migrainous vertigo- an underdiagnosed entity
TRANSCRIPT

MIGRAINOUS VERTIGOMIGRAINOUS VERTIGOAN UNDERDIAGNOSED ENTITYAN UNDERDIAGNOSED ENTITY
DR.ANITA BHANDARIDR.ANITA BHANDARICONSULTANT NEUROTOLOGIST CONSULTANT NEUROTOLOGIST VERTIGO AND EAR CLINICVERTIGO AND EAR CLINICJAIPURJAIPUR
Vertigo, imbalance, dizziness, Vertigo, imbalance, dizziness, disequilibrium – these are all terms used disequilibrium – these are all terms used by the pt. to describe a sensation of by the pt. to describe a sensation of altered orientation to the environment.altered orientation to the environment.
They are all symptoms , not diagnoses.They are all symptoms , not diagnoses.
A careful history ,physical examination & A careful history ,physical examination & investigations can help in establishing the investigations can help in establishing the cause in most pts.cause in most pts.
The vestibular system operates The vestibular system operates below the level of consciousness. below the level of consciousness. Only when it is abnormal does the pt. Only when it is abnormal does the pt. recognize that something is wrong. recognize that something is wrong. Because a person is so rarely Because a person is so rarely conscious of his own vestibular conscious of his own vestibular system, he has a great deal of system, he has a great deal of trouble describing his symptoms.trouble describing his symptoms.
CLASSIFICATION OF VERTIGOCLASSIFICATION OF VERTIGO
OTOLOGICALOTOLOGICAL CENTRALCENTRAL MEDICAL / SYSTEMICMEDICAL / SYSTEMIC UNLOCALIZEDUNLOCALIZED
CENTRALCENTRAL
DYSFUNCTION OF CENTRAL DYSFUNCTION OF CENTRAL STR.THAT PROCESS SENSORY INPUT STR.THAT PROCESS SENSORY INPUT FROM THE INNER EARFROM THE INNER EAR
2 to 23% OF VERTIGO DIAGNOSES 2 to 23% OF VERTIGO DIAGNOSES DEPENDING ON THE SPECIALITY DEPENDING ON THE SPECIALITY SETTINGSETTING
MIGRAINE RELATED VERTIGO / MIGRAINE RELATED VERTIGO / VERTIGINOUS MIGRAINEVERTIGINOUS MIGRAINE
MYTH OR REALITY ?MYTH OR REALITY ? ADAM & VICTORADAM & VICTOR’’S PRINCIPLES OF S PRINCIPLES OF
NEUROLOGY [ 2005] – The putative NEUROLOGY [ 2005] – The putative relationship of migraine & vertigo was relationship of migraine & vertigo was mentioned earlier. This refers to otherwise mentioned earlier. This refers to otherwise mundane migraine in which vertigo is mundane migraine in which vertigo is perhaps an aura.perhaps an aura.
However literature supported by several However literature supported by several standard neurotological textbooks & standard neurotological textbooks & publications fully recognize MRV as a distinct publications fully recognize MRV as a distinct entity.entity.
