midtarsal joint between calcaneus and cuboid on lateral side between talus and navicular on the...
TRANSCRIPT

Midtarsal joint
• between calcaneus and cuboid on lateral side
• between talus and navicular on the medial side
Talocrural joint
• inferior tibiofibular jnt.
• tibiotalar jnt.Subtalar joint
• aka talocalcaneal• between talus and
calcaneus
medial
lateral

Talocrural Joint
• Articulation between the tibia and fibula (inferior tibiofibular joint) and between the tibia and the talus (tibiotalar joint).
• This joint is responsible for plantar flexion and dorsiflexion and some abduction/adduction.
• The axis of rotation is a line between the two malleoli.

Subtalar Joint• Allows pronation/supination and
rotation.• The talus articulates with the
calcaneus anteriorly, posteriorly and medially.
• The axis of rotation runs diagonally from the posterior, lateral, plantar surface to the anterior, medial, dorsal surface.
• The orientation of this axis makes pronation/supination triplanar with reference to the cardinal planes.
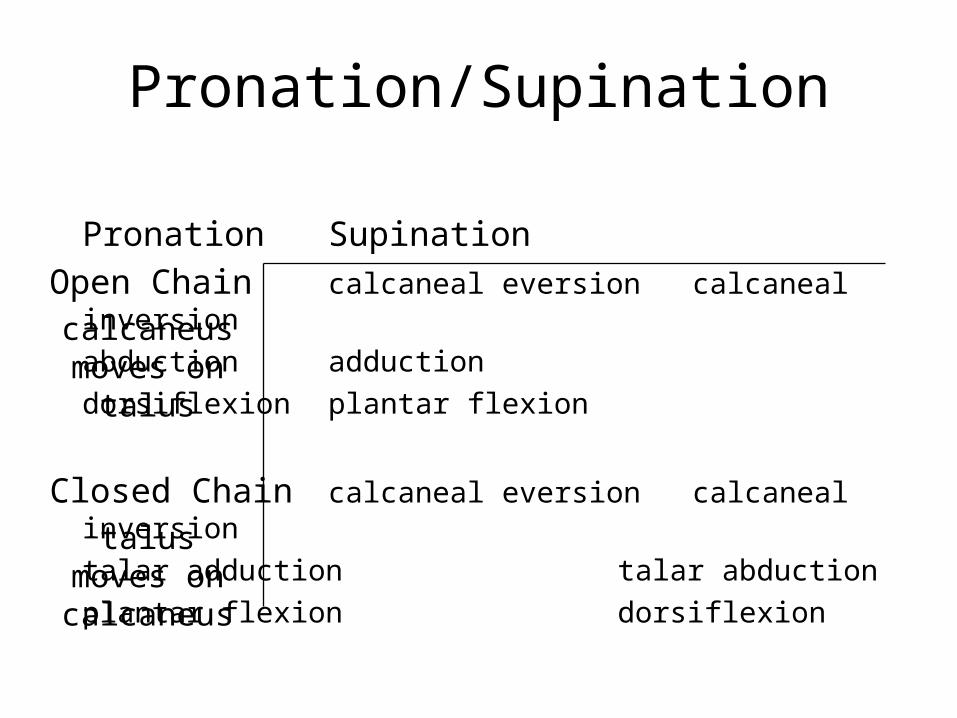
Pronation/Supination
Pronation Supination
Open Chain calcaneal eversion calcaneal inversion
abduction adduction
dorsiflexion plantar flexion
Closed Chain calcaneal eversion calcaneal inversion
talar adduction talar abduction
plantar flexion dorsiflexion
calcaneus moves on
talus
talus moves on calcaneus
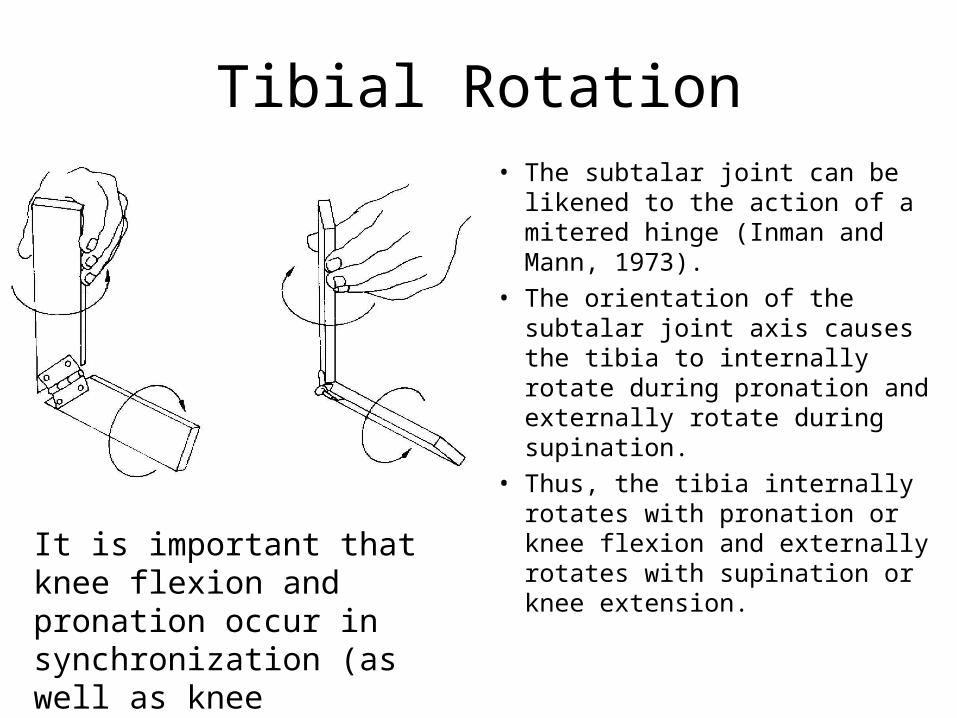
Tibial Rotation• The subtalar joint can be likened
to the action of a mitered hinge (Inman and Mann, 1973).
• The orientation of the subtalar joint axis causes the tibia to internally rotate during pronation and externally rotate during supination.
• Thus, the tibia internally rotates with pronation or knee flexion and externally rotates with supination or knee extension.
It is important that knee flexion and pronation occur in synchronization (as well as knee extension and supination).

