module one - circle - university of victoriacahr.uvic.ca/nearbc/documents/2010/team3revised.docx ·...
TRANSCRIPT

1
Skill Building & Capacity I: Developing and Maintaining the
Collaborative Team

2
Welcome to the Developing and Maintaining the Collaborative Team Workshop brought to you by The Network Environments for Aboriginal Health Research BC (NEARBC – Northern Node) in collaboration with the University of Northern British Columbia, BC Rural and Remote Health Research Network and Northern Health.
In today’s world the role of collaboration has become the most effective way of conducting research and in the provision of services. The collaboration between organizations, communities and individuals is often done through the formation of “teams”. However, the formation of a team moves beyond just a group of individuals with “good intentions” but is a delicate balance of relationships between each other, the organization and community. Leadership style, trust, sharing information, and problem solving are key areas in the establishment of effective team work. A team is also a sliding continuum and in a constant state of change. The influence of obvious and subtle factors has a rebound effect on team functions and can quickly turn an effective and established team into chaos. The measurement of a teams' developmental stage is not a reflection of “negative” or “positive”; it is but a sliding scale of growth and development.
This workshop brings together researchers, community, organizations, students and concerned individuals in an effort to provide a foundation, or a bridge of skills, to create increased capacity in team work.
The format of the workshop is one of integrated team building skills, knowledge and education. This workbook is a supplement to your workshop instruction.
Several icons will draw your attention to specific actions throughout the day:
Means a group or individual exercise A section for your notes Take away skill building

3
MODULE ONE
Workshop Schedule Day One
9:00 am – 4:00 pmOctober 13, 2009
Learning objectives : DAY ONE
□ Identify the need for and importance of collaboration □ Describe the different types of teams□ Describe the phases of team development□ Demonstrate components of successful teamwork
9:00 am – 9:40 am1. Greetings and Introduction 2. Housekeeping & Structure of the Workshop3. Respect 4. What YOU want to learn at this workshop (Charting)
9:30 am – 10: 15 am Round Table team introductions(5 of 5)
Workbook Page 6: Exercise in team formation
10:15-10:30 BREAK
10:30-11:30 Team Basics 101 Workbook Pages 7-14
11:30 – 12:00 The Plan Practice Plan Exercise
12:00 pm – 1:00 pm Lunch Break
1:00 pm – 3:00 pm Theory and Principles Workbook Pages 15-24
3:00 pm – 3:15 pm BREAK
3:15- 3:45 Practice Skills Breakout Practice Plan Exercise
3:45- 4:00 Debriefing & Closure for Day Evaluation

4
Table of Contents Pages
Language and Meanings ……………………………………………………… 5
Team Basics 101 ………………………………………………………………………… 6-8
1. Team Working Exercise2. Team vs Work Group 3. Types of Teams4. Structure of Teams
The Collaborative Team ……………………………………………………………… 9-14
1. Types of Collaboration2. Characteristics of Collaboration3. Seven Essential Elements for Collaboration4. Challenges of Collaboration5. When to Develop a Collaborative Team6. Team Essentials (Chart)7. Elements of Team Formation8. A Collaborative Team is / is not (Group Exercise)9. Where would you find the Collaborative Team?
Theory & Models ……………………………………………………………………… 15-201. Phases of Team Formation2. Aspects of Team Formation3. Sliding Continuum of team Development Stages (Chart)4. Aspects Affecting Team Development5. Team in Context of environmental variables (Chart)
Principles of Successful Teamwork ……………………………………………… 21-23
1. Characteristics of Effective Teams2. Developing Team Member Vision and Rules
Language and Meaning

5
Drinka & Clark (2000) note that “each discipline views themselves as somewhat exclusive, unique and special” and there is a certain culture of language that is used to separate and divide—to maintain discipline status. The goal of inter-professional practice is to understand that no single discipline can address complex health problems.
Team Formation Team is a process that is structured and guides the actions of two or more individuals within both the expectations of the organization and that of the patient (client, participant) (Drinka & Clark, 2000).
Team - A team is a group of people who collaborate and interact to reach a common goal
Inter-professional – A fully integrated practice by a team of professionals from a diverse background of disciplines. Each member of the team has an integrated knowledge of the other team members’ roles, and all work from an equally valued team mandate. “When two or more professions purposely interact in order to learn with, from and about each other to improve effectiveness and the quality of care” (Gilbert, 2001).
Collaboration – An effort to consult and co-operate as a group or team in developing a shared direction or vision. Each member still maintains a separate functional identity. A collaborative practice is an active and often ongoing practice partnership between professionals, teams or organizations” (Gilbert, 2001).
Integration – The merging of differences into a single vision – a dependency between the parties where all hold equal value.
Patient-Centered - Patient-centered practice recognizes that the patient’s participation in the development and implementation of his/her care plan is integral. A patient-centered approach recognizes that health care is influenced by genetic, environmental, social and behavioural factors.
Person (people) Centered— Describes that not only are patients at the center but also healthy community members. It is a term “most often used to refer to health care systems that offer service to healthy individuals, as well as those with acute or chronic health concerns” . . . “understood for what it is not—technology centered, doctor centered, hospital centered, disease centered”. (Vancouver Coastal Health, 2006).
Determinants of Health - The Public Health Agency of Canada states the determinants of health “are: income and social status; social support networks; education; employment/working conditions; social environments; physical environments; personal health practices and coping skills; healthy child development; biology and genetic endowment; health services; gender; and culture. Each of these factors is important in it’s own right. At the same time, the factors are interrelated” (Cited on web site:http://www.phac-aspc.gc.ca/ph-sp/phdd/determinants/determinants.html#unhealthy).

6
Team working moment
Consider these questions:
1. What are your experiences with team work?2. What types of teams can you indentify?3. Who were members of these teams?4. What were the qualities that made the team work?5. What were the challenges? 6. What impact does your past experience have on your perception of
team work?
Your Notes:
Team Basics 101:

7
Team vs. Work Group
Work Group TeamOne “boss” each member reports too group does not necessarily collaborate with each other
The leader is not a boss but a coach or facilitator to the team
Each person completes tasks as per job description and Boss directives.
A group of individuals with complementary skills committed to a common/shared goal/vision
Emphasis on individual performance Interdependence and accountability between team members is encouraged
Uni-directional: Communication flows down from boss to individual
Dual directional: Communication is both top down and bottom up
Boss is the authority and directs work processes Team has the authority to manage it’s own work processes
Goals set by organization Clear boundaries and tasks
Types of Teams
1. Working Team2. Project Team3. Special Team4. Research Team5. Multi-purpose Team6. Independent Team7. Management Team8. Trouble Shooting Team
Structure of Teams
ONSITE, OFFSITE. VIRTUAL: Discuss your experiences with each . What are the strengths and challenges

8
Unidisciplinary:A group of people from the same discipline who work together.
Multidisciplinary:A group of people from different disciplines who develop plans independently.Generally, each discipline conducts an independent assessment of their interest group. Often one discipline is the case manager, orders the services and coordinates the care. The group may meet but, in general, each discipline implements its independent plan as an additionallayer of services.
Interdisciplinary:A group of people from different disciplines who assess and plan care in a collaborativemanner. A common goal is established and each discipline works to achieve that goal.Care is interdependent, complimentary, and coordinated. Joint decision making is thenorm. Members feel empowered and assume leadership on the appropriate issue(depending upon needs and their expertise).
The Collaborative Team
Team
Collaborative(Facilitated)
Multi-Disciplinary
Inter-Professional
Workgroup(unidirectional)
Uni-disciplinary
Multi-disciplinary
Inter-disciplinary

9
Types of Collaboration:
1. Day to day2. Clinical teams (health or disease focus)3. Integrated teams4. Cross integration: mandated and non-mandated5. Consultative
Characteristics of Collaborative Practice Include ( MCFD, 1997 ):
Active participation of the client Sharing or transferring of information and skills across traditional boundaries Participants view themselves as part of a team and contribute to a common goal Relationship between participants is non-hierarchical and power is shared Leadership is shared and participants are inter-dependent Participants work together in planning and decision making Participants offer their expertise, share in the responsibility and are acknowledged by
other members of the group for their contribution to the goal Clear definition and understanding by team members of participants' roles/responsibilities Respect for autonomous professional judgement and decision making of the client/family Effective communication skills and group dynamics Supported by organizational structures and vision
Seven Essential Elements for Collaboration (Way & Jones, 2001)
1. Responsibility and Accountability Independent and Shared Shared decision making Accept shared responsibility for the outcome of the care plan
2. Co-ordination Joint decisions about who will do what to ensure that the care plan is carried out
3. Communication Sharing with the other providers critical information Information is relevant, concise and timely Clear identification of information sharing expectations
4. Co-operation Respecting other disciplines’ professional opinions and viewpoints Being willing to examine and alter your own professional views and perspectives
5. Assertiveness

