models of preventive care in clinical practice to achieve ... · models of preventive care in...
TRANSCRIPT

Models of preventive care in clinical practice to achieve
‘25 by 25’
Professor David A WoodGarfield Weston
Professor of Cardiovascular MedicineInternational Centre for Circulatory Health
Imperial College London United Kingdom


Guidelines
Implementation
Evaluation

Finland
Czech RepublicFrance
Germany
Hungary
Italy
Netherlands
SloveniaSpain
EUROASPIRE IV
Belgium
Ireland
UK
Greece
Poland
Latvia
Lithuania
Romania
Russia
Croatia
Bulgaria
CyprusTurkey
Serbia
Bosnia and Herzegovina Ukraine
Sweden
Eur J Prevent Cardiol 2015

Prevalence of smoking, obesity* and central obesity**
* BMI ≥ 30 kg/m²; **Waist circumference ≥ 88 cm for women and ≥ 102 cm for men
p=0.55
p=0.007
p=0.04
EUROASPIRE IIEUROASPIRE IIIEUROASPIRE IV

Prevalence of smoking by age and sex

Prevalence of raised BP*, elevated LDL-C** and diabetes***
* SBP/DBP ≥ 140/90 mmHg (≥ 140/80 mmHg for patients with diabetes); LDL ≥ 1.8 mmol/L (≥ 70 mg/dL);***Fasting glucose ≥ 7 mmol/L (≥ 126 mg/dL) for patients without history of diabetes
p=0.01
P<0.0001
p=0.0004
EUROASPIRE IIEUROASPIRE IIIEUROASPIRE IV
p=0.78

Cardiovascular protective drug therapies
P<0.0001EUROASPIRE IIEUROASPIRE IIIEUROASPIRE IV
P<0.0001
P<0.0001P<0.0001

Cardiopulmonary rehabilitation
“Cardiac rehabilitation is a branch of rehabilitation medicine dealing with
optimizing physical function in patients with cardiac disease or recent cardiac surgeries”
Wickipedia March 25th 2015

Cardiac rehab §°
95% CI Secondary prevention ¶
95% CI
Total mortality 0.80 0.68, 0.93 0.85 0.77, 0.94
CHD mortality 0.74 0.61, 0.90 - -
Myocardial re-infarction 0.79 0.57, 1.09 0.83 0.74, 0.94
§ Taylor R et al, Am J Med 2004; 116:682-692 ¶ Clark A M et al Annals of Internal Medicine 2005;143:659-672. °Heran B S, et al Cochrane Database of Systematic Reviews 2011
Randomised controlled trials of cardiac rehabilitation

Randomised controlled trials of secondary prevention
All cause mortalityTreatment Control Relative
Risk95% CI
Programmewith no exercise
4598 4604 0.87 0.76, 0.99
Programmewith exercise
2404 2251 0.88 0.74, 1.04
Exercise only 1165 1120 0.72 0.54, 0.95
Overall* 8167 7975 0.85 0.77, 0.94
*p=0.001
Clark A M et al Annals of Internal Medicine 2005;143:659-672

Treatment Control Relative Risk
95% CI
Programmewith no exercise
2787 2742 0.86 0.72, 1.03
Programmewith exercise
2075 1922 0.62 0.44, 0.87
Exercise only 1124 1073 0.76 0.57, 1.01
Overall* 5986 5737 0.83 0.74, 0.94*p=0.002
Clark A M et al Annals of Internal Medicine 2005;143:659-672
Randomised controlled trials of secondary prevention
Recurrent myocardial infarction

Cardiac rehabilitation+
Secondary prevention

Cardiac rehabilitation is a branch of rehabilitation medicine dealing with
optimizing physical function in patients with cardiac disease.
While the ‘glue’ of cardiac rehabilitation is exercise, programmes are evolving to
become comprehensive prevention centerswhere all aspects of
care are delivered.
Wickipedia March 25th 2015

Comprehensive prevention centers where all aspects of care are
delivered.
Wickipedia March 25th 2015

Lifestyle (smoking cessation, diet, physical activity) intervention, taking account of psycho-social factors, and using a behavioural approach Measuring, monitoring and managing other risk
factors (blood pressure, lipids and glucose) to target
Understanding of, and adherence with, cardioprotective drug therapies for life

SCORE: the European Risk Prediction System
1994199820033rd Joint European Societies Task Force
2004European Society of Cardiology
Score enabled HeartScore, an interactive tool
• 12 European cohort studies• wide geographic spread of
countries at different levels of cardiovascular risks
• 3-million person-years of observation
• 7,934 fatal cardiovascular events
Data from:
SCORE
Total risk assessment

