mindfulness-based stress reduction versus pharmacotherapy...
TRANSCRIPT

dp
Io2if(oi
ah
ORIGINAL RESEARCH
MINDFULNESS-BASED STRESS REDUCTION VERSUS PHARMACOTHERAPY FOR CHRONIC
PRIMARY INSOMNIA: A RANDOMIZED CONTROLLED CLINICAL TRIALCynthia R. Gross, PhD,1,2# Mary Jo Kreitzer, PhD, RN,3 Maryanne Reilly-Spong, PhD,1 Melanie Wall, PhD,4
Nicole Y. Winbush, MD,5 Robert Patterson, PhD,6 Mark Mahowald, MD,7 and Michel Cramer-Bornemann, MD7
Objective: The aim of this study was to investigate the potentialof mindfulness-based stress reduction (MBSR) as a treatment forchronic primary insomnia.
Design: A randomized controlled trial was conducted.
Setting: The study was conducted at a university health center.
Patients: Thirty adults with primary chronic insomnia based oncriteria of the Diagnostic and Statistical Manual of Mental Disor-
ers, Text Revision, 4th Edition were randomized 2:1 to MBSR orharmacotherapy (PCT).
nterventions: Mindfulness-based stress reduction, a programf mindfulness meditation training consisting of eight weekly.5 hour classes and a daylong retreat, was provided, with ongo-ng home meditation practice expectations during three-monthollow-up; PCT, consisting of three milligrams of eszopicloneLUNESTA) nightly for eight weeks, followed by three monthsf use as needed. A 10-minute sleep hygiene presentation was
ncluded in both interventions.i
stbi
poicae-mail: [email protected]
76 © 2011 Elsevier Inc. All rights reserved.ISSN 1550-8307/$36.00
Main Outcomes: The Insomnia Severity Index (ISI), PittsburghSleep Quality Index (PSQI), sleep diaries, and wrist actigraphywere collected pretreatment, posttreatment (eight weeks), and atfive months (self-reports only).
Results: Between baseline and eight weeks, sleep onset latency(SOL) measured by actigraphy decreased 8.9 minutes in the MBSRarm (P � .05). Large, significant improvements were found on theISI, PSQI, and diary-measured total sleep time, SOL, and sleepefficiency (P � .01, all) from baseline to five-month follow-up in theMBSR arm. Changes of comparable magnitude were found in thePCT arm. Twenty-seven of 30 patients completed their assignedtreatment. This study provides initial evidence for the efficacy ofMBSR as a viable treatment for chronic insomnia as measured bysleep diary, actigraphy, well-validated sleep scales, and measures ofremission and clinical recovery.
Key words: Chronic primary insomnia, mindfulness, medita-tion, sleep latency
(Explore 2011; 7:76-87. © 2011 Elsevier Inc. All rights reserved.)
INTRODUCTIONIt is estimated that close to one in 10 adults in the United Stateshas chronic insomnia, with higher rates among women, olderadults, and clinical populations.1,2 Chronic insomnia is associ-ted with many comorbidities; increased risks for depression,ypertension, and heart disease; and has a pervasive, negative
1 College of Pharmacy, University of Minnesota, Minneapolis, MN2 School of Nursing, University of Minnesota, Minneapolis, MN3 Center for Spirituality & Healing, University of Minnesota, Minneap-olis, MN4 Division of Biostatistics, University of Minnesota, Minneapolis, MN5 Department of Family Practice and Community Health, University ofMinnesota, Minneapolis, MN6 Physical Medicine and Rehabilitation, University of Minnesota, Min-neapolis, MN7 Minnesota Regional Sleep Disorders Center, Hennepin County Med-ical Center, Minneapolis, MNSupported by a faculty development grant from the Academic HealthCenter, University of Minnesota to Drs. Gross & Kreitzer and by also theNational Institutes of Health, National Center for Research Resources(grant M01 RR00400, Dr. Seaquist, PI) This trial is NCT0051577 inClinicalTrials.gov.
# Corresponding Author. Address:308 Harvard St SE, Minneapolis, MN 55455
mpact on individuals’ quality of life.3-7 Insomnia also has aprofoundly negative impact on the economy through lost pro-ductivity and increased healthcare costs.8,9 Although both cog-nitive behavioral therapy and pharmacotherapy (PCT) havebeen shown to improve sleep outcomes, most people do notobtain effective insomnia treatment.3,8,10 Complementary andalternative medicine (CAM) approaches have the potential toreduce, at least in part, the gap between the prevalence ofchronic insomnia and the number of patients effectively treated.In 2007, 1.4% of adults in the United States reported using CAMapproaches to treat insomnia or difficulty sleeping.11 However,no CAM treatments have conclusively established efficacy andsafety for treatment of chronic insomnia.1 Mindfulness-basedtress reduction (MBSR) is a mind-body based CAM interven-ion that has been identified as a potential therapy for insomniaut lacks evidence from adequately powered and controlled clin-cal trials.12
MBSR and SleepThe MBSR program was developed to facilitate adaptation to thestresses of living with chronic illness.13 The MBSR program teachesarticipants to learn how to focus their attention through a varietyf meditative techniques. Participants are trained to perceive theirmmediate emotional and physical state, including pain or dis-omfort, and to let thoughts come and go in awareness with no
ttempt to change, suppress, or elaborate on thoughts. ThroughEXPLORE March/April 2011, Vol. 7, No. 2doi:10.1016/j.explore.2010.12.003

oPaMims�
vvrr
Mi
RTaptos
1
2
3
4
MSTtM
idtbumd
mindfulness training, participants learn to view their thoughts asmental events and not facts. In this way, participants becomeexposed to the positive and negative content of their thoughtsand do not get absorbed in thought, caught up in planning forthe future, or worrying about the past. The practice of mindful-ness throughout the day is posited to enable one to skillfullyrespond to stressors with appropriate actions, as opposed toreacting “on automatic pilot” with conditioned responses thatcan be emotionally arousing or harmful. By “breaking up” cyclesof rumination and worry, mindfulness is hypothesized to reduce“verbal overregulation” and facilitate the disengagement neces-sary to fall asleep.14
Mindfulness programs have been found to improve sleepquality in longitudinal studies of patients with medical orpsychiatric illnesses.12 Patients with cancer15 and recipients
f organ transplants16,17 reported significantly improvedittsburgh Sleep Quality Index (PSQI) scores after attendingn MBSR program, with medium-to-large effect sizes forBSR (d � 0.60-0.65). Among the transplant recipients, find-
ngs supported a dose-response relationship between homeeditation practice and sleep quality: more practice was as-
ociated with a greater decline in PSQI scores (correlation,0.47; P � .04).16,17 Mindfulness-based stress reduction was
used by Bootzin and Stevens18 in a multicomponent inter-ention to improve sleep and reduce substance abuse recidi-ism among adolescents. Improvements in several sleep pa-ameters measured by diary were found, and actigraphyesults were marginally significant (P � .06) for improved
total sleep time (TST). Two studies of mindfulness-based cog-nitive therapy (MBCT), a depression-relapse prevention pro-gram modeled after MBSR that shares its mindfulness train-ing techniques, reported improved sleep outcomes forpatients with mood and anxiety disorders.19,20 The impact of
BSR on patients with primary sleep disorders has not beennvestigated.
esearch Objectivehe objective of this study was to determine if MBSR couldchieve clinically meaningful reductions in insomnia severity inatients with primary chronic insomnia. This trial was designedo be a pilot for a future full-scale comparative effectiveness trialf MBSR as a treatment for chronic insomnia. The main re-earch questions for this pilot were as follows:
. Will MBSR impact sleep quality and quantity as mea-sured by sleep diary, actigraphy, and standardized scalesat eight weeks, and if so, are impacts sustained at five-month follow-up?
. Are the magnitudes of MBSR effects on sleep outcomesgenerally comparable to the impact of nightly use of a Foodand Drug Administration (FDA)–approved sedative hyp-notic?
. Will MBSR show benefit to health-related quality of life andreduce activity impairment among chronic insomnia pa-tients?
. Are relationships between sleep outcomes and medi-tation practice time consistent with a dose-response
relationship?Mindfulness for Insomnia
ETHODStudy Design and Sample Sizehis was a two-group randomized, controlled pilot study. Pa-
ients were stratified by gender and then randomized 2:1 toBSR (n � 20) or PCT (n � 10) by using computer-generated
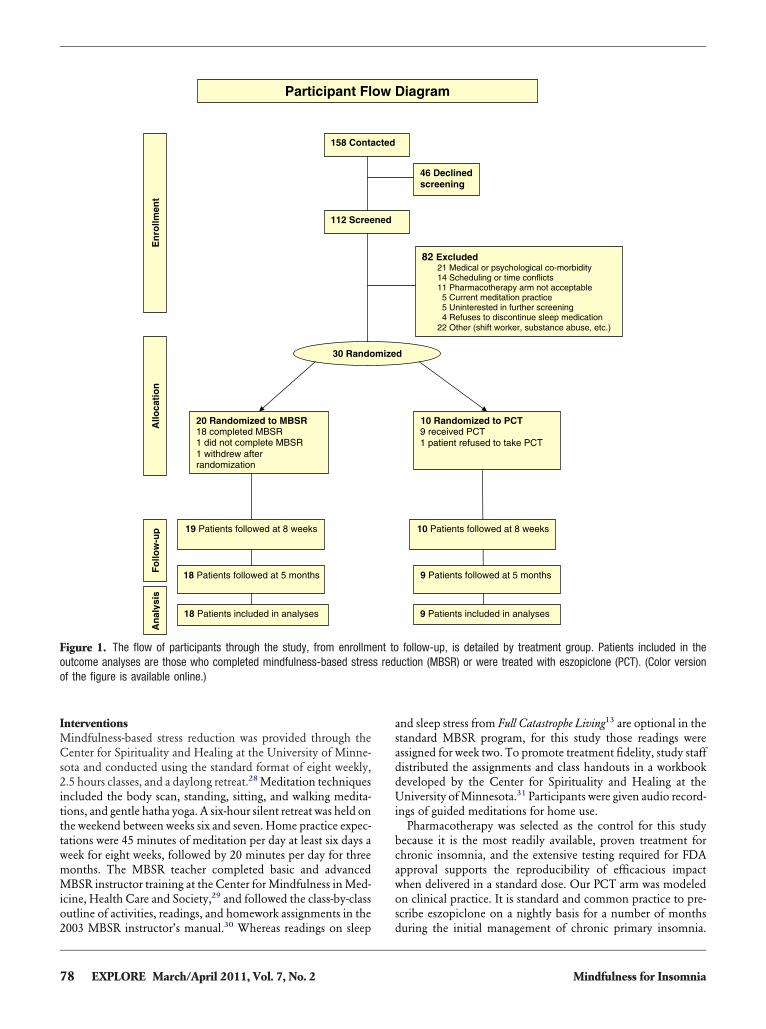
randomization schedules with small randomly permuted blocksto ensure balance within strata and across study arms (Figure 1).The study coordinator was notified by e-mail of random assign-ments after baseline data collection, and then the coordinatornotified the patient and other study personnel. Outcomes weremeasured at three time points: prerandomization baseline, endof the active intervention period, and five-month follow-up. Thepilot sample was chosen to be sufficient to detect moderate tolarge treatment effects within the MBSR group (effect size, 0.68,assuming n � 19 due to 10% dropouts, a precorrelation-postcor-relation of 0.50, 80% power, and two-sided 0.05 �).21 Based onthe pooled baseline standard deviations, this effect size corre-sponds to 2.3, 1.7, 6.3, and 4.2 points on the Insomnia SeverityIndex (ISI); PSQI; Short Form-12 version 2 Physical and MentalHealth Component Summaries; respectively, or 18.9 minutesfor sleep latency measured by sleep diary.
