multidisciplinary treatment of thoracic malignancies
TRANSCRIPT

Multidisciplinary treatment of thoracic malignancies
Jussuf T. Kaifi, M.D., Ph.D., F.A.C.S.
Chief, Division for Cardiothoracic Surgery
Co-Director, Clinical Trials Office
Ellis Fischel Cancer Center

Medical Oncologist
Pulmonologist
Radiologist
RadiationOncologist
Surgical
Oncology
Multidisciplinary Care in Thoracic Diseases
PATIENT
Nutritionist
Respiratory therapists
Cancer RegistrarsNurse Navigators
Patient Navigators
• HIGHEST VALUE
• ENROLL IN CLINICAL TRIALS

Value in (multidisciplinary) Healthcare
‘The State of Value in U.S. Health Care’, University of Utah, Nov. 2017

Smoking in Missouri
• 7th highest smoking rate in the US (22.1%)
• Average pack of cigarrettes: $5.25
• 30 pack years:
– 219,000 cigarettes
– $57,488

Lung cancer
• USA:
– >220,000 new lung cancer cases/year
– 160,000 deaths/year
– 440 deaths/day
• Worldwide: Never-smoker: 20% men, >50% women
• Overall 5-year survival: 18%
Boeing 747: 416 passengers
Parkin et al. Global cancer statistics, 2002., CA Cancer J Clin. 2005
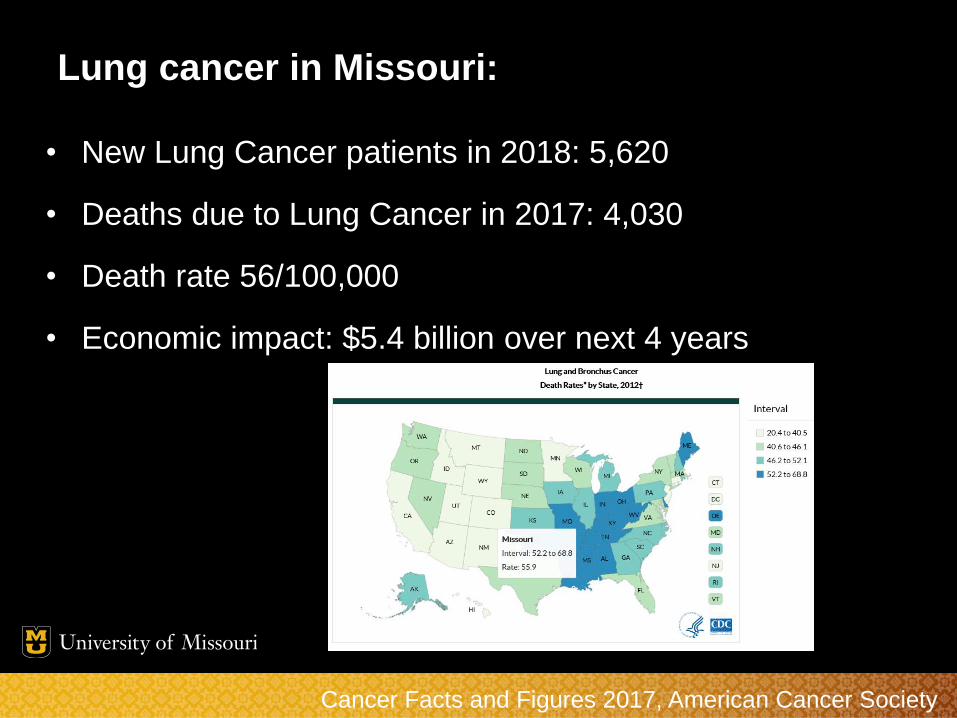
Lung cancer in Missouri:
• New Lung Cancer patients in 2018: 5,620
• Deaths due to Lung Cancer in 2017: 4,030
• Death rate 56/100,000
• Economic impact: $5.4 billion over next 4 years
Cancer Facts and Figures 2017, American Cancer Society

