multidisciplinary approach to acute pancreatitis medical...
TRANSCRIPT
Timothy B. Gardner, MD, FACG
Multidisciplinary Approach to Acute Pancreatitis
Medical Management of
Acute Pancreatitis
Timothy B. Gardner, MD MS FACG Assistant Professor of Medicine
Geisel School of Medicine at Dartmouth
Director, Pancreatic Disorders
Medical Director, Islet Cell Transplant Program
Section of Gastroenterology and Hepatology
Dartmouth-Hitchcock Medical Center
ACG Postgraduate Course
1. Fluid Resuscitation
Objectives
2. Antibiotic Therapy
3. Nutritional Support
4. Guideline Recommendations
Timothy B. Gardner, MD, FACG
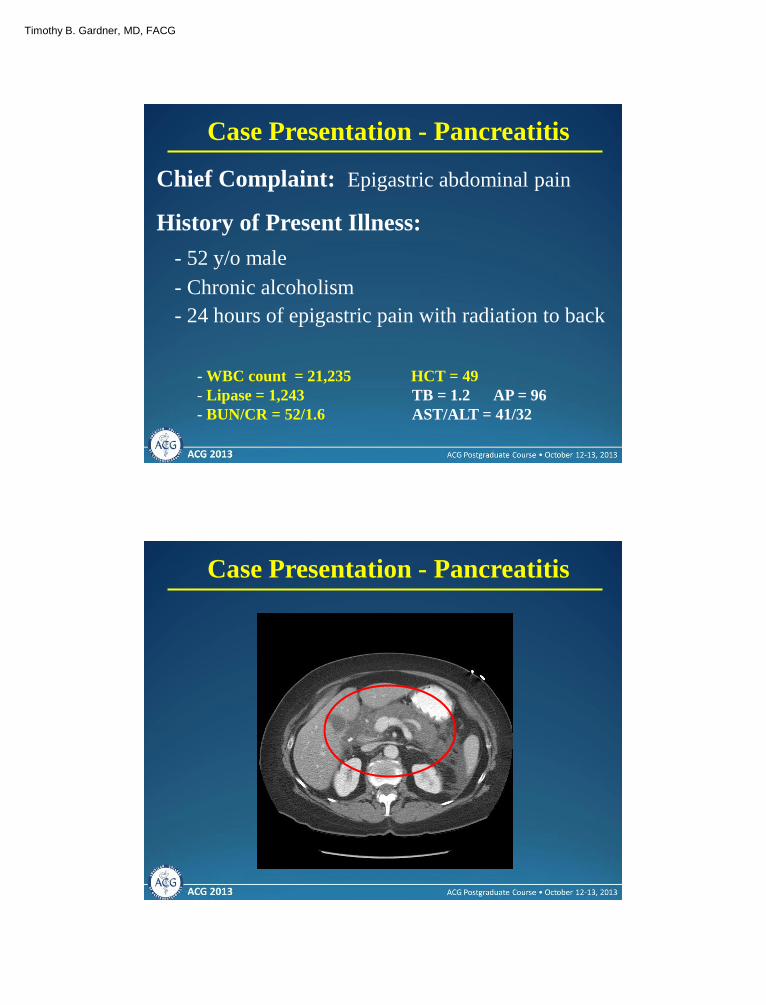
Chief Complaint: Epigastric abdominal pain
Case Presentation - Pancreatitis
History of Present Illness:
- 52 y/o male
- Chronic alcoholism
- 24 hours of epigastric pain with radiation to back
- WBC count = 21,235 HCT = 49
- Lipase = 1,243 TB = 1.2 AP = 96
- BUN/CR = 52/1.6 AST/ALT = 41/32
Case Presentation - Pancreatitis
Timothy B. Gardner, MD, FACG
Case Presentation - Pancreatitis
Questions to Consider
What is this entity?
What can I do medically to
improve this patient’s
outcome?
1. Fluid Resuscitation
Objectives
2. Antibiotic Therapy
3. Nutritional Support

Timothy B. Gardner, MD, FACG
Fluid Resuscitation
• Acute pancreatitis leads to approximately 210,000 admissions annually – most common GI admission
• Associated with significant morbidity and mortality of approximately 5%
