method for enhancing real-world use of a more affected arm...
TRANSCRIPT

1
Constraint-induced movement therapy (CI therapy) has been found in multiple randomized controlled trials to
be efficacious for rehabilitating upper-extremity function in chronic and subacute stroke in adults1 and cerebral palsy in children from 1 year through adolescence.2 Case series support the efficacy of CI therapy for rehabilitating upper-extremity function in traumatic brain injury3 and multiple sclerosis,4 and lower-extremity function in chronic stroke,5 traumatic brain injury,6 and multiple sclerosis.7 The magnitude of the treat-ment effect that has been reported, however, has been mark-edly variable.
The upper-extremity CI therapy protocol, as practiced in this laboratory, consists of 4 basic components8–10: (1) inten-sive training of the more affected arm for multiple days; (2) training by shaping (see Interventions section); (3) the
transfer package (TP), a set of behavioral techniques to facili-tate transfer of therapeutic gains from the treatment setting to daily life (see Interventions section and Methods in the online-only Data Supplement); and (4) prolonged motor restriction of the less affected arm.
In a representative randomized controlled trial of the full CI therapy protocol from this laboratory with 41 patients with chronic stroke, the value of the effect size index d for post-treatment gains in real-world spontaneous use of the more affected arm was 3.6.8 For comparison, 0.8 is considered a large value in the meta-analysis literature.11 All but 2 of the >400 CI therapy studies published by other laboratories report a positive treatment effect, but it is usually smaller than that obtained here. For example, a widely cited meta-analysis reports a mean d value of 0.8 for 21 CI therapy studies (total
Original Contribution
Background and Purpose—Constraint-induced movement therapy is a set of treatments for rehabilitating motor function after central nervous system damage. We assessed the roles of its 2 main components.
Methods—A 2×2 factorial components analysis with random assignment was conducted. The 2 factors were type of training and presence/absence of a set of techniques to facilitate transfer of therapeutic gains from the laboratory to the life situation (Transfer Package; TP). Participants (N=40) were outpatients ≥1-year after stroke with hemiparesis. The different treatments, which in each case targeted the more affected arm, lasted 3.5 hours/d for 10 weekdays. Spontaneous use of the more affected arm in daily life and maximum motor capacity of that arm in the laboratory were assessed with the Motor Activity Log and the Wolf Motor Function Test, respectively.
Results—Use of the TP, regardless of the type of training received, resulted in Motor Activity Log gains that were 2.4 times as large as the gains in its absence (P<0.01). These clinical results parallel previously reported effects of the TP on neuroplastic change. Both the TP and training by shaping enhanced gains on the Wolf Motor Function Test (P<0.05). The Motor Activity Log gains were retained without loss 1 year after treatment. An additional substudy (N=10) showed that a single component of the TP, weekly telephone contact with participants for 1 month after treatment, doubled Motor Activity Log scores at 6-month follow-up.
Conclusions—The TP is a method for enhancing both spontaneous use of a more affected arm after chronic stroke and its maximum motor capacity. Shaping enhances the latter. (Stroke. 2013;44:00-00.)
Key Words: constraint-induced movement therapy ■ hemiplegia ■ shaping ■ stroke rehabilitation ■ task practice ■ transfer package
Method for Enhancing Real-World Use of a More Affected Arm in Chronic Stroke
Transfer Package of Constraint-Induced Movement Therapy
Edward Taub, PhD; Gitendra Uswatte, PhD; Victor W. Mark, MD; David M. Morris, PT, PhD; Joydip Barman, PhD; Mary H. Bowman, OTR/L, C/NDT; Camille Bryson, PT; Adriana Delgado, BS;
Staci Bishop-McKay, BS
Received December 20, 2012; final revision received February 11, 2013; accepted February 25, 2013.From the Departments of Psychology (E.T., G.U., V.W.M., J.B., M.H.B., C.B., A.D., S.B.-M.), Physical Therapy (G.U., D.M.M.), Physical Medicine and
Rehabilitation (V.W.M.), and Neurology (V.W.M.), University of Alabama, Birmingham, AL.The online-only Data Supplement is available with this article at http://stroke.ahajournals.org/lookup/suppl/doi:10.1161/STROKEAHA.111.
