modifications of the impression to prevent cast breakage
TRANSCRIPT

Modifications of the impression to prevent cast breakage
Marty G. Moon, DDS," and Robert G. Holmes, DMD b Bernheim Dental Clinic, Fort Benning, Ga.
Broken teeth on a diagnostic or master cast, which usually occurs during separation from the impression, is a common Problem experienced by dentists. This article aids in diagnosing and modifying noncritical areas of the impression to prevent this problem. One advantage of this method is that casts of periodontally involved teeth can be prevented from breaking. Disadvantages include time involved in modification and loss o f noncritical areas of the tooth, (J Prosthet Dent 1997;77:323-5.)
A common problem experienced by many den- tists is a broken tooth or teeth on a diagnostic or master cast. Most tooth breakage occurs during the separation of the impression from the cast. This can be due to a poor removal procedure, improper clinical or technical use o f dental materials, or improper clinical diagnosis. Manufacturer 's instruction sheets, refereed dental jour- nals, and dental textbooks ~ provide excellent informa- tion for proper removal procedures, use o f dental mate- rials, and clinical diagnosis.
The purpose of this article is to aid in the clinical di- agnosis and modification of the impression to prevent tooth breakage.
D I A G N O S I S
Maldng a successful impression starts in the dental chair when the patient arrives for the initial examination ap- pointment. During the intraoral examination of soft and hard tissues, the dentist should mentally diagnose the steps of the treatment plan. Careful consideration should be given to the patient and oral factors that have a major influence on the type of impression material used. Mal<- ing impressions of patients with thin teeth (mandibular incisors), supraerupted teeth, malpositioned and rotated teeth, periodontally involved teeth with gingival reces- sion, exposed roots, soft tissue undercuts, tori, or a lone- standing single tooth presents difficult challenges.
Ident i fy critical and noncri t ica l surfaces
Before modifying the impression to prevent brealdng teeth on the cast, several things should be considered, such as critical and noncritical tooth surfaces, soft tissue surfaces, impression material, and gypsum product char- acteristics.
Identify the critical and noncritical surfaces before
The opinions contained herein are those of the authors and not to be construed as those of the U.S. Army or the Department of Defense.
~Major(P), U.S. Army, DC, Chief, Prosthodontics, Bernheim Dental Clinic.
bCivilian contractor, General Dentistry Section, Bernheim Dental Clinic.
making the impression. A critical surface is the surface of a tooth or soft tissue that is critical in diagnosing, fabrica- tion, or wearing the prosthesis. A noncritical surface is one that will not be used in the diagnosis or fabrication of the prosthesis. For example, when a cast crown is made for the mandibular left first molar, the occluding surfaces of the opposing teeth (critical surfaces) are needed but the gingival, interproximal, lingual, or fadal surfaces (non- critical surfaces) of the opposing teeth are not.
Severe tooth or soft tissue undercuts of the opposing arch that are noncritical surfaces can be blocked out intraorally 2 or can be modified. When the surfaces are critical, they must not be blocked out in the mouth, but the impression can be modified for success.
Select ing the impress ion material
The impression material characteristics play a major role in preventing tooth breakage. Construction of the gypsum cast requires a lmowledge of the impression material. Some types of inelastic impression materials are thermoplastic (such as impression modeling com- pound) and the impression and cast may be immersed in warm water until the impression modeling compound softens sufficiently to permit easy separation. 3
Other inelastic impression materials such as zinc ox- ide-eugenol can be poured up in the usual manner be- cause they are usually used as washes. Some stiff elastic materials such as polyethers can be difficult to remove from the gypsum cast if hard or soft tissue undercuts are present. Other elastic materials such as reversible or ir- reversible hydrocolloids are easy to separate from a gyp- sum cast if they are separated at the appropriate time under the right conditions. 4'5
Select ing a gypsum produc t
The criteria for the selection of any gypsum product depend on its intended use and characteristics. The use of a dental plaster is more economical than a dental stone. Dental plaster is a better impression-registration material than dental stone is. However, after 1 hour of setting, dental stone has a much greater compressive strength than dental piaster does (3000 to 7000 versus 1300 psi).
