model-based extraction of femoral medulla ducts from radiographic images
TRANSCRIPT

Model-based extraction of femoral medulla ducts
from radiographic images
Franco Bartolinia,†, Monica Carfagnib, Lapo Governib,*
aDipartimento di Elettronica e Telecomunicazioni, Universita di Firenze, Via Santa Marta 3, Firenze 50139, ItalybDipartimento di Meccanica e Tecnologie Industriali, Universita di Firenze, Via Santa Marta 3, Firenze 50139, Italy
Received 25 June 2002; received in revised form 3 June 2003; accepted 12 June 2003
Abstract
The planning of the hip prosthesis surgical operation is usually performed manually by the surgeon, who ‘draws’ on a patient’s X-ray
image the outline of the prosthetic stem in order to choose the one most suitable for the case at hand. In an attempt to give some repeatability
and objectivity to the planning phase, a procedure has been devised for hip prosthesis’ stem selection based on the extraction of the femoral
relevant outlines.
This work presents a computer aided method aimed at automatically extracting the medulla duct outlines from a human femur radiographic
image. The outlines are retrieved by referring to a suitable geometric model of the generic femoral cross-section; the projection function
obtained by simulating the radiographic acquisition of such a model is fitted on the grey-level functions corresponding to the rows of the
actual digitised radiographic image by means of a least squares algorithm. The resulting outlines are used in a software tool performing the
hip prosthesis pre-operational planning.
q 2003 Published by Elsevier B.V.
Keywords: Model-based image processing; Medical images processing; Surgery aiding tools
1. Introduction
The Total Hip Replacement pre-operational planning is a
procedure meant to help surgeons to choose the proper
prosthesis for a given patient. The pre-operational planning
is usually carried out by using templates provided by hip
prostheses manufacturers. Such templates contain the
profiles of each different prosthesis model available for
the surgical operation. The surgeon superimposes each
template on a radiographic image of the coxo-femoral
region of the patient, manually trying to match the
prosthesis profile with the patient bone anatomy. Once a
suitable template is found, the corresponding prosthesis is
chosen to be implanted. It is obvious that such a procedure is
highly subjective and its results, consequently, may vary
depending on the surgeon performing the planning.
For this reason a system [1] has been previously
developed capable of performing part of the planning in a
completely automatic way. The system is based on the
estimation of the femoral geometry performed through the
extraction, from a digitised X-ray tomography of the patient
(Fig. 1), of the contours of the medulla duct’s and of the
femoral outlines.
Unfortunately X-ray tomographic machines are not often
found in hospital equipment, while radiographic devices are
widely available. Consequently, the applicability of the
system to conventional radiographic images was tested. In
Fig. 2 the poor performance of an edge extraction procedure
applied to a conventional radiographic image, is shown,
compared with the results obtained from the application of
the same procedure to a tomographic image (in both cases a
classical Laplacian of Gaussian—LoG—edge detector with
standard deviation of 3.5 is used). Such behavior can be
explained by considering the different method used by,
respectively, the tomographic and the radiographic
machines to generate the images. The first type of
techniques makes use of the relative motion between the
0262-8856/$ - see front matter q 2003 Published by Elsevier B.V.
doi:10.1016/S0262-8856(03)00118-5
Image and Vision Computing 22 (2004) 173–182
www.elsevier.com/locate/imavis
† In memory of Franco, Friend and Colleague, whose untimely on
January 1st, 2004 passing occurred* Corresponding author. Tel.: þ39-55-479-6509; fax: þ39-55-479-6394.
E-mail address: [email protected] (L. Governi).

patient and the X-ray source to focus a desired plane of
interest in the patient’s anatomy, hiding all the structures
that lie, along the optical axis, above or behind that plane;
while the second type of techniques produces a simple
projection of all the anatomic structures located between the
X-ray source and the image support, thereby overlapping
different anatomic regions. As a matter of fact, usual edge
detection techniques, that detect the loci of maxima of the
image gradient (or of the zeros of second order derivative)
demonstrated not to be a good choice for this problem, given
that such loci do not have, in the case of radiographic images,
a real physical correspondent. This is better exemplified in
Fig. 3, where the step edge profile (that corresponds to the
model of contours detected by the common derivative-based
Fig. 1. Contour extraction and prosthesis choice performed by the software for pre-operation planning.
