multidisciplinary management of locally advanced breast cancer
TRANSCRIPT

© 1999 Blackwell Science Inc., 1075-122X/99/$14.00/0The Breast Journal, Volume 5, Number 5, 1999 303–307
Multidisciplinary Management of
Locally Advanced Breast Cancer
Robert W. Carlson, MD and Anne M. Favret, MD
Department of Medicine, Division of Oncology, Stanford University Medical Center,Stanford, California
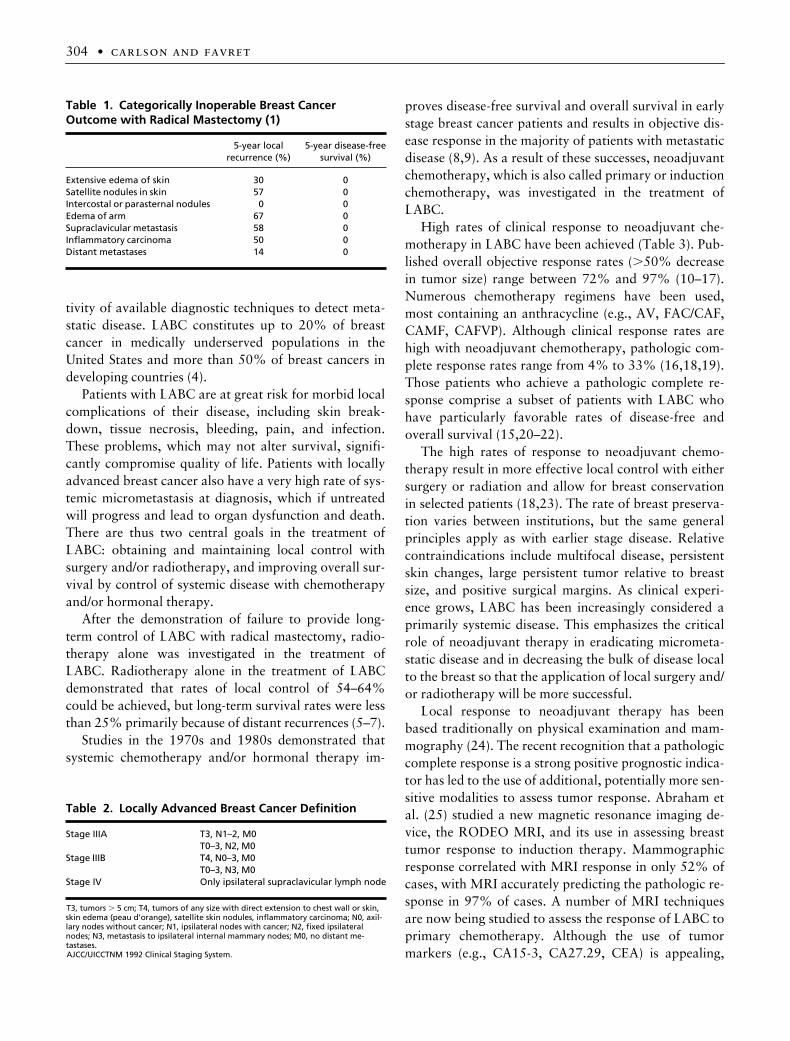
satellite nodules, intercostal or parasternal nodules, armedema, supraclavicular metastasis, inflammatory carci-noma, or distant metastasis, or the presence of two ormore of the following: ulceration of the skin, skin edemaof limited extent (more than one-third of the breast), fix-ation to the chest wall, axillary lymph nodes larger than2.5 cm, or fixation of axillary lymph nodes to the skinor deep structures of the skin (Table 1). This classicaldescription of the clinical contraindications to the pri-mary surgical management of primary breast cancer is,in general, still valid today. In Haagensen’s series of pa-tients with these grave signs, local recurrence rates were42% despite radical mastectomy, and no patient sur-vived disease-free for 5 years. Patients with these charac-teristics (and having no distant metastases) are currentlyincluded in the category of locally advanced breast can-cer (LABC). The poor outcome of these patients whentreated with radical mastectomy led to the investigationof other treatment strategies.
The definition of LABC has evolved from that ofHaagensen and Stout, and generally includes TNMstage III and some stage IV disease, characterized by tu-mors larger than 5 cm, bulky or matted axillary nodes,inflammatory carcinoma (T4d), and patients with iso-lated ipsilateral supraclavicular lymph nodes as theironly site of metastatic disease (M1) (Table 2) (3). Someinvestigators also include patients with primary tumorslarger than 4 cm in diameter or with multiply involvedaxillary lymph nodes on physical examination. Locallyadvanced breast cancer thus represents a heterogeneousand evolving group of patients.