• There are no pharmacological therapies with a proven clinical benefit for treating acute pancreatitis
Alterations in the Pancreatic Microcirculation Hypovolemia
Increased Permeability – free radicals
Microthrombi
Acinar Cell Injury Proinflammatory mediators
(TNF, Bradykinin, Il-1, IL-6)
Further Capillary Vasconstriction
Release of second stage proinflammatory mediators
Fluid Resuscitation
Timothy B. Gardner, MD, FACG
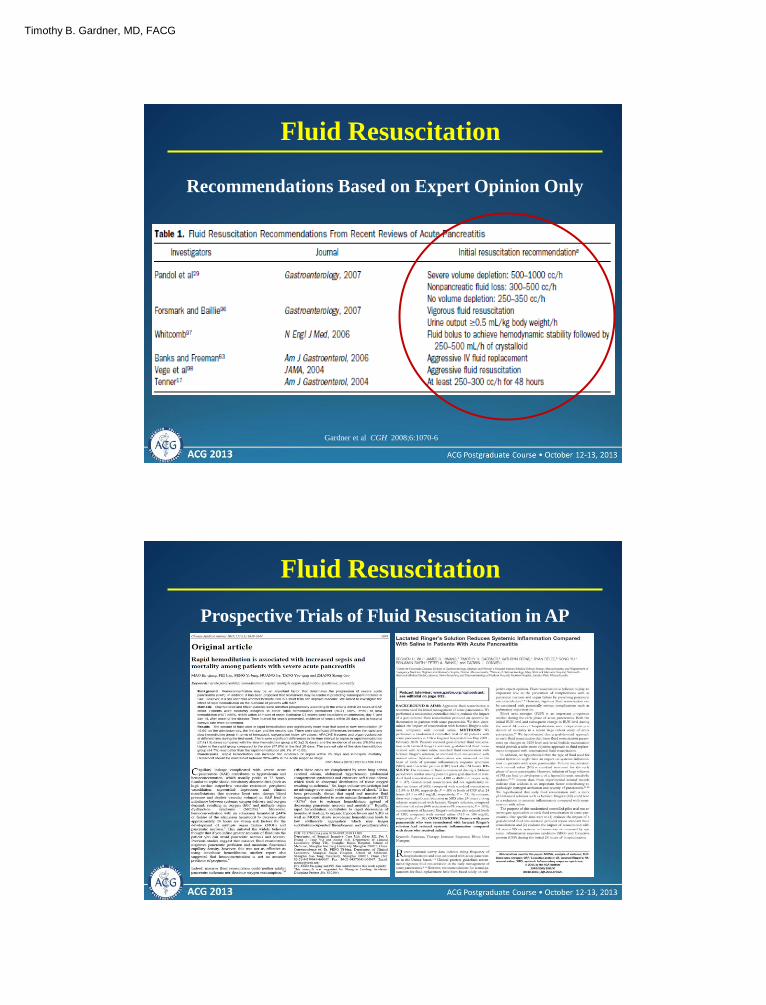
Gardner et al CGH 2008;6:1070-6
Fluid Resuscitation
Recommendations Based on Expert Opinion Only
Fluid Resuscitation
Prospective Trials of Fluid Resuscitation in AP
Timothy B. Gardner, MD, FACG
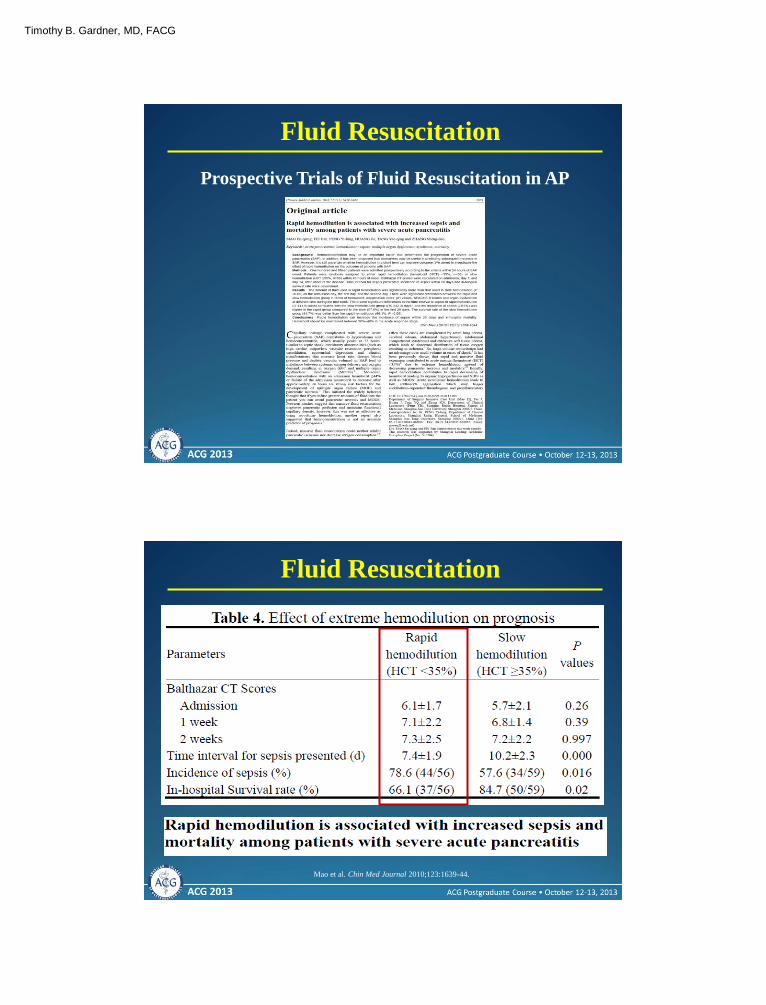
Fluid Resuscitation
Prospective Trials of Fluid Resuscitation in AP
Mao et al. Chin Med Journal 2010;123:1639-44.
Fluid Resuscitation
Timothy B. Gardner, MD, FACG
Fluid Resuscitation
Prospective Trials of Fluid Resuscitation in AP
• Praised for large number of
patients and only those with
SAP included
• Criticized for a somewhat
unusual treatment approach
Mao et al. Chin Med Journal 2010;123:1639-44.
Fluid Resuscitation
Prospective Trials of Fluid Resuscitation in AP
Timothy B. Gardner, MD, FACG
Wu, et al. Clin Gastro and Hepatology. 2011;9:710-7.
Group 1 Group 4 Group 3 Group 2
Goal-Directed Therapy
Standard of Care Therapy
LR LR NS NS
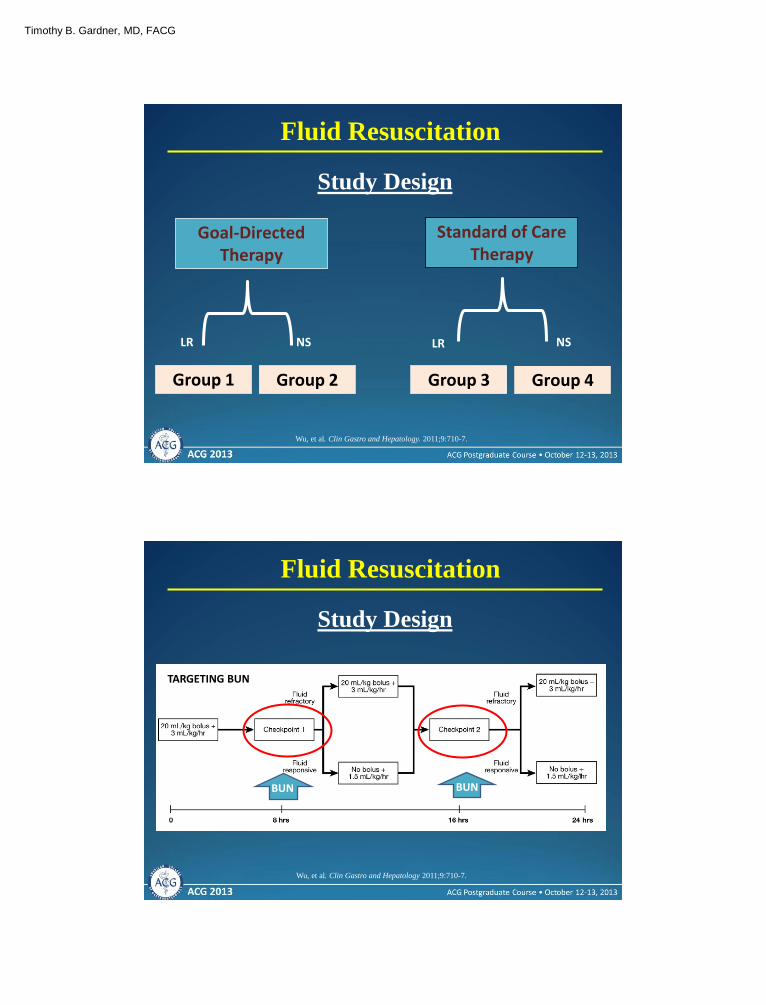
Fluid Resuscitation
Study Design
Wu, et al. Clin Gastro and Hepatology 2011;9:710-7.
