregnant, she will be declared temporarily unfit until she has completed six weeks after confinement/miscarriage and the candidate will be required to undergo a medical examination of fitness.
(15) Signs of mental retardation will
render a candidate unfit for employment.
(16) DEFECTS Congenital or acquired defects, if
any/noticed, will be recorded on the medical examination forms, with a clear opinion as to whether it is likely to interfere with the
36
efficient performance of the duties for which the candidate is under consideration for employment.
(17) SYSTEMIC EXAMINATION Examination of all systems is
very essential to rule out any pathological condition which will make a candidate unfit for employment (eg. hypertension, diabetes mellitus, heart disease, tuberculosis, bronchial asthma, fits (seizure disorder), malignant disease, potentially malignant conditions, renal failure, collagen disease, cerbrovascular insufficiency, parkinsonism, schizophrenia, glaucoma, diseases of the retina, cataract, psoriasis, etc.
(18) RADIOLOGICAL EXAMINATION Skiagram chest of all the
candidates will be essentially required. Cases diagnosed as suffering from pulmonary tuberculosis will be declared unfit.
(19) The content of the medical
examination usually includes a medical history, occupational history, clinical examination supplemented by laboratory tests. The laboratory tests that will be performed include TC; DC; Hb; ESR; Platelets; HCT; RBC; Blood group & Rh; Blood sugar(Random); Glucose Tolerance test if required; Serum Creatinine; Blood R.P.R, (Rapid Plasma Reagin test)/V.D.R.L. for serodiagnosis of syphilis; test for detection of antibodies to HIV 1 & HIV 2 in blood; test for detection of hepatitis B surface antogen (HBs Ag) in blood; test
for pregnancy (detection of human chorionic gonadatrophin (HCG) in the urine), (for women candidates); routine urine examination; Eye examination tests for colour vision, visual acuity etc; Pulmonary function tests-spirometry; Pure tone airconduction audiometry; Electrocardiogram-all leads (at rest); X ray chest PA view. The candidates who require further clinical evaluation/additional tests will be referred to the concerned specialists.
6.0 PERIODIC HEALTH EXAMINATION The periodic examination should
be carried out at regular intervals after the initial preplacement examination. It may not always be necessary to conduct a full-scale medical examination at the routine periodic check-ups, especially if there are no overt signs of illness.
The procedure for periodic health
checks is different from that for preplacement examinations. A special form needs to be designed, with emphasis on the aspects of the history and physical examination most relevant to the exposure in question. The scope and periodicity of the health examination should depend on the nature and extent of the risk involved. The examination should focus on the body organs and systems most likely to be affected by the harmful agents in the workplace. For example, audiometry is the most important test for those working in a noisy environment. For each harmful agent, the period between

37
exposure and the development of a health impairment (latency period) is a major factor in determining the frequency of examination. However, in many cases the latency period is not known. For such agents, the frequency should be determined on the basis of: (a) the natural history of the disease, including the rapidity with which the biochemical, morphological behavioural, etc. changes might occur or be detected by screening tests; (b) the level of exposure to the hazardous agent and to any other interacting agent or agents; (c) the anticipated susceptibility of the exposed population and individuals.
6.1 BIOLOGICAL MONITORING Measurement of the
concentration of substances in breathing zone air does not ensure that the employee is totally protected from adverse health effects resulting from exposure to chemicals in the workplace. The actual body burden of the chemical resulting from all routes of exposure is more directly related to potential adverse health effects. The uptake of the workplace chemical by the inhalation route, absorption of the chemical through the skin or the gastrointestinal tract and non occupational exposure to the chemical all influence the body burden. Interaction of the chemical with other environmental and workplace chemicals may stimulate or inhibit its metabolism and elimination and thus influence the toxicity of the chemical in the employee. Thus, the
environmental concentration of a chemical is related to the body burden of the same chemical under specified conditions only. To further evaluate a potential health hazard in the workplace, biological monitoring should be used.
Biological monitoring can be
defined as assessment of employee exposure by measurement of some "index" chemical in a body fluid as evidence of exposure to a chemical.
