mini-gastric bypass: best surgery;
Post on 19-Oct-2014
2.082 views
DESCRIPTION
Presentaion; Selection of the "Best" Bariatric Surgical Procedure; Discussion of the risk of "Marginal Ulcer" in MGB and in RNY gastric bypassTRANSCRIPT

SELECTION OF THE “BEST” BARIATRIC SURGERY PROCEDURE
The Mini-Gastric Bypass
Dr Rutledge: Training & Background
• Undergrad/Medical School; Teacher Dr. Lester Dragstedt Pioneer / Inventor of the Highly Controversial Vagotomy and Pyloroplasty
• 2 Years Cardiac Surgery National Institutes of Health National Heart Lung Blood Institute
• 20 years University of NC; Professor of Surgery, Associate Chief of Staff, Director of Section Medical Informatics, Director North Carolina Trauma Registry
• Author of 93 papers and articles
Dr Rutledge: Training & Background
• Specialty: Trauma, Critical Care, Medical Informatics and Bariatric Surgery (1978-1998 20 years University NC)
• Experience: Trauma Surgery, Director NC Trauma Registry• Peptic Ulcer Surgery; Vagotomy & Pyloroplasty;
Antrectomy & Billroth II
• Bariatric Surgery 33 years: Open RNY & Vertical Banded Gastroplasty
