molar pregnancy
TRANSCRIPT

Molar pregnancy
Presented ByNirsuba Gurung
Masters in nursing Women health and development
Gestational Trophoblastic disease comprises a spectrum of interrelated conditions originating from the placenta.

Gestational trophoblastic disease is a prolifirative disorder of trophoblastic cells
It can be benign, premalignant or malignant
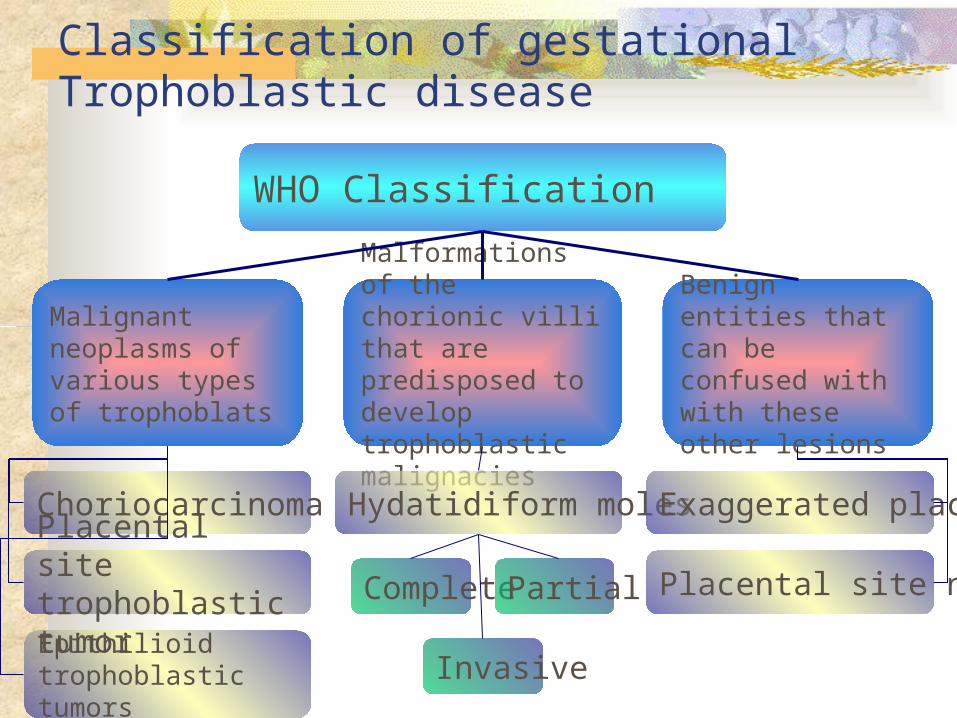
Classification of gestational Trophoblastic disease
WHO Classification
Malignant neoplasms of various types of trophoblats
Malformations of the chorionic villi that are predisposed to develop trophoblastic malignacies
Benign entities that can be confused with with these other lesions
Choriocarcinoma
Complete
Hydatidiform moles
Placental site nodule
Exaggerated placental site
Epithilioid trophoblastic tumors
Placental site trophoblastic tumor Partial
Invasive

Non-metastatic disease: confined to the uterus
Metastatic A- low risk-good prognosis B – high risk-poor prognosis
Low risk Disease present in less than 4 mooths
duration Initial serum hCG level < 40,000 IU/ml Metastasis limited to lung and vagina No prior chemotherapy No preceding term pregnancy

