multiple mandibular nerve canals: radiographic observations and
TRANSCRIPT

VOLUME 38 • NUMBER 9 • OCTOBER 2007 781
QUINTESSENCE INTERNATIONAL
The mandibular canal, or the inferior alveolar
canal, transmits the inferior alveolar nerve, a
branch of the third division of the fifth cranial
nerve (trigeminal nerve), and the associated
vessels. The canal typically extends from the
mandibular foramen to the mental foramen.
The terminal dental and incisive branches
leave the inferior alveolar nerve within the
canal to supply the teeth and adjacent struc-
tures. A terminal branch leaves the canal at the
mental foramen to become the mental nerve.1
Occurrence of bifid mandibular nerve
canals is very rare, and its reported inci-
dence is less than 0.9%.1 Chavez-Lomeli and
colleagues2 suggested that during embryon-
ic development there may be 3 inferior den-
tal nerves innervating 3 groups of mandibu-
lar teeth. Later they fuse to form a single
nerve. Incomplete fusion of these nerves can
explain the presence of bifid or trifid nerve
canals3 in some patients.
It is important for clinicians to recognize
the presence of bifid canals on panoramic
radiographs and modify the dental treatment
accordingly. This article describes 5 cases of
bifid mandibular nerve canal and 1 case of
trifid mandibular canal and discusses their
radiographic diagnosis and clinical anesthet-
ic, orofacial surgical, and prosthetic implica-
tions in dental practice.
CASE REPORTS
Case 1A 35-year-old woman was referred for a
panoramic radiograph (College of Dental
Sciences [CODS], Manipal, India) to evaluate
periodontal bone loss. The radiograph
revealed generalized loss of crestal cortica-
tion along with significant bone loss and a
bifid mandibular canal on the left side (Fig 1).
Multiple mandibular nerve canals: Radiographic observations and clinical relevance.Report of 6 casesAjit Auluck, MDS1/Keerthilatha M. Pai, MDS2/
Muralidhar Mupparapu, DMD, MDS3
Variation in the normal anatomic pattern of the inferior alveolar nerve canal such as bifid
or trifid mandibular nerve canal is one of the reasons for local anesthetic failure in dental
practice. The present article reports 5 cases of bifid mandibular nerve canal and 1 case of
trifid mandibular canal and discusses their diagnostic criteria, radiographic features, and
clinical implications in dental practice. The objective of this review is to help clinicians
identify bifid and trifid mandibular canals on panoramic radiographs and subsequently
use the information in the modification of dental treatment planning. Once the multiple
canals are identified, the local anesthetic injection technique, prosthetic design, and surgi-
cal procedures can be modified to prevent pain and discomfort during treatment proce-
dures. (Quintessence Int 2007;38:781–787)
Key words: bifid mandibular canal, inferior alveolar nerve, local anesthesia, mandibular
canal, panoramic radiograph, trifid mandibular canal
1Assistant Professor, Oral Medicine and Radiology, Manipal
College of Dental Sciences, Mangalore, India.
2Professor and Head, Oral Medicine and Radiology, Manipal
College of Dental Sciences, Manipal, India.
3Associate Professor and Director, Division of Oral and
Maxillofacial Radiology, University of Medicine and Dentistry of
New Jersey, New Jersey Dental School, Newark, New Jersey.
Reprint requests: Dr M. Mupparapu, Diagnostic Sciences, D-
860, UMDNJ New Jersey Dental School, 110 Bergen Street, PO
Box 1709, Newark, NJ 07101-1709. Fax: 973-972-3164. E-mail:
Auluck.qxd 9/6/07 11:35 AM Page 781

782 VOLUME 38 • NUMBER 9 • OCTOBER 2007
QUINTESSENCE INTERNATIONAL
Auluck et a l
Case 2A 27-year-old woman presented (CODS) with
a prescription for a panoramic radiograph for
pre–implant placement evaluation. The
radiograph revealed an impacted maxillary
right canine and bifid mandibular canal on
the right side (Fig 2).
