molar incisor hypomineralization (mih) ojus
TRANSCRIPT

MOLAR INCISOR HYPOMINERALIZATION (MIH)
OJUOLA G.T

OUTLINE Introduction Definition Epidemiology Diagnosis Differential diagnosis Treatment Conclusion References.

Introduction MIH was reported in the past as:
Hypomineralized permanent first molars(PFMs) Idiopathic enamel hypomineralization Dysmineralized PFMs Nonfluoride hypomineralization cheese molars
This condition was termed MIH in the European academy of paediatric dentistry 2000.

Definition MIH is a clinical appearance of enamel
hypomineralization of systemic origin affecting one or more permanent first molars (PFMs) that are associated frequently with affected incisors (Weerheijm 2001)

Definition Molar incisor hypomineralisation (MIH) is
defined as the developmentally derived dental defect that involves hypomineralisation of 1 to 4 first permanent molars (FPM) and frequently associated with similarly affected permanent incisors (Weerheijm 2003)

Definition MIH-like defects have also been observed on
secondprimary molars and permanent cuspids.
These MIH-like defects in the primary molars are now described as Deciduous Molar Hypomineralization (DMH). (Elfrink et al. 2010)
Epidemiology The prevalence ranges from 2.5-40.2 % Prevalence in Nigeria among 8-10 years old in
ile -ife is 17.6% (Oyedele et al. 2015) Another study in ile ife, Nigeria among the
same age group puts it at 9.7% (Temilola et al. 2015)
Some Studies done in other countries are shown in the next slide.


Aetiology It is multifactorial Children with poor health during the first 3
years of life are more likely to be at increased risk for MIH(William et al. 2005)

Aetiology Various causes of MIH have been implicated:
Environmental conditions Respiratory tract infections Perinatal complications Dioxins Oxygen starvation and low birth weight Calcium and phosphate metabolic disorders Childhood diseases Antibiotics Prolonged breast feeding
the aetiology of MIH still remains unclear

Diagnosis Weerheijm et al. 2003 developed diagnostic
criteria for MIH: demarcated opacities posteruption breakdown (PEB) atypical restorations extracted PFMs due to MIH
This is best done at 8yrs of age and done on a wet tooth.
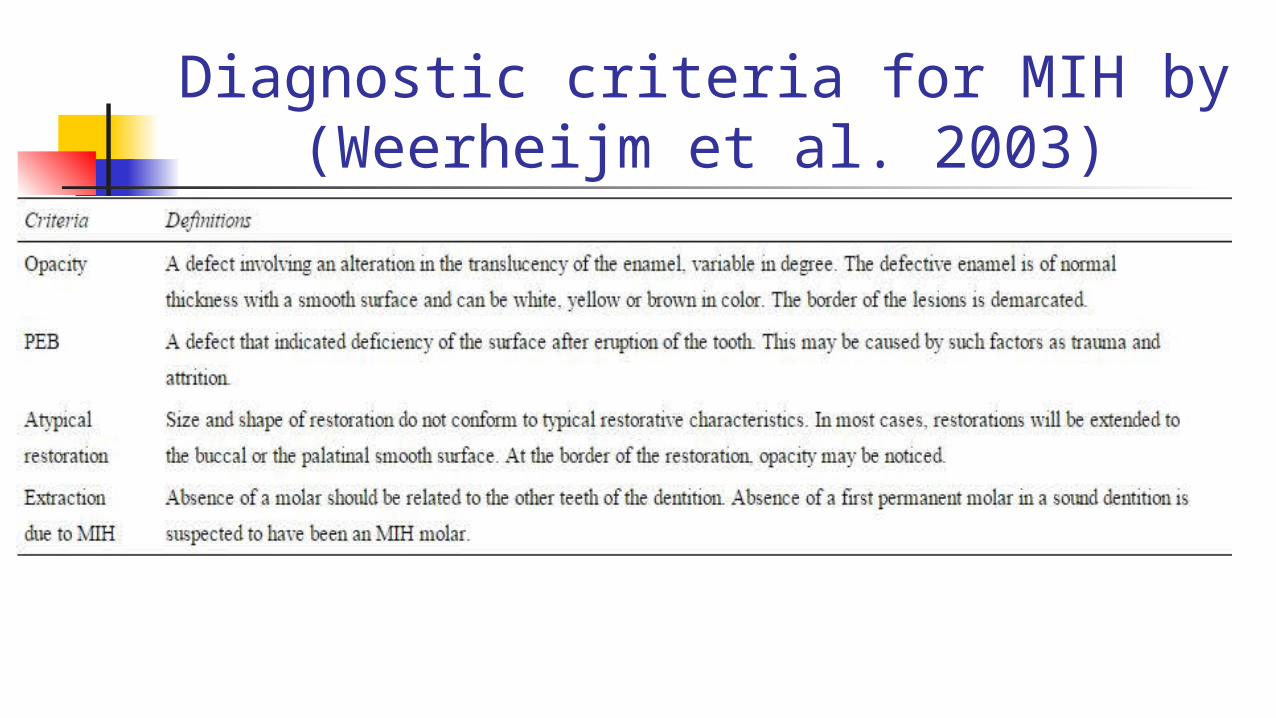
Diagnostic criteria for MIH by (Weerheijm et al. 2003)

