modifying parental smoking habits – why and how?
TRANSCRIPT

PERSONAL PRACTICE
Modifying parental smokinghabits e why and how?Steve Turner
Chest infections
Asthma
Ear infections
Re
spo
nd
en
ts a
gre
ein
g t
ha
t E
TS
ex
po
sure
incr
ea
sed
a c
hil
d’s
ris
k f
or
illn
ess
(%
)
100
75
50
25
0
Introduction
Exposure to second hand smoke (SHS) is associated with several
adverse health outcomes in children. Removing children from
SHS exposure is a priority shared by policy makers and health-
care professionals alike. In addition to the burden of childhood
illnesses, the children of parents who smoke are also at increased
risk for becoming smokers in adulthood and this puts the young
individual at increased risk for conditions likely to shorten their
life span, e.g. malignancies, myocardial infarction, chronic
obstructive pulmonary disease and stroke. Parents love their
children and endeavour to provide a safe and healthy environ-
ment for their offspring and smokers know that SHS exposure is
harmful to children (Figure 1) but approximately 40% of children
in the UK continue to be exposed to SHS by their parents.
Exposure of children to SHS is an issue involving a complex
blend of addiction, social pressures and health outcomes. The
aims of this review are (i) to provide clinicians with an up-to-date
brief of what is known about modifying children’s exposure to
SHS, (ii) a summary of what remains to be understood about SHS
exposure and (iii) to provide clinicians with practical advice on
approaching parent who smoke.
What is known about parental smoking?
Approximately three quarters of mothers who smoke and have
children who attend hospital have tried to quit in the past and
a similar proportion is either contemplating or prepared to quit.
Smoking mothers are up to six times more likely to have
a partner who smokes compared to non-smoking mothers and
therefore interventions aimed at reducing SHS should be directed
beyond the child’s mother. One study found evidence to suggest
that having an ill child in hospital presented a “teachable
moment” where by parents are more likely to quit, but this has
not been replicated elsewhere. Coming to hospital with an ill
child is a stressful business and might be exactly the wrong time
to raise the subject of cessation, and this has been our anecdotal
experience. Having completed a semi-qualitative/epidemiolog-
ical study we saw that many parents who smoked were prepared
to quit and expressed an interest in smoking cessation. We were
heartened by this and undertook a feasibility study to recruit
parents attending hospital outpatients onto a smoking cessation
programme; of the 250 parents approached, 80 were smokers
Steve Turner MD MRCP FRCPCH is a Senior Lecturer in Child Health at the
University of Aberdeen School of Medicine and the Department of Child
Health, Royal Aberdeen Children’s Hospital, Foresthill, Aberdeen AB25
2ZG, UK. Conflict of interest: none.
PAEDIATRICS AND CHILD HEALTH 20:9 447
and of these only one was enrolled. Engaging parents in smoking
cessation in the child health setting is a big challenge and
perhaps should be done at home rather than in the hospital
setting.
What remains to be understood
In a perfect world
In a perfect world, the interventions which are effective in adults
who wish to quit smoking would be effective parents (who are
adults after all) but life is rarely straightforward! The brief
interventions which are effective in changing smoking behav-
iour, for example handing out an information leaflet, are not
effective when given to parents in the child health setting. In
a randomized control trial on Tayside, parents of 500 children
were given a brief intervention, warned of the harmful effects
of passive smoke exposure on children and followed up after
12 months. On review, 98% of parents continued smoking, the
children’s SHS exposure (urinary cotinine) was unchanged
between the intervention and control groups and the authors
suggest that the brief intervention might even have entrenched
smoking habits in some parents. A second randomized controlled
trial, also of almost 500 parents, involved a brief intervention in
the form of a 15 min interview but this did not alter quit rates or
daily cigarette consumption. A recent Cochrane review identified
36 intervention studies aimed at reducing children’s SHS expo-
sure, including 19 studies from the USA where the findings may
not necessarily be transferable to the UK. In only 11 studies did
the intervention reduce SHS exposure of children compared to
controls; often SHS exposure was reduced in both groups. The
more successful studies tended to include intensive counselling,
for example three 45 min interviews and four follow-up tele-
phone calls. One American study where parents were random-
ized to receive seven counselling sessions over 3 months
reported a 50% reduction in urinary cotinine 12 months after
entering the study; importantly this study changed the children’s
Non-
smokers
Ex-
smokers
‹ 20
cigarettes/
day
› 20
cigarettes/
day
Figure 1 The proportion of adults who agree that environmental tobacco
smoke (ETS) exposure is a risk for children’s chest infections, asthma and
ear infections. Figure made from raw published data.