Comparisons of LABC patient outcomes across dif-ferent series are difficult because of the evolving criteriafor patient selection and because of the increasing sensi-
j
Abstract:
The treatment of locally advanced breast can-cer is aimed at achieving long-term local control with localsurgery and/or radiation therapy and at improving disease-free and overall survival through the application of systemiccytotoxic chemotherapy and hormonal therapy. Studies of lo-cal therapy alone with surgery or radiotherapy have demon-strated high rates of local recurrence and low rates of long-term survival. The application of anthracycline-based neoad-juvant chemotherapy has resulted in rates of response rang-ing from 72% to 97%, clinical complete responses of 12–52%,and pathologic complete responses of 4–33%. Multidisci-plinary treatment with neoadjuvant therapy, followed by lo-cal surgery and/or radiation therapy, followed by additionalchemotherapy, has resulted in rates of local control that ex-ceed 80%, and 5-year survival rates exceeding 50% are notunusual. The use of anthracycline-based neoadjuvant chemo-therapy in the treatment of locally advanced breast cancer isthus now firmly established. Research in the treatment of lo-cally advanced breast cancer is needed to further define theoptimal method of local therapy and the role of new agentssuch as the taxanes.
j
Key Words:
breast cancer, local control, locally advancedbreast cancer, neoadjuvant chemotherapy, survival
I
Address correspondence and reprint requests to: Robert W. Carlson,MD, 1000 Welch Rd., Suite 202, Palo Alto, CA 94304, U.S.A., or e-mail:[email protected]
n 1943, Haagensen and Stout (1,2) identified clinicalfeatures predicting poor outcome in women with pri-
mary breast cancer treated with radical mastectomy. Thesefeatures include the presence of extensive skin edema,
304
•
carlson and favret
tivity of available diagnostic techniques to detect meta-static disease. LABC constitutes up to 20% of breastcancer in medically underserved populations in theUnited States and more than 50% of breast cancers indeveloping countries (4).
Patients with LABC are at great risk for morbid localcomplications of their disease, including skin break-down, tissue necrosis, bleeding, pain, and infection.These problems, which may not alter survival, signifi-cantly compromise quality of life. Patients with locallyadvanced breast cancer also have a very high rate of sys-temic micrometastasis at diagnosis, which if untreatedwill progress and lead to organ dysfunction and death.There are thus two central goals in the treatment ofLABC: obtaining and maintaining local control withsurgery and/or radiotherapy, and improving overall sur-vival by control of systemic disease with chemotherapyand/or hormonal therapy.
After the demonstration of failure to provide long-term control of LABC with radical mastectomy, radio-therapy alone was investigated in the treatment ofLABC. Radiotherapy alone in the treatment of LABCdemonstrated that rates of local control of 54–64%could be achieved, but long-term survival rates were lessthan 25% primarily because of distant recurrences (5–7).
Studies in the 1970s and 1980s demonstrated thatsystemic chemotherapy and/or hormonal therapy im-
proves disease-free survival and overall survival in earlystage breast cancer patients and results in objective dis-ease response in the majority of patients with metastaticdisease (8,9). As a result of these successes, neoadjuvantchemotherapy, which is also called primary or inductionchemotherapy, was investigated in the treatment ofLABC.
High rates of clinical response to neoadjuvant che-motherapy in LABC have been achieved (Table 3). Pub-lished overall objective response rates (
.
50% decreasein tumor size) range between 72% and 97% (10–17).Numerous chemotherapy regimens have been used,most containing an anthracycline (e.g., AV, FAC/CAF,CAMF, CAFVP). Although clinical response rates arehigh with neoadjuvant chemotherapy, pathologic com-plete response rates range from 4% to 33% (16,18,19).Those patients who achieve a pathologic complete re-sponse comprise a subset of patients with LABC whohave particularly favorable rates of disease-free andoverall survival (15,20–22).
