mtp 6: calcium disorders hypocalcemia and hypercalcemia · mtp 6: calcium disorders hypocalcemia...
TRANSCRIPT
MTP 6: Calcium Disorders Hypocalcemia and Hypercalcemia 15th Asia-Oceana Congress of Endocrinology
Radisson Blu Hotel Cebu City, Philippines
October 8-11, 2014
Bart L. Clarke, M.D. Chair, Metabolic Bone Disease Core Group
Division of Endocrinology, Diabetes, Metabolism, and Nutrition
Professor of Medicine Mayo Clinic College of Medicine
Rochester, Minnesota, USA

Faculty Disclosures 10/10/14
• Relevant Financial Relationships: None
• Off-Label Usage: None

Hypocalcemia Case #1
• 45-year-old premenopausal female referred for evaluation of newly discovered low bone density
• Previously healthy, and not had fractures • Does not take calcium or vitamin D supplementation • Moderately active, walking for exercise 30 minutes
each day, five days each week • Takes L-thyroxine 100 mcg once each day for
autoimmune hypothyroidism • Drinks wine once each week at dinner • Does not smoke cigarettes • Caffeine intake three cups of coffee each day

Hypocalcemia Case #1
• Physical exam: – Height 173 cm, weight 72.5 kg, BMI 24.2 kg/m2
– Left arm BP 136/84 mm Hg while sitting, HR 72 bpm and regular
– Lungs, heart, abdomen, spine and lymph nodes normal • Laboratory studies:
– Serum calcium 7.8 mg/dL (N, 8.9-10.1) – Serum phosphorus 4.7 mg/dL (N, 2.5-4.5) – Serum total alkaline phosphatase 40 Units/L (N, 37-98) – Serum creatinine 0.9 mg/dL (N, 0.6-1.1) – Serum 25-hydroxyvitamin D 35 ng/mL (optimal, 30-80) – Serum PTH 8 pg/mL (N, 15-65) – 24-hr urine calcium 55 mg (N, 25-275)
Hypocalcemia Case #1
• Bone Mineral Density: – L2-L4 lumbar spine BMD 0.737 g/cm2 (Z-score -1.8) – Left femoral neck BMD 0.688 g/cm2 (Z-score -1.7) – Left total hip BMD 0.630 g/cm2 (Z-score -1.5) – Right femoral neck BMD 0.692 g/cm2 (Z-score -1.5) – Right total hip BMD 0.615 g/cm2 (Z-score -1.3)
Hypocalcemia Case #1
• What is the best treatment for her low serum calcium? – A. Calcium citrate 600 mg once daily – B. Calcium citrate 600 mg three times daily – C. Vitamin D 400 IU once daily – D. Calcitriol 0.25 mcg once a week – E. Forteo 20 mcg once daily

Hypocalcemia Case #1
• What is the best treatment for her low serum calcium? – A. Calcium citrate 600 mg once daily – B. Calcium citrate 600 mg three times daily – C. Vitamin D 400 IU once daily – D. Calcitriol 0.25 mcg once a week – E. Forteo 20 mcg once daily
Hypocalcemia Case #1
• Discussion: – Patient has premenopausal low bone density without fxs – Laboratory studies diagnostic of hypoparathyroidism – Serum calcium is mildly decreased and serum
phosphorus mildly increased, but patient remains asymptomatic
– 24-hr urine calcium is low-normal mainly due to low serum calcium
– Further investigation showed no evidence of hypomagnesemia, and no other causes of hypoparathyroidism
– Given that patient has never had neck surgery, she was diagnosed with presumed autoimmune hypoparathyroidism

Hypocalcemia Case #1
• Discussion: – Patient requires calcium supplementation to keep serum
calcium above 8.0 mg/dL – Patients with hypoparathyroidism usually require divided
doses of calcium supplementation to maintain serum calcium above 8.0 mg/dL
– Vitamin D 400 IU each day is reasonable, but not sufficient by itself to treat hypoparathyroidism
– Calcitriol 0.25 mcg once each week will not be sufficient in most cases of hypoparathyroidism
– Forteo is not FDA-approved for treatment of hypoparathyroidism, but sometimes used off-label
– PTH 1-84 may soon be approved for treatment of hypoparathyroidism
Hypocalcemia Case #2
• 68-year-old postmenopausal female referred for evaluation of moderate osteopenia
• Previously healthy, but had a T6 vertebral fracture with fall • Previously took alendronate for one year, but stopped this
due to significant GI distress • Takes calcium 1200 mg and vitamin D 1000 IU each day • Walks for exercise 30 minutes each day, 5 days each week • Drinks wine once each week at dinner • Does not smoke cigarettes • Caffeine intake one cup of coffee each day