• 1997 one first surgeons laparoscopic RNY • Mini-Gastric Bypass; 14 years, over 6,000 cases
Dr. Rutledge
USA 001-702-714-0011 [email protected]
CONSIDERING THE MGB?MGB IS A SUPERB SURGERY BUT…
WARNING: “THERE ARE “TRICKS AND TRAPS”
OFFER A SAFE & SUCCESSFUL MGB PROGRAM
• Call / Email: Anytime question or advice on any clinical, technical or patient MGB question
• USA 001-702-714-0011 [email protected]
• Personal Visit: Dr. Rutledge Visiting Professor: France, Turkey, Austria & India, Upcoming visits Greece, Istanbul, United KingdomCzech Republic, Italy, Germany, UAE, Pakistan,
• Please Use the Knowledge of Others Before You Start; Experience; over 14 years, over 6,000 patients
• USA 001-702-714-0011 [email protected]
UPCOMING “HANDS ON” MGB IN INDIA“TRICKS AND TRAPS” TRAINING PROGRAM
• Didactic SessionsTalk with the Leading World Experts
• Hands On Surgery (with approval)Scrub in on casesAssist and Participate in MGB Surgery
• This Fall and Next Year
• Bija India, Dr Rutledge & Dr Kular
• USA 001-702-714-0011 [email protected]
SURGERYHISTORY OF POOR DECISIONS
JOSEPH LISTER:
AMERICAN SURGEONS DELAYED ADOPTION OF ANTISEPSIS 10 YEARS
REPTILIAN BRAINPOOR DECISION MAKING