� 2010 Elsevier Ltd. All rights reserved.

Smoking behaviours which do not reduce children’s
PERSONAL PRACTICE
SHS exposure by modifying mother’s smoking practices but not
by significantly altering the mother’s own cotinine.
exposure to second hand smoke3
Idealism versus pragmatism
� Opening windows or doors
� Smoking less
� Not smoking in front of the children
� Smoking in different rooms
� Smoking out of the window
� Smoking outside in front of an open door
� Smoking under the kitchen extractor fan
� Air purifiers
Table 2
Whilst idealists might focus on motivating parents to quit
smoking, pragmatists might argue that in the child health setting
the focus should be reducing the child’s SHS exposure by
whatever means. One method for reducing children’s SHS
exposure is to introducing a smoke-free home, i.e. all residents
and visitors do not smoke in the house, but these can be difficult
to establish (Table 1). Smoke-free homes are becoming more
acceptable in the UK where the proportion rose from 21% to 37%
between 1996 and 2007. Importantly, smoke-free homes are
effective in reducing children’s SHS exposure (Figure 2) and can
be introduced as part of an acceptable change in behaviour.
Many households continue to permit smoking indoors but
restrict this activity to certain rooms but this behaviour does not
reduce children’s SHS exposure (also see Table 2). Whereas SHS
exposure in the home is usually chronic but relatively low, SHS
exposure in cars can be brief but relatively high and introducing
a smoke-free car may also reduce SHS exposure, although the
evidence for this is lacking. What is known is that SHS exposure
in cars can be unsafe for children. In summary, what is known is
that children’s SHS exposure can be reduced and this requires
fairly intensive counselling but not necessarily parents quitting.
What is not known about second hand smoke exposure?
Although the presumption is that SHS is harmful to children,
supportive evidence can only arise from intervention studies and
there are surprisingly little data upon which to promote SHS
avoidance. In fact, at the time of writing, there are only two
published studies (both from USA) which have reported the
impact of reduced SHS exposure on children’s health. In the first
study, parents of 87 asthmatic children were randomized to
receive standard asthma education or standard education plus
three smoking counselling sessions (including a video titled
“Poisoning Our Children”); over the following 12 months, the
enhanced intervention was associated with reduced visits to the
doctor or hospital with acute asthma. The enhanced intervention
was not associated with a significant reduced SHS exposure, as
evidence by urinary cotinine, but the study was underpowered to
detect a difference. In the second study, 133 mothers who
smoked and who had asthmatic children were randomized to
receive either smoking cessation advice or advice which focused
on the child’s risk from SHS (including giving mothers their
child’s measured nicotine exposure). Both arms of the study
received three interviews at home and a 5e10 min follow-up
Factors that might prevent mothers from introducingsmoke-free homes
� Partner, relations (e.g. grandparents) and visitors continue to
smoke indoors
� Inability to leave child unsupervised while smoking outside
� It can be cold and wet when smoking outside
� Addiction to tobacco
Table 1
PAEDIATRICS AND CHILD HEALTH 20:9 448
telephone consultation. The children’s nicotine exposure fell five
fold in those whose mothers were given smoking cessation
advice and by only 20% in the other group. Children’s asthma
symptoms improved significantly in both groups although at the
end of the study, somewhat surprisingly, only those children
whose mothers were given risk reduction advise had less asthma
symptoms. This study perhaps asks more questions than it
answers but it suggests that an intervention which takes place in
the home (and not hospital), which focuses on the child’s
exposure (and not mother quitting) and where biofeedback (e.g.
nicotine) may be effective in improving children’s health. There
is indirect evidence that reduced SHS exposure yields health
benefits for children provided by studies in pregnant women
where smoking cessation interventions are associated with
increased birth weight. Despite the absence of overwhelming
evidence, the precautionary principle* empowers policy makers
and clinicians to tell parents that SHS exposure is harmful.