High risk Long duration of disease Initial serum hCG level > 40,000 IU/ml Brain or liver metastasis Failure of prior chemotherapy Following term pregnancy
Hydatidiform Mole Definition:
In latin"hydatid" means "drop of water”"mole" means "spot”
Pathologically,Hydatidiform moles represents placentas with
abnormally developed chorionic villi (enlarged, edematous and vesicular villi with variable amounts of proliferative trophoblast)
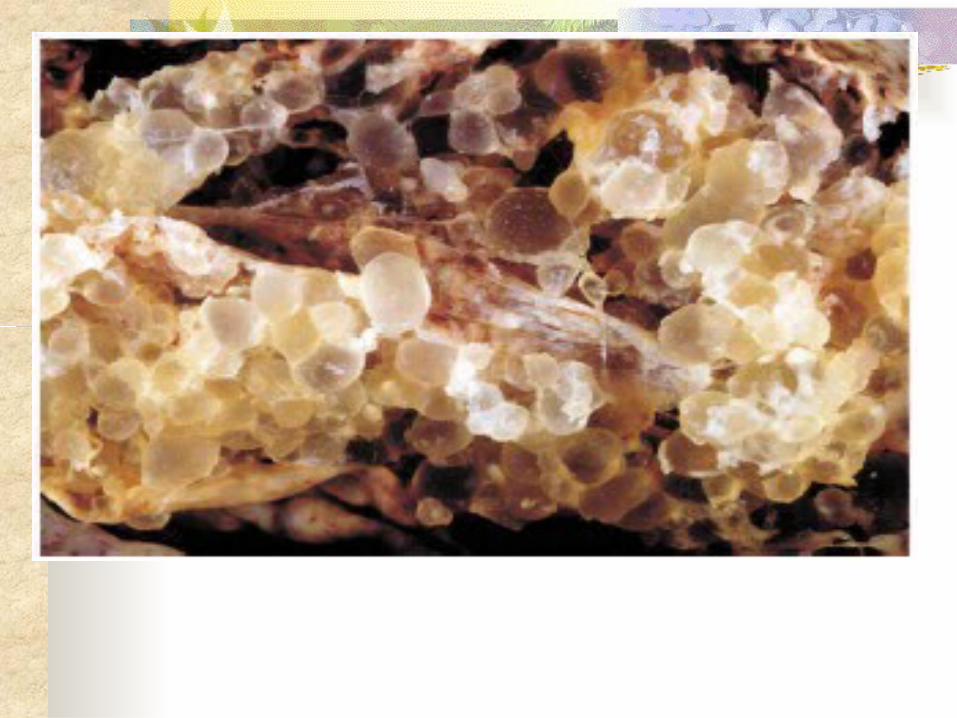
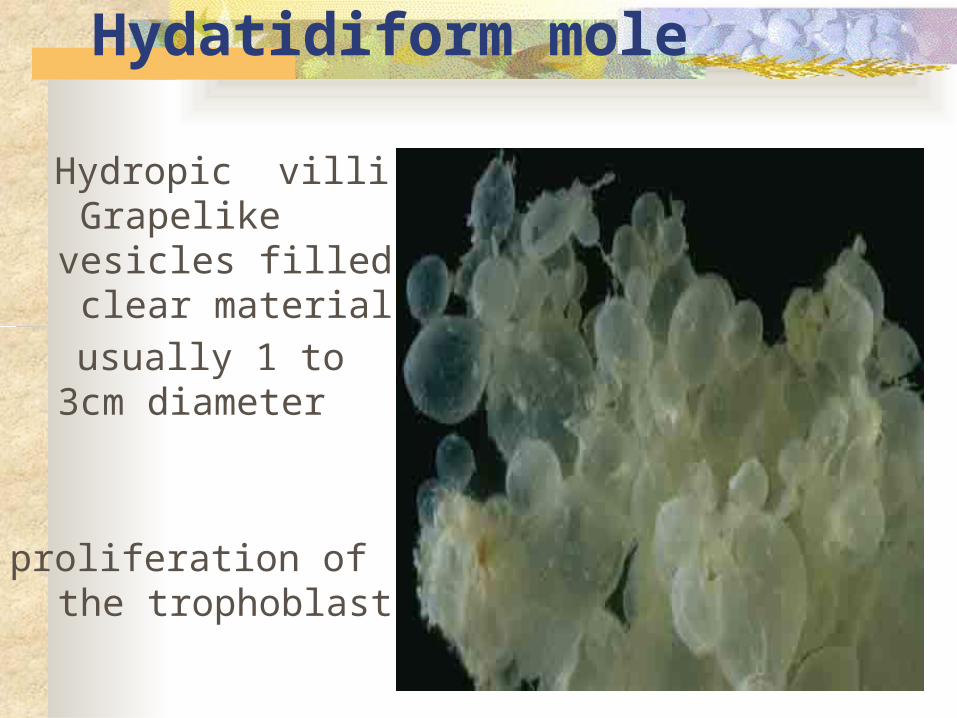
Macroscopic of Hydatidiform mole
Hydropic villi Grapelike vesicles filled clear material
usually 1 to 3cm diameter
proliferation of the
trophoblast
Hydatidiform mole(molar pregnancy)Molar pregnancy is an abnormal form of
pregnancy, wherein a non viable , fertilized egg implants in the uterus, and thereby converts pregnancy process into pathological ones.
It is characterized by presence of hyadatidiform moles.
It is an abnormal condition of the placenta where there are partly degenerative and partly proliferative changes in the young chorionic villi.
These results in the formation of clusters of small cysts of varying size
It is regarded as a begin neoplasia of the chorion with malignant potential
INCIDENCE There is considerable geographical
and environmental influences in incidence.
The incidence is higher in eastern than western countries. Its incidence in India is 1:160 and 1:2000 in UK.
Hydatidiform Mole Incidence:
In the United States, 1in 600 therapeutic abortions 1 in 1,500 pregnancies
Internationally: In Japan & China, 1-2 in 1,000 pregnancies In Indonesia & India, 12 in 1,000 pregnancies
In the United Arab of Emirates, 2 in 1000 deliveries (population-based study; Graham IH,
Fajardo AM; 1988) In Saudi Arabia;
1.48 in 1000 live births (hospital-based study; Felemban AA, et al; 1969)
In the United States, • 1in 600
therapeutic abortions
• 1 in 1,500 pregnancies
In Asian countries, • The rate is 10 times
higher than in Europe and North America
In Saudi Arabia;, • 1.48 in 1000 live births
(hospital-based study; Felemban AA, et al; 1969)
Contd……. It is prevalent among teenage and elderly
patient with high parity.

TYPES1. COMPLETE2. PARTIAL
Complete mole A complete mole is caused by a single
sperm combining with an egg which has lost its DNA.
The genotype is typically 46XX due to subsequent mitosis of fertilizing sperm but can also be 46XY.
Partial mole Partial mole occurs when an egg is
fertilized by 2 sperm or by ,sperm which reduplicates itself yielding the genotype of 69 XXY or 92XXXY

