multiple myeloma updates from the 2015 asco annual … · slides multiple myeloma update from the...
TRANSCRIPT

1
SLIDES
Multiple Myeloma Update From the
2015 ASCO Annual Meeting and 20th Congress of EHA
Multiple Myeloma Updates From
the 2015 ASCO Annual Meeting
and 20th Congress of EHA
Welcome and Introductions
Joan Levy, PhD
Multiple Myeloma Research Foundation
Norwalk, CT
2

2
SLIDES
Multiple Myeloma Update From the
2015 ASCO Annual Meeting and 20th Congress of EHA
Multiple Myeloma Updates From the 2015 ASCO
Annual Meeting and 20th Congress of EHA
Jesus Berdeja, MD
Tennessee Oncology
Nashville, TN
Saad Zafar Usmani, MD
Levine Cancer Institute
Charlotte, NC
Faculty
3
Smoldering Multiple Myeloma
Jesus Berdeja, MD
Tennessee Oncology
Nashville, TN
Saad Zafar Usmani, MD
Levine Cancer Institute
Charlotte, NC
Faculty
4

3
SLIDES
Multiple Myeloma Update From the
2015 ASCO Annual Meeting and 20th Congress of EHA
Mateos MV. ASCO Educational Book 2015; e484.
Differential Diagnosis for MGUS,
SMM, and Symptomatic MM
5
Feature MGUS SMM MM
Serum-M Protein <3 g/dL and ≥ 3 g/dL and/or
Clonal BMPC
Infiltration
<10% 10-60% ≥ 10% biopsy-
proven
plasmacytoma
Symptomatology Absence of CRAB* Absence of MDE**
or amyloidosis
Presence of
MDE**
* CRAB Includes (1) hypercalcemia: serum calcium > 0.25 mmol/L (>1 mg/dL) higher than the upper
limit of normal or > 2.75 mmol/L (>11 mg/dL); (2) renal insufficiency: serum creatinine > 177µ mol/L
(2 mg/dL) or creatinine clearance < 40 ml/minute; (3) anemia: hemoglobin value of > 2 g/dL below the
lower normal limit or a hemoglobin value < 10 g/dL; (4) bone lesions: one or more osteolytic lesion
revealed by skeletal radiography, CT, or PET-CT.
** MDE: Myeloma-defining events include CRAB symptoms (above) or any one or more of the following
biomarkers or malignancy: clonal bone marrow plasma cell percentage ≥ 60%; involved/uninvolved
serum free light-chain ratio ≥ 100; > 1 focal lesions revealed by MRI studies.
MGUS, monoclonal gammopathy of undetermined significance; SMM, smoldering multiple myeloma; MM, multiple
myeloma; BMPC, bone marrow plasma cell
Treatment of High-Risk Smoldering
MM With Len/Dex
Mateos MV, et al. ASH 2014: abstract 3465
ITT analysis TTP to active disease (n = 119)
Len/Dex
Median TTP: NR
14 Progressions (25%)
HR: 6.1; 95% IC (3.3–11); p < 0.0001
Time from inclusion
Pro
po
rtio
n o
f p
ati
en
ts p
rog
ressio
n-f
ree
10 0 20 30 40 50 60
1,0
0,8
0,6
0,4
0,2
0,0
No treatment
Median TTP: 21m
53 Progressions (85%)
Median follow-up: 64 months (range 49-81)
Len/Dex, lenalidomide-dexamethasone; HR, hazard ratio; ITT, intention to treat; TTP, time-to-progression
6

4
SLIDES
Multiple Myeloma Update From the
2015 ASCO Annual Meeting and 20th Congress of EHA
Treatment of High-Risk Smoldering
MM With Len/Dex (cont)
Mateos MV, et al. ASH 2014: abstract 3465
OS from inclusion (n=119) Median follow-up: 64 months (range 49–81)
Len/Dex
94% at 7 years
No treatment
64% at 7 years
Time from inclusion
Pro
po
rtio
n o
f p
ati
en
ts a
live
HR: 4.6; 95% IC (1.5–13.1); p=0.001
1,0
0,8
0,6
0,4
0,2
0,0
20 0 30 40 50 70 80 10 60
Median follow-up: 64 months (range 49-81)
Len/Dex, lenalidomide-dexamethasone; HR, hazard ratio; OS, overall survival
7
Progression From SMM to
Active MM – Clinical Variables
• An elevated involved/uninvolved light chain ratio (>100)
• More than 60% bone marrow plasmacytosis
• More than 1 focal lesion on either an axial skeletal MRI
or a whole body MRI
Rajkumar SV et al. Lancet 2014; 15:e538-48. 8