The study protocol was approved by the institutional reviewpanels of the University of Minnesota and the HennepinCounty Medical Center, site of the Minnesota Regional SleepDisorders Center, and all patients completed written informedconsent.
PatientsPatients were recruited between July 2007 and September 2008through newspapers, Internet, and radio advertisements, and byclinician referral. Inclusion criteria were age 18 to 65 years, abil-ity to read and speak English, and a diagnosis of primary chronicinsomnia. Chronic insomnia was defined as difficulty initiatingor maintaining sleep despite adequate opportunity for sleep,with related daytime dysfunction on three or more nights a weekfor the past six months or longer, consistent with the Diagnosticand Statistical Manual of Mental Disorders, 4th Edition Text Revi-sion (307.42)22 and International Classification of Sleep Disorders.23
A four-part screening protocol applied consensus diagnostic cri-teria for primary insomnia.24 Telephone screening was followedby a structured psychiatric interview,25 completion of a screen-ng sleep diary, and a history and physical examination con-ucted by a sleep physician.24,26,27 Persons with medical condi-ions, mental disorders, or different sleep disorders suspected ofeing directly related to the insomnia were excluded. Thosesing prescription or nonprescription sleep aids prior to enroll-ent could be included if willing to discontinue use for the
uration of the study. Patients (n � 20) who reported use ofprescription or over-the-counter sleep aids at the first stage of thescreening process were required to discontinue use prior to con-tinuation in screening. Washout periods varied, but the mini-mum period of discontinuation prior to baseline sleep data col-lection was 10 days. Of the 158 persons who initially contactedthe study, 46 declined to be screened (Figure 1). Eighty-twopersons were excluded: 69 during telephone screening and 13following the psychiatric interview or sleep physician examina-tion. Among the exclusions were 11 people who would not
accept the possibility of being randomized to PCT.77EXPLORE March/April 2011, Vol. 7, No. 2
a
InterventionsMindfulness-based stress reduction was provided through theCenter for Spirituality and Healing at the University of Minne-sota and conducted using the standard format of eight weekly,2.5 hours classes, and a daylong retreat.28 Meditation techniquesincluded the body scan, standing, sitting, and walking medita-tions, and gentle hatha yoga. A six-hour silent retreat was held onthe weekend between weeks six and seven. Home practice expec-tations were 45 minutes of meditation per day at least six days aweek for eight weeks, followed by 20 minutes per day for threemonths. The MBSR teacher completed basic and advancedMBSR instructor training at the Center for Mindfulness in Med-icine, Health Care and Society,29 and followed the class-by-classoutline of activities, readings, and homework assignments in the158 Conta
20 Randomized to MBSR 18 completed MBSR 1 did not complete MBSR 1 withdrew after randomization
En
rollm
ent
Allo
cati
on
19 Patients followed at 8 weeks
Fo
llow
-up
Participant Fl
30 Rando
18 Patients followed at 5 months
112 Scree
18 Patients included in analyses
An
aly s
is
Figure 1. The flow of participants through the study, from enrollmoutcome analyses are those who completed mindfulness-based stresof the figure is available online.)
2003 MBSR instructor’s manual.30 Whereas readings on sleep
78 EXPLORE March/April 2011, Vol. 7, No. 2
nd sleep stress from Full Catastrophe Living13 are optional in thestandard MBSR program, for this study those readings wereassigned for week two. To promote treatment fidelity, study staffdistributed the assignments and class handouts in a workbookdeveloped by the Center for Spirituality and Healing at theUniversity of Minnesota.31 Participants were given audio record-ings of guided meditations for home use.
Pharmacotherapy was selected as the control for this studybecause it is the most readily available, proven treatment forchronic insomnia, and the extensive testing required for FDAapproval supports the reproducibility of efficacious impactwhen delivered in a standard dose. Our PCT arm was modeledon clinical practice. It is standard and common practice to pre-scribe eszopiclone on a nightly basis for a number of months
82 Excluded 21 Medical or psychological co-morbidity 14 Scheduling or time conflicts 11 Pharmacotherapy arm not acceptable 5 Current meditation practice 5 Uninterested in further screening 4 Refuses to discontinue sleep medication 22 Other (shift worker, substance abuse, etc.)
10 Randomized to PCT9 received PCT 1 patient refused to take PCT
iagram
d
10 Patients followed at 8 weeks
9 Patients followed at 5 months
46 Declined screening
9 Patients included in analyses
follow-up, is detailed by treatment group. Patients included in theuction (MBSR) or were treated with eszopiclone (PCT). (Color version
cted
ow D
mize
ned
ent tos red
during the initial management of chronic primary insomnia.
Mindfulness for Insomnia

iewwodimMws
MSwswdfdssvc3“t
lrfii
dfisn1Rst
mcfoosb
swtn
hcpi(Frp
The PCT treatment consisted of three milligrams of eszopiclone(LUNESTA (R), Sepracor, Inc.) nightly for eight weeks, followedby use as needed for three months. Patients initially met in asmall group with the sleep physician, who gave instructions forproperly taking medication and explained potential side effects.Patients were then given their first 30-day supply of three-milli-gram eszopiclone tablets in a bottle with a Medication EventMonitoring System cap (MEMS cap). Refills were mailed. Pa-tients were instructed to pour refill tablets into the MEMScapped bottle when taking their next pill. The MEMS cap re-cords a date/time stamp when opened but provides no feedbackto the patient. Patients were told that the MEMS cap recordsadherence.
Adherence was also tracked electronically in the MBSRarm. Participants were instructed to turn on a logger whenthey began a meditation or yoga session and to switch thelogger off at the end of the session. The logger, a pocket-sized,battery-operated recording device (HOBO data logger, OnsetComputer Corporation, Pocasset, MA) stores a date/timestamp whenever it is switched on or off and provides nofeedback to the patient. Patients were told that the loggerrecords practice time.
A 10-minute presentation about sleep hygiene was given at thefirst MBSR class and at the PCT group meeting with the sleepphysician. Sleep hygiene booklets developed at the NationalInstitutes of Health32 were distributed to all patients to standard-ze knowledge of sleep hygiene across treatment arms. Adversevents were monitored in both treatment arms. Monitoring callsere made weekly during the first eight weeks, tapered to bi-eekly in month three, and once in months four and five. A callne month after study completion monitored for problems withrug discontinuation (PCT arm only). In the MBSR arm, mon-toring calls also promoted regular meditation practice. The
onitoring calls were made by study research staff, not theBSR teacher or sleep physician. In cases where adverse events
ere reported in the PCT arm, the sleep physician was con-ulted. No adverse events were reported in the MBSR arm.
easuresleep diaries, wrist actigraphy, and self-report questionnairesere used to measure outcomes. Participants kept a standard
leep diary and wore a wrist actigraph on their nondominantrist for 14 days prior to the start of the study interventions,uring the final two weeks of the active intervention period, andor two weeks during month five (sleep diary only). The sleepiary variables are averages at each interval and include TST,leep onset latency (SOL), wake after sleep onset (WASO), andleep efficiency (SE, time asleep divided by time in bed). Theseariables were also objectively estimated using actigraphy re-ordings (Actiwatch AW64, analyzed by Actiware Sleep, version.4, Mini Mitter Company, Inc, Bend, OR).26 Benchmarks forpoor sleep” are SOL or WASO of 30 minutes or more, TST lesshan six hours, and SE under 85%.
