moderated by: amy hansen, m.a., ccc-slp, managing...
TRANSCRIPT

7/7/2011
1
Updating Evidence Against NSOME for Speech Sound Production
PPresenter:Gregory Lof, Ph.D., CCC-SLP
Moderated by:
Amy Hansen, M.A., CCC-SLP, Managing Editor, SpeechPathology.com
Live Expert eSeminar
ATTENTION! SOUND CHECK!Unable to hear anything at this time?Please contact Speech Pathology for technical support at 800 242 5183800 242 5183
TECHNICAL SUPPORTNeed technical support during event?Please contact Speech Pathology for technical support at 800 242 5183 ORSubmit a question using the Q&A Pod - please include your phone number.
Earning CEUsEARNING CEUS•Must be logged in for full time requirement•Must pass 10-question multiple-choice exam
Post event email within 24 hours regarding the CEU exam Post-event email within 24 hours regarding the CEU exam ([email protected])
•Log in to your account and go to Pending Courses under the Continuing Education tab.
•The test for the Live Event will be available after attendance records have been processed, approximately 1 hour after the event ends•Must pass exam within 7 days of today•Two opportunities to pass the exam
Peer Review Process
Interested in Becoming a Peer Reviewer?
APPLY TODAY!
3+ years SLP Professional Experience Required
Contact: Amy Natho [email protected]
Sending Questions
Type question or Type question or comment and click the send button
Download Handouts
Cli k t hi hli ht Click to highlight handout
Click Save to My Computer

7/7/2011
2
Updating Evidence Against Updating Evidence Against Nonspeech Oral Motor Exercises Nonspeech Oral Motor Exercises
(NSOME) for Speech Sound (NSOME) for Speech Sound ProductionsProductions
Gregory L. Lof, PhD, CCC-SLPDepartment Chair/Professor
July, 2011
Boston, MA
A special thanks to…
Dr Maggie WatsonDr. Maggie WatsonUniversity of Wisconsin-
Stevens Point
Why not Nonspeech Oral Motor Exercises (NSOME) to change(NSOME) to change
speech sound productions?
• Do SLPs routinely use oral motor exercises?
• Why do SLPs use them?
Are SLPs using Evidence Based
Practice?
Some Practical Questions About Oral Motor Exercises
• What exercises do SLPs use?• What proof do SLPs have that they
are effective in bringing about changes in speech-sound productions?
Practice
Outline of Talk
Trends (using survey data)
Logical Reasons
Not to Use
Outline of Talk
Not to Use
Oral Motor
Exercises

7/7/2011
3
Theoretical Reasons
Not to Use
Outline of Talk
Not to Use
Oral Motor
Exercises
Evidence Why
Not to Use
Outline of Talk
Not to Use
Oral Motor
Exercises
Nonspeech Oral
Definitions
p
Motor Exercises
Any technique that does not require the child to produce
Nonspeech Oral Motor Exercises Defined
q pa speech sound but is used
to influence the development of speaking abilities.
Lof & Watson (2008)
A collection of nonspeech methods and procedures that are purported
to influence tongue lip and jaw
Nonspeech Oral Motor Exercises Defined
to influence tongue, lip, and jaw resting postures, increase strength,
improve muscle tone, facilitate range of motion, and develop
muscle control.(Ruscello, 2008)
Oral-motor exercises (OMEs) are nonspeech activities that involve sensory stimulation to or
actions of the lips, jaw, tongue, soft palate, larynx, and respiratory muscles which are intended to
Nonspeech Oral Motor Exercises Defined
and respiratory muscles which are intended to influence the physiologic underpinnings of the
oropharyngeal mechanism and thus improve its functions. They include active muscle exercise,
muscle stretching, passive exercise, and sensory stimulation.
McCauley, Strand, Lof, et al. (2009)

7/7/2011
4
Note that I will be talking about procedures and techniques that
Nonspeech Oral Motor Exercises Defined
do not use speech.
NSOMENSOME
Not about: Not about: feeding, swallowing, droolingfeeding, swallowing, drooling
Nonspeech Oral Motor Exercises Defined
g g gg g g
S p e e c h
Do SLPs Use NSOME?
Nationwide Survey
Do SLPs Use NSOME?
Lof & Watson (2008)
Nationwide survey of 537 SLPs
85% use NSOME to
Do SLPs Use NSOME?
85% use NSOME to change speech sound
productions
Lof & Watson (2008)
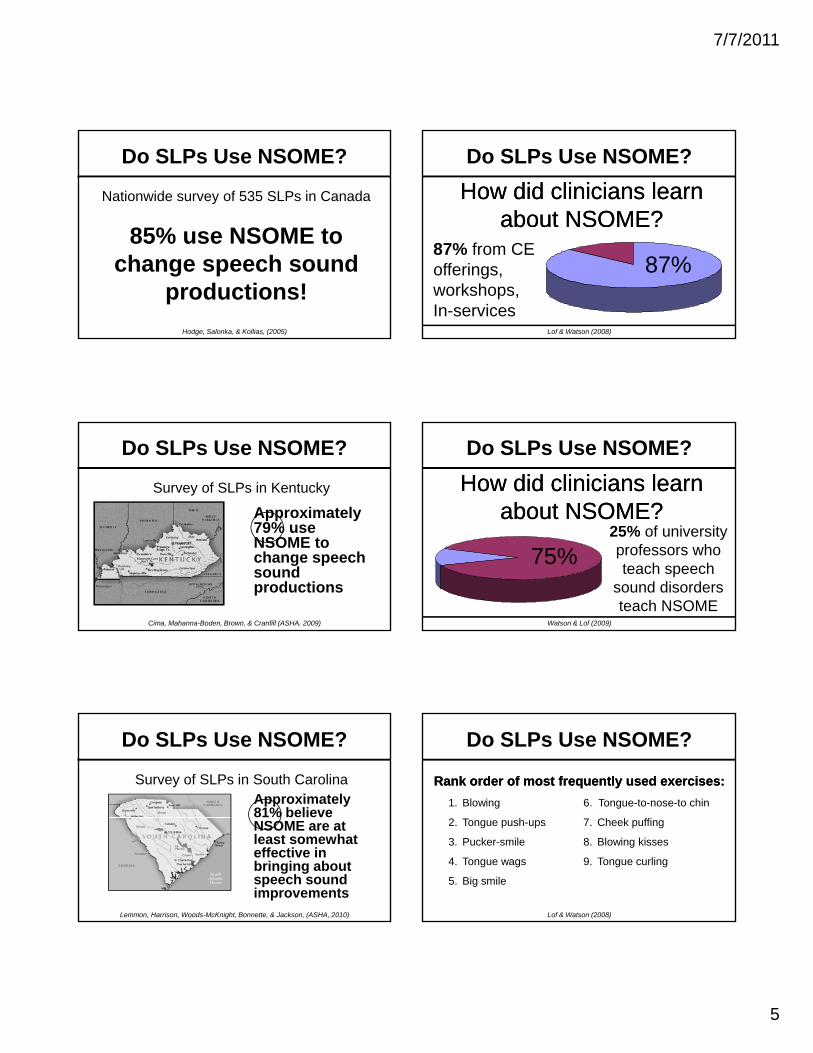
Nationwide survey of 535 SLPs in Canada
Do SLPs Use NSOME?
Hodge, Salonka, & Kollias, (2005)
7/7/2011
5
Nationwide survey of 535 SLPs in Canada
85% use NSOME to
Do SLPs Use NSOME?
85% use NSOME to change speech sound
productions!
Hodge, Salonka, & Kollias, (2005)
Survey of SLPs in Kentucky
Do SLPs Use NSOME?
Approximately 79% use
Cima, Mahanna-Boden, Brown, & Cranfill (ASHA, 2009)
79% use NSOME to change speech sound productions
Survey of SLPs in South Carolina
Do SLPs Use NSOME?
Approximately 81% believe
Lemmon, Harrison, Woods-McKnight, Bonnette, & Jackson, (ASHA, 2010)
NSOME are at least somewhat effective in bringing about speech sound improvements
Do SLPs Use NSOME?
How did clinicians learn How did clinicians learn about NSOME?about NSOME?
Lof & Watson (2008)
87% from CE offerings, workshops, In-services
87%
Do SLPs Use NSOME?
How did clinicians learn How did clinicians learn about NSOME?about NSOME?
25% f i it
Watson & Lof (2009)
25% of university professors who teach speech
sound disorders teach NSOME
75%
Rank order of most frequently used exercises:Rank order of most frequently used exercises:
1. Blowing 6. Tongue-to-nose-to chin
Do SLPs Use NSOME?
2. Tongue push-ups
3. Pucker-smile
4. Tongue wags
5. Big smile
7. Cheek puffing
8. Blowing kisses
9. Tongue curling
Lof & Watson (2008)