5
SLIDES
Multiple Myeloma Update From the
2015 ASCO Annual Meeting and 20th Congress of EHA
FDG-PET/CT Focal Lesions as a
Marker of Progression
Zamagni E, Nani C, Gay F, et al. Poster 267 presented at EHA Learning Center May 31, 2015.
• PET/CT reliably assesses early skeletal involvement
• PET/CT positivity significantly increased the risk of
progression from SMM to MM
• PET/CT could become a new risk factor to define
high-risk SMM
9
Predictors of Myeloma Progression
(SWOG S0120)
Dhodapkar M, et al. Blood. 2014;123:78-85.
• A prospective observational study of 331 AMG patients
• Baseline data from clinical variables, GEP, and MRI
findings correlated with risk of progression to CMM
• An increased risk score was an independent predictor
of risk of progression
• Combination of elevated serum free light chain,
M-spike, and GEP70 risk score identified high risk of
progression to CMM
AMG, asymptomatic monoclonal gammopathy; GEP, gene expression profiles; MRI, magnetic
resonance imaging; CMM, clinical multiple myeloma.
10

6
SLIDES
Multiple Myeloma Update From the
2015 ASCO Annual Meeting and 20th Congress of EHA
Upfront Therapy
Jesus Berdeja, MD
Tennessee Oncology
Nashville, TN
Saad Zafar Usmani, MD
Levine Cancer Institute
Charlotte, NC
Faculty
11
12
Update From the FIRST Study
12
Newly
diagnosed
patients
Continuous lenalidomide/dex (N = 535)
18 cycles of lenalidomide/dex (N = 541)
12 cycles of melphalan, prednisone, thalidomide (N = 547)
Median follow-up of 45.5 months
Cont. Len/dex 18 cycles Len/dex MPT
Median OS
(months)
58.9 56.7 48.5
Facon T et al J Clin Oncol 33, 2015 (suppl; abs 8524)
MPT, melphalan–prednisone–thalidomide; OS, overall survival

7
SLIDES
Multiple Myeloma Update From the
2015 ASCO Annual Meeting and 20th Congress of EHA
13
Update From the FIRST Study (cont)
Median follow-up of 37 months
Cont. Len/dex 18 cycles Len/dex MPT
Age≤75 Age>75 Age≤75 Age>75 Age≤75 Age>75
3-Yr OS % 74 63 70 58 67 54
PFS* 27.4 21.2 21.3 19.4 21.8 19.2
Duration of
Response*
77 71 77 66 66 55
Hulin C. EHA20 Abstract 429. June 2015.
*Median, months
OS, overall survival; PFS, progression-free survival.
14
Toxicity Related Dose Adjustment
Effects Cost Savings With LEN
Arikian S. 2015 EHA Abstract P284.
• Treatment costs of NDMM (n=2843) and second line
MM patients (n=1361) were analyzed
• Quarterly cost reduction patterns were consistent
• Over 3 years average monthly total costs were lower
for NDMM LEN patients due to extended interval prior
to 2nd line therapy initiation
NDMM, newly diagnosed multiple myeloma; LEN, lenalidomide