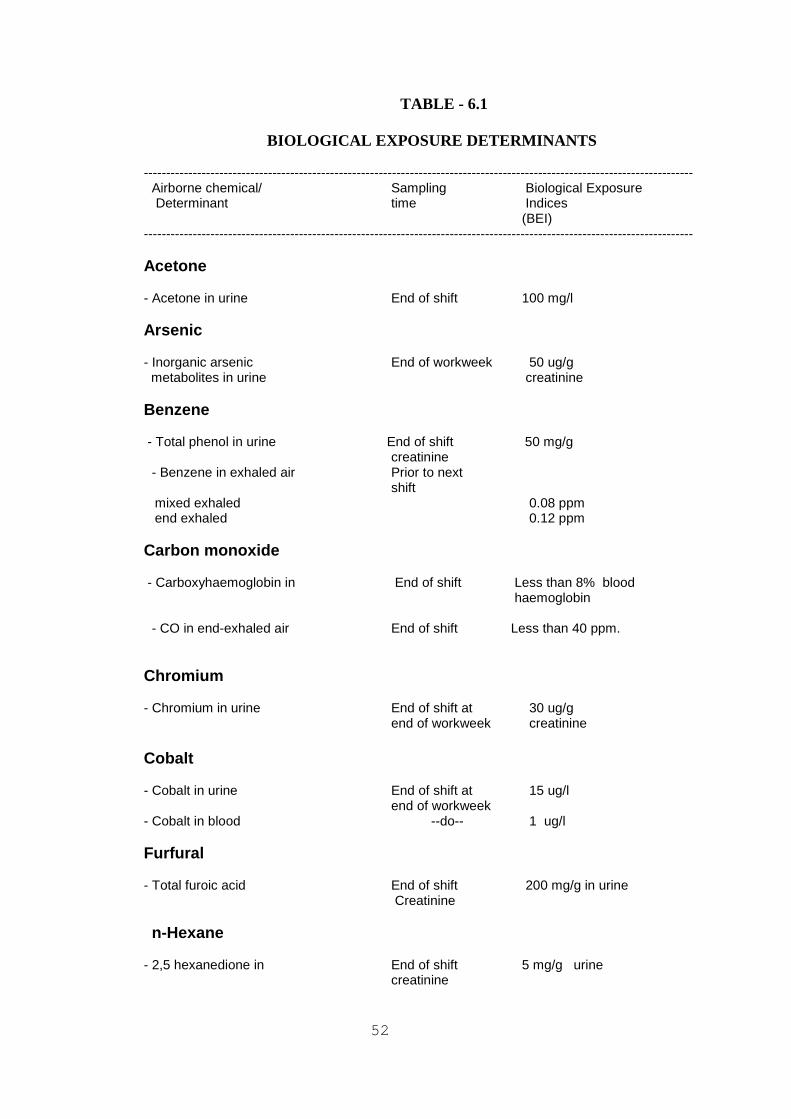
The Biological Exposure Index
(BEI) is defined as an "index" chemical that appears in a biological fluid or in expired air following an exposure to a workplace chemical. The BEI serves as a warning of exposure by (1) the appearance of chemical or (2) the appearance of biological response indicative of exposure. The BEI is primarily an index of exposure and not a sentinel of some health effect that may have been produced from exposure to a workplace chemical. Permissible Biological Exposure Indices for various chemicals are given in the Table - 6.1. (Table - 6.4 may be referred to regarding periodicity of the examination).
52
TABLE - 6.1
BIOLOGICAL EXPOSURE DETERMINANTS
---------------------------------------------------------------------------------------------------------------------------- Airborne chemical/ Sampling Biological Exposure Determinant time Indices (BEI)
---------------------------------------------------------------------------------------------------------------------------- Acetone - Acetone in urine End of shift 100 mg/l Arsenic - Inorganic arsenic End of workweek 50 ug/g metabolites in urine creatinine Benzene - Total phenol in urine End of shift 50 mg/g
creatinine - Benzene in exhaled air Prior to next
shift mixed exhaled 0.08 ppm end exhaled 0.12 ppm Carbon monoxide - Carboxyhaemoglobin in End of shift Less than 8% blood
haemoglobin - CO in end-exhaled air End of shift Less than 40 ppm.