Midtarsal Joint
Actually consists of two joints: the calcaneocuboid on the lateral side and the talonavicular on the medial side.
During pronation, the axes of these two joints are parallel, this unlocks the joint and creates a hypermobile foot that can absorb shock. During supination the axes are not parallel and this joint becomes locked allowing efficient transmission of forces.

Foot Orientation

A forefoot valgus exists when the forefoot is everted relative the rearfoot. This is not as common as forefoot varus.
A forefoot varus exists when the forefoot is inverted to the rearfoot. This is the most common cause of excessive pronation.
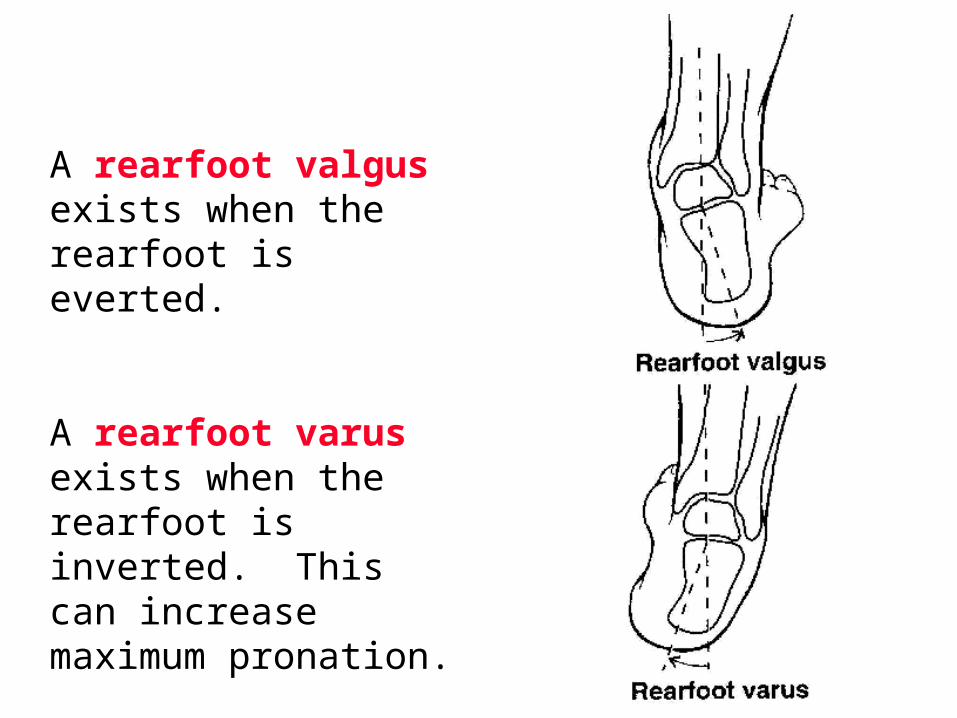
A rearfoot valgus exists when the rearfoot is everted.
A rearfoot varus exists when the rearfoot is inverted. This can increase maximum pronation.
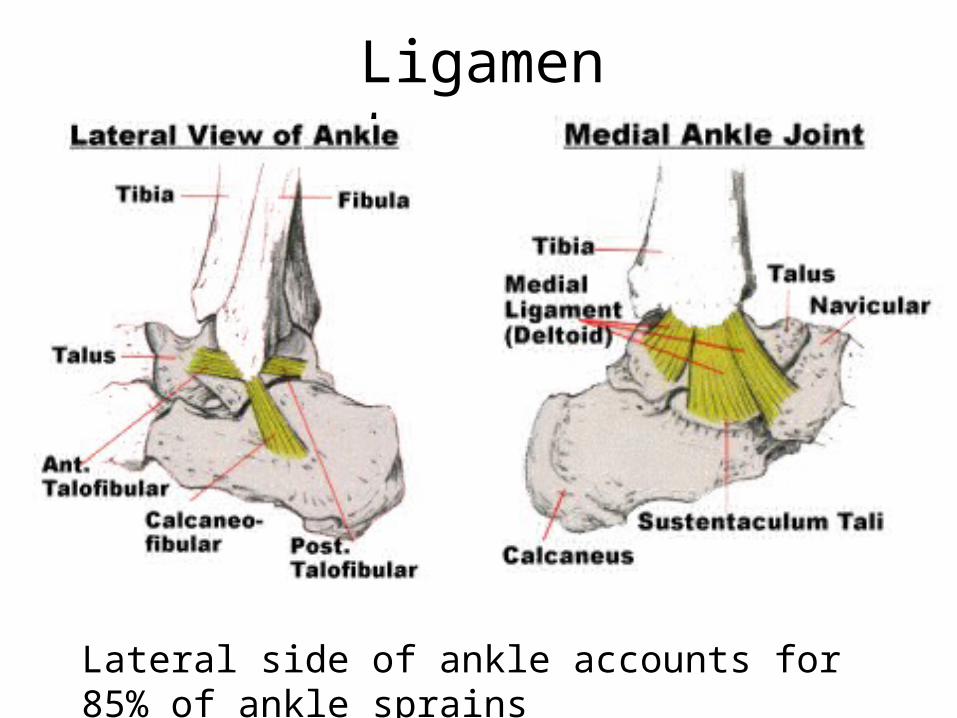
Ligaments
Lateral side of ankle accounts for 85% of ankle sprains

Arches of the Foot
There are 3 arches in the foot that contribute to support and shock absorption. These arches are maintained by the shape of the tarsal and metatarsal bones, ligaments and plantar fascia.
Plantar surface
Fascia

Arch Types• Feet are often classified according to the height of
the medial arch.– Normal– high-arched or pes cavus– flat-footed or pes planus
• Arches can also be rigid or flexible.• High-arched, rigid feet make poor shock absorbers.• Flat-footed, flexible arches often allow excessive
pronation.

Plantar Flexors
NOTE:1) Soleus liesdeep togastrocnemius
2) Both insert intothe calcanealtendon akaAchilles tendon
SoleusGastrocnemius
Posterior View

AssistantPlantar Flexors
Tibialis Posterior
PeroneusBrevis
PeroneusLongus
FlexorDigitorum
Longus
FlexorHallucisLongus Plantaris
Note: Their tendons passposteriorly to the malleoli
Note:insertionis wrong!