8
SLIDES
Multiple Myeloma Update From the
2015 ASCO Annual Meeting and 20th Congress of EHA
15
FIRST Study Sub-Analysis
Dimpooulos 2015 EHA Abstract 274
Normal Renal Mild RI Moderate RI Severe RI
PFS*
Len/dex cont 37.7 26.7 18.7 17.2
Len/dex 18 cycles 24.6 21.0 18.7 12.1
MPT 24.9 21.4 17.5 11.7
OS*
Len/dex cont NR NR 43.7 33.2
Len/dex 18 cycles 53.6 NR 41.8 42.6
MPT NR NR 38.5 42.9
*Median, months
Impact of Renal Impairment on Outcomes
• Len/dex continuous was well tolerated consistently across renal
subgroups
• Renal function also improved more in patients treated with len/dex
continuous therapy vs 18 cycles or MPT
Len, lenalidomide; dex, dexamethasone; MPT, melphalan-prednisone-thalidomide; RI, renal impairment
16
Quadruplet Induction in Transplant
Eligible NDMM Patients
Pawlyn C. 2015 EHA Abstract S428
• Upfront KCRD quadruplet vs sequential triplet IMiD
combinations (followed by PI triplet if response
suboptimal)
• Patients (n=257) completed mean 4.2 KCRD cycles
prior to transplant
• Dose modifications required in 63% of KCRD patients
but low incidences of toxicities reported
• Quadruplet KCRD induction presents a promising
option
IMiD, immunomodulatory drug; KCRD, carfilzomib-cyclophosphamide-lenalidomide-dexamethasone;
PI, proteasome inhibitor
9
SLIDES
Multiple Myeloma Update From the
2015 ASCO Annual Meeting and 20th Congress of EHA
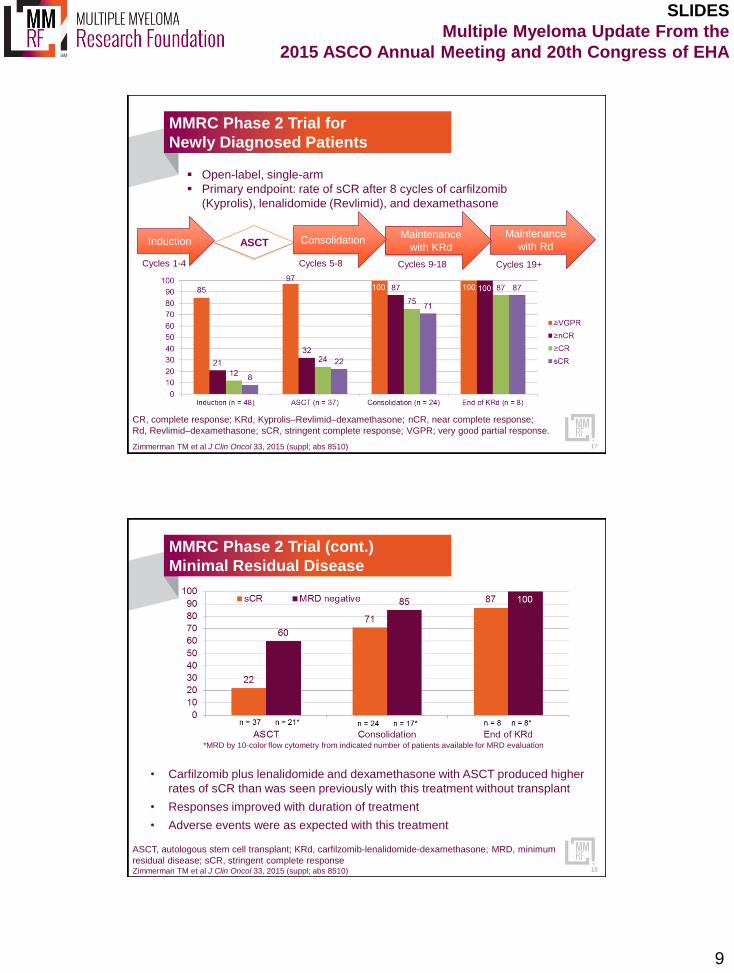
MMRC Phase 2 Trial for
Newly Diagnosed Patients
Open-label, single-arm
Primary endpoint: rate of sCR after 8 cycles of carfilzomib
(Kyprolis), lenalidomide (Revlimid), and dexamethasone
ASCT Maintenance
with Rd Maintenance
with KRd Induction Consolidation
Cycles 1-4 Cycles 19+ Cycles 9-18 Cycles 5-8
Zimmerman TM et al J Clin Oncol 33, 2015 (suppl; abs 8510)
CR, complete response; KRd, Kyprolis–Revlimid–dexamethasone; nCR, near complete response;
Rd, Revlimid–dexamethasone; sCR, stringent complete response; VGPR; very good partial response.
17
MMRC Phase 2 Trial (cont.)
Minimal Residual Disease
*MRD by 10-color flow cytometry from indicated number of patients available for MRD evaluation
• Carfilzomib plus lenalidomide and dexamethasone with ASCT produced higher
rates of sCR than was seen previously with this treatment without transplant
• Responses improved with duration of treatment
• Adverse events were as expected with this treatment
Zimmerman TM et al J Clin Oncol 33, 2015 (suppl; abs 8510)
ASCT, autologous stem cell transplant; KRd, carfilzomib-lenalidomide-dexamethasone; MRD, minimum
residual disease; sCR, stringent complete response 18

