methylation framework of cell cycle gene inhibitor … framework of cell cycle gene inhibitor...
TRANSCRIPT

Methylation Framework of Cell Cycle Gene Inhibitor p16INK4A In Hepatocellular Carcinoma Patients
Thesis Submitted for partial fulfilments
of M.D. degree in Clinical & Chemical Pathology
By
Hany Ahmed Fouad ElghobaryM.B.B.Ch, M.Sc. of Clinical & Chemical Pathology
Faculty of MedicineCairo University
Supervised By
Prof. DR. Fatma Ahmed El-MougyProfessor of Clinical & Chemical Pathology
Faculty of MedicineCairo University
Prof. DR. Nabil Mostafa Khalil El-KadyProfessor of Tropical Medicine
Faculty of MedicineCairo University
Prof. DR. Sahar Abd El-Atty SharafProfessor of Clinical & Chemical Pathology
Faculty of MedicineCairo University
DR. Hany Hussein El-SayedLecturer of Clinical & Chemical Pathology
Faculty of MedicineCairo University
Faculty of MedicineCairo University
2012
Acknowledgement
First of all I would like to thank ALLAH for giving me the power to
complete this work, ALLAH the most merciful, gracious and
compassionate.
I am greatly honored to express my deep gratitude and faithfulness to
Prof.Dr.Fatma Ahmed Fathy EL-Mougy Professor of clinical and
chemical Pathology, Faculty of Medicine-Cairo University for her
encouragement, sustained support and guidance throughout the work.
I would like to express my thanks and deep regards to Prof.Dr.
Nabil Mostafa El Kady, Professor of Tropical Medicine, Faculty of
Medicine-Cairo University for hir great help throughout the work. His
fatherhood attitude was so supportive for the completion of this work.
I feel extremely grateful to Prof. Dr. Sahar Abd EL-Atty Sharaf
professor of clinical and chemical pathology, Faculty of Medicine-Cairo
University for her sincere efforts in supervising this work and for her
advices and guidance throughout the work of the thesis.
I would like to thank dr. Hany Hussein El-Sayed lecturer of
clinical and chemical pathology, Faculty of Medicine-Cairo University for
his friendly attitude and kind supervision.
I would like also to thank my colleague Dr. Walaa Ahmed Rabie
lecturer of clinical and chemical pathology, as well as Dr. Mohamad
Mahmoud Nabil, Ass. Prof. of tropical medicine for their kind care and help.
Furthermore, I dedicate the thesis to all the members of my family
for their moral support and patience during this work.
A special dedication to my wife for her never ending care. She was
always supporting me and encouraging me to continue and finish this work.
Abstract
Hepatocellular carcinoma (HCC) is currently the fifth most
common solid tumor worldwide and the third leading cause of cancer
related death.
The tumor suppressor gene p16INK4A is located on chromosome
9p21 and encodes the p16 protein, which binds selectively to CDK4 to
inhibit activation of the CDK4/cyclin D complex in the G1 phase.
Inactivation of this gene which normally inhibits progression to the
G1 phase of the cell cycle is involved in the initiation of tumors.
Several studies have shown that p16INK4A is frequently
downregulated by aberrant methylation of the 5'cytosine phosphoguanine
island within the promotor region.
This study was performed to evaluate the frequency of methylated
p16INK4A in the peripheral blood of HCC and liver cirrhosis patients and
to evaluate its role as a risk factor for HCC using methylation specific
PCR (MSP).
Methylation of p16INK4A was detected in 6.7% (2/30) of HCC
patients and 5% (1/20) of LC patients.
Results of the present study revealed that methylated p16INK4A
cases in the HCC group had the highest AFP levels.
Results of this study could not conclude hypermethylation of
p16INK4A as a risk factor for HCC.
Key word: p16INK4A- Hepatocellular- Cell Cycle Gene.