7/7/2011
6
Rank order of most frequently identified Rank order of most frequently identified “benefits” of these exercises:“benefits” of these exercises:
Do SLPs Use NSOME?
1. Tongue elevation
2. Awareness of articulators
3. Tongue strength
4. Lip strength
5. Lateral tongue movements
6. Jaw stabilization
7. Lip/tongue protrusion
8. Drooling control
9. VP competence
10.Sucking ability
Lof & Watson (2008)
Clinicians Clinicians USUALLYUSUALLY use these use these exercises for children with…exercises for children with…
Do SLPs Use NSOME?
1. Dysarthria
2. Childhood Apraxia of Speech (CAS)
3. Structural anomalies (e.g., clefts)
4. Down syndrome
Lof & Watson (2008)
Do SLPs Use NSOME?
Clinicians Clinicians FREQUENTLYFREQUENTLY use these use these exercises for children with…exercises for children with…
1. In early intervention
2. Late talkers
3. Phonologically impaired
4. Hearing impaired
5. Functional misarticulatorsLof & Watson (2008)
Evidence-Based Practice
• The conscientious, explicit, and unbiased use of current best research results in making decisions about the care of i di id l li t
Evidence-Based Practice
individual clients.
• Treatment decisions should be administered in practice only when there is a justified (evidence-based) expectation of benefit.
Sackett et al., (1996)
Research Evidence
Evidence-Based Practice
EBP
Clinical Experience Client Values

7/7/2011
7
EBP is the integration of best research evidence along with clinical expertise
and the client values
Evidence-Based Practice
and the client values
EBP uses the best evidence available, in consultation with the client or parents to
decide upon the options that suits the client best.
The Purpose of EBP
P t
Evidence-Based Practice
Promotethe adoption of effective interventions
The Purpose of EBP
Evidence-Based Practice
Delaythe adoption of unproved interventions
The Purpose of EBP
Evidence-Based Practice
Preventthe adoption of ineffective interventions
Evidence-Based Practice
Most of the evidence th ffi f
Levels of Evidence from Studies
on the efficacy of NSOME is on the somewhat weaker
side, but…
Evidence-Based Practice
Levels of Evidence from Studies
LEVEL Ib: STRONG Well designed randomized controlled study
LEVEL Ia: STRONGEST Well-designed meta-analysis of >1 RCT
LEVEL Ib: STRONG Well-designed randomized controlled study
LEVEL IIa: MODERATE Well-designed controlled study without randomization
LEVEL IIb: MODERATE Well-designed quasi-experimental study
LEVEL IV: WEAK Opinion of authorities, based on clinical experience
LEVEL III: LIMITED Nonexperimental studies (i.e., correlational and case studies)

7/7/2011
8
Dollaghan (2004, 2007) reminds clinicians that when using the EBP paradigm, valid and reliable evidence needs to be given more credence than intuition anecdote and
Evidence-Based Practice
more credence than intuition, anecdote and expert authority.
While opinions and clinician's own clinical experiences can be useful, they
can also be biased and even wrong!
Finn, Bothe, & Bramlett (2005)
Evidence-Based Practice
Science and Pseudoscience in Communication Disorders: Criteria and Applications
Science
Evidence-Based Practice
vs. Pseudoscience
Finn, Bothe, & Bramlett (2005)
Science:Science:
Evidence-Based Practice
Information is developed through research and other empirically based activities.
Finn, Bothe, & Bramlett (2005)
Pseudoscience:Pseudoscience:“A pretend or spurious science; a
Evidence-Based Practice
p p ;collection of related beliefs about the world mistakenly regarded as being
based on scientific method or as having the status that scientific truths
now have.”Finn, Bothe, & Bramlett (2005)
Quackery and Pseudoscience can go together
Quackery is anything
Evidence-Based Practice
Quackery is anything involving over-promotion
in a clinical field
Finn, Bothe, & Bramlett (2005)
Includes questionable ideas and questionable products and services, regardless of the sincerity of the promoters

7/7/2011
9
You know it is
Evidence-Based Practice
it is Pseudoscience
when…
Finn, Bothe, & Bramlett (2005)
Disconfirming evidence
is ignored and practice
You know it is …
You know it is pseudoscience when…
is ignored and practice
continues even though
the evidence is clear.
Finn, Bothe, & Bramlett (2005)
The only “evidence” is anecdotal,
supported with
You know it is …
You know it is pseudoscience when…
supported with statements from
personal experience
(testimonials)Finn, Bothe, & Bramlett (2005)
Inadequate
You know it is …
You know it is pseudoscience when…
evidence is
accepted
Finn, Bothe, & Bramlett (2005)
The printed materials
You know it is …
You know it is pseudoscience when…
are not peer
reviewedFinn, Bothe, & Bramlett (2005)
Grandiose outcomes are proclaimed
You know it is …
You know it is pseudoscience when…
Finn, Bothe, & Bramlett (2005)

