monitoring communicative contact contact and connection glasgow 2014 17/10/2015
TRANSCRIPT

Monitoring Communicative Contact
Contact and ConnectionGlasgow 2014
20/04/23

Mathias Dekeyser
Garry ProutyRobert ElliottMia Leijssen
University of LeuvenPsychosociaal Centrum Leuven
20/04/23

Monitoring Communicative Contact
1. What is contact and why monitor it?
2. What measures of contact are there?
3. What can we use those measures for?
3

Monitoring Communicative Contact
1. What is contact and why monitor it?
• Rogers
• Prouty
• Dinacci
2. What measures of contact are there?
3. What can we use those measures for?
4

Rogers (1957): core condition of change
□ Psychological contact□ “a minimal relationship”□ “each makes some perceived difference in
the experiential field of the other”
□ Monitoring contact to check whether the core conditions are met.
5
Prouty (1994): psychological function
□ 3 psychological contact functions◊ Awareness
◊ External world: Reality Contact◊ Internal world: Affective Contact
◊ Expression◊ Communicative Contact
□ Monitoring contact to check ...□ when contact reflections are appropriate;□ if Pre-Therapy really works.
6

Dinacci (1997): communication
□ Observing psychological contact through:□ client reactivity = “communicative sign”□ meaningfulness, verbality, (non)verbal
coordination (= language pragmatics)□ touch
□ Monitoring contact to check if Pre-Therapy really works.
7

Monitoring Communicative Contact
1. What is contact and why monitor it?
2. What measures of contact are there?
• PTRS (Hinterkopf & Prouty-v1; Prouty-v2)
• ECPI (Dinacci; Brenner-additions)
• CCS (Dekeyser, Elliott, Leijssen)
3. What can we use those measures for?
8

Pre-Therapy Rating Scale (PTRS)
□ Counting markers in annotated transcripts to measure two dimensions:
□ Reality/Communication (verbal)□ Affective contact (verbal+nonverbal)
□ High inter-rater agreement is possible□ Increased scores reportedly associated
with carer’s observed change
9

Evaluation Criterion for Pre-Therapy Interview (ECPI)
◊ Detecting and scoring client reactivity in video recording, to measure
◊ Reactivity (moderate reliability)◊ Elements of [language pragmatics] (low to
moderate)◊ Touch, eye contact (low to high reliability)◊ General Index
◊ Language related subscales associated with measures of pragmatic performance (ALICC)
◊ Increased scores reportedly associated with carer’s observed change
10
Communicative Contact Scale (CCS)
◊ Self-report perceived communicative contact in the other, with two subscales
◊ Meaningfulness◊ Reactiveness
□ Developed with help of expert group, tested on parents, students, (therapists, clients)
□ Meaning of the (sub)scales may vary
□ Positively associated with evaluation of interaction (self-report), but not with affective color or clinical symptoms (high level functioning clients GAF/BSI scores)
11
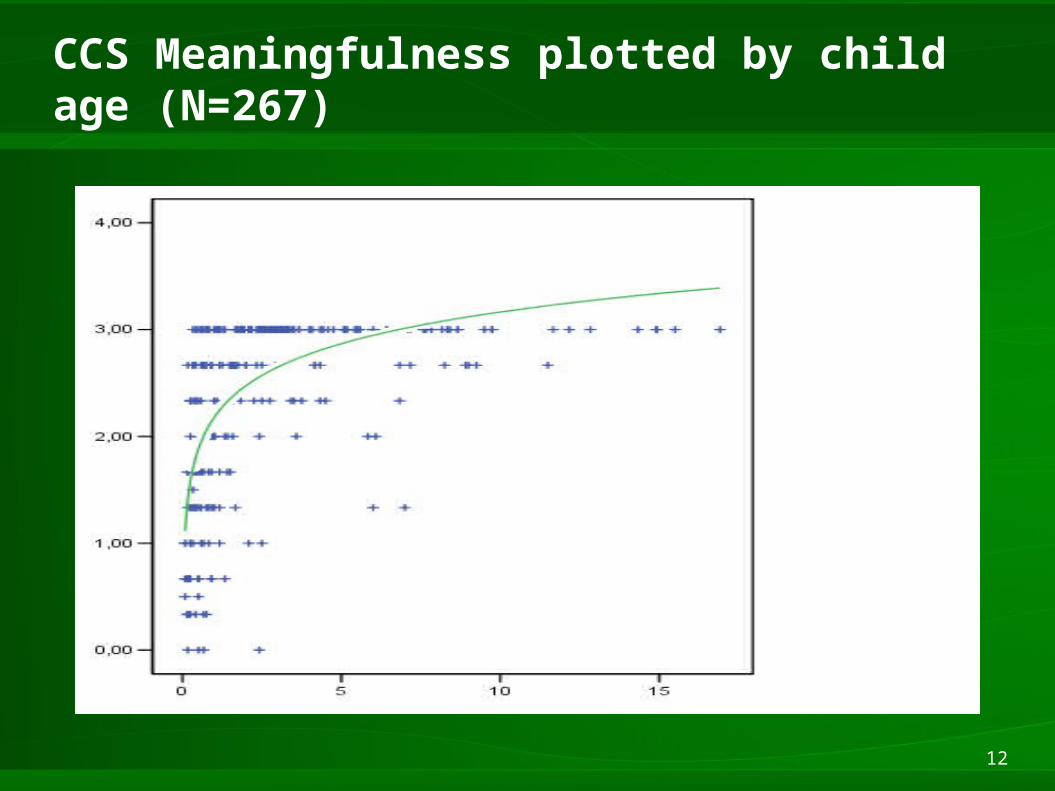
CCS Meaningfulness plotted by child age (N=267)
12