10
Opinions and view points presented in a manner that fosters the integration of approaches
6. Autonomy Providers can independently make decisions and carry out the care plan
7. Mutual Trust and Respect Provider able to depend upon the integrity of the other as the foundation for their
professional relationship.
Challenges of Collaboration:
“Group Think” Becoming homogeneous Becoming too ridged / structured Slowness Trust Not everyone comes to the team with an equal value Member reward differences
Some can ---- Some can’t ------ Some will ---- Some won’t
11
When to Develop a Collaborative Team
When Benefits ChallengesNo one individual has the right combination of skills, knowledge and practice to do the job
The situation is multi-faceted, complex and/or a unique / infrequent challenge
Requires a high degree of interdependence, coordination and communication
When the objectives are clear but multi-leveled
Can be creative and unique approach
Teams can bring multi-skills to bear on intractable situations
Enlist more information and ability by tapping into different skill sets and networks
Increased collaboration and communication
Can be more “person focused”
Time to organize
Must be managed with care and skill
Silos
Buy in
Knowing who to involve
Knowing when to involve them
Developing the right combination of skills, knowledge and experience
Balancing time, authority and systemic issues
Your Notes:

12
Clear Common Goal
A supportive environment (Physical and Systemic)
Co-location
Organizations are compatible with team based work
Commitment to Common Goals
US, WE, OUR
Each member contributes and benefits
Supportive Leader & Mentor
Team Member selection
Competence
Defined performance expectations
Membership manual – road map – welcome package
TEAM
ESSENTIALS
Elements of Team Formation1. Systemic – Management Support
Support from all involved levels of the organization (union, directors, managers, policy etc) Budget / Financial commitment defined Environmental structures: works space, supplies, transportation and equipment. Agreements at the upper levels Clearly defined reporting, documenting and decision authority
2. Team Vision & Agreement Provides the means of “how” to meet the memo of agreement and is specific to each team. Provides the commonality, contribution and direction of the team Defines the team – clearly outlines roles, times of involvement and expectations Defines the relationship and interaction of members Defines reporting, conflict management and communication The approach to decision making for the team (i.e.: work schedule, plans and holidays) Clarify objectives – team vs. employer Environmental Factors: Co-location – work space – equipment – Kitchen
3. Team member selection

13
Team member selection is the hardest part of team formation, however, membership is critical to team cohesiveness and success.
Three methods of coming to a team:
Factors: Skills (Technical, problem-solving, interpersonal, organizational) Potential Open Flexible Collective Role – short or long term team member
Behaviors: Attendance Involvement Interruptions Ability to offer and accept constructive criticism Agree to discuss and share information Confidentiality Action oriented
4. Team based Leadership
Every team needs a leader but not necessarily as a “BOSS” Coach, Mentor, working member of the team Keep the vision focus Smooth out conflict Mediates – in particular “turf” or “Silo” ing Co-ordination of activities Act as a liaison between team and community / systemic Negotiate relationships Identify gaps and resources Obtain resources Set and monitor milestones Ensure member involvement, contribution and benefits Keep work on track
Differs from Work Group1. Decision Maker, delegator, and scheduler2. BOSS – with bottom line of direction and results3. Stands outside of the team – or as the top of the hierarchy
No choice Part of job
AssignedWant to be involvedCommitteesNon Profit
VoluntaryChoiceElected processset time
Nominated

14
YOUR NOTES
A Collaborative Team IS?
IS NOT?
Where would you find Collaborative Teams?
Research Primary health (pre/post natal,
obstetrics, new born care) Mental health care Addiction Treatment Outreach Palliative Care In home support Education & Prevention Chronic disease management
Maternal & child care supports Occupational health Community health Care of the vulnerable Rehab services Parenting Social and community services Counseling Family services Youth service
Theory & Models

15
The definition of a team is broad and crosses all disciplines, practices and education forums. However, despite the variant of models there exists the fundamental understanding that a team moves beyond just a “group” of people. At its fundamental level a team is an integrated, directed group of individuals who share a common goal and vision. Researchers note that a team is a fluid concept, not one that is based on an automatic template format. Team development is not static and linear, but is based on an evolutionary process of growth. The concept of evaluation of team development and effectiveness has its foundation in the field of business and sales management - Tuckman, Parker and LaFasto are some of the recognized leaders in this area, and their concepts form the foundation for many of the discipline specific models that have been developed. The Tuckman model is considered the standard foundation of the team processes.
TUCKMAN MODEL:There is a general consensus amongst researchers that, the beginning standard, for evaluating team performance and formation, is based on Tuckman’s (1965) model stages of: forming, storming, norming and performing (Farrell et.al., 2001). Within this model, team dynamics move through a predicable format of development and growth, but the process is subject to the impact of individual team dynamics and environment. Essentially, the forming stage is the one in which a new team comes together and begins to develop team processes, expectations and roles. The storming stage is the one in which the team goes through the conflict of team growth—this is the stage in which the clashes of personality, mandates and roles become issues and need to be worked out. The norming stage of development is the time in which the team begins to collaborate and work within the established roles brought about in the storming stage of development. The performing stage is when the team has meshed into a collaborative unit and is no longer focusing as much on the internal team process but is able to function and achieve goals. However, as the team evaluation concepts expands into the disciplines outside of the business arena, the need to capture the influences of the work environment on team practices increases.
In the health care field the impact of the patient, staffing and community relationships on the team dynamics is critical to team performance. Several models have been developed to try and capture the uniqueness of the Health Care team for example, Drinka, Heinemann and Mead all have established health care models.
DRINKA MODEL Drinka & Clark (2000), expand Tuckman’s model by adding the layer of “leaving”, which acknowledges there is significant impact on team efficiency due to high rates of staff turnovers and/or students. This model also presents “four essential team components and their variables” which define the effectiveness of the health care team as issues that directly affect practice, Intra-team issues, Organizational issues and Actions necessary for team maintenance. Fundamentally, integrating the models proposed by Tuckman, Parker and LaFasto & Larson into single model concept
HEINEMANN MODELHeinemann and Zeiss,(2002) established a concept of best team practices in health care within the Tuckman model, but identified health care teams as having a unique structure that cannot be articulated in the same format as general team structures. The Heinemann & Zeiss model concludes that the effectiveness of the health care team is defined within the four categories of structure, context, process and productively, which mirrors much of the Drinka & Clark model, (with the exception that Heinemann & Zeiss model de-emphasis the impact of individual factors on the team effectiveness).
MEAD MODELMead, 2005 argues that primary health care is moving towards Inter-professional practices as health care costs continue to rise and the adoption of integrated team work is driven by finances, practices and professional effectiveness. Mead suggests there are five levels that must be achieved and integrated: Collaboration, Accountability, Focusing, Development, and Education. Within the Mead model best

16
practices are the result of a balance between the inter-professional relationships (professional, partners, policy, public and patients), organizational structures/systems/processes and a holistic commitment. The extent that a team is able to achieve success in the provision of inter professional practices is also based on the preconditions of
Directness – Clear roles, responsibilities, conflict management, expectations and supportive process
Multiplexity Continuity – Consistency for team, partners, community Parity – Equality of power, authority and participation Commonality – of goals, visions and mandates
Benefits and Perks (incentives of collaboration) – Improved outcomes, personal/professional organization/community
Phases of Team Formation
Groups do not become well-functioning interdisciplinary teams by deciding to become a team. All teams develop through a series of phases each of which can last several months or longer. Sometimes a developed team will even return to a previous phase for a period of time and work out of it. Tuckman first labeled these phases and many experts who work with groups use these labels:
Forming: creation stage for the group. Storming: tasks and roles are worked out through conflict. Norming: norms and patterns are worked out. Confronting: conflictual stage (some professionals use this label or the storming label but not
both). Performing: team working together for the care of the patient.
Drinka has described six phases of team development – and presented stages and interventions:
Forming: Group is created. Superficial sharing of name and background information. Members size up and test each other categorizing with outside roles and status. Members are guarded, more impersonal than personal, a few are active, others are passive. Uncertainty over purpose. Conflict is neither discussed nor addressed.
Norming: Difficulty in understanding goals and purpose of the team. Attempt to establish common goals. Mistrust of each other exhibited by caution and conformity. Role overlaps become evident. Conflicts are present but are openly covered up or glossed over. A few members attempt to establish bonds with others having similar views. Team establishes ground rules and begins to clarify common roles. Team may want leader(s) to assume responsibility. Numerous strategies for increasing equality of leadership (e.g., rotating leadership). Increase in defensive communication and disruptive behavior. Frustration among team members. Some members project blame and responsibility toward the perceived leaders. Competition among team members. Some members come late or do not come to meetings.