Fluid Resuscitation
Study Design
TARGETING BUN
BUN BUN
Timothy B. Gardner, MD, FACG
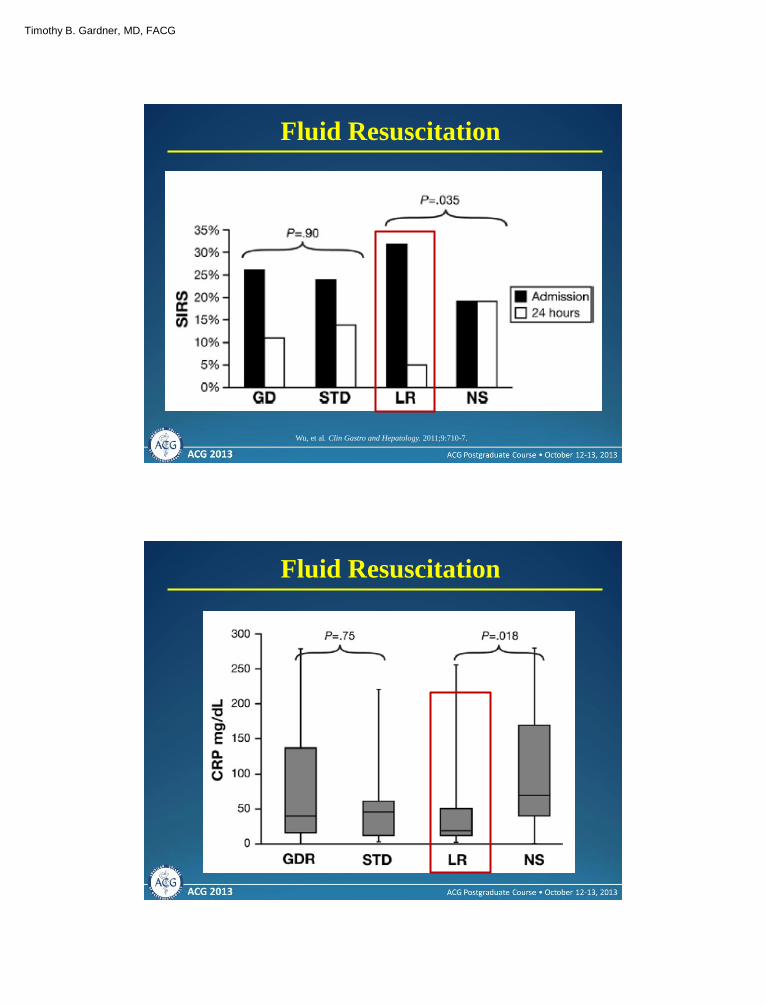
Fluid Resuscitation
Wu, et al. Clin Gastro and Hepatology. 2011;9:710-7.
Fluid Resuscitation
Timothy B. Gardner, MD, FACG
Fluid Resuscitation
Prospective Trials of Fluid Resuscitation in AP
• Praised for employing
standard clinical
resuscitation parameters
• Criticized for small number
of patients and surrogate
clinical outcomes
Wu, et al. Clin Gastro and Hepatology 2011;9:710-7.