Communicative Contact Scale (CCS)
□ All scores predicted by□ Acquaintance with the observed□ Mindfulness of observer (acting with awareness)□ Child ability to involve the parent (-4y)□ Child pragmatic performance (4y+)□ Empathic attitude (association varies with role of observer)□ Working alliance of reporting therapist and observed client
□ Meaningfulness predicted by□ age of observed child – logarithmic curve□ mutual attunement of parent and child (-4y)
13

Monitoring Communicative Contact
1. What is contact and why monitor it?
2. What measures of contact are there?
3. What can we use those measures for?
• Research on the concept of contact
• Clinical research: outcome, process
• Practice and training
14

Research on the concept of contact
- Do people develop (implicit) mental models of communicative contact?
- Do we assess contact differently according to the situation?
- How is the development of contact skills related to the development of language, mentalisation, social skills?
- How do we naturally assess reality contact and affective contact in another person?

Clinical research: outcome
□Effect sizes are promising, but larger studies are needed.□After treatment, the PTRS-Reality/ ECPI test score was
likely to increase in 86% of the cases, and likely to be higher than 74% of similar patients.
□Development of PTRS/ECPI norm scores would be helpful.
□Can we think of less labor-intensive approaches? Other, indirect measures?□Nurses in contact work training have reported
symptom decrease in patients (Ondracek, 2004)□Where are clients’ qualitative reports? (Traynor, in
preparation)

Clinical research: process
□PTRS and ECPI offer great detail of within-session process
□Much more is possible than we do now.
□Can we build a collection of coded transcripts?
□CCS can be used to analyse the evolution of perceived contact across interactions/sessions
□Can CCS be used to discriminate between phases in a session?

PTRS: 1 session (schizoaffective, mental disability)(Prouty, 1994)
18
start middle end
0
20
40
60
80
100
120
RealityAffectSocial Communication

PTRS: 1 session (female, schizophrenia)(Van Werde, 1993; Van den Mooter, 2006)
19
start middle end
0
2
4
6
8
10
12
14
16
RealityAffectSocial Communication

CCS: 1 session (12 clients)
20
start rest of session
0,00
0,50
1,00
1,50
2,00
2,50
3,00
C4.GG
C6.JG
C8.EDS
C8.MVE
C9.BE
C9.IVH
C14.MK
C14.ALT
C14.MM
C10.PVDG
C9.LP
C8.TR

Practice and training
□ Can studying PTRS/ECPI coded transcripts be part of training?□ PTRS more closely related to theory (Prouty)
□ CCS scale can be used to:□ give a quick feel of the topic□ discuss cases and concepts□ support intervision/supervision?
21