17
Confronting: Conflicts can no longer be avoided and some members verbally attack other members. Increased conflicts over leadership, equality, and commitment Anxiety over expression of affect. Some conflicts are addressed in a direct manner. Some members withdraw from the team. Search for leader who will resolve conflicts. Functional leaders emerge. Realization that power is not equal. Realization that everyone has power for leadership and decision making. Constructive confrontation when conflict occurs Goals and roles are re-clarified. Coalitions form but change according to needs of the team.
Performing: Differences of members are appreciated. Members encourage and help each other. Reality testing increases and grows stronger. Self-initiated active participation is the norm. Relationships are strengthened and members must trust each other. Attendance at meetings is regular. Conflicts seen as normal and are used as impetus for program improvement. Emphasis on productivity and problem solving. Increased responsibility for leadership in teaching, wherever skills warrant it.
Leaving: Individual leaves. Anger toward members of the team in general. Denial of impending termination from team by disbelief and regret. Expression of wish to remain with the team. Regression to an earlier phase. Member may express happiness over leaving the team. Team Terminates. Withdrawal by some members, depression, sadness. Expressions of team’s superiority. Feelings are expressed as testimonials. Need to affirm that team membership has been a valuable experience.
Your Notes:
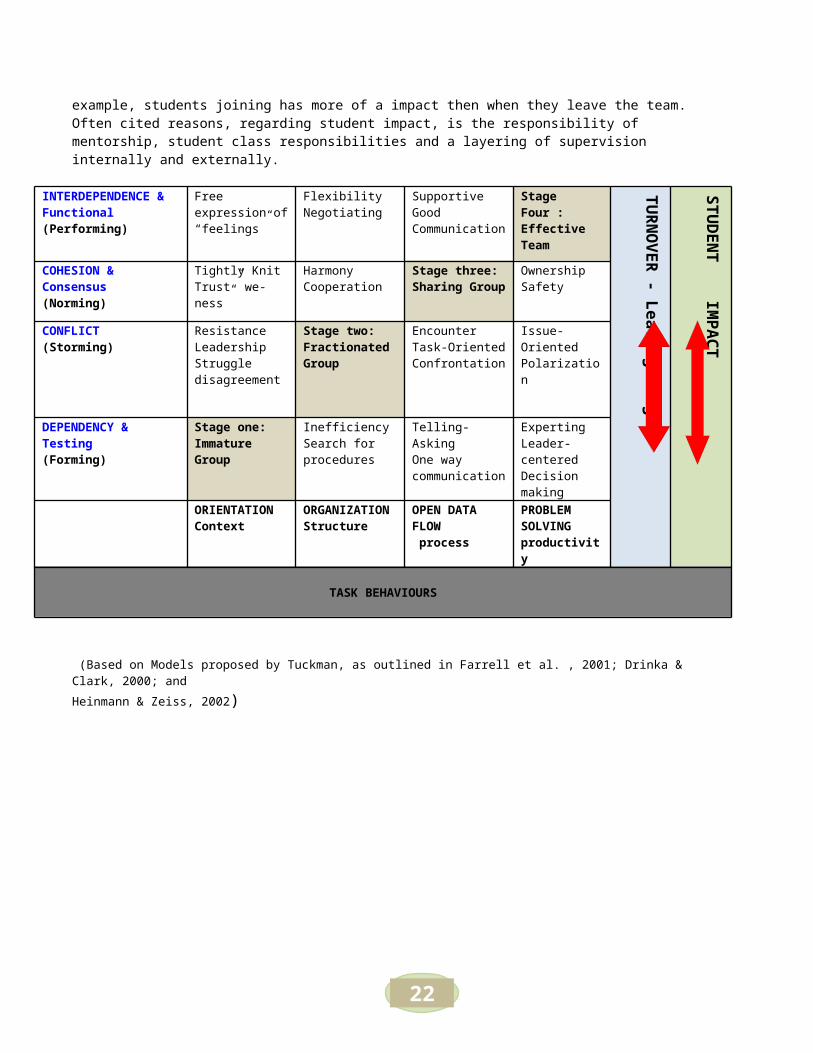
Chart One: A Sliding Continuum of Team Developmental Stages

18
The impact of the leaving stage, member turnover or student involvement, is a sliding scale and is dependant upon on factors such as stage of team operation, individual personalities, time of team membership and organizational influences. Consequently, there is no set pattern of impact when a member of the team leaves, nor is there a predetermined movement within the stages of development. The degree of the impact on teams vary for example, students joining has more of a impact then when they leave the team. Often cited reasons, regarding student impact, is the responsibility of mentorship, student class responsibilities and a layering of supervision internally and externally.
INTERDEPENDENCE & Functional(Performing)
Free expression of “feelings”
FlexibilityNegotiating
SupportiveGood Communication
Stage Four : Effective Team
TUR
NO
VER - Leaving Stage
STUD
ENT IM
PAC
T
COHESION & Consensus(Norming)
Tightly Knit Trust” we-ness”
HarmonyCooperation
Stage three: Sharing Group
OwnershipSafety
CONFLICT(Storming)
Resistance LeadershipStruggle disagreement
Stage two: Fractionated Group
EncounterTask-OrientedConfrontation
Issue-OrientedPolarization
DEPENDENCY & Testing(Forming)
Stage one:Immature Group
InefficiencySearch forprocedures
Telling-AskingOne way communication
ExpertingLeader-centeredDecision making
ORIENTATION Context
ORGANIZATION Structure
OPEN DATA FLOW process
PROBLEM SOLVINGproductivity
TASK BEHAVIOURS
(Based on Models proposed by Tuckman, as outlined in Farrell et al. , 2001; Drinka & Clark, 2000; and Heinmann & Zeiss, 2002)
Aspects Affecting Team Development

19
Several variables can affect the development of teams. These variables fall under four specific areas:
1) Personal/professional (what the individual brings to a team);2) Intra-team (the structure and processes of the team);3) Organizational (institutional contributions and commitment to the team); 4) Team maintenance
Personal/Professional Commitment to team concept; Willingness to engage in the work of the team and to improve it; Commitment to learn the values and knowledge bases of other professions; Mix of leadership styles; Openness to new knowledge and willingness to risk; Collective knowledge to do the job; Mesh of client needs and professional expertise; Interdisciplinary protocols developed and used by the team.
Intra-Team Desk/office placement and structure for formal/informal interaction; Physical arrangement and technology Range of formal and informal team leaders ; All members view themselves and are recognized by others as leaders; Employ leadership according to the need; Common goals; Team goals are negotiated and reviewed periodically by the team; Negotiated roles; Members understand their team roles; Ongoing mechanisms for managing conflict; Conflict viewed as healthy; Willingness to address conflicts as they rise; All team members perceived as having power for decision-making.
Organizational Organization’s philosophy consistent with the team’s philosophy on patient care; Ongoing resource support from local organization; External organization(s) recognize and are willing to work on common problems.
Team Maintenance Team regularly evaluates and improves itself (products, protocols, and processes); Team empowers new members’ Members teach team leadership skills to newer members; Team members welcome a questioning environment; Feedback is open and direct.
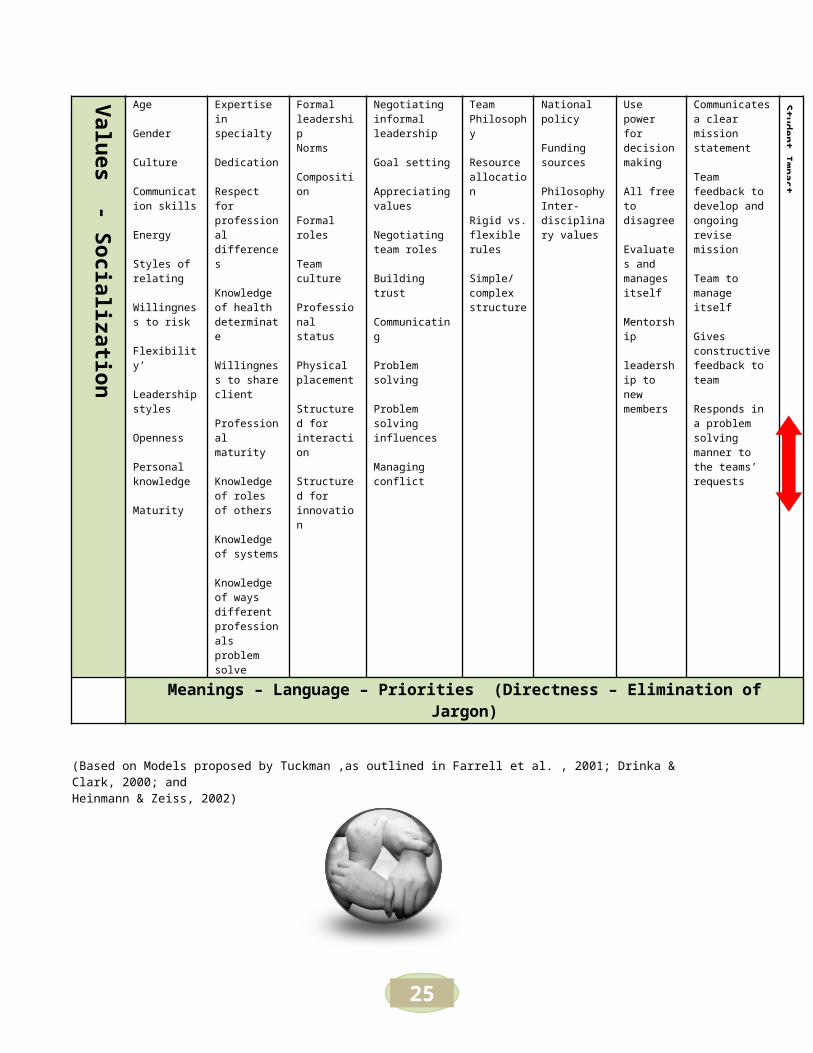
Chart Two: A Team in Context of Environmental Variables