Chromium - Chromium in urine End of shift at 30 ug/g end of workweek creatinine Cobalt - Cobalt in urine End of shift at 15 ug/l end of workweek - Cobalt in blood --do-- 1 ug/l Furfural - Total furoic acid End of shift 200 mg/g in urine
Creatinine n-Hexane
- 2,5 hexanedione in End of shift 5 mg/g urine
creatinine

53
----------------------------------------------------------------------------------------------------------------------------
Airborne chemical/ Sampling Biological Exposure Determinant time Indices (BEI)
---------------------------------------------------------------------------------------------------------------------------- Lead
- in blood not critical 50 ug/100ml - in urine not critical 150 ug/g Creatinine - Zinc protoporphyrin After one month 100ug/100 ml in blood exposure blood. Methanol - Methanol in urine End of shift 15 mg/l Methemoglobin inducers - Methaemoglobin in During or end of 1.5% of blood shift haemoglobin
Methyl ethyl ketone - MEK in urine End of shift 2 mg/l. MIBK - MIBK in urine End of shift 2 mg/l Naphtha - Phenol in urine End of shift 50 mg/g creatinine Phenol - Total phenol in urine End of shift 250 mg/g Creatinine PNA compounds - Phenol in urine End of shift 50 mg/g creatinine Toluene - Hippuric acid End of shift 2.5 g/g in urine Creatinine - Toluene in End of shift 1 mg/l venous blood
54
----------------------------------------------------------------------------------------------------------------------------
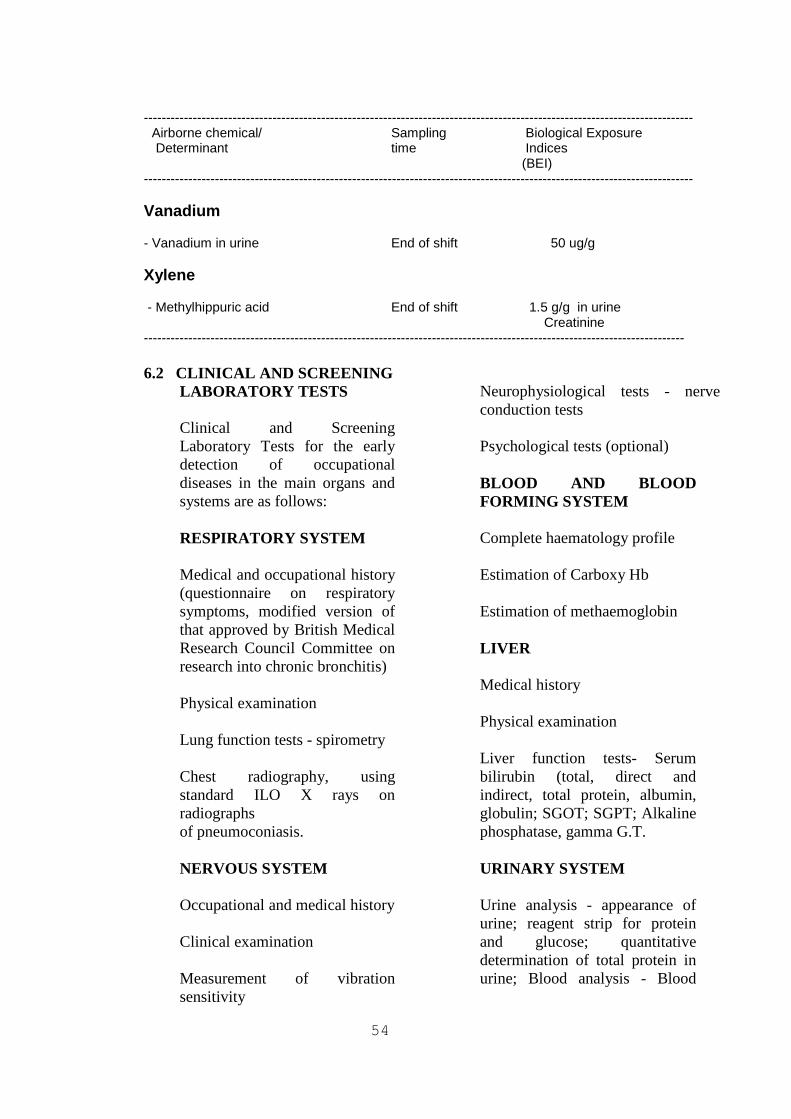
Airborne chemical/ Sampling Biological Exposure Determinant time Indices (BEI)
----------------------------------------------------------------------------------------------------------------------------
Vanadium - Vanadium in urine End of shift 50 ug/g Xylene - Methylhippuric acid End of shift 1.5 g/g in urine
Creatinine -------------------------------------------------------------------------------------------------------------------------- 6.2 CLINICAL AND SCREENING
LABORATORY TESTS Clinical and Screening
Laboratory Tests for the early detection of occupational diseases in the main organs and systems are as follows:
RESPIRATORY SYSTEM Medical and occupational history
(questionnaire on respiratory symptoms, modified version of that approved by British Medical Research Council Committee on research into chronic bronchitis)
Physical examination Lung function tests - spirometry Chest radiography, using
standard ILO X rays on radiographs
of pneumoconiasis. NERVOUS SYSTEM Occupational and medical history Clinical examination Measurement of vibration
sensitivity
Neurophysiological tests - nerve
conduction tests Psychological tests (optional) BLOOD AND BLOOD
FORMING SYSTEM Complete haematology profile Estimation of Carboxy Hb Estimation of methaemoglobin LIVER Medical history Physical examination Liver function tests- Serum
bilirubin (total, direct and indirect, total protein, albumin, globulin; SGOT; SGPT; Alkaline phosphatase, gamma G.T.