DIAGNOSTIC CRITERIADIAGNOSTIC CRITERIA
Vertigo is not included in the IHS Vertigo is not included in the IHS Classification as a migrainous Classification as a migrainous symptom except in basilar migrainesymptom except in basilar migraine
Hence most pts. who have MV Hence most pts. who have MV cannot be classified with the current cannot be classified with the current IHS criteriaIHS criteria
PROPOSED DIAGNOSTIC PROPOSED DIAGNOSTIC CRITERIACRITERIA
DEFINITE MIGRAINOUS VERTIGODEFINITE MIGRAINOUS VERTIGO• Episodic vestibular symptoms of at Episodic vestibular symptoms of at
least mod. Severityleast mod. Severity• H/O migraine acc. to IHS criteriaH/O migraine acc. to IHS criteria• One of the following migrainous One of the following migrainous
symptoms during 2 or more vertigo symptoms during 2 or more vertigo attacks: migrainous headache , attacks: migrainous headache , photophobia , phonophobia, visual or photophobia , phonophobia, visual or other aurasother auras
• Other causes ruled outOther causes ruled out
PROBABLE MIGRAINOUS PROBABLE MIGRAINOUS VERTIGOVERTIGO
Episodic vestibular symptoms of at least Episodic vestibular symptoms of at least moderate severity moderate severity
One of the followingOne of the following• Current or previous H/o migraineCurrent or previous H/o migraine• Migrainous symptoms during vestibular Migrainous symptoms during vestibular
symptomssymptoms• Migraine precipitants of vertigo in more than Migraine precipitants of vertigo in more than
50% of attacks : food triggers , sleep 50% of attacks : food triggers , sleep irregularities, hormonal changeirregularities, hormonal change
• Response to migraine T/t in >50% of attacksResponse to migraine T/t in >50% of attacks Other causes ruled outOther causes ruled out
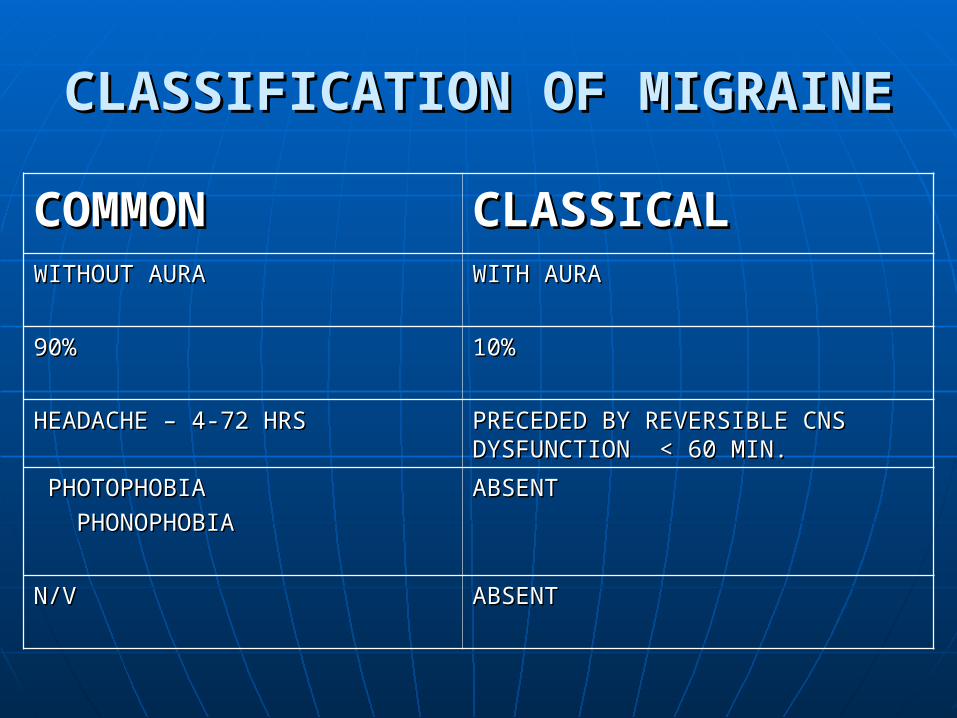
CLASSIFICATION OF MIGRAINECLASSIFICATION OF MIGRAINE
COMMONCOMMON CLASSICALCLASSICALWITHOUT AURAWITHOUT AURA WITH AURAWITH AURA
90%90% 10%10%
HEADACHE – 4-72 HRSHEADACHE – 4-72 HRS PRECEDED BY REVERSIBLE CNS PRECEDED BY REVERSIBLE CNS DYSFUNCTION < 60 MIN.DYSFUNCTION < 60 MIN.