7/7/2011
10
Muttiah, Georges, & Brackenbury
(2011)
Evidence-Based Practice
Qualitative Study:Interviews with
• 11 clinicians who use NSOME
• 11 researchers who are against their use
Oral Motor Tasks…
This is the logical part
Tongue Push-UpsObjective: to strengthen tongue Procedure: child holds up an M&M, cheerio, etc. on upper ridge just
behind teeth (not on teeth) and pushes up with tongue.
Some Exercises From the Web:http://www.widesmiles.org/cleftlinks/WS-563.html
Tongue PopsObjective: To strengthen tongue Procedure: Suck tongue up on the top of the mouth, pull it back and
release it, making a popping sound.Pointy TongueObjective: To increase tongue movement and coordinationProcedure: Protrude tongue and point it at the tip.
WhistleObjective: To increase lip strengthProcedure: Have child pucker lips and blow attempting to whistle.Fish Mouth
Some Exercises From the Web:http://www.widesmiles.org/cleftlinks/WS-563.html
Objective: To increase oral-motor strengthProcedure: Pucker lips and suck cheeks in to make a "fish-face"Pucker-SmileObjective: To increase oral-motor coordinationProcedure: Have child close mouth with back teeth together. Have
child pucker lips (while keeping back teeth together). Once mastered, have child alternate a pucker with a smile.
Some questions to ask yourself as you
Do NSOME make logical sense?
yourself as you evaluate these tasks…

7/7/2011
11
Do NSOME make logical sense?
There is evidence that shows that NSOME doshows that NSOME do
not work. Why is it being ignored?
Do NSOME make logical sense?
There is NO evidence that shows thatthat shows that
NSOME do work. Why is this being ignored?
Do NSOME make logical sense?
Why are the materials and procedures used inand procedures used in NSOME not brought up
for peer-review scrutiny?
Do NSOME make logical sense?
Why are the materials and proceduresand procedures promoted only in
self-published materials and on websites?
Do NSOME make logical sense?
Why do these websites h ti fhave a section for
“testimonials” but not for “research”?
Do NSOME make logical sense?
How could one procedure work toprocedure work to remediate so many disparate types of
problems?

7/7/2011
12
Do NSOME make logical sense?
For example, look at some of the catalogs
that promote NSOME…
From a Catalog:
Grandiose outcomes are proclaimed
If i i d
Remember Pseudoscience
If it is too good to be true, it probably is not true!
Finn, Bothe, & Bramlett (2005)
Do NSOME make logical sense?
What is the monetary benefits to the
promoters of NSOME?
Are NSOME Logical?
?

7/7/2011
13
Now For the Theory Part
Part-whole training and transfer
Strengthening the structures
Why Exercises are THOUGHT to be Effective
Strengthening the structures
Relevancy to the act of speaking
Task specificity
Warm-up/Awareness/Metamouth
Part-Whole Training and Transfer
Part-Whole Training and Transfer
Premise:
If we teach smaller parts of aIf we teach smaller parts of a
speech gesture, it will help in
the acquisition of the whole
speech gesture.
Part-Whole Training and Transfer
However, it has been shown that…
Tasks that comprise highly organized or g y gintegrated parts will not be enhanced by learning of the constituent parts; rather,
training on parts of these organized behaviors may diminish learning.
Part-Whole Training and Transfer
What this means...
Highly organized tasks require
l i f th i f tilearning of the information
processing demands as well as
learning time sharing and other
intercomponent skills.
7/7/2011
14
Part-Whole Training and Transfer
“Fractionating a behavior that is composed of interrelated parts i t lik l t id l tis not likely to provide relevant information for the appropriate
development of neural substrates.”
Forrest (2002)
Part-Whole Training and Transfer
It is the breaking the whole task
i t llinto small, meaningless
subtasks that will not be effective.
Part-Whole Training and Transfer
An example of this was recently reported to me by a student clinician who was assigned to a practicum
with a school SLP. The student described how they had been extensively drilling a child to use a “lowerhad been extensively drilling a child to use a lower
lip biting” maneuver with the ultimate goal of evoking the /f/ sound. During the many sessions with the child, they never worked on the actual
speech sound, instead only practiced the isolated exaggerated lingual-dental gesture.
Part-Whole Training and Transfer
“Training the Whole”Ingram & Ingram (2001)
“Whole-Word Phonology and Templates”
Velleman & Vihman (2002)
Part-Whole Training and Transfer
Summary– Learning of tasks with interdependent parts
is not improved by decomposition.– Fractionation and simplification of a task do
not yield any improvements in learning a target behavior.
– Do not break things into small subtasks because there probably will be no transfer of that skill to the whole.
Part-whole training and transfer
Strengthening the structures
Why Exercises are THOUGHT to be Effective
Strengthening the structures
Relevancy to the act of speaking
Task specificity
Warm-up/Awareness/Metamouth
7/7/2011
15
Increase in Strength
Do SLPs USE NSOME?
Rank order of most frequently identified
“benefits” of these exercises:
1. Tongue elevation
2. Awareness of articulators
3. Tongue strength
4. Lip strength
5. Lateral tongue movements
6. Jaw stabilization
7. Lip/tongue protrusion
8. Drooling control
9. VP competence
10.Sucking ability
Lof & Watson (2008)
Four Questions about Strength:
1. Is strength needed for speech?
Increase in Strength
2. Will NSOME actually increase strength?
3. How is strength adequately measured?
4. Do children with speech sound disorders
have weakness?
Question Question 11
Is strength needed
Increase in Strength
Is strength needed
for speech?
Strength needs for speech are VERY low
– Lip muscle force for speaking is only about 10-
20% of the maximal capabilities of lip force.
Increase in Strength
p p
– The jaw uses only about 11- 15% of available
amount of force that can be produced.
– Activation of the laryngeal muscles is between
10% - 20% of maximum.
Strength needs for speech are VERY low
In other words, the speaking strength
d d t h l t
Increase in Strength
needs do not come anywhere close to
the maximum strength abilities of the
articulators.

7/7/2011
16
Strength needs for speech are VERY low
“…only a fraction of maximum tongue force is
used in speech production, and such
Increase in Strength
used in speech production, and such
strength tasks are not representative of the
tongue's role during typical speaking. As a
result, caution should be taken when directly
associating tongue strength to speech…”
Wenke, Goozee, Murdoch, & LaPointe (2006)
Strength needs for speech are VERY low
Children need agility and fine
ti l t t
Increase in Strength
articulatory movements
Strength needs for speech are VERY lowChildren need agility and fine articulatory movements
–Need agility, not strength
Increase in Strength
Need agility, not strength
–NSOME encourages gross and exaggerated
ranges of motion, not small, coordinated
movements that are required for talking
Strength needs for speech are VERY lowChildren need agility and fine articulatory movements
– Motor SKILL training induces motor map
Increase in Strength
g p
reorganization, whereas strength training does
not (Remple et al., 2001).
– Exercise alone (as opposed to skill training) will
not alter motor map organization (Kleim et al.,
2002).
Strength needs for speech are VERY lowChildren need agility and fine articulatory movements
– Different adaptive changes are evoked with
Increase in Strength
p g
strength training than with skill training (Jensen et
al., 2005).
Question Question 22
Will NSOME
Increase in Strength
Will NSOME
actually strengthen
the articulators?