Standardized measures of sleep and health-related quality ofife were reported in questionnaires completed at home andeturned by mail at prerandomization baseline, eight weeks, andve months. The seven-item ISI assesses the current severity of
nsomnia symptoms, sleep dissatisfaction, daytime impacts, and
Mindfulness for Insomnia
istress about sleep difficulties.33 Each ISI item is rated on ave-point scale, with total scores ranging from zero to 28. In-omnia Severity Index clinical cut points are defined as follows:o insomnia (zero to seven), subthreshold insomnia (eight to4), moderate insomnia (15-21), and severe insomnia (22-28).esponse to treatment on the ISI has been defined as a change of
even or more points from baseline, and remission as reductiono a score less than eight.34
The PSQI measures sleep quality and quantity, based on recallof sleep behaviors in the past month.35,36 The 19 PSQI questions
easure seven domains of sleep: quality, latency, duration, effi-iency, disturbances, use of sleep medications, and daytime dys-unction. Domain scores are coded from zero to three, and anverall PSQI score is obtained by summing across domains. Theverall PSQI score can range from zero to 21, three points con-titutes a meaningful change, and a score greater than five haseen proposed to identify poor sleepers.The Dysfunctional Beliefs and Attitudes about Sleep mea-
ures perceived consequences of insomnia, helplessness andorry about sleep, sleep expectations, and physical and emo-
ional attributions that are hypothesized to perpetuate insom-ia.27,37 Sixteen statements are rated on a zero-to-10 scale and
averaged, with higher scores indicating more dysfunction. TheSleep Self-Efficacy Scale consists of nine items that measureconfidence in perceived ability to engage in behaviors that in-fluence sleep.38 Item responses were scored on a zero-to-10 scaleand then averaged, with higher scores indicating greater confi-dence.39
Secondary outcomes include widely used, well-validated mea-sures of anxiety, depression, health-related quality of life, andactivity limitation. The 20-item State-Trait Anxiety Inventory,state version, was used to measure anxiety at the present time.40
Scores range from 20 to 80, and cut points have been proposedfor mild (�40), moderate (40-59), and severe (�60) anxietysymptoms. Depression symptom intensity was measured by the20-item Center for Epidemiologic Studies Depression Scale;scores range from zero to 60, and a score of 16 or higher has beenproposed to identify clinically meaningful depression symp-toms.41
Health-related quality of life was measured by mental andphysical component summary scores of the Short Form-12, ver-sion 2.42 The Short Form-12 items measure the eight aspects of
ealth and well-being that form the SF-36 health profile: physi-al functioning, role limitations due to physical health, bodilyain, general health perceptions, energy/fatigue, social function-ng, role limitations due to emotional health, and mental healthpsychological distress and emotional well-being). The Shortorm-12 mental component and physical component summa-ies are unbiased, close approximations to their SF-36 counter-arts.43 Activity impairment was assessed by a question that asks,
“In the last 7 days, to what extent did insomnia affect your abilityto carry out normal daily activities, not including your job?”with responses marked on an 11-point scale, with zero being“Insomnia did not affect my daily activities,” to 10 being “In-somnia did not permit me to do daily activities at all.”44 It isexpressed as an impairment percentage, with higher scores indi-
cating more impairment.79EXPLORE March/April 2011, Vol. 7, No. 2
aprcmuaC
RTimnduattapw
c5tvaS
Statistical AnalysisThe balance between treatment groups on baseline variables wasexamined using descriptive statistics, Fisher exact tests, andMann-Whitney U tests. Changes from baseline to eight weeksand to five months were tested within treatment groups by usingpaired t tests or by Wilcoxon tests when normality could not beassumed.45 Cohen’s d effect sizes were estimated by the differ-ence between follow-up and baseline values divided by thepooled standard deviation at baseline.21 Cohen’s criteria forsmall, medium, and large treatment effects are 0.2, 0.5, and 0.8,respectively.46 Repeated measures analyses of variance were con-ducted to compare outcomes between groups over time, al-though only very large differences would be detectable in thispilot study. Clinical importance was estimated by examining“percent recovered” in conjunction with using the reliablechange index,47 which requires that a patient’s outcome scoremoves from the abnormal to the normal range, and moreover,that the amount of change exceeds measurement error, based onthe reliability of the outcome scale.
For all efficacy analyses, three patients were omitted: onepatient randomized to PCT who refused to take the studymedication; one patient who withdrew after randomizationto MBSR, failing to return baseline data and without attend-ing any intervention sessions; and one patient who attendedonly four MBSR classes (attendance at five or more classes isthe benchmark for MBSR course completion48). Sample sizesre indicated for each analysis; missing data were not im-uted. Adherence and treatment satisfaction were summa-ized using descriptive statistics. Meditation practice time wasorrelated with change in primary outcomes by using Spear-an’s rho correlations. Descriptive statistics were obtained
sing SPSS 17.0 (SPSS Inc, Chicago, IL). All other statisticalnalyses were conducted using SAS 9.1 (SAS Institute Inc,ary, NC).
ESULTShe sample consisted of 22 women and eight men, who ranged
n age from 19 to 65 years and were well educated (Table 1). Theajority (80%) were working full or part-time. History of insom-
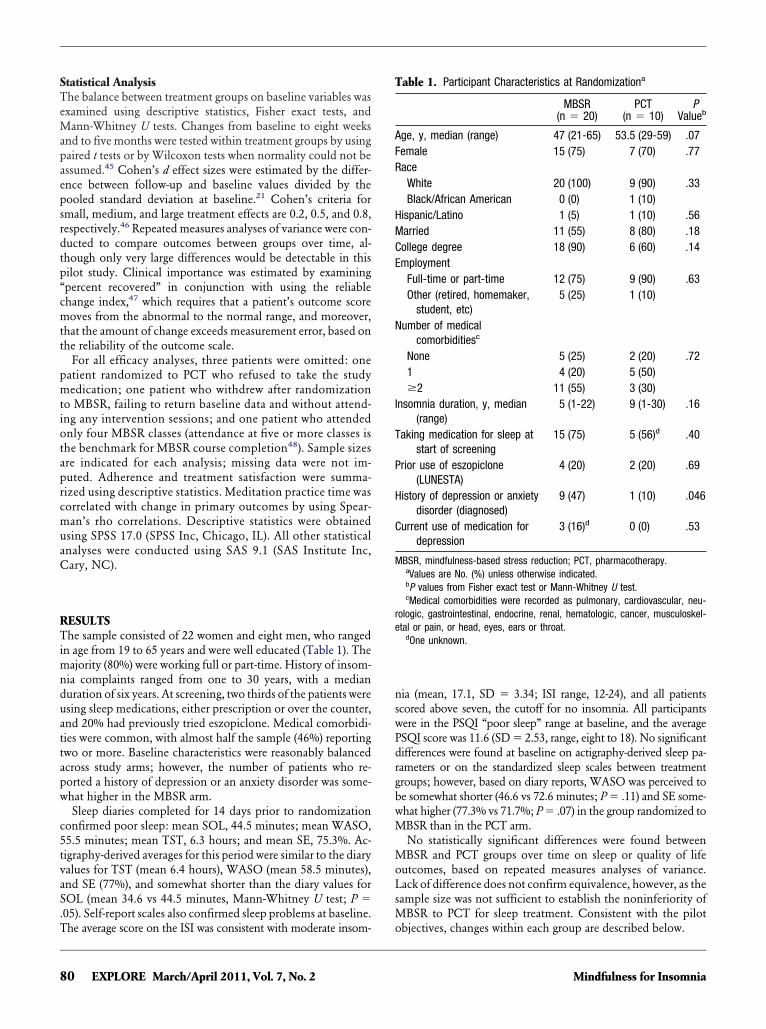
ia complaints ranged from one to 30 years, with a medianuration of six years. At screening, two thirds of the patients weresing sleep medications, either prescription or over the counter,nd 20% had previously tried eszopiclone. Medical comorbidi-ies were common, with almost half the sample (46%) reportingwo or more. Baseline characteristics were reasonably balancedcross study arms; however, the number of patients who re-orted a history of depression or an anxiety disorder was some-hat higher in the MBSR arm.Sleep diaries completed for 14 days prior to randomization
onfirmed poor sleep: mean SOL, 44.5 minutes; mean WASO,5.5 minutes; mean TST, 6.3 hours; and mean SE, 75.3%. Ac-igraphy-derived averages for this period were similar to the diaryalues for TST (mean 6.4 hours), WASO (mean 58.5 minutes),nd SE (77%), and somewhat shorter than the diary values forOL (mean 34.6 vs 44.5 minutes, Mann-Whitney U test; P �
.05). Self-report scales also confirmed sleep problems at baseline.
The average score on the ISI was consistent with moderate insom-80 EXPLORE March/April 2011, Vol. 7, No. 2
nia (mean, 17.1, SD � 3.34; ISI range, 12-24), and all patientsscored above seven, the cutoff for no insomnia. All participantswere in the PSQI “poor sleep” range at baseline, and the averagePSQI score was 11.6 (SD � 2.53, range, eight to 18). No significantdifferences were found at baseline on actigraphy-derived sleep pa-rameters or on the standardized sleep scales between treatmentgroups; however, based on diary reports, WASO was perceived tobe somewhat shorter (46.6 vs 72.6 minutes; P � .11) and SE some-what higher (77.3% vs 71.7%; P � .07) in the group randomized toMBSR than in the PCT arm.
No statistically significant differences were found betweenMBSR and PCT groups over time on sleep or quality of lifeoutcomes, based on repeated measures analyses of variance.Lack of difference does not confirm equivalence, however, as thesample size was not sufficient to establish the noninferiority ofMBSR to PCT for sleep treatment. Consistent with the pilot
Table 1. Participant Characteristics at Randomizationa
MBSR(n � 20)
PCT(n � 10)
PValueb
Age, y, median (range) 47 (21-65) 53.5 (29-59) .07Female 15 (75) 7 (70) .77Race
White 20 (100) 9 (90) .33Black/African American 0 (0) 1 (10)
Hispanic/Latino 1 (5) 1 (10) .56Married 11 (55) 8 (80) .18College degree 18 (90) 6 (60) .14Employment
Full-time or part-time 12 (75) 9 (90) .63Other (retired, homemaker,
student, etc)5 (25) 1 (10)
Number of medicalcomorbiditiesc
None 5 (25) 2 (20) .721 4 (20) 5 (50)�2 11 (55) 3 (30)
Insomnia duration, y, median(range)
5 (1-22) 9 (1-30) .16
Taking medication for sleep atstart of screening
15 (75) 5 (56)d .40
Prior use of eszopiclone(LUNESTA)
4 (20) 2 (20) .69
History of depression or anxietydisorder (diagnosed)
9 (47) 1 (10) .046
Current use of medication fordepression
3 (16)d 0 (0) .53
MBSR, mindfulness-based stress reduction; PCT, pharmacotherapy.aValues are No. (%) unless otherwise indicated.bP values from Fisher exact test or Mann-Whitney U test.cMedical comorbidities were recorded as pulmonary, cardiovascular, neu-
rologic, gastrointestinal, endocrine, renal, hematologic, cancer, musculoskel-etal or pain, or head, eyes, ears or throat.
dOne unknown.
objectives, changes within each group are described below.