PHOTOPHOBIAPHOTOPHOBIA
PHONOPHOBIAPHONOPHOBIA
ABSENTABSENT
N/VN/V ABSENTABSENT
BASILAR MIGRAINEBASILAR MIGRAINE
VARIANT OF CLASSICAL MIGRAINEVARIANT OF CLASSICAL MIGRAINE FEATURES OF BASILAR ART. INV. FEATURES OF BASILAR ART. INV.
• VERTIGO VERTIGO • TINNITUS TINNITUS • DYSARTHRIA DYSARTHRIA • ATAXIA ATAXIA • VISUAL SYMPTOMS VISUAL SYMPTOMS • TINGLING , NUMBNESS, WEAKNESS OF TINGLING , NUMBNESS, WEAKNESS OF
LIMBSLIMBS
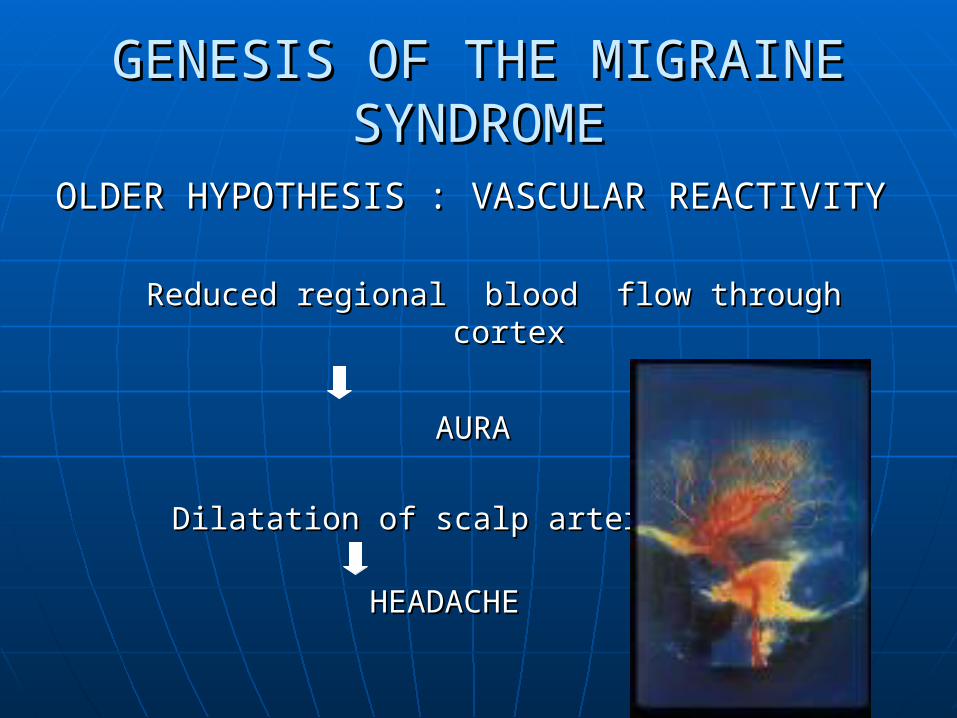
GENESIS OF THE MIGRAINE GENESIS OF THE MIGRAINE SYNDROMESYNDROME
OLDER HYPOTHESIS : VASCULAR REACTIVITYOLDER HYPOTHESIS : VASCULAR REACTIVITY
Reduced regional blood flow through cortexReduced regional blood flow through cortex
AURAAURA
Dilatation of scalp arteriesDilatation of scalp arteries
HEADACHEHEADACHE

NEURONAL THEORY NEURONAL THEORY
Welch & Ramadan , 1995Welch & Ramadan , 1995
Systemic and brain Magnesium Systemic and brain Magnesium deficiencydeficiency