Hydatidiform mole Complete mole Partial mole Partial mole
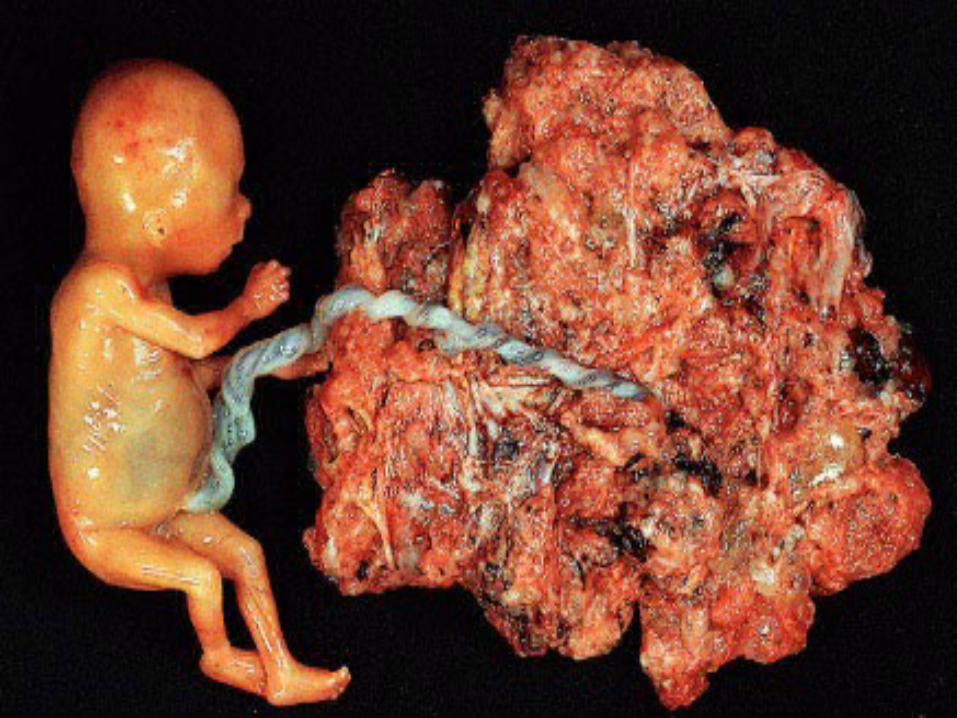
Partial mol ( fetal tissue)Grossly placenta a mixture of normal and hydropic villi
Fetus Severe growth restriction Multiple congenital anomalies
Risk Factors hydatidiform mole Strongest risk factors are Age and a history of prior hydatidiform
mole
Both extremes of reproductive age adolescents twofold risk Older than 40 tenfold risk
History of Prior mole High parity Disturbed maternal immune mechanism
suggested by: Rise in gammaglobulin level in absence of
hepatic disease Increased association with AB blood group
which possess no ABO antibody
An ethnic predisposition Diet (Deficiencies of protein or) (Vitamin A deficiency) Animal fat Smoking Increased paternal age

The risk of another mole Complete mole is 1.5 percent Partial mole is 2.7 percent
Two prior molar pregnancies the risk is 23 percent
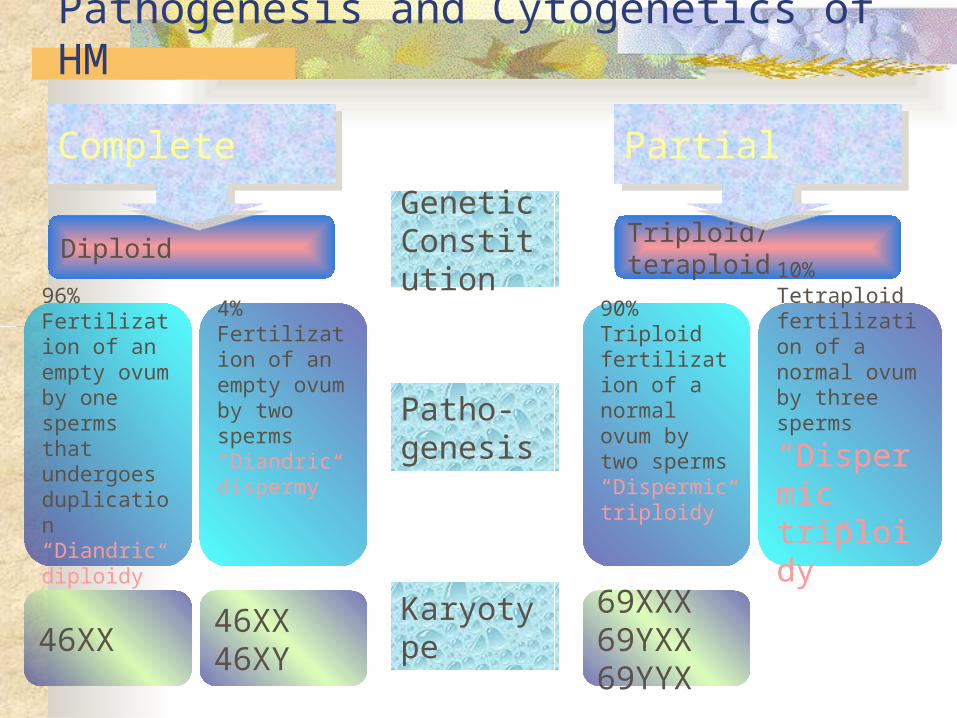
Pathogenesis and Cytogenetics of HM
Genetic Constitution
Diploid Triploid/ teraploid
Patho-genesis
4%Fertilization of an empty ovum by two sperms“Diandric dispermy”
90%Triploidfertilization of a normal ovum by two sperms“Dispermic triploidy”
96%Fertilization of an empty ovum by one sperms that undergoes duplication“Diandric diploidy”
10%Tetraploidfertilization of a normal ovum by three sperms“Dispermic triploidy”
Karyotype46XX
69XXX69YXX69YYX
46XX46XY
Complete Partial