Hypocalcemia Case #2
• Physical exam: – Height 161 cm, weight 71.3 kg, BMI 27.5 kg/m2
– Left arm BP 122/74 mm Hg while sitting, HR 66 bpm and regular – Lungs, heart, abdomen, spine and lymph nodes normal
• Laboratory studies: – Serum calcium 8.5 mg/dL (N, 8.9-10.1) – Serum phosphorus 2.4 mg/dL (N, 2.5-4.5) – Serum total alkaline phosphatase 128 Units/L (N, 46-118) – Serum creatinine 0.7 mg/dL (N, 0.6-1.1) – Serum 25-hydroxyvitamin D 38 ng/mL (optimal, 30-80) – Serum PTH 150 pg/mL (N, 15-65) – 24-hr urine calcium 78 mg (N, 25-275) – IgA tissue transglutaminase antibody 100 Units/L (N, <4.0)

Hypocalcemia Case #2
• Bone Mineral Density: – L2-L4 lumbar spine BMD 0.903 g/cm2 (T-score -2.4) – Left femoral neck BMD 0.792 g/cm2 (T-score -1.8) – Left total hip BMD 0.826 g/cm2 (T-score -1.5) – Right femoral neck BMD 0.814 g/cm2 (T-score -1.6) – Right total hip BMD 0.839 g/cm2 (T-score -1.3)
Hypocalcemia Case #2
• What is the best treatment for her low serum calcium? – A. Calcium carbonate 500 mg once daily – B. Vitamin D 600 IU each day – C. Gluten-free diet – D. Intravenous calcium gluconate – E. Magnesium oxide 400 mg twice daily

Hypocalcemia Case #2
• What is the best treatment for her low serum calcium? – A. Calcium carbonate 500 mg once daily – B. Vitamin D 600 IU each day – C. Gluten-free diet – D. Intravenous calcium gluconate – E. Magnesium oxide 400 mg twice daily

Hypocalcemia Case #2
• Discussion: – Patient has postmenopausal osteopenia with T6 fx – Findings are consistent with malabsorption of calcium
and phosphorus – Diagnosis of celiac disease suggested by increased
tissue transglutaminase antibody, confirmed by upper GI endoscopy showing flattening of villi in duodenum
– Gluten-free diet will lead to resolution of inflammation and malabsorption
– Patient will continue calcium and vitamin D supplementation

Hypocalcemia Case #2
• Discussion: – Patient has postmenopausal osteopenia with T6 fx – Findings are consistent with malabsorption of calcium
and phosphorus – Diagnosis of celiac disease suggested by increased
tissue transglutaminase antibody, confirmed by upper GI endoscopy showing flattening of villi in duodenum
– Gluten-free diet will lead to resolution of inflammation and malabsorption
– Patient advised to continue calcium and vitamin D supplementation

Hypocalcemia Case #3
• 58-year-old postmenopausal female referred for evaluation of secondary hyperparathyroidism for several years
• Previously had jejuno-ileal bypass for medically complicated obesity 32 years ago, with postoperative weight loss of 40% of her excess weight
• Current weight is about same as before previous weight loss surgery • No hypo- or hypercalcemia ever documented • No history of fractures • Iron, calcium, vitamin D, vitamin B12, and thiamine deficiencies
replaced with appropriate supplements for at least three years • No previous treatment with hormone therapy or antiresorptive agents • Takes calcium 1200 mg and vitamin D 800 IU each day • Not exercising currently • No alcohol, cigarettes, or caffeine
Hypocalcemia Case #3
• Physical exam: – Height 163 cm, weight 94.0 kg, BMI 35.6 kg/m2
– Left arm BP 140/78 mm Hg while sitting, HR 88 bpm and regular – Lungs, heart, spine, and lymph nodes normal – Abdomen is obese without purplish striae
• Laboratory studies: – Serum calcium 8.9 mg/dL (N, 8.9-10.1) – Serum phosphorus 3.6 mg/dL (N, 2.5-4.5) – Serum total alkaline phosphatase 79 Units/L (N, 46-118) – Serum creatinine 0.9 mg/dL (N, 0.6-1.1) – Serum 25-hydroxyvitamin D 35 ng/mL (optimal, 30-80) – Serum PTH 73 pg/mL (N, 15-65) – 24-hr urine calcium not measured
Hypocalcemia Case #3
• Bone Mineral Density: – L1-L2 lumbar spine BMD 1.018 g/cm2 (T-score -1.3) – Left femoral neck BMD 0.857 g/cm2 (T-score -1.4) – Left total hip BMD 0.897 g/cm2 (T-score -0.9) – Right femoral neck BMD 0.807 g/cm2 (T-score -1.7) – Right total hip BMD 0.887 g/cm2 (T-score -1.0)
Hypocalcemia Case #3
• What is the best treatment for her hyperparathyroidism? – A. Increase her calcium and vitamin D supplementation – B. Reverse her jejuno-ileal bypass – C. Perform Roux-en-Y bypass – D. Refer her for subtotal parathyroidectomy – E. B and C
Hypocalcemia Case #3
• What is the best treatment for her hyperparathyroidism? – A. Increase her calcium and vitamin D supplementation – B. Reverse her jejuno-ileal bypass – C. Consider Roux-en-Y bypass – D. Increase her vitamin B12 and iron supplementation – E. B and C

