monitoring(ibd(paents:(drug( levels,(an.body(tests(and(fecal( … · 2016-05-26 · result:...
TRANSCRIPT

Monitoring IBD Pa.ents: Drug Levels, An.body Tests and Fecal
Calprotec.n CDDW 2014
Drs J. Jones and B. Bressler February 2014

Disclosures
• Dr Jones – Consul.ng, educa.onal support and speaker bureau for Takeda, Janssen Inc., Abbvie, SHIRE
• Dr Bressler – Consul.ng, educa.onal support and speaker bureau for Takeda, Janssen Inc., Abbvie, SHIRE, Ferring, Aptalis, Warner ChilcoN

2014 CDDW/CASL Winter Mee3ng
ü Medical Expert (as Medical Experts, physicians integrate all of the CanMEDS Roles, applying medical knowledge, clinical skills, and professional attitudes in their provision of patient-centered care. Medical Expert is the central physician Role in the CanMEDS framework.)
Communicator (as Communicators, physicians effectively facilitate the doctor-patient relationship and the dynamic exchanges that occur before, during, and after the medical encounter.)
ü Collaborator (as Collaborators, physicians effectively work within a healthcare team to achieve optimal patient care.)
ü Manager (as Managers, physicians are integral participants in healthcare organizations, organizing sustainable practices, making decisions about allocating resources, and contributing to the effectiveness of the healthcare system.)
Health Advocate (as Health Advocates, physicians responsibly use their expertise and influence to advance the health and well-being of individual patients, communities, and populations.)
ü Scholar (as Scholars, physicians demonstrate a lifelong commitment to reflective learning, as well as the creation, dissemination, application and translation of medical knowledge.)
ü
Professional (as Professionals, physicians are committed to the health and well-being of individuals and society through ethical practice, profession-led regulation, and high personal standards of behaviour.)
CanMEDS Roles Covered:
Objec.ves • To understand in what clinical circumstances drug levels / an.-‐drug an.body levels should be ordered
• To understand in what clinical circumstances fecal calprotec.n (FC) should be ordered.
• To gain knowledge of the evidence for the use of drug levels / an.-‐drug an.body tes.ng and fecal calprotec.n in IBD
• To understand how to interpret and respond to the results of drug levels/ an. drug an.bodies and fecal calprotec.n in IBD

Case 1
– Ms. Jones is a 32 year old female with well characterized ileocolonic Crohn’s disease who you are seeing in your office with a disease flare.
– The pa.ent was diagnosed 5 years ago. Although ini.ally steroid dependent she entered a steroid free clinical remission 3 years ago on AZA 2 mg/kg body weight. No EIMIBD.
– She has been experiencing diarrheal symptoms with 10 to 12 BM per day in associa.on with lower abdominal cramping as well as 10 lb weight loss over the past 6 months
Case 1: Ques.on
1. What tests should be ordered now?