I
Table of Contents
Page
Introduction 1
Aim of work 3
Review of literature 4
Chapter one: Hepatocellular carcinoma 4
I. Introduction 4
II. Risk factors for HCC 4
III. Diagnosis of HCC: 17
A. Clinical Picture 17
B. Radiologic Investigations 19
C. Laboratory findings 21
D. Histological diagnosis of HCC 32
Chapter two: Cell cycle 33
Regulation of eukaryotic cell cycle 35
Role of cyclins and CDKs 36
Checkpoint 39
Tumor suppressor genes 40
Epigenetics 52
DNA methyltion 52
Histone modification 57
Nucleosome positioning and remodeling 58

II
Genomic imprinting 59
Noncoding RNAs 60Chapter three: p16 gene 61Gene location and mapping of the p16INK4A gene 61Cellular location of p16 INK4A
63
Function of p16 INK4A 63
Role of p16 INK4A in HCC 68
Molecular mechanism of p16INK4A DNA methylation in HCC 69
Subjects and methods 71
Results 93
Discussion 106
Summary 120
Conclusion & Recommendation 124
References 125
III
List of tables
Page
82 Carrier RNA and Buffer BL volumesTable 1
82Bisulfite Reaction componentsTable 2
83 Bisulfite Conversion Thermal Cycler ConditionsTable 3
87 PCR reaction mixtureTable 4
93 Presenting symptoms & signs in subjects of different
groups
Table 5
94 Radiological findings of patients in different groupsTable 6
94 Site and number of hepatic focal lesion (HFL) in
HCC cases
Table 7
95 Haematological testsTable 8
95 Biochemical testsTable 9
96 Number and percentage of viral and bilharzial
markers in different groups
Table 10
96 Comparisons of lab data between different groupsTable 11
99Number & percentage of p16INK4A methylated cases
among different groups
Table 12
102Important data of subjects with methylated p16INK4ATable 13
IV
List of figures
Page
6Cellular signaling pathways implicated in
hepatitis B virus (HBV) X protein-related
hepatocarcinogenesis.
Figure 1
7A hypothetical model depicting potential
genetic and epigenetic changes induced by
HBV infection
Figure 2
9Cellular signaling pathways implicated in
hepatitis C virus (HCV)
Figure 3
14Main oncogenic pathways associated with
hepatocarcinogenesis
Figure 4
33Schematic representation of the cell cycleFigure 5
37Mammalian cell cycle regulation by
CDK/cyclin holoenzymes and CKIs
Figure 6
38 Rb and cell cycle machinery.Figure 7
41Regulation of the G1/S transition by the
Cdk4/6–cyclin D/INK4/Rb pathway.
Figure 8
44Schematic representation of alterations in
p53/ARF and RB/INK4A pathways in HCC.
Figure 9
45 The roles of p53 in growth arrest and
apoptosis
Figure 10
48Function of p21Figure 11
59Nucleosome and histone modificationsFigure 12
61Genomic structure, mutations, and transcripts
of the INK4b (p15) and INK4a (p16/p19ARF)
locus.
Figure 13

V
Page
64 A simplified view of the pRB−E2F pathwayFigure 14
78QIAamp Spin ProcedureFigure 15
94Number of focal lesions in HCC groupFigure 16
97correlation between AFP & ASTFigure 17
98correlation between AFP & ALPFigure 18
98ROC curve for AFPFigure 19
99Number & percent of p16INK4A methylated
cases among groups