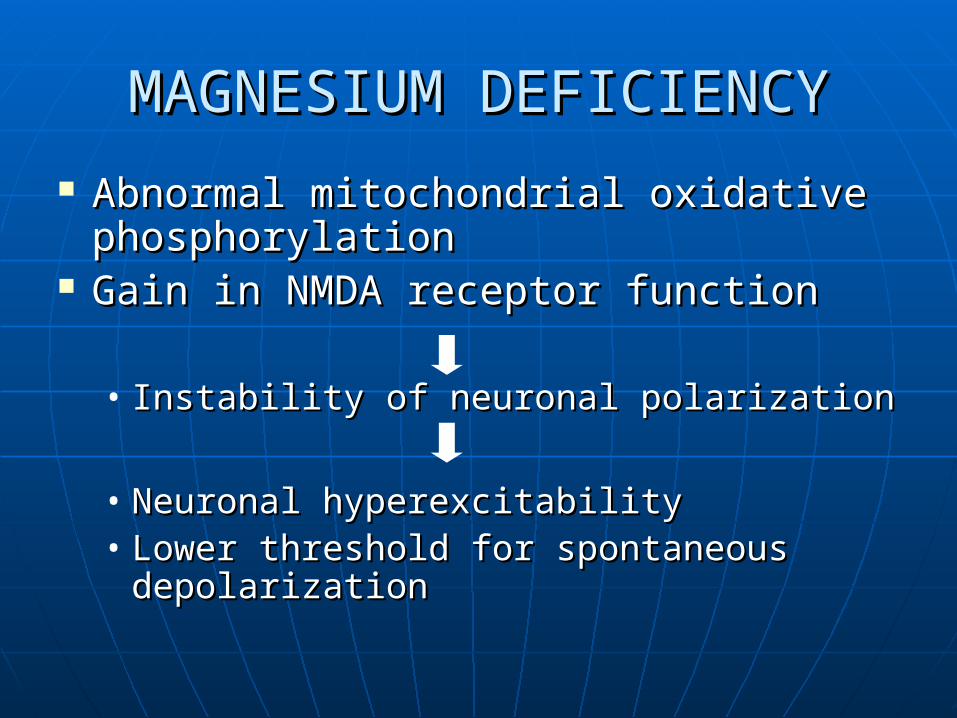
MAGNESIUM DEFICIENCYMAGNESIUM DEFICIENCY
Abnormal mitochondrial oxidative Abnormal mitochondrial oxidative phosphorylationphosphorylation
Gain in NMDA receptor functionGain in NMDA receptor function
• Instability of neuronal polarizationInstability of neuronal polarization
• Neuronal hyperexcitabilityNeuronal hyperexcitability• Lower threshold for spontaneous Lower threshold for spontaneous
depolarizationdepolarization

MAGNESIUM DEFICIENCYMAGNESIUM DEFICIENCY
Mitochondrial dysfunctionMitochondrial dysfunction Impairment of energy metabolismImpairment of energy metabolism Prolonged hypometabolismProlonged hypometabolism Enhanced neuronal excitabilityEnhanced neuronal excitability Susceptability to spontaneous Susceptability to spontaneous
depolarizationdepolarization Changes in blood vessel caliberChanges in blood vessel caliber
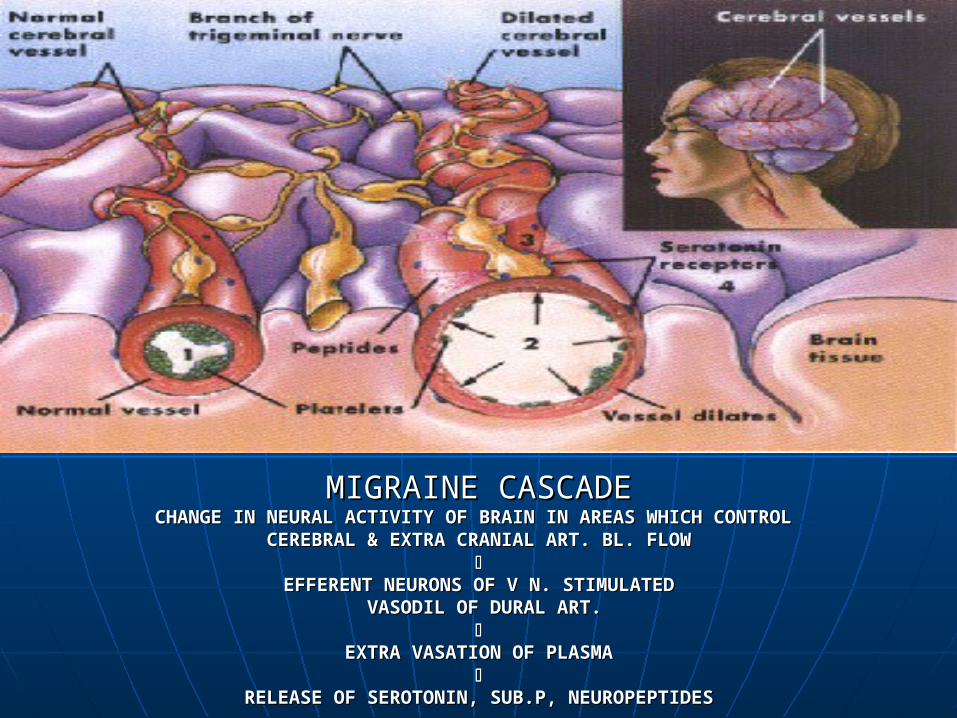