Dorsiflexion
peroneus tertius (usually very close to extensor digitorum longus and often considered as part of this muscle)
tibialisanterior
extensordigitorum
longus
extensorhallucislongus(deep to ext.digitorumlongus)
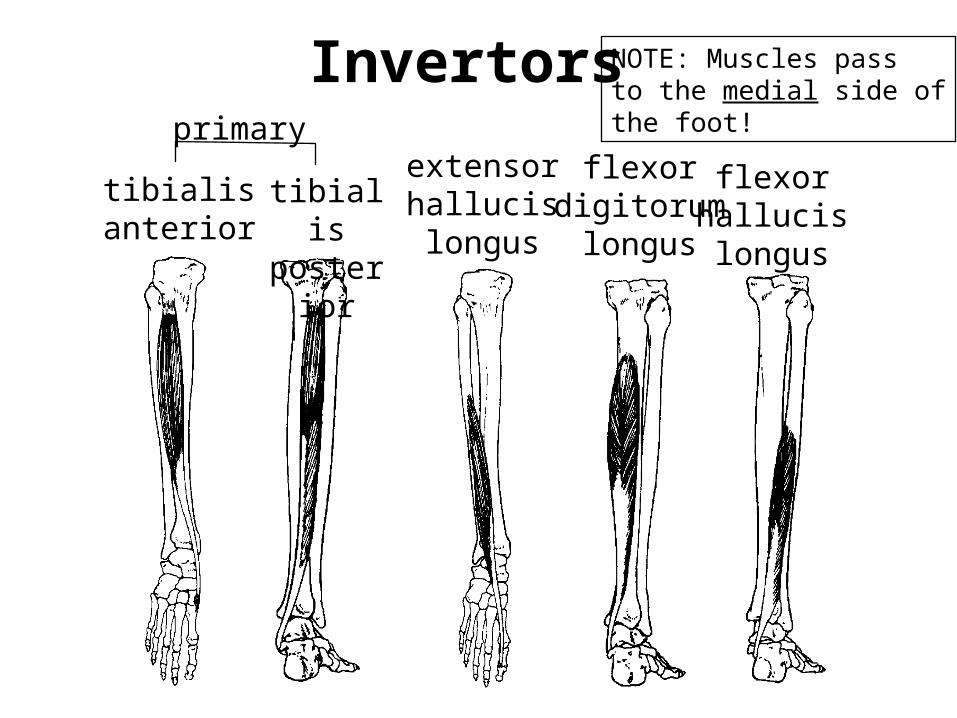
tibialisanterior
extensorhallucislongus
flexordigitorum
longus
flexorhallucislongus
tibialisposterior
Invertorsprimary
NOTE: Muscles passto the medial side ofthe foot!

peroneusbrevis
peroneuslongus
peroneustertius
extensordigitorum
longus
Evertorsprimary
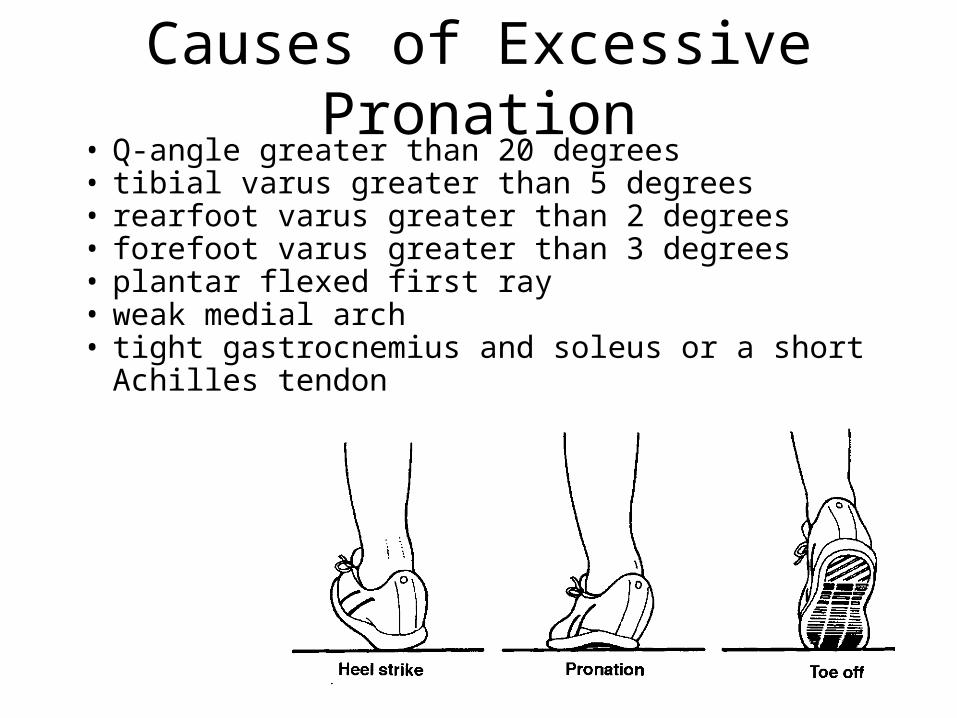
Causes of Excessive Pronation• Q-angle greater than 20 degrees• tibial varus greater than 5 degrees• rearfoot varus greater than 2 degrees• forefoot varus greater than 3 degrees• plantar flexed first ray• weak medial arch• tight gastrocnemius and soleus or a short Achilles tendon

The Problem with Excessive Pronation
Excessive or prolonged pronation during the support phase will disrupt the normal tibial-femoral rotation relationship at the knee. The tibia continues to internally rotate with the prolonged pronation while the knee is extending. Knee extension is normally associated with external tibial rotation.