Hypocalcemia Case #3
• Discussion: – Patient has hyperparathyroidism without fractures due to decreased
absorption of calcium and vitamin D – Hyperparathyroidism was originally physiological, but may have
become autonomous over many years of chronic parathyroid gland stimulation
– No evidence of hypercalcemia or other complications to justify parathyroidectomy
– Reversal of jejuno-ileal bypass and performance of Roux-en-Y bypass should address her medically complicated obesity and allow for better calcium and vitamin D absorption
– Continue calcium and vitamin D supplementation to optimize replacement, modifying dose as needed to control hyperparathyroidism
– Consider parathyroidectomy only if hypercalcemia develops over time

Hypercalcemia Case #1
• 21-year-old premenopausal female referred for evaluation of persistent primary hyperparathyroidism after two previous parathyroidectomies
• Initial diagnosis of hypercalcemia and primary hyperparathyroidism one year ago, with serum calcium 10.9 mg/dL (N, 8.9-10.1)
• No evidence of kidney stones, osteoporosis, or fractures • Fatigue was major symptom • First parathyroidectomy removed right inferior and left superior glands,
but hypercalcemia persisted • Second parathyroidectomy removed left inferior parathyroid gland, but
hypercalcemia persisted • Takes dietary calcium intake of 500 mg each day, and no vitamin D
supplement • Exercising intermittently • Denies alcohol, cigarettes, or caffeine

Hypercalcemia Case #1
• Physical exam: – Height 164 cm, weight 68.4 kg, BMI 25.4 kg/m2
– Left arm BP 117/72 mm Hg while sitting, HR 74 bpm and regular – Lungs, heart, abdomen, spine, and lymph nodes normal
• Laboratory studies: – Serum calcium 11.3 mg/dL (N, 8.9-10.1) – Serum phosphorus 2.6 mg/dL (N, 2.5-4.5) – Serum total alkaline phosphatase 49 Units/L (N, 52-144) – Serum creatinine 0.5 mg/dL (N, 0.6-1.1) – Serum 25-hydroxyvitamin D 30 ng/mL (optimal, 30-80) – Serum PTH 71 pg/mL (N, 15-65) – 24-hr urine calcium 453 mg (N, 25-275)

Hypercalcemia Case #1
• What is the best localization study for her persistent primary hyperparathyroidism? – A. Parathyroid scan – B. Neck ultrasound – C. Venous sampling for parathyroid hormone – D. MRI neck/chest – E. 4D-CT scan