MIGRAINE CASCADEMIGRAINE CASCADECHANGE IN NEURAL ACTIVITY OF BRAIN IN AREAS WHICH CONTROL CHANGE IN NEURAL ACTIVITY OF BRAIN IN AREAS WHICH CONTROL
CEREBRAL & EXTRA CRANIAL ART. BL. FLOWCEREBRAL & EXTRA CRANIAL ART. BL. FLOW
EFFERENT NEURONS OF V N. STIMULATEDEFFERENT NEURONS OF V N. STIMULATED VASODIL OF DURAL ART.VASODIL OF DURAL ART.
EXTRA VASATION OF PLASMAEXTRA VASATION OF PLASMA
RELEASE OF SEROTONIN, SUB.P, NEUROPEPTIDESRELEASE OF SEROTONIN, SUB.P, NEUROPEPTIDES
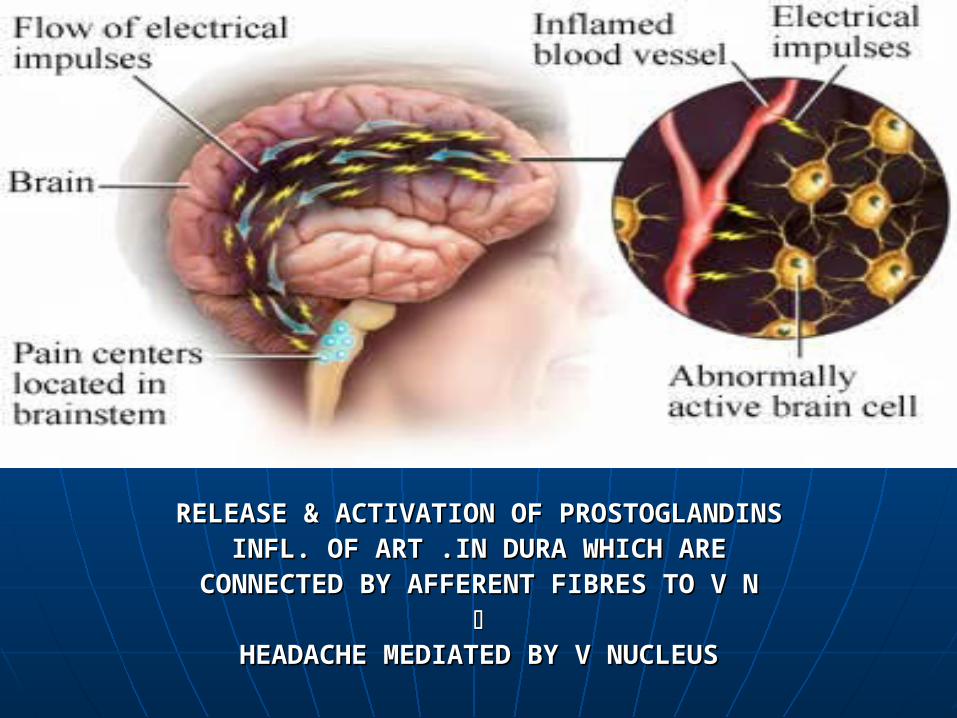
RELEASE & ACTIVATION OF PROSTOGLANDINSRELEASE & ACTIVATION OF PROSTOGLANDINS INFL. OF ART .IN DURA WHICH ARE INFL. OF ART .IN DURA WHICH ARE
CONNECTED BY AFFERENT FIBRES TO V NCONNECTED BY AFFERENT FIBRES TO V N
HEADACHE MEDIATED BY V NUCLEUSHEADACHE MEDIATED BY V NUCLEUS
NEUROGENIC INFLAMMATIONNEUROGENIC INFLAMMATION
Supported by the fact that Supported by the fact that medications that block neurogenic medications that block neurogenic inflammation & mediate inflammation & mediate vasoconstriction are successfully vasoconstriction are successfully used to abort attackused to abort attack