Case 3A 30-year-old woman had an overretained
maxillary left primary canine, and the perma-
nent canine was missing. A panoramic
radiograph, obtained (CODS) to investigate
the missing permanent canine, showed an
impacted maxillary left permanent canine and
bifid mandibular canal on the left side (Fig 3).
Case 4A 16-year-old girl who had recently under-
gone orthodontic treatment reported for a
prescribed panoramic radiograph (CODS).
The radiograph showed apical root resorption
of the anterior and premolar teeth as well as a
trifid mandibular canal on the left side (Fig 4).
Case 5A 45-year-old man reported to the Oral and
Maxillofacial Radiology Clinic (New Jersey
Dental School [NJDS], Newark, New Jersey)
from the Oral Diagnosis Clinic seeking gen-
eral dental care. The panoramic radiograph
showed multiple missing teeth in the maxilla
and mandible, caries, residual roots, and
multiple restorations, and the mandibular
nerve was noticed to be bifid bilaterally (Fig
5). The mesial extent of the inferior portion of
the bifid canal could not be traced com-
pletely. It is assumed that it either extends
beyond the tomographic layer mesially or
does not have enough canal space to be
captured as radiolucent on the film.
Case 6A 29-year-old woman was referred to the oro-
facial pain clinic (NJDS) for evaluation of
chronic paroxysmal pain in relation to the
mandibular left third molar region. Despite
treatment with anti-inflammatory medication,
pain was persistent.
Fig 1 Cropped panoramic radiograph demon-strating the bifid mandibular canal on the left side.The duplicated canal is toward the posterior andinferior border of the mandibular angle.
Fig 2 Cropped panoramic radiograph demon-strating the bifid mandibular canal on the right side.
Auluck.qxd 9/6/07 11:35 AM Page 782

VOLUME 38 • NUMBER 9 • OCTOBER 2007 783
QUINTESSENCE INTERNATIONAL
Auluck et a l
To assess the proximity of the impacted
and inverted third molar to the inferior alveo-
lar nerve canal, a computerized tomograph-
ic (CT) scan was obtained. During examina-
tion of the hard tissue anatomy of the region
in the mandibular coronal views in bone win-
dows, the variation in the mandibular canal
was noticed on the left side. The canal
appeared dumbbell shaped superiorly with
an extension inferiorly at its origin, and in the
more anterior sections it appeared separate
(Figs 6a and 6b). The sections in the region
of the mental foramen failed to show addi-
tional evidence of this duplication and prob-
ably were not captured well because of
miniaturization.
Fig 3 Cropped panoramic radiograph showingthe bifid mandibular canal on the left.
Fig 4 Cropped panoramic radiograph showingthe trifid mandibular canal on the left side.
Fig 5 Bilateral bifid mandibular canal. (arrowheads) Primary canal; (arrows) duplicated (bifid) canal.
Auluck.qxd 9/6/07 11:35 AM Page 783

QUINTESSENCE INTERNATIONAL
Auluck et a l
DISCUSSION
The term bifid is derived from the Latin word
meaning cleft into 2 parts or branches. For
the mandibular nerve, this occurs at the level
of the mandibular foramen.3 Various studies
using panoramic radiographs have depicted
the presence of bifid mandibular nerve
canals. Its incidence is considered very low
and is reported to be 0.08%, 0.4%, and
0.9%4,5 in various studies. It is suggested that
bifid mandibular canals occur more fre-
quently in females.1,4 Interestingly, 5 of our 6
cases were in women.
Chavez-Lomeli and colleagues2 suggest-
ed that during embryonic development 3
separate canals fuse to form a single
mandibular canal. The bifid and trifid
mandibular canals seen in the present cases
possibly represent unfused canals that per-
sisted as separate, distinct mandibular
canals. Case 4 is the second reported case
in the literature of a trifid mandibular canal.3
Bifid mandibular canals may show multiple
patterns, and 2 distinct classifications were
proposed by Langlais et al4 and Nortje et al5
(Tables 1 and 2).