• Lister published antisepsis
paper:
• 1867
Dr. Gross; Gross Clinic 1875
Definition of the Problem
• Obesity Epidemic
• History of Failure of Bariatric Surgical Procedures
• Selecting the “Ideal / BEST” Bariatric Surgical Procedure
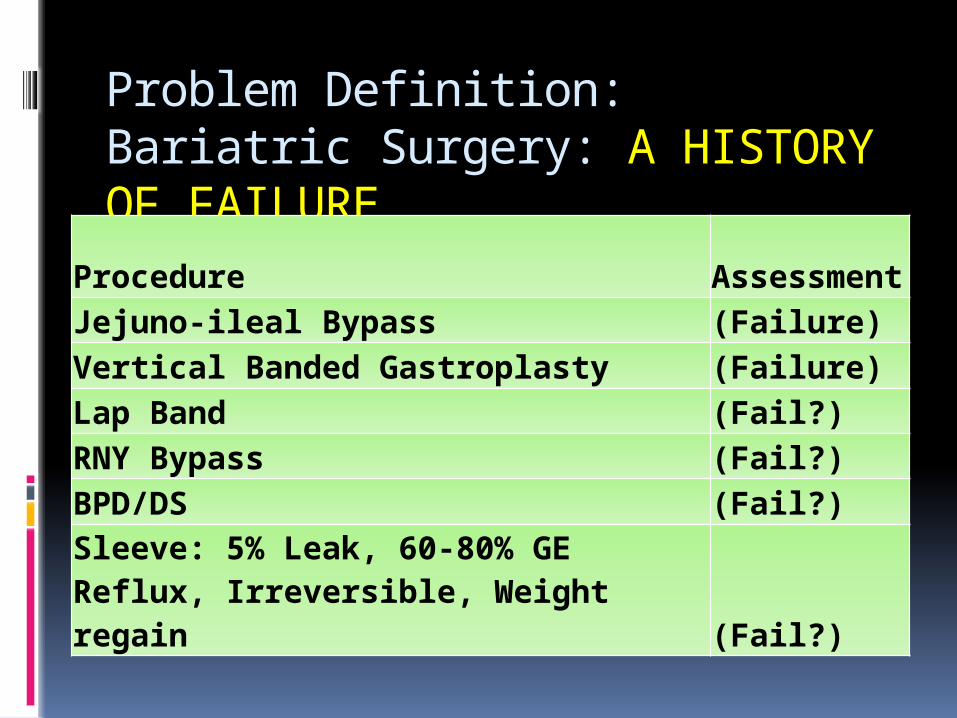
Problem Definition:Bariatric Surgery: A HISTORY OF FAILURE
ProcedureAssessment
Jejuno-ileal Bypass (Failure)Vertical Banded Gastroplasty (Failure)Lap Band (Fail?)RNY Bypass (Fail?)BPD/DS (Fail?)Sleeve: 5% Leak, 60-80% GE Reflux, Irreversible, Weight regain (Fail?)
THE GASTRIC SLEEVE:NOT AS BAD AS THE BANDNOT AS DANGEROUS AS THE RNY
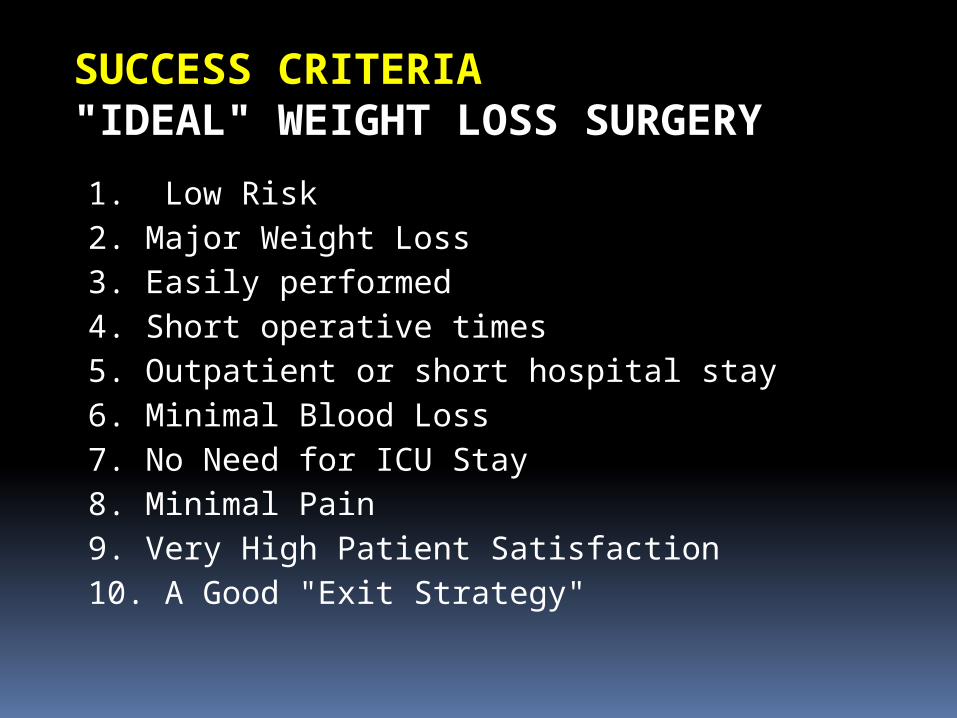
1. Low Risk2. Major Weight Loss3. Easily performed4. Short operative times5. Outpatient or short hospital stay6. Minimal Blood Loss7. No Need for ICU Stay8. Minimal Pain9. Very High Patient Satisfaction10. A Good "Exit Strategy"
SUCCESS CRITERIA"IDEAL" WEIGHT LOSS SURGERY
SUCCESS CRITERIA"IDEAL" WEIGHT LOSS SURGERY11. Change Behavior & Preferences; Marked Decrease in Hunger