Figure 20
101Detection of products of MSP for aberrant
p16INK4A methylation in HCC subjects
Figure 21
101Detection of products of MSP for aberrant
p16INK4A methylation in LC subjects
Figure 22
102Detection of products of the unmethylated
(quality control) primer
Figure 23
VI
List of abbreviations
microgramµgmicrogram/litreµg/LmicrolitreµlAflatoxin B1 AFB1 Alpfa fetoproteinAFPAlpha-1- fucosidase AFUalbuminALBAlkaline phosphataseALPAlanine aminotransferaseALTAcivator proteinAP-1Apoptotic Protease Activating Factor 1 Apaf
Adenomatous Polyposis ColiAPCAnaphase-promoting complexAPCAlternative reading frame ARFapoptosis signal-regulating kinase 1ASK1 Aspartate aminotransferaseAST Activated transcription factorATFActivating Transcription Factor 2. ATF-2 Adenosine triphosphateATP Bcl-2-associated X protein BaxBase pairbpBreast Cancer BRCABub1-related kinase 1; Bub1, budding uninhibited by benzimidazoles 1
BubR1
C1q receptor C1qR Calcium Ca++ Caspase 3CASP 3Complete blood countCBCCyclin D2 CCND2Cluster of differentiation CDCell devision cycle 2cdc2 Cyclin-dependent kinase inhibitor 2A CDKN2A cyclin-dependent kinases CDKsComplementary deoxyribonucleic acidcDNA CDK interacting protein/Kinase inhibitory protein CIP/KIPcyclin-dependent kinase inhibitory protein-1CIP-1Cyclin kinase inhibitor CKIcentimeter cm

VII
Cytosine phosphoguanineCpGc-AMP response element bindingCREBComputed tomography CTCytochrome C Cyto CDistilled waterD.WDeoxyadenosine TriphosphatedATPDirect bilirubinDBilDeleted in colorectal carcinomaDCCDes-gamma-caboxy prothrombinDCPDeoxycytidine TriphosphatedCTPDamage specific-DNA binding proteinDDBDeoxyguanosine TriphosphatedGTPDeoxy ribonucleic acidDNADNA methyltransferasesDNMTsdeoxynucleotide triphosphatesdNTPs dimerization partner 1 DP1Deoxythymidine triphosphatedTTP E-cadherinEcadEthylene diamine tetraacetateEDTAEnzyme linked immunosorbent assayELIZAEstrogen receptors ERExtracellular Signal-Regulated Kinase ERKFibrosis scoreFFine needle aspiration biopsyFNABgram gGap 0 phase G0 phaseGap 1 phaseG1 phaseGap 2 phase G2 phaseGrowth Arrest and DNA Damage-inducible GADDGamma glutamyl transferaseGGTGolgi protein 73GP73Glipican 3GPC3Gene associated with Retinoid-Interferon-induced Mortality
GRIM
glutathione S-transferase promoterGSTP1 Helicobacter pyloriH.pyloriHistone acetyl transferaseHATHaemoglobin Hb Hepatitis B envelope antigen HBe Ag Hepatitis B surface antigenHBs Ag
VIII
Hepatitis B virusHBVHepatitis B x protein HBxHepatocellular carcinoma HCC Hydrochloric acid HCLHepatitis C virusHCVhistone deacetylasesHDAC Histone demethylaseHDMT Hepatic focal lesionHFLhepatocyte growth factorHGFhuman herpes virus-8HHV-8Hypoxia inducible factor 1α HIF-1 αHuman immunodeficiency virusHIVhistone methyltransferaseHMTHigh performance liquid chromatographyHPLChepatic stellate cells HSChuman telomerase hTERT insulin-like growth factor IIIGF II Inhibitor of Kinase 4AINK4AInsulin resistance IRc-Jun NH-terminal kinaseJNK kilobytekbkilodaltonKDaKaposi's sarcoma-associated herpesvirus KSHV litreLLiver cirrhosisLCLens culinaris agglutininLCAlow-density lipoproteinLDLLarge hepatitis B envelopeLHBeMole MMitosis phaseM phase mitogen-activated protein kinase MAPKMilli absorbance unitmAUmurine double minute (mdm2) MDM2milligram mgMagnesium chloride MgCl2minuteminMicro ribonucleic acidmiRNAmillilitremlmillimolemMMatrix metalloproteinases MMPs