Guideline Recommendations
Timothy B. Gardner, MD, FACG
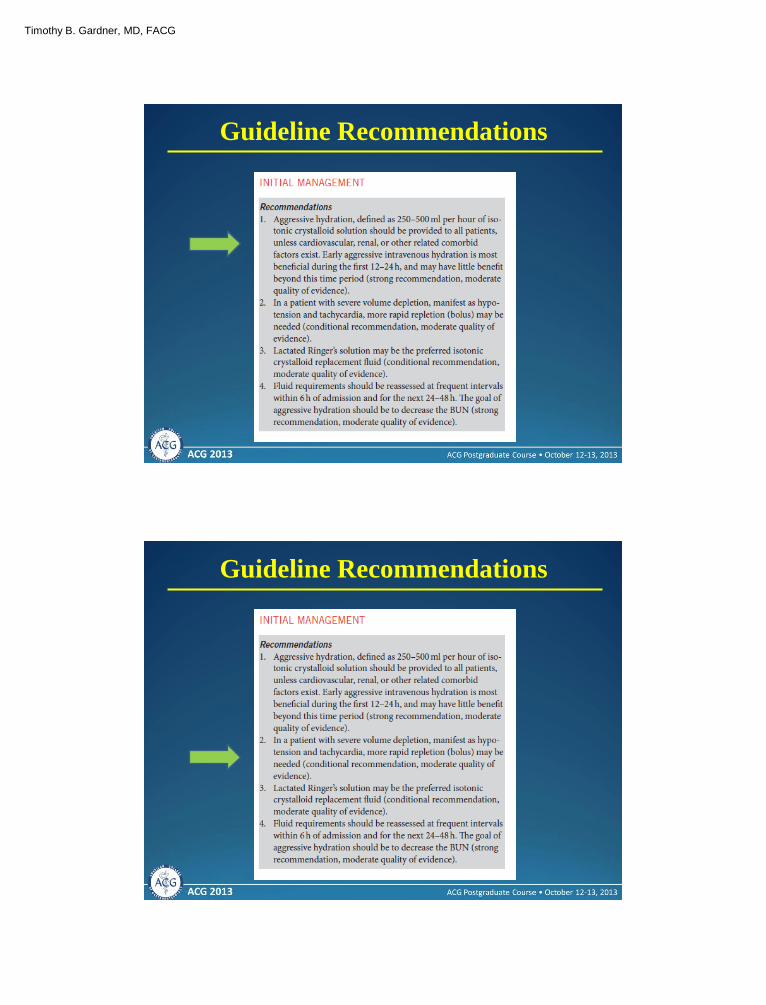
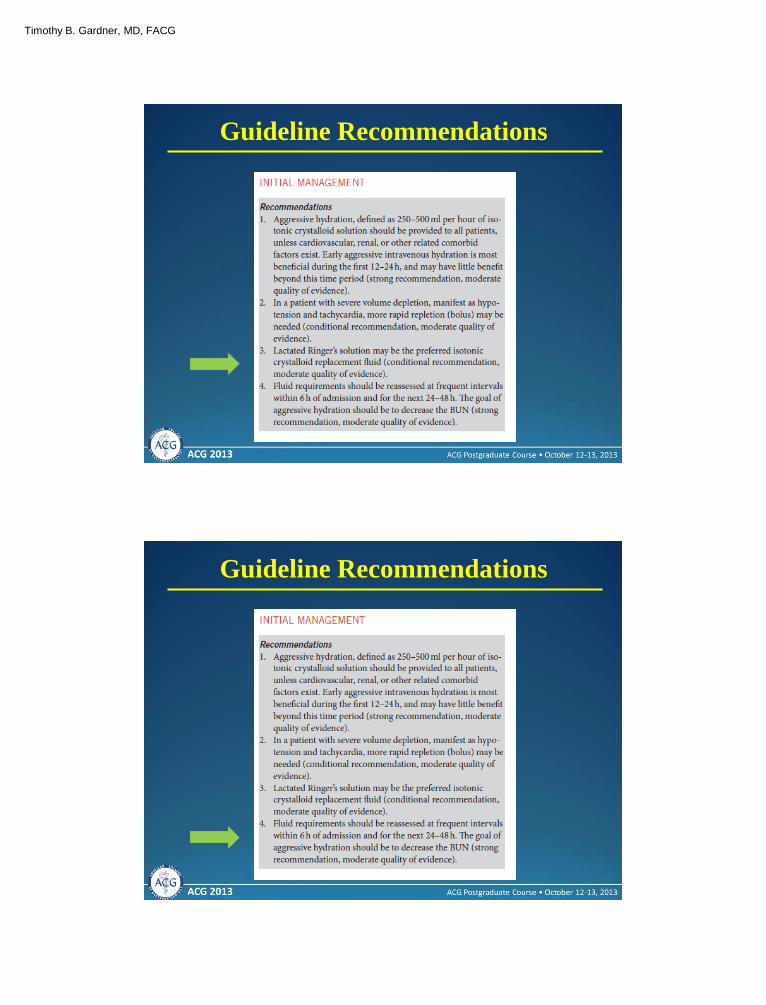
Guideline Recommendations
Guideline Recommendations
Timothy B. Gardner, MD, FACG
Guideline Recommendations
Guideline Recommendations
Timothy B. Gardner, MD, FACG
1. Fluid Resuscitation
Objectives
2. Antibiotic Therapy
3. Nutritional Support
Antibiotic Therapy
Admission Antibiotics “Do they prevent a bad clinical outcome?”
Infected Pancreatic Necrosis “Can we get away with medical therapy only?”
Timothy B. Gardner, MD, FACG
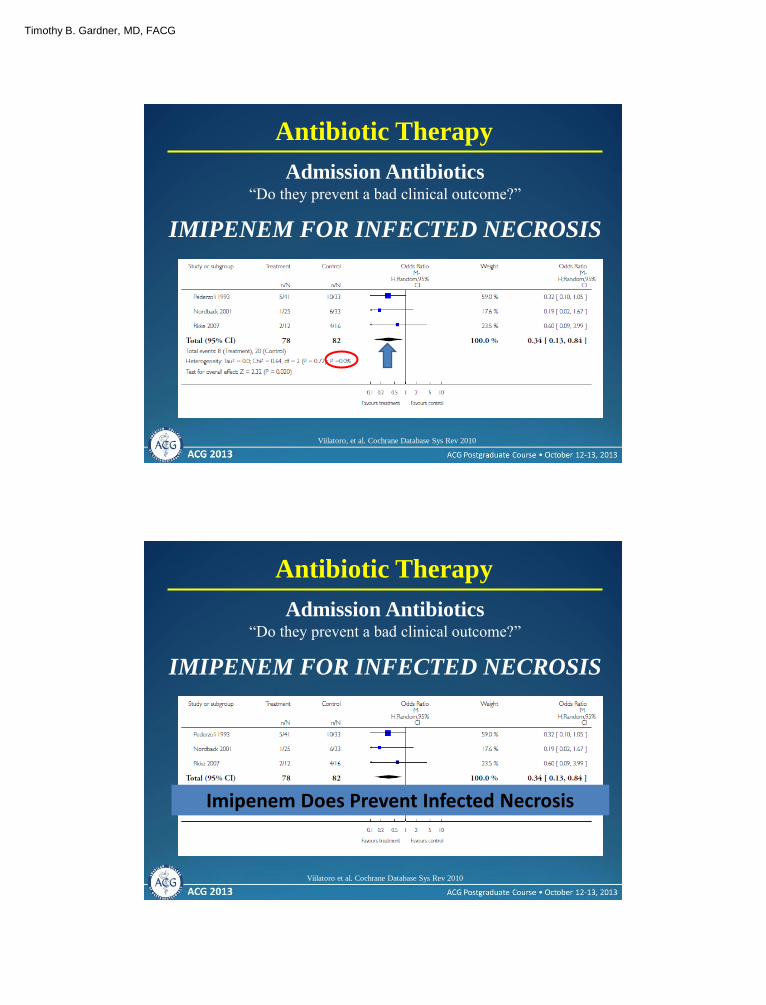
Antibiotic Therapy
Admission Antibiotics “Do they prevent a bad clinical outcome?”