Fecal Calprotec.n Correlates More Closely With SES-‐CD Than CRP, Blood Leukocytes, and the CDAI
Scatterplot demonstrating the correlation of the Simple Endoscopic Score of Crohn’s Disease (SES-CD) with fecal calprotectin (Spearman’s rank correlation coefficient r=0.75, P<0.001).
Schoepfer AM, et al. Am J Gastroenterol. 2010;105:162-169.
MAJOR RESULTS
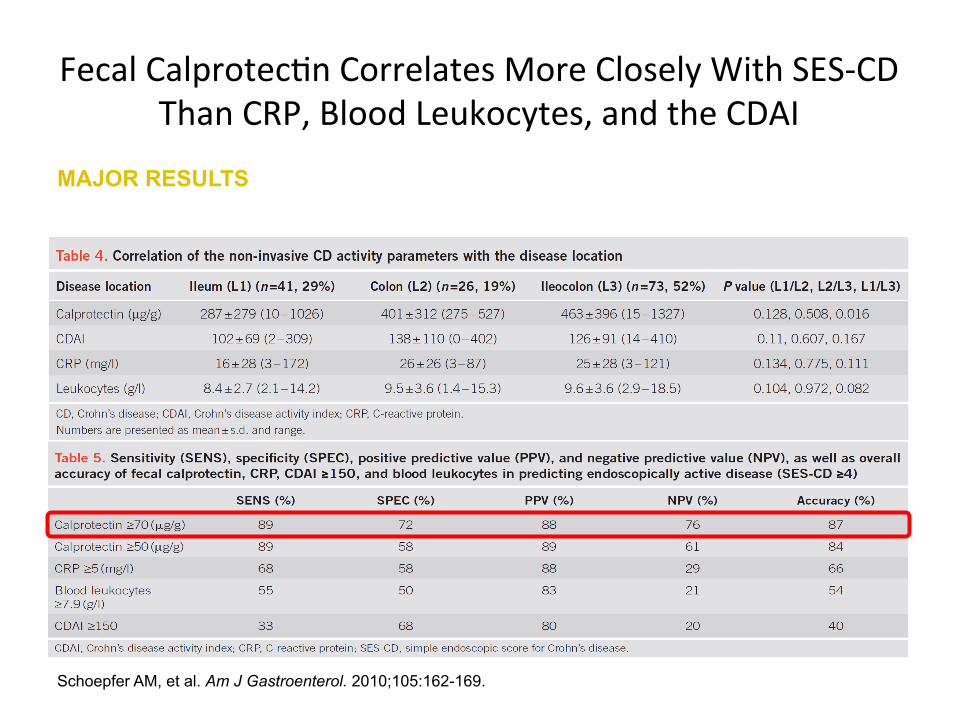
Fecal Calprotec.n Correlates More Closely With SES-‐CD Than CRP, Blood Leukocytes, and the CDAI
Schoepfer AM, et al. Am J Gastroenterol. 2010;105:162-169.
MAJOR RESULTS

Case 1 . . .
– laboratory inves.ga.ons reveal the following abnormali.es: Hb 96 (MCV 68); PLT 800; Alb 20; hsCRP 100; ferri.n 5; fecal Cp 500. Stool neg for enteric pathogens.
– Ileocolonoscopy (by yourself) demonstrates ac.ve inflamma.on characterized by the presence of large ulcera.ons (> 1cm) and patchy erythema throughout the ileum and en.re colon (rela.ve rectal sparing).

Colonoscopy
TI Colon

A Combina.on of Fecal Calprotec.n and hsCRP to Predict Mucosal Healing* A subanalysis of the STORI trial
78%
39%
82% 74%
53% 72%
Sensitivity
Specificity
hsCRP <5 mg/L Calpro ≤250 µg/g hsCRP <5 mg/L and Calpro ≤250 µg/g
Lémann M, et al. UEGW 2010, Barcelona, Spain, October 23-27:OP370.
* Defined as CDEIS ≤3