10
SLIDES
Multiple Myeloma Update From the
2015 ASCO Annual Meeting and 20th Congress of EHA
19
Maintenance With Lenalidomide
Following Single ASCT
Holstein SA et al J Clin Oncol 33, 2015 (suppl; abs 8523)
Time to progression and overall survival were significantly improved with
len regardless of response
Len may be associated with a risk of secondary primary malignancies
ASCT CR
PR
SD
Placebo
Lenalidomide
Time to Progression Overall Survival
Time Since ASCT (Months)
Pro
bab
ilit
y
0.0
0.2
0.4
0.6
0.8
1.0
Placebo
Time Since ASCT (Months)
Pro
bab
ilit
y
0.0
0.2
0.4
0.6
0.8
1.0
0 20 40 60 80 100 0 20 40 60 80 100
Lenalidomide
Median: 53 vs 26 mos
Hazard ratio 0.54
(p<0.001)
Median: NR vs 76 mos
Hazard ratio 0.60
(p=0.001)
ASCT, autologous stem cell transplant; CR, complete response; NR, not reached; PR, partial response;
SD, stable disease.
Placebo
Lenalidomide
Improved Response Beyond Day
+100 is Rare Without Maintenance
De Larrea 2015 EHA P278
Objective - Evaluate patients who improve response beyond day
+100 after ASCT with and without maintenance
• Patients (N=144) who had ASCT with melphalan-based
conditioning were studied
• Of the 74 who did not receive maintenance, only 1 patient
improved response from VGPR to CR at +100 days after ASCT
• The remaining patients received maintenance with either
interferon (37%), glucocorticoids (20%), thalidomide (4.9%), or
thalidomide + bortezomib (6.9%)
• Beyond day +100 after ASCT 8.3% of patients receiving
maintenance improved response
− The outcome of these patients was better than those who did not
upgrade their response in terms of PFS and OS
20

11
SLIDES
Multiple Myeloma Update From the
2015 ASCO Annual Meeting and 20th Congress of EHA
Transplant
Jesus Berdeja, MD
Tennessee Oncology
Nashville, TN
Saad Zafar Usmani, MD
Levine Cancer Institute
Charlotte, NC
Faculty
21
Transplant
• Dr. Usmani noted that only approximately 13% of
multiple myeloma patients in the United States receive
a stem cell transplant
• Two pivotal studies (from the French Myeloma Group,
and Medical Research Council UK) showed transplants
do improve PFS and OS
• Further clinical study from Dr. Palumbo solidified the
importance of ASCT
• Importance of ASCT timing?
− Awaiting results of the Dana-Farber/IFM trial
1. Attal M. N Engl J Med. 1996;335:91-97 2.Child JA. N Engl J Med. 2003;348:1875-1883
3. Palumbo A. N Engl J Med. 2014;371:895-905. 22

12
SLIDES
Multiple Myeloma Update From the
2015 ASCO Annual Meeting and 20th Congress of EHA
23
Lenalidomide (Revlimid) Plus
Dexamethasone ±ASCT
Lenalidomide,
dexamethasone
Collect
stem
cells
Lenalidomide,
dexamethasone
(N = 29)
ASCT
(n = 31)
Continue
lenalidomide,
dexamethasone
Response rates, progression-free survival, and overall survival were similar in
patients with and without ASCT
Lentzsch S et al J Clin Oncol 33, 2015 (suppl; abs 8530)
Overall Survival Progression-free Survival
Time from First Treatment (Months)
Pro
po
rtio
n A
liv
e
0.0
0.2
0.4
0.6
0.8
1.0
0 6 12 24 30 36 42 48 54 66 78 60 72 18
Arm A (Ld+ASCT) Arm B (Ld alone)
Time to Progression or Death (Months)
Pro
po
rtio
n A
liv
e o
r P
rog
ressio
n F
ree
0.0
0.2
0.4
0.6
0.8
1.0
0 6 12 24 30 36 42 48 54 66 78 60 72 18
HR (Arm B [Ld alone]: Arm A [Ld+ASCT] = 0.73; 95% CI, 0.26–2.01; p=0.54
Arm A (Ld+ASCT) Arm B (Ld alone)
HR (Arm B [Ld alone]: Arm A [Ld+ASCT] = 1.02; 95% CI, 0.51–2.05; p=0.96
24
Transplant Versus No Transplant
Lenalidomide,
dexamethasone
6 cycles: cyclophosphamide,
lenalidomide, dexamethasone
(CRD)
2 cycles: Mel200/ASCT
N = 389 Mel200/ASCT CRD P value
4-year PFS 42% 28% 0.014
4-year OS 87% 71% 0.028
Grade 3 or 4 hematologic AEs 84% 26% 0.001
Grade 3 or 4 non-hematologic AEs 39% 22% 0.008
Gay F et al. EHA 2015 (abs S101)
AE, adverse event; ASCT, autologous stem cell transplant; PFS, progression-free survival.