SCORE

SCORE: the European Risk Prediction System
1994199820033rd Joint European Societies Task Force
2004European Society of Cardiology
Score enabled HeartScore, an interactive tool
• 12 European cohort studies• wide geographic spread of
countries at different levels of cardiovascular risks
• 3-million person-years of observation
• 7,934 fatal cardiovascular events
Data from:
SCORE
Total risk assessment
Total risk management

Lifestyle (smoking cessation, diet, physical activity) intervention, taking account of psycho-social factors, and using a behavioural approach Measuring, monitoring and managing other risk
factors (blood pressure, lipids and glucose) to target
Understanding of, and adherence with, cardioprotective drug therapies for life

Lancet 2008; 371: 1999-2012
EUROACTIONA European Society of Cardiology demonstration project:8 countries and 24 hospital and general practice centres

General hospitals and general practices
Dr Antonio Salvador, Cristina Buigues, Ana Bonet, Arancha Ruescas and Rosario Cuevas
Hospital General de Dr. Peset
Dr Jorge Navarro and Gemma Medez Perez
Centro de Salud de San Pau

Ambulatory nurse-coordinated multidisciplinary approach
The EUROACTION team in Boldrini Hospital, Thiene, Italy The EUROACTION nurse and
the lead GP in Hoensbroek, The Netherlands

Lifestyle change in families• No smoking• Saturated Fat: <10% total
Energy• Fruits and vegetables:
>400g/day• Fish: >20g/day• Oily Fish: >3 times/week• 30-45 minutes of physical
activity at 60–75% of the average maximum heart rate on four-five days of the week
• Weight reduction ≥ 5%• Waist <94 cm in men and
<80 cm in women
Smoking cessation
IncreasingPhysical activity
Healthy eating,Weight
management

Family based lifestyle programme
Sweden
Poland

Health promotion workshops
Gemona, Italy Valencia, Spain

Thiene, Italy
Halmstad, Sweden Valencia, Spain
Supervised hospital and home based physical activity
programme
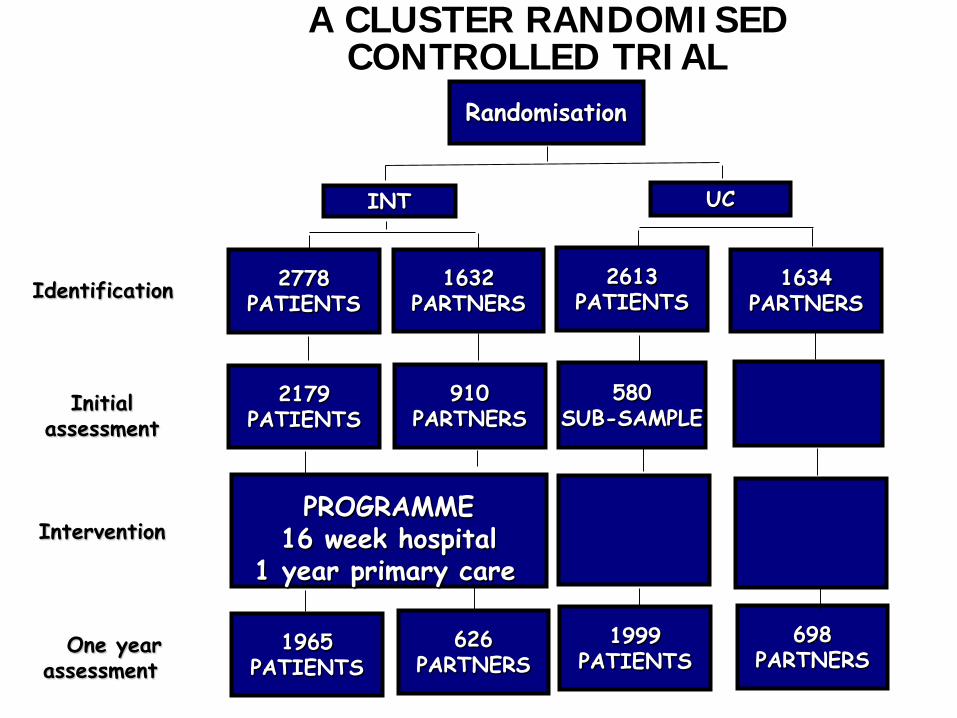
One year assessment
Identification
Intervention
Randomisation
INT
PROGRAMME16 week hospital
1 year primary care
1965PATIENTS
UC
A CLUSTER RANDOMISED CONTROLLED TRIAL
Initial assessment
580SUB-SAMPLE
2179PATIENTS
2778PATIENTS
1632PARTNERS
910PARTNERS
626PARTNERS
2613PATIENTS
1999PATIENTS
1634PARTNERS
698PARTNERS