20
Overlapping the model of team developmental stages are also the evaluative measures as outlined in this chart. Issues that directly
affect Practice Process
Intra-Team Issues Context
Organizational Issues Structure
Actions necessary for Team MaintenanceProductivity
Values - Socialization
Personal Professional Team Structure
Team Process Internal External Organization
Team Organization
Age
Gender
Culture
Communication skills
Energy
Styles of relating
Willingness to risk
Flexibility’
Leadership styles
Openness
Personal knowledge
Maturity
Expertise in specialty
Dedication
Respect for professional differences
Knowledge of health determinate
Willingness to share client
Professional maturity
Knowledge of roles of others
Knowledge of systems
Knowledge of ways different professionals problem solve
Formal leadershipNorms
Composition
Formal roles
Team culture
Professional status
Physical placement
Structured for interaction
Structured for innovation
Negotiating informal leadership
Goal setting
Appreciating values
Negotiating team roles
Building trust
Communicating
Problem solving
Problem solving influences
Managing conflict
Team Philosophy
Resource allocation
Rigid vs. flexible rules
Simple/complex structure
National policy
Funding sources
PhilosophyInter-disciplinary values
Use power for decision making
All free to disagree
Evaluates and manages itself
Mentorship
leadership to new members
Communicates a clear mission statement
Team feedback to develop and ongoing revise mission
Team to manage itself
Gives constructive feedback to team
Responds in a problem solving manner to the teams’ requests
Student Impact
Meanings – Language – Priorities (Directness – Elimination of Jargon)
(Based on Models proposed by Tuckman ,as outlined in Farrell et al. , 2001; Drinka & Clark, 2000; and Heinmann & Zeiss, 2002)
Principles of Successful Teamwork
21
The key essential principles of teamwork are:
1. Coordination of services, 2. Shared responsibility, and3. Communication.
Characteristics of Effective Teams
Purpose, goals, and objectives are known and agreed upon. Roles and responsibilities are clear. Communication is open, sharing, and honest. There is disagreement without
tyranny and constructive criticism without personal attack. Team members listen to each other. Team members are competent, professional, personally effective, and make
appropriate contributions. Teams cooperate and coordinate activities. Decisions are reached by
consensus. When decisions are made, assignments are made clearly, accepted, and
carried out. Leadership shifts depending on the circumstances. Team members support each other and act as different resources for the group. Team members trust each other, minimize struggles for power, and focus on
how best to get the job done.
Developing Team Member Vision & RuleTeam rules, both for team management and for member behavior, are needed in the early stages of team development. Not having these rules is a primary cause of later team problems and can slow or stop team development completely. Rules for team governance should include some or all of the following:
Effective teams must work across settings and have well-organized mechanism to share information. Because the focus of the team is on the person, providers must share information clearly and effectively. By focusing on the client, the team shares a common goal.
What type of vision, rules, expectations or agreements does your team have? Are some unspoken? How is this information shared with new team members?
22
All members share a clear understanding (and the larger organization within which it operates) about the overall purpose of the team and the goals for each meeting.
Determine the composition of the team, including which disciplines are needed as members and the number of members (enough to get the job done; not so many that the work cannot get done).
Allow the problem to define the composition of the team, not vice versa. Determine how often the team needs to meet and specify attendance requirements (Is there a
core team of doctor, nurse, and social worker? Are other disciplines asked to participate on cases that require their expertise?).
Identify time, place, and duration of team meetings. Determine a system by which cases are to be presented and by whom. Identify how care plans
and action will be carried out and documented (Is one member chosen to write down the care plan or does this responsibility rotate?).
Identify opportunities or requirements for team-building meetings and/or team training. Create mechanism for enforcing both governance and behavior rules (if rules are made and not
enforced, the team can quickly become ineffective and be a negative experience for everyone involved).
Clear communication of what is occurring and why it is necessary. The time spent with participants clarifying rules and getting a commitment for involvement will prevent team problems and support the development of an effective and efficient team.
Behavior rules and expectations are also needed for each team. They can include some or all of the following:
Ensure clear understanding by all team members of what a collaborative team is. Promote understanding and respect for others’ expertise. Recognize the culture of the professions involved. Learn how to articulate your information clearly to others (for example, client and patient mean the
same thing in different professional groups. Share information and expertise openly.
TEAM BUILDING IS
Not a linear process
Can take 3-5 years with NO changes

23
Identify and follow a decision process when roles overlap. Resist setting rigid boundaries on roles. Instead, promote effective ways of sharing responsibilities
and tasks. Define acceptable behavior (for example, willingness to work with other professionals to develop a
care plan, active participation, respect for others’ roles).
Your Notes:
Workshop Schedule Day Two 9:00 am – 4:00 pm October 14, 2009
Learning objectives : DAY TWO
□ Identify skills of different individuals within teams□ Articulate barriers that affect communication exchange □ Demonstrate effective communication tools □ Identify sources and types of conflict in teamwork.□ Identify strategies for managing conflict within a team

24
9:00 am – 9:30 amGreetings and Introduction Housekeeping & Structure of the Workshop
9:30 am – 10: 15 am Team Roles and Responsibilities
Leadership
Workbook Pages 26-33
Workbook Pages 35-37
10:15-10:30 BREAK
10:30-11:30 Communication Workbook Pages 38-44
11:30 – 12:00 The Plan Practice Plan Exercise Page 39
12:00 pm – 1:00 pm Lunch Break
1:00 pm – 3:00 pm Communication Skills Con’tWorkbook Pages 44-52
3:00 pm – 3:15 pm BREAK
3:15- 3:45 Module Three Workbook Pages 54-62
3:45- 4:00 Debriefing & Closure for day Evaluation
25
MODULE TWO
Leadership, Communication and Conflict Management
MODULE TWO
Table of Contents Pages Section 1:

26
Team Roles and Responsibilities ………………………………………… 27-34
1. Skills of different Professionals on Teams2. Specific roles/skills of Team Members3. Decisions, Power and Authority (Chart)4. Influences on Team5. What does an Empowered Team Look Like?6. Power Types (Chart)7. Resistance8. Trust (Exercise)9. Signs of Dysfunctional Teams10. Key Components of Productive Teams
Leadership …………………………………………………………………… 35-381. Shifting Leadership roles2. Team Based Leadership3. Characteristics of a Leader (Chart)4. Leadership Approaches & Roles (Chart)
Section 2:
Effective Team Communication ……………………………………………. 38-411. Planning the Event2. Techniques that Encourage Communication3. Styles of Communication
Team Conflict ………………………………………………………………… 41-441. Team Responsibility2. Healthy vs unhealthy Conflict (Chart)3. Conflict Dynamics and Factors4. Conflict Roles and Perceptions5. Conflict and Resistance (Chart)
Conflict & Styles of Practice …………………………………………………… 45-53
1. Self Assessment of Conflict2. Strategies for Preventing, Reducing and Managing Conflict3. Addressing Conflict (Team, Private and Personal)4. Common Approaches Conflict Resolutions5. Characteristics of Constructive Feedback6. Conflict Management Techniques7. Role and When to Use
Team Roles and Responsibilities
Many professionals and community members are not familiar with the education base, the roles, or the range of functions of members of other disciplines. This lack of familiarity is due, in part, to the manner in which each group is trained – a unique professional environment with its own language, terminology, problem-solving methods, and professional behaviors. This approach to training coupled with a general
27
lack of knowledge leads to under utilization of skills and capabilities and to disputes about areas of overlapping practice.
Skills of Different Professionals on Teams
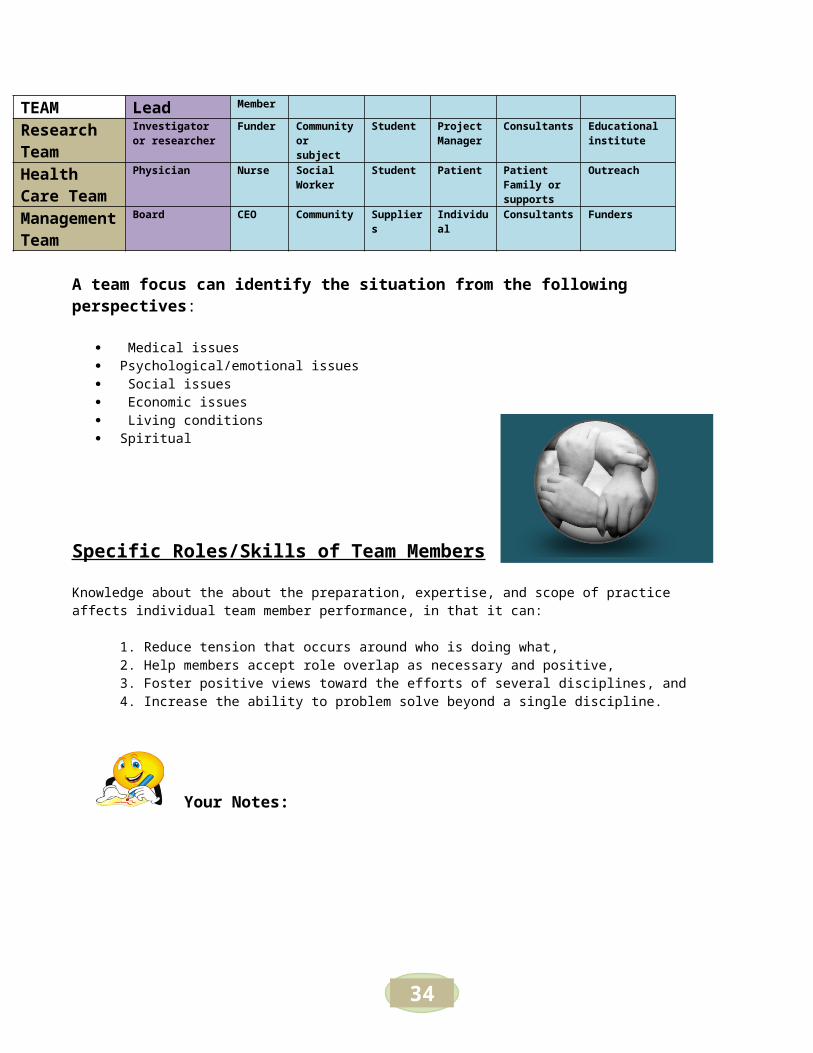
Team members from different disciplines bring a unique set of skills (Table) skills will overlap. It is important to recognize that each profession trains its members in a culture that adopts a common language, professional behaviors, values, and beliefs. When members of a team do not share a common team vision and understanding, disagreements can arise. Most professionals do not recognize the training of others and learn what other professionals do only after they are practicing as professionals.
TEAM Lead Member
Research Team
Investigator or researcher
Funder Community or subject
Student Project Manager
Consultants Educational institute
Health Care Team
Physician Nurse Social Worker
Student Patient Patient Family or supports
Outreach
Management Team
Board CEO Community Suppliers Individual Consultants Funders
A team focus can identify the situation from the following perspectives:
Medical issues Psychological/emotional issues Social issues Economic issues Living conditions Spiritual
Specific Roles/Skills of Team Members
Knowledge about the about the preparation, expertise, and scope of practice affects individual team member performance, in that it can:
1. Reduce tension that occurs around who is doing what,2. Help members accept role overlap as necessary and positive,3. Foster positive views toward the efforts of several disciplines, and4. Increase the ability to problem solve beyond a single discipline.
Reflect back to the opening of this workshop – what skills, professions, experience, and knowledge does your team have or bring?