Fig. 2. Edges extracted from the radiographic image (left) compared to those extracted from the X-ray tomographic image (right).
Fig. 3. Comparison between the step edge profile (left) representing the
model of contour profile assumed by common derivative-based edge
detector (e.g. LoG), and the edge profile (right) that is the suitable model for
the contour of the medulla duct internal outline.
F. Bartolini et al. / Image and Vision Computing 22 (2004) 173–182174

edge detectors) is compared to the contour profile that is
found in radiographic images in correspondence to the
medulla duct internal outline.
Accordingly conventional image processing techniques
[2–4] proved to be not effective. On the other hand,
several studies demonstrated the effectiveness of active
contours, known as snakes curves, in detecting continu-
ous outlines in X-ray images [5,6]. This approach,
however, has the drawback of requiring an accurate
tuning of the coefficients in the mathematical formulation
of the active contour itself in order to obtain robust
results; moreover it generally does not take into account
a priori knowledge on the 3D geometry of the object to
be analysed (in our case the bone). In order to bypass
this drawback, a new methodology for femoral contours
extraction was developed, that explicitly take into
account the characteristics of the process of image
formation.
2. The femoral cross-section model
The considerations drawn in the previous paragraph lead
us to develop a new methodology strictly related to the
specific kind of images we have to work on. The basic idea
of the new approach is to employ a geometrical parametric
model of the generic cross-section of the human femur. By
using such a model it is possible to anticipate the trend of the
grey-level function exhibited by radiographic images. The
use of a model will also contribute to avoid the image noise
to mislead the contour extraction process. Let us now see the
details of the model development.
First of all many different images of the human femur’s
cross-sections (Fig. 4) were examined. For this purpose the
Visible Human Project database (URL: http://www.nlm.nih.
gov/research/visible/) was used. At a first glance, we
assumed it was possible to model the femur’s cross-section
by an annular hoop, parameterised by the x co-ordinates of
the two circumferences centres—C and c—and by the two
radii—R and r—(Fig. 5).
By considering that a radiography basically measures the
transparency of human body matter went through by X-rays
along directions of projection orthogonal to the radiographic
plane, and by assuming that the transparency of the medulla
Fig. 4. An image of a femoral cross-section taken from the Visible Human
Project database.
Fig. 5. The annular hoop model.
Fig. 6. Projection function obtained by subtracting the two circumferences.
In the figure it is assumed that C ; c:
F. Bartolini et al. / Image and Vision Computing 22 (2004) 173–182 175
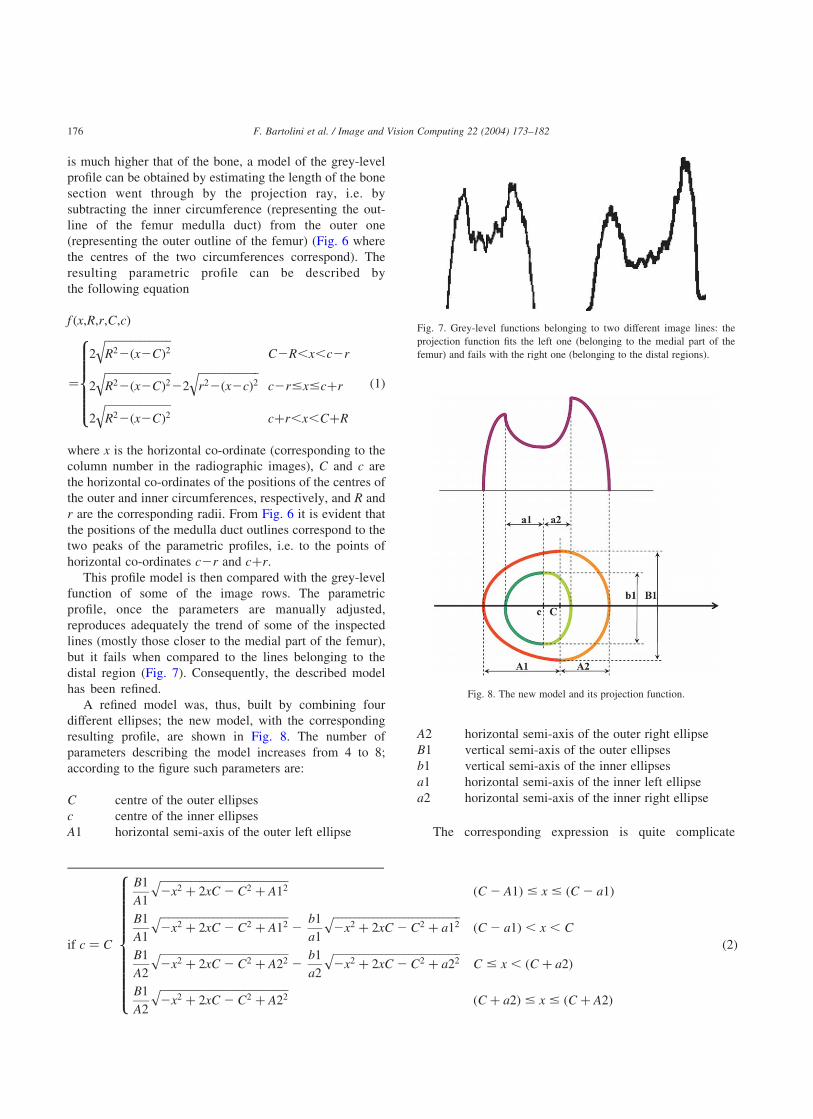
is much higher that of the bone, a model of the grey-level
profile can be obtained by estimating the length of the bone