IX
Magnetic resonance imaging MRIMessenger ribonucleic acidmRNAMethyl Specific Polymerase Chain ReactionMSPmultiple tumor suppressor 1 MTS-1Non alcoholic fatty liver diseaseNAFLD Non alcoholic steatohepatitisNASHNon coding ribonucleic acidncRNANuclear factor kappa betaNF-κB nanogramngNumber No.Degrees centigrade/Celsiusº Copen reading frame ORFprobabilityp
،p53 Inducible Ribonucleotide Reductase P53R2 Peripheral blood PBProthrombin concentrationPCProliferating cell nuclear antigenPCNAPolymerase chain reactionPCRPlatelet derived growth factorPDGFpicogrampgPhosphoinositide 3-KinasePI3K Proteins induced by vit K absence PIVKA2Protein kinase CPKCplateletsPltsPeroxisome Proliferator Activated Receptor PPARPhosphorylated retinoblastoma pRBC-terminally phosphorylated Smad3 pSmad3C linker-phosphorylated Smad3 pSmad3L Prothrombin timePTphosphatase and tensin homologue deleted on chromosome ten
PTEN
correlationrRapidly Accelerated Fibrosarcoma RAF Rat sarcoma rasRetinoblastoma 1Rb1Restriction landmark genomic scanningRLGSRibonucleic acid RNA Receiving operating characteristicROCReactive oxygen speciesROSRevolutions per minuterpm
X
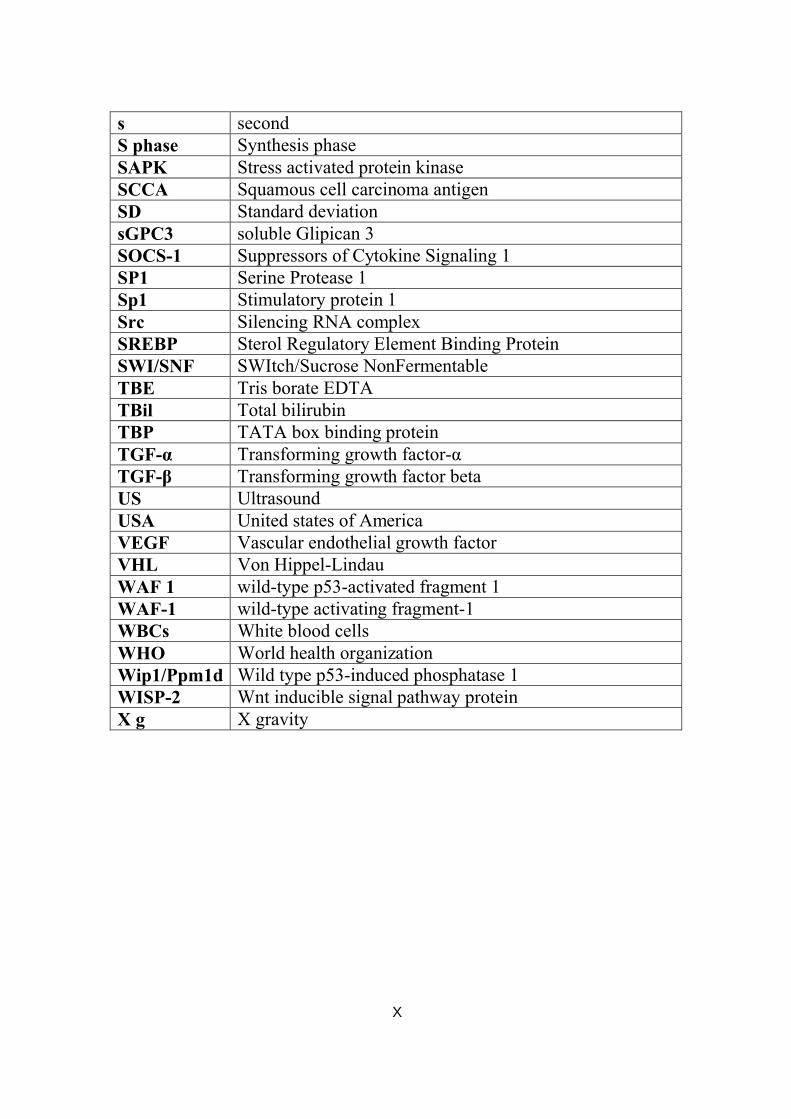
secondsSynthesis phase S phaseStress activated protein kinaseSAPKSquamous cell carcinoma antigenSCCAStandard deviationSDsoluble Glipican 3sGPC3Suppressors of Cytokine Signaling 1SOCS-1Serine Protease 1 SP1 Stimulatory protein 1 Sp1 Silencing RNA complexSrc Sterol Regulatory Element Binding Protein SREBPSWItch/Sucrose NonFermentable SWI/SNF Tris borate EDTATBETotal bilirubinTBilTATA box binding proteinTBPTransforming growth factor-αTGF-α Transforming growth factor betaTGF-βUltrasound US United states of AmericaUSAVascular endothelial growth factorVEGFVon Hippel-LindauVHLwild-type p53-activated fragment 1 WAF 1 wild-type activating fragment-1 WAF-1White blood cellsWBCsWorld health organization WHO Wild type p53-induced phosphatase 1 Wip1/Ppm1d Wnt inducible signal pathway protein WISP-2 X gravity X g

Introduction & Aim of work
1
Introduction
Hepatocellular carcinoma (HCC) is the fifth most common and the
third most fatal malignancy worldwide (Eric et al., 2010). It showed a
dramatic increase of its incidence worldwide over the last three decades
and is associated with a very poor prognosis. Except for patients accessible
for surgical treatment, the 5-year survival is less than 3% (Antal et al.,
2010). The burden of hepatocellular carcinoma (HCC) has been increasing
in Egypt, with a doubling in the incidence rate in the past 10 years (Anwar
et al., 2008).