URINARY SYSTEM Urine analysis - appearance of
urine; reagent strip for protein and glucose; quantitative determination of total protein in urine; Blood analysis - Blood
53
urea, creatinine, Beta 2 microglobulin
CARDIOVASCULAR
SYSTEM Medical history Clinical examination 12-lead ECG - at rest and
computerised stress ECG; 24 hour holter monitoring if
required at work place; Chest radiograph MUSCULOSKELETAL
SYSTEM
Medical history Physical examination Radiography of skeletal system,
if required. Various Biochemistry and
Haematological Tests alongwith the normal range of values are given in the Table - 6.2.
Table - 6.3 gives Analytical
Techniques for Biochemical Parameters.
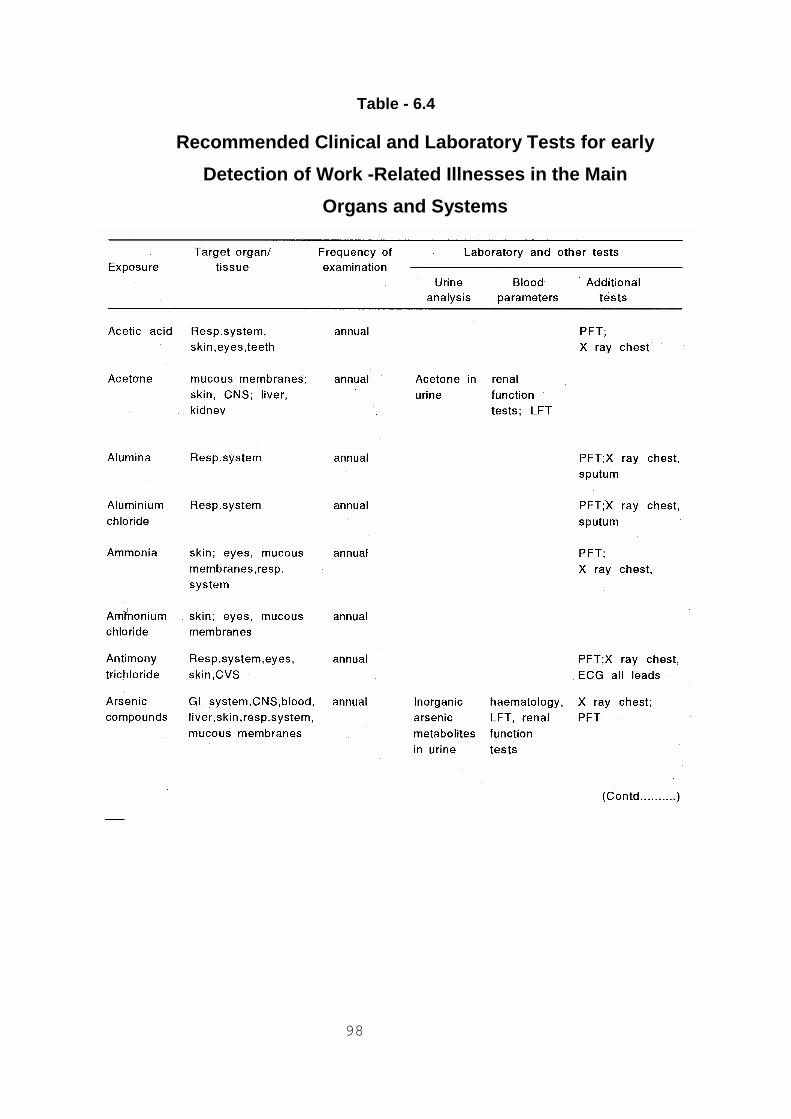
Recommended Clinical Laboratory
Tests for early detection of work related illness in the main organ and system are given in the Table - 6.4.