The high rates of response to neoadjuvant chemo-therapy result in more effective local control with eithersurgery or radiation and allow for breast conservationin selected patients (18,23). The rate of breast preserva-tion varies between institutions, but the same generalprinciples apply as with earlier stage disease. Relativecontraindications include multifocal disease, persistentskin changes, large persistent tumor relative to breastsize, and positive surgical margins. As clinical experi-ence grows, LABC has been increasingly considered aprimarily systemic disease. This emphasizes the criticalrole of neoadjuvant therapy in eradicating micrometa-static disease and in decreasing the bulk of disease localto the breast so that the application of local surgery and/or radiotherapy will be more successful.
Local response to neoadjuvant therapy has beenbased traditionally on physical examination and mam-mography (24). The recent recognition that a pathologiccomplete response is a strong positive prognostic indica-tor has led to the use of additional, potentially more sen-sitive modalities to assess tumor response. Abraham etal. (25) studied a new magnetic resonance imaging de-vice, the RODEO MRI, and its use in assessing breasttumor response to induction therapy. Mammographicresponse correlated with MRI response in only 52% ofcases, with MRI accurately predicting the pathologic re-sponse in 97% of cases. A number of MRI techniquesare now being studied to assess the response of LABC toprimary chemotherapy. Although the use of tumormarkers (e.g., CA15-3, CA27.29, CEA) is appealing,
Table 1. Categorically Inoperable Breast Cancer Outcome with Radical Mastectomy (1)
5-year localrecurrence (%)
5-year disease-freesurvival (%)
Extensive edema of skin 30 0Satellite nodules in skin 57 0Intercostal or parasternal nodules 0 0Edema of arm 67 0Supraclavicular metastasis 58 0Inflammatory carcinoma 50 0Distant metastases 14 0
Table 2. Locally Advanced Breast Cancer Definition
Stage IIIA T3, N1–2, M0T0–3, N2, M0
Stage IIIB T4, N0–3, M0T0–3, N3, M0
Stage IV Only ipsilateral supraclavicular lymph node
T3, tumors
.
5 cm; T4, tumors of any size with direct extension to chest wall or skin, skin edema (peau d’orange), satellite skin nodules, inflammatory carcinoma; N0, axil-lary nodes without cancer; N1, ipsilateral nodes with cancer; N2, fixed ipsilateral nodes; N3, metastasis to ipsilateral internal mammary nodes; M0, no distant me-tastases.AJCC/UICCTNM 1992 Clinical Staging System.

Multidisciplinary Management of Locally Advanced Breast Cancer
•
305
there are no studies supporting their use in monitoringthe response to treatment of LABC.
A multidisciplinary approach thus appears to providean optimal outcome in patients with LABC. Most con-temporary treatment programs utilize neoadjuvant an-thracycline-based chemotherapy, followed by localtreatment consisting of radiation with or without sur-gery, followed by additional chemotherapy and hor-monal therapy. Overall long-term survival with this ap-proach ranges from 36% to 73% (Table 4) (14,21,22).
There exists, however, controversy regarding the op-timal local treatment for patients with LABC. Reportedlocal control rates using multimodality treatments varybetween 60% and 87% (Table 5) (12,14,17,21,22). Astudy by the Eastern Cooperative Oncology Group es-tablished the role of radiotherapy in decreasing local re-currence in LABC (26). After mastectomy, 332 patientsreceived six cycles of an anthracycline-containing regi-men and were subsequently randomized to radiotherapyor observation. The group who received radiotherapyhad fewer local recurrences (15% versus 24%), butthere was no difference in time to relapse or overall sur-vival. There are several randomized studies evaluatingthe use of surgery and radiotherapy for patients with
stage III breast cancer. The Cancer and Leukemia GroupB treated 113 patients with neoadjuvant chemotherapyfor three cycles, after which 91 were deemed operable(17). The patients were then randomized to have a mas-tectomy or receive radiotherapy, followed by mainte-nance chemotherapy for 2 years. At a median follow-upof 37 months, there was no significant difference in dis-ease-free or overall survival between the two groups.DeLena et al. (12) randomized 132 women with LABCwho had received three cycles of doxorubicin and vin-cristine (AV) to either mastectomy or radiotherapy, fol-lowed by seven additional cycles of AV. There was nosignificant difference between the groups in patterns oftreatment failure or overall survival. However, otherstudies demonstrate an advantage to the combination ofradiotherapy and surgery (27,28).
The optimal length of treatment and the benefit ofmaintenance chemotherapy remain unresolved. In astudy by DeLena et al. (11), patients were randomizedto receive further chemotherapy or observation afterneoadjuvant chemotherapy and radiotherapy. Therewas a statistically significant improvement in rates oflocal recurrence and disease-free survival in patientswho received maintenance chemotherapy. More recentstudies have failed to support this finding (10,29,30).