and Increased Satiety12. Minimal Retching and Vomiting 13. Few adhesions or hernias14. Minimal impact on Heart and Lung Function15. Low Failure Rate16. Low Cost17. Short Recovery Time18. Rapid Return to Work19. Low Risk of Pulmonary Embolus20. Durable weight loss
SUCCESS CRITERIA"IDEAL" WEIGHT LOSS SURGERY
21. Low Risk of Ulcer22. Fat Malabsorption; low cholesterol & CV risk 23. No Plastic Foreign Body 24. Easily Verifiable Results; > 10 years of Results25. Low Risk of Bowel Obstruction26. Based upon sound surgical principles 27. Independent confirmation of results28. Healthy life after surgery29. Supported by LEVEL I Evidence; RCT (Controlled Prospective
Randomized Trial)30. Block “Sweet Eater” Failures
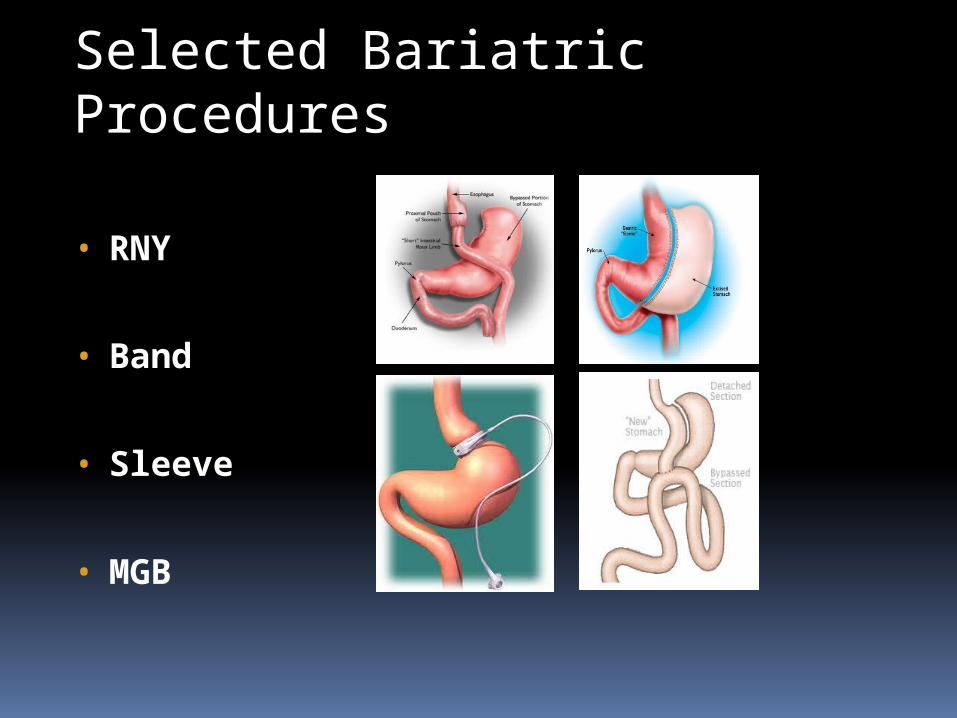
Selected Bariatric Procedures
• RNY
• Band
• Sleeve
• MGB
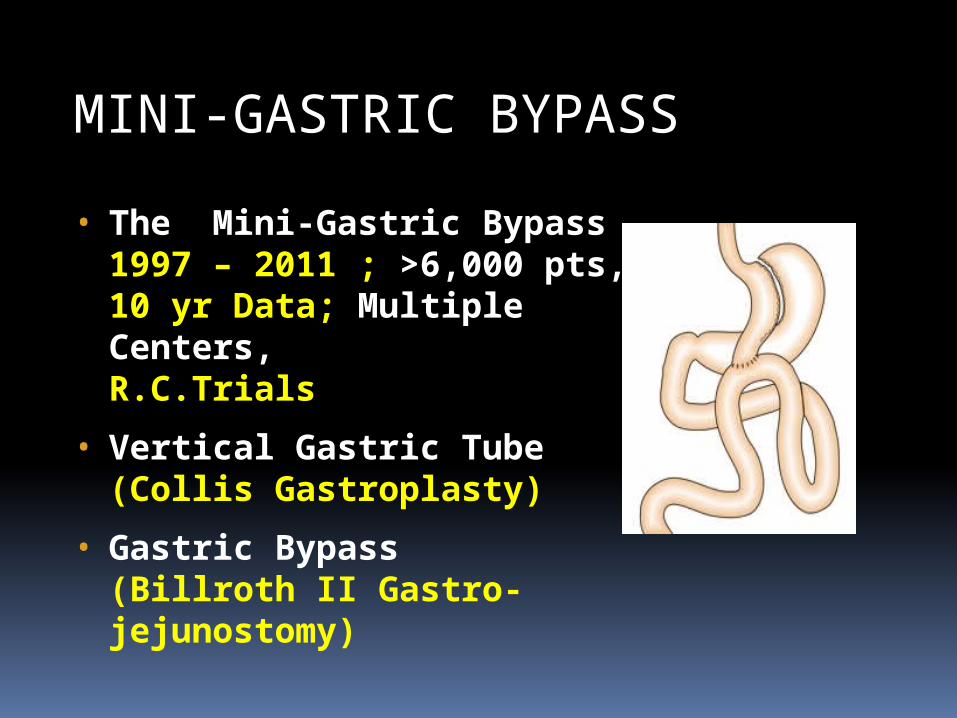
MINI-GASTRIC BYPASS
• The Mini-Gastric Bypass1997 – 2011 ; >6,000 pts, 10 yr Data; Multiple Centers, R.C.Trials
• Vertical Gastric Tube(Collis Gastroplasty)
• Gastric Bypass(Billroth II Gastro-jejunostomy)
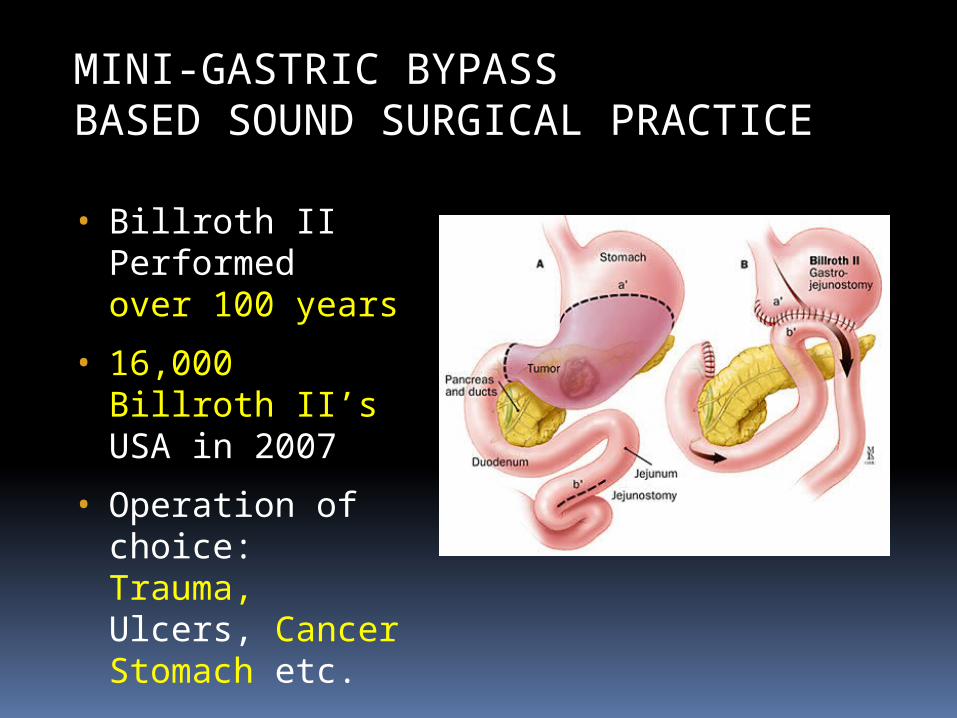
MINI-GASTRIC BYPASSBASED SOUND SURGICAL PRACTICE
• Billroth II Performed over 100 years
• 16,000 Billroth II’sUSA in 2007
• Operation of choice: Trauma, Ulcers, Cancer Stomach etc.