Schoepfer AM. Inflamm Bowel Dis 2009;15:1851-8
Correla.on of Faecal Calprotec.n With Endoscopic Ac.vity in UC
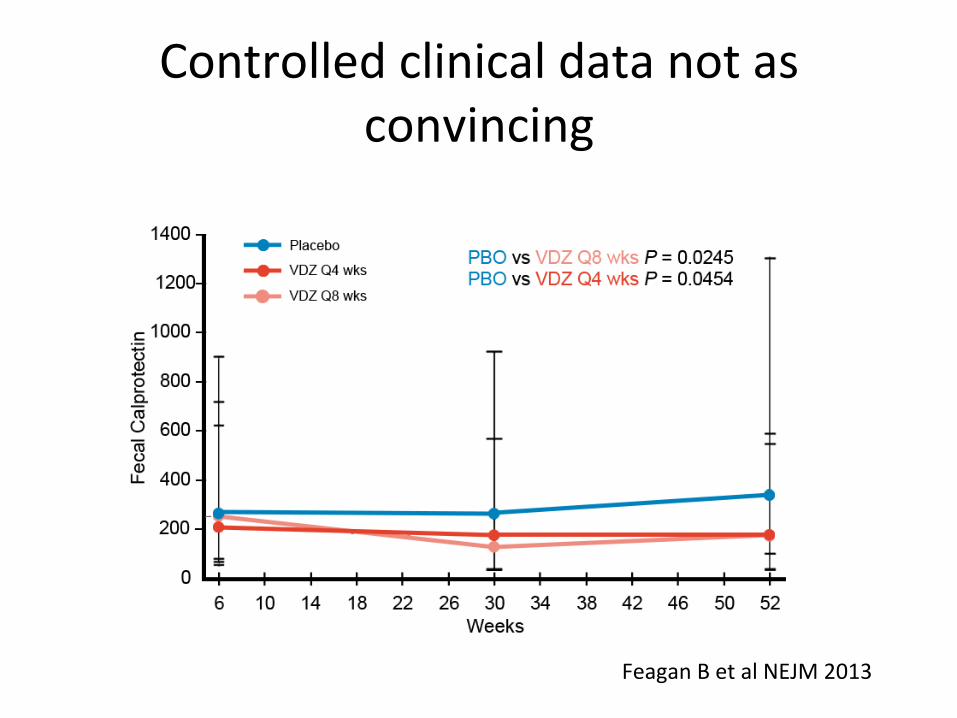
Controlled clinical data not as convincing
Feagan B et al NEJM 2013

Case 1 . . .
• You discuss remaining treatment op.ons with the pa.ent and she decides to start infliximab.
• You prescribe prednisone 40 mg po OD while she awaits provincial reimbursement. AZA is con.nued.
• One week later she starts infliximab induc.on dosing at weeks 0, 2 and 6.
• You see her back in your office 3 months aker ini.a.on of infliximab
Case 1: Follow-‐up Visit
• Ms. Jones tells you that she is feeling great! • She is having 1 to 2 formed BM per day & stools are formed & non bloody
• She has regained 5 lbs • Labs: Hb 110 (aker iron supplementa.on); PLT 200; Alb 28; hsCRP 15; Fe 26
• Fecal CP: 180

Case 1: Ques.ons
1. Are you sa.sfied with Ms. Jones’s clinical and biochemical response to infliximab therapy?
2. If not what lab values are of concern to you and how would you interpret them in the context of this case?
3. Are there any addi.onal tests that you would like to order?

Empiric vs. TDM
Loss of response (or inadequate response?)

81 %
19%
0.7
Shorten interval
Increase dose
Stop IFX
If shortening the interval, 72% shorten to q6w
A survey of 336 Canadian gastroenterologists asked: What do you do when patient loses response?
Jones J. et al. Can J Gastroenterol 2011;25(10):565-9.

Patients who re-established clinical response after crossover due to medication change: Patients Randomized as Responders (ACCENT I Trial: All Patients)
Janssen, Data on file
86 84 79
0
20
40
60
80
100
Single Dose 5 mg/kg 10 mg/kg
Frac
tion
of P
atie
nts
(%)