Complete Mole, Pathogenesis
Duplication 46XX
Empty ovum
23X
Diandric diploidyAndrogenesis
Paternal chromosomes only
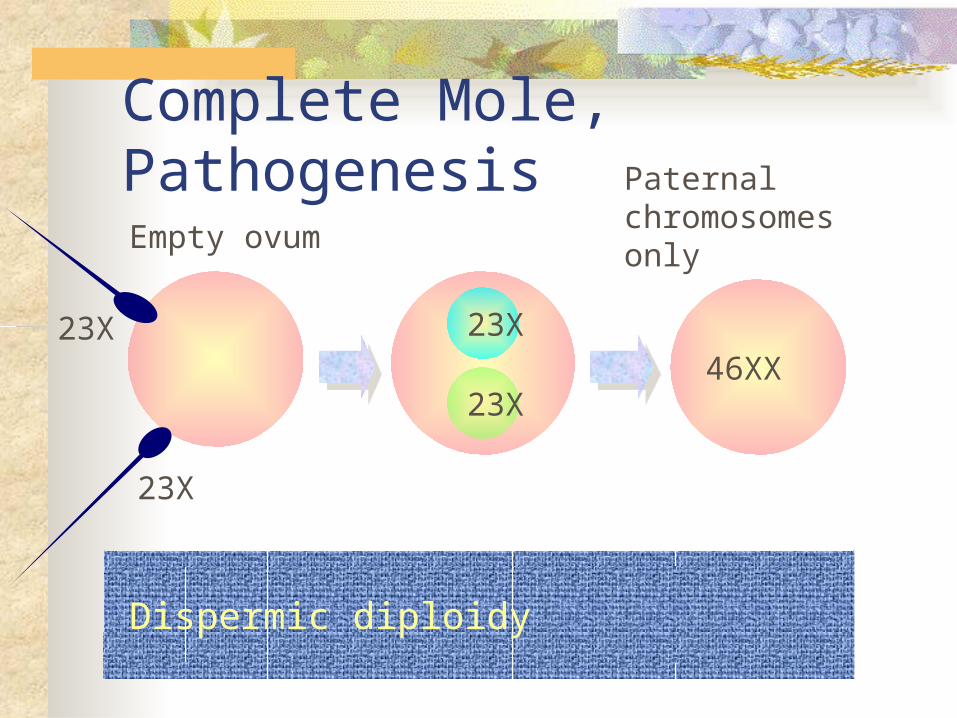
Complete Mole, Pathogenesis
46XX
Empty ovum
23X
Dispermic diploidy
Paternal chromosomes only
23X 23X
23X
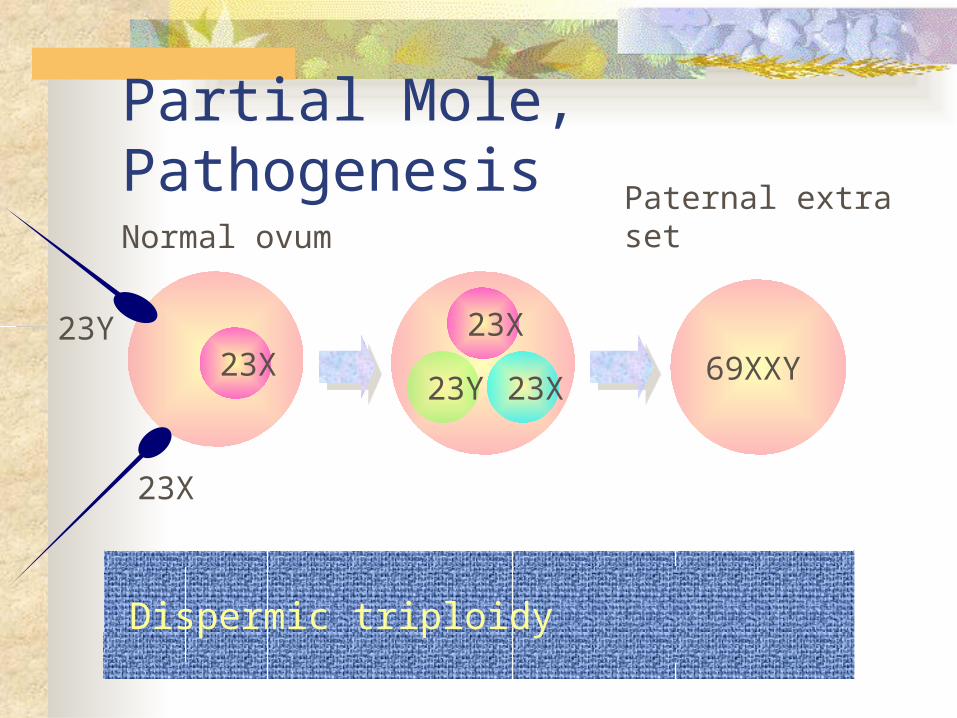
Partial Mole, Pathogenesis
69XXY
Normal ovum
23X
Dispermic triploidy
Paternal extra set
23Y 23X23Y 23X23X

Hydatidiform Mole
Alterations in gene expression profiles
Up-regulation and down-regulation of proteins committed to cell growth control
e.g. Up-regulation of growth factor and cytokine mediated pathways, and antiapoptosis genes
Trophoblastic hyperplasia
e.g. Down-regulation of insulin growth factor binding proteins and tumor necrosis factor receptor
Pathogenesis Principally a disease of the chorion Death of the ovum ir failure of the embryo
to grow is essential to develop complete H. mole
The secretion from the hyperplastic cells and transferred substances from the maternal blood accumulates in the stroma of the villi which are deviod of blood vessels
This results in distension of the villi to form small vesicles
The distension may also be due to edema and liquification of the stroma
Vesicle fluid is interstitial fluid and is almost similar to ascitic or edema fluid but rich in hCG