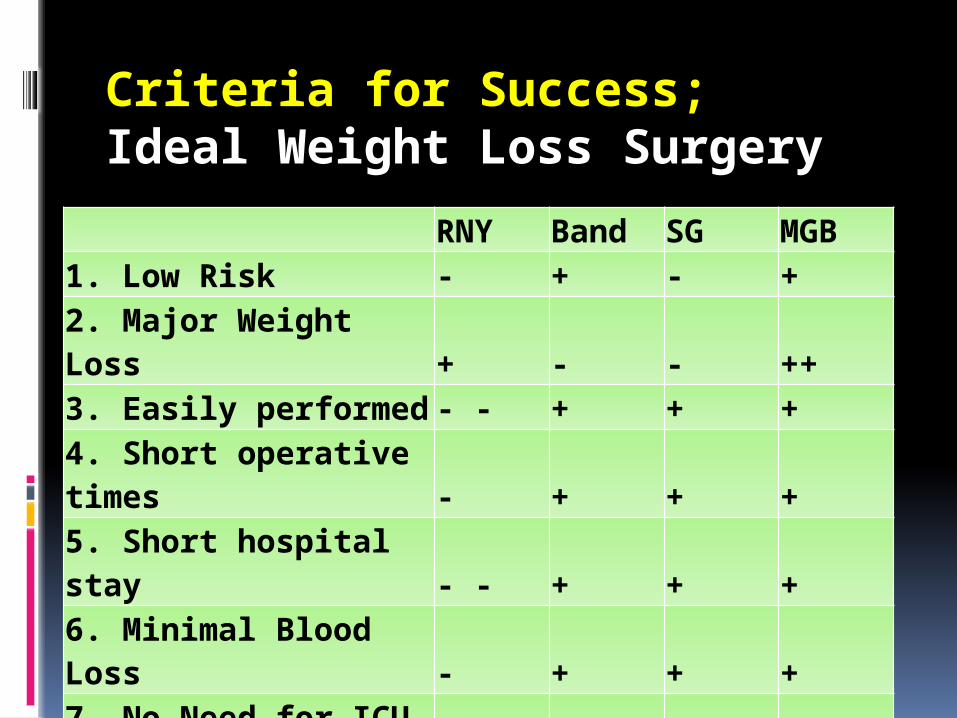
Criteria for Success; Ideal Weight Loss Surgery
RNY Band SG MGB1. Low Risk - + - +2. Major Weight Loss + - - ++3. Easily performed - - + + +4. Short operative times - + + +5. Short hospital stay - - + + +6. Minimal Blood Loss - + + +7. No Need for ICU Stay - + + +8. Minimal Pain - + + +9. High Patient Satisfaction - - - +10. A Good "Exit Strategy" - - - + - - +
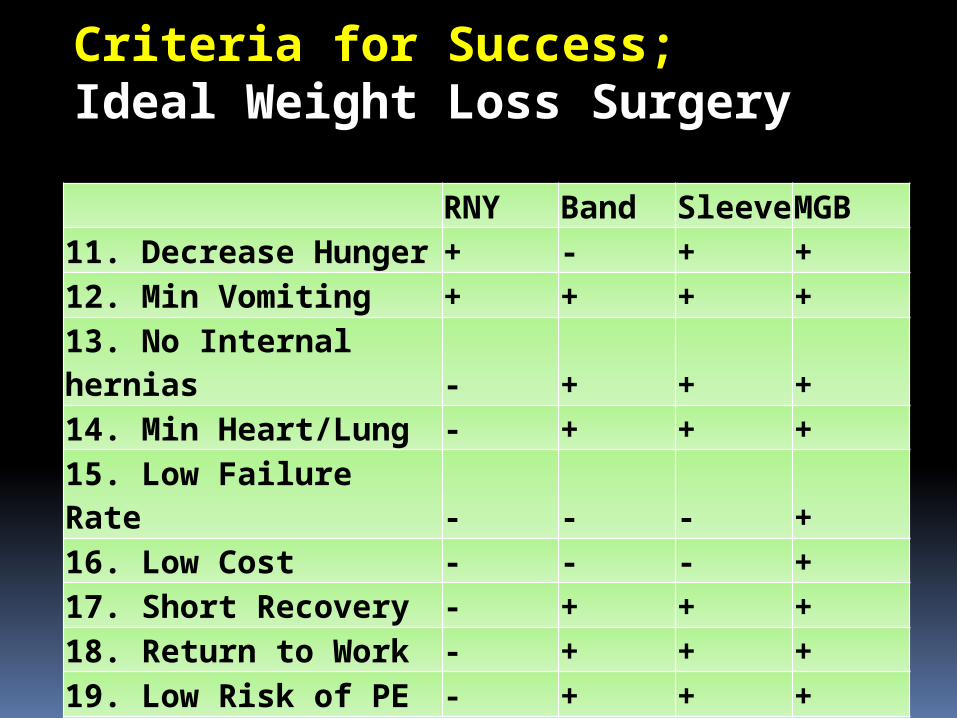
Criteria for Success; Ideal Weight Loss Surgery
RNY Band Sleeve MGB11. Decrease Hunger + - + +12. Min Vomiting + + + +13. No Internal hernias - + + +14. Min Heart/Lung - + + +15. Low Failure Rate - - - +16. Low Cost - - - +17. Short Recovery - + + +18. Return to Work - + + +19. Low Risk of PE - + + +20. Durable Weight Loss - - - +

Criteria for SuccessRNY Band SG MGB
21. Low Risk of Ulcer - + + -
22. Malabsorption of fat + - - +