Viilatoro, et al. Cochrane Database Sys Rev 2010
IMIPENEM FOR INFECTED NECROSIS
Antibiotic Therapy
Admission Antibiotics “Do they prevent a bad clinical outcome?”
Viilatoro et al. Cochrane Database Sys Rev 2010
IMIPENEM FOR INFECTED NECROSIS
Imipenem Does Prevent Infected Necrosis
Timothy B. Gardner, MD, FACG
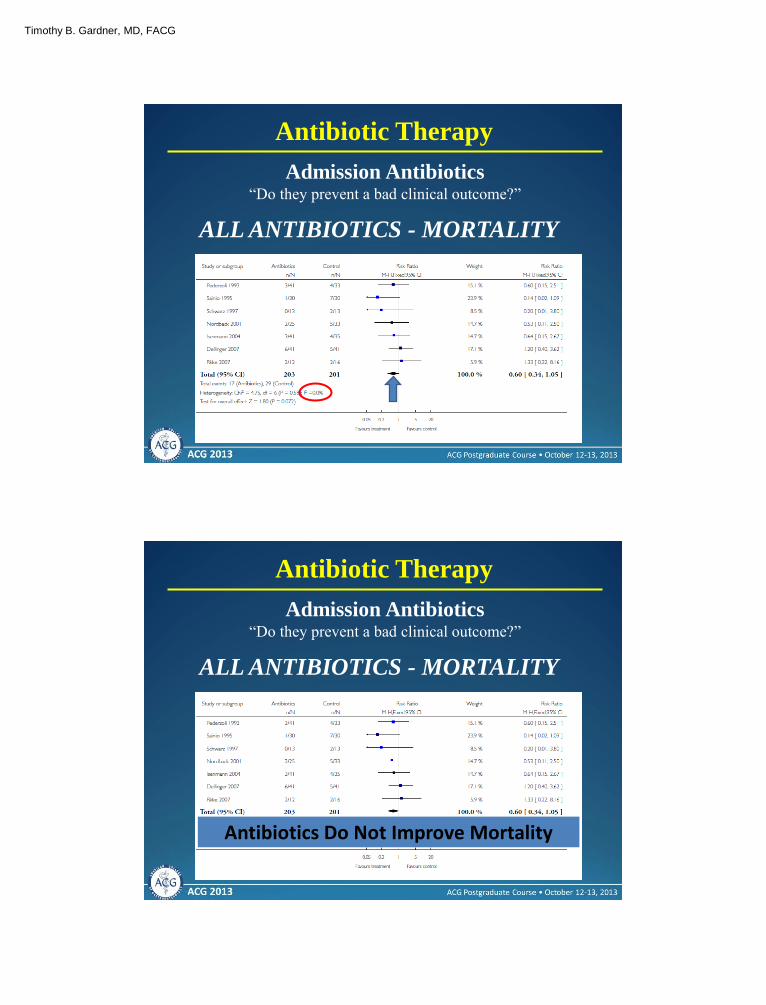
Antibiotic Therapy
Admission Antibiotics “Do they prevent a bad clinical outcome?”
ALL ANTIBIOTICS - MORTALITY
Antibiotic Therapy
Admission Antibiotics “Do they prevent a bad clinical outcome?”
ALL ANTIBIOTICS - MORTALITY
Antibiotics Do Not Improve Mortality
Timothy B. Gardner, MD, FACG
Garg, et al. Clin Gastro and Hepatology 2010;8:1089-4.
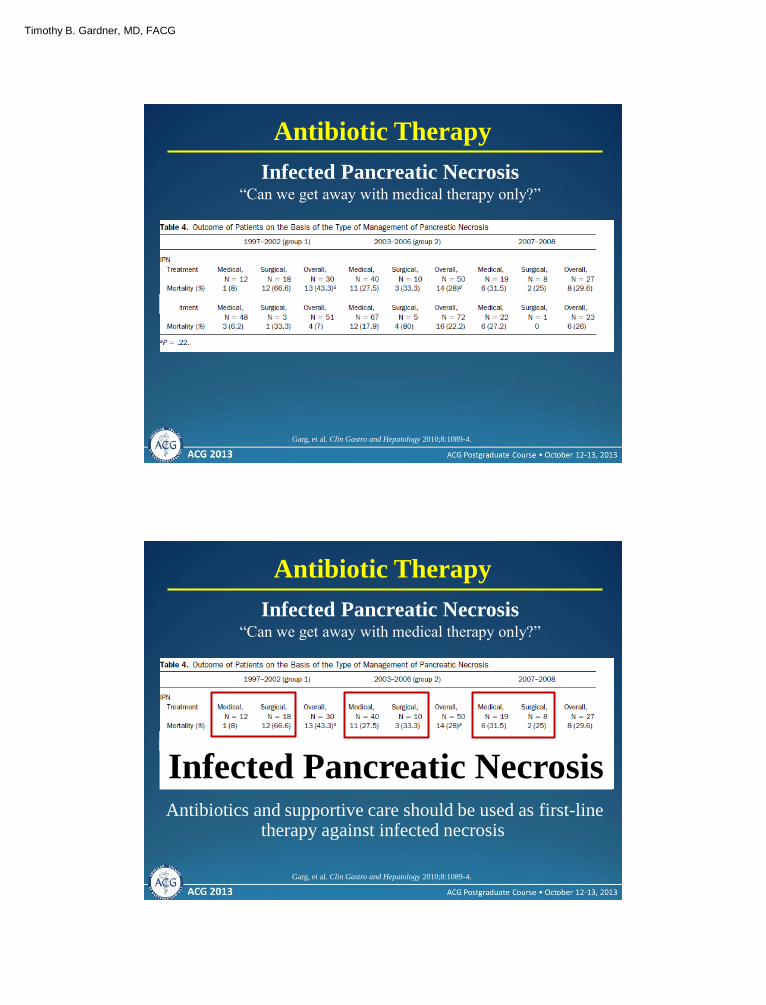
Antibiotic Therapy
Infected Pancreatic Necrosis “Can we get away with medical therapy only?”