MARCH 1997 THE JOURNAL OF PROSTHETIC DENTISTRY 323
THE JOURNAL OF PROSTHETIC DENTISTRY M O O N AND HOLMES
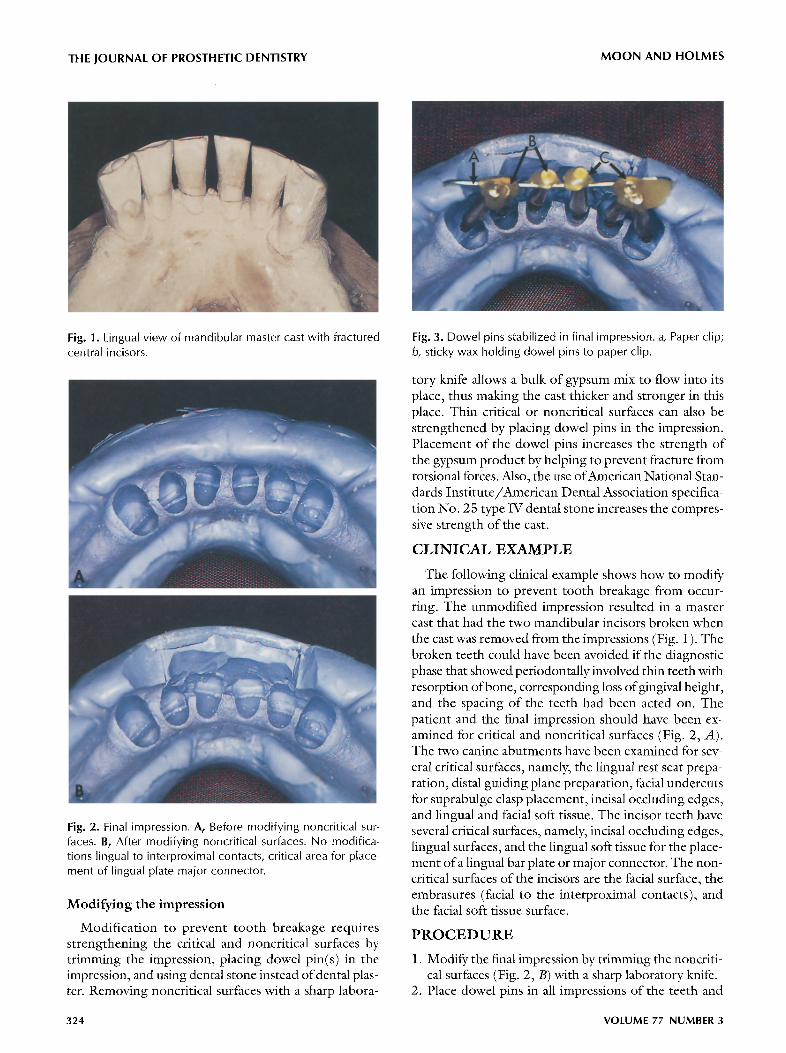
Fig. 1. Lingual view of mandibular master cast with fractured central incisors.
Fig. 2. Final impression. A, Before modifying noncritical sur- faces. B, After modifying noncritical surfaces. No modifica- tions lingual to interproximal contacts, critical area for place- ment of lingual plate major connector.
Modifying the impression
Modification to prevent tooth breakage requires strengthening the critical and noncritical surfaces by trimming the impression, placing dowel pin(s) in the impression, and using dental stone instead of dental plas- ter. Removing noncritical surfaces with a sharp labora-
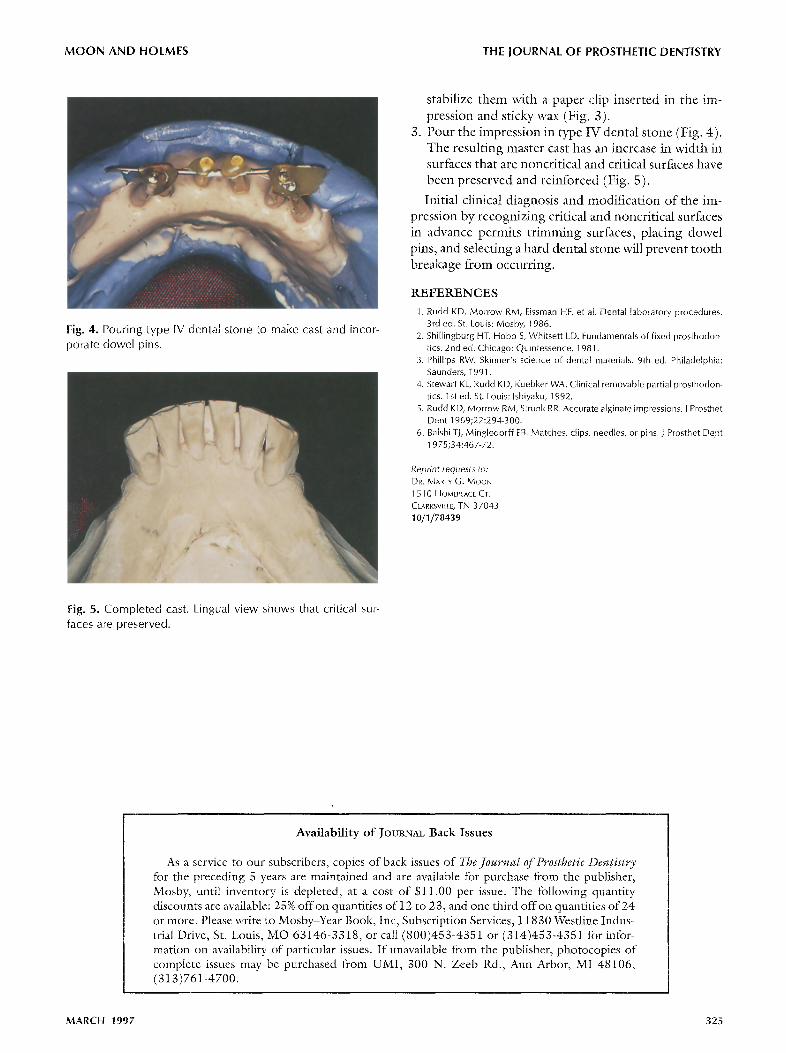
Fig. 3. Dowel pins stabilized in final impression, a, Paper clip; b, sticky wax holding dowel pins to paper clip.