section went through by the projection ray, i.e. by
subtracting the inner circumference (representing the out-
line of the femur medulla duct) from the outer one
(representing the outer outline of the femur) (Fig. 6 where
the centres of the two circumferences correspond). The
resulting parametric profile can be described by
the following equation
f ðx;R;r;C;cÞ
¼
2
ffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiR22ðx2CÞ2
qC2R,x,c2r
2
ffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiR22ðx2CÞ2
q22
ffiffiffiffiffiffiffiffiffiffiffiffiffiffir22ðx2cÞ2
qc2r#x#cþr
2
ffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiR22ðx2CÞ2
qcþr,x,CþR
8>>>>><>>>>>:
ð1Þ
where x is the horizontal co-ordinate (corresponding to the
column number in the radiographic images), C and c are
the horizontal co-ordinates of the positions of the centres of
the outer and inner circumferences, respectively, and R and
r are the corresponding radii. From Fig. 6 it is evident that
the positions of the medulla duct outlines correspond to the
two peaks of the parametric profiles, i.e. to the points of
horizontal co-ordinates c2r and cþr:
This profile model is then compared with the grey-level
function of some of the image rows. The parametric
profile, once the parameters are manually adjusted,
reproduces adequately the trend of some of the inspected
lines (mostly those closer to the medial part of the femur),
but it fails when compared to the lines belonging to the
distal region (Fig. 7). Consequently, the described model
has been refined.
A refined model was, thus, built by combining four
different ellipses; the new model, with the corresponding
resulting profile, are shown in Fig. 8. The number of
parameters describing the model increases from 4 to 8;
according to the figure such parameters are:
C centre of the outer ellipses
c centre of the inner ellipses
A1 horizontal semi-axis of the outer left ellipse
A2 horizontal semi-axis of the outer right ellipse
B1 vertical semi-axis of the outer ellipses
b1 vertical semi-axis of the inner ellipses
a1 horizontal semi-axis of the inner left ellipse
a2 horizontal semi-axis of the inner right ellipse
The corresponding expression is quite complicate
if c ¼ C
B1
A1
ffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffi2x2 þ 2xC 2 C2 þ A12
pðC 2 A1Þ # x # ðC 2 a1Þ
B1
A1
ffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffi2x2 þ 2xC 2 C2 þ A12
p2
b1
a1
ffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffi2x2 þ 2xC 2 C2 þ a12
pðC 2 a1Þ , x , C
B1
A2
ffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffi2x2 þ 2xC 2 C2 þ A22
p2
b1
a2
ffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffi2x2 þ 2xC 2 C2 þ a22
pC # x , ðC þ a2Þ
B1
A2
ffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffi2x2 þ 2xC 2 C2 þ A22
pðC þ a2Þ # x # ðC þ A2Þ
8>>>>>>>>>>><>>>>>>>>>>>:
ð2Þ
Fig. 7. Grey-level functions belonging to two different image lines: the
projection function fits the left one (belonging to the medial part of the
femur) and fails with the right one (belonging to the distal regions).