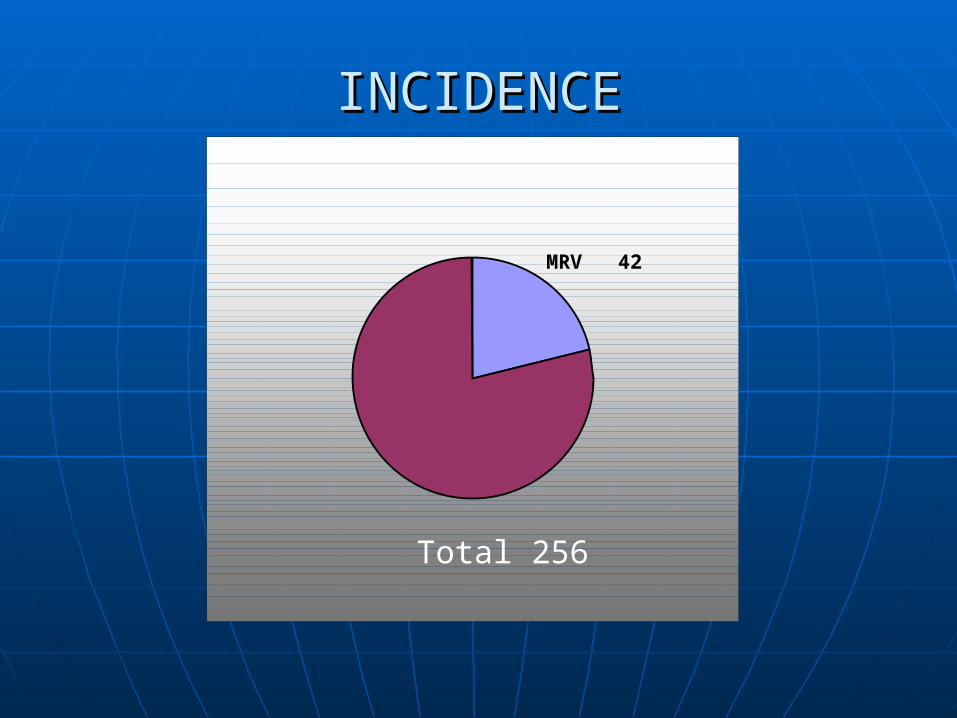
MRV 42
INCIDENCEINCIDENCE
Total 256
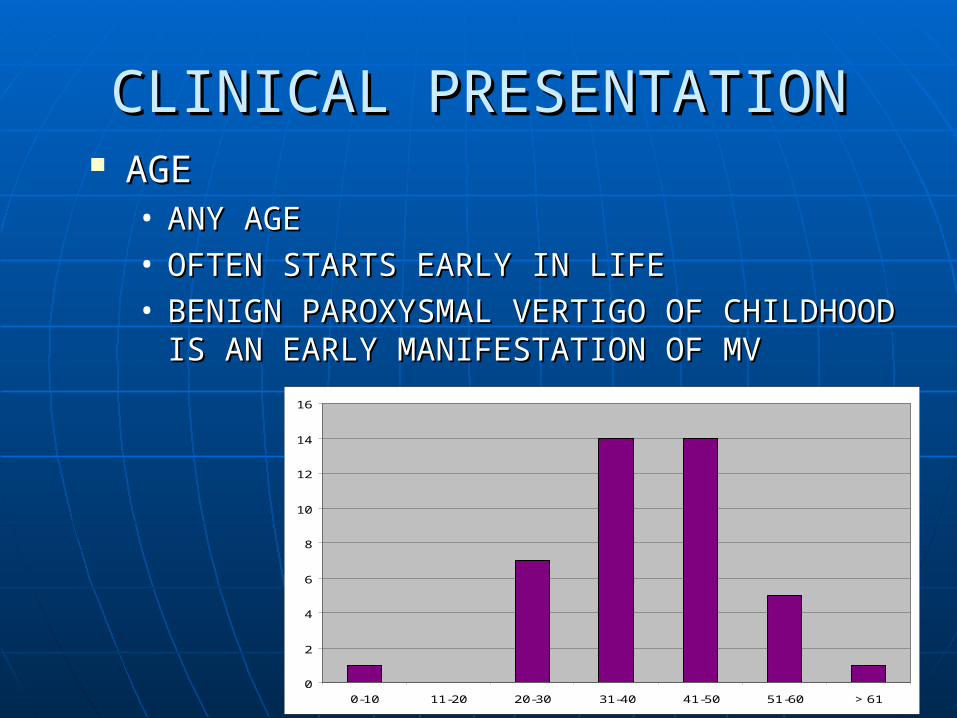
CLINICAL PRESENTATIONCLINICAL PRESENTATION AGEAGE
• ANY AGE ANY AGE • OFTEN STARTS EARLY IN LIFEOFTEN STARTS EARLY IN LIFE• BENIGN PAROXYSMAL VERTIGO OF BENIGN PAROXYSMAL VERTIGO OF
CHILDHOOD IS AN EARLY MANIFESTATION OF CHILDHOOD IS AN EARLY MANIFESTATION OF MVMV
0
2
4
6
8
10
12
14
16
0-10 11-20 20-30 31-40 41-50 51-60 > 61
MALE : FEMALE MALE : FEMALE
FEMALE PREPONDERANCEFEMALE PREPONDERANCE
FEMALE
MALE
CLINICAL PRESENTATIONCLINICAL PRESENTATION
Headache – only 50% pts. presented Headache – only 50% pts. presented with H/o headache along with or with H/o headache along with or after vertigo .Several patients had after vertigo .Several patients had headaches earlier in life but now headaches earlier in life but now vertigo was the predominant vertigo was the predominant symptomsymptom
Duration – usually few hrs.Duration – usually few hrs.
Photophobia & phonophobia were Photophobia & phonophobia were common symptoms.common symptoms.
AUDIOLOGICAL PRESENTATIONAUDIOLOGICAL PRESENTATION
Most had normal hearingMost had normal hearing
Any SNHL was not related to MVAny SNHL was not related to MV
MOTION SICKNESSMOTION SICKNESS
Has been reported to occur Has been reported to occur commonly in MV due to a optokinetic commonly in MV due to a optokinetic stimulation.stimulation.
5 in our series5 in our series
BPPV AND MVBPPV AND MV
5 cases had BPPV5 cases had BPPV BPPV is a well documented sequelae BPPV is a well documented sequelae
to ischemic damage of the inner ear to ischemic damage of the inner ear presumably d/t release of otoconia presumably d/t release of otoconia from the macular membrane.from the macular membrane.