Mindfulness for Insomnia
.Wosmsiv
AAcesi�t
a
T
lS
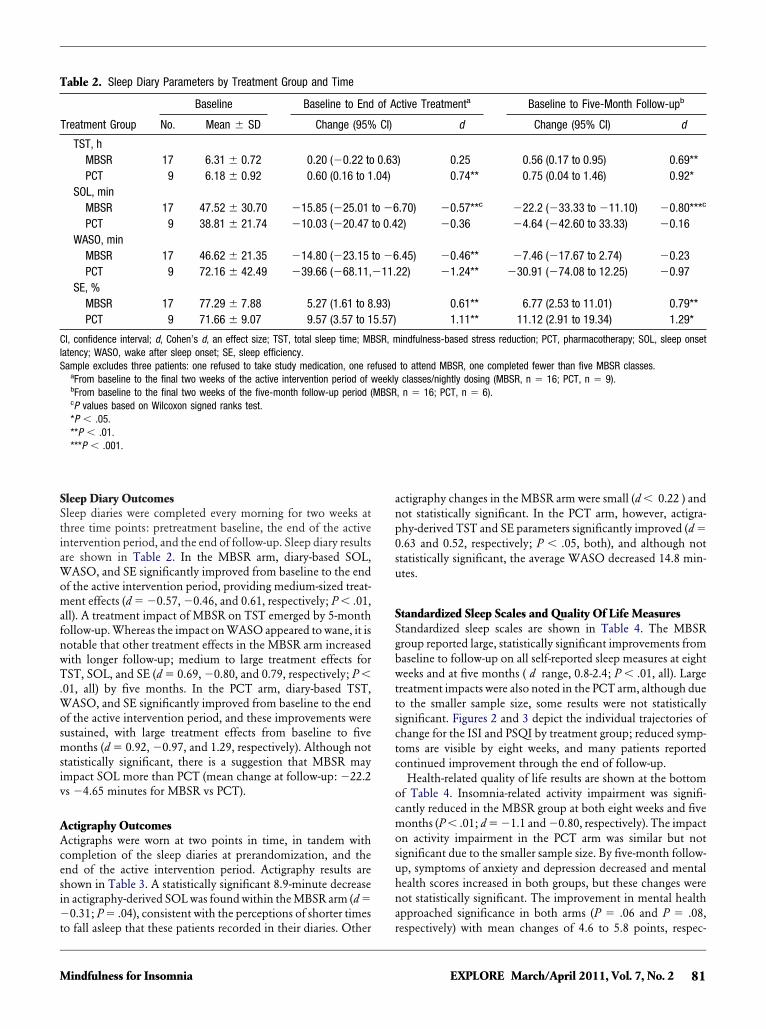
Sleep Diary OutcomesSleep diaries were completed every morning for two weeks atthree time points: pretreatment baseline, the end of the activeintervention period, and the end of follow-up. Sleep diary resultsare shown in Table 2. In the MBSR arm, diary-based SOL,WASO, and SE significantly improved from baseline to the endof the active intervention period, providing medium-sized treat-ment effects (d � �0.57, �0.46, and 0.61, respectively; P � .01,all). A treatment impact of MBSR on TST emerged by 5-monthfollow-up. Whereas the impact on WASO appeared to wane, it isnotable that other treatment effects in the MBSR arm increasedwith longer follow-up; medium to large treatment effects forTST, SOL, and SE (d � 0.69, �0.80, and 0.79, respectively; P �01, all) by five months. In the PCT arm, diary-based TST,
ASO, and SE significantly improved from baseline to the endf the active intervention period, and these improvements wereustained, with large treatment effects from baseline to fiveonths (d � 0.92, �0.97, and 1.29, respectively). Although not
tatistically significant, there is a suggestion that MBSR maympact SOL more than PCT (mean change at follow-up: �22.2s �4.65 minutes for MBSR vs PCT).
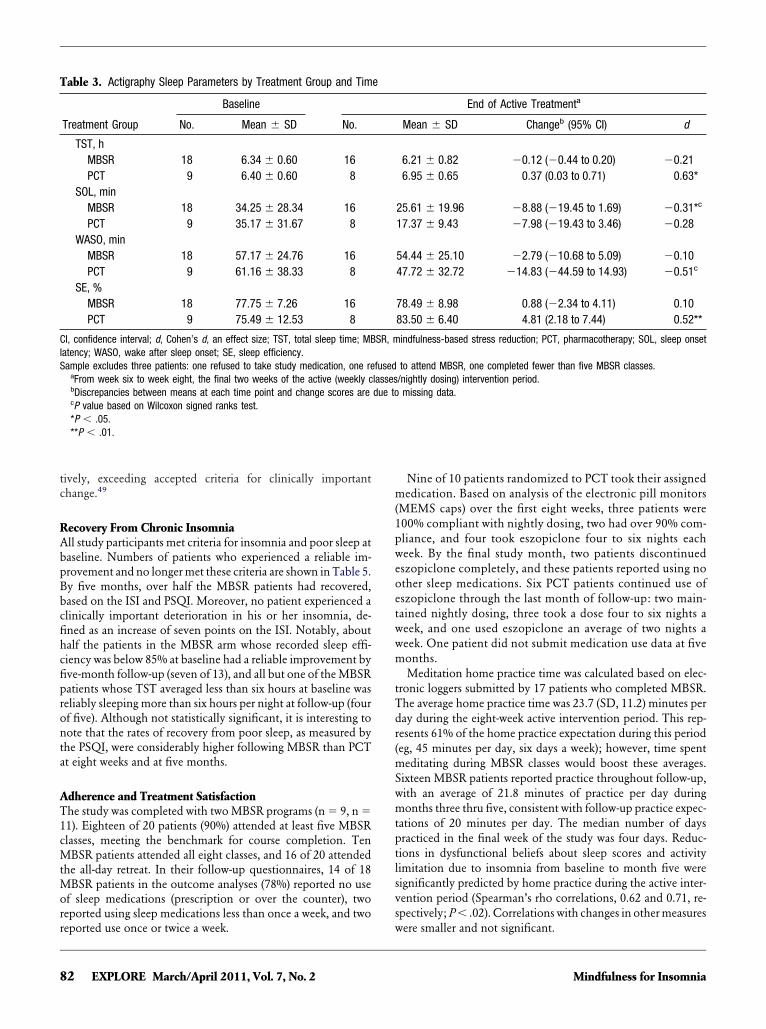
ctigraphy Outcomesctigraphs were worn at two points in time, in tandem withompletion of the sleep diaries at prerandomization, and thend of the active intervention period. Actigraphy results arehown in Table 3. A statistically significant 8.9-minute decreasen actigraphy-derived SOL was found within the MBSR arm (d �
0.31; P � .04), consistent with the perceptions of shorter times
able 2. Sleep Diary Parameters by Treatment Group and Time
Baseline Baseline to End
Treatment Group No. Mean � SD Change (95%
TST, hMBSR 17 6.31 � 0.72 0.20 (�0.22 toPCT 9 6.18 � 0.92 0.60 (0.16 to 1
SOL, minMBSR 17 47.52 � 30.70 �15.85 (�25.01PCT 9 38.81 � 21.74 �10.03 (�20.47
WASO, minMBSR 17 46.62 � 21.35 �14.80 (�23.15PCT 9 72.16 � 42.49 �39.66 (�68.11,
SE, %MBSR 17 77.29 � 7.88 5.27 (1.61 to 8PCT 9 71.66 � 9.07 9.57 (3.57 to 1
CI, confidence interval; d, Cohen’s d, an effect size; TST, total sleep time; MBatency; WASO, wake after sleep onset; SE, sleep efficiency.ample excludes three patients: one refused to take study medication, one re
aFrom baseline to the final two weeks of the active intervention period of wbFrom baseline to the final two weeks of the five-month follow-up period (cP values based on Wilcoxon signed ranks test.*P � .05.**P � .01.***P � .001.
o fall asleep that these patients recorded in their diaries. Other r
Mindfulness for Insomnia
ctigraphy changes in the MBSR arm were small (d � 0.22 ) andnot statistically significant. In the PCT arm, however, actigra-phy-derived TST and SE parameters significantly improved (d �0.63 and 0.52, respectively; P � .05, both), and although notstatistically significant, the average WASO decreased 14.8 min-utes.
