m.unverdorben; acc march 2008 martin unverdorben rotenburg/fulda, germany and richmond, va, usa...
TRANSCRIPT

M.Unverdorben; ACC March 2008
Martin UnverdorbenRotenburg/Fulda, Germany and Richmond, VA, USA Clinical Research Institute, Center for Cardiovascular
Diseases
On behalf of the PEPCAD II Investigators
The Paclitaxel-Eluting PTCA-Balloon Catheter in Coronary
Artery Disease
PEPCAD II-ISR

M.Unverdorben; ACC March 2008 2
Presenter Disclosure Information
PEPCAD II 12-Month Follow-up
The following relationships exist related to this presentation:
M.Unverdorben Nothing to disclose
B.Scheller Consulting and lecture fees from BBraun, co-patent owner of Sequent® Please
M.Unverdorben; ACC March 2008 3
AgendaAgendaThe PACCOCATH technology
PEPCAD II ISR 6-month angiographic and clinical follow-up
PEPCAD II ISR 12-month clinical follow-up
Descriptive statistics: Mean ± SD Inferential statistics: Student’s t-test, Fisher’s
exact test, Logrank test Level of significance: p < 0.05
StatisticsStatistics

M.Unverdorben; ACC March 2008 4
Scheller Heart 2007, 93: 539-41
DES vs. DEB (PACCOCATH)DES vs. DEB (PACCOCATH)
Hwang, Circulation 2001; 104: 600-5
Instant and short term drug release from balloon
~ 300 - 600 µg PaclitaxelNo polymersStenting optional
Slow and continuous drug release from stent struts
~100 - 200 µg Paclitaxel Sirolimus
Polymers with associated reactions
Implies stent deployment
DES
DEB
Creel, Circ Res 2000; 86: 879-884
ex vivo perfusion of calf carotid ex vivo perfusion of calf carotid arteries,transmural distributionarteries,transmural distribution

M.Unverdorben; ACC March 2008 5
The Matrix CoatingThe Matrix CoatingPACCOCATH technology creates a unique matrix
coatingpure
paclitaxel
paclitaxel + hydrophilic
spacer
without with PACCOCATH technology
huge contact surface between lipophilic drug and the vessel wall
high bioavailability of paclitaxel at the target site for rapid drug absorption by the vessel wall
uniform/complete application of the drug after 1st balloon
expansion

M.Unverdorben; ACC March 2008 6
*SeQuent® Please (B.Braun Vascular Systems, Berlin, Germany) is manufactured
based on the PACCOCATH technology with 3µg paclitaxel/mm²; CE mark filed in the EU
SeQuent® (uncoated balloon)
SeQuent® Please* (coated balloon)

M.Unverdorben; ACC March 2008 7
Objective
Safety and efficacy of the Sequent® Please
DEB in the treatment of ISR in native coronary
arteries (reference Ø: 2.5mm, 3.5mm;
lesion length: ≤22mm) for procedural success
and preservation of vessel patency in
comparison to the Taxus® DES
Study Design
Prospective, randomized, multi-center,
two-arm phase-II pilot study conducted in
Germany
M.Unverdorben; ACC March 2008 8
Primary Variable
6-month late lumen loss
Secondary Variables
Procedural success (≤30%)6-month binary restenosis rate6-month MACEMACE at 1 and 3 years

