mutants genetic variation in human development lecture 8 fall 2006 bennington college
TRANSCRIPT

MUTANTSgenetic variation in human development
Lecture 8
Fall 2006Bennington College

Some Disorders linked to bone growth
cleidocranial dysplasia
thanatophoric dysplasia
sclerosteosis
fibrodysplasia ossificans progressiva (FOP)
pseuodoachondroplasia
achondroplasia
osteogenesis imperfecta
osteoporosis
osteopetrosis
pycnodysostosis

cleidocranial dysplasia
A rare condition inherited as an autosomal dominant trait and characterized by partial or complete absence of the clavicles, defective ossification of the skull, and faulty occlusion due to missing, misplaced, or supernumerary teeth.

cleidocranial dysplasia
Current evidence suggestscause is mutation in theCbfa1 transcription factor(Core binding factor 1)
Bone is always a “work in progress” - not a static entity
Bone is derived from the same embryonic tissues that makethe flesh surrounding bones (connective tissue, muscle)
all derived from the mesoderm
Osteogenesis - the formation of bones

Two major modes of osteogenesis:
intramembranous ossification - direct conversion of tissue into bone; this is how flat bones, such as the cranium,are formed.
endochondral ossification - cells first differentiate intoa cartilage intermediate which is later replaced by bone;this is how long bones, such as the femur and humerus, are formed

Intramembranous ossification: layer of osteoblasts secrete a proteinmatrix. Calcium phosphate forms on this matrix and then encloses the osteoblasts (at which point they become osteocytes)
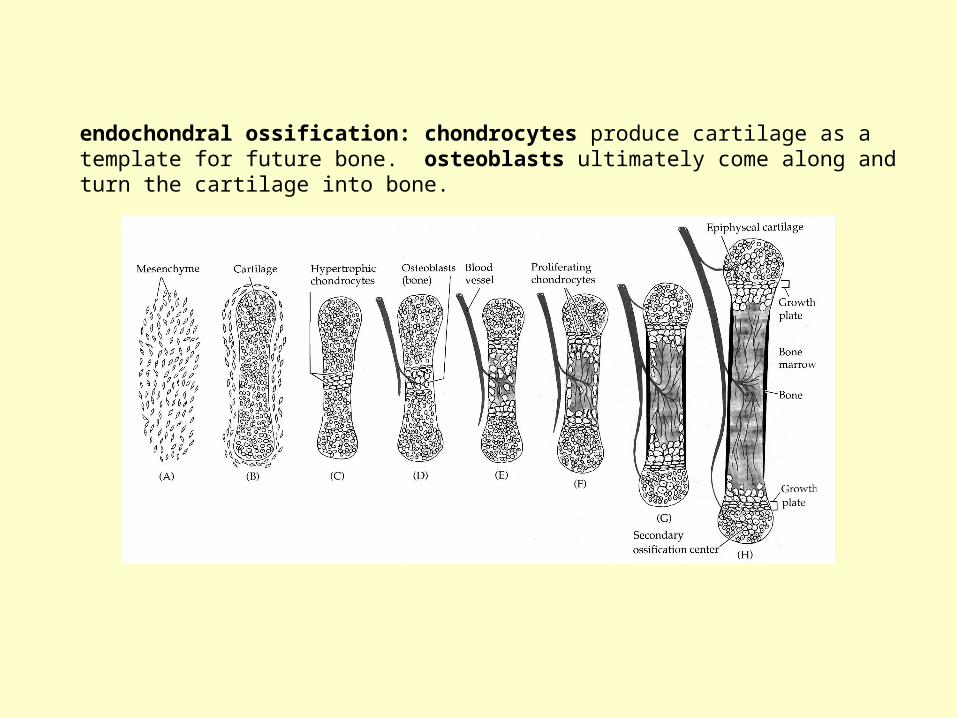
endochondral ossification: chondrocytes produce cartilage as a template for future bone. osteoblasts ultimately come along andturn the cartilage into bone.

zoom-in of endochondral ossification

Back to the role of cbfa1 in cleidocranial dysplasia…Cbfa1 is a transcription factor that promotes the differentiation of bone-producing cells (osteoblasts and chondrocytes) from mesoderm (mesenchymal cells)