7/7/2011
17
A non-speaking example:
Bicep weight training
Increase in Strength
• Repetitions to failure?• Repetitions to failure?
• Against resistance?
• Increase agility and range of motion?
A non-speaking example:
Bicep weight training
Increase in Strength
Do people who use NSOME follow this basic strength training paradigm?
Will NSOME actually strengthen the articulators?
Bl i i id i
Increase in Strength
A Speaking Example: VP Closure
Blowing exercises can aid in
velopharyngeal closure for
other blowing tasks; but this
closure is not maintained for
speaking.
Will NSOME actually strengthen the articulators?
Li l i i
Increase in Strength
A Tongue Exercise Example with Normal Adults
Lingual exercises using
protrusion and
lateralization, 30 repetitions
a day, 7 days a week, for
9 weeks
Clark, O’Brien, Calleja, & Corrie (2009)
Will NSOME actually strengthen the articulators?
P d d 6% t 26%
Increase in Strength
A Tongue Exercise Example with Normal Adults
Produced 6% to 26%
increase in strength.
Significant loss of strength
(back to baseline) once
training ended.
Clark, O’Brien, Calleja, & Corrie (2009)
Will NSOME actually strengthen the articulators?
Increase in Strength
A Swallowing Example
Lingual exercises can strengthen the tongue
and it can have an effect on swallowing.
Robbins, J., Gangnon, R., Theis, S., Kays, S., Hewitt, A., & Hind, J. (2005)

7/7/2011
18
But it takes A LOT of exercises:
• 8 weeks
• 30 exercises against resistance
A Swallowing Example
Increase in Strength
• 3 times a day
• Every other day
Strength increased: only ~ 6 kPa or
~ 17% increase in 8 weeks
Increase in Strength
Lip Strengthening Exercises• 8 7-19 year olds with Myotonic Dystrophy Type 1• Counter balanced design for 32 weeks• Exercised 16 minutes 5 days/week against resistance
Sjögreena, L., Tuliniusb, M., Kiliaridisc, S., & Lohmanderd, A. (2010). The effect of lip strengthening exercises in children and
adolescents with myotonic dystrophy type 1. International Journal of Pediatric Otorhinolaryngology, 74(10), 1126-1134.
• Exercised 16 minutes, 5 days/week against resistance• Results:
• Only 4 improved maximal lip strength• Lip strength did not lead to improved function for
speech, eating, drinking, mobility, or saliva control• Strength was not maintained over time
Increase in Strength
Will NSOME actually strengthen the articulators?
Only if the standard strength training paradigm is followedtraining paradigm is followed.
But it may not improve function!
Question Question 33
How is strength
Increase in Strength
How is strength
adequately measured?
Measurements of
Increase in Strength
strength are usually
highly subjective
Measurement of strength is
typically done subjectively
Increase in Strength
For example, feeling the force of the tongue
pushing against a tongue depressor or against
the cheek

7/7/2011
19
Measurement of strength is
typically done subjectivelyT t t th li i i l h ld
Increase in Strength
To assess tongue strength, clinicians commonly hold a
tongue depressor beyond the lips and the patient pushes the
tongue against the depressor. Strength is rated perceptually,
often with a 3-5 point equal-appearing interval scale or with
binary judgments of “normal” or “weak.”
Solomon & Monson (2004)
Measurement of strength is
typically done subjectively
Increase in Strength
Objective measures of strength have been
recommended as more valid and reliable than subjective
measures for the assessment of tongue function, yet
subjective measures remain the more commonly used
clinical method.
Clark, Henson, Barber, Stierwalt & Sherrill (2003)
Measurement of strength is
typically done subjectively
Increase in Strength
Because of this, clinicians cannot initially verify
that strength is diminished and
they cannot report increased strength following
NSOME
Only objective measures can corroborate
statements of strength needs and strength
improvement.
Increase in Strength
p
(e.g., dynamometer, force transducer, IOPI)
Without such measurements, testimonials
of strength gains are suspect.
Tongue Force Transducer
Iowa Oral Performance Instrument (IOPI)

7/7/2011
20
When tongue strength assessments were done with
a tongue depressor compared with the IOPI, it was
found that there was only a weak correlation.
Increase in Strength
Student clinicians were actually better at estimating
strength than were experienced clinicians
(but nether were very good).
Clark, Henson, Barber, Stierwalt & Sherrill (2003)
How is strength adequately
measured?
Increase in Strength
Usually with subjectivity so
statements about weakness are
questionable.
Question Question 44
Do children with speech
Increase in Strength
Do children with speech sound disorders have
weak tongues?
Sudberry, Wilson, Broaddus, & Potter (2006)
• Used the Iowa Oral Pressure Instrument (IOPI)
Increase in Strength
• 30 typically developing preschool children and 15 with speech sound disorders.
• Children with speech sound disorders had STRONGER tongues than typically developing children!!!
Dworkin & Culatta (1980)No difference in tongue strength comparing controls with children who “lisp” and children
Increase in Strength
controls with children who “lisp” and children with a tongue thrust.
Dworkin & Culatta (1980)
“The present findings suggest that tongue
Increase in Strength
The present findings suggest that tongue strengthening exercises may be
superfluous to the correction of tongue thrusting or associate frontal lisping.”

7/7/2011
21
Tone vs. Strength• Muscle tone refers to the resilience or elasticity of
the muscle at rest.
Increase in Strength
• "Low tone" indicates less contraction of the fibers than typical.
• Observing low tone does not automatically mean that the child has weakness.
• Working on strengthening probably will not influence tone.
Clark, 2010
Summary Strength needs for speaking are very low.
We need agile movements not strong
Increase in Strength
We need agile movements, not strong movements.
NSOME probably are not adding strength.
Subjective measures of strength are not valid.
Children with speech sound disorders probably don’t have weak tongues.
Part-whole training and transfer
Strengthening the structures
Why Exercises are THOUGHT to be Effective
Strengthening the structures
Relevancy to the act of speaking
Task specificity
Warm-up/Awareness/Metamouth
Relevancy of NSOME to Speech
NSOME
Relevancy of NSOME to Speech
lack
RELEVANCY
RELEVANCY is the issue
Relevancy is the way to get changes in the neural system
Relevancy of NSOME to Speech
Context is Crucial

7/7/2011
22
RELEVANCY is the issue
Relevancy is the way to get changes in the neural system
Relevancy of NSOME to Speech
Context is CrucialIn order to obtain transfer from one skill to another, the learned skill
must be relevant to the other skills.
For sensory motor stimulation to improve articulation, the stimulation must be done with relevant behaviors with a defined end goal, using
integration of skills.
RELEVANCY is the issue
Relevancy is the way to get changes in the neural system
Relevancy of NSOME to Speech
Context is Crucial
“The purpose of a motor behavior has a profound influence on the manner in which the relevant neural topography is
marshaled and controlled.”
Weismer (2006)
A non-speaking example:
Sh ti b k tb ll
Relevancy of NSOME to Speech
Shooting a basketball
Why DIS-INTEGRATE?
Another non-speaking example:
Relevancy of NSOME to Speech
Dribbling a
Basketball
Another non-speaking example:
Relevancy of NSOME to Speech
Playing
the Piano
One final non-speaking example:
Why shoot a basketball
Relevancy of NSOME to Speech
Why shoot a basketball
without an actual hoop?
The end goal needs to be practiced!