Hypercalcemia Case #1
• What is the best localization study for her persistent primary hyperparathyroidism? – A. Parathyroid scan – B. Neck ultrasound – C. Venous sampling for parathyroid hormone – D. MRI neck/chest – E. 4D-CT scan
Hypercalcemia Case #1
Hypercalcemia Case #1
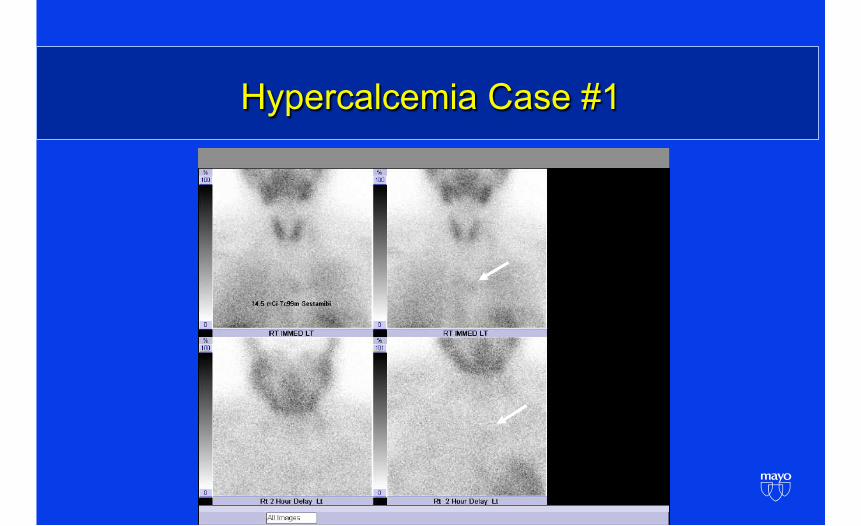
• Discussion: – Patient has persistent primary hyperparathyroidism with mild hypercalciuria
and symptoms, but without kidney stones, osteoporosis, or fractures – Previous imaging prior to surgeries not helpful – Parathyroid scan showed faint mediastinal uptake only, with no uptake
elsewhere – MRI chest confirmed apparent parathyroid adenoma in her aortopulmonary
window – Patient underwent median sternotomy with parathyroidectomy – Portion of parathyroid adenoma autotransplanted in left chest wall – Postoperative serum calcium 8.5 mg/dL (N, 8.9 to 10.1), with PTH 6.8 pg/
mL (N, 15-65) – Dismissed from hospital on calcium 2000 mg and calcitriol 0.5 mcg each
day
Hypercalcemia Case #2 • 37-year-old premenopausal female referred for evaluation of persistent
primary hyperparathyroidism after six previous parathyroidectomies • Initial diagnosis of hypercalcemia 14 years earlier, with primary
hyperparathyroidism diagnosed at that time, with serum calcium unknown, but as high as 16.3 mg/dL since then
• She passed a single kidney stone once only, no evidence of recurrence • No evidence of renal dysfunction, osteoporosis, or fractures • Fatigue is her major symptom • Her parathyroidectomies removed multiple inferior and superior glands,
but hypercalcemia has always persisted • Takes dietary calcium intake of 500 mg each day, with no vitamin D
supplement, with cinacalcet 60 mg twice daily • Exercising intermittently • Denies alcohol, cigarettes, or caffeine

Hypercalcemia Case #2 • Physical exam:
– Height 165 cm, weight 91.4 kg, BMI 33.7 kg/m2
– Left arm BP 126/86 mm Hg while sitting, HR 94 bpm and regular – Lungs, heart, abdomen, spine, and lymph nodes normal – No palpable parathyroid tissue, well-healed neck scar
• Laboratory studies: – Serum calcium 12.0 mg/dL (N, 8.9-10.1) – Serum phosphorus 1.9 mg/dL (N, 2.5-4.5) – Serum total alkaline phosphatase 170 Units/L (N, 37-98) – Serum creatinine 0.9 mg/dL (N, 0.6-1.1) – Serum 25-hydroxyvitamin D 18 ng/mL (optimal, 30-80) – Serum PTH 587 pg/mL (N, 15-65) – 24-hr urine calcium 378 mg (N, 25-275)
Hypercalcemia Case #2 • What is the best imaging study for her persistent primary
hyperparathyroidism? – A. Parathyroid scan – B. Neck ultrasound – C. Venous sampling for parathyroid hormone – D. MRI neck/chest – E. 4D-CT scan
Hypercalcemia Case #2 • What is the best imaging study for her persistent primary
hyperparathyroidism? – A. Parathyroid scan – B. Neck ultrasound – C. Venous sampling for parathyroid hormone – D. MRI neck/chest – E. 4D-CT scan

Hypercalcemia Case #2

Hypercalcemia Case #2 • Discussion:
– Patient has persistent primary hyperparathyroidism with mild hypercalciuria, and previous kidney stone and fatigue due to parathyromatosis
– Previous imaging prior to six surgeries not very helpful – Parathyroid scan shows multiple areas of discordant uptake in her neck,
with no uptake in her chest – Outside CT chest and neck confirmed parathyroid tissue in her neck only – Patient underwent seventh neck re-exploration with removal of 2.7 grams
of parathyroid tissue, with evident tissue left behind – Postoperative serum calcium 10.5 mg/dL (N, 8.9 to 10.1), with PTH 667 pg/
mL (N, 15-65) – Dismissed from hospital on no calcium or vitamin D supplement, with
cinacalcet dose continued, and chemotherapy planned at home