23. No Foreign Body + - + +
24. Verifiable Results - - - ++
25. Bowel Obstruction - - + + ++
26. Sound Surgical + - + +
27. Independent confirm - - - ++
28. Healthy life - - - ++
29. RCT; LEVEL I Evidence - - - ++
30. Block Sweet Eater + - - ++
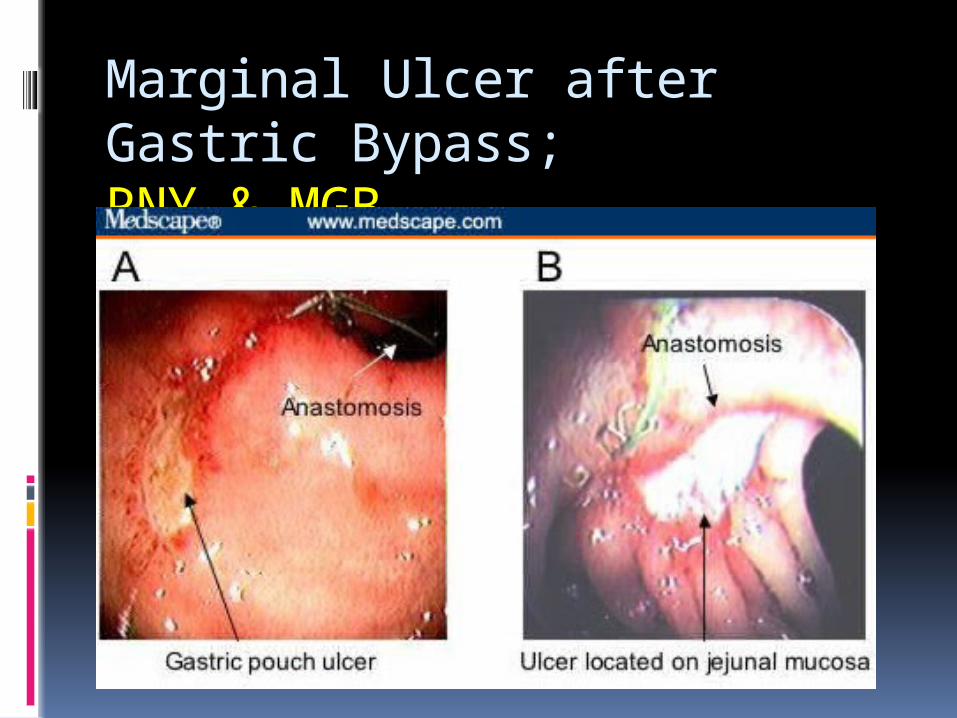
Marginal Ulcer after Gastric Bypass; RNY & MGB Marginal Ulcers after Roux-en-Y Gastric Bypass:
Pain for the Patient…Pain for the Surgeon January 2010 by Camellia Racu, Bariatric Times. 2010;7(1):23–25
Marginal Ulcer after Gastric Bypass; RNY & MGB
Marginal Ulcer after Gastric Bypass; RNY & MGB Marginal ulcers RNY ranging from 0.6 to 16% True incidence is very likely much higher Csendes prospective study
routine postoperative endoscopic evaluation 28% of marginal ulcers were asymptomatic Gastric Bypass (RNY & MGB)
HIGH incidence of Marginal Ulcer BILE MAKES NO DIFFERENCE!!!