It is commonly associated with chronic liver diseases caused by
infection with hepatitis B virus (HBV) and/or hepatitis C virus (HCV),
excessive alcohol consumption, aflatoxin, and certain metabolic diseases
(Oranous et al., 2011).
Although alpha-fetoprotein (AFP) measurement and ultrasonography
are useful surveillance tests for detecting HCCs at a stage at which they
may be treated, both tests have limitations: AFP shows low sensitiviyy and
specificity , while the results of ultrasonograpy are dependent on the skill
of those performing the examination and on the condition of the patient
(Ahmed et al., 2010).
Inactivation of tumor suppressor genes and activation of oncogenes
initiated by genetic and epigenetic differences may play an important role
in carcinogenesis (Oranous et al., 2011).
The P16INK4A gene is a tumor suppressor that acts as a negative
regulator of the cell cycle by binding to and inhibiting cyclin-dependent
kinase 4 (CDK4). Reduced expression of the p16INK4A gene results in
uncontrolled division of cells. Several mechanisms that lead to p16INK4A
Introduction & Aim of work
2
inactivation have been described, including point mutations, homozygous
deletions, and promoter hypermethylation (Matsuda, 2008). The later
having been shown to occur more frequently in HCC patients (Csepregi et
al., 2010).
The tumor suppressor gene p16INK4A is located on chromosome 9p21
and encodes the p16 protein, which binds selectively to CDK4 to inhibit
activation of the CDK4/cyclin D complex in the G1phase of the cell cycle
(Thorgeirsson and Grishan,2002) .
Inactivation of p16 INK4A gene resulting from its methylation leads to
disruption of cell cycle control, a finding which has been reported in HCC
(Shim et al., 2003).
However, reports on p16 INK4A methylation in HCC were remarkably
diverse (Zang et al., 2011) (Patopova et al., 2011).
Aberrant methylation of the p16INK4A promotor has also been
reported in early preneoplastic lesions in the lung, colon, oesophagus and
pancreas. These findings suggest that loss of p16INK4A function, often due
to promotor methylation, may be an early event in the pathogenesis of
various types of tumors (Kaneto et al., 2006).

Introduction & Aim of work
3
Aim of work
The present study was performed to estimate the frequency of
methylated p16INK4A in the peripheral blood of patients with liver cirrhosis
(LC) and HCC to evaluate its role as a risk factor for hepatocellular
carcinoma (HCC).
Hepatocellular Carcinoma
4
Chapter 1
Hepatocellular Carcinoma
I. Introduction:
Hepatocellular carcinoma (HCC) is one of the leading causes of
worldwide cancer mortality, with an estimated 1 million deaths annually
and a 5-year survival rate of less than 5% (El-Serag, 2007). The incidence
of HCC varies considerably depending on, geographical location and the
cause of liver disease. HCC incidence of 4 to 15 per 100,000 has been
reported in Western countries, compared with 120 per 100,000 in Asia and
Africa (Hashem, 2011).
In most countries, HCC accounts for 70%–85% of primary liver
cancer cases (Ahmed et al., 2008), with the burden of disease expected to
increase in coming years (Alan et al., 2010).
II. Risk factors for HCC:
HCC is a complex disease associated with many risk factors and
cofactors (Gomaa et al., 2008). In most patients, HCC is preceded by
cirrhosis of the liver (Llovet, 2005) and, unsurprisingly, common causes of
cirrhosis have been identified as key risk factors for HCC. Of particular
importance is chronic infection with HBV or hepatitis C virus (HCV).