7/7/2011
23
One final non-speaking example:
Breaking down basketball
Relevancy of NSOME to Speech
gshooting or the speaking
task into smaller, unrelated chunks that are irrelevant
to the actual performances is not effective.
Talk about irrelevant…
For example practicing tongue
Relevancy of NSOME to Speech
For example, practicing tongue elevation to the alveolar ridge with the desire that this isolated task will
improve production of /s/ is dis-integrating the highly integrated
task of speaking.
Improving speaking ability must be
practiced in the context of speaking.
Relevancy of NSOME to Speech
To improve speaking, children must
practice speaking, rather than using
tasks that only superficially appear
to be like speaking.
Isolated movements of the tongue, lips and
other articulators are not the actual
gestures used for the production of sounds
Relevancy of NSOME to Speech
g p
in English.
Oral movements that are irrelevant to the
speech movements will not be effective
therapeutically.
No speech sound requires the tongue tip
to be elevated toward the nose no
Relevancy of NSOME to Speech
to be elevated toward the nose, no
sound is produced by puffing out the
cheeks, no sound is produced in the
same way as blowing is produced.
Relevancy of NSOME to Speech

7/7/2011
24
Summary Only movements relevant to speaking are
effective.
Relevancy of NSOME to Speech
The end goal—speaking–must be practiced.
Disintegrating highly integrated movements are not effective.
No speech sounds are produced with the tongue in strange positions, cheeks puffed out, etc.
Part-whole training and transfer
Strengthening the structures
Why Exercises are THOUGHT to be Effective
Strengthening the structures
Relevancy to the act of speaking
Task specificity
Warm-up/Awareness/Metamouth
Task Specificity
Do the same structures used
for other “mouth tasks”
Task Specificity
for other “mouth tasks”
function the same as for
speech?
Respondents who reported they believe speech develops from early oral motor
Do SLPs USE NSOME?
speech develops from early oral motor behaviors such as sucking and chewing:
Lof & Watson (2008)
60%
This means that clinicians believe that early experiences with sucking and chewing
lead directly to speech.
Task Specificity
lead directly to speech.
However, chewing and babbling have been shown to have no relation.
Early mouth movements are not precursors to speech.
Moore & Ruark (1996)
7/7/2011
25
T k S ifi it
Task Specificity
Task Specificity
T k S ifi it
Task Specificity
Task SpecificitySame Structures but Different Functions
The same structures used for speaking and other “mouth tasks” (e.g., feeding, sucking, swallowing, breathing, etc.) function in different ways depending on the task
Task Specificity
ways depending on the task.
Each task is mediated by different parts of the brain.
The organization of movements within the nervous system is not the same for speech and nonspeech.
Although identical mouth structures are used these
Task Specificity
structures are used, these structures function differently
for speech and for nonspeech activities.
The control of motor behavior
Task Specificity
is task specific, not effector (muscle or organ) specific.
There is strong evidence
Task Specificity
against the “shared control” for speech and nonspeech.

7/7/2011
26
Bonilha, Moser, Rorden, Baylis, & Bridriksson (2006). Speech apraxia
ith t l i C l b i
Task Specificity
without oral apraxia: Can normal brain function explain the physiopathology? Neuro Report, 17 (10), 1027-1031.
Bonilha, Moser, Rorden, Baylis, & Bridriksson (2006)
Finding:
Non-speech motor movements
Task Specificity
pelicited activation of different
parts of the brain than did speech motor movements.
Bonilha, Moser, Rorden, Baylis, & Bridriksson (2006)
Schulz, Dingwall, & Ludlow (1999).Speech and oral motor learning in
Task Specificity
Speech and oral motor learning in individuals with cerebral atrophy. Journal of Speech, Language and Hearing Research,
42, 1157-1175.
Schulz, Dingwall, & Ludlow (1999)
• Normal adults and adults with cerebral pathology
Task Specificity
• Practiced speech and nonspeech movements
• FINDINGS:
Schulz, Dingwall, & Ludlow (1999)
• Difference in the effect of learning between speech and nonspeech movements for both groups.
• There is a difference in the degree of change in cortical physiology in response to training for speech and
Task Specificity
physiology in response to training for speech and nonspeech tasks.
• It cannot be assumed that the type of pattern of cortical or behavior adaptations are equivalent for speech and nonspeech tasks.
• Important to consider “speech motor control” that is different from other motor control.
Schulz, Dingwall, & Ludlow (1999)
Task Specificity
Ludlow, C., Hoit, J., Kent, R., Ramig, L., Shrivastav, R., Strand, E., Yorkston, K., & Sapienza C (2008) Translating principles ofSapienza, C. (2008). Translating principles of neural plasticity into research on speech motor control recovery and rehabilitation. Journal of Speech, Language and Hearing Research, 51, S240-S258.
Ludlow et al. (2008)

7/7/2011
27
• Changes in neural function with practice are limited to the specific function being trained.
• For example, training on lip strength will only
Task Specificity
benefit the neural control for lip movement and force with no spontaneous transfer to speech production.
• Changes occur only in the neural substrates involved in the particular behavior being trained.
Ludlow et al. (2008)
Yee, Vick, Venkatesh, Campbell, Shriberg, Green, Rusiewicz, & Moore (Nov., 2007).
Task Specificity
Green, Rusiewicz, & Moore (Nov., 2007). Children’s mandibular movement patterns in two nonspeech tasks.
74 36-60 month olds:
42 with “speech delay”
32 typically developing
Task Specificity
32 typically developing
2 tasks:1. Silent jaw oscillations (imitation of speech
movements in response to a model) 2. Mastication (chewing a single Goldfish
cracker)Yee et al. (2007)
Analyzed the cyclic movements of the mandible across groups and tasks
FINDINGS
Task Specificity
FINDINGS
• Speech and nonspeech tasks exhibited distinct patterns
• Typically developing and children with speech disorders did not differ
Yee et al. (2007)
7 Research Examples of Task Specificity
Babbling and Early Oral Behaviors
NOT related to each other
Moore & Ruark (1996)
7 Research Examples of Task Specificity
Speech and Swallowing• Dysphagia with speech problems• Dysphagia without speech problems• Speech problems without dysphagia
Green & Wang (2003); Martin (1991); Ziegler (2003)

7/7/2011
28
S h d S ll i
7 Research Examples of Task Specificity
Speech and SwallowingCan strengthen the oral structures for the oral phase of swallowing but it will
have no impact on speaking
Robbins et al. (2005)
7 Research Examples of Task Specificity
Strengthening VPCan strengthen the VP complex, but it
does not reduce nasalized speech
(many studies since the 1960s)
7 Research Examples of Task Specificity
Breathing for SpeechDifferent than breathing at rest or
during other activities
e.g., Moore, Caulfield, & Green (2001)
7 Research Examples of Task Specificity
Tongue Thrust Therapy
Oral myofunctional therapy improves the tongue thrust, but not speech
productions
Gommerman & Hodge (1995); Christensen & Hanson (1981)
7 Research Examples of Task Specificity
Diadochokinetic Syllable RepetitionSyllable repetition and speech production
rate and accuracy are unrelated; training these movements will not improve speech.
McAuliffe, Ward, Murdoch, & Farrell (2005)
7 Research Examples of Task Specificity
Silent Tongue MovementsSilent tongue movements produced
symmetric brain activation in the right and left primary motor regions; phonation with tongue movements produced activation in
the left hemisphere.Terumitsu, Fujii, Suzuki, Kwee, & Nakada (2006)