Naked eye appearance The mass filling the uterus is made of
multiple chains and clusters of cysts of varying sizes
No trace of embryo or the amniotic sac Hemorrhage, if occurs, takes place in the
decidual space
Microscopic appearance Marked prolifiration of syncitial and
cytotrophoblastic epithelium Marked thining of the sromal tissue due to
hydropoc degeneration Absence of blood vessels
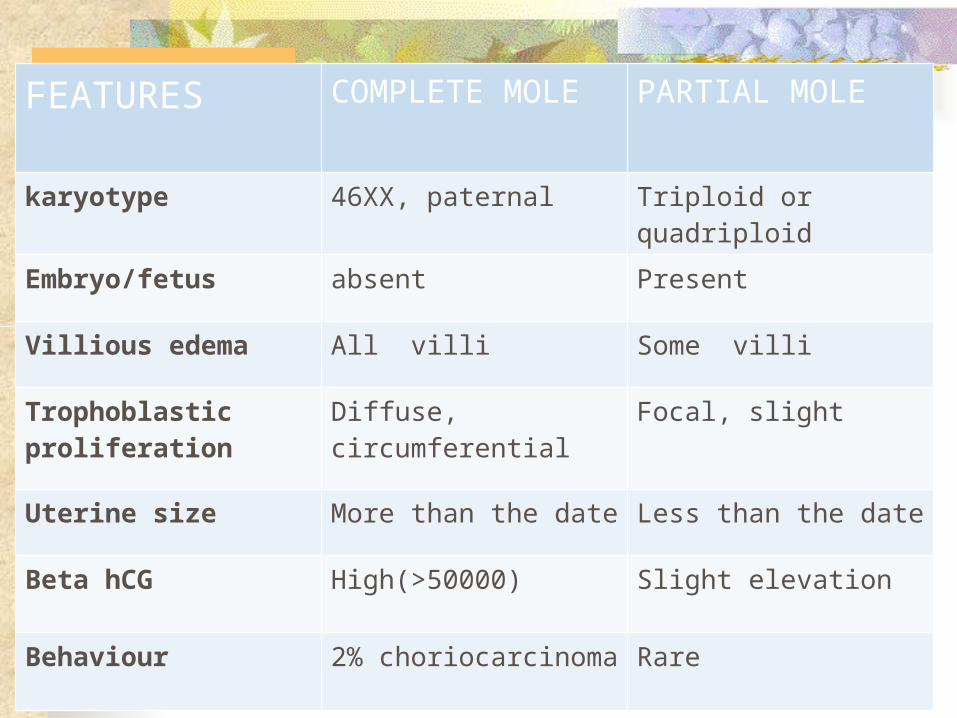
FEATURES COMPLETE MOLE PARTIAL MOLE
karyotype 46XX, paternal Triploid or quadriploid
Embryo/fetus absent Present
Villious edema All villi Some villi
Trophoblastic proliferation
Diffuse, circumferential Focal, slight
Uterine size More than the date Less than the date
Beta hCG High(>50000) Slight elevation
Behaviour 2% choriocarcinoma Rare
Clinical features Amenorrhea 8-12 weeks with following
manifestation Vaginal bleeding Varying degree of abdominal pain Constitutional symptoms
Patient become sick without any apparent reason Vomiting of pregnancy becomes excessive Breathlessness Thyrotoxic symptoms
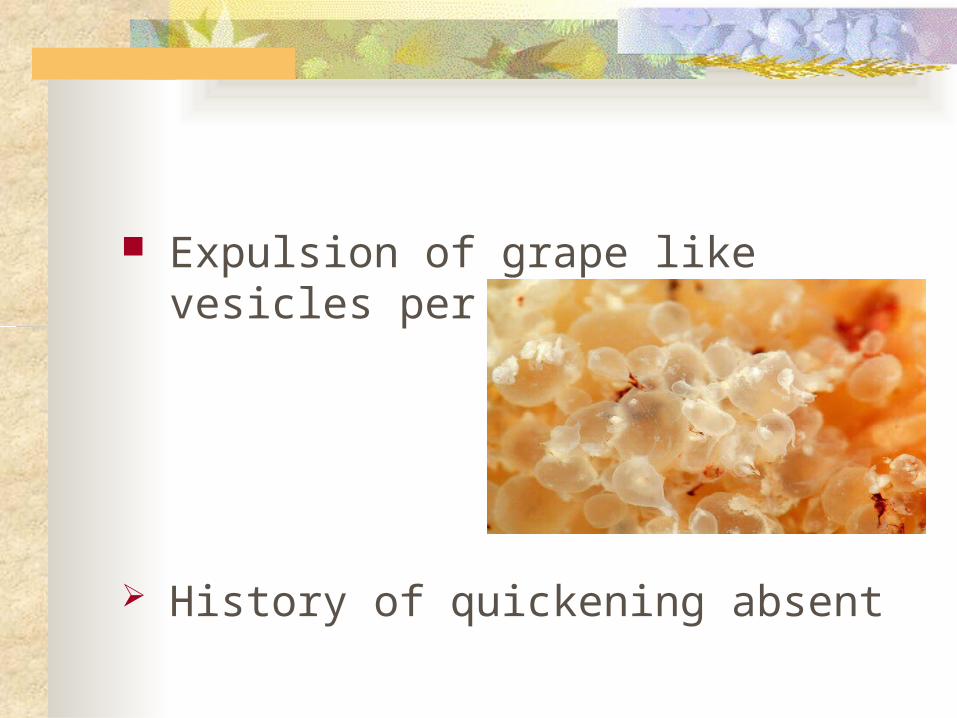
Expulsion of grape like vesicles per vaginum
History of quickening absent