Incidence of perforated gastrojejunal anastomotic ulcers after RNY
April 2002 to April 2010, 1213 patients underwent laparoscopic RYGB
Operative mortality was .15% 10 perforated GJA ulcers (.82%) at a mean of 13.5
(6-19) months Morbidity and mortality rate was 30% and 10% Perforated GJA ulcers can develop in 1 of 120
Roux en Y Gastric Bypasses & DEADLY
Marginal Ulcers: Achilles Heel of Gastric Bypass Management 1. Warn Patients & Surgeon “Be Vigilant” 2. Aggressive anti-H. Pylori Rx 3. Aggressive use of Antacids 4. Strict Avoidance of Ulcerogenic Agents
(NSAIDS, Etoh, Smoking, Coffee, Soda, Nitrates) 5. Encourage: Probiotics, Yogurt, Fruits Vegetables BILE MAKES NO DIFFERENCE!!!
CONCLUSIONS: Best Choice: Mini-Gastric Bypass
• Choice of Obesity Surgery
• Objectives “Ideal” Weight Loss Surgery
• RNY, Band, Sleeve, MGB
• MGB Best meets all objectives/success criteria
• Beware of Marginal Ulcer
• Rational Decision Making: Best Choice; Mini-Gastric Bypass
WHY CRITICS ONLY CARE FOR MGB?• Why do Critics only care about the
Mini-Gastric Bypass?
• 100,000’s of people already have and are living with and are getting the Billroth II every day
• Why haven’t concerned bariatric surgeons stepped forward to stop all general, trauma and oncologic surgeons from performing this Billroth II surgery?
WHY CRITICS ONLY CARE FOR MGB?•Why do Critics only care about the
Mini-Gastric Bypass?
•Why haven’t concerned bariatric surgeons stepped forward to start a fund to help suffering Billroth II patients get needed conversions of their surgery to Roux-en-Y?
•Why don’t they write letters to the editor calling for the Billroth II to be declared a operation non-grata?
WHY CRITICS ONLY CARE FOR MGB?• Why do Critics only care about the
Mini-Gastric Bypass?
• Why haven’t concerned bariatric surgeons stepped forward to national funding for lifetime endoscopic screening of Billroth II patients to find dreaded gastric cancers?
• It seems odd doesn’t it?
• There is a simple reason
WHY CRITICS ONLY CARE FOR MGB?• There is a simple reason
• The critics of the MGB do not do those things because they are ridiculous
• Such actions are Not supported by the data
• The Billroth II and the MGB are both good operations
• Published data Does Not support the critics misreading of the medical literature
CRITICS OF THE MINI-GASTRIC BYPASS
SHOULD BE EMBARRASSED
Rational Data Analysis vs.Irrational FEAR Gastric Cancer
• 1. Gastric Cancer Declining Rapidly
• 2. GC Environmental Causes; Easily Prevented
• 3. Some studies show Small Increased Risk Probably from Ulcers / H. Pylori
• 4. Many large studies: NO increased risk
• 5. Endoscopic Screening: Not Recommended
• 6. General, Trauma & Oncologic Surgeons Use Billroth II