M.Unverdorben; ACC March 2008 9
Inclusion Criteria
Stable or unstable angina (no MI) ISR in native coronary arteries
Medication
ASS ≥ 100 mg dailyClopidogrel 75 mg daily
–3 months DEB
–6 months DES
M.Unverdorben; ACC March 2008 10
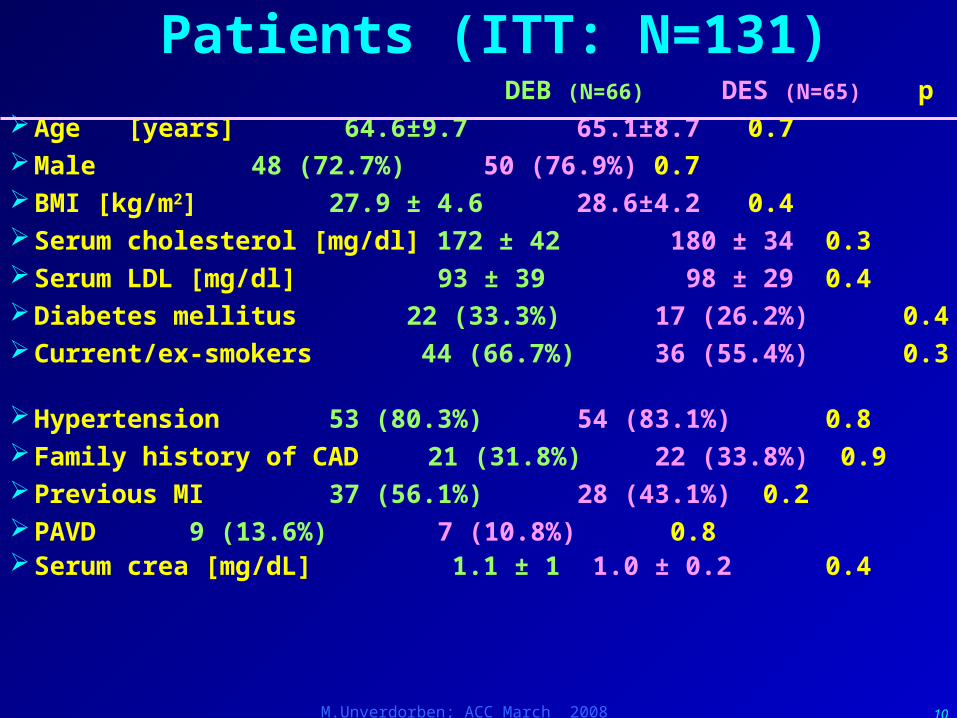
Patients (ITT: N=131) DEB (N=66) DES (N=65) pAge [years] 64.6±9.7 65.1±8.7 0.7Male 48 (72.7%) 50 (76.9%) 0.7 BMI [kg/m2] 27.9 ± 4.6 28.6±4.2 0.4Serum cholesterol [mg/dl] 172 ± 42 180 ± 34 0.3Serum LDL [mg/dl] 93 ± 39 98 ± 29 0.4Diabetes mellitus 22 (33.3%) 17 (26.2%) 0.4Current/ex-smokers 44 (66.7%) 36 (55.4%) 0.3
Hypertension 53 (80.3%) 54 (83.1%) 0.8Family history of CAD 21 (31.8%) 22 (33.8%) 0.9Previous MI 37 (56.1%) 28 (43.1%) 0.2PAVD 9 (13.6%) 7 (10.8%) 0.8Serum crea [mg/dL] 1.1 ± 1 1.0 ± 0.2 0.4

M.Unverdorben; ACC March 2008 11
Baseline Angiography (ITT: N=131)DEB (N=66) DES (N=65) p
1-vessel disease [%]
28.8 35.4
2-vessel disease [%]
40.9 35.4 0.7
3-vessel disease [%]
30.3 29.2
Stenosis length [mm]
15.7 6.6 15.4 6.6 0.8
Mehran I 31 (47.0%) 25 (38.5%)
Mehran II 20 (30.3%) 26 (40.0%) 0.7
Mehran III 14 (21.2%) 12 (18.5%)
Mehran IV 1 ( 1.5%) 2 ( 3.1%)
MLD pre PCI [mm] 0.74 0.27 0.77 0.30 0.6
Stenosis pre PCI [%]
74 9 73 9 0.5
MLD post PCI [mm] 2.30 0.40 2.56 0.41 <0.0001
Stenosis post PCI [%]
20 10 11 8 <0.001

M.Unverdorben; ACC March 2008 12
Outcome (ITT: N=131)DEB (N=66) DES (N=65) p
Follow-up: clinical [months]
6.2 ± 0.9 6.2 ± 0.9 1
Follow-up: clinical [N] 64 (97.0%) 65 (100%) 0.5
Follow-up: angiographic [N]
57 (86.4%) 59 (90.8%) 0.6
Late lumen loss [mm] 0.20 ± 0.45 0.45 ± 0.68 0.02
Binary restenosis in segment
4/57 (7.0%) 12/59(20.3%) 0.06
TLR 4/64 (6.3%) 10/65 (15.4%) 0.1
Myocardial infarction 0/64 (0.0%) f1/65 (1.5%) 1
Death *2/64 (3.1%) **1/65 (1.5%) 1
Total MACE (w/o noncardiac death) 5/64 (7.8%) 11/65 (16.9%) 0.2
*1 each: non-cardiac & cardiac but not lesion related
** non-cardiac death
fNSTEMI due to side branch occlusion

M.Unverdorben; ACC March 2008 13
As-TreatedRandomization
N=131
Sequent Pleasen=66
Taxusn=65
4 protocol violators
Lesion too long (41.1mm)Multilesion PCI in metal
jacketSignificant flap after PCI
Severe renal failure
1 crossing failure treat/w convent balloon
4 crossing failure treat/w Sequent Please
60 DES2 with additional DES
66 DEB56 DEB only6 DEB + BMS4 DEB (cross-
over)