28
Your Notes:
Decisions, Power and Authority :
How are decisions made ? Provide examples of each

29
Influences on Team
A clearly defined problem or issue Agreement on who has responsibility for what Agreement on procedures and methods to be used before discussion begins Clarity about the level of authority Effective communication Effective means of recording & documenting Appropriate team members A method for building commitment and ownership of direction Support from the organization to carry out the decision
Decision Making
Methods
Consensus
Decision by Non
Decision
Autocratic
Autocratic with Polling
Majority Rule
Voting
Minority Rule
No competition
Other
Majority is not always RIGHT !
When to use consensus1. When a number of options need to be explored and considered2. When it is important to explore many facets of an issue 3. When the solution creates more problems4. When the decision is final

30
What Does an Empowered Team Look Like? Have ability to speak for oneself Stay focused on task and process Clear on the “who, what, when, why and how” Ability to restate Ability to determine personal preference and state it before a team Ability to distinguish facts from opinions Ability to identify and name feelings (yours and others) Low level of defensiveness as people question ideas Willingness to listen: process others viewpoints Commitment to finding the best options Low level of competitiveness Sufficient self-esteem to say NO Ability to look for mutually supported alternatives Listening for and synthesizing areas of agreement Patience to hold back from premature decision making Desire to try
Your Notes:
POWER
Power Types
Can a team agree to disagree and still maintain goal and direction?
31
Your Notes
Resistance to giving up status of control & power
What you would see Overcoming
Detach from the team Walking out
Blaming
Saying too busy
Refusing to participate “or just doing
Understand and discuss the resistance openly
Acknowledge feelings
Comfort members without trying to fix
Real & Appropriat
eMisused
competative
position
victim
guilt
selfesteem
position
expert
Role & Authority
Verbal
Or
Non Verbal
Overt
&
Covert
Explore with your Team what experiences you have had with power!

32
lip service”
Threatening to quit
their discomfort to changeAnticipate and plan for resistance
Convert the resistance to positive
Educate – train individualsComfort members without trying to fix their discomfort to change
Discipline members and define the consequences for lack of collaboration
Promote gains & benefits for the individual, the team and the client
Slow to do things, suggest long debates over pro/con “put off”
Having a rejection reaction “you didn’t include me”
Viewing team building and work as separate
Stating that team work is ‘to much”
Procrastinating
Discounting the roles & contributions of others
Recruitment and manipulation of team members
Saying too busy Actively or passively sabotage the team efforts
Stating team building not part of “job”
Poison talk re: waste of time, team worse than ever…
Undermining
Being negative – hopeless
“management will do what they want anyways”
Attacking others
Using clients – members in the cause “well you will have to ask or work with if you want to continue”…
OTHERS?
ResistanceTrust & Confidence
Trust how do we gain it?
Team trusts is often based on whether we perceive a balance between what we are giving to the situation and what we are getting from it”
“Synergy = when the team shifts from individuals to a entity that is greater than its parts”

33
How do we lose it?
Signs that we don’t have it?
Your Notes
When team members are feeling a of lack of Trust this can lead to greater effort to gain personal control
Signs of Dysfunction Teams
34
Key Components of Productive Teams
Personal agendas are sidelined Respect and flexibility Culturally (lifestyle, spirituality, etc safe) Shared vision and goals Team climate is comfortable and empowering Individual competition is limited Open communication Respect for diversity Collaboration & open-minded Strength based Trust Conflict and differences are considered “opportunities” Team practices reflection of procedures, process, practices
and experiment with changes Regular meetings – that are clear, specific and time
sensitive Planning for and recognition of the impact of arrival /departure of team members Orientation for new members Opportunities for social and professional relationship & education development Rotating leadership Consensus decisions Lack of service duplication PERSON FOCUS
Leadership
Lack of team vision, goals and objectives
Lack of support from management
Lack of buy in & commitment
Splinter groups or cliques
Turfing & returning to silo services
Not maximizeing the skills of team members
Lack of training or education for members
Lack of key members
Too many members
Not showing up & lack of being involved in team
/workplaceteam can't make decision
Hidden Agendas
Lack of clarity about roles and responsibilities
Incompatable polices, procedures and decision
team members lack of willingness to cooperate
Team focus at the expense of team
realtionship development
Anti - team culture & lack of sharing
information/resources
Lack of Leadership &
Direction

35
The concept of different roles held by members of a interdisciplinary team is anessential and very complex element of effective team function. Membership and leadership roles are inseparable and involve an emphasis on role functions rather than on a particular discipline or a set of personality traits. Success involves the effective utilization of a team’s total resources. Although one or more individuals may have a formal designation as a group leader, the effective use of resources means that all team members need to share responsibility for informal and formal leadership. In true inter-professional teams, the functions of leadership and membership are viewed as synonymous.
Shifting Leadership Roles on Teams
Collaborative teams demand equal participation and responsibility from all team members with shifting leadership determined by the nature of the problem to be solved.
Even when one team member, has administrative authority over others (e.g., as supervisor), members of a team treat one another as colleagues rather than as a single leader and subordinates.
Emphasis by the team moves beyond the a narrow focus and broadens the roles and responsibilities of team members.
Team Based Leadership
Every team needs a leader but not necessarily as a “BOSS” Coach, Mentor, working member of the team Keep the vision focus Smooth out conflict Mediates – in particular “turf” or “Silo” ing Co-ordination of activities Act as a liaison between team and community / systemic Negotiate relationships Identify gaps and resources Obtain resources Set and monitor milestones Ensure member involvement, contribution and benefits Keep work on track
Characteristics of a Leader - Add Yours

36
In a team situation the leadership must adopt a different approach to management as:
1. Most team members will not have direct reporting/accountability responsibility to the team leader2. They have no compensational control3. Can often have different “experiential” level from members4. Does not have a “boss” authority5. Are also a member of the team
However the leader is critical to team success and must adopt several roles to moderate the team.
Respectful
Clear
Trusting
Knowledgable Goal oriented
Enthusiastic
Supportive
Patient Observant
Assertive
Explore with your Team:What experiences you have had with Leadership? What worked? What didn’t? What changed when you held the leadership role?!
37
Your Notes
Initiator
RoleModel
RelationshipsNegotiator
Coach
Manager
Mediator

38
Planning the Event1. Each team will be provided with a scenario of a event or project they will have to plan2. Each team member will be provided with a envelope with a description of their role in the team –
One person will be the observer 3. Each team member will also be provided with a sticker – you will take the sticker and turn to the
person on your right. Without showing the person the sticker you will place the sticker on their hat/forehead/shoulder.
4. The person receiving the sticker cannot look at what the sticker says but others may view it5. Plan you event (you will have 15 minutes)
Observer:You will note the interactions between the team members and provide your feedbacks to the team at the end of the exercise
Participants:Pay attention to how you feel and perceive you are being treated during the exercise
Communication and Conflict Resolution
Effective Team Communication To provide effective, coordinated services, a team must have an efficient mechanism for exchange of information. At the simplest level, this requires the time, space, and regular opportunity for members to meet and discuss patient cases.
With your group complete the “plan the event” exercise

39
An ideal system for team communication includes:
A well-designed record system. A regularly scheduled forum for members to discuss client issues. A regularly scheduled forum to discuss and evaluate team function and
development, and to address related interpersonal issues. A mechanism for communicating with the external within which the team operates.
Effective communication relies on: Listening, Explaining perceptions, Acknowledging, and discussing the differences and similarities in views, Negotiating agreement.
The group process must integrate: Openness and confrontation, Support and trust, cooperation and conflict, Sound procedures for solving problems and getting things done and good
communication.
Some barriers to effective communication and teamwork include:
Lack of a clearly stated, shared and measurable purpose. Lack of training in interdisciplinary collaboration. Role and leadership ambiguity. Team too large or too small. Team not composed of appropriate professionals. Lack of appropriate mechanisms for timely exchange of information. Time for meetings
The following tips will be helpful for valuing diversity on your team:
Reasonable people can—and do—differ with each other. No two people are the same. Diversity among team members enhances creativity.
Learn as much as you can from others. Learning the various backgrounds, cultures, and professional values of others can enrich your own skills and abilities.
Evaluate a new idea based on its merits. Avoid evaluating ideas based on who submitted them or how closely they mirror your own personal preferences.
Avoid comments and remarks that draw negative attention to a person’s unique characteristics.
Humor is a key factor in a healthy team environment but should never be used at the expense of another’s identity or self-esteem.
Don’t ignore the differences among team members. The differences should be honored and utilized to advance the goals of the team.
People do not need to think the same to be unified. The key to team success is to value the differences on the team and use such diversity to achieve the team’s common purpose.