What is a safe exposure?
The exposureeresponse relationship between SHS and child
health is also not described but evidence from studies of foetuses
and adults with cardiovascular disease suggests that the relation-
ship is not linear and passes through zero (Figure 3). The rela-
tionship between birth weight and maternal daily cigarette intake
is linear below five to eight cigarettes and flattens out thereafter. A
similar relationship is described for adult cardiovascular risk and
indoor air pollution, where SHS is a major contributor. The prac-
tical relevance of these observations is that reducing SHS exposure
from a high to intermediate value may not translate into greatly
reduced child health outcomes (Figure 3); there is almost certainly
no safe level of SHS exposure.
In the future, what is needed is (i) a better understanding of
how to engage parents in reducing their child’s SHS exposure and
(ii) a better understanding of the exposureeresponse slope
between SHS and health outcomes.
* Where an action or policy has suspected risk of causing harm to the
public or to the environment, in the absence of a scientific consensus that
harm would not ensue, the burden of proof falls on those who would
advocate taking the action.
� 2010 Elsevier Ltd. All rights reserved.
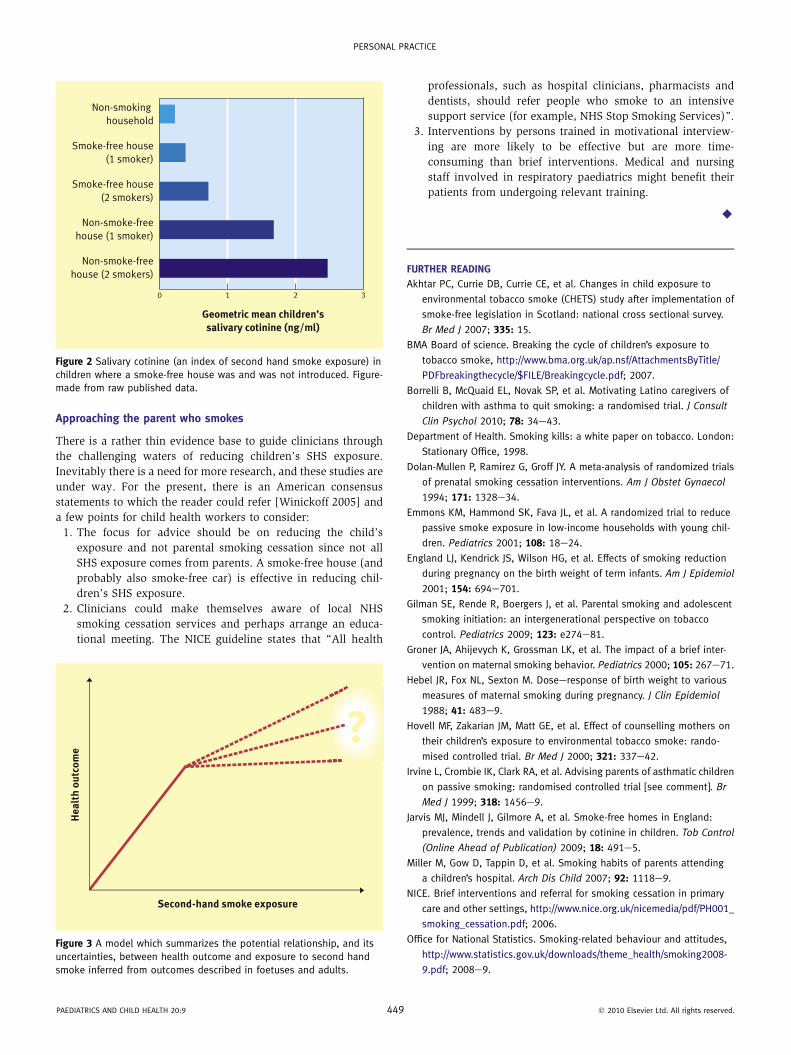
Geometric mean children’ssalivary cotinine (ng/ml)
Non-smoking
household
Smoke-free house
(1 smoker)
Smoke-free house
(2 smokers)
Non-smoke-free
house (1 smoker)
Non-smoke-free
house (2 smokers)
0 1 2 3
Figure 2 Salivary cotinine (an index of second hand smoke exposure) in
children where a smoke-free house was and was not introduced. Figure-
made from raw published data.