Op3mizing beEer than Switching within class

Consider Dose Op3misa3on with Current An3-‐TNF Prior to Switching:
ADA Dose: 160/80 160/80 80/40 40 mg EOW All patients IFX-naïve IFX-experienced
Remission at 4 weeks Maintenance of remission in Week-4 responders (CHARM)
Adapted from: Hanauer SB, et al. Gastroenterology 2006;130(2):323-33, Colombel JF, et al. Gastroenterology 2007;132(1):52-65, Sandborn WJ, et al. Ann Intern Med 2007;146(12):829-38.
21
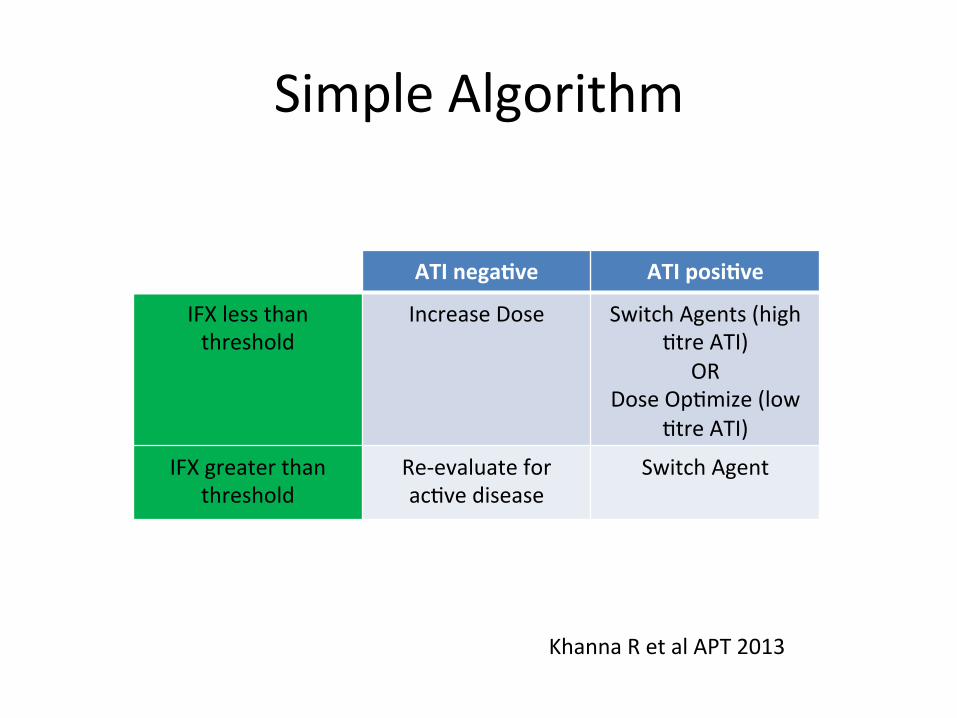
Simple Algorithm
ATI nega3ve ATI posi3ve
IFX less than threshold
Increase Dose Switch Agents (high .tre ATI)
OR Dose Op.mize (low
.tre ATI)
IFX greater than threshold
Re-‐evaluate for ac.ve disease
Switch Agent
Khanna R et al APT 2013

Result: Detectable ATI Result: Subtherapeutic IFX
Afif W, et al. Am J Gastroenterol 2010;105(5):1133-9.
p <0.004
Frac
tion
of P
ts
With
Res
pons
e (%
)
n = 12 n = 17 Increase
IFX Change Anti-TNF
n = 29 n = 6 Increase
IFX Change Anti-TNF
p <0.016
Frac
tion
of P
ts
With
Res
pons
e (%
)
Prometheus ELISA assay
• Single centre, retrospective study, n = 155 pts with TDM test • 177 tests assessed; subtherapeutic IFX defined as undetectable
trough or IFX<12 µg/ ml at 4 wks after infusion • Patients with subtherapeutic IFX had a significantly increased response
when dose optimized as compared to switching within class

Monitoring Infliximab Values and An.bodies: U.lity
DESIGN • Randomized, mul.center, controlled, 12-‐wk, single-‐blind study
OBJECTIVE • Assess u.lity of monitoring of drug and related Ab to op.mize IFX therapies
• CD pts, 2° failure IFX (N=69) • IFX dose intensifica.on 5 mg/kg q 4 wks (n=36) or tx based on serum [IFX] or IFX Ab values (n=33)
OUTCOMES • 70% pts w/2° failure: + [IFX] and undetectable Ab at .me of failure
• 20% pts: + IFX Ab, sub-‐therapeu.c [IFX] • 4% pts: undetectable IFX Ab, sub-‐therapeu.c [IFX]
• 6% pts: + [IFX], + IFX Ab
OUTCOMES
Steenholdt C, et al. Gut. 2013.
Treatment algorithm for patients with Crohn’s disease (CD) with secondary loss of response to infliximab (IFX). Ab=antibody; IV=intravenously; sc=subcutaneously; TNF=tumor necrosis factor

Monitoring Infliximab Values and An.bodies: U.lity
OUTCOMES
Steenholdt C, et al. Gut. 2013.