If you have one mutant copy of Cbfa1, the result is cleidocranial dysplasia
If you have two mutant copies of Cbfa1, the result is death immediatelyfollowing birth…
Defective Cbfa1 means defective bone formation - no bones and all cartilage means no ribs to support the ability of the lungs to expandand contract - this results in asphyxiation.

endochondral ossification is what results from theobserved “condensations” during embryogenesis.
what tells these condensations that they will becomebone is BMP (bone morphogenetic protein)
BMP tells the mesenchymal cells (cells from the mesoderm)to become bone instead of muscle or connective tissue

you may recall, earlier in embryogenesis, BMP was tellingthe developing embryo to form front, not back (while nogginwas telling it to form back, not front)
Noggin
BMP4
Later in life if we get a fracture - BMP4 will appear and say “make bone”
Basically, BMPs can induce bone wherever they are…

Chiba et al., Histological study of effect of bone morphogenetic protein derived from bovine tooth on periosteum in rats. Journal of Bone and Mineral Metabolism. 8(3): 24-29. 1990.
control injection into femur
BMP injection into femur

Too little bone is a problem…too much bone is also a problem
Sclerosteosis - a rare, potentially lethal, autosomal recessive, progressive sclerosing (hardening) bone dysplasia with characteristic facial and skeletal features.
Usually results in massive, thick skulls
May become lethal if excess bone crushes a vital nerve

Figure 1. Lateral view of a patient from the Brazilian sclerosteosis family showing the characteristic high forehead and the protruding large chin.
Balemans et al. Increased bone density in sclerosteosis is due to the deficiency of a novel secreted protein (SOST). Human Molecular Genetics 10(5): 537-543, 2001.
Identified a gene, SOST (sclerostin), thatis the cause of sclerosteosis.
sclerostin is a negative regulator of BMPs.

B
B
BMP4
BMP4
BMP4
BMP4
A
SOSTSOST
SOST
SOST
SOST
SOST

B
B
BMP4
BMP4
BMP4
BMP4
A
go make bone now!
fibrodysplasia ossificans progressiva (FOP)
An extremely rare disease (~250 worldwide cases known)in which connective tissue and muscle tends to ossify(turn into bone) over time. Also, any injury is repaired with osteoblasts, increasing bone formation. Ultimatelyleads to complete immobilization of the patient.
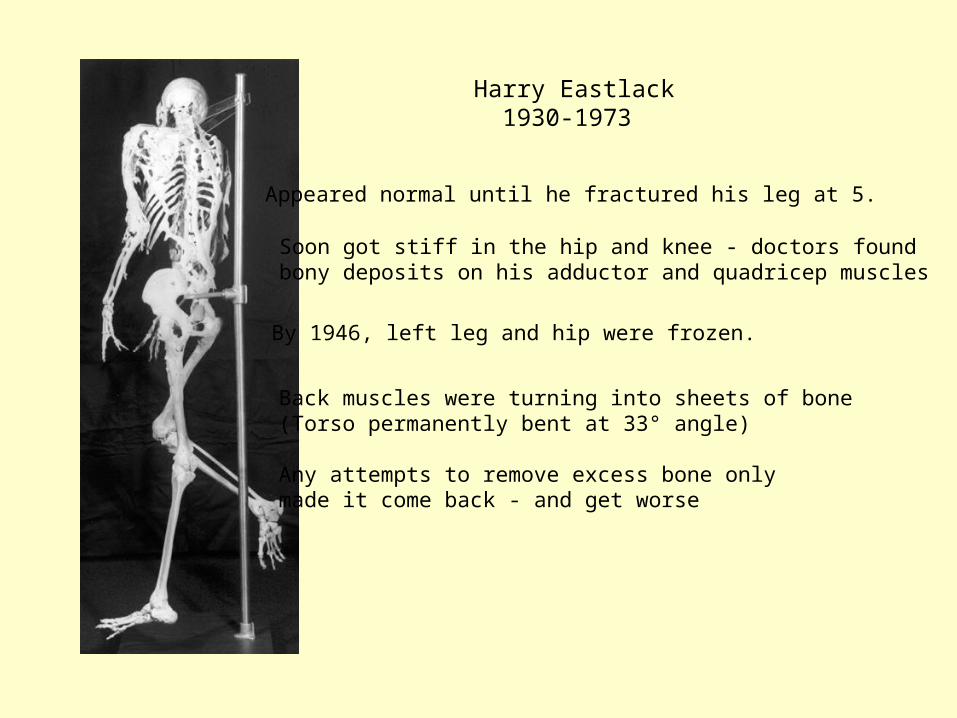
Harry Eastlack 1930-1973
Appeared normal until he fractured his leg at 5.
Soon got stiff in the hip and knee - doctors foundbony deposits on his adductor and quadricep muscles
By 1946, left leg and hip were frozen.
Back muscles were turning into sheets of bone(Torso permanently bent at 33° angle)
Any attempts to remove excess bone only made it come back - and get worse