Each of the nerve canals is surrounded by
upper and lower cortical boundaries that are
easily visible on radiographs. These nerve
canals originate from the mandibular fora-
men. The cortical boundaries surrounding
the nerve canals can fuse to form a triangular
area of bone. If, on a panoramic radiograph,
a triangle having its vertex at the root of sep-
aration of bifid mandibular canal is seen, it is
a pathognomonic feature indicating the pres-
ence of double canals.1 In cases 1 to 5 where
panoramic radiographs were used, this trian-
gular area of bone was identified on the
radiograph. In case 6, bifid canals were iden-
tified incidentally on a CT scan.
There may occasionally be a false appear-
ance of multiple canals on panoramic radio-
graphs. This can be due to the imprint of the
mylohyoid nerve on the internal mandibular
surface where it separates from the inferior
alveolar nerve and travels to the floor of the
mouth.6,7 The false radiographic appear-
ances can also be due to radiologic osteo-
condensation caused by the insertion of the
mylohyoid muscle into the internal mandibu-
lar surface, with a distribution parallel to the
dental canal.1
On panoramic radiographs, to detect bifid
mandibular canals, clinicians must look for
the presence of accessory mandibular fora-
men or the triangular area of bone formed by
the inner cortical boundaries of canals. On a
cross-sectional tomogram or a CT scan (refor-
matted coronal slices), a well-corticated outer
ring of the inferior alveolar canal can be iden-
tified, and the position can be traced in multi-
ple cross-sectional slices until it extends up to
the mental foramen region. The traditional
cortical notching technique can also be used
to identify the canal on CT studies.8 A Denta-
Scan (GE Healthcare) or a SIM-PLANT
(Materialise) software programs can be used
to obtain the dental CT reformatted images.8
784 VOLUME 38 • NUMBER 9 • OCTOBER 2007
Fig 6a Coronal CT view of the mandible in bonewindow demonstrating the bifid mandibular canalimmediately beneath the impacted and invertedmandibular left third molar.
Fig 6b A more posterior coronal CT section of themandible in bone window, showing the mandibularcanal beneath the impacted left third molar. Notethe area of confluence just before the canal sepa-rates into 2 different canals.
Auluck.qxd 9/6/07 11:35 AM Page 784

VOLUME 38 • NUMBER 9 • OCTOBER 2007 785
QUINTESSENCE INTERNATIONAL
Auluck et a l
Identification of the second or third canal
is an important task for the practicing clini-
cian because of its implications on local
anesthetic outcomes. In the authors’ experi-
ence, the inferior alveolar nerve can appear
in various anatomic positions. The nerve
may start out as separate canals within the
ramus of the mandible only to fuse at the
molar region. From there it runs a common
course until the region of the mental fora-
men. This is the most common and easily
identifiable pattern with the triangular bony
island between the 2 canals. It is likely that in
patients with bifid or trifid canals the branch-
es of the nerve run parallel courses within
the body of the mandible until the mental
foramen and possibly end up giving rise to a
secondary mental foramen.