• 270 IBD pa.ents on IFX maintenance therapy. All pts had their IFX trough levels adjusted to 3-‐7 mg/ml.
• Pts randomized to 2 groups, then will be followed for 1 year: – group 1: IFX trough levels maintained at 3-‐7 μg/ml – group 2: dosing and op.miza.on based on clinical symptoms
Individualized IFX Treatment Using Therapeu.c Drug Monitoring: Baseline Data
Vande Casteele et al. ECCO 2012, Abstract OP11
> 7 μg/ml
3-‐ 7 μg/ml (43 %)
Undetectable
< 3 μg/ml
Serum IFX Trough Levels of Pa3ents in Remission (N = 270)
Dose decreased (26 %) Dose increased
(22 %)
Dose increased (9 %)
(77 % ATI-‐posi3ve)
TAXIT

Drug Level and Symptom Based Treatment Produce Similar Outcomes in Pa.ents with IBD
• N = 251 stable IBD pts (178 CD, 85 UC) on IFX therapy had their TL adjusted to 3-‐7 μg/ml and were randomized to 2 groups:
• Clinically** or TL based: IFX TL maintained at 3-‐7 μg/ml • CD/UC dura3on of dis. ~15/11 y & IFX treatment ~6/4 y, con-‐IS ~5% • Treatment guided by TL resulted in less rescue therapy; rates of clinical & biological remission were similar for both groups
Vande Casteele et al. UEGW 2013, Abstract OP001
TAXIT
Primary Endpoint: Remission* at 1 Year
69 72
0 20 40 60 80
100
Clinically based
Level based
*Clinical (HBI ≤ 4 or pMayo ≤ 2) and biologic (CRP < 5 mg/l) remission **Clinically based: dosing & op3miza3on based on symptoms
Frac3o
n of Pa3
ents (%
)
P = NS Characteris3cs CB
n = 110
LB n = 113
P-‐value
IFX TL 3-‐7 µg/ml 56% 78% <0.001
ATI +ve 2.7% 0% 0.1
Required rescue therapy† 17.3% 5.5% <0.01
Secondary Endpoints: Aper Maintenance Phase (1 Year)
†Use of steroids or TNF-‐op3miza3on/switch
n = 110 n = 113

Case 1 . . .
• You order a trough serum infliximab drug and an.body level and it reveals infliximab concentra.on of 2 μg/ml
• The ADA level is undetectable

Case 1: Ques.on
• What is your interpreta.on of these results?
• How would you respond to these results?
• How many of you have access to drug level and ADA tes.ng?
• How many have access to FC tes.ng?

Case 1 . . .
• You and Ms. Jones decide jointly to increase the infliximab dose to 10 mg / kg body weight with plans to repeat a colonoscopy within 3 -‐ 6 months if the FC does not normalize
• Ms. Jones con.nues to do well clinically and aker another 3 months you recheck her inflammatory markers – hsCRP 5 – FC 30 – All other laboratory parameters normal

Normaliza.on of Fecal Calprotec.n Aker Induc.on Predicts Clinical Outcomes in Pa.ents with IBD
Molander et al. UEGW 2011, poster P0397
• N=72 (39 CD, 33 UC) pts treated with IFX (n=49) or ADA (n=23) induction and maintenance therapy. Clinical remission defined by partial Mayo or HBI
• Cut-off concentration of 139 µg/g for FC had 71% sensitivity and 82% specificity to predict risk of active disease within 1 year
81
31
0
25
50
75
100
Normal calprotec3n aper induc3on
Elevated calprotec3n aper induc3on
p<0.001
Percen
t pa3
ents (%
)
11/35 30/37
Pa3ents in Clinical Remission at 12 Months
median 41 μg/g (0-‐97)
median 424 μg/g (114-‐5859)