By the age of 23 his jaws had entirely seized upand he could only partake of a liquid diet.Had to be institutionalized for care.

At the time of his death (due to pneumonia) he could move only his lips. Donated his body to science.


Victor Chandler Twitty 1901-1967
Twitty aimed to discover where the information governing limb growth came from
Experiment: Use a larger species and a smaller species of salamander. Chop off a limb from each.When the limb bud regenerates, excise it and transplant it to the other salamander.
What happens? Does the donor (and therefore the limb bud) control the ultimate size of the limb?
Or does information from the host (hormones,other signaling pathways) tell the limb what sizeit should become for that particular species?

Results of Twitty’s limb bud grafting experiment
The limb bud graftedfrom the donor containedall the information togovern the ultimate sizeof the limb.
The host, and thereforethe host’s hormones,did not influence thisprocess.

Twitty thus demonstrated local control of bone growth
But how does the bone know how long it should grow to be?
Perhaps by studying what happens when they fail to do sowe can gain some insight…
dwarfism

Shortly after the time that Twitty spent in Hans Spemann’slaboratory in Germany, another young scientist was beginninghis career at the Kaiser Wilhelm Institute of Anthropology.
This student was Josef Mengele
1935 dissertation described work measuringhundreds of jawbones looking for distinctiveracial differences
The world does not remember Mengele forhis doctoral work, but for the horrific careerpath he then followed.

The medical practice paradigm during the Hitler period saw the physician as a "selector" acting on behalf of the state in order to improve the “health of the nation” (Volksgesundheit). People defined as “underclass” and therefore a “risk to the genetic or racial health of the population”. These people could be selected for enforced sterilization, incarceration, and eventual extermination.
Mengele was encouraged by his mentor, von Verschuer, to go and takeadvantage of the “extraordinary research opportunities” at Auschwitz.
Research on eugenics and racial hygiene was conducted in university research institutes and those of the Kaiser-Wilhelm organization.
The helpless human quarry incarcerated by the state was viewed by medical science as a unique opportunity for the kinds of research which under German law were not even permitted on animals. These victims were exploited in the name of “science” both before death for inhuman research, and their bodies were exploited after death.
When Mengele arrived at Aushwitz in May 1943,there were >100,000 prisoners. Killing took place daily.
Aushwitz survivors usually remember Mengele -he was a very complicated entity:
- very attractive- well groomed- charming- could speak nicely to a child then send it off to the gas chamber
(sociopathic?)
Mengele often performed the initial “sorting” to life or deathof prisoners arriving by train. He kept the most interesting“specimens” for his “research”

One such “lucky” (or unlucky?) group of “subjects” was a familyafflicted with dwarfism.
The father of the Ovitz family had a type of dwarfism knownas psuedoachondroplasia
Of his 9 children, 7 were dwarfed. After his unexpected death,the mother got the children musical training to engineer a wayfor them to earn a living.
They hid their Jewish heritage for a few years, but were eventuallycaptured and sent to Auschwitz - much to the delight of Mengele

They became Mengele’s favorite experimental subjects
-those who were married were subjected to gynecological experiments uterine injections, blood samples, other tissue samples
-all subjected to numerous other “medical” tests includingextraction of spinal fluid, flushing of ears with extremely hot orcold water, hair extraction, painful brain and face examinations.
-forced to stand naked on display while Mengele lectured about them to Nazi higher-ups