40
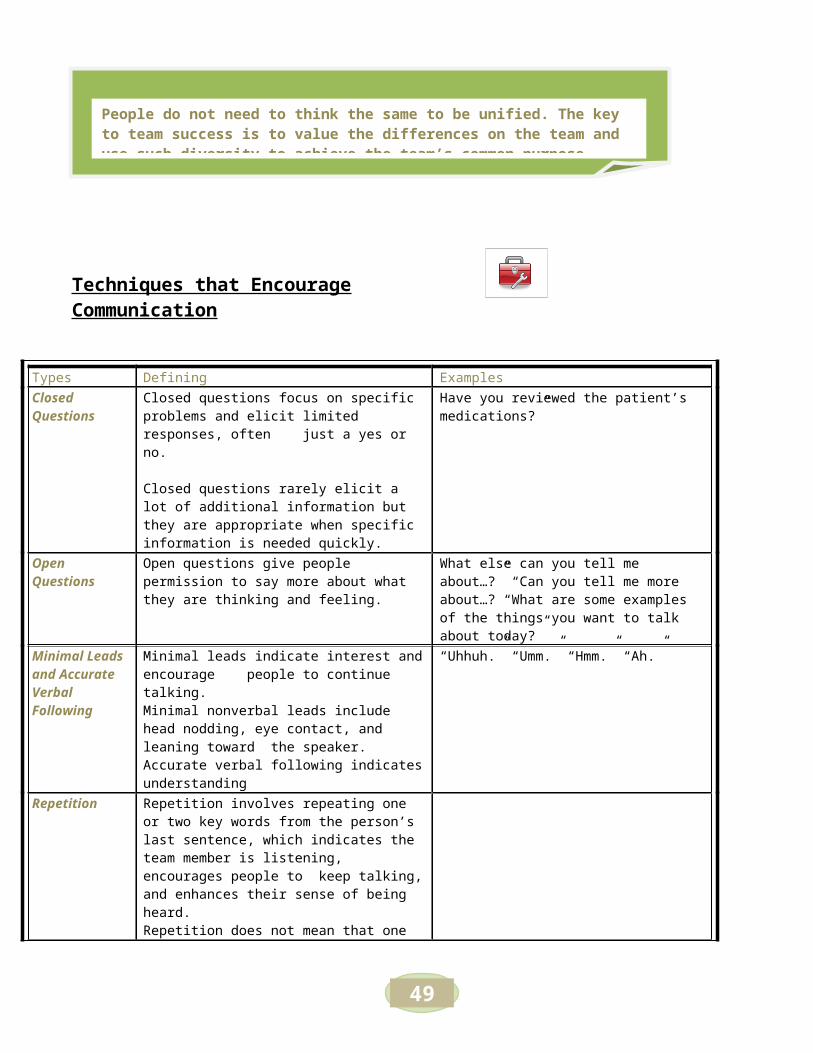
Techniques that Encourage Communication
Types Defining ExamplesClosed Questions
Closed questions focus on specific problems and elicit limited responses, often just a yes or no.
Closed questions rarely elicit a lot of additional information but they are appropriate when specific information is needed quickly.
Have you reviewed the patient’s medications?”
Open Questions
Open questions give people permission to say more about what they are thinking and feeling.
What else can you tell me about…?” “Can you tell me more about…? “What are some examples of the things you want to talk about today?”
Minimal Leads and Accurate Verbal Following
Minimal leads indicate interest and encourage people to continue talking.Minimal nonverbal leads include head nodding, eye contact, and leaning toward the speaker.Accurate verbal following indicates understanding
“Uhhuh.” “Umm.” “Hmm.” “Ah.”
Repetition Repetition involves repeating one or two key words from the person’s last sentence, which indicates the team member is listening, encourages people to keep talking, and enhances their sense of being heard.Repetition does not mean that one agrees with another; it only means the person is listening.Repetition is an important skill, but it should be mixed with other techniques to avoid sounding like a parrot.
Paraphrasing and Reflecting
When people paraphrase and reflect, they repeat a person’s statement in their own words to ensure that the message is understood.
Clarifying Responses
Clarifying responses help people understand the facts and the other person’s feelings and attitudes.
Clarifying responses also help people think about what they have just said, examine their choices, and look at their life patterns.
“Is it possible that you feel…?” “Can you give me an example of what you are talking about?”
Confrontation and Honest Labeling
Confrontation and honest labeling are techniques for gently exploring uncomfortable subjects such as distortions of reality or differences between words and actions. This is not an angry demand that people confront any subject.
“I hear anger in your voice…” or “You sound sad even though you say everything is fine.”
Integrating and Summarizing
Integrating and summarizing help ensure that the main concerns are understood. They help

41
team members clarify their thoughts and feelings and encourage them to further explore confusing and conflicting issues.
Styles of Communication DESTRUCTIVE CONSTRUCTIVE
The Aggressor InitiatorThe Blocker Information SeekerThe Withdrawer Information GiverRecognition Seeker EncouragerTopic Jumper ClarifiersDominator Harmonizers
Devil’s Advocate Gatekeeper
Your Notes
ConflictConflict does not stay private but will spill out into direct and indirect relationships. This will have short and long term ramifications for the team and the clients in some situations conflict can expand to the point of immobilization.
Can change depending on topic , position of power & authority.

42
Team Responsibility
Open to difference & different ways of working Listen to each other “actively” Willing to understand difference of views even if do not agree To question assumptions in a objective depersonalized manner Look for opportunities to collaborate Sharing your skills and knowledge Develop working relationships getting to know at personal and professional (does not
meaning becoming best friends but understanding motivation and context) Being committed and believing in the team and the goals Being a reliable and trustworthy team member Following up on commitments, promises Being prompt and focused on task at hand A team is made up of individuals and personalities with various degrees of needs/wants and
abilities – CONFLICT IS NORMAL and can be HEALTHY
What is identified sits above water
What is real is beneath

43
Conflict needs to be broken down - But maintain a sense of
Control Independence Competent
Inclusion Belonging Consulted
Equality Recognition Heard
Healthy Conflict
Work with more rather than less information sharingDevelop a debate including multiple options, suggestions and opinionsRally around and actively work towards goalsDemonstrates healthy humor in the workplaceIssues discussed and resolved without threat or forced consensusMaintained a team atmosphere and a balanced power structureShared work environmentOther members sharing resources, time, or space to team members who may need …Team not individual focusedA group sharing of creditOne to one settling of differencesDisagreements are de-personalizedUnderstand that you do not have to be “best friends” but respectful
UnHealthy Conflict
Individuals taking a glorified “lime light” and credit for team workOver verbalization – talking overRapid escalation of minor disagreementsDemanding of more resourcesUnwilling to share information Isolation (self or group imposed)Group / peer pressure to conformTeam or individual aggressive behaviorsNegative humor – unproductive criticismsDouble edged comments “underlying” meaning Manipulative behaviors “trying to make others look bad”Environmental changes “office, sitting head of meeting table, office arrangement”Cutting off members Closed door syndrome“not my job attitude”Developing cliquesIntimidationDeflecting – “kitchen sink
Elements That influence Conflict
CollaborationInformation SharingLack of problem solving / decision building skillsDisagreements on priorities Power imbalances (discipline / roles)Differences in communication styleslack of clearly defined expectations – agreements – responsibilities
What Motivates Conflict?

44
Conflict Dynamics and Factors
Roles and Perceptions
We feed the cycle Who we think we are Who we perceive others perceive us Those we fall into Who we want to be
DeservingPerceptionEmotion
Fairness
OptionsChoicesReaction
ValuesPowerStatusProcesses
Authority
VictimAbsolving of responsibilityBlame Game, Not meLooks to others to fixLack of control & power “taken from”?
FixerProtector: Wants to please everyone with the least amount of anxietySelf- proclaimed or ascribed, Power Struggle with the “IP”
IPIdentified ProblemOften a supervisor, stereotype as having controlCommon problem – goal to address.