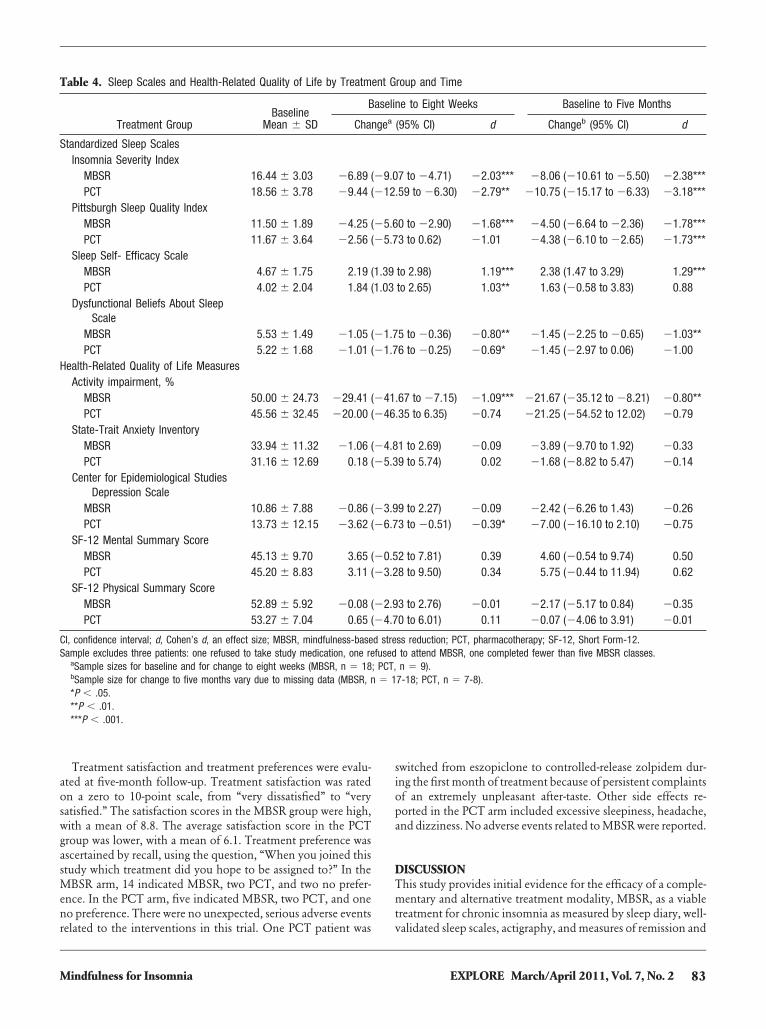
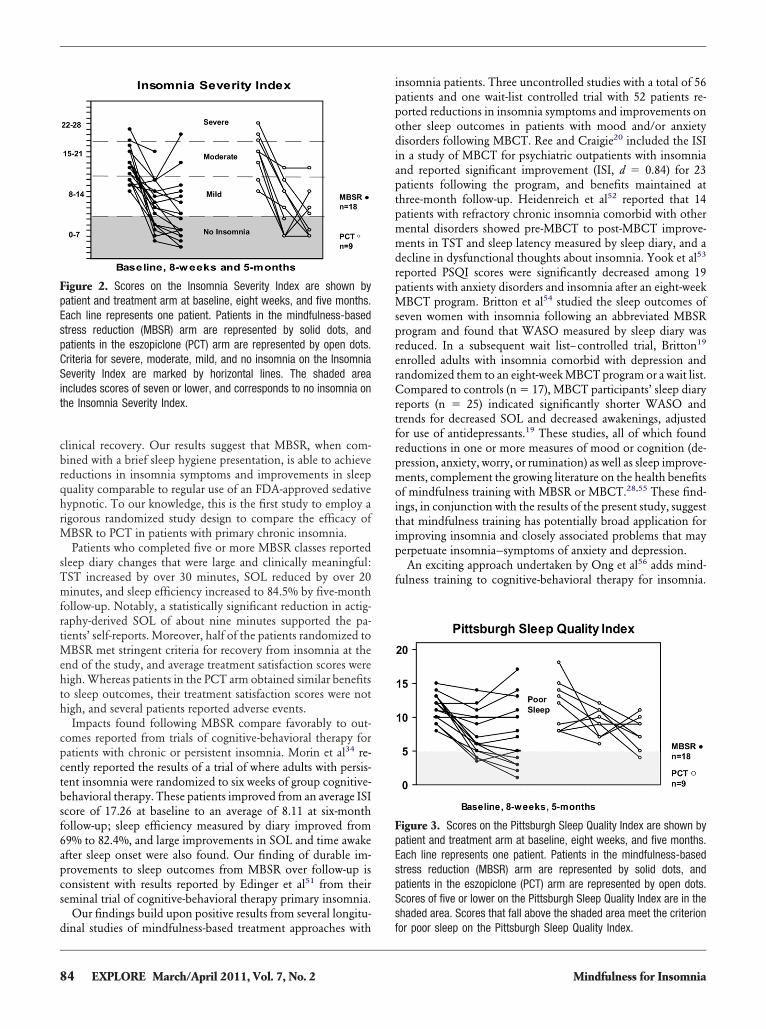
Standardized Sleep Scales and Quality Of Life MeasuresStandardized sleep scales are shown in Table 4. The MBSRgroup reported large, statistically significant improvements frombaseline to follow-up on all self-reported sleep measures at eightweeks and at five months ( d range, 0.8-2.4; P � .01, all). Largetreatment impacts were also noted in the PCT arm, although dueto the smaller sample size, some results were not statisticallysignificant. Figures 2 and 3 depict the individual trajectories ofchange for the ISI and PSQI by treatment group; reduced symp-toms are visible by eight weeks, and many patients reportedcontinued improvement through the end of follow-up.
Health-related quality of life results are shown at the bottomof Table 4. Insomnia-related activity impairment was signifi-cantly reduced in the MBSR group at both eight weeks and fivemonths (P � .01; d � �1.1 and �0.80, respectively). The impacton activity impairment in the PCT arm was similar but notsignificant due to the smaller sample size. By five-month follow-up, symptoms of anxiety and depression decreased and mentalhealth scores increased in both groups, but these changes werenot statistically significant. The improvement in mental healthapproached significance in both arms (P � .06 and P � .08,
ctive Treatmenta Baseline to Five-Month Follow-upb
d Change (95% CI) d
) 0.25 0.56 (0.17 to 0.95) 0.69**0.74** 0.75 (0.04 to 1.46) 0.92*
.70) �0.57**c �22.2 (�33.33 to �11.10) �0.80***c
2) �0.36 �4.64 (�42.60 to 33.33) �0.16
.45) �0.46** �7.46 (�17.67 to 2.74) �0.2322) �1.24** �30.91 (�74.08 to 12.25) �0.97
0.61** 6.77 (2.53 to 11.01) 0.79**1.11** 11.12 (2.91 to 19.34) 1.29*
indfulness-based stress reduction; PCT, pharmacotherapy; SOL, sleep onset
to attend MBSR, one completed fewer than five MBSR classes.classes/nightly dosing (MBSR, n � 16; PCT, n � 9).
, n � 16; PCT, n � 6).
of A
CI)
0.63.04)
to �6to 0.4
to �6�11.
.93)5.57)
SR, m
fusedeekly
MBSR
espectively) with mean changes of 4.6 to 5.8 points, respec-
81EXPLORE March/April 2011, Vol. 7, No. 2
lS
tively, exceeding accepted criteria for clinically importantchange.49
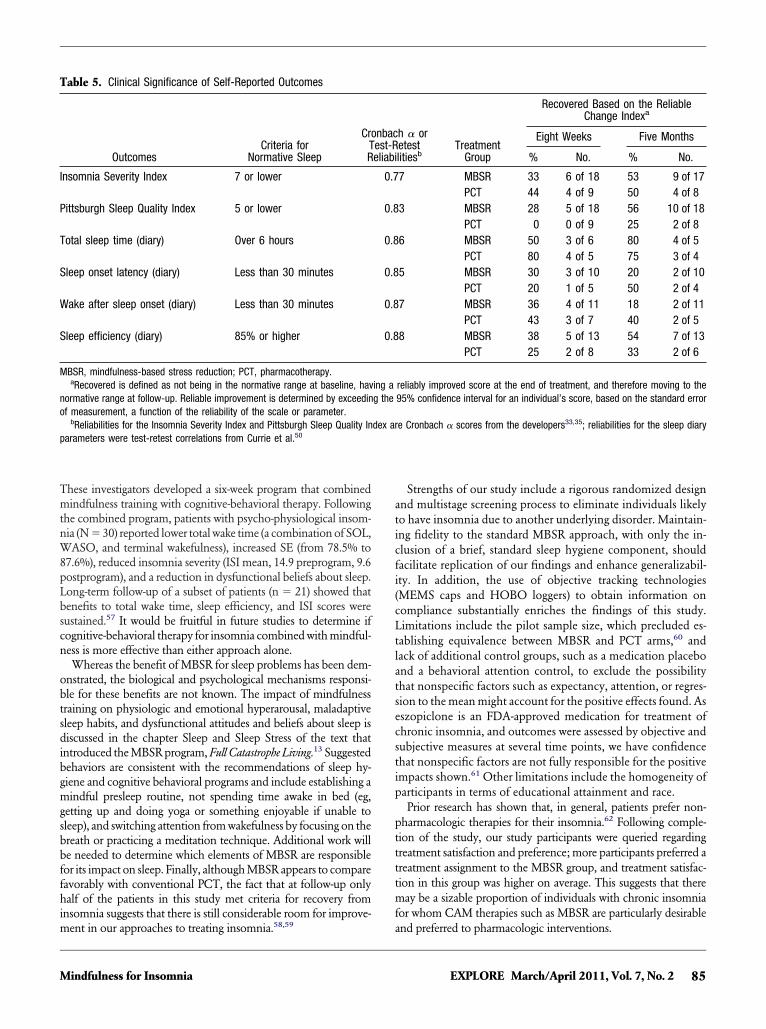
Recovery From Chronic InsomniaAll study participants met criteria for insomnia and poor sleep atbaseline. Numbers of patients who experienced a reliable im-provement and no longer met these criteria are shown in Table 5.By five months, over half the MBSR patients had recovered,based on the ISI and PSQI. Moreover, no patient experienced aclinically important deterioration in his or her insomnia, de-fined as an increase of seven points on the ISI. Notably, abouthalf the patients in the MBSR arm whose recorded sleep effi-ciency was below 85% at baseline had a reliable improvement byfive-month follow-up (seven of 13), and all but one of the MBSRpatients whose TST averaged less than six hours at baseline wasreliably sleeping more than six hours per night at follow-up (fourof five). Although not statistically significant, it is interesting tonote that the rates of recovery from poor sleep, as measured bythe PSQI, were considerably higher following MBSR than PCTat eight weeks and at five months.
Adherence and Treatment SatisfactionThe study was completed with two MBSR programs (n � 9, n �11). Eighteen of 20 patients (90%) attended at least five MBSRclasses, meeting the benchmark for course completion. TenMBSR patients attended all eight classes, and 16 of 20 attendedthe all-day retreat. In their follow-up questionnaires, 14 of 18MBSR patients in the outcome analyses (78%) reported no useof sleep medications (prescription or over the counter), tworeported using sleep medications less than once a week, and two
Table 3. Actigraphy Sleep Parameters by Treatment Group and Tim
Baseline
Treatment Group No. Mean � SD No.
TST, hMBSR 18 6.34 � 0.60 16PCT 9 6.40 � 0.60 8
SOL, minMBSR 18 34.25 � 28.34 16PCT 9 35.17 � 31.67 8
WASO, minMBSR 18 57.17 � 24.76 16PCT 9 61.16 � 38.33 8
SE, %MBSR 18 77.75 � 7.26 16PCT 9 75.49 � 12.53 8
CI, confidence interval; d, Cohen’s d, an effect size; TST, total sleep time; MBatency; WASO, wake after sleep onset; SE, sleep efficiency.ample excludes three patients: one refused to take study medication, one re
aFrom week six to week eight, the final two weeks of the active (weekly cbDiscrepancies between means at each time point and change scores arecP value based on Wilcoxon signed ranks test.*P � .05.**P � .01.
reported use once or twice a week.