Operable patient: Surgery
Lymph node status:
N0 N1
NSCLC: Stage I/II
Tumor size

NSCLC Survival Stage I/II: 30-60%
Silvestri GA, Gould MK et al, Chest 2007, 132(3) 179S

Low-dose CT screening improves survival
53,454 high-risk patients
Randomized:
3x/year low-dose CT vs. CXR
(Effective radiation doses:
chest x-ray: 0.1 mSv; LDCT: 2 mSv; traditional chest CT: 7 mSv)
low-dose CT:
20% reduction in lung cancer-related mortality

Lung cancer screening eligibility
- 55-80 years old
- ≥30py smoking history
- Current smoker or quit within past 15 years
- Ellis Fischel Cancer Center:
- >1500 screened since 2016

Screening with LDCT: - 1 out of 4 has lung nodule
- False-positive rate >95%
Benign
(necrotizing granuloma/
histoplasmosis)
Lung cancer
(NSCLC stage IA)

Case• 72 yo female
• 50 py smoking history
• Screening low-dose CT:
right upper lobe lung mass
• PET/CT: FDG-avid, no mediastinal
lymphadenopathy
• Good PFTs (FEV1: 2l, DLCO 85%)
• Robotic wedge (frozen: cancer), right upper
lobectomy with mediastinal lymphadenectomy
• Pathology: stage IA NSCLC (SCC)

Lung Lobectomy
• Indications:
– Stage I-II
– Selected stage IIIA (single-level N2)
– Selected stage IV (oligometastatic to lung, brain or adrenal)
• 30 day mortality: 2.2%
– Society for Thoracic Surgery (STS) Database 2010:
n=18,800 from 111 centers in the US

Minimally invasive (VATS) Lobectomy
• Standard lobectomy
• No rib spreading
• Small incisions
• Safe, oncologically equivalent
• Decreased pain, faster recovery
Hansen et al., Surg Endosc 2011

Slow adoption of VATS lobectomy in the US
AHRQ HCUPnet database
Open
Open
VATS16 years


Robotic lung surgery:
Same advantages as VATS,
better vision and instrumentation

Robotic lobectomy trend 2009-17
Premier multihospital database
Open
VATS
Robotic
%
2009 2017

Multicenter registry study of long-term
oncologic results of robotic lobectomy
• 2002-2010, 3 centers, n=325
• >95% stage I
• Median operative time: 206 minutes
• Conversion rate: 8%
• Mortality rate: 0.3%
• Major complications (BPF, PE, ARI, hemorrhage, MI): 3.7%
• Median chest tube duration: 3 days (1-23)
• Median LOS: 5 days (2-28) Park BJ, et al. Robotic lobectomy for
NSCLC: long term oncologic results
JTCVS 2012

Robotic thoracic surgery at Mizzou
• 05/2016 - 04/2018: 117 cases
• 54 lung lobectomies:
– No 90-day mortality, 7 conversions (13%), 1 re-operation (hemothorax),
no major complications (BPF, PE, ARI, MI),
median LOS: 3 days (range 1-14), 5 (9%) readmissions
• 63 others (wedges, thymectomies, esophagectomies,
mediastinal/pleural tumors, etc.):
– No 90-day mortality/conversions/major complications
– 44 lung wedges, median LOS: 2 days (range 1-8), 2 (5%) readmissions

Case• 79yo male, 80py
• Low-dose screening CT: RLL lung mass
• Biopsy: TTF-1+ adenocarcinoma
• Clinical stage IA
• Medically inoperable: FEV1 0.6l, home oxygen, immobility
• Treatment:
Stereotactic body radiation

SBRT• Stage IA lung cancer
• 55 Gy in 5 fractions, 30 minutes daily over 5 days
• Meticulous tissue sparing (esophagus, chest wall)
• Challenges: central tumors with proximity to airway, major
vessels, spinal cord; local recurrences
Heinzerling, The Cancer Journal 2011

SBRT: NCCN guidelines
• Medically inoperable
• No lymph node metastases (cN0)
• Tumor size <5cm

Higher risk patients: Sublobar resections
(wedge resection/segmentectomy)
McKenna RJ, Ann Thorac Surg 2008
Wedge resection Segmentectomy Lobectomy
Local recurrence 16-31% 2-23% 1-11%
5-year survival 26-69% 43-93% 67-90%