PERSONAL PRACTICE
Approaching the parent who smokes
There is a rather thin evidence base to guide clinicians through
the challenging waters of reducing children’s SHS exposure.
Inevitably there is a need for more research, and these studies are
under way. For the present, there is an American consensus
statements to which the reader could refer [Winickoff 2005] and
a few points for child health workers to consider:
1. The focus for advice should be on reducing the child’s
exposure and not parental smoking cessation since not all
SHS exposure comes from parents. A smoke-free house (and
probably also smoke-free car) is effective in reducing chil-
dren’s SHS exposure.
2. Clinicians could make themselves aware of local NHS
smoking cessation services and perhaps arrange an educa-
tional meeting. The NICE guideline states that “All health
He
alt
h o
utc
om
e
Second-hand smoke exposure
Figure 3 A model which summarizes the potential relationship, and its
uncertainties, between health outcome and exposure to second hand
smoke inferred from outcomes described in foetuses and adults.
PAEDIATRICS AND CHILD HEALTH 20:9 449
professionals, such as hospital clinicians, pharmacists and
dentists, should refer people who smoke to an intensive
support service (for example, NHS Stop Smoking Services)”.
3. Interventions by persons trained in motivational interview-
ing are more likely to be effective but are more time-
consuming than brief interventions. Medical and nursing
staff involved in respiratory paediatrics might benefit their
patients from undergoing relevant training.
A
FURTHER READING
Akhtar PC, Currie DB, Currie CE, et al. Changes in child exposure to
environmental tobacco smoke (CHETS) study after implementation of
smoke-free legislation in Scotland: national cross sectional survey.
Br Med J 2007; 335: 15.
BMA Board of science. Breaking the cycle of children’s exposure to
tobacco smoke, http://www.bma.org.uk/ap.nsf/AttachmentsByTitle/
PDFbreakingthecycle/$FILE/Breakingcycle.pdf; 2007.
Borrelli B, McQuaid EL, Novak SP, et al. Motivating Latino caregivers of
children with asthma to quit smoking: a randomised trial. J Consult
Clin Psychol 2010; 78: 34e43.
Department of Health. Smoking kills: a white paper on tobacco. London:
Stationary Office, 1998.
Dolan-Mullen P, Ramirez G, Groff JY. A meta-analysis of randomized trials
of prenatal smoking cessation interventions. Am J Obstet Gynaecol
1994; 171: 1328e34.
Emmons KM, Hammond SK, Fava JL, et al. A randomized trial to reduce
passive smoke exposure in low-income households with young chil-
dren. Pediatrics 2001; 108: 18e24.
England LJ, Kendrick JS, Wilson HG, et al. Effects of smoking reduction
during pregnancy on the birth weight of term infants. Am J Epidemiol
2001; 154: 694e701.
Gilman SE, Rende R, Boergers J, et al. Parental smoking and adolescent
smoking initiation: an intergenerational perspective on tobacco
control. Pediatrics 2009; 123: e274e81.
Groner JA, Ahijevych K, Grossman LK, et al. The impact of a brief inter-
vention on maternal smoking behavior. Pediatrics 2000; 105: 267e71.