Garg, et al. Clin Gastro and Hepatology 2010;8:1089-4.
Antibiotics and supportive care should be used as first-line therapy against infected necrosis
Infected Pancreatic Necrosis
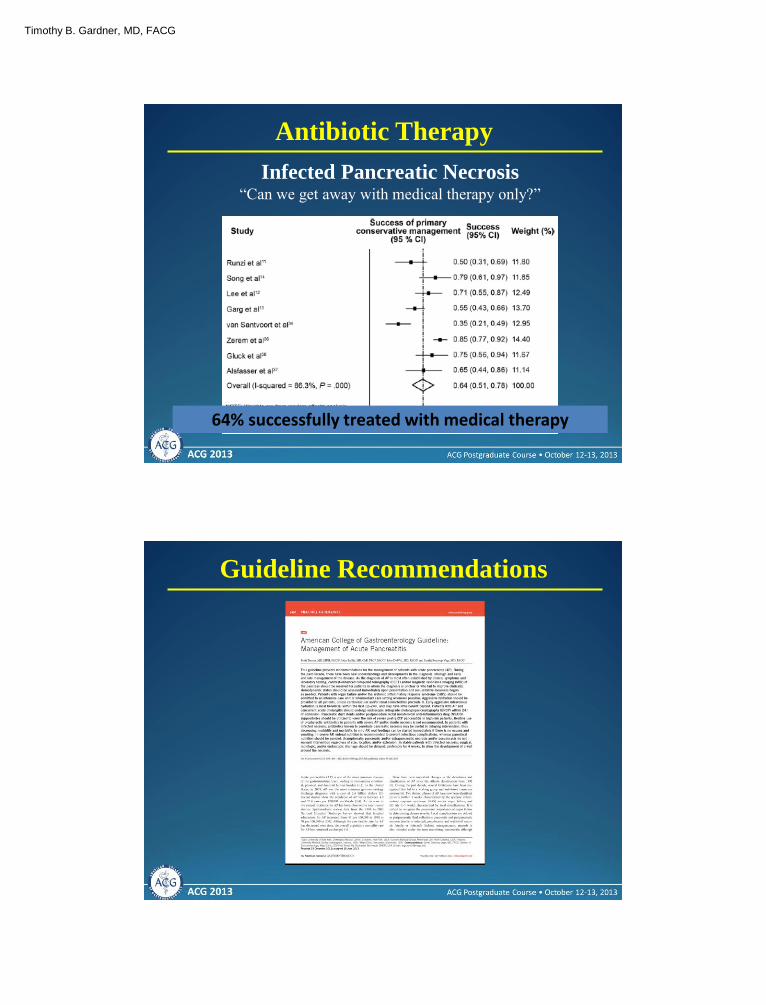
Antibiotic Therapy
Infected Pancreatic Necrosis “Can we get away with medical therapy only?”
Timothy B. Gardner, MD, FACG
Antibiotic Therapy
Infected Pancreatic Necrosis “Can we get away with medical therapy only?”
Mouli, et al. Gastroenterology 2013;144:333-40.
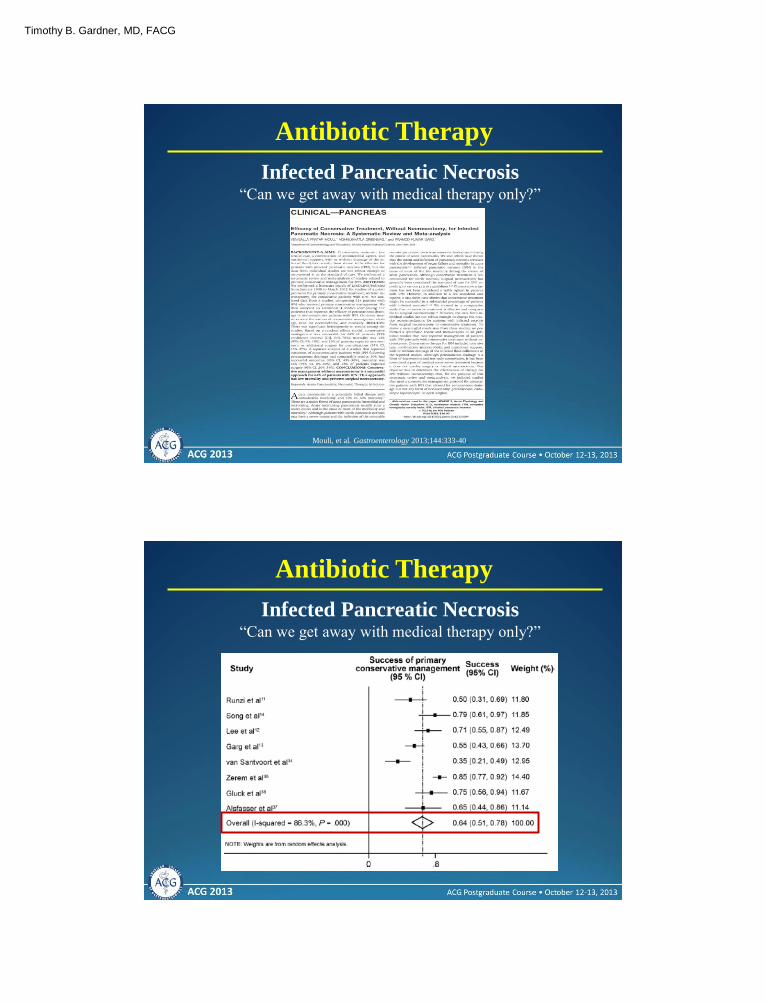
Antibiotic Therapy
Infected Pancreatic Necrosis “Can we get away with medical therapy only?”