Ablative techniques (RFA, microwave)• Percutaneous, CT-guided ablation:
– Microwave superior: lung has low electrical conductivity & poor thermal
conduction, allowing larger ablation zone than RFA
• Peripheral lesions <3cm (clinical stage I)
• Contraindication: adjacent to major bronchovascular
structures, diaphragm or esophagus; severe emphysema
• Few clinical studies, can be repeated, less collateral damage,
can be integrated in multimodal treatment
2 years post-ablationRUL NSCLC Microwave ablation

NSCLC Survival by Stage
Silvestri GA, Gould MK et al, Chest 2007, 132(3) 179S
N2 N3
Stage III: definitive chemoradiation

mN2L1 mN2L2+ cN2L1 cN2L2+
5-yr survival 34% 11% 8% 3%
Andre F et al. J Clin Oncol 2000;18:2981-2989.
702 pts, N2 disease
(stage IIIA)
Resection with curative
intent
N2: ≥ Stage IIIA
Single level N2: better survival after surgery

Stage IIIA (T1-3, single level N2)
resectable
Neoadjuvant
chemo(radio)therapy
If ypN2: adjuvant mediastinal radiation
Stable disease or remission:
Surgery
Multimodal treatment for stage IIIA (single level N2)

NSCLC Survival by Stage
Silvestri GA, Gould MK et al, Chest 2007, 132(3) 179S
Stage IV:
Median survival
8-10 months
Palliative
chemotherapy

Oligometastatic NSCLC
• Synchronous or metachronous
• Sites: lung, brain, and adrenal gland
• Multimodal management: radiation, surgery, chemotherapy
• Brain: SBRT / surgery followed by SBRT/WBRT; prospective single-arm
phase II trial: 3-year OS 18%
• Adrenals: adrenalectomy / SBRT (5 year survival: 34% vs. 0%)
• Phase II RCT: local consolidative therapy (RT/surgery) to oligometastatic
lesions (≤3), not progressing on systemic treatment:
median PFS 11.9 vs. 3.9 months
De Ruysscher et al; J Thorac Oncol. 2012
Raz et al; Ann Thorac Surg 2011
Gomez et al; Lancet Oncol 2016

Targeted treatment to improve
survival of early stage lung cancer
Resected NSCLC stage I-III:
• 5-year survival: 30-60%
• Adjuvant chemotherapy (4 cycles; platinum-based double):
+5% survival benefit / 5 years
Hirsch et al., Lancet 2017The IALT Collaborative Group, NEJM 2004
JBR.10 Trial Investigators. NEJM 2005

Targeted therapies: NSCLC
• EGFR overexpression/mutation (IHC, mutational analysis):
– 30% never-smoking females of East Asian origin, 15% in Caucasians (adenocarcinomas)
– Erlotinib: PFS benefit: 10.4 vs. 5.2 months (median)
• EML4/ALK fusion (FISH):
– 5% NSCLC/adenocarcinomas
– Crizotinib: PFS benefit for untreated stage IV: 10.9 vs. 7.0 months (median)
• PD-L1 overexpression (IHC):
– 30% of NSCLC PD-L1+
– Immune checkpoint inhibitors, also for SCC
– Pembrolizumab: PFS benefit for stage IV: 10.3 vs. 9.0 months (median); response rates 45% vs. 28%
Shepherd et al, NEJM 2005
Garon et al, NEJM 2015
Herbst et al, NEJM 2016

Clinical Trials Office, EFCC
• Ken Baker, RN (Manager)
• Angela Waller, RN
• Sue Prenger, RN
• Elizabeth Porting-Jackson
• Marta Fuemmeler
• Sherezad Mistry
Co-Directors:
• Puja Nistala, MD
• Jussuf T. Kaifi, MD

– ALCHEMIST group
– NCI-sponsored National Clinical Trials Network (NCTN)
initiative
– Addresses the need to refine therapy for early-stage NSCLC

observation
observation