53
Table - 6.2
BIOCHEMISTRY AND HAEMATOLOGY TESTS ------------------------------------------------------------------------------------------------------- Parameter Findings Normal Range ------------------------------------------------------------------------------------------------------- GTT: Whole Blood Sugar (75 gms of glucose) (F) : mg/dl upto 100 mg/dl (1 Hour) : mg/dl upto 180 mg/dl (2 Hour) : mg/dl upto 120 mg/dl Blood Sugar (PP) : mg/dl upto 140 mg/dl Blood Sugar (R) : mg/dl upto 140 mg/dl Urea : mg/dl 10 - 40 mg/dl Creatinine : mg/dl 0.5 - 1.2 mg/dl Uric acid : mg/dl 3.0 - 7.6 mg/dl Total Cholesteral : mg/dl 120 - 240 mg/dl Triglycerides : mg/dl 10 - 170 mg/dl HDL Cholesterol : mg/dl 30 - 70 mg/dl LDL Cholesterol : mg/dl 120 - 180 mg/dl Ratio of Total Chol./HDL Chol : upto 4.5 Bilirubin Total : mg/dl 0.2 - 1.0 mg/dl Direct : mg/dl 0.1 - 0.4 mg/dl Indirect : mg/dl Total Protein : g/dl 6.0 - 8.0 g/dl Albumin : g/dl 3.5 - 5. g/dl Globulin : g/dl SGOT : u/l 5.0 - 40 u/l SGPT : u/l 5.0 - 37 u/l Alkaline Phosphatase : u/l 60 - 170 u/l Gamma GT : u/l 5 - 37 u/l Calcium : mg/dl 8.4 - 10.4 mg/dl

54
------------------------------------------------------------------------------------------------------- Parameter Findings Normal Range ------------------------------------------------------------------------------------------------------- Sodium : mmol/l 135 - 155 mmol/l Potassium : mmol/l 3.5 - 5.5 mmol/l Chloride : mmol/l 98 - 109 mmol/l Glycosylated Hb : % 4.5 - 8.0 % HAEMATOLOGY Total WBC Count : cells/cumm Differental Count : Haemoglobin : g/dl Total RBC : million cells/cumm HCT : % ESR : 1/2 Hour: mm, 1 Hour: mm Platelets : lakhs MCV : Cu.u MCH : uugm MCHC : % Blood Group : Rh Factor : SEROLOGY VDRL/RPR : HbsAg : URINE Specific Gravity : Colour : Appearence : Reaction : Sugar (F) : (1 Hour) : (2 Hour) : (PP) : (R) :
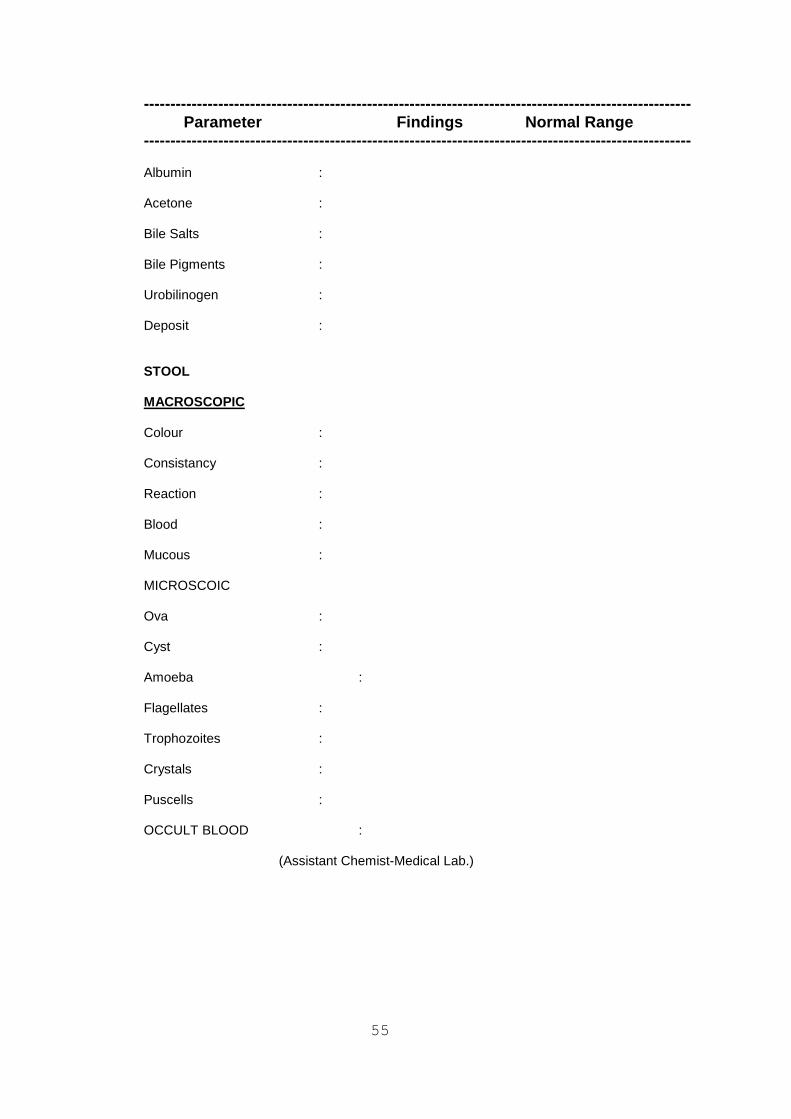
55
------------------------------------------------------------------------------------------------------- Parameter Findings Normal Range ------------------------------------------------------------------------------------------------------- Albumin : Acetone : Bile Salts : Bile Pigments : Urobilinogen : Deposit : STOOL MACROSCOPIC Colour : Consistancy : Reaction : Blood : Mucous : MICROSCOIC Ova : Cyst : Amoeba : Flagellates : Trophozoites : Crystals : Puscells : OCCULT BLOOD : (Assistant Chemist-Medical Lab.)