000559/-/DC1.Correspondence to Edward Taub, PhD, Department of Psychology, University of Alabama, Birmingham, CPM 712, 1530 3rd Ave, S, Birmingham, AL
35294. E-mail [email protected]© 2013 American Heart Association, Inc.
Stroke is available at http://stroke.ahajournals.org DOI: 10.1161/STROKEAHA.111.000559
2013
26
lww
by guest on June 22, 2018http://stroke.ahajournals.org/
Dow
nloaded from
by guest on June 22, 2018http://stroke.ahajournals.org/
Dow
nloaded from
by guest on June 22, 2018http://stroke.ahajournals.org/
Dow
nloaded from
by guest on June 22, 2018http://stroke.ahajournals.org/
Dow
nloaded from
by guest on June 22, 2018http://stroke.ahajournals.org/
Dow
nloaded from
by guest on June 22, 2018http://stroke.ahajournals.org/
Dow
nloaded from
by guest on June 22, 2018http://stroke.ahajournals.org/
Dow
nloaded from
by guest on June 22, 2018http://stroke.ahajournals.org/
Dow
nloaded from
by guest on June 22, 2018http://stroke.ahajournals.org/
Dow
nloaded from
by guest on June 22, 2018http://stroke.ahajournals.org/
Dow
nloaded from
by guest on June 22, 2018http://stroke.ahajournals.org/
Dow
nloaded from
by guest on June 22, 2018http://stroke.ahajournals.org/
Dow
nloaded from
by guest on June 22, 2018http://stroke.ahajournals.org/
Dow
nloaded from
by guest on June 22, 2018http://stroke.ahajournals.org/
Dow
nloaded from
by guest on June 22, 2018http://stroke.ahajournals.org/
Dow
nloaded from
by guest on June 22, 2018http://stroke.ahajournals.org/
Dow
nloaded from
by guest on June 22, 2018http://stroke.ahajournals.org/
Dow
nloaded from
by guest on June 22, 2018http://stroke.ahajournals.org/
Dow
nloaded from
by guest on June 22, 2018http://stroke.ahajournals.org/
Dow
nloaded from
by guest on June 22, 2018http://stroke.ahajournals.org/
Dow
nloaded from

2 Stroke May 2013
N=508), ≈1/3 the d value reported here.12 However, most of these studies used attenuated or partial versions of our method. The usual missing component is the TP. In contrast, the results from this laboratory have been largely duplicated in studies from 4 laboratories that adhered to our method and whose therapists were trained here.13–16
Previous studies have found prolonged restraint of the less affected arm is not necessary to obtain a full treatment effect.5,17,18 This article reports on a study testing the contribu-tion of 2 other components: training with shaping and the TP. In a previous article derived from this study using voxel-based morphometry, we reported that treatment with the full CI ther-apy protocol, including the TP, resulted in a profuse increase in gray matter in motor areas of the brain. Use of the same proto-col, but with no TP, did not produce any detectable neuroplastic changes.19 The clinical findings from the subjects in that study are reported here; subjects were recruited from 2005–2007.