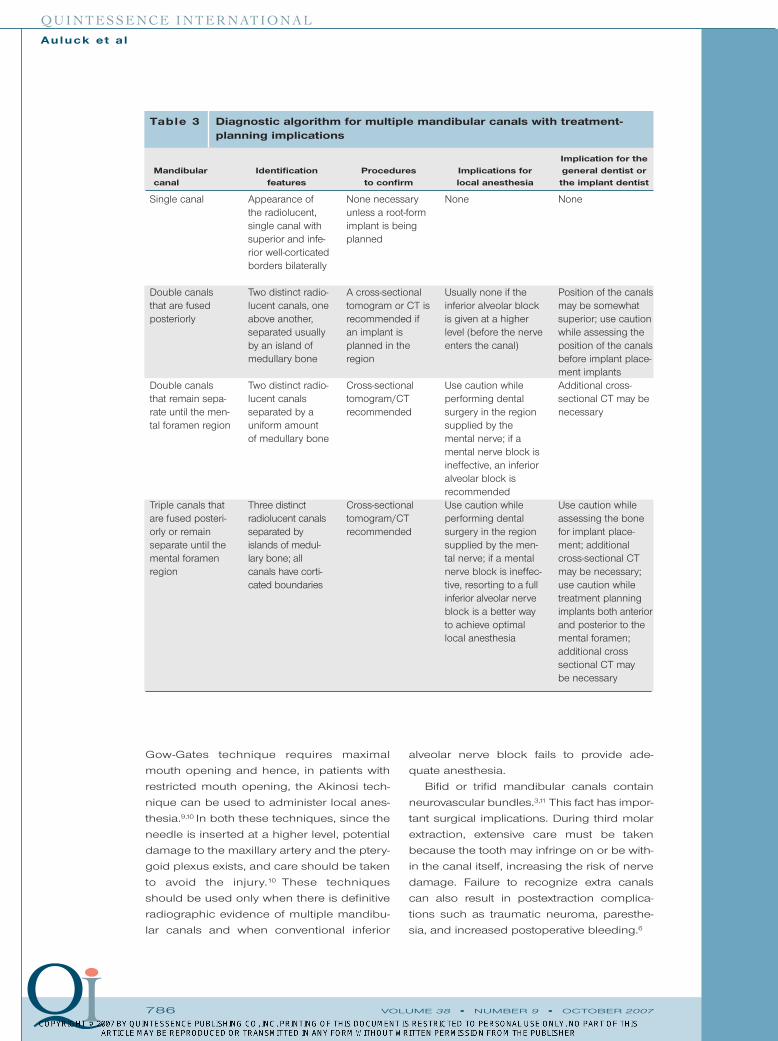
Based on this anatomic variation, an algo-
rithm (Table 3) was developed for a quick
identification of these canals on the
panoramic radiographs, selection of
advanced radiographic procedures, and to
help in the decision-making process. One
should remember that panoramic radio-
graphs and cross-sectional tomograms
should not be prescribed for identification
purposes of these canals alone. If there is
already an indication for obtaining the
panoramic radiograph, either to identify the
position of the tooth in question or to visual-
ize the pathosis that was not completely
seen on an intraoral periapical or occlusal
film, then the radiograph can be examined
for the presence of the mandibular canals.
Inadequate anesthesia is the most com-
mon problem encountered in patients with
bifid mandibular nerve canals. There is no
specific pattern of division or duplication of
the nerve canals.9 This makes it difficult to pre-
dict the efficacy of inferior alveolar nerve
block injections. Inadequate anesthesia of the
region supplied by the mental nerve may be a
problem because 2 separate mental foramina
may exist and the anesthetic solution may
have affected only 1 of the 2 neural bundles.
In cases of bifid canals, a high inferior
alveolar nerve block, such as the Gow-Gates
technique, can be used wherein the anes-
thetic solution is deposited around the trunk
of the mandibular nerve. This technique
simultaneously anesthetizes both the buccal
and lingual nerves along with anomalous or
minor divisions of the mandibular nerve.1,6,9,10
Type I Consists of unilateral or bilateral bifid mandibular canals extending to the third molar or immediatesurrounding area.
Type II Consists of unilateral or bilateral bifid mandibular canals extending along the course of the maincanal and region within the ramus or body of the mandible.
Type III Combination of first 2 categories. Consists of a bifid canal extending to the third molar or surround-ing area or 1 side, as in type 1, and a bifid canal extending along the course of the major canalregions within the ramus or body of mandible in the other side, as in type 2.
Type IV Consists of 2 canals, each of which originates from a separate mandibular foramen and then joinsto form 1 canal.
Table 1 Langlais et al4 classification of bifid mandibular canals
Type I (Most common) Duplicate canals originating from a single mandibular foramen; the canals are usu-ally the same size.
Type Ia The lower canal is smaller. Type Ib The upper canal is the smaller of the 2 canals.Type II A short upper canal extending to the second or third molar areas.Type III (Least common) 2 canals of equal size, arising from separate foramina that join in the molar area.Type IV A double canal variation in which the supplemental canals arise from the retromolar pad area and
join the main canals in the retromolar areas.