Timothy B. Gardner, MD, FACG
Antibiotic Therapy
Infected Pancreatic Necrosis “Can we get away with medical therapy only?”
64% successfully treated with medical therapy
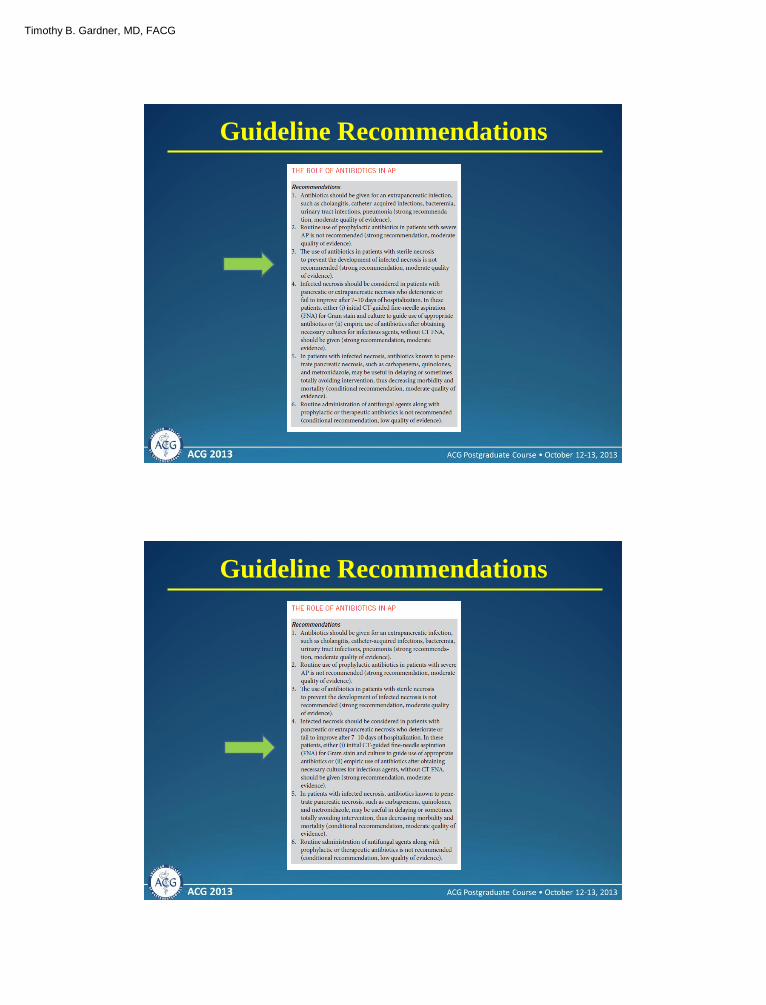
Guideline Recommendations

Timothy B. Gardner, MD, FACG
Guideline Recommendations
Guideline Recommendations
Timothy B. Gardner, MD, FACG
Guideline Recommendations
Guideline Recommendations

Timothy B. Gardner, MD, FACG
Guideline Recommendations
Guideline Recommendations

Timothy B. Gardner, MD, FACG
1. Fluid Resuscitation
Objectives
2. Antibiotic Therapy
3. Nutritional Support
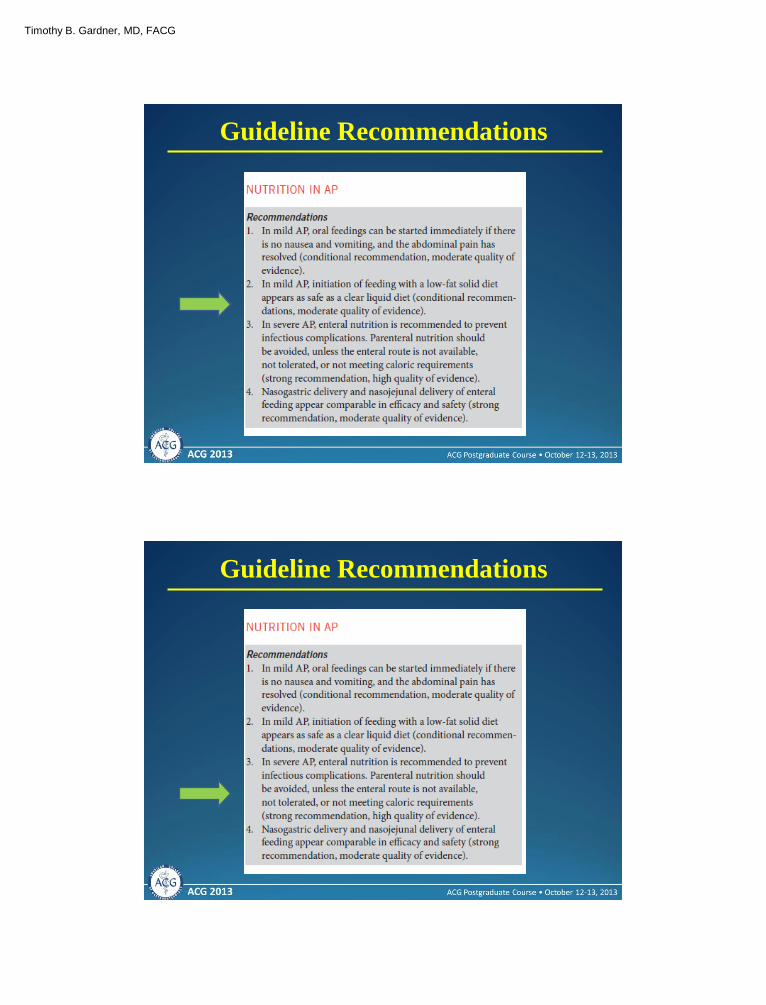
Nutritional Support
Mild Disease
• Most patients able to eat within 7 days
• Initial diet can be low-fat (no need to start
with clear liquids)
• Do not use probiotics
Timothy B. Gardner, MD, FACG