Diagnosis Based on the diagnostic criteria, severity of MIH
is classified into: Mild Moderate severe

Diagnosis Mild MIH
Demarcated opacities are in nonstress-bearing areas of the molar
No enamel loss from fracturing is present in opaque areas
occasional sensitivity to external stimuli e.g. air/water but not brushing
There are no caries associated with the affected enamel
Incisor involvement is usually mild if present

Diagnosis Moderate MIH
Atypical restorations can be present Demarcated opacities are present on occlusal/incisal
third of teeth without posteruptive enamel breakdown
Posteruptive enamel breakdown/caries are limited to 1 or 2 surfaces without cuspal involvement.
There is sensitivity

Diagnosis Severe MIH
Posteruptive enamel breakdown is present Persistent/spontaneous hypersensitivity affecting
function. Caries is associated with the affected enamel Crown destruction can advance to pulpal
involvement Defective atypical restoration Aesthetic concerns are expressed by the patient or
parent

Differential diagnosis Enamel hypoplasia
MIH and enamel hypomineralization (EH) can be difficult to differentiate when affected molars have posteruptive enamal breakdown (PEB) due to caries or masticatory trauma
However, in hypoplasia, the borders of the deficient enamel are smooth, while in posteruptive enamel breakdown the borders to normal enamel are irregular

Differential diagnosis Amelogenesis imperfecta
Positive family history Generalized and can be detected preeruptively on
radiograph Fluorosis
Diffuse area of enamel opacities as opposed to demarcated area of enamel opacities in MIH.

Treatment MIH’s clinical management is challenging due
to: The sensitivity and rapid development of dental
cariesin affected PFMs.
The limited cooperation of a young child. The difficulty in achieving anesthesia The repeated marginal breakdown of restorations.

Treatment Six step management approach by William et
al. 2006 Risk identification. Early diagnosis. Remineralization and desensitization. Prevention of caries and posteruption breakdown. Restorations and extractions. Maintenance.
Risk identification, remineralization, andpreventive management Identify children at risk by relevant history of
putative aetiological factors in the first 3 years and from careful study of the unerupted molar on radiographs
Dietary assessment and necessary modification during PFMs eruption.
Commencement of Oral hygiene includint a desensitizing toothpaste

Risk identification, remineralization, andpreventive management When the surface of the PFM is accessible,
remineralization therapy should commence.# Remineralization and desensitization may be
accomplished with casein phosphopeptide-amorphous calcium phosphate (CPP-ACP) oral care products. E.g. tooth mousse
Use of topical fluoride Fluoride varnish Application of Fluoride gels several times in a week
by the parent.

Risk identification, remineralization, andpreventive management Use of fissure sealant.
Use of GIC in partially erupted PFM

Restoration of hypomineralized PFMS Restoring affected PFMs is complicated
frequently by: difficulties in achieving anesthesia managing the child’s behavior determining how much affected enamel to remove selecting a suitable restorative material

Restoration of the hypomineralized permanent incisors. Microabrasion can be an effective treatment in
shallow defects. A conservative approach in managing yellow-
brown hypomineralized enamel involves: etching the lesion with 37% phosphoric acid; bleaching with 5% sodium hypochlorite; and then re-etching the enamel prior to placing a sealant over
the surface to occlude porosities and prevent restaining

Restoration of the hypomineralized permanent incisors. Enamel reduction combined with opaque resin Porcelain veneer delayed until late adolescence
because of continued eruption exposing the margin.


Full coverage restorations Cast restorations are rarely indicated for PFMs
in young children due to placement difficulties associated with: short crowns large pulps long treatment time and high cost The child’s limited cooperation



Conclusion it is not surprising that a MIH child who has had
pain, difficulties with anaesthesia, and retreatment develops poor behavior and dental anxiety (William et al. 2006).
Therefore, identification of risk factors, early diagnosis and institution of preventive measures reduces the severity of MIH which inturn helps in better cooperation of the child.

References Molar Incisor Hypomineralization: Review and
Recommendations for Clinical Management (Vanessa William et al. 2006)
Best Clinical Practice Guidance for clinicians dealing with children presenting with Molar-Incisor-Hypomineralisation (MIH) An EAPD Policy Document by N.A. Lygidakis et.al 2010

References The prevalence and pattern of deciduous molar
hypomineralization and molar-incisor hypomineralization in children from a suburban population in Nigeria (Temilola et al. 2015)
Garg N, Jain AK, Saha S, Singh J. Essentiality of Early Diagnosis of Molar Incisor Hypomineralization in Children and Review of its Clinical Presentation, Etiology and Management. Int J Clin Pediatr Dent 2012;5(3):190-196