Table 2 Nortje et al5 description of the patterns of duplication of mandibularcanals
Auluck.qxd 9/6/07 11:35 AM Page 785
786 VOLUME 38 • NUMBER 9 • OCTOBER 2007
QUINTESSENCE INTERNATIONAL
Auluck et a l
Gow-Gates technique requires maximal
mouth opening and hence, in patients with
restricted mouth opening, the Akinosi tech-
nique can be used to administer local anes-
thesia.9,10 In both these techniques, since the
needle is inserted at a higher level, potential
damage to the maxillary artery and the ptery-
goid plexus exists, and care should be taken
to avoid the injury.10 These techniques
should be used only when there is definitive
radiographic evidence of multiple mandibu-
lar canals and when conventional inferior
alveolar nerve block fails to provide ade-
quate anesthesia.
Bifid or trifid mandibular canals contain
neurovascular bundles.3,11 This fact has impor-
tant surgical implications. During third molar
extraction, extensive care must be taken
because the tooth may infringe on or be with-
in the canal itself, increasing the risk of nerve
damage. Failure to recognize extra canals
can also result in postextraction complica-
tions such as traumatic neuroma, paresthe-
sia, and increased postoperative bleeding.6
Implication for theMandibular Identification Procedures Implications for general dentist or canal features to confirm local anesthesia the implant dentist
Table 3 Diagnostic algorithm for multiple mandibular canals with treatment-planning implications
Appearance ofthe radiolucent,single canal withsuperior and infe-rior well-corticatedborders bilaterally
Two distinct radio-lucent canals, oneabove another,separated usuallyby an island ofmedullary bone
Two distinct radio-lucent canals separated by auniform amountof medullary bone
Three distinct radiolucent canalsseparated byislands of medul-lary bone; allcanals have corti-cated boundaries
Single canal
Double canalsthat are fusedposteriorly
Double canalsthat remain sepa-rate until the men-tal foramen region
Triple canals thatare fused posteri-orly or remainseparate until themental foramenregion
None necessaryunless a root-formimplant is beingplanned
A cross-sectionaltomogram or CT isrecommended ifan implant isplanned in theregion
Cross-sectionaltomogram/CT recommended
Cross-sectionaltomogram/CT recommended
None
Usually none if theinferior alveolar blockis given at a higherlevel (before the nerveenters the canal)
Use caution whileperforming dentalsurgery in the regionsupplied by the mental nerve; if amental nerve block isineffective, an inferioralveolar block is recommendedUse caution whileperforming dentalsurgery in the regionsupplied by the men-tal nerve; if a mentalnerve block is ineffec-tive, resorting to a fullinferior alveolar nerveblock is a better wayto achieve optimallocal anesthesia
None
Position of the canalsmay be somewhatsuperior; use cautionwhile assessing theposition of the canalsbefore implant place-ment implantsAdditional cross-sectional CT may benecessary
Use caution whileassessing the bonefor implant place-ment; additionalcross-sectional CTmay be necessary;use caution whiletreatment planningimplants both anteriorand posterior to themental foramen;additional cross sectional CT may be necessary
Auluck.qxd 9/6/07 11:35 AM Page 786

VOLUME 38 • NUMBER 9 • OCTOBER 2007 787
QUINTESSENCE INTERNATIONAL
Auluck et a l
Epker12 suggested that in surgical proce-
dures such as mandibular osteotomy, it is
necessary to protect the vascularity of the
mandible. Hence, the presence of additional
neurovascular bundles adds to the complex-
ity of surgical procedures. Furthermore, in
cases of trauma, all mandibular fractures
should be handled with care to ensure that
the neurovascular bundles line up exactly, to
avoid impingement when fracture is
reduced. Alignment of the fractured frag-
ments becomes more difficult when the sec-
ond neurovascular bundle is located in a dif-
ferent plane.6 Therefore, while planning the
surgical procedures, the dental surgeon
must look for radiographic evidence of such
an anomaly, determine its location, and mod-
ify the surgical techniques accordingly.