Auschwitz was liberated in January 1945.
The Ovitz family survived with their lives (but at what cost?)
Mengele was also fascinated with other subjects,especially twins, who he would kill just to dissectand compare the similarity of their organs.
Mengele was never tried for his crimes against humanity.
He died on a beach in Brazil in 1979.

psuedoachondroplasia
Dominantly inherited form of dwarfism. The gene mutated in thiscondition is cartilage oligomeric protein (COMP).
Growth plates are the active sites of bone growth at theends of developing/growing bones.
Growth plates remain uncalcified until around the age of 18 (when we stop growing).

normally, there are columnsof chondrocytes that secretea cartilagenous matrix, thendie.
if COMP is mutated, it failsto be secreted to the matrixand prematurely kills the chondrocytes in the process(halting growth )
therefore, COMP and other proteinsthat control the activity of the growth plate play a large rolein determining the final lengthof the bone.

achondroplasia
Inherited in an autosomal dominant fashion, but over 80% ofcases arise from spontaneous mutation. Phenotypically characterized by short stature with disproportionately short arms and legs, a large head, and characteristic facial features

achondroplasia
The mutation responsible is a single amino acid changein FGFR3resulting in a glycine to arginine change atposition 380.
glycine
arginine
achondroplasia
The mutation responsible is a single amino acid changein FGFR3resulting in a glycine to arginine change atposition 380.
This mutation makes the Fibroblast Growth Factor Receptorinappropriately active (mimics excess FGF)
Too much FGF would inhibit chondrocytes from travelling upthe growth plate - thus this mutation results in lackof bone growth from the growth plates.(no chondrocytes, no secreted matrix, no future bone)
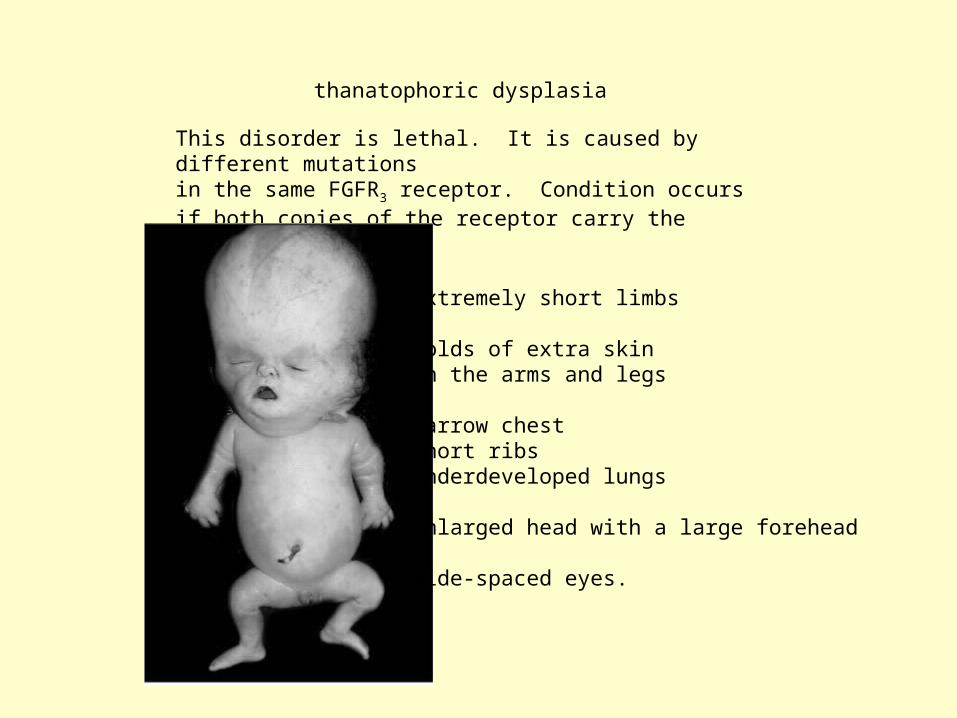
thanatophoric dysplasia
This disorder is lethal. It is caused by different mutationsin the same FGFR3 receptor. Condition occurs if both copies of the receptor carry the mutation.
extremely short limbs
folds of extra skin on the arms and legs
narrow chestshort ribsunderdeveloped lungs
enlarged head with a large forehead
wide-spaced eyes.

HAVE A NICE WEEKEND!!!