97
Table - 6.3 ANALYTICAL TECHNIQUES FOR BIOCHEMICAL PARAMETERS ------------------------------------------------------------------------------------------------------- Parameter Method ------------------------------------------------------------------------------------------------------- Glucose Enzymatic(Glucose Oxidase/peroxidase Urea Enzymatic (Urease) Creatinine Alkaline piruvate method Uric acid Enzymatic (Uricase-P-aminophenazone) Cholesterol Enzymatic(Cholesterol esterase- cholesterol oxidase-peroxidase) Triglycerides Enzymatic(Glycerol-3,phosphate oxidase p-amino antipyrine) HDL Enzymatic (phospho tungstate-p, amino antipyrine Total protein Biuret method Albumin Bromo cresol green method Bilirubin T&D Jendrassik-Grof method SGOT UV Kinetic SGPT UV Kinetic Alk. Phosphate P-nitro phenyl phosphate method Gama GT Szasz method Sodium Kinetic/Flame photometry Potassium Kinetic/Flame photometry Chloride Kinetic/Flame photometry Calcium Spectrophotometry -------------------------------------------------------------------------------------------------------
98
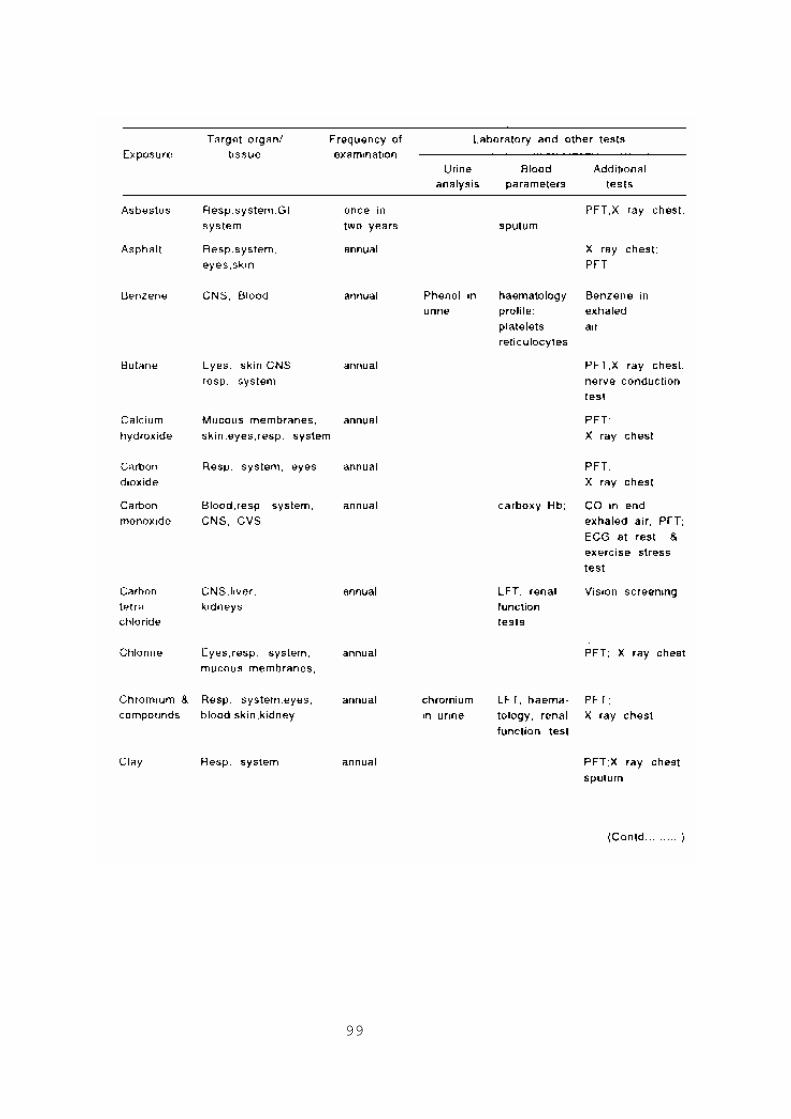
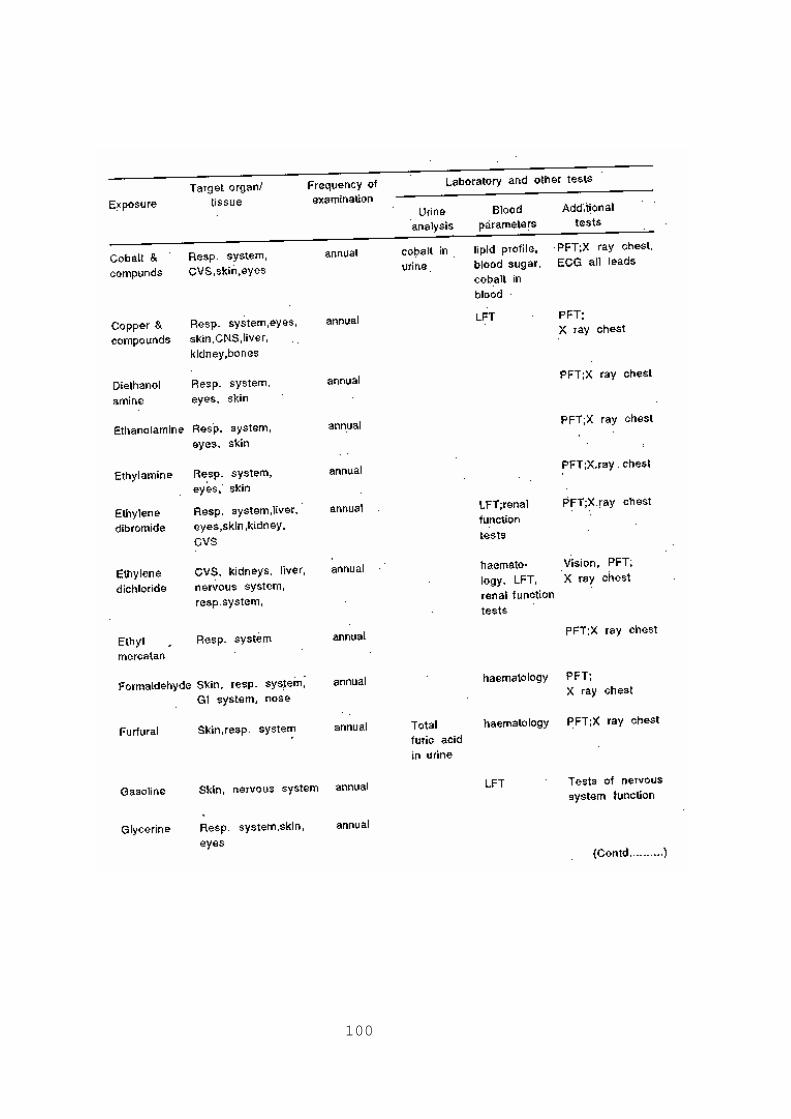
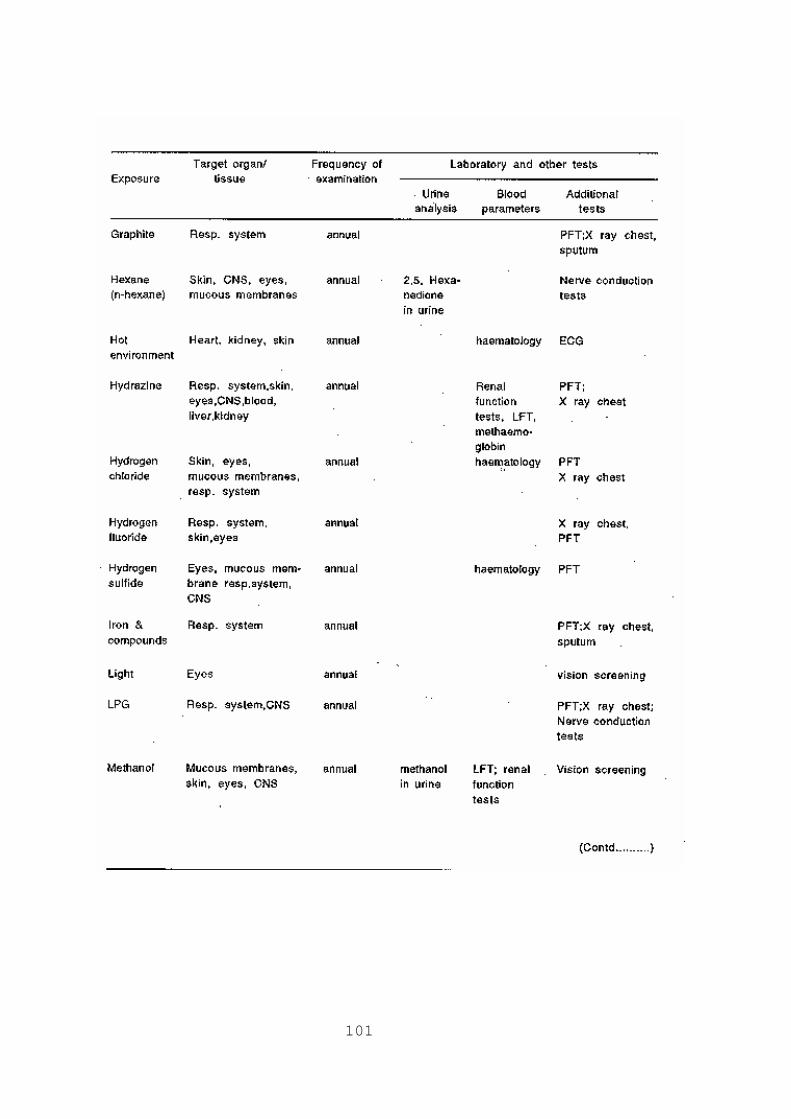
Table - 6.4
Recommended Clinical and Laboratory Tests for early
Detection of Work -Related Illnesses in the Main
Organs and Systems
99
100
101

102

103

104
7.0 INFRASTRUCTURE FOR OCCUPATIONAL HEALTH MONITORING
For effective implementation of
the occupational health Monitoring group in the oil industry, occupational health centre should be provided with the minimum of following facilities :