Indeed, it has been estimated that HBV is responsible for 50%–80% of
HCC cases worldwide, whereas 10%–25% of cases are thought to be a
result of HCV infection (Block et al., 2003). Antiviral therapy resulting in
viral suppression is known to significantly decrease the risk for HCC in
patients infected with HBV (Liaw et al., 2004).
Cancer emerges when immunological control fails and transformed
cells develop resistance against cell death signaling pathways. The same
Hepatocellular Carcinoma
5
mechanisms underlie the poor responsiveness of HCC towards
chemotherapy (Schattenberg et al., 2011).
Age of 50 years or older, male gender, and advanced fibrotic stage
were associated with an increased risk of HCC. Liver fibrosis seems to be a
crucial factor in determining carcinogenesis (Sandra et al., 2010).
A. Hepatitis B Virus:
Human hepatitis B virus is a member of the hepadnavirus family; it
is a DNA enveloped virus, which is remarkably stable to organic solvents,
and also heat- and pH-resistant (Gripon et al., 2002).
HBV CarcinogenesisThe geographic distribution patterns of HCC and hepatitis B virus
(HBV) almost coincide with each other (Marchio et al., 2000), as with
many malignancies, the carcinogenesis of HCC is a multi-step process
involving a number of different genetic alterations that ultimately lead to
malignant transformation of the hepatocyte (Laurent-Puig et al., 2001).
The role of HBV in tumor formation appears to be complex and may
involve both direct and indirect mechanisms. Integration of HBV DNA into
the host genome occurs at early steps of clonal tumor expansion, and it has
been shown to induce direct insertion mutagenesis of cancer-related genes
in a number of cases (Chemin and Zoulim, 2009)
The X gene of the viral genome codes for functionally active
transactivator proteins, including the X protein (HBx), which is oncogenic
in transgenic mice (Chan et al., 2008). HBx transactivates several
cytoplasmic signaling pathways, including PKC (protein kinase C), Smad
and Wnt and by binding to nuclear transcription factors, including cAMP
response element binding (CREB) and activating transcription factor 2
(ATF-2) (Feitelson and Lee, 2007; Feitelson et al., 2009).

Hepatocellular Carcinoma
6
Figure 1 Cellular signaling pathways implicated in hepatitis B virus (HBV) X protein-related hepatocarcinogenesis. Bolded boxes indicate key driving forces for carcinogenesis (Tsai and Chung, 2010).
Prolonged expression of the viral regulatory protein HBx and the
large envelope protein (LHBe) may contribute in deregulating the cellular
transcription program and proliferation control, and sensitize liver cells to
carcinogenic factors (Liu et al., 2008).
Chronic liver inflammation and hepatic regeneration induced by
cellular immune responses may favor the accumulation of genetic
alterations in infected hepatocytes (Liu et al., 2006).
Genetic studies have provided insight into the mechanisms
underlying viral associated hepatocarcinogenesis (Paterlini-Brechot et al.,
2003; Huang et al., 2005; and Park and Chung., 2007). It has been shown
that the rate of chromosomal alterations is significantly increased in HBV-
related tumors compared with tumors associated with other risk factors.
HBV might therefore play a role in enhancing genomic instability
(Murakami et al., 2005). Inactivation of tumor suppressor gene p53 by
mutations and allelic deletions is found more frequently in tumors
associated with HBV infection (Hytiroglou and Theise, 2006).
Hepatocellular Carcinoma
7
Nishida and Goel, 2011 suggested that viral proteins affect the
function of the p53 protein and contribute to HCC formation. For example,
HBx protein itself reportedly binds to p53 and disturbs its capacity for
DNA binding, transcription and induction of apoptosis. Also, HBV-related
tumors harbor a low rate of oncogene β-catenin mutations (Liu et al.,
2008). Together, these data strongly support the notion that chronic HBV
infection might trigger specific oncogenic pathways, thus playing a role
beyond stimulation of host immune responses and chronic necro-
inflammatory liver disease (Liu et al., 2008).