7/7/2011
29
Summary of 11 Research StudiesSummary of 11 Research StudiesSpeech and Nonspeech are different for:
Other Research Examples of Task Specificity
•facial muscles
•jaw motion
•jaw operating space
•jaw coordination
•lingual movement
•lip motions
•levator veli palatini
•mandibular control
Weismer (2006)
Summary The same oral structures function differently for
speech and for nonspeech movements.
Task Specificity
p p
Working on nonspeech activities will not develop the necessary neural pathways for speaking.
Speech is special and unlike other oral movements.
Part-whole training and transfer
Strengthening the structures
Why Exercises are THOUGHT to be Effective
Strengthening the structures
Relevancy to the act of speaking
Task specificity
Warm-up/Awareness/Metamouth
Warm-Up, Awareness and Metamouth
Do SLPs USE NS-OME?
Rank order of most frequently identified “benefits” of these exercises:
1. Tongue elevation
2. Awareness of articulators
3. Tongue strength
4. Lip strength
5. Lateral tongue movements
6. Jaw stabilization
7. Lip/tongue protrusion
8. Drooling control
9. VP competence
10. Sucking ability
Lof & Watson (2008)
2 points about this…1 Warm-up from a physiological
Warm-Up, Awareness and Metamouth
1. Warm up from a physiological point of view
2. “Meta-mouth” awareness

7/7/2011
30
Warm up from a physiological point of view
Awareness and “Warm-Up”
Purpose of warm-up muscle exercise:
To increase blood circulation so muscle viscosity drops, thus
allowing for smoother and more elastic muscle
contractions
Warm up from a physiological point of view
Awareness and “Warm-Up”
When is muscle warm-up appropriate?
When a person is about to initiate an exercise regimen that will maximally tax the
system (e.g., distance running, weight lifting)
Warm up from a physiological point of view
Awareness and “Warm-Up”
When is muscle warm-up NOT appropriate?
Muscle warm-up is not required for tasks that are
below the maximum
(e.g., walking, lifting a spoon-to-mouth)
Warm up from a physiological point of view
Awareness and “Warm-Up”
When waking up in the morning it is doubtful that many peopleit is doubtful that many people
warm-up their arms before dressing, or warm-up their
mouths before uttering their first “good morning” because the
muscles are already prepared for such tasks.
Metamouth
?
Providing some form of knowledge
Metamouth
about the articulators’ movement and placement

7/7/2011
31
For articulation awareness, children age 5 and 6 years have very little
Metamouth
age 5 and 6 years have very little consciousness of how speech sounds
are made; 7 year olds are not very proficient with this either.
Klein, Lederer & Cortese (1991)
Children can make use of metamouth knowledge perhaps
Metamouth
metamouth knowledge perhaps after age 7 if they have the
“…cognitive maturity required to understand the concept of a
sound.”
Koegel, Koegel, & Ingham (1986)
It appears that young children cannot take advantage of the non
Metamouth
cannot take advantage of the non-speech mouth-cues provided during
NSOME that can be transferred to speaking tasks.
SummaryMuscles do not need to be warmed up if they
are not being taxed.
Warm-Up, Awareness and Metamouth
g
NSOME do not “wake up” the mouth for speaking.
Children probably cannot make use of the mouth cues provided during NSOME that will aid in articulatory movements for speech.
Disorders that SLPs Use NSOME
The L O N G
list oflist of disorders that clinicians use
NSOME in therapy…
Disorders that SLPs Use NSOME
Childhood Apraxia of Speech (CAS) Dysarthria Structural anomalies (e.g., clefts)
D d Down syndrome In early intervention Late talkers Phonologically impaired Hearing impaired Functional misarticulators
Lof & Watson (2008)

7/7/2011
32
NSOME and
Childh d A i f S h
Disorders that SLPs Use NSOME
Childhood Apraxia of Speech
(CAS)
It is puzzling why clinicians would use NSOME, especially for children with CAS.
Disorders that SLPs Use NSOME—CAS
By definition, children with CAS have adequate oral structure movements for nonspeech activities but not for volitional speech (Caruso & Strand, 1999).
There can be no muscle weakness of children with CAS, so there is no need to do strengthening exercises.
Disorders that SLPs Use NSOME—CAS
If there is weakness, then the correct diagnosis is dysarthria, not apraxia.
“The focus of intervention for the child diagnosed with CAS is on improving the
planning, sequencing, and coordination of
Disorders that SLPs Use NSOME—CAS
p g, q g,muscle movements for speech. Isolated
exercises designed to "strengthen" the oral muscles will not help. CAS is a disorder of
speech coordination, not strength.”
ASHA Position Paper and Technical Report (2007)
NSOME and
Disorders that SLPs Use NSOME
NSOME and Cleft Lip/Palate
The VP mechanism can be strengthened through exercise, but added strength will not improve speech production.
Disorders that SLPs Use NSOME—Cleft Lip/Palate
Blowing exercises are not an appropriate therapeutic technique.
Peterson-Falzone, Trost-Cardamone, Karnell, Hardin-Jones (2006)

7/7/2011
33
Disorders that SLPs Use NSOME—Cleft Lip/Palate
See these references:• Peterson-Falzone, Trost-Cardamone,
Karnell, Hardin-Jones (2006), ( )
• Goldening-Kushner, K. (2001)
• Ruscello (2008)
“Do not invest time or advise a parent to invest time and money addressing a muscle strength problem
that may not (and probably does not) exist. It is very frustrating to see clinicians working on “exercises” to
Disorders that SLPs Use NSOME—Cleft Lip/Palate
frustrating to see clinicians working on “exercises” to strengthen the lips and tongue tip when bilabial and
lingua-alveolar sounds are already evident in babble, or when bilabial and lingual/lingua-alveolar functions
are completely intact for feeding and other nonspeech motor behaviors.”
Peterson-Falzone, Trost-Cardamone, Karnell, Hardin-Jones (2006)
“Having a repaired cleft does not mean a child will lack the muscle strength needed to produce
consonant sounds adequately. The presence of a cleft palate (repaired or unrepaired) has no
Disorders that SLPs Use NSOME—Cleft Lip/Palate
p ( p p )bearing on tongue strength or function (why would it?). The majority of children who demonstrate VPI do so because their palate is too short to achieve VP closure. Muscle strength or lack thereof is not
a primary causal factor associated with phonological delays in this population.”
Peterson-Falzone, Trost-Cardamone, Karnell, Hardin-Jones (2006)
“…blowing should never be used to “strengthen” labial or soft palate musculature; it does not work.
Children who appear to improve over time in
Disorders that SLPs Use NSOME—Cleft Lip/Palate
therapy when using these tools are likely demonstrating improvement related to maturation
and to learning correct motor speech patterns. Had therapy focused only on speech sound
development, these children probably would have shown progress much sooner.”
Peterson-Falzone, Trost-Cardamone, Karnell, Hardin-Jones (2006)
“Blowing exercises, sucking, swallowing, gagging, and cheek puffing have been suggested as useful in
improving or strengthening velopharyngeal closure and speech. However, multiview videofluoroscopy
Disorders that SLPs Use NSOME—Cleft Lip/Palate
p pyhas shown that velopharyngeal movements of these
nonspeech functions differ from velopharyngeal movements for speech in the same speaker.
Improving velopharyngeal motion for these tasks do not result in improved resonance or speech. These
procedures simply do not work and the premises and rationales behind them are scientifically unsound.”
Goldening-Kushne, 2001
NSOME for
Non-Motor Speech Disorders
Disorders that SLPs Use NSOME
Non Motor Speech Disorders
(e.g., Late Talkers, Children in early intervention, Hearing impaired,
Phonological disorder, etc.)
—