Hormone therapy is of unrefutable benefit in thetreatment of primary or metastatic hormone receptor-positive breast cancer. Although data is limited inLABC, tamoxifen should benefit this subset of patients.A randomized trial compared radiotherapy alone, radio-therapy plus chemotherapy, radiotherapy plus hormonetherapy, and radiotherapy plus hormone therapy pluschemotherapy (31). The best survival results were seenin the group who received chemotherapy and hormonaltherapy, supporting the use of tamoxifen in LABC.
Table 3. Clinical Response to Neoadjuvant Chemotherapy
Series ChemotherapyResponserate (%)
Completeresponserate (%)
Pathologiccomplete
response rate (%)
Perloff et al. (17) CAFVP 72 18Touboul et al. (22) AVCF 79 42DeLena et al. (12) AV 86 15Hortobagyi et al. (14) FAC 87 17Veronesi et al. (19) Multiple 90 12 4Lippman et al. (16) CATPrMFL 90 52 33Jacquillat et al. (21) VTMFAP 91 23Merajver et al. (18) CAMF 97 28Kuerer et al. (36) CAF 19
C
5
cyclophosphamide; A
5
adriamycin (doxorubicin); F
5
5-flourouracil; V
5
vincristine; P
5
prednisone; Pr
5
premarin; M
5
methotrexate; L
5
leucovorin.
Table 4. Locally Advanced Breast Cancer 5-Year Survival
Series Therapy Survival (%)
Valagussa et al. (38) CT
1
RT
1
CT 36Cardenas et al. (37) CT
1
S
1
RT
1
CT 56Hortobagyi et al. (14) CT
6
RT
6
S
1
CT 55Jacquillat et al. (21) CT
1
RT
1
CT 65Touboul et al. (22) CT
1
RT
6
S
1
CT 80
CT
5
chemotherapy; RT
5
radiotherapy; S
5
surgery.

306
•
carlson and favret
As the focus of treatment of LABC continues toevolve toward effectively treating micrometastatic dis-ease, there exist many new areas to be explored. Potentnew agents have high rates of response in metastaticbreast cancer. Paclitaxel, docetaxel, and vinorelbine, forexample, have proven activity in advanced breast cancerand warrant investigation in LABC (32–34). The use ofhigh-dose therapy with stem cell support is currently un-der investigation, but studies to date have not shown asignificant difference in clinical or pathologic response,disease-free survival, or overall survival (35).
LABC provides a unique opportunity to evaluate theeffects of treatment in vivo and possibly modify subse-quent therapy based on response. Treatment programsutilizing chemotherapy tailored to response warrant in-vestigation. Therefore methods for assessing response totreatment are an important area for investigation andinclude studies aimed at MRI, PET scanning, and radio-labeled monoclonal antibody imaging.
The management of LABC is a multidisciplinary en-deavor. Ideally all involved specialists (pathologists,diagnostic radiologists, breast surgeons, radiation oncol-ogists, and medical oncologists) should review the perti-nent data and assist in determining an appropriate treat-ment plan. Patients with suspected LABC should havebilateral mammograms and an ultrasound of the in-volved breast. A fine needle aspirate (FNA) or core nee-dle biopsy is adequate for confirming the diagnosis andobtaining hormone receptors and other biomarker levelssuch as the level of HER-2/neu expression. Prior to initi-ation of chemotherapy, patients should have liver func-tion studies, a chest radiograph, and a bone scan, withsubsequent plain films of any abnormal areas to rule outdistant metastatic disease. Between three and six cyclesof anthracycline-based induction chemotherapy is givenwith careful physical examination before each cycle toassess disease response. After completion of neoadju-vant chemotherapy, repeat imaging of the breast is per-formed to evaluate persistent disease. Based on tumor
response, patients may proceed to breast-conservingtherapy, mastectomy followed by radiotherapy, or ra-diotherapy alone to provide local control. Regardless ofwhether a patient undergoes a surgical procedure, allpatients should have radiotherapy to the breast (or chestwall) and supraclavicular and axillary lymph nodes. Atthis time, it is reasonable to use a taxane-based regimenfor consolidative therapy for four to six cycles. All pa-tients who are estrogen receptor positive receive 5 yearsof tamoxifen.