Clinical Presentation:Complete mole:
Vaginal bleeding
Severe anemia
Passage of hydropic villi
Signs Features suggestive of early pregnancy Pallor Features of pre-eclampsia Per abdomen
Uterus –more than gestational period (70%) Uterus feels firm elastic(doughy ) Fetal parts not palpable Absence of fetal movement and FHS

Vaginal examination Internal ballotement cannot be elicited Unilaternal or bilaternal enlargement of
ovary (25-50%) Finding of vesicles in the vaginal discharge Open cervical os
Classical symptom of a complete mole Abnormal vaginal bleeding Lower abdominal pain Hyperemesis gravidarum Features of early onset of pre-eclampsia Uterus > dates No fetal parts and FHS
Classical symptoms contd….
Expulsion of vesicular tissues Theca lutein cyst of ovaries Hyperthyriodism Serum hCG >1,00,000 IU/ml USG –snow strom appearance

Hydatidiform Mole Diagnosis:
History Clinical examination Ultrasound examination Serum hCG levels Histopathological examination Cytogenetic and molecular biological
examination
Hydatidiform Mole Diagnosis:
Ultrasonography:* The diagnosis of molar pregnancy is nearly always
made by ultrasonography
Complete mole• The classical finding is a
“snow storm" pattern• Theca lutein cysts are frequent
findings on ultrasound
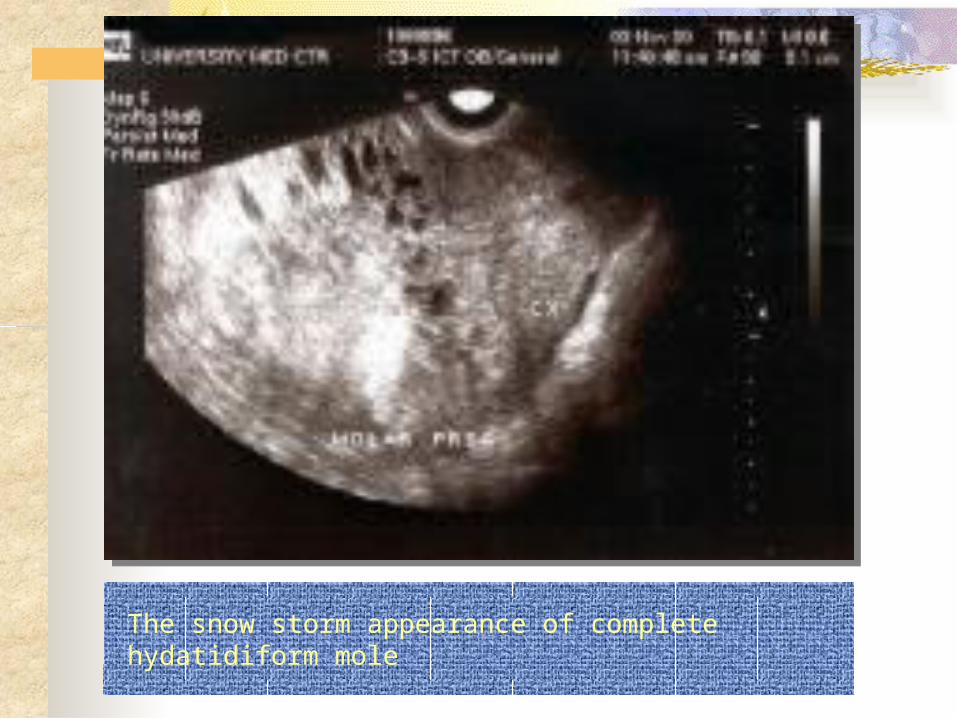
The snow storm appearance of complete hydatidiform mole
Theca lutein cysts, a frequent finding on ultrasound