tory knife allows a bulk of gypsum mix to flow into its place, thus maldng the cast thicker and stronger in this place. Thin critical or noncritical surfaces can also be strengthened by placing dowel pins in the impression. Placement of the dowel pins increases the strength of the gypsum product by helping to prevent fracture from torsional forces. Mso, the use of Amcrican National Stan- dards Institute/American Dental Association specifica- tion No. 25 type IV dental stone increases the compres- sive strength of the cast.
C L I N I C A L E X A M P L E
The following clinical example shows how to modify an impression to prevent tooth breakage from occur- ring. The unmodified imprcssion resulted in a master cast that had the two mandibular incisors broken when the cast was removed from the impressions (Fig. 1). The broken teeth could have been avoided if the diagnostic phase that showed periodontally involved thin teeth with resorption of bone, corresponding loss of gingival height, and the spacing of the teeth had been acted on. The patient and the final impression should have been ex- amined for critical and noncritical surfaces (Fig. 2, A). The two canine abuunents have been examined for sev- eral critical surfaces, namely, the lingual rest seat prepa- ration, distal guiding plane preparation, facial undercuts for suprabulge clasp placement, incisal occluding edges, and lingual and facial soft tissue. The incisor teeth have several critical surfaces, namely, incisal occluding edges, lingual surfaces, and the lingual soft tissue for the place- ment of a lingual bar plate or major connector. The non- critical surfaces of the incisors are the facial surface, the embrasures (facial to the interproximal contacts), and the facial soft tissue surface.
P R O C E D U R E
1. Modify the final impression by trimming the noncriti- cal surfaces (Fig. 2, B) with a sharp laboratory knife.
2. Place dowel pins in all impressions of the teeth and
324 VOLUME 77 NUMBER3
M O O N AND HOLMES THE JOURNAL OF PROSTHETIC DENTISTRY
Fig. 4. Pouring type IV dental stone to make cast and incor- porate dowel pins.
stabilize them with a paper clip inserted in the im- pression and sticky wax (Fig. 3).
3. Pour the impression in type IV dental stone (Fig. 4). The resulting master cast has an increase in width in surfaces that are noncritical and critical surfaces have been preserved and reinforced (Fig. 5).
Initial clinical diagnosis and modification of the im- pression by recognizing critical and noncritical surfaces in advance permits t r imming surfaces, placing dowel pins, and selecting a hard dental stone will prevent tooth breakage from occurring.
REFERENCES
1. Rudd KD, Morrow RM, Eissman HF, et a[. Dental laboratory procedures. 3rd ed. St. Louis: Mosby, 1986.
2. Shi[lingburg HT, Hobo S, Whitsett LD. Fundamentals of fixed prosthodon- tics. 2nd ed. Chicago: Quintessence, 1981.
3. Phillips RW. Skinner's science of dental materials. 9th ed. Philadelphia: Saunders, 1991.
4. Stewart KL, Rudd KD, Kuebker WA. Clinical removable partial prosthodon- tics. 1st ed. St. Louis: Ishiyaku, 1992.
5. Rudd KD, Morrow RM, Strunk RR. Accurate alginate impressions. J Prosthet Dent 1969;22:294-300.
6. Ba[shi TJ, Mingledorff EB. Matches, dips, needles, or pins. J Prosthet Dent 1975;34:467-72.
Reprint requests to: DR. /kg~ARTY G. MOON 1510 HOMEPLACE CT. CLARKSVlLLE, TN 37043 10/1/78439
Fig. 5. Completed cast. Lingual view shows that critical sur- faces are preserved.
Availability o f JotJm-~a~ Back Issues
As a service to our subscribers, copies of back issues of The Journal of Prosthetic Dentistry for the preceding 5 )rears are maintained and are available for purchase from the publisher, Mosby, until inventory is depleted, at a cost of $11.00 per issue. The following quantity discounts are available: 25% offon quantities of 12 to 23, and one third offon quantities of 24 or more. Please write to Mosby-Year Book, Inc, Subscription Services, 11830 Westline Indus- trial Drive, St. Louis, MO 63146-3318, or call (800)453-4351 or (314)453-4351 for infor- mation on availability of particular issues. If unavailable from the publisher, photocopies of complete issues may be purchased fi-om UMI, 300 N. Zeeb Rd., Ann Arbor, MI 48106, (313)761-4700.
MARCH 1997 325