The use of multidisciplinary treatment, includingneoadjuvant chemotherapy, has substantially improvedthe rate of local control and survival of women withLABC. Continued research is necessary to more accu-rately define which therapies are optimal for selectedsubsets of women with LABC and to identify more ef-fective and less toxic methods of treatment.
REFERENCES
1. Haagensen C, Stout AP. Carcinoma of the breast: crite-ria of inoperability.
Am Surg
1943;118:859.2. Haagensen C.
Diseases of the breast.
Philadelphia:W.B. Saunders, 1971.
3. Beahrs O, Henson D, Hutter R, Kennedy B.
Manual forstaging of cancer.
Philadelphia: J.B. Lippincott, 1993:161–67.4. Seidman H, Gelb SK, Silverberg E, LaVerda N, Lubera
JA. Survival experience in the breast cancer detection demon-stration project.
Cancer J Clin
1987;37:258.5. Barker JL, Nelson AJ, Montague ED. Inflammatory
carcinoma of the breast.
Radiology
1976;121:173–76.6. Rubens RD, Armitage P, Winter PJ, Tong D, Hayward
JL. Prognosis in inoperable stage III carcinoma of the breast.
Eur J Cancer
1977;13:805–11.7. Bruckman JE, Harris JR, Levene MB, Chaffey JT, Hell-
man S. Results of treating stage III carcinoma of the breast byprimary radiation therapy.
Cancer
1979;43:985–93.8. Early Breast Cancer Trialists’ Collaborative Group.
Tamoxifen for early breast cancer: an overview of the ran-domised trials.
Lancet
1998;351:1451–67.9. Early Breast Cancer Trialists’ Collaborative Group.
Table 5. Rates of Local Control
Series TherapyMedian
follow-up (months)Local
control (%)
DeLena et al. (12) CT
1
RT/S
1
CT 69Hortobagyi et al. (14) CT
6
S
1
RT
1
CT 59 85Jacquillat et al. (21) CT
1
RT
1
CT 40 87Perloff et al. (17) CT
1
S/RT
1
CT 77Touboul et al. (22) CT
1
RT
6
S
1
CT 93 84
CT
5
chemotherapy; S
5
surgery; RT
5
radiotherapy.

Multidisciplinary Management of Locally Advanced Breast Cancer
•
307
Polychemotherapy for early breast cancer: an overview of therandomised trials.
Lancet
1998;352:930–42.10. Buzdar AU, Singletary SE, Booser DJ, Frye DK, Wasaff
B, Hortobagyi GN. Combined modality treatment of stage IIIand inflammatory breast cancer. M.D. Anderson Cancer Cen-ter experience.
Surg Oncol Clin N Am
1995;4:715–34.11. DeLena M, Zucali R, Viganotti G, Valagussa P, Bona-
donna G. Combined chemotherapy-radiotherapy approach inlocally advanced (T3b–T4) breast cancer.
Cancer ChemotherPharmacol
1978;1:53–59.12. DeLena M, Varini M, Zucali R. Multimodality treat-
ment for locally advanced breast cancer.
Cancer Clin Trials
1981;4:229–30.13. Heys SD, Sarkar TK, Ah-See AK, Eremin JM, Brit-
tenden J, Eremin O. Multimodality treatment in the manage-ment of locally advanced breast cancer.
J R Coll Surg Edinb
1993;38:9–15.14. Hortobagyi G, Ames F, Buzdar A. Management of
stage III primary breast cancer with primary chemotherapy,surgery and radiation therapy.
Cancer
1988;62:2507–16.15. Kuerer H, Newman L, Smith T,
et al.
Clinical course ofbreast cancer patients with complete pathologic primary tumorand axillary lymph node response to doxorubicin-based neoad-juvant chemotherapy.
J Clin Oncol
1999;17:460–69.16. Lippman M, Sorace R, Bagley C. Treatment of locally
advanced breast cancer using primary induction chemotherapywith hormonal synchronization followed by radiation therapywith or without debulking surgery.
Natl Cancer Inst Monogr
1986;1:153.17. Perloff M, Lesnick GJ, Korzun A,
et al.
Combinationchemotherapy with mastectomy or radiotherapy for stage IIIbreast carcinoma: a Cancer and Leukemia Group B study.
JClin Oncol
1988;6:261–69.18. Merajver SD, Weber BL, Cody R,
et al.
Breast conser-vation and prolonged chemotherapy for locally advancedbreast cancer: the University of Michigan experience.
J ClinOncol
1997;15:2873–81.19. Veronesi U, Bonadonna G, Zurrida S,
et al.