82 EXPLORE March/April 2011, Vol. 7, No. 2
Nine of 10 patients randomized to PCT took their assignedmedication. Based on analysis of the electronic pill monitors(MEMS caps) over the first eight weeks, three patients were100% compliant with nightly dosing, two had over 90% com-pliance, and four took eszopiclone four to six nights eachweek. By the final study month, two patients discontinuedeszopiclone completely, and these patients reported using noother sleep medications. Six PCT patients continued use ofeszopiclone through the last month of follow-up: two main-tained nightly dosing, three took a dose four to six nights aweek, and one used eszopiclone an average of two nights aweek. One patient did not submit medication use data at fivemonths.
Meditation home practice time was calculated based on elec-tronic loggers submitted by 17 patients who completed MBSR.The average home practice time was 23.7 (SD, 11.2) minutes perday during the eight-week active intervention period. This rep-resents 61% of the home practice expectation during this period(eg, 45 minutes per day, six days a week); however, time spentmeditating during MBSR classes would boost these averages.Sixteen MBSR patients reported practice throughout follow-up,with an average of 21.8 minutes of practice per day duringmonths three thru five, consistent with follow-up practice expec-tations of 20 minutes per day. The median number of dayspracticed in the final week of the study was four days. Reduc-tions in dysfunctional beliefs about sleep scores and activitylimitation due to insomnia from baseline to month five weresignificantly predicted by home practice during the active inter-vention period (Spearman’s rho correlations, 0.62 and 0.71, re-spectively; P � .02). Correlations with changes in other measures
End of Active Treatmenta
Mean � SD Changeb (95% CI) d
6.21 � 0.82 �0.12 (�0.44 to 0.20) �0.216.95 � 0.65 0.37 (0.03 to 0.71) 0.63*
25.61 � 19.96 �8.88 (�19.45 to 1.69) �0.31*c
17.37 � 9.43 �7.98 (�19.43 to 3.46) �0.28
54.44 � 25.10 �2.79 (�10.68 to 5.09) �0.1047.72 � 32.72 �14.83 (�44.59 to 14.93) �0.51c
78.49 � 8.98 0.88 (�2.34 to 4.11) 0.1083.50 � 6.40 4.81 (2.18 to 7.44) 0.52**
indfulness-based stress reduction; PCT, pharmacotherapy; SOL, sleep onset
to attend MBSR, one completed fewer than five MBSR classes./nightly dosing) intervention period.missing data.
e
SR, m
fusedlassesdue to
were smaller and not significant.
Mindfulness for Insomnia
Treatment satisfaction and treatment preferences were evalu-ated at five-month follow-up. Treatment satisfaction was ratedon a zero to 10-point scale, from “very dissatisfied” to “verysatisfied.” The satisfaction scores in the MBSR group were high,with a mean of 8.8. The average satisfaction score in the PCTgroup was lower, with a mean of 6.1. Treatment preference wasascertained by recall, using the question, “When you joined thisstudy which treatment did you hope to be assigned to?” In theMBSR arm, 14 indicated MBSR, two PCT, and two no prefer-ence. In the PCT arm, five indicated MBSR, two PCT, and oneno preference. There were no unexpected, serious adverse events
Table 4. Sleep Scales and Health-Related Quality of Life by Treatm
BaselineMean � SD
B
Treatment Group Cha
Standardized Sleep ScalesInsomnia Severity Index
MBSR 16.44 � 3.03 �6.89 (PCT 18.56 � 3.78 �9.44 (
Pittsburgh Sleep Quality IndexMBSR 11.50 � 1.89 �4.25 (PCT 11.67 � 3.64 �2.56 (
Sleep Self- Efficacy ScaleMBSR 4.67 � 1.75 2.19 (PCT 4.02 � 2.04 1.84 (
Dysfunctional Beliefs About SleepScale
MBSR 5.53 � 1.49 �1.05 (PCT 5.22 � 1.68 �1.01 (
Health-Related Quality of Life MeasuresActivity impairment, %
MBSR 50.00 � 24.73 �29.41 (PCT 45.56 � 32.45 �20.00 (
State-Trait Anxiety InventoryMBSR 33.94 � 11.32 �1.06 (PCT 31.16 � 12.69 0.18 (
Center for Epidemiological StudiesDepression Scale
MBSR 10.86 � 7.88 �0.86 (PCT 13.73 � 12.15 �3.62 (
SF-12 Mental Summary ScoreMBSR 45.13 � 9.70 3.65 (PCT 45.20 � 8.83 3.11 (
SF-12 Physical Summary ScoreMBSR 52.89 � 5.92 �0.08 (PCT 53.27 � 7.04 0.65 (
CI, confidence interval; d, Cohen’s d, an effect size; MBSR, mindfulness-baseSample excludes three patients: one refused to take study medication, one re
aSample sizes for baseline and for change to eight weeks (MBSR, n � 18bSample size for change to five months vary due to missing data (MBSR, n*P � .05.**P � .01.***P � .001.
related to the interventions in this trial. One PCT patient was
Mindfulness for Insomnia
switched from eszopiclone to controlled-release zolpidem dur-ing the first month of treatment because of persistent complaintsof an extremely unpleasant after-taste. Other side effects re-ported in the PCT arm included excessive sleepiness, headache,and dizziness. No adverse events related to MBSR were reported.
DISCUSSIONThis study provides initial evidence for the efficacy of a comple-mentary and alternative treatment modality, MBSR, as a viabletreatment for chronic insomnia as measured by sleep diary, well-
roup and Time
e to Eight Weeks Baseline to Five Months
(95% CI) d Changeb (95% CI) d
7 to �4.71) �2.03*** �8.06 (�10.61 to �5.50) �2.38***.59 to �6.30) �2.79** �10.75 (�15.17 to �6.33) �3.18***
0 to �2.90) �1.68*** �4.50 (�6.64 to �2.36) �1.78***3 to 0.62) �1.01 �4.38 (�6.10 to �2.65) �1.73***
to 2.98) 1.19*** 2.38 (1.47 to 3.29) 1.29***to 2.65) 1.03** 1.63 (�0.58 to 3.83) 0.88
5 to �0.36) �0.80** �1.45 (�2.25 to �0.65) �1.03**6 to �0.25) �0.69* �1.45 (�2.97 to 0.06) �1.00
.67 to �7.15) �1.09*** �21.67 (�35.12 to �8.21) �0.80**
.35 to 6.35) �0.74 �21.25 (�54.52 to 12.02) �0.79
1 to 2.69) �0.09 �3.89 (�9.70 to 1.92) �0.339 to 5.74) 0.02 �1.68 (�8.82 to 5.47) �0.14
9 to 2.27) �0.09 �2.42 (�6.26 to 1.43) �0.263 to �0.51) �0.39* �7.00 (�16.10 to 2.10) �0.75
2 to 7.81) 0.39 4.60 (�0.54 to 9.74) 0.508 to 9.50) 0.34 5.75 (�0.44 to 11.94) 0.62
3 to 2.76) �0.01 �2.17 (�5.17 to 0.84) �0.350 to 6.01) 0.11 �0.07 (�4.06 to 3.91) �0.01
ss reduction; PCT, pharmacotherapy; SF-12, Short Form-12.to attend MBSR, one completed fewer than five MBSR classes.n � 9).
7-18; PCT, n � 7-8).
ent G
aselin
ngea
�9.0�12
�5.6�5.7
1.391.03
�1.7�1.7
�41�46
�4.8�5.3
�3.9�6.7
�0.5�3.2
�2.9�4.7
d strefused
; PCT,� 1
validated sleep scales, actigraphy, and measures of remission and
83EXPLORE March/April 2011, Vol. 7, No. 2
iaptpmmd
spr
tf
itip
clinical recovery. Our results suggest that MBSR, when com-bined with a brief sleep hygiene presentation, is able to achievereductions in insomnia symptoms and improvements in sleepquality comparable to regular use of an FDA-approved sedativehypnotic. To our knowledge, this is the first study to employ arigorous randomized study design to compare the efficacy ofMBSR to PCT in patients with primary chronic insomnia.
Patients who completed five or more MBSR classes reportedsleep diary changes that were large and clinically meaningful:TST increased by over 30 minutes, SOL reduced by over 20minutes, and sleep efficiency increased to 84.5% by five-monthfollow-up. Notably, a statistically significant reduction in actig-raphy-derived SOL of about nine minutes supported the pa-tients’ self-reports. Moreover, half of the patients randomized toMBSR met stringent criteria for recovery from insomnia at theend of the study, and average treatment satisfaction scores werehigh. Whereas patients in the PCT arm obtained similar benefitsto sleep outcomes, their treatment satisfaction scores were nothigh, and several patients reported adverse events.
Impacts found following MBSR compare favorably to out-comes reported from trials of cognitive-behavioral therapy forpatients with chronic or persistent insomnia. Morin et al34 re-cently reported the results of a trial of where adults with persis-tent insomnia were randomized to six weeks of group cognitive-behavioral therapy. These patients improved from an average ISIscore of 17.26 at baseline to an average of 8.11 at six-monthfollow-up; sleep efficiency measured by diary improved from69% to 82.4%, and large improvements in SOL and time awakeafter sleep onset were also found. Our finding of durable im-provements to sleep outcomes from MBSR over follow-up isconsistent with results reported by Edinger et al51 from theirseminal trial of cognitive-behavioral therapy primary insomnia.