Hydatidiform Mole Diagnosis:
Ultrasonography:
Partial mole
Abnormal gestational sac The classic vesicular
sonographic findings of a complete mole are usually not seen
Focal sonographic cystic changes and/or hydropic changes in the placenta are significantly associated with the diagnosis of a partial molar pregnancy
Hydatidiform Mole Diagnosis:
Ultrasonography: However, based on ultrasound, correct diagnosis
can be suspected in only: • 84% of patients with complete mole and • 30% of patients with partial mole (Lindholm and Flam, 1999)
The accuracy of ultrasonogrophy is gestational age dependentIn comlete mole:• 100% of cases cane be diagnosed at a gestational age of
13 weeks or more• 50% of cases cane be diagnosed in earlier pregnancies(Lazarus et al, 1999)
Hydatidiform Mole Diagnosis:
Serum hCG levels: Serum hCG levels of greater than 92 000 IU/l
associated with absent fetal heart beat indicate a diagnosis of complete hydatidiform moles (Romero et al, 1985)
Serum hCG level decreases quickly if the patient has an abortion, but it does not in molar pregnancy
Hydatidiform Mole Diagnosis:
Histopathological examination: It should always be done as far as possible and
samples should be kept for DNA analysis for a final diagnosis when histology can not differentiate molar pregnancy from abortion
Table3: Pathological features of complete and partial hydatidiform mole
Complete Mole Partial MoleMacro-scopically
A mass of large, edematous villi that are diffusely distributed, typically described as resembling a cluster of grapes
The placental tissue is less bulkyA few enlarged villi with a focal distributionA fetus may be identified grossly that often has multiple congenital anomalies including syndactyly of the fingers & toes
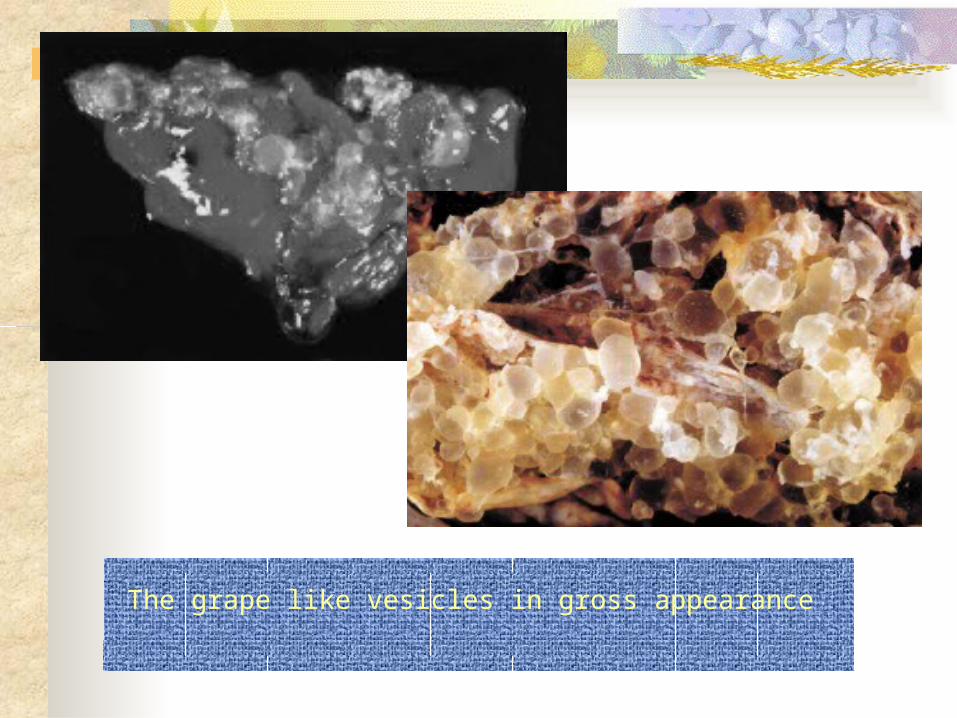
The grape like vesicles in gross appearance
Table3: Pathological features of complete and partial hydatidiform mole
Complete Mole Partial MoleMicro-scopically
Enlarged edematous villi which show a central acellular fluid-filled space referred to as a “central cistern” Abnormal trophoblastic proliferation that is circumferential in contrast to normal villi in which trophoblastic proliferation is at one end of the villusAbsence of fetal tissue
Two distinct populations of villi. One with large, edematous villi with central cisterns. The other contains small villi that show some degree of stromal fibrosisAbnormal circumferential trophoblastic proliferationFetal tissue, RBSs
DIFFERENTIAL DIAGNOSIS1. THREATENED ABORTION2. FIBROID OR OVARIAN TUMOR WITH
PREGNANCY.3. MULTIPLE PREGNANCY4. MISTAKEN DATE5. ACUTE HYDRAMINOS
Complications associated with molar pregnacy: Those related to the increased trophoblastic
tissue volume: Theca-lutein cysts Pregnancy-induced hypertension, hyperthyroidism, Respiratory distress Hyperemesis
Those related to its management: Uterine perforation
Hydatidiform Mole, complications Theca-lutein cysts:
Prevalence: Clinically evident theca lutein cysts (usually >5–6 cm) are
detected in about 25-35% of women with molar pregnancies Association:
They usually correlate with marked elevation of serum hCG levels above 100,000 IU/l
Complications: Pain or pressure that may require percutaneous aspirations. Torsion, rupture, or bleeding are rare complications that can
require oophorectomy Bilateral theca letein cysts increase the risk of post-molar GTD
Course: The mean time for theca luteal cysts to regress is approximately
8 weeks

Hydatidiform Mole, complications Respiratory distress syndrome:
Prevalence: Rare
Pathophysiology: Embolization of trophoblastic tissue Transient impairment of left ventricular function
during induction of anesthesia for suction D&C of molar pregnancy
coexisting conditions such as anemia, hyperthyroidism, hypertension from preeclampsia
Risk factors: Uterine size larger than 14 to 16 weeks’ High levels of hCG