As alveolar bone resorbs in the proximity
of the mental foramen, patients with a
mandibular prosthesis experience pain
because of the pressure on the neurovascu-
lar bundle. In cases of bifid mandibular canal
with branches extending to the third molar
and retromolar pad areas, such a problem
can be encountered.6 Therefore, recognition
of this possible anomaly will allow the clini-
cian to modify the prosthetic design and
impression techniques.
Another important aspect of duplication
of the mandibular canals concerns the iden-
tification of the neurovascular bundles pre-
cisely before placement of any root-form
implants. The duplicate canals may or may
not be visible on head and neck radio-
graphs; it is possible that the bone in cross
section can be evaluated more easily using
either a complex motion tomography, cone
beam CT, or conventional CT utilizing dental
reformation software.13
Awareness and detection of bifid canals is
of considerable interest to the general den-
tist. Careful radiographic observation can
help the clinician recognize this anomaly,
achieve appropriate local anesthesia, and
modify dental treatment accordingly.
Identification of the multiple mandibular
canals also will help the clinician in the plan-
ning and placement of root-form implants
within the mandibular body.
ACKNOWLEDGMENT
The authors would like to thank Dr Gary Heir, professor,
Department of Diagnostic Sciences, University of
Medicine and Dentistry of New Jersey, New Jersey
Dental School, Newark, for allowing us to use the mate-
rial in case 6.
REFERENCES
1. Sanchis JM, Penarrocha M, Soler F. Bifid mandibular
canal. J Oral Maxillofac Surg 2003;61:422–424.
2. Chavez-Lomeli ME, Mansilla Lory J, Pompa JA, Kjaer
I. The human mandibular canal arises from three
separate canals innervating different tooth groups.
J Dent Res 1996;75:1540–1544.
3. Auluck A, Pai KM. Trifid mandibular nerve canal.
Dentomaxillofac Radiol 2005;34:259.
4. Langlais RP, Broadus R, Glass BJ. Bifid mandibular
canals in panoramic radiographs. J Am Dent Assoc
1985;110:923–926.
5. Nortje CJ, Farman AG, Grotepass FW. Variation in
the normal anatomy of inferior dental (mandibu-
lar) canal: A retrospective study of panoramic radi-
ographs from 3612 routine dental patients. Br J
Oral Surg 1977;15(1):55–63.
6. Wilson S, Johns P, Fuller PM.The inferior alveolar and
mylohyoid nerves: An anatomic study and relation-
ship to local anaesthesia of the anterior mandibular
teeth. J Am Dent Assoc 1984; 108:350-352.
7. Sillanpaa M, Vuori V, Lehtinen R. The mylohyoid
nerve and mandibular anesthesia. Int J Oral
Maxillofac Surg 1988;17:206–207.
8. Mupparapu M, Beideman R. Imaging for maxillofa-
cial reconstruction and implantology. In: Fonseca
RJ (ed). Oral and Maxillofacial Surgery. Vol 7:
Reconstructive and implant surgery. Philadelphia:
Saunders, 2000:17–34.
9. Desantis JL, Liebow C. Four common mandibular
nerve anomalies that lead to local anesthesia fail-
ures. J Am Dent Assoc 1996;127:1081–1086.
10. Meechan JG. How to overcome failed local anaes-
thesia. Br Dent J 1999;186:15–20.
11. Claeys V, Wackens G. Bifid mandibular canal:
Literature review and case report. Dentomaxillofac
Radiol 2005;34:55–58.
12. Epker BN. Vascular consideration in orthognathic
surgery. I. Mandibular osteotomies. Oral Surg Oral
Med Oral Pathol 1984;57:467–472.
13. Mupparapu M, Singer SR. Implant imaging for the
dentist. J Can Dent Assoc 2004;70(1):32.
Auluck.qxd 9/6/07 11:35 AM Page 787