7/7/2011
34
It makes no logical sense that motor exercises could help improve the
speech of children who have non-motor
Disorders that SLPs Use NSOME—Non-Motor Problems
speech of children who have non-motor problems, such as language-phonemic-phonological problems, like children in Early Intervention diagnosed as late
talkers.
Why would children with a language-based sound
Disorders that SLPs Use NSOME—Non-Motor Problems
g gproblem improve with a motor-
based treatment approach?
NSOME and
Disorders that SLPs Use NSOME
Children with Dysarthria
Should NSOME be used for children with the diagnosis of
Disorders that SLPs Use NSOME—Dysarthria
dysarthria?
What does the acquired dysarthria literature say?
“…strengthening exercises are probably only appropriate for a small
number of patients ”
Disorders that SLPs Use NSOME—Dysarthria
number of patients.”
“…weakness is not directly related to intelligibility..for patients with ALS.”
Duffy (2005)
Mackenzie, C., Muir, M., & Allen, C. (2010). Non-speech oro-motor exercise use in acquired dysarthria management:
Disorders that SLPs Use NSOME—Dysarthria
use in acquired dysarthria management: Regimes and rationales. International
Journal of Language and Communication Disorders, 1-13.
7/7/2011
35
81% of SLPs in Scotland, Wales, and Northern
Disorders that SLPs Use NSOME—Dysarthria
Ireland, working with adult-acquired dysarthria, use
NSOME
Mackenzie, Muir, & Allen (2010)
“That NSOME are appropriate in dysarthria is part of the folklore of SLT, and folklore may be a potent influence,
Disorders that SLPs Use NSOME—Dysarthria
and folklore may be a potent influence, even impending the adoption of
approaches which have scientific validity, in favour of what is handed down by word
of mouth or demonstration.”
Mackenzie, Muir, & Allen (2010)
Should NSOME be used for children with the diagnosis of dysarthria?
Disorders that SLPs Use NSOME—Dysarthria
Based on the adult acquired dysarthria literature, it appears that NSOME are not recommended as a technique that can
improve speech productions.
Duffy (2005); Yorkston, Beukelman, Strand, & Hakel (2010)
Evidence Against NSOME
Evidence
Evidence Against NSOME
Based Practice
EBP
There are a limited number of
Evidence Against NSOME
published (peer reviewed) articles that have sufficient
scientific rigor.

7/7/2011
36
ASHA National Center for Evidence-Based Practice in Communication Disorders
Evidence Against NSOME
Communication Disorders (NCEP)
Purpose:To conduct evidence-based systematic reviews
on NSOME
McCauley, Strand, Lof, Schooling, & Frymark, (2009)
ASHA National Center for Evidence-Based Practice in Communication Disorders (NCEP)
Findings:
Evidence Against NSOME
Based on the 8 published peer-reviewed articles, the evidence is equivocal due to the lack of well-designed experimentally
controlled studies with adequate statistical power and adequate description of
subjects.
McCauley, Strand, Lof, Schooling, & Frymark, (2009)
CONVINCING evidence that they do not work
Evidence Against NSOME
do not work
NO real data that supports their use
There is some research evidence, most of which has been presented at
Evidence Against NSOME
most of which has been presented at various
ASHA Conventions…
RESEARCH: Non Speech Oral Motor Exercises
Do Not Work
1. Christensen & Hanson (1981)
2. Gommerman & Hodge (1995)
3. Colone & Forrest (2000)
4 Occhino & McCane (2001) 12345
64. Occhino & McCane (2001)
5. Abrahamsen & Flack (2002)
6. Bush, Steger, Mann-Kahris, & Insalaco (2004)
7. Roehrig, Suiter, & Pierce (2004)
8. Guisti & Cascella (2005)
9. Hayes (2006)
10. Forrest & Iuzzini (2008)
78
9 10
1. Fields & Polmanteer (2002)
RESEARCH: Non Speech Oral Motor Exercises
Do Work
11
But this study has MANY methodological fatal flaws (more on this later)

7/7/2011
37
There are 11 studies il bl 10 th t h h
Evidence Against NSOME
available, 10 that have shown that NSOME were not
effective as a treatment approach.
Evidence-Based Practice
Levels of Evidence from Studies
LEVEL Ib: STRONG Well designed randomized controlled study
LEVEL Ia: STRONGEST Well-designed meta-analysis of >1 RCT
LEVEL Ib: STRONG Well-designed randomized controlled study
LEVEL IIa: MODERATE Well-designed controlled study without randomization
LEVEL IIb: MODERATE Well-designed quasi-experimental study
LEVEL IV: WEAK Opinion of authorities, based on clinical experience
LEVEL III: LIMITED Nonexperimental studies (i.e., correlational and case studies)
RESEARCH:Non Speech Oral Motor Exercises Do Not Work
Christensen and Hanson (1981)
• 10 children • Aged 5;8 to 6;9 years• 14 weeks• 14 weeks• Half of the children received only articulation therapy; the other
half received articulation and “neuromuscular facilitation techniques”
• Both groups made equal speech improvements• The exercises did not help for better speech sound production
BUT were effective in remediating tongue-thrusting (probably due to task specificity)
Gommerman & Hodge (1995)
• 16 year-old girl with tongue thrust and sibilant distortions
RESEARCH:Non Speech Oral Motor Exercises Do Not Work
• A Phase, no treatment; B Phase, myofunctional treatment; C Phase articulation therapy.
• Tongue thrust was eliminated with myofunctional therapy but speech was unchanged.
• With articulation therapy, sibilant productions improved.
Colone & Forrest (2000)
• Monozygotic twin boys age 8;11 year old• Motor treatment for Twin 1, phonological
RESEARCH:Non Speech Oral Motor Exercises Do Not Work
treatment for Twin 2• NO improvements with motor training (Twin 1);
good results using a phonological approach (Twin 2)
• When Twin 1 received phonological treatment, there were the same improvements as Twin 2
Occhino & McCane (2001)• Single Subject Design (A-B-C-B-C)• 5 year old child• Results were that oral motor exercises alone
RESEARCH:Non Speech Oral Motor Exercises Do Not Work
Results were that oral motor exercises alone produced no improvement in the articulation of one of two phonemes
• Also no improvements in oral motor skills• Oral motor exercises prior to or along with articulation
therapy did not have an additive or facilitative effect• Articulation improved with articulation therapy