M.Unverdorben; ACC March 2008 14
Outcome (AsT: N=126)DEB (N=66) DES (N=60) P=
Follow-up: clinical [months]
6.2 ± 0.8 6.2 ± 0.8 0.7
Follow-up: clinical [N] 64 (97.0%) 60 (100%) 0.4
Follow-up: angiographic [N]
58 (87.9%) 54 (90.0%) 0.8
Late lumen loss [mm] 0.19 ± 0.38
0.47 ± 0.71 0.03
Binary restenosis in segment
2/58 (3.4%)
11/54 (20.4%)
0.007
TLR 2/64 (3.1%)
10/60 (16.7%) 0.02Myocardial infarction 0/64 (0.0%) f1/60 (1.7%) 1
Death *2/64 (3.1%) **1/60 (1.7%) 1
Total MACE (w/o noncardiac death) 3/64 (4.7%) 11/60 (18.3%)
0.02
fNSTEMI due to side branch occlusion
*1 cardiac, not lesion related 2 non cardiac
** non-cardiac death
M.Unverdorben; ACC March 2008 15
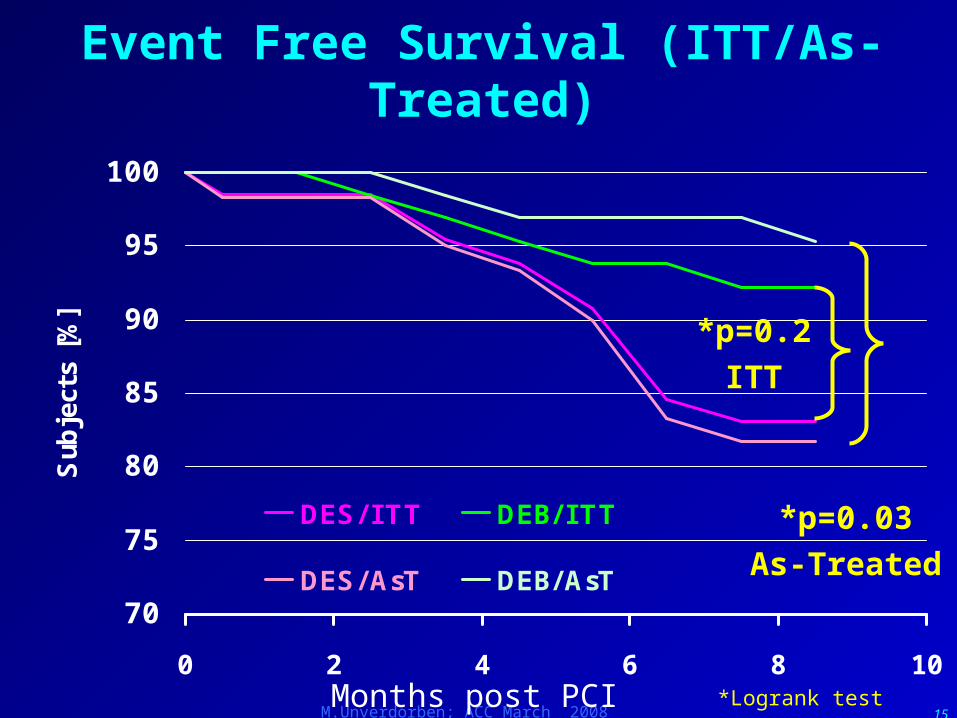
Event Free Survival (ITT/As-Treated)
70
75
80
85
90
95
100
0 2 4 6 8 10
Sub
ject
s [%
]
DES/ I TT DEB/ I TT
DES/AsT DEB/AsT
*p=0.2ITT
*p=0.03As-Treated
Months post PCI *Logrank test