13
SLIDES
Multiple Myeloma Update From the
2015 ASCO Annual Meeting and 20th Congress of EHA
25
ASCT ±Consolidation vs. Tandem
ASCT With Len Maintenance
• Phase III, 3-arm study (BMT CTN 0702)
• Consolidation is RVD (lenalidomide, bortezomib, and
dexamethasone
• All 3 arms receive len maintenance
• Fully accrued, results anticipated in 2016
www.clinicaltrials.gov, trial identifier NCT01109004
Relapsed/Refractory
Multiple Myeloma
Jesus Berdeja, MD
Tennessee Oncology
Nashville, TN
Saad Zafar Usmani, MD
Levine Cancer Institute
Charlotte, NC
Faculty
26

14
SLIDES
Multiple Myeloma Update From the
2015 ASCO Annual Meeting and 20th Congress of EHA
27
Several Relapsed/Refractory Studies
Presented at ASCO
Phase 3 Trials
• ELOQUENT-2
− Lenalidomide and dexamethasone with/without
elotuzumab
• ENDEAVOR
− Carfilzomib and dexamethasone vs bortezomib and
dexamethasone
• ASPIRE
− Carfilzomib, lenalidomide, and dexamethasone vs
lenalidomide and dexamethasone
Phase 2 Trial
• Daratumumab Monotherapy
− Patients with ≥ 3 lines of prior therapy
or double refractory multiple myeloma
ENDEAVOR Phase 3 Trial
Relapsed/ refractory
1-3 prior treatments
Carfilzomib plus
dexamethasone
N = 464
Bortezomib plus
dexamethasone
N = 465
Dimopoulos MA et al J Clin Oncol 33, 2015 (suppl;abs 8509); Dimopoulos MA et al EHA LB2071
Carfilzomib/dex Bortezomib/dex
ORR 77% 63%
CR 13% 6%
≥VGPR 54% 29%
• Median PFS with carfilzomib was 18.7 months vs 9.4 months with bortezomib
(P< .0001)
• Rates of grade ≥ 2 peripheral neuropathy were 6.3% vs 32.0% (P< .0001)
CR, complete response; ORR, overall response rate; VGPR, very good partial response
28

15
SLIDES
Multiple Myeloma Update From the
2015 ASCO Annual Meeting and 20th Congress of EHA
ASPIRE Phase 3 Trial
Relapsed/refractory
1-3 prior therapies
Carfizomib, lenalidomide
and dexamethasone
Lenalidomide and
dexamethasone
Dimopoulos MA et al J Clin Oncol 33, 2015 (suppl; abs 8525); Dimopoulos MA et al EHA abs S427
1 prior therapy ≥2 prior therapies
Carf/Len/dex Len/dex Carf/Len/dex Len/dex
PFS (months) 29.6 17.6 25.8 16.7
ORR 87% 70% 87% 64%
Stringent CR 13% 3% 15% 5%
CR 21% 4% 15% 6%
VGPR 42% 36% 34% 28%
PR 11% 27% 23% 26%
29
ELOQUENT-2 Phase 3 Trial
Relapsed/Refractory
1-3 prior therapies
not lenalidomide
refractory
Elotuzumab, lenalidomide, and dexamethasone
(N = 321)
Lenalidomide and dexamethasone
(N = 325)
Lonial S et al J Clin Oncol 33, 2015 (suppl; abs 8508)
Elo/Len/dex Len/dex P value
PFS (months) 19.4 14.9 0.0004
ORR 79% 66% 0.0002
• Median number of prior therapies was 2
• Elotuzumab added very little toxicity
30

16
SLIDES
Multiple Myeloma Update From the
2015 ASCO Annual Meeting and 20th Congress of EHA
Phase 2 Trial:
Daratumumab Monotherapy
Relapsed/refractory
≥ 3 prior therapies Daratumumab 16 mg/kg
(N = 106)
Lonial S et al J Clin Oncol 33, 2015 (suppl; abs LBA8512)
• Median of 5 prior therapies
• Median time to progression: 3.7 months
• ORR: 29.2%
− 3 sCR, 10 VGPR, and 18 PR
• Median duration of response: 7.4 months
• Estimated 1-year OS: 65%
31
Panobinostat Update
• Panobinostat combined with bortezomib and
dexamethasone was recently approved for patients with
relapsed/refractory MM
− Treated w/≥ 2 prior therapies including IMiDs and bortezomib
• PANORAMA 1 Phase 3 trial
− Patients w/1-3 prior therapies (IMiDs and bortezomib)
− Panobinostat or placebo in combo w/bortezomib and
dexamethasone
− Panobinostat combination was very active but with significant
GI and hematologic toxicities
1. San-Miguel JF et al J Clin Oncol 33, 2015 (suppl; abs 8526); 2. Hungria VTM et al J Clin Oncol 33, 2015 (suppl; abs
8575); San-Miguel JF, et al. Lancet Oncol. 2014;15:1195-1206. 32