7/7/2011
38
Abrahamsen & Flack (2002)
• Single Subject Design
4 year old child
RESEARCH:Non Speech Oral Motor Exercises Do Not Work
• 4 year old child
• 10 hours of individual treatment
• Used blowing, licking, and oral stimulation
• No evidence of effectiveness in changing speech-sound productions
Bush, Steger, Mann-Kahris, & Insalaco (2004)
• ABAB Withdrawal Single Subject Design• 9 year old boy
RESEARCH:Non Speech Oral Motor Exercises Do Not Work
• 9 year old boy• OME added to articulation treatment, then
removed, then re-added• /r/ /s/ /z/ /l/• “Oral motor treatment did not improve or reduce
treatment's success.”
Roehrig, Suiter, & Pierce (2004)
• AB or BA Single Subject Design• Six 3;6 - 6;0 boys and girls
RESEARCH:Non Speech Oral Motor Exercises Do Not Work
• 15 weeks total Tx: (A) Tradition, production-based Tx twice a week for ½ hour; (B) Passive OME and traditional Txtwice a week for ½ hour
• “The addition of OME to the traditional articulation therapy approach did not add to participants overall progress; improvement following therapy with OME was not different from improvements following articulation therapy alone.”
Guisti & Cascella (2005)
• Single Subject Design using 2 boys and 2 girls
• All in first grade
RESEARCH:Non Speech Oral Motor Exercises Do Not Work
• Followed Easy Does it for Articulation: An Oral Motor Approach (1997)
• 15 ½ hour individual treatment sessions
• No evidence of effectiveness in changing speech-sound productions
Hayes (2006)
• Six 4 year olds, 5 boys and 1 girl
• All had “functional misarticulations”
C b l d i i d i bj
RESEARCH:Non Speech Oral Motor Exercises Do Not Work
• Counterbalanced intervention design so subjects were randomly assigned to a specific order; Oral motor approach and traditional articulation approach.
• The traditional treatment resulted in significant change; no support for using oral motor for change.
• Some support that NSOME actually hindered learning.
Forrest & Iuzzini (2008)
• 9 children, 3;3 to 6;3 years
• Alternating treatment design: 1 sound treated with NSOME 1 sound with production treatment (PT) 1 not
RESEARCH:Non Speech Oral Motor Exercises Do Not Work
NSOME, 1 sound with production treatment (PT), 1 not treated
• At least 20 treatments sessions lasting 60 minutes
• RESULTS: – 30% increase in sound accuracy with PT; 3% with NSOME
– NSOME did not even improve movement control when assessed using a Volitional Oral Motor test

7/7/2011
39
Fields & Polmanteer (2002)• Eight 3- to 6-year-old children • Randomly assigned to one of two groups • Four children received 10 minutes of oral motor
RESEARCH:Non Speech Oral Motor Exercises Do Not Work
Four children received 10 minutes of oral motor treatment and10 minutes of speech therapy; four children received 20 minutes of only speech therapy
• Fewer errors at the end of 6 weeks of treatment for the children who received the combination of treatments
BUT….
Fields & Polmanteer (2002)
Many methodological and statistical issues• Severity distribution not equal (speech-only group
RESEARCH:Non Speech Oral Motor Exercises Do Not Work
Severity distribution not equal (speech only group more severe)
• Gender distribution not equal• The treated sounds and the equivalency of the
sounds between groups were not reported.
VERY Questionable Results
The evidence that is available…OVERWHELMINGLY
Evidence Against NSOME
demonstrates that NSOME are not
effective in bringing about
speech-sound changes.
Based on the findings as of now, th f NSOME t b
Evidence Against NSOME
the use of NSOME must be considered exploratory and the clients should be informed of this
prior to initiating their use in therapy
Recent Reviews of the Literature
Evidence Against NSOME
CLINICAL FORUM: The Use of Nonspeech Oral Motor Treatments forNonspeech Oral Motor Treatments for
Developmental Speech Sound Production Disorders: Interventions
and Interactions
Language, Speech and Hearing Services in the SchoolsJuly, 2008
Many SLPs use a combination of treatment approaches, so it is difficult to “tease apart”
which approach is providing therapeutic
What about Combining Treatment Approaches?
benefit.Whenever intervention approaches are
combined, it is unknown if and how they actually work in conjunction with each
other to enhance performance.
7/7/2011
40
There is much evidence that the NSOME portion of combined treatments is irrelevant to speech
improvements.
NSOME b bl d t h th hild h
What about Combining Treatment Approaches?
NSOME probably do not harm the child when used in combination with other approaches.
SLPs should eliminate the approach that is not effective (i.e., NSOME) so as to not waste valuable therapy time with an ineffectual
technique.
that are used in articulation therapy are
Phonetic Placement CuesPhonetic Placement Cues
articulation therapy areNOT the same as
NSOME
NSOME are a
NSOME are NOT Goals
procedure, NOT a goal!!!
Oral motor exercises are a procedure, NOT a goal!!!
The goal of therapy is NOTto produce a tongue wag to
NSOME are NOT Goals
to produce a tongue wag, to have strong articulators, to
puff out cheeks, to blow “harder” horns, etc.
Oral motor exercises are a procedure, NOT a goal!!!
R th th l i t
NSOME are NOT Goals
Rather, the goal is to produce intelligible speech
Why Do SLPs Use NSOME?
Some potential reasons why NSOME is used so frequentlyNSOME is used so frequently in the remediaton of speech
sound disorders:
Lof (2008)

7/7/2011
41
The procedures can be followed in a step-by-step “cookbook” fashionThe exercises are tangible with the
Why Do SLPs Use NSOME?
appearance that something therapeutic is being done at a physical level (even if the disorder is not motor in nature as would be the case for hearing impairment or phonological impairment)
There is a lack of understanding the theoretical literature addressing the dissimilarities of speech-nonspeech
Why Do SLPs Use NSOME?
p pmovements
The techniques can be written out to produce handouts to give to caregivers for use outside of the therapy setting
There are a wide variety of techniques and tools available that are attractively presented for purchase
Why Do SLPs Use NSOME?
Many practicing clinicians do not read peer-reviewed articles but instead rely on unscientific writings (e.g., web sites, the popular press, marketed therapy tools, etc.)
They attend non-peer reviewed activities(e.g., continuing education events) that encourage the use of these activities
Why Do SLPs Use NSOME?
encourage the use of these activities
Parents and occupational/physical therapists on multidisciplinary teamsencourage using NSOME
Frequently, other clinicians persuade their colleagues to use these techniques, which is reminiscent of a statement by
Why Do SLPs Use NSOME?
which is reminiscent of a statement by Kamhi (2004) who stated, “…no human being is immune to hearing a not-so-good idea and passing it on to someone else.”
Been burned before….
Clinicians often resort to “because it works”
observations
Remember, we wrongfully embraced
facilitated communication!!

7/7/2011
42
A Helpful
Reference
Nov., 2008
CLINICAL FORUM:The Use of Nonspeech Oral
Motor Treatments for
Another Helpful Reference…
Motor Treatments for Developmental Speech Sound
Production Disorders: Interventions and Interactions
Language, Speech and Hearing Services in the SchoolsJuly, 2008
What questions/commentsdo you have?
1
Updating Evidence Against Updating Evidence Against Nonspeech Oral Motor Exercises Nonspeech Oral Motor Exercises
(NSOME) for Speech Sound (NSOME) for Speech Sound ProductionsProductions
Gregory L. Lof, PhD, CCC-SLPDepartment Chair/Professor
July, 2011
Boston, MA