EUROACTION: HospitalSmoking cessation at one year in coronary patients who were smokers in the month
prior to their event
p = 0.06
+ 10% ( - 0.3% to + 21%)

EUROACTION + Intensive Smoking Cessation with
Varenicline
ItalyUK
Netherlands Spain
Eur Heart J 2014; 35: 1411-1420

Study Participants
N=696 Eligible patientsN=559 High-Risk patientsN=137 Vascular patients
EA+ ARMN=350 patients
N=276 High-Risk patientsN=74 Vascular patients
N=328 Baseline assessmentN=313 Participated in EA+
N=299 85.4%16-weeks assessment
USUAL CARE ARMN=346 patients
N=283 High-Risk patientsN=63 Vascular patients
N=288 83.2%16-weeks assessment
N=346 Primary endpoint N=335 Primary endpoint
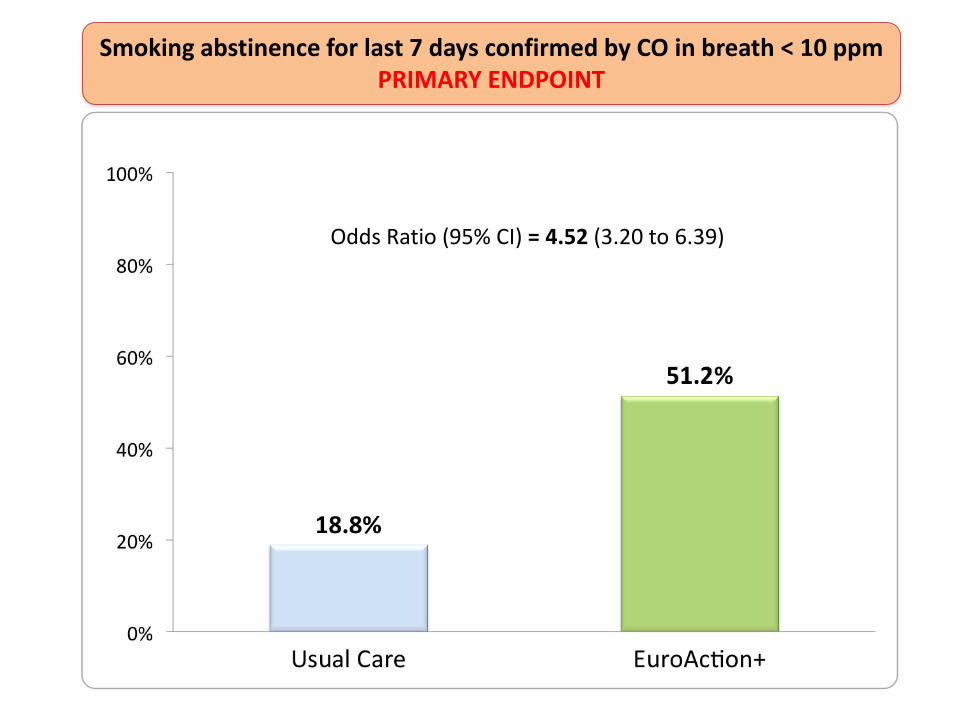
Smoking abstinence for last 7 days confirmed by CO in breath < 10 ppmPRIMARY ENDPOINT
Odds Ratio (95% CI) = 4.52 (3.20 to 6.39)

Lancet 2008; 371: 1999-2012
EUROACTIONA European Society of Cardiology demonstration project:8 countries and 24 hospital and general practice centres

Proportions of patients achieving the European targets for a
healthy dietHospital General Practice
Intervention Usual Care
p = 0.005
p = 0.26
p = 0.13
p = 0.009
p = 0.004
p = 0.91
p = 0.04

Proportions of partners achieving the European targets for a
healthy dietHospital General Practice
p = 0.002
p = 0.42
p = 0.09
p = 0.31 p = 0.002
p = 0.98
p = 0.77
Intervention Usual Care

P = 0.002
General Practice+ 29% ( + 11% to + 48%)
Hospital+ 36% (+20% to + 51%)
P = 0.001
Proportion of patients achieving European Guidelines for physical
activity