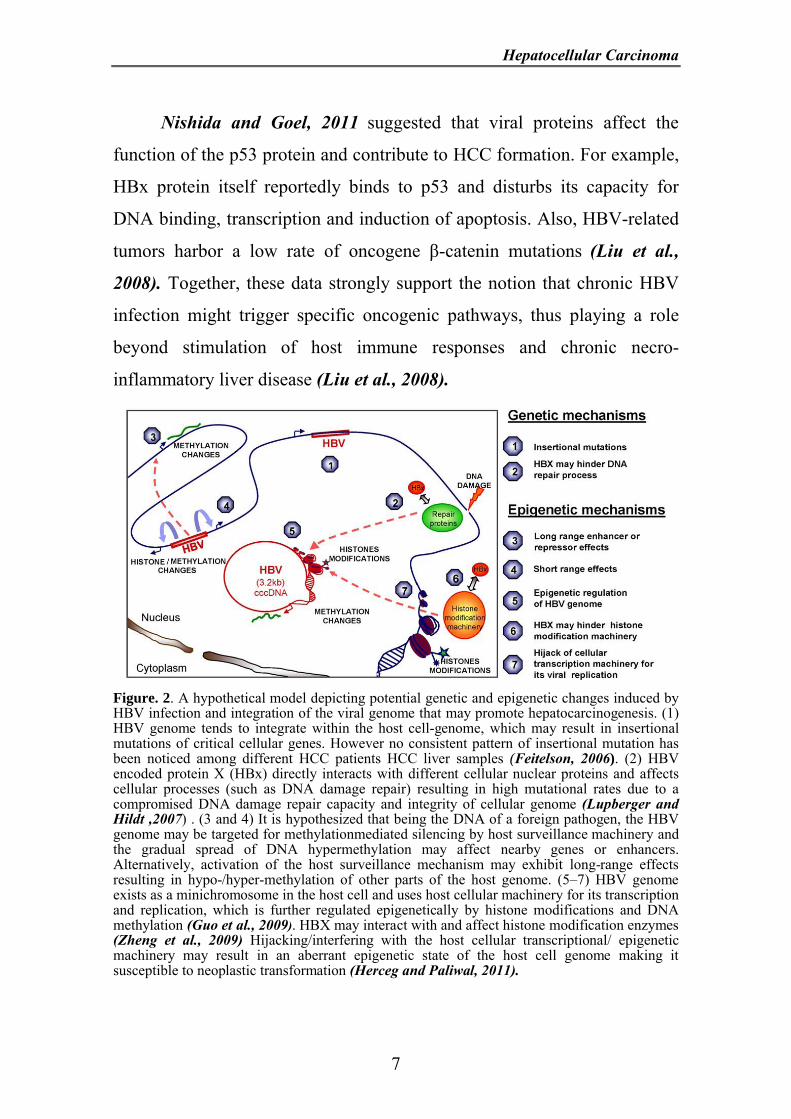
Figure. 2. A hypothetical model depicting potential genetic and epigenetic changes induced by HBV infection and integration of the viral genome that may promote hepatocarcinogenesis. (1) HBV genome tends to integrate within the host cell-genome, which may result in insertional mutations of critical cellular genes. However no consistent pattern of insertional mutation has been noticed among different HCC patients HCC liver samples (Feitelson, 2006). (2) HBV encoded protein X (HBx) directly interacts with different cellular nuclear proteins and affects cellular processes (such as DNA damage repair) resulting in high mutational rates due to a compromised DNA damage repair capacity and integrity of cellular genome (Lupberger andHildt ,2007) . (3 and 4) It is hypothesized that being the DNA of a foreign pathogen, the HBV genome may be targeted for methylationmediated silencing by host surveillance machinery and the gradual spread of DNA hypermethylation may affect nearby genes or enhancers. Alternatively, activation of the host surveillance mechanism may exhibit long-range effects resulting in hypo-/hyper-methylation of other parts of the host genome. (5–7) HBV genome exists as a minichromosome in the host cell and uses host cellular machinery for its transcription and replication, which is further regulated epigenetically by histone modifications and DNA methylation (Guo et al., 2009). HBX may interact with and affect histone modification enzymes (Zheng et al., 2009) Hijacking/interfering with the host cellular transcriptional/ epigenetic machinery may result in an aberrant epigenetic state of the host cell genome making it susceptible to neoplastic transformation (Herceg and Paliwal, 2011).