Hydatidiform Mole, complications
Respiratory distress syndrome: Presentation:
Tachypnia and tachycardia following evacuation Bilateral pulmonary infiltrates on chest x-ray
Management: Central venous monitoring Ventilatory support
Course: It should resolve within 24 to 48 hours after molar
evacuation
Hydatidiform Mole, complications
Hyperthyroidism: Prevalence:
Clinical hyperthyroidism is seen in less than 10% of patients with molar pregnancies
A small number of patients may have elevated thyroid function tests without clinical evidence of disease
Management: Beta-blockers should be administered prior to
molar evacuation to prevent thyroid storm that may be induced by anesthesia and surgery.
A hydatidiform mole and a co-existent fetus: Prevalence:
Rare (1 in 22,000–100,000) partial moles and twin gestations with co-existent fetuses
and molar gestations Diagnosis:
Usually, by ultrasound Few, after examination of the placenta following delivery
Complications: Increased risk of medical complications Increased risk for postmolar gestational trophoblastic
disease Management:
No clear guidelines for management
Risk Factors for post-molar gestational trophoblastic disease: Advanced maternal age Factors that reflect the volume of trophoblastic tissue:Clinical
factors that are associated with high hCG levels (>100,000 mIU/mL) uterus large for date, bilateral theca lutein cysts, Respiratory distress syndrome after molar evacuation, eclampsia, hyperthyroidism, Uterine subinvolution with post evacuation hemorrhage.
(With any one of these factors or a combination of many, the risk of post-molar GTD has ranges from 25% to 100%)
Hydatidiform Mole Risk Factors for post-molar gestational trophoblastic disease:
The presence of “invasive trophoblast antigen (ITA)” which has 100% sensitivity and specificity for invasive trophoblastic tumors(Cole et la, 2003)
*There is no correlation between the degree of anaplasia and the risk of post-molar GTD
COMPLICATIONS
IMMEDIATE1. Hemorrhage and shock2. Sepsis3. Perforation of uterus4. Pre-eclampsia 5. Acute pulmonary insufficiency6. Coagulation failure
LATE Development of choriocarcinoma (2 to 20%)
Risk factors of malignant change: Patient’s age>40 or <20 Parity >3 Serum hCG> 100000 mIU/mL Uterine size> 20 wk Previous history of molar pregnancy Thece leutin cysts: large(>6cm diameter)
MANAGEMENT The principle of the management:1. Suction evacuation of the uterus2. Supportive therapy3. Counselling for regular follow up
The patient are grouped into two: Group A:the mole is in the process of
expulsion Group B:the uterus remains inert
Management Complete history and physical examination
Investigations
Medical and surgical care
1
3
2
History and physcal examination: Should aim to rule out the classic symptoms and
signs that would lead to a diagnosis of: severe anemia dehydration preeclampsia thyrotoxicosis
The patient should be stabilized hemodynamically
Management: Investigations:
Laboratory: Pre-evacuation hCG Complete blood count Electrolytes, BUN, creatinine Liver function tests Thyroid function tests
Imaging: Pelvic ultrasound Chest x-ray
Hydatidiform Mole Management:
Medical care: Correction of:
Anemia Dehydration Hyperthyroidism hypertension
Management:Surgical Suction curettage (with oxytocin or prostaglandin infusion)
Hysterectomy
• The method of choice
• Increased risk of medical complications
• Associated with a markedly decreased rate of malignant sequelae (3.5%) when compared with suction evacuation.

Hysterectomy Hysterectomy: is indicated in: a)Patient with over 35, b)Patient complete her family
irrespective of age, c)Uncontrolled hemorrhage or
perforation during surgical evacuation,
Counselling Counselling for follow up: Routine follow up is mandatory for all cases
for at least 1 year.Intervals: initially the check up must be made at an
interval of 1 week till the serum hCG levels become negative.This usually happen by 4-8 weeks.
once negative within 56 days,the patient is followed up at every 1 month intervals for 6 months.
Women undergone chemotherapy should be followed up for 1 year after hCG has been normal.
Methods employed in each visit: a)enquire about each symptoms b)abdomino vaginal examination c)investigations:hCG,chest x-ray
PROPHYLACTIC CHEMOTHERAPY If the hCG levels fails to normal by
the stipulated time(10-12) weeks or relevation at 4-8 weeks.
Post evacuation hemorrhage. Where follow up facilities are not
adequate. Evidence of metastasis irrespective of
the level of hCG.
Prophylactic Chemotherapy: In one randomized clinical trial, a single
course of methotrexate and folinic acid reduced the incidence of postmolar trophoblastic disease from 47.4% to 14.3% (P <.05) in patients with high-risk moles:hCG levels greater than 100,000
mIU/mL,uterine size greater than gestational age, ovarian size greater than 6 cm),
However, the incidence was not reduced in patients with low-risk moles
On the other hand, the use or prophylactic chemotherapy increases the risk of drug resistance
Because of the excellent primary cure rates among women with post-molar GTD, and mortality achieved by monitoring patients with serial hCG determinations and instituting chemotherapy only in patients with postmolar gestational trophoblastic disease outweighs the potential risk and small benefit of routine prophylactic chemotherapy.
Pregnancy after Hydatidiform Mole: Risk of another molar pregnancy:
Increased by 10-fold (1–2% incidence) Current recommendations for management of
subsequent pregnancies: an early ultrasound to confirm normal gestational
development and dates A chest x-ray to screen for occult metastasis
masked by the hCG rise of pregnancy Examination of the placenta or products of
conception histologically at the time of delivery or evacuation for evidence of occult trophoblastic disease
An hCG level should be obtained 6 weeks post evacuation or delivery to confirm normalization.
CONTRACEPTIVE ADVICE
The patient is advised not to be pregnant for at least 1 year.
Use of contraception IUD is contraindicated. OCP:after hCG value have been
normal. Barrier method.
Hydatidiform Mole Prognosis:
Post-molar gestational trophoblastic disease: Risk:
Following complete mole: 20% Following partial mole: 5%
Type: 70% to 90% are persistent or invasive moles 10% to 30% are choriocarcinomas
Diagnosis: A rising, plateauing, or persistent elevation of human chorionic
gonadotropin after evacuation of a hydatidiform mole or an ectopic or term pregnancy
PROGNOSIS More than 80% of H. moles are benign. The
outcome after treatment is usually excellent. Highly effective means of contraception are recommended to avoid pregnancy for at least 6 to 12 months.
About 15 to 20% of cases may develop into persistent GTD.
In 2 to 10% of cases it may change into choriocarcinoma.

Over 90% of women with malignant, non spreading cancer are able to survive and retain their ability to conceive and bear children.
In those with metastatic cancer, remission remains at 75 to 85%, although their childbearing ability is usually lost.

NURSING DIAGNOSISAcute pain related to uterine contraction.Risk for fluid volume deficit related to
execessive vascular loss.Ineffective uteroplacental tissue perfusion
related to abnormal trophoblastic proliferation.Risk for maternal injury related to blood
loss,abnormal blood profile,impaired immune system.

Fear related to fetal loss and outcome of pregnancy.