Proportion of partners achieving European Guidelines for physical
activity
P = 0.06
General PracticeHospital
p = 0.03
+ 19% (- 0.6% to + 38%) + 27% (+ 4% to + 50%)

Proportion of patients achieving the European target for
blood pressure
P = 0.04
General PracticeHospital
p = 0.03
+ 17% (+ 2% to + 32%)+ 10% (+ 0.6% to + 20%)
Intervention Usual Care
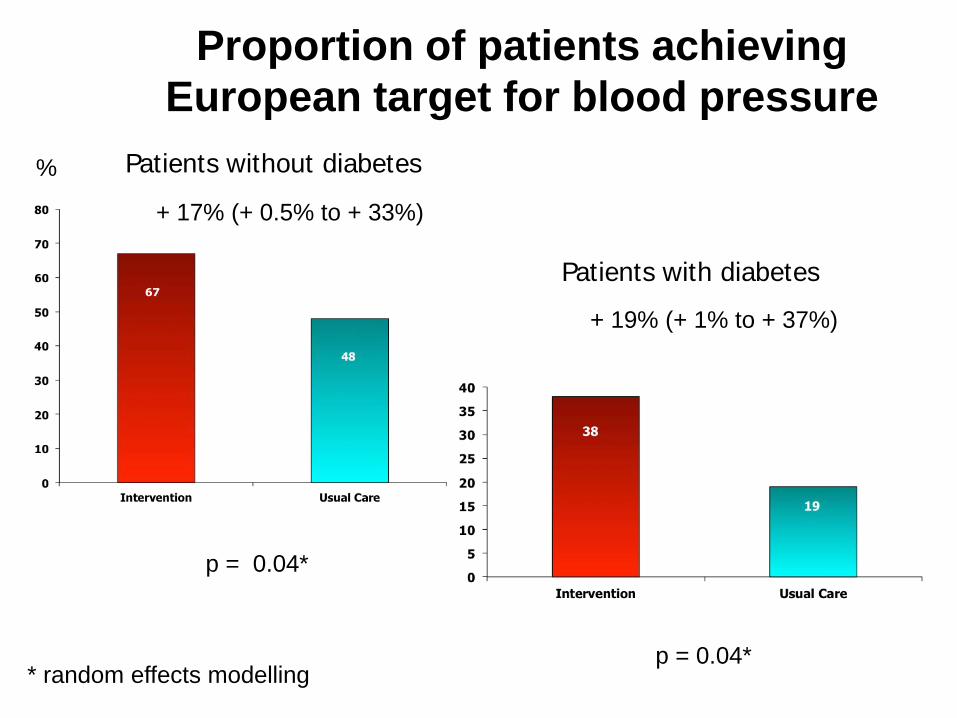
Proportion of patients achieving European target for blood pressure
p = 0.04*
+ 17% (+ 0.5% to + 33%)
* random effects modelling
%
+ 19% (+ 1% to + 37%)
p = 0.04*
Patients without diabetes
Patients with diabetes

Proportion of patients on cardiovascular protective drug therapy
General PracticeHospital
Intervention Usual Care
p=0.28
p=0.16
p=0.26
p=0.53
p=0.04
p=0.06
p=0.91p=0.02
p=0.24
p=0.03
0.19

‘EUROACTION set a new standard for preventive
cardiology – in both secondary and primary prevention

TerminologyCardiac rehabilitation
Cardiovascular rehabilitationRehabilitation and secondary
preventionCardiac rehabilitation and
preventionCardiovascular prevention and
rehabilitation
NICE Guideline: MI - secondary prevention
Cardiac rehabilitation programme is defined as:
ExerciseHealth education and information
Psychology and social support
NICE Guideline: MI - secondary prevention
Cardiac rehabilitation does NOT include:Lifestyle changes after MI:
Smoking cessationChanging dietary regimen
Alcohol consumptionWeight managementDrug therapy after MI

TerminologyCardiac rehabilitation
Cardiovascular rehabilitationRehabilitation and secondary
preventionCardiac rehabilitation and
preventionCardiovascular prevention and
rehabilitation

Cardiac rehabilitation and secondary prevention for patients with
established atherosclerotic disease+
Primary prevention for asymptomatic individuals at high risk of developing CVD including patients with diabetes
mellitus, CKD and other high risk diseases
Primary
Prevention
Secondary
Prevention

Integrate secondary and primary prevention in one programme