Our findings build upon positive results from several longitu-
Figure 2. Scores on the Insomnia Severity Index are shown bypatient and treatment arm at baseline, eight weeks, and five months.Each line represents one patient. Patients in the mindfulness-basedstress reduction (MBSR) arm are represented by solid dots, andpatients in the eszopiclone (PCT) arm are represented by open dots.Criteria for severe, moderate, mild, and no insomnia on the InsomniaSeverity Index are marked by horizontal lines. The shaded areaincludes scores of seven or lower, and corresponds to no insomnia onthe Insomnia Severity Index.
dinal studies of mindfulness-based treatment approaches with
84 EXPLORE March/April 2011, Vol. 7, No. 2
insomnia patients. Three uncontrolled studies with a total of 56patients and one wait-list controlled trial with 52 patients re-ported reductions in insomnia symptoms and improvements onother sleep outcomes in patients with mood and/or anxietydisorders following MBCT. Ree and Craigie20 included the ISIn a study of MBCT for psychiatric outpatients with insomniand reported significant improvement (ISI, d � 0.84) for 23atients following the program, and benefits maintained athree-month follow-up. Heidenreich et al52 reported that 14atients with refractory chronic insomnia comorbid with otherental disorders showed pre-MBCT to post-MBCT improve-ents in TST and sleep latency measured by sleep diary, and a
ecline in dysfunctional thoughts about insomnia. Yook et al53
reported PSQI scores were significantly decreased among 19patients with anxiety disorders and insomnia after an eight-weekMBCT program. Britton et al54 studied the sleep outcomes ofeven women with insomnia following an abbreviated MBSRrogram and found that WASO measured by sleep diary waseduced. In a subsequent wait list–controlled trial, Britton19
enrolled adults with insomnia comorbid with depression andrandomized them to an eight-week MBCT program or a wait list.Compared to controls (n � 17), MBCT participants’ sleep diaryreports (n � 25) indicated significantly shorter WASO andrends for decreased SOL and decreased awakenings, adjustedor use of antidepressants.19 These studies, all of which found
reductions in one or more measures of mood or cognition (de-pression, anxiety, worry, or rumination) as well as sleep improve-ments, complement the growing literature on the health benefitsof mindfulness training with MBSR or MBCT.28,55 These find-ngs, in conjunction with the results of the present study, suggesthat mindfulness training has potentially broad application formproving insomnia and closely associated problems that mayerpetuate insomnia—symptoms of anxiety and depression.An exciting approach undertaken by Ong et al56 adds mind-
fulness training to cognitive-behavioral therapy for insomnia.
Figure 3. Scores on the Pittsburgh Sleep Quality Index are shown bypatient and treatment arm at baseline, eight weeks, and five months.Each line represents one patient. Patients in the mindfulness-basedstress reduction (MBSR) arm are represented by solid dots, andpatients in the eszopiclone (PCT) arm are represented by open dots.Scores of five or lower on the Pittsburgh Sleep Quality Index are in theshaded area. Scores that fall above the shaded area meet the criterion
for poor sleep on the Pittsburgh Sleep Quality Index.Mindfulness for Insomnia
W8pL
latsecsti
These investigators developed a six-week program that combinedmindfulness training with cognitive-behavioral therapy. Followingthe combined program, patients with psycho-physiological insom-nia (N � 30) reported lower total wake time (a combination of SOL,
ASO, and terminal wakefulness), increased SE (from 78.5% to7.6%), reduced insomnia severity (ISI mean, 14.9 preprogram, 9.6ostprogram), and a reduction in dysfunctional beliefs about sleep.ong-term follow-up of a subset of patients (n � 21) showed that
benefits to total wake time, sleep efficiency, and ISI scores weresustained.57 It would be fruitful in future studies to determine ifcognitive-behavioral therapy for insomnia combined with mindful-ness is more effective than either approach alone.
Whereas the benefit of MBSR for sleep problems has been dem-onstrated, the biological and psychological mechanisms responsi-ble for these benefits are not known. The impact of mindfulnesstraining on physiologic and emotional hyperarousal, maladaptivesleep habits, and dysfunctional attitudes and beliefs about sleep isdiscussed in the chapter Sleep and Sleep Stress of the text thatintroduced the MBSR program, Full Catastrophe Living.13 Suggestedbehaviors are consistent with the recommendations of sleep hy-giene and cognitive behavioral programs and include establishing amindful presleep routine, not spending time awake in bed (eg,getting up and doing yoga or something enjoyable if unable tosleep), and switching attention from wakefulness by focusing on thebreath or practicing a meditation technique. Additional work willbe needed to determine which elements of MBSR are responsiblefor its impact on sleep. Finally, although MBSR appears to comparefavorably with conventional PCT, the fact that at follow-up onlyhalf of the patients in this study met criteria for recovery frominsomnia suggests that there is still considerable room for improve-
Table 5. Clinical Significance of Self-Reported Outcomes
OutcomesCriteria for
Normative Sleep
CrTR
Insomnia Severity Index 7 or lower
Pittsburgh Sleep Quality Index 5 or lower
Total sleep time (diary) Over 6 hours
Sleep onset latency (diary) Less than 30 minutes
Wake after sleep onset (diary) Less than 30 minutes
Sleep efficiency (diary) 85% or higher
MBSR, mindfulness-based stress reduction; PCT, pharmacotherapy.aRecovered is defined as not being in the normative range at baseline, hav
normative range at follow-up. Reliable improvement is determined by exceedinof measurement, a function of the reliability of the scale or parameter.
bReliabilities for the Insomnia Severity Index and Pittsburgh Sleep Quality Inparameters were test-retest correlations from Currie et al.50
ment in our approaches to treating insomnia.58,59
Mindfulness for Insomnia
Strengths of our study include a rigorous randomized designand multistage screening process to eliminate individuals likelyto have insomnia due to another underlying disorder. Maintain-ing fidelity to the standard MBSR approach, with only the in-clusion of a brief, standard sleep hygiene component, shouldfacilitate replication of our findings and enhance generalizabil-ity. In addition, the use of objective tracking technologies(MEMS caps and HOBO loggers) to obtain information oncompliance substantially enriches the findings of this study.Limitations include the pilot sample size, which precluded es-tablishing equivalence between MBSR and PCT arms,60 andack of additional control groups, such as a medication placebond a behavioral attention control, to exclude the possibilityhat nonspecific factors such as expectancy, attention, or regres-ion to the mean might account for the positive effects found. Asszopiclone is an FDA-approved medication for treatment ofhronic insomnia, and outcomes were assessed by objective andubjective measures at several time points, we have confidencehat nonspecific factors are not fully responsible for the positivempacts shown.61 Other limitations include the homogeneity ofparticipants in terms of educational attainment and race.
Prior research has shown that, in general, patients prefer non-pharmacologic therapies for their insomnia.62 Following comple-tion of the study, our study participants were queried regardingtreatment satisfaction and preference; more participants preferred atreatment assignment to the MBSR group, and treatment satisfac-tion in this group was higher on average. This suggests that theremay be a sizable proportion of individuals with chronic insomniafor whom CAM therapies such as MBSR are particularly desirable
h � oretestlitiesb
TreatmentGroup
Recovered Based on the ReliableChange Indexa
Eight Weeks Five Months
% No. % No.
7 MBSR 33 6 of 18 53 9 of 17PCT 44 4 of 9 50 4 of 8
3 MBSR 28 5 of 18 56 10 of 18PCT 0 0 of 9 25 2 of 8
6 MBSR 50 3 of 6 80 4 of 5PCT 80 4 of 5 75 3 of 4
5 MBSR 30 3 of 10 20 2 of 10PCT 20 1 of 5 50 2 of 4
7 MBSR 36 4 of 11 18 2 of 11PCT 43 3 of 7 40 2 of 5
8 MBSR 38 5 of 13 54 7 of 13PCT 25 2 of 8 33 2 of 6
reliably improved score at the end of treatment, and therefore moving to the95% confidence interval for an individual’s score, based on the standard error
e Cronbach � scores from the developers33,35; reliabilities for the sleep diary
onbacest-Reliabi
0.7
0.8
0.8
0.8
0.8
0.8
ing ag the
dex ar
and preferred to pharmacologic interventions.
85EXPLORE March/April 2011, Vol. 7, No. 2

CONCLUSIONSAlthough the time commitment associated with participating inand practicing a behavioral intervention such as MBSR is morethan with medication, our results suggest that this is not a deter-rent to most of our participants. Given patient preferences, theside effects of PCT, evidence of the efficacy of MBSR, and thepotential positive benefits of meditation that go beyond man-agement of insomnia symptoms, it is important that healthcareproviders be aware of the range of nonpharmacologic therapyapproaches and that clinicians offer patients options that in-clude MBSR. Future studies of MBSR for insomnia should em-ploy larger sample sizes and longer follow-up to assess the dura-bility of treatment impacts, and include design features thatcould reveal mechanisms of action and deduce the most effec-tive components of this intervention.
AcknowledgmentWe thank the meditation instructor, Terry Pearson, and thepatients who participated in this study.
REFERENCES1. Buscemi N, Vandermeer B, Friesen C, et al. Manifestations and Man-
agement of Chronic Insomnia in Adults. Rockville, MD: Agency forHealthcare Research and Quality; 2005. AHRQ Publication No.05-E021-1.
2. Ohayon MM. Epidemiology of insomnia: what we know and whatwe still need to learn. Sleep Med Rev. 2002;6:97-111.
3. Anonymous. National Institutes of Health State-of-the-ScienceConference Final Statement on Manifestations and Management ofChronic Insomnia in Adults. Sleep. 2005;28:1049-1057.
4. Ford DE, Kamerow DB. Epidemiologic study of sleep disturbancesand psychiatric disorders. An opportunity for prevention? JAMA.1989;262:1479-1484.
5. Mallon L, Broman JE, Hetta J. Sleep complaints predict coronaryartery disease mortality in males: a 12-year follow-up study of amiddle-aged Swedish population. J Intern Med. 2002;251:207-216.
6. Suka M, Yoshida K, Sugimori H. Persistent insomnia is a predictorof hypertension in Japanese male workers. J Occup Health. 2003;45:344-350.
7. Zammit GK, Weiner J, Damato N, Sillup GP, McMillan CA. Qual-ity of life in people with insomnia. Sleep. 1999;22(suppl 2):S379-S385.
8. Colten HR, Altevogt MB. Sleep Disorders and Sleep Deprivation: AnUnmet Public Health Problem. Washington, DC: National AcademiesPress; 2006.
9. Ozminkowski R, Wang S, Walsh J. The direct and indirect costs ofuntreated insomnia in adults in the United States. Sleep. 2007;30:263-273.
10. Morin CM, LeBlanc M, Daley M, Gregoire JP, Merette C. Epidemi-ology of insomnia: prevalence, self-help treatments, consultations,and determinants of help-seeking behaviors. Sleep Med. 2006;7:123-130.