Conserva-tion surgery after primary chemotherapy in large carcinomas ofthe breast [see comments].
Ann Surg
1995;222:612–18.20. Feldman LD, Hortobagyi GN, Buzdar AU, Ames FC, Blu-
menschein GR. Pathological assessment of response to inductionchemotherapy in breast cancer.
Cancer Res
1986;46:2578–81.21. Jacquillat C, Baillet F, Weil M,
et al.
Results of a con-servative treatment combining induction (neoadjuvant) andconsolidation chemotherapy, hormonotherapy, and externaland interstitial irradiation in 98 patients with locally advancedbreast cancer (IIIA–IIIB).
Cancer
1988;61:1977–82.22. Touboul E, Buffat L, Lefranc JP,
et al.
Possibility ofconservative local treatment after combined chemotherapy andpreoperative irradiation for locally advanced noninflammatorybreast cancer [see comments].
Int J Radiat Oncol Biol Phys
1996;34:1019–28.23. Bonadonna G, Veronesi U, Brambilla C. Primary che-
motherapy to avoid mastectomy in tumors with diameters ofthree centimeters or more.
J Natl Cancer Inst
1990;82:1539–45.24. Helvie MA, Joynt LK, Cody RL, Pierce LJ, Adler DD,
Merajver SD. Locally advanced breast carcinoma: accuracy ofmammography versus clinical examination in the prediction ofresidual disease after chemotherapy.
Radiology
1996;198:327–32.
25. Abraham DC, Jones RC, Jones SE,
et al.
Evaluation ofneoadjuvant chemotherapeutic response of locally advancedbreast cancer by magnetic resonance imaging.
Cancer
1996;78:91–100.
26. Olson J, Neuberg D, Pandya K,
et al.
The role of radio-therapy in the management of operable locally advanced breastcarcinoma.
Cancer
1997;79:1138–49.27. Pierce LJ, Lippman M, Ben-Baruch N,
et al.
The effectof systemic therapy on local-regional control in locally advancedbreast cancer.
Int J Radiat Oncol Biol Phys
1992;23:949–60.28. Perez CA, Fields JN, Fracasso PM,
et al.
Managementof locally advanced carcinoma of the breast. II. Inflammatorycarcinoma.
Cancer
1994;74:466–76.29. Schaake-Koning C, van der Linden EH, Hart G, En-
gelsman E. Adjuvant chemo- and hormonal therapy in locallyadvanced breast cancer: a randomized clinical study.
Int J Ra-diat Oncol Biol Phys
1985;11:1759–63.30. Rouesse J, Friedman S, Sarrazin D,
et al.
Primary che-motherapy in the treatment of inflammatory breast carcinoma:a study of 230 cases from the Institut Gustave-Roussy.
J ClinOncol
1986;4:1765–71.31. Bartelink H, Rubens RD, van der Schueren E, Sylvester
R. Hormonal therapy prolongs survival in irradiated locallyadvanced breast cancer: a European Organization for Researchand Treatment of Cancer randomized phase III trial.
J Clin On-col
1997;15:207–15.32. Piccart M. Docetaxel: a new defense in the manage-
ment of breast cancer.
Anticancer Drugs
1995;6:7–11.33. Moliterni A, Tarenzi E, Capri G,
et al.
Pilot study ofprimary chemotherapy with doxorubicin plus paclitaxel inwomen with locally advanced or operable breast cancer.
SeminOncol
1997;24:S17-10–S17-14.34. Trudeau M. Docetaxel (taxotere): an overview of first-
line monotherapy.
Semin Oncol
1995;22:17–21.35. Ayash L, Elias A, Ibrahim J. High-dose multimodality
therapy with autologous stem-cell support for stage IIIB breastcarcinoma.
J Clin Oncol
1998;16:1000–07.36. Kuerer HM, Newman LA, Buzdar AU,
et al.
Pathologictumor response in the breast following neoadjuvant chemo-therapy predicts axillary lymph node status [see comments].
Cancer J Sci Am
1998;4:230–36.37. Cardenas J, Ramirez T, Noriega J. Multidisciplinary
therapy for locally advanced breast cancer: an update.
Proc AmSoc Clin Oncol
1987;6:67.38. Valagussa P, Zambetti M, Bignami PD,
et al.
T3b-T4breast cancer: factors affecting results in combined modalitytreatment.
Clin Exp Metastasis
1983;1:191–202.