Fig. 8. The new model and its projection function.
F. Bartolini et al. / Image and Vision Computing 22 (2004) 173–182176

since many different cases must be pointed out as shown
in the following equations:
if c , C
ffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffi2x2 þ 2xC 2 C2 þ A12
B1
A1
rðC 2 A1Þ # x # ðc2 a1Þ
ffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffi2x2 þ 2xC 2 C2 þ A12
B1
A1
r2
ffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffi2x2 þ 2xc2 c2 þ a12
b1
a1
rðc2 a1Þ , x , c
ffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffi2x2 þ 2xC 2 C2 þ A12
B1
A1
r2
ffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffi2x2 þ 2xc2 c2 þ a22
b1
a2
rc # x # C
ffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffi2x2 þ 2xC 2 C2 þ A22
B1
A2
r2
ffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffi2x2 þ 2xc2 c2 þ a22
b1
a2
rC , x , ðcþ a2Þ
ffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffi2x2 þ 2xC 2 C2 þ A22
B1
A2
rðcþ a2Þ # x # ðC þ A2Þ
8>>>>>>>>>>>>>>>>><>>>>>>>>>>>>>>>>>:
ð3Þ
if c . C
ffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffi2x2 þ 2xC 2 C2 þ A12
B1
A1
rðC 2 A1Þ # x # ðc2 a1Þ
ffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffi2x2 þ 2xC 2 C2 þ A12
B1
A1
r2
ffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffi2x2 þ 2xc2 c2 þ a12
b1
a1
rðc2 a1Þ , x , C
ffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffi2x2 þ 2xC 2 C2 þ A22
B1
A2
r2
ffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffi2x2 þ 2xc2 c2 þ a12
b1
a1
rC # x # c
ffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffi2x2 þ 2xC 2 C2 þ A22
B1
A2
r2
ffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffi2x2 þ 2xc2 c2 þ a22
b1
a2
rc , x , ðcþ a2Þ
ffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffi2x2 þ 2xC 2 C2 þ A22
B1
A2
rðcþ a2Þ # x # ðC þ A2Þ
8>>>>>>>>>>>>>>>>><>>>>>>>>>>>>>>>>>:
ð4Þ
Adjusting the parameters values it is now possible to fit
the grey-level function of any image row crossing the femur
(Fig. 9).
The refined models can then be fitted according to a least
squares [7] criterion to every row of the radiographic image
in such a way to identify, for each row, the horizontal co-
ordinates of the medulla duct outlines. The details of the
actual fitting procedure are given in next section.
3. The contour extraction procedure
On the basis of the described model of the femur’s cross-
section, a procedure to automatically retrieve the medulla
duct outlines has been developed. The basic steps may be
summarised as follows:
1. Definition of an user selected guiding outline.
2. Definition of an area of interest (AoI) on the basis of the
guiding outline.
3. Detection of auxiliary external outlines.
4. Extraction of the femoral medulla duct’s outlines (i.e.
the desired outlines).
A detailed description of all these steps follows in next
subsections.
3.1. The guiding outline
The guiding outline is a user defined curve, created by
picking some desired points on the image by means of the
mouse. At the beginning of the procedure the user is
asked to draw a rough profile approximating the femur’s
external outline. This task is accomplished by selecting
the nodes of two poly-lines approximating, respectively,
the right and left external femoral contours (Fig. 10, left).
After the nodes have been selected, the resulting poly-
lines are converted into two spline curves, of degree 5,
interpolating the nodes; these curves will be called from
now on guiding outline. Such user defined outline was
used, in a previous work to allow the computation of the
direction perpendicular to the edges to be extracted [1],
but in this work it has been introduced for a completely
different reason. In the following subsection its purpose
will be explained.