Nutritional Support
Severe Disease
• Start low fat enteral nutrition as soon as
possible (Peptamen)
• Nasogastric tube feedings probably comparable
to nasojejunal feedings
• Avoid TPN unless cannot deliver full nutritional
support enterally
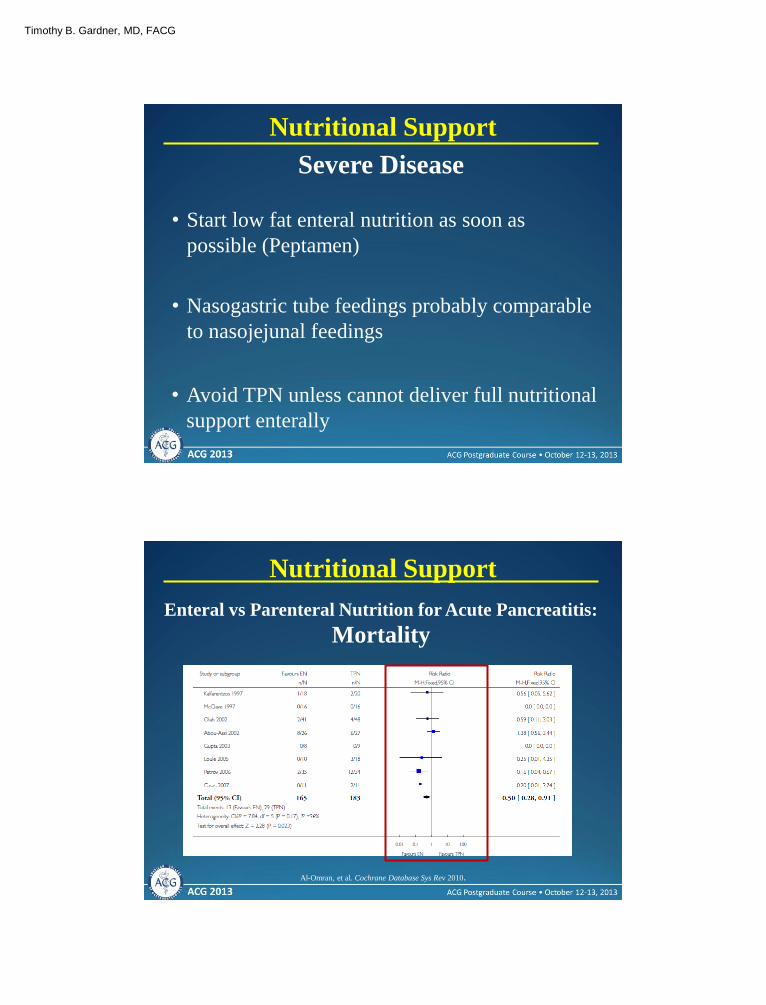
Nutritional Support
Enteral vs Parenteral Nutrition for Acute Pancreatitis:
Mortality
Al-Omran, et al. Cochrane Database Sys Rev 2010.
Timothy B. Gardner, MD, FACG
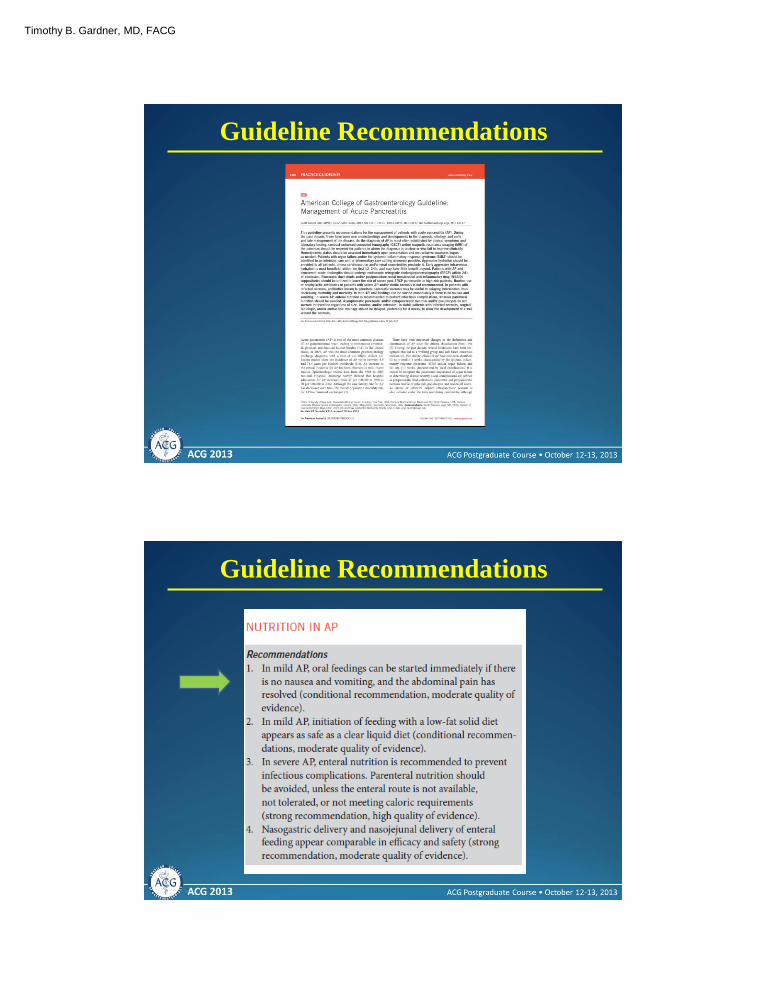
Guideline Recommendations
Guideline Recommendations
Timothy B. Gardner, MD, FACG
Guideline Recommendations
Guideline Recommendations
Timothy B. Gardner, MD, FACG
Guideline Recommendations
1. Fluid Resuscitation
Objectives
2. Antibiotic Therapy
3. Nutritional Support
4. Guideline Recommendations
Timothy B. Gardner, MD, FACG
Thank You