(1) Building Oil industry will make available
premises to adequately house Occupational Health Monitoring Facilities with necessary provisions for power and water supplies, air conditioning, access and other indispensable facilities. The functional units of Occupational Health Monitoring will include occupational medicine, occupational hygiene and toxicology, biochemistry, health education, health statistics and emergency medical care.
(2) Man Power
(i) Occupational Health Physician One full time medical doctor
for employees upto 1000, preferably a specialist in occupational health/public health or adequately trained in occupational medicine for a minimum period of three months, recognised by the Government, or a minimum experience of 3 years in an industrial setting/a large hospital. The doctor will be incharge of Occupational Health Monitoring to ensure administrative supervision of all the staff and responsible for all the activities of Occupational Health Monitoring.

98
(ii) Occupational Hygienist One Occupational Hygienist
having educational background with a graduate degree in chemistry/ physics/ environmental toxicology and experience in occupational hygiene practice.
(iii) Occupational Health Nurse One Nurse for employees upto
1500-2000; he/she will have educational background with a degree in B.Sc.(Nursing) or Diploma in general nursing of 3 years duration and midwifery of 6 months duration and a minimum experience of 3 years in an industrial set-up or recognised hospital.
(iv)Medical laboratory technologist One Medical laboratory
technologist for employees upto 1500.He/She will have educational background with a degree in B.Sc (Biochemistry)/Medical Lab. Technology/Chemistry, and with diploma in clinical pathology laboratory and a minimum experience of 3 years in a clinical pathological laboratory in an industrial or large hospital. Experience with the use of auto analyzer and automated haematology testing equipment is desirable.
(v) Others The Occupational Health
Monitoring Group will have adequate number of paramedical and administrative staff.
(3) Equipment The equipment will comprise of
medical diagnostic equipment, toxicology laboratory and sampling equipment and occupational hygiene field testing equipment. Occupational Health Monitoring Group should also be equipped with technical books and periodicals etc. Some of the equipment required are given below :
Occupational Hygiene and
Toxicology Unit (i) Wet Bulb Globe Temperature
(WBGT) instrument - for evaluation of heat stress.
(ii) Sound level meter with Octave
filter set and impulse noise meter,Acoustic calibrator and Personal noise dose meter - for evaluation of exposure to noise
(iii)Luxmeter - for illumination
measurement. (iv)Direct reading instrument
intrinsically safe portable infra-red analyzer; Direct reading colorimetric tubes- short term, long term; Intrinsically safe,battery operated personal sampling pumps with suitable media for collection (liquid media samplers, solid - sorbent tubes etc.; for gases and vapour.
(v):Intrinsically safe, battery
operated personal sampling pumps with suitable media for collection - filters, cyclones etc - for Particulate matter.
<< Back Home Next >>