45
Resistance
Two forms of : 1. Active (Open refusal)2. Passive (Non attendance)
INFLUENCES: RESPONSE: Emotions & Physical
SocializationHABIT – Comfort Zone even chaos can be comfortingHierarchy – “Pecking Order” Hurt when Hurt barriersPower strugglesNattering & Sabotage Insider vs OutsiderControlAssumptions of RoleStatusDiscipline (profession)Stereotype
FEAR of :Fear of the unknownFear of responsibilityFear of failureFear of loss of controlFear of rejectionFear of successFear of changeFear of abandonment
Fight or FlightFreezePassiveSilenceClosed Door SyndromeWithdrawalResistance
Anger, Mistrust, Envy, Fear, Passivity,
RigidityBullyingShakingEye rolling“secret” looksBody Language
Conflict & Styles of practice
Three questions
1. What fears can we do something about?2. What fears are beyond our control?3. How will we let go of the ones out of our
control

46
Conflict is a natural and unavoidable part of human affairs, especially in such groups asCollaborative teams that seek to grow and develop. The various individuals on a team have underlying differences in their modes and methods of practice that affect their relationships with each other, as well as with their clients.
This difference may be characterized by two different styles of practice.
1. One of these is “ruling out” problems by systematically eliminating possibilities until only one problem and a corresponding solution remain. For example, physicians are trained in diagnostic techniques that narrow the range of options, relying heavily on such objective data as laboratory tests in the process.
2. The other approach of “ruling in” problems relies on expanding the range of professional view to encompass an increasingly long list of potential factors. Social workers, on the other hand, are taught to go beyond the narrow presenting problems to view it within larger, encompassing psychosocial issues, such as income, family relationships, and environment.
Other factors that may lead to conflict in team care include Scarce resources and Organizational or professional change that threatens individuals or the overall program.
Each of these types of conflict influences the others, and team leaders will have to determine whether and how to intervene when conflict occurs. Participation on an interdisciplinary team requires individual professionals to relinquish familiar hierarchies and freedoms.
Self-Assessment of ConflictEach individual has a personal way of handling conflict and an important aspect of managing conflict in teamwork is gaining a self-awareness regarding each member’s way of handling differences between themselves and others.
It is also important to ask oneself, “What experiences in my life affect my response to conflict? How do I overcome my ‘natural’ conflict handling style if it is inappropriate in some situations?” Perhaps a team member grew up in a conflictual family and tries to avoid battles at all costs.
Perhaps one thrives on argument. These styles need to be identified and recognized in how they shape the team’s work.
Reflect back to the stages of team development and the influences that affect them Intrapersonal: Interpersonal: Intra-group: Inter-group:

47
Strategies for Preventing, Reducing, and Managing Conflict
Strategies for preventing, reducing, and managing conflict within an interdisciplinary team practice include the use of one or all of the following:
Built-in process to review decisions, including review and definition of goals, the direction of the team, and priorities
Role clarification through the discussion of such topics and knowledge base, professional stereotypes, specializations, autonomy, competencies, responsibilities, and codes of ethics.
Examination of overlapping roles and renegotiation of role assignments. Recognition of professional hierarchies and discussion of their impact on team functioning (status
and delegation of authority issues are a part of this activity). Opportunities for improving inter-professional skills of team members teaching processes for
handling conflict.
“Using Conflict to Promote Interdisciplinary Problem Solving,” identifies various methods and strategies for managing conflict along with the key variable of power. In interdisciplinary teams, there are different sources of internal power (e.g., knowledge or tenure), so some members have more power than others do. Mature teams and team members are able to select the most appropriate conflict-handling style for the situation (Julia & Thompson, 1994).
If I close my eyes it will go away. I will be on vacation ..
LOSE/LEAVE.Avoid
Withdrawing
It is ok - you are ok - I am ok would you like a coffee? YIELD /LOSE
Smoothing
It is ok it was not that important to me I will make do with half the sandwich
NEUTRAL
Compromising
If you don't like it you know what you can do. this is the way it is
WIN/LOSE
Forcing
Lets focus on ... what can make this work for --- What about us
WIN/WIN
Problem Solving
ReflectionWhat is your baggage?
What are your triggers? OR‘He/she knows how to PUSH MY BUTTONS”
Successful resolution of conflict requires the ability to communicate effectively, as well as to confront issues, not people, focusing on the search for win-win solutions.

48
Your Notes
Addressing Conflict
Two approaches in addressing Conflict:
Think BACK to your Team Vision, Rules and Expectations….. DID you include rules on how conflict was to be addressed?
49
Team Discussion:
1. Plan and identify possible “conflict” areas and brain storm solutions with as a team2. Create an environment that supports discussion 3. Encourage discussion that “wants” the tough issues addressed4. Acknowledge issue in an open fact based manner5. Encourage specificity 6. Keep the discussion “de-personalized” 7. Do not assign blame or “point fingers” discuss WHAT not WHO8. Encourage a discussion around the behavior and motivation rather than making assumptions9. Leave the discussion with concrete suggestions, plan for improvement – not everything will have
an immediate solution10. Give space and time to cool down and to enable a sense of control – it may be better to come
back to the discussion.
Private Levels: Encourage members to address conflict at the one to one level Provide format for dealing with conflict procedure/protocol If members engage in public conflict – suggest individuals continue discussion in private “remind
them of the impact on team and clients”
Personal Level:1. Take the emotional temp. of yourself and others2. Defuse3. Separate “venting”4. Put in time and space5. Reflection before action6. Separate the emotion – problem – process
Your Role:
Ask Questions rather than provide answers Assess motivation Focus on the “task” or “concern NOT the individual Trust but Verify Pay Attention “Be present physically and mentally.
Open Team Discussion
Often the starting point
Keep discussion depersonalized
Private / Personal
Discussion
Used for inter-personal conflicts
Can be guided by processess

50
Common Approaches Conflict ResolutionTake the following actions to manage team
Welcome the existence of the conflict, bring it into the open, and use it as potential for change. Separate the person from the problem in an effort to diffuse the emotional component of the
conflict by showing respect, listening carefully, and giving all parties an opportunity to express views.
Clarify the nature of the problem as seen by both parties. Is this the real problem? Deal with one problem at a time, beginning with the easier issues. Listen with understanding (interest) rather than evaluation. Use the communication skills of listening, reflecting, and clarifying. Attack data, facts, assumptions, and conclusions but not individuals (e.g., “I Disagree with your
assumptions”). Brainstorm about possible solutions. Use objective criteria when possible.
o Invent new solutions where both parties gain.o Implement the plan.o Evaluate and review the problem-solving process after implementing the plan.o Identify areas of agreement. Focus on common interests not positions.
Characteristics of Constructive Feedback
Listen
Ask/Clarify
Explore
FocusedChallenge
Agreement
Accountable
The Conflict Meetin

51
Conflict Management TechniquesWorking with Differences
1. Questions to consider:o What creates differences?o What are the underlying factors that cause differences?o How are differences played out?
2. Types of Differences: what people fight over:o Information/factso Goalso Methodso Values
3. Underlying factors that cause differences:o Different personal histories -- experiences that influence mindset.o Varied access -- to same information.o Perceptual differences -- perceptions become one’s reality.o Role factors -- expectations and resources differ.
4. Stages of evolutions of differences:o Anticipation -- know something will happen that will result in a dispute.o Aware -- but unexpressed verbal differences to others.o Discussion -- differences begin to emerge openly during discussions.o Open dispute -- differences are sharpened.o Open conflict -- positions are locked in, often a win-lose mentality. Attempts are
made to undermine the other side.
Positive and Negative
Given with attention to
context and caring
Motivated in a positive way
Invited by the recipient Expressed directly
Expressed fully
Not based on evaluative
judgements
Timely Easily Acted Upon
Private
Checked and clarified

52
5. Transforming conflict into a problem solving situation:o Encourage differences to surface and be expressed.o Listen with understanding rather that evaluation.o Clarify the nature of the conflict.o Recognize and accept feelings of the involved individuals.o Explore who and how the decision will be made.o Discuss ground rules for resolving differences up front.o Attend to the relationship as well as the business.o Create humane vehicles for communicating with others.o Focus on content and processes issued at the same time.o Explore ways to facilitate problem solving
6. Key summary points:o People: separate people from the problem.o Interests: focus on interests not position.o Options: generate possibilities.o Criteria: results based on mutually agreed standards.
7. Some Competencies that influence encounters with difference.o Active listening.o Suspending judgment.o Attack problems not people.o Identify, explore, and use resistance.o Ability to disengage.o Ability to bracket.o Ability to manage emotions.o Ability to depersonalize.o Ability to alter behavior, context, judgments, interfaces, and communication.o Grace in ourselves, faith in others.
8. Mediating differences -- varied roles of a facilitator.o Working through differences involves creating mutuality and respect for opposing
positions and people.o Engaging intense differences requires being adaptive, strong, and emphatic, while
not loosing track of issues and feelings. o Creating common ground involves expressing relational energy in varied ways:
catharsis, catalyst, confronting, prescribing, and supporting.
Role and When to Use

53
Your Notes
Catalyst
Creatively sharing new information (e.g., stories,examples).Helping others to see things in new ways.Exploring alternatives.Organizing data into information.
Catharsis
Provides opportunity to ventilate feelings and common emotions Clarify, restate, paraphrase, and reflect.Develops openness and fruitful trust levels.Lowers tensions and anxiety.
Confrontation
Directly challenging the status quo.Gently but persistently questioning the underlying rationale.Keeping the focus on the conflict. Maintain the tension.Compare critical positions and assessments (yours/theirs).
Prescription
Occurs after assessing/diagnosing the situation.Recommends course of actions or previously discussed options.Ask check out questions: “Does that make sense to you
Conflict Resolution Ideas:
Place conflict within the context of agreements “place the disagreement in perspective”
Separate acceptable and unacceptable solutions Articulate underlying “needs” and “perspectives” Record agreements so they are not forgotten in the discussion Temporary time outs Ongoing check ins on the process Develop a team conflict and/or improvement plan