The vasospasm associated with The vasospasm associated with classical visual aura is secondary to a classical visual aura is secondary to a primary neuronal metabolic defectprimary neuronal metabolic defect
MANAGEMENTMANAGEMENT
Lifestyle changesLifestyle changes• Explaining to the pt. what is going onExplaining to the pt. what is going on• Avoidance of irregular lifestyle and Avoidance of irregular lifestyle and
stress. Migrainous and nonmigrainous stress. Migrainous and nonmigrainous brains are wired differently. Migraine brains are wired differently. Migraine pts. are more susceptable to the effects pts. are more susceptable to the effects of overexertion – mental & physical , of overexertion – mental & physical , irregular eating and sleeping habits.irregular eating and sleeping habits.
AVOIDANCE OF TRIGGER AVOIDANCE OF TRIGGER FACTORSFACTORS
A personal vertigo and diet diaryA personal vertigo and diet diary Common triggers Common triggers
• bright and blinking lights bright and blinking lights • monosodium glutamate monosodium glutamate • caffeine caffeine • cheese cheese • chocolates chocolates • alcohol alcohol • pills pills • strong smells strong smells
TREATMENT OF ACUTE MVTREATMENT OF ACUTE MV TriptansTriptans – Sumatriptan – Sumatriptan Vestibular suppressantsVestibular suppressants
• promethazine promethazine • dimenhydrinate dimenhydrinate • meclizinemeclizine
PROPHYLACTIC TREATMENTPROPHYLACTIC TREATMENT
INDICATIONSINDICATIONS• 3 or more attacks per month3 or more attacks per month• Attacks which are incapacitating & Attacks which are incapacitating &
impair normal activities impair normal activities • Cannot tolerate or are not helped by Cannot tolerate or are not helped by
abortive therapyabortive therapy• Cannot psychologically cope with Cannot psychologically cope with
attacksattacks
PROPHYLACTIC TREATMENTPROPHYLACTIC TREATMENT Beta blockers Beta blockers
• Propanolol – 40 -240 mg / dayPropanolol – 40 -240 mg / day• Metoprolol – 50 -120 mg / dayMetoprolol – 50 -120 mg / day
Side effects –fatigue , hypotension , impotence , Side effects –fatigue , hypotension , impotence , depression , nightmares , bronchial constrictiondepression , nightmares , bronchial constriction
Calcium channel blockersCalcium channel blockers• Flunerizine – 5-10 mg / dayFlunerizine – 5-10 mg / day• Verapamil -120 -240 mg / dayVerapamil -120 -240 mg / day
Tricyclic antidepressantsTricyclic antidepressants• Nortryptiline – 10 mg initially , upto 25 mg / day Nortryptiline – 10 mg initially , upto 25 mg / day
Second line of drugs include Valproic acid and Second line of drugs include Valproic acid and methysergide.methysergide.
PROPHYLAXIS TREATMENTPROPHYLAXIS TREATMENT
Acetazolamide Acetazolamide • Beneficial effect results from its altering Beneficial effect results from its altering
the pH within the cerebellum thus the pH within the cerebellum thus stabilizing the mutated calcium channel stabilizing the mutated calcium channel [Baloh][Baloh]
• Dose -250 mg BDDose -250 mg BD• Side effects – paraesthesias ,inability to Side effects – paraesthesias ,inability to
drink carbonated drinks , long term risk drink carbonated drinks , long term risk of renal stonesof renal stones
PROPHYLAXIS TREATMENTPROPHYLAXIS TREATMENT
Botulinum toxoid [Botox] injections Botulinum toxoid [Botox] injections into the scalp or neckinto the scalp or neck• Mechanism – inhibition of acetylcholine Mechanism – inhibition of acetylcholine
in brainin brain• Efficacy after pericranial injection can Efficacy after pericranial injection can
last for 3 or more monthslast for 3 or more months• Used in case studies and trials , not yet Used in case studies and trials , not yet
approvedapproved