17
SLIDES
Multiple Myeloma Update From the
2015 ASCO Annual Meeting and 20th Congress of EHA
Panobinostat Plus Carfilzomib
Ongoing Phase 1/2 trial
• Evaluating the dose of the combination
• All patients had received prior bortezomib and/or carfilzomib
− 81% had received prior IMiDs
− 58% previously had ASCT
• Responses so far:
− 1 (3%) CR, 10 (29%) VGPR, 14 (45%) PR, 4 (13%) MR,
4 (13%) SD
− ORR was 77%
• Most gastrointestinal toxicities were grade 1 or 2
• Grade 3/4 toxicities:
− Thrombocytopenia (47%)
− Neutropenia (8%)
− Anemia (9%)
− Diarrhea (6%)
Berdeja JG et al ASCO 2015 (abs 8513) 33
34
Novel Agents For
Relapsed, Refractory Patients
Drug Class
CAR-T cells Immunotherapy
CUDC-907 Histone deacetylase inhibitor
Ixazomib Oral proteasome inhibitor
Melflufen Alkylator
MOR202 Monoclonal antibody against CD38
Oprozomib Oral proteasome inhibitor
Ricolinostat Histone deacetylase inhibitor
SAR650984 Monoclonal antibody against CD38
Venetoclax (ABT-199) BCL-2 inhibitor
Raab M EHA 2015, abs S789; Raab M ASCO abs 8574; Raje N et al EHA 2015 P279; Magarotto V et al EHA P285; Moreau P EHA
P289; Kumar S EHA P658; Oki Y et al EHA P325; Vij R et al EHA P646

18
SLIDES
Multiple Myeloma Update From the
2015 ASCO Annual Meeting and 20th Congress of EHA
Galetto R, et al. EHA 2015 Abstract P724.
Allogenic CAR-T Cells
Targeting CS1
• CS1 glycoprotein (SLAMF7) highly expressed on MM tumor
cells
• Immunotherapy against MM studying chimeric antigen receptor
(CAR)-redirected T-cells in the targeting of CS1
• CAR approach restricted to targeting antigens on the tumoral
cells surface but absent from T-cells
• Galetto evaluated CS1 expression on T-cells to ensure
approach enabled harnessing activated T-cells to attack MM
cells
• CS1-gene-edited CAR cells found to have significantly
increased cytotoxic activity against MM cells with percentage of
CD8+ T-cells remaining unaffected
35
36
Novel Agents For
Relapsed, Refractory Patients
Drug Class
CAR-T cells Immunotherapy
CUDC-907 Histone deacetylase inhibitor
Ixazomib Oral proteasome inhibitor
Melflufen Alkylator
MOR202 Monoclonal antibody against CD38
Oprozomib Oral proteasome inhibitor
Ricolinostat Histone deacetylase inhibitor
SAR650984 Monoclonal antibody against CD38
Venetoclax (ABT-199) BCL-2 inhibitor
Raab M EHA 2015, abs S789; Raab M ASCO abs 8574; Raje N et al EHA 2015 P279; Magarotto V et al EHA P285; Moreau P EHA
P289; Kumar S EHA P658; Oki Y et al EHA P325; Vij R et al EHA P646

19
SLIDES
Multiple Myeloma Update From the
2015 ASCO Annual Meeting and 20th Congress of EHA
STRATUS Phase 3b Trial
1. Cavo M, et al. EHA20 June 13, 2015. 2. Weisel K, et al. J Clin Oncol. 33:2015 (suppl; abstr 8593).
• Pomalidomide plus low-dose dexamethasone in heavily
pretreated RRMM
• Most patients were refractory to both bortezomib and
lenalidomide
• The combination was active and well tolerated
37
Closing Remarks
Joan Levy, PhD
Multiple Myeloma Research Foundation
Norwalk, CT
To learn more about the MMRF, please visit:
www.multiplemyeloma.org
38