54
MODULE THREE
Elements that Bring the Team Together
MODULE THREE

55
Table of Contents Pages
Team Meetings ……………………………………………………….. 56-581. Meetings2. Responsibilities3. Facilitator Examples (Chart)4. Facilitating meetings
Team Culture & Ethics ……………………………………………… 591. Professional2. Discipline Power and Hierarchy
Information Sharing & Confidentiality ………………………………. 60-61
Legislation ……………………………………………………………….. 62

56
Team MeetingsAlthough team members work in many situations in which leadership roles and functions can be shared and assumed, a critical arena for effective leadership is the team conference or meeting. Managing the team meeting process in order to achieve the team objectives demands a high level of skill and should not be taken lightly. The team coordinator or facilitator is responsible for moving the team efficiently through the process of the team meeting to make sure that the work of patient care planning is completed. Some teams rotate this leadership responsibility to ensure leadership and the associated tasks are shared.
Meetings
1. Agenda2. Structure3. Action
Clear purpose and goal Define step by step Set time and limits Discuss subject Alternatives Summarize Agree – consensus Action Identify and assign tasks and steps Set for follow up
Responsibilities
Team Leader/Coordinator:
Schedules, arranges, and conducts the meeting. Prepares and distributes agenda before the meeting and ensures that agenda is followed during
the meeting. Clarifies purpose and helps the team identify goals. Ensures that all team functions are assigned to various team members. Encourages everyone to participate throughout the discussion. Summarizes and organizes the ideas discussed to gain commitment (with help of recorder). Identifies common topics or subjects in discussion to maintain direction of discussion. Asks questions to clarify comments and restates if members are confused. Encourages team to finish each agenda item before moving on to the next. Encourages the integration of new members.

57
The Recorder
The Recorder has four major tasks during meetings:
1. Documenting the efforts of the group, including summaries of decisions, action items (or assigned tasks), and deadlines.
2. Maintaining the group’s focus and direction.3. Actively clarifying the group’s progress by using strategies such as summarizing and seeking.4. Producing written summaries.
The Timekeeper:
1. Informing the group of the beginning time and ending time, allowing enough time for the members to begin and come to an end to the discussion.
2. Indicating when the group is using more time than available on one issue and remind them of the number of tasks and time remaining.
3. Helping the team use its time on issues on which the whole team is needed.
Facilitator Roles Dialogue Examples :
Get the meeting started. Today we need to review__ patients/cases/clients. Are there any urgent concerns?”
Encourage communication and involvement of all members.
What are the ________ needs you see?”
Ask team members for opinions and feelings to encourage discussion
What is your view of the family’s request?”
Ask for a summary of the discussion.
What are the care plan goals we have agreed upon? Can someone summarize?”
Paraphrase what someone has said to help members understand each other.
“Are you saying that we need more information on _________?”
Ask for specific examples to improve understanding.
“Please give some examples.”
Clarify assumptions. “Your recommendation assumes that the patient is too confused to make an independent decision.”
Ask for explanation in order to eliminate confusion and repetition
“We keep avoiding a plan for this. Can someone suggest how we should proceed?”
Probe an idea in greater depth. What are other ways to help Mrs. S stay at home.”Suggest a break or rest “Let’s take a brief break.”Move the team toward an action. “What should we do first?”

58
Facilitating Meetings
1) Get the meeting started2) Encourage communication and involvement of all members3) Ask team members for opinions and feelings to encourage discussion4) Ask for a summary of the discussion5) Paraphrase what someone has said to help members understand each other6) Ask for specific examples to improve understanding7) Clarify assumptions8) Ask for explanation in order to eliminate confusion and repetition9) Probe an idea in greater depth10) Suggest a break or a rest11) Move the team toward action12) Poll members13) Encourage open-mindness14) Recommend a process15) Step out of the facilitator role16) Stop discussion to focus on team feelings17) Encourage greater participation18) Reflect for the team what someone else is feeling19) Get back on track20) Surface differences of opinion21) Check team progress22) Encourage new thinking23) Explore potential results24) Test for consensus of the team25) Handle consensus blockers26) Move towards a decision
Your Notes
Agenda focus:1) problem2) planning3) information sharing

59
The Ethics Culture of Team Care
Each of us has a internal set of values, beliefs and expectations. We also belong to various concepts of groups, organizations, communities and affiliations. It is though identifying and developing a sense of belonging with these organizations that we develop a sense of “culture”. Most people have layers of culture each of which are fluid and become prominent depending on the situation.
Service providers are educated within cultures that pass on instructions and assumptions about how services should be provided and who should receive it. It is a constant push and pull struggle in collaborative team work to negotiate the territory between general agreement among the culture of the professionals about goals of care and the specific perspective and what is the best outcome and for each team members contribution to toward that goal. The culture is not just external, it is also an internal task of members of the team, who have to negotiate agreement and disagreement regarding expectations of team members concerning what the person/community/project needs, how it should be provided, and who should provide it.
Professional CulturesEach of the cultures that influences collaborative team development, has its own view of its responsibility toward the individual, project and the community 's responsibility. Much of the energy in teamwork is about the interaction of team members the "shared constraints" of the individual disciplines and the focus of all the disciplines.
Representatives of individual professions frequently have little understanding of the ethical commitments of other professions or of the service that the other professions provide. Cultures of disciplines and professions express some of the constraints that they impose on their members in ethical codes. Codes also establish norms that can protect individuals. A code provides a window on, or a snapshot of, a discipline's view of the situation, and of the discipline's understanding of its responsibility in responding to that situation.
Your Notes
What are Discipline Power and Hierarchy?
List different types of culture that you belong to… ie work culture!What are some of the rules, expectations, group thinks that come along with that culture.

60
Professional Beliefs Each profession has a discipline specific “world view & practice”
o valueso language “acronyms”o problem viewing & solvingo common understanding
Socialization & education Attitudes Hidden curriculum Scopes of practice
Information Sharing and Confidentiality
a) Information that must be shared is:a. Required by law and related policyb. To protect the health, safety, well-being of clients or others
b) Information that should be shared is:a. Information necessary to support continuity of care, ITCP or quality of service
c) Information that should not be shared is:a. Information that is not relevant to the caseb. Information that is not absolutely necessary to assist clients and fulfil job requirements
Discussion Questions:
Confidentiality: Personal Reflection Questions
What is your reference point for making that decision (i.e. organizational policy, legislation, relationship with family or other service providers, etc.)?
How would the task of creating a joint plan affect information sharing? How did people decide with whom they would share information or how much they were willing to share? Did it have anything to do with the relationships people had with one other? With families and individuals? Did it have anything to do with personal beliefs, values ethics, or legislation?

61
Legislation, Policies and Principles Influencing Collaborative Team work
What are my personal beliefs
regarding confidentuality?
How does the inclusion of families, communities impact confidentuality?
Who owns the material I may gather?
Who do I owe a responsibility of confidentuaility?
What does my professional code of
ethics say about confidentuality?
How do I incorporate all of the personal, professional and
organizational requirements into ethical practice?
What is my understanding of "need
to Know?
What are the organization's requirements
around confidentuality?
Do the requirements presents ethical
dilemmas or challanges that impact my sharing
of information?
Where do I establish my loyality ?

62
Ethics BoardTRI PARTICanada Health ActCanada Information and Privacy ActsIndian ActCharter of Rights and Freedoms
Health Care (Consent) & Care Facility Admissions Act (HCCCFAA) Adult Guardianship ActChild, Family and Community Services ActFirst Peoples’ Heritage, Language and Culture ActFreedom of Information and Protection of Privacy (FOIPPA)Health Act & AmendmentsMental Health ActVenereal DiseasesHealth Professional ActHealth and Social Services Delivery Improvement ActHuman Rights CodePersonal Information Protection ActPatients Property Act
Professional Practice StandardsProfessional Ethics StandardsUnion Codes and Standards (Collective Agreements)
Individual Agency Mandates and DirectivesRespect in the Workplace Policy
References

63
Drinka & Clark (2000). Health Care Teamwork: interdisciplinary practice and teaching. Westport, CT Auburn House Publishing.
Farrell, M. P.; Schmitt, M.H. & Heinemann, G. D. (2001) Informal roles and the stages of interdisciplinary team development. Journal of Interprofessional Care, Vol 15, NO. 3, 2001 Carafax Publishing
Gilbert, J., & Bainbridge, L. (2001). Interprofessional Education and Collaboration: Theoretical Challenges, Practical Solutions.
Heinemann, G. D., & Zeiss, A. M., (2002). Team performance in health care: Assessment and development. New York: Kluwer Academic/Plenum. MCFD, 1997
Meads, G., Ashcroft, J., Barr, H., Scott, R., & Wild, A. (2005). The case for Interprofessional collaboration: In health and social care. Oxford, UK: Blackwell.
Vancouver Coastal Health, 2006).
Way, D, Jones, L., & Baskerville, N.B. (2001). Improving the effectiveness of primary health care through nurse practitioner/family physician structured collaborative practice. University of Ottawa.
Julia & Thompson, 1994