Case 1 . . .
• You con.nue to follow her every 6 months • One year later you see her in clinic and she has developed .nea versicolor. She has also started to experience alopecia.
• However, clinically she con.nues to do excep.onally well
• Her laboratory parameters remain normal save for mild lymphopenia.
Case 1: Ques.ons
1. Do you have any concerns about Ms. Jones’s presenta.on a this .me?
2. How would you advise Ms. Jones at this .me?
3. Are there any other inves.ga.ons you might order at this .me?

Case 1 . . .
• You have concerns about cell mediated immunity and opt to repeat the serum infliximab drug level again
• The trough serum infliximab concentra.on is 15 μg/ml

Case 1 . . .
• You decrease the pa.ent’s infliximab dose to 7.5 mg/kg of body weight and con.nue to follow Ms. Jones q 12 months
• She does well long term

Case 2
• Mr. Smith is a 25 year-‐old male who you have been following for ileal CD for 4 years.
• He exhibited steroid refractory disease early in his disease course and has been on maintenance therapy with combo azathioprine 175 mg daily (51 kg) and infliximab 5 mg/kg q 8 week intervals for 2 years
Case 2 . . .
• While undergoing an orthopedic procedure 8 months ago he had a 16 week hiatus between infliximab infusions
• You are seeing him in clinic in follow-‐up and he presents with worsening symptoms of RLQ abdominal pain, increased stool frequency (5-‐6 loose non-‐bloody stools per day) and post-‐prandial bloa.ng
Case 2 . . .
• You elect to reevaluate the pa.ent’s disease ac.vity, extent and severity – Lab: Hb 110 (microcy.c); Fe 12; WBC 12; PLT 400; hsCRP 5; Alb 22; FC 350
– CTE: long segment inflammatory CD (25cm) with bowel wall thickening, enhancement and comb sign
– Ileocolonoscopy: Inflammatory stricture at the ICV with ulcera.on, edema and friability

CT Enterography

Case 2: Ques.ons
• What would you do next?
a. Stop current therapy and switch to another an.-‐TNF?
b. Empirically increase the infliximab dose? c. Increase the azathioprine? d. Check the pa.ent’s infliximab drug and an.body
levels?

Calprotec.n as a possible predictor of symptoma.c relapse
De Surray N. ECCO 2012: P274
STORI: calprotec3n data months before relapse
0
800
–14
600
400
200
–12 –10 –8 –6 –4 –2 0 Time before relapse (months)
Calpro (m
icrog/g)
p=0.0004
Relapsers
Non-‐relapsers
STORI enrolled 115 Crohn's disease pa3ents who were treated with infliximab plus an immunomodulator for at least 1 year, and who were in stable remission for at least 6 months. Infliximab was discon3nued, and 39% of pa3ents relapsed within 1 year.

Case 2 . . .
• You elect to recheck the infliximab trough and ADA levels
Ø Serum infliximab trough level: 1 μg/ml
Ø ADA level was detectable at 10 Au/ml

Case 2: Ques.ons
1. How do you interpret these results in light of this case?
2. How would you respond to these lab results?

Summary • Measurement of infliximab trough levels and ADA levels is clinically useful – Primary non-‐responder or par.al responder – Maintenance therapy – Infec.ous and immune mediated complica.ons
• Unclear as to long term outcomes from TDM based interven.ons
• FC is a useful adjunct in the management of IBD – Within individual comparisons to baseline concentra.ons to guage response to therapy and predict disease relapse
• Its accuracy and reliability as a surrogate if intes.nal inflamma.on is s.ll under study