11. Barnes, P. M., Bloom, B., & Nahin, R. (2008). Complementary and Alter-native Medicine Use Among Adults and Children: United States, 2007.Center for Disease Control National Health Statistics Report #12.Available at: http://nccam.nih.gov/news/camstats/2007/72_dpi_CHARTS/chart6.htm. Accessed January 12, 2011.
12. Winbush NY, Gross CR, Kreitzer MJ. The effects of mindfulness-based stress reduction on sleep disturbance: a systematic review.
Explore (NY). 2007;3:585-591.86 EXPLORE March/April 2011, Vol. 7, No. 2
13. Kabat-Zinn J. Full Catastrophe Living: Using the Wisdom of Your Bodyand Mind to Face Stress, Pain, and Illness. New York, NY: Dell Pub-lishing; 1990.
14. Lundh LG. The role of acceptance and mindfulness in the treatmentof insomnia. J Cogn Psychother. 2005;19:29-40.
15. Carlson LE, Garland SN. Impact of mindfulness-based stress reduc-tion (MBSR) on sleep, mood, stress and fatigue symptoms in canceroutpatients. Int J Behav Med. 2005;12:278-285.
16. Gross CR, Kreitzer MJ, Russas V, Treesak C, Frazier PA, Hertz MI.Mindfulness meditation to reduce symptoms after organ transplant:a pilot study. Altern Ther Health Med. 2004;10:58-66.
17. Kreitzer MJ, Gross CR, Ye X, Russas V, Treesak C. Longitudinalimpact of mindfulness meditation on illness burden in solid-organtransplant recipients. Prog Transplant. 2005;15:166-172.
18. Bootzin RR, Stevens SJ. Adolescents, substance abuse, and the treat-ment of insomnia and daytime sleepiness. Clin Psychol Rev. 2005;25:629-644.
19. Britton W. Meditation and Depression [dissertation]. Tucson, AZ:University of Arizona; 2006.
20. Ree M, Craigie M. Outcomes following mindfulness-based cogni-tive therapy in a heterogenous sample of adult outpatients. Behav-iour Change. 2007;24:70-86.
21. Dunlop WP, Cortina JM, Vaslow JB, Burke MJ. Meta analysis ofexperiments with matched groups or repeated measures designs.Psychol Methods. 1996;1:170-177.
22. American Psychological Association. Diagnostic and Statistical Man-ual of Mental Disorders, 4th Edition. Washington, DC: American Psy-chological Association; 2000.
23. American Academy of Sleep Medicine. International Classification ofSleep Disorders: Diagnostic and Coding Manual. 2nd ed. AmericanAcademy of Sleep Medicine Chicago, Illinois; 2005.
24. Edinger JD, Bonnet MH, Bootzin RR, et al. Derivation of researchdiagnostic criteria for insomnia: report of an American Academy ofSleep Medicine Work Group. Sleep. 2004;27:1567-1596.
25. First MB, Spitzer RL, Gibbon M, Williams JBW. Structured ClinicalInterview for DSM-IV Axis I Disorders: Patient Edition (SCID I/P, Ver-sion 2.0). New York, NY: Biometrics Research Department, NewYork State Psychiatric Institute; 1997.
26. Buysse DJ, Ancoli-Israel S, Edinger JD, Lichstein KL, Morin CM.Recommendations for a standard research assessment of insomnia.Sleep. 2006;29:1155-1173.
27. Morin CM. Measuring outcomes in randomized clinical trials ofinsomnia treatments. Sleep Med Rev. 2003;7:263-279.
28. Baer R, ed. Mindfulness-Based Treatment Approaches: A Clinician’sGuide to Evidence-Base and Applications. Amsterdam, Netherlands:Elsevier Academic Press; 2006.
29. Center for Mindfulness in Medicine, Health Care and Society.Available at: http://www.umassmed.edu/cfm. Accessed January 12,2011.
30. Santorelli SF, Kabat-Zinn J, eds. Mindfulness-Based Stress ReductionProfessional Training: MBSR Curriculum Guide and Supporting Materi-als. Worcester, MA: Center for Mindfulness in Medicine, HealthCare and Society; 2002.
31. Center for Spirituality and Healing, University of Minnesota. Avail-able at: http://www.csh.umn.edu/. Accessed January 13, 2011.
32. Patlak M. Your Guide to Healthy Sleep. National Institutes of Health;2005. Report No. 06-5271, Bethesda, Maryland.
33. Bastien CH, Vallieres A, Morin CM. Validation of the InsomniaSeverity Index as an outcome measure for insomnia research. SleepMed. 2001;2:297-307.
34. Morin CM, Vallieres A, Guay B, et al. Cognitive behavioral therapy,singly and combined with medication, for persistent insomnia, A
randomized controlled trial. JAMA. 2009;301:2005-2015.Mindfulness for Insomnia

3
3
4
5
5
35. Buysse DJ, Reynolds CF, Monk TH, Berman SR, Kupfer DJ. ThePittsburgh Sleep Quality Index: a new instrument for psychiatricpractice and research. Psychiatry Res. 1989;28:193-213.
36. Carpenter JS, Andrykowski MA. Psychometric evaluation of thePittsburgh Sleep Quality Index. J Psychosom Res. 1998;45:5-13.
37. Morin CM, Blais F, Savard J. Are changes in beliefs and attitudesabout sleep related to sleep improvements in the treatment of in-somnia? Behav Res Ther. 2002;40:741-752.
8. Lacks P. Behavioral Treatment for Persistent Insomnia. New York, NY:Pergamon Press; 1987.
9. Edinger JD, Sampson WS. A primary care “friendly” cognitive be-havioral insomnia therapy. Sleep. 2003;26:177-182.
40. Spielberger C. Manual for the State-Trait Anxiety Inventory (Form Y).Redwood City, CA: Mind Garden, Inc; 1983.
41. Radloff LS. The CES-D scale: a self-report depression scale for re-search in the general population. Appl Psychol Meas. 1977;3:385-401.
42. Ware JE Jr, Kosinski MA, Turner-Bowker DM, Gandek B. How toScore Version 2 of the SF-12 Health Survey. Boston MA: QualityMetricInc. and Health Assessment Lab; 2002.
43. Ware J, Kosinski M, Dewey J. How to Score Version 2 of the SF-36(R)Health Survey. Lincoln, RI: QualityMetric Incorporated; 2000.
44. Reilly MC, Zbrozek AS, Dukes EM. The validity and reproducibil-ity of a work productivity and activity impairment instrument. Phar-macoeconomics. 1993;4:353-365.
45. Royston PJ. Approximating the Shapiro-Wilk W-Test for non-nor-mality. Stat Comput. 1992;2:117-119.
46. Cohen J. Statistical Power Analysis for the Behavioral Sciences. 2nd ed.Hillsdale, NJ: Lawrence Erlbaum Associates; 1988.
47. Jacobson NS, Roberts LJ, Berns SB, McGlinchey JB. Methods fordefining and determining the clinical significance of treatment ef-fects: description, application, and alternatives. J Consult Clin Psy-chol. 1999;67:300-307.
48. Roth B, Robbins D. Mindfulness-based stress reduction and health-related quality of life: findings from a bilingual inner-city patientpopulation. Psychosom Med. 2004;66:113-123.
9. Gross CRWyrwich KW. Criteria for evaluating quality of life mea-
surement tools. In: Verster JC, Pandi-Perumal SR, Streiner D, eds.Mindfulness for Insomnia
Sleep and Quality of Life in Clinical Medicine. Totowa, NJ: HumanaPress, Springer Publishing; 2008:19-28.
0. Currie SR, Wilson KG, Curran D. Clinical significance and predic-tors of treatment response to cognitive-behavioral therapy for in-somnia secondary to chronic pain. J Behav Med. 2002;25:135-153.
1. Edinger JD, Wohlgemuth WK, Radtke RA, Marsh GR, Quillan RE.Cognitive behavioral therapy for treatment of chronic primaryinsomnia: a randomized controlled trial. JAMA. 2001;285:1856-1864.
52. Heidenreich T, Tuin I, Pflug B, Michal M, Michalak J. Mindfulness-based cognitive therapy for persistent insomnia: a pilot study [letterto the editor]. Psychother Psychosom. 2006;75:188-189.
53. Yook K, Lee S-H, Ryu M, et al. Usefulness of mindfulness-basedcognitive therapy for treating insomnia in patients with anxietydisorders. A pilot study. J Nerv Ment Dis. 2008;196:501-503.
54. Britton W, Shapiro S, Penn P, Bootzin R. Treating insomnia withmindfulness-based stress reduction. Sleep. 2003;26:A309-A310.
55. Grossman P, Niemann L, Schmidt S, Walach H. Mindfulness-basedstress reduction and health benefits. A meta-analysis. J Psychosom Res.2004;57:35-43.
56. Ong JC, Shapiro SL, Manber R. Combining mindfulness medita-tion with cognitive-behavior therapy for insomnia: a treatment-de-velopment study. Behav Ther. 2008;39:171-182.
57. Ong JC, Shapiro SL, Manber R. Mindfulness meditation and cog-nitive behavioral therapy for insomnia: a naturalistic 12-month fol-low-up. Explore (NY). 2009;5:30-36.
58. Benca RM. Diagnosis and treatment of chronic insomnia: a review.Psychiatr Serv. 2005;56:332-343.
59. Edinger JD, Means MK. Cognitive-behavioral therapy for primaryinsomnia. Clin Psychol Rev. 2005;25:539-558.
60. Piaggio G, Elbourne DR, Altman DG, Pocock SJ, Evans SJ. Report-ing of noninferiority and equivalence randomized trials: an exten-sion of the CONSORT statement. JAMA. 2006;295:1152-1160.
61. Lindquist R, Wyman J, Talley K, Findorff M, Gross C. Design ofcontrol group conditions in clinical trials of behavioral interven-tions. J Nurs Scholarsh. 2007;39:214-221.
62. Vincent N, Lionberg C. Treatment preference and patient satisfac-
tion in chronic insomnia. Sleep. 2001;24:411-417.87EXPLORE March/April 2011, Vol. 7, No. 2