M.Unverdorben; ACC March 2008 16
12-Month Follow-up: As-Treated
60 DES2 with additional
DES
66 DEB56 DEB only6 DEB + BMS4 DEB (cross-
over)
Unknown today
2/60 (3.3%)
Lost to FU1/60 (1.7%)
Follow-up12.3±0.8 months
57/60 (95.0%)
Deaths3/60 (5%)
Unknown today
1/66 (1.5%)
Lost to FU0/60 (0%)
Follow-up12.3±0.7 months
59/60 (98.3%)
Deaths2/66 (3.0%)
M.Unverdorben; ACC March 2008 17
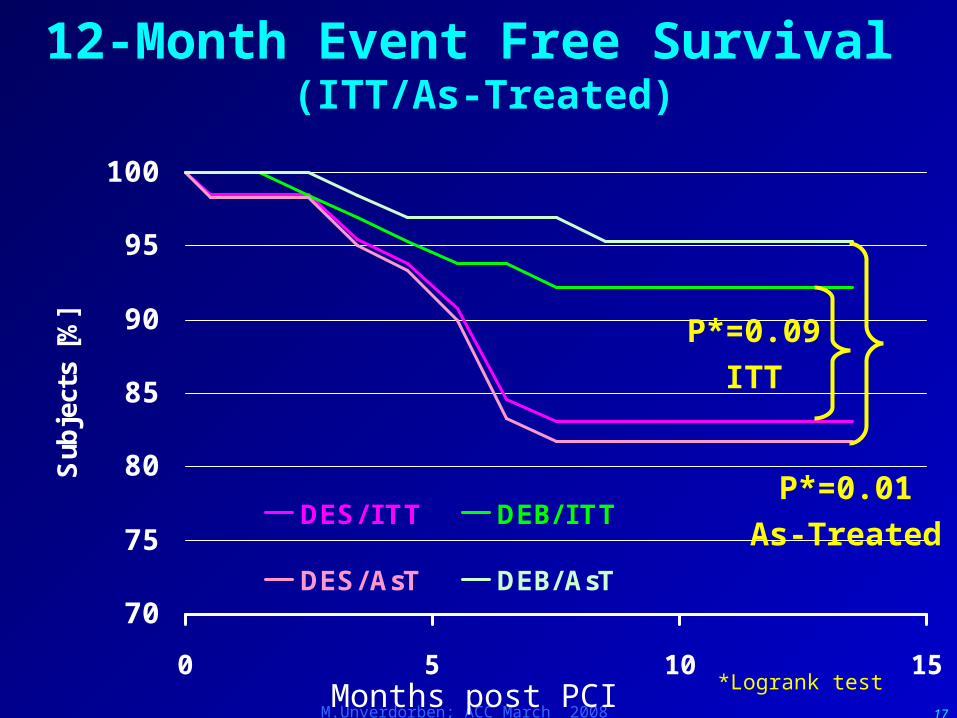
12-Month Event Free Survival (ITT/As-Treated)
70
75
80
85
90
95
100
0 5 10 15
Sub
ject
s [%
]
DES/ I TT DEB/ I TT
DES/AsT DEB/AsT
P*=0.09ITT
P*=0.01As-Treated
Months post PCI *Logrank test

M.Unverdorben; ACC March 2008 18
Events From 6 to 12 Months
DEB
–2 Px with PCI in non-target vessel
–1/66 (1.5%) Px with re-re PCI in target lesion
DES
–2 Px with non-cardiac death
–3/60 (5%) Px with re-re PCI in target lesion
No new patient with MACE
M.Unverdorben; ACC March 2008 19
Summary PEPCAD II
In the treatment of ISR the paclitaxel-eluting balloon catheter Sequent® Please (B.Braun Melsungen AG) … –was safe and associated with a high procedural success rate,
–exhibited a significant reduction in 6-month late lumen loss and 6/12-month MACE when compared to the Taxus® stent, and
–was not associated with late thrombosis in 250 patient years.

M.Unverdorben; ACC March 2008 20
The PEPCAD II InvestigatorsF.X. Kleber, Unfallkrankenhaus Berlin
H. Heuer, N. Schulze-Waltrup; St. Johannes Hospital,
Dortmund
C. Vallbracht; Herz- und Kreislaufzentrum, Rotenburg an der
Fulda
B. Scheller; Universitätsklinikum des Saarlandes,
Homburg/Saar
C. Hengstenberg, Universitätsklinikum, Regensburg
M. Leschke; Städtische Kliniken, Esslingen C. Hamm, M. Rau; Kerckhoff Klinik, Bad Nauheim
G. Werner; Städtisches Klinikum, Darmstadt
D. Antoni; Krankenhaus Bogenhausen, MünchenW. Bocksch; Charité Virchow, Berlin
H.Ackermann; Department for Biostatistics, University of Frankfurt/M
M.Boxberger, B.Braun, BerlinR.Degenhardt, M.Unverdorben; Clinical Research Institute,
Rotenburg an der Fulda

M.Unverdorben; ACC March 2008 21
The PEPCAD ProgramPaclitaxel-Eluting PTCA-Catheter in Coronary Artery
Disease Title Design Status PIPEPCAD I SVD
Sequent in ≤2.8mm, 120px, multi-center, GER
6mo-FU 12mo-FU
MU, CRI
PEPCAD II ISR
Sequent vs Taxus in ISR, 131px, multi-center, GER
6mo-FU 12mo-FU
MU, CRI
PEPCAD III Sequent + pre-loaded Coroflex Blue vs Cypher, 600 px, Europe
Q2/07 recruiting
B.SchellerC.Hamm
PEPCAD IV DM
Sequent vs Taxus in DM, 160px, multi-center, Thailand, Malaysia
Q2/07 recruiting
D.Rosli, MU, CRI
PEPCAD V BIF Sequent, 25px, dual-center, GER
Q3/ 07 recruiting
D.Mathey F.Kleber MU, CRI INDICOR Coroflex
Blue+Sequent, Real World, 100px
IRB U.Kaul, MU,CRI

M.Unverdorben; ACC March 2008 22
This is not the end. It is not even the beginning of the end. But it is, perhaps, the end of the beginning.
(Sir Winston S.Churchill)