3.2. The area of interest
The first reason to introduce the guiding outline is to
F. Bartolini et al. / Image and Vision Computing 22 (2004) 173–182 177

identify an AoI on the original image. The AoI is delimited
by the highest and the lowest horizontal segments joining
both the left and right part of the guiding outline and by the
guiding outline itself (Fig. 10, right). In this way the medulla
duct contour to be retrieved is entirely contained in the AoI,
and, consequently, the size of the image portion to be
processed is considerably reduced.
3.3. The auxiliary external outlines
Once the portion of the image to be processed has
been reduced through the definition of the AoI, a least
square best fitting procedure is repeated for each row in
order to automatically determine the proper parameters to
approximate the grey-level row profile. As already
Fig. 9. Two sample image rows fitted with the new projection function.
F. Bartolini et al. / Image and Vision Computing 22 (2004) 173–182178

mentioned, the basic idea is to use the obtained best
fitting parametric profile to determine the two relative
maximum points and, consequently, the location of the
medulla duct edges for that image row (Fig. 11).
Unfortunately this objective can be reached only if the
parameters starting values are close enough to the
optimal ones. This fact is due to the large number of
parameters to be simultaneously optimised, and to the
non-linear nature of the best fitting problem at hand.
Consequently it is necessary to devise a method to cope
with this problem. This has been done by developing a
procedure capable of firstly detecting the external femoral
outlines.
The external femoral outlines provide a very useful tool
for reducing the number of parameters involved in the
search for the best fitting projection function: in fact, for
each image row, the external outlines have the same
position of the two most external points of the correspond-
ing cross-section model. Once such points are known, three
out of the eight parameters determining the projection
function are not independent any more. In particular, by
naming xL and xR; respectively, the left and right co-
ordinates of the so determined external outlines, it results
that C ¼ xL þ A1; and A2¼ xR 2 xL 2A1: Consequently,
the least squares minimisation, needed to identify the best
fitting profile, has to estimate only six of the eight initial
parameters. This reduction proved to be very effective in
decreasing the minimisation procedure sensitivity to the
starting parameters values.
The procedure for detecting the external outlines,
which is applied to all the rows of the image, is based,
in its turn, on a least squares minimisation algorithm.
First, a tolerance range is automatically defined by a
width depending on the images resolution, across the
guiding outline (here it is the second reason for the
guiding outline to be introduced), and only in such a
range the external outlines is actually looked for (Fig. 12,
Fig. 10. The user defined poly-line approximating the femoral external
outlines (left) and the resulting area of interest (right).
Fig. 11. The medulla duct’s outlines for a given line correspond to the local
maxima of the best fitting projection function.
Fig. 12. The automatically defined tolerance range across the guide outline (left), and a portion of the projection function used to fit a desired row segment (right).