Hebel JR, Fox NL, Sexton M. Doseeresponse of birth weight to various
measures of maternal smoking during pregnancy. J Clin Epidemiol
1988; 41: 483e9.
Hovell MF, Zakarian JM, Matt GE, et al. Effect of counselling mothers on
their children’s exposure to environmental tobacco smoke: rando-
mised controlled trial. Br Med J 2000; 321: 337e42.
Irvine L, Crombie IK, Clark RA, et al. Advising parents of asthmatic children
on passive smoking: randomised controlled trial [see comment]. Br
Med J 1999; 318: 1456e9.
Jarvis MJ, Mindell J, Gilmore A, et al. Smoke-free homes in England:
prevalence, trends and validation by cotinine in children. Tob Control
(Online Ahead of Publication) 2009; 18: 491e5.
Miller M, Gow D, Tappin D, et al. Smoking habits of parents attending
a children’s hospital. Arch Dis Child 2007; 92: 1118e9.
NICE. Brief interventions and referral for smoking cessation in primary
care and other settings, http://www.nice.org.uk/nicemedia/pdf/PH001_
smoking_cessation.pdf; 2006.
Office for National Statistics. Smoking-related behaviour and attitudes,
http://www.statistics.gov.uk/downloads/theme_health/smoking2008-
9.pdf; 2008e9.
� 2010 Elsevier Ltd. All rights reserved.

Practice points for reducing children’s second handsmoke exposure
� Preventing exposure is probably the single most effective
method of improving a child’s health in the short, medium and
long term.
� The focus should be on reducing the child’s exposure and not
primarily parents quitting.
� Clinicians should be more aware of local smoking cessation
services.
� Brief, single interventions are less successful in changing
parents smoking behaviour compared with a series of meet-
ings between parent and trained advisor.
PERSONAL PRACTICE
Phillips R, Amos A, Ritchie D, et al. Smoking in the home after the smoke-
free legislation in Scotland: qualitative study. Br Med J 2007; 335: 15.
Pope 3rd CA, Burnett RT, Krewski D, et al. Cardiovascular mortality and
exposure to airborne fine particulate matter and cigarette smoke:
shape of the exposureeresponse relationship. Circulation 2009; 120:
941e8.
Priest N, Roseby R, Waters E, et al. Family and carer smoking control
programmes for reducing children’s exposure to environmental
tobacco smoke. Cochrane Database Syst Rev 2008; 4.
Roseby R, Waters E, Polnay A, et al. Family and carer smoking control
programmes for reducing children’s exposure to environmental
tobacco smoke. Cochrane Database Syst Rev 2003; 3.
Spencer N, Blackburn C, Bonas S, et al. Parent reported home smoking
bans and toddler (18e30 month) smoke exposure: a cross-sectional
survey. Arch Dis Child 2005; 90: 670e4.
Strachan DP, Cook DG. Health effects of passive smoking. 1. Parental
smoking and lower respiratory illness in infancy and early childhood.
Thorax 1997; 52: 905e14.
Wilson SR, Yamada EG, Sudhakar R, et al. A controlled trial of an envi-
ronmental tobacco smoke reduction intervention in low-income chil-
dren with asthma. Chest 2001; 120: 1709e22.
Winickoff JP, Hibberd PL, Case B, et al. Child hospitalization: an oppor-
tunity for parental smoking intervention. Am J Prev Med 2001; 21:
218e20.
PAEDIATRICS AND CHILD HEALTH 20:9 450
Winickoff JP, Hillis VJ, Palfrey JS, et al. A smoking cessation intervention
for parents of children who are hospitalized for respiratory illness: the
Stop tobacco outreach program. Pediatrics 2003; 111: 140e5.
Winickoff JP, Berkowitz AB, Brooks K, et al. State-of-the-art interventions
for office-based parental tobacco control. Pediatrics 2005; 115:
750e60.
� 2010 Elsevier Ltd. All rights reserved.