F. Bartolini et al. / Image and Vision Computing 22 (2004) 173–182 179
left), then the projection of a portion of the cross-section
model is fitted on the row segment delimited by the
tolerance range (Fig. 12, right). The considered projection
function portions are constituted by the left and right
external ellipses, respectively, for the left and right
external outline; consequently the parameters required to
define them are only the centre of the outer ellipses C; the
vertical semi-axis B1 and one of the horizontal semi-axis
A1 or A2: Using such a number of parameters the best
fitting function for each line is easily found out, therefore
allowing the location of the external outline. The
extraction of the external femoral outline is only
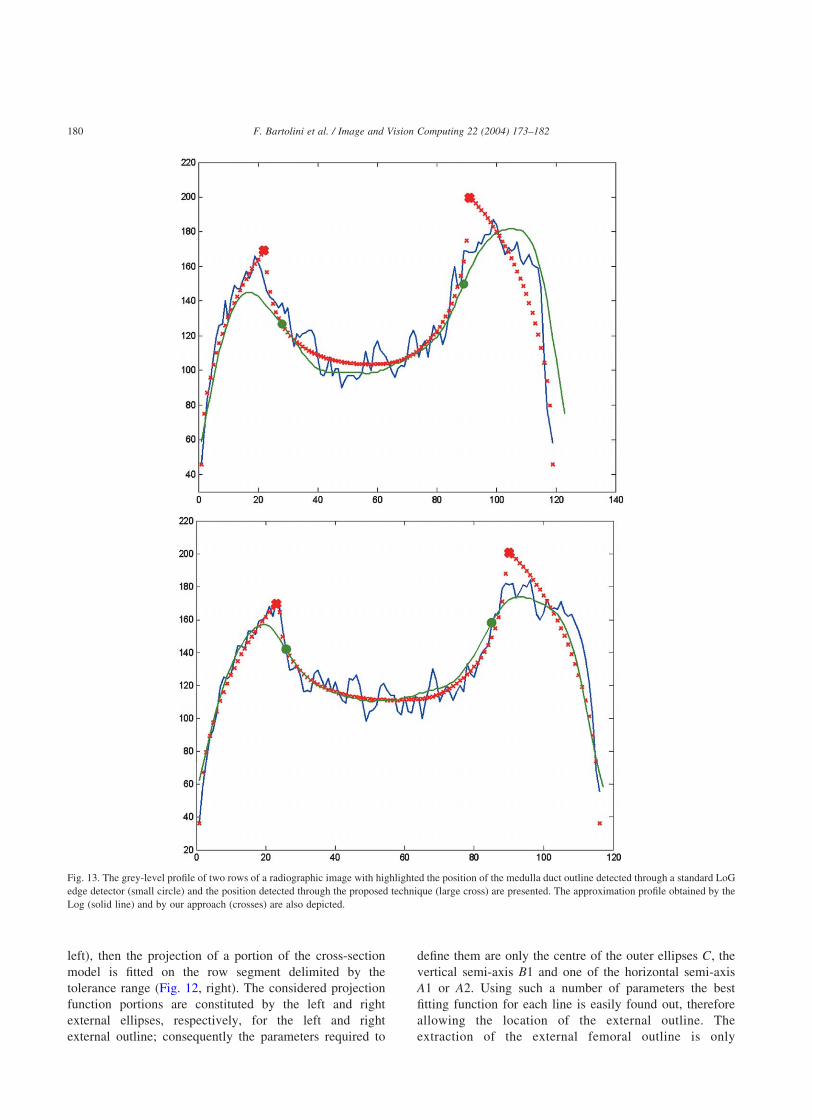
Fig. 13. The grey-level profile of two rows of a radiographic image with highlighted the position of the medulla duct outline detected through a standard LoG
edge detector (small circle) and the position detected through the proposed technique (large cross) are presented. The approximation profile obtained by the
Log (solid line) and by our approach (crosses) are also depicted.
F. Bartolini et al. / Image and Vision Computing 22 (2004) 173–182180

dependent on the location of the tolerance range (Fig. 12,
left): while we are proposing to define this range by
identifying a guiding outline, alternative approaches are
feasible, as for example the definition of a strip where
the actual position of the femoral external outline is
known to be included.
3.4. The actual extraction of the medulla duct outlines
Once the external outlines are located it is a relatively
easy task to extract the medulla duct outlines.
† Starting from the lowest image row in the AoI a least
square minimisation algorithm is applied, using default
starting values for the six required parameters. These
default values are chosen based on the guiding outline;
more in particular it is assumed, for the first image row,
that the femoral cross-section can be represented by a
perfect annular hoop with the inner circle having a radius
equal to 45% of the outer one (the outer circle radius is
provided by the guiding outline).
† The corresponding best fitting profile is thereby com-
puted and the edge (maxima) points are located.
† The following image row is selected (according to a
user defined step index) and the least square estimation
performed again. The initial values for the parameters
are determined on the basis of both the optimised
values deriving from the previous line and the trend of
the external outline enclosed between the current row
and the previous one.
† This last step is iterated for each desired row belonging
to the AoI so that the complete medulla duct outline is
retrieved.
4. Results
The described procedure has been applied to several
test X-ray images, in order to evaluate its performance in
terms of repeatability and robustness; the sensitivity to
the user’s errors in selecting the guiding outline has been
also tested. In this section some selected results are
presented.
First of all to prove the major effectiveness of the
model-based approach with respect to standard edge
extraction techniques for the problem at hand, in Fig. 13
the grey-level profiles of two rows of a radiographic
image are depicted. The position of the medulla duct
outline detected by the proposed technique is highlighted
with a large cross, while the position detected by means
of a classical LoG edge detector with standard deviation
of 3.5 is highlighted with a small circle. The approxi-
mation profiles obtained by the two methods are also
plotted (with a solid line the profile approximated by the
LoG, and with crosses the profile approximated through
our model-based approach). It is evident that the precision
of the proposed approach is much higher. In fact, given
the profile of the projection function, the position
identified by the LoG, i.e. the point of zero second
Fig. 14. The effects of inaccurate user selected guiding outline and (centre and right) of poorly contrasted image (left) are presented. The medulla duct outline is
always well detected.
F. Bartolini et al. / Image and Vision Computing 22 (2004) 173–182 181

order derivative, has almost nothing to do with the edge
of the medulla duct outline.
In Fig. 14 the effects of inaccurate user selected guiding
outlines and of differently contrasted images are shown: it is
evident that the proposed method is strongly insensitive
both to the very inaccurate initial manual selection of the
guiding outline and to the variations of dynamic range of the
images to be processed. A similar insensitivity is exhibited
by the proposed approach with respect to the number of
points used for defining the guiding outlines.
For comparison the results obtained by a previous
method [1] relying on a standard LoG operator are shown
in Fig. 15. Anyway it is important to stress again that the use
of LoG operator can be source of a systematic error, given
that it detects the points of the profile where second order
derivatives become null, but, because of the particular
formation process of radiographic images, these do not have
any physical meaning. On the contrary the maxima of the
profile estimated by the proposed model-based approach
correspond to the location of the femur medulla duct.
5. Conclusions
In this paper a novel approach has been presented for
extracting the femoral medulla duct outlines from radio-
graphic images. The effectiveness of the approach is based
on the use of a model of the femoral cross-section and on
the simulation of the radiographic projection process, to
build up a parametric grey-level profile which is fitted to
the pixels values extracted from the rows of the radio-
graphic images. The approach has proved to be very
robust, repeatable and immune to user errors. The
implemented procedure has been included in the pre-
operational system described in Ref. [1], thus enabling
processing of both X-ray tomographic and conventional
radiographic images.
Future work will be addressed to retrieve the geometry of
mutually orthogonal femoral cross-sections, by applying the
procedure to two distinct radiographic images (frontal and
lateral views). Once both the axes are computed it will be
possible to perform a complete reconstruction of the entire
3D femoral geometry at an extremely low cost.
Acknowledgements
The authors would like to thank Francesco Crispini for
the help provided in implementing the system.
References
[1] D. Bongini, M. Carfagni, L. Governi, Hippin: a semiautomatic
computer program for selecting hip prosthesis femoral components,
Computer Methods and Programs in Biomedicine 63 (2000)
105–115.
[2] R.C. Gonzales, R.E. Woods, Digital Image Processing, Addison-
Wesley, New York, 1992.
[3] J.C. Russ, The Image Processing Handbook, CRC Press, Boca Raton,
FL, 1992.
[4] E.R. Davies, Machine Vision: Theory, Algorithms, Practicalities,
Academic Press, London, 1990.
[5] R. Saxena, S.G. Zachariah, J.E. Sanders, Processing computer
tomography bone data for prosthetic finite element modeling: a
technical note, Journal of Rehabilitation Research and Development 39
(5) (2002) US Department of Veteran’s Affairs.
[6] T.T. Peng, Detection of femur fractures in X-Ray images, Master of
Science Thesis, National University of Singapore, 2002.
[7] W.H. Press, B.P. Flannery, S.A. Teukolsky, W.T. Vetterling,
Numerical Recipes in C: The Art of Scientific Computing, second
ed., Cambridge University Press, Cambridge, January 1993.
Fig. 15. Medulla duct outline detected by means of a standard LoG
operator.
F. Bartolini et al. / Image and Vision Computing 22 (2004) 173–182182