Study 1: Methods
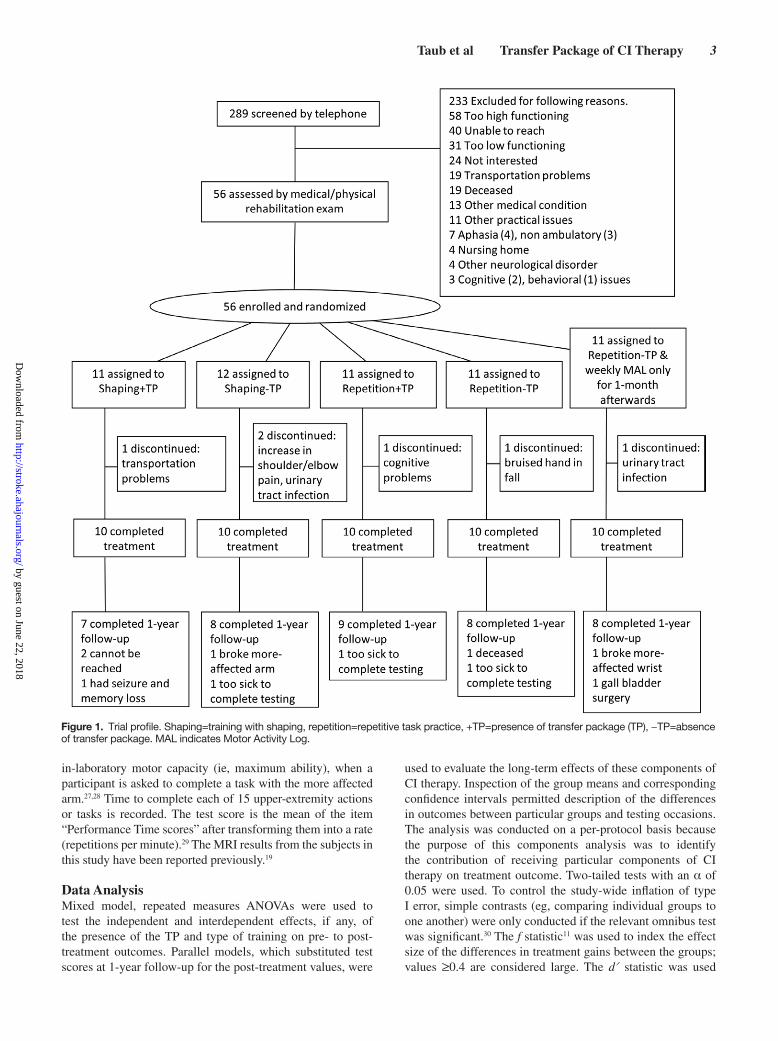
Participants, Randomization, and Informed ConsentForty-five community residents ≥1-year after stroke with upper-extremity hemiparesis were enrolled; 40 completed treatment (Figure 1). All had mild-to-moderate motor impair-ment of the more affected arm, which is categorized as a grade 2 deficit according to a classification schema used in CI ther-apy studies (Table I in the online-only Data Supplement).20 Specifically, participants were required to have extension of ≥10° at the metacarpophalangeal and one of the interphalan-geal joints of each finger, ≥10° extension or abduction of the thumb, and ≥20° extension of the wrist from a fully flexed starting position.8,21 Exclusion criteria were as follows: (1) presence of medical conditions severe enough to interfere with participation in treatment; (2) profound bilateral hearing loss with use of hearing aids (90 dB or worse); (3) legally blind status; (4) ferrous metal in the body or any condition that would preclude an MRI; (5) uncontrolled seizures; (6) phar-macological treatment for motor disability ≤3 months before treatment, for example, botulinum toxin or oral/intrathecal baclofen; and (7) previous CI therapy.
All participants provided signed informed consent before randomization. The study was performed at the University of Alabama at Birmingham, where the institutional review board for human research approved the research. Participants were informed that they would be enrolling in a project to test the importance of different components of CI therapy. Participants were randomized in equal numbers using a computer-gener-ated random numbers table to receive 1 of 4 possible combi-nations of the 2 factors to be tested: presence versus absence of the TP (+TP versus –TP) and training with shaping versus repetitive task practice (shaping versus repetition; Figure 1).
InterventionsComponents analysis was conducted with a 2×2 factorial design. The possible combinations of the 2 treatment fac-tors were represented by 4 separate groups: shaping+TP, repetition+TP, shaping-No TP, repetition-No TP.
For all groups, training took place for 10 consecutive week-days; 3 hours/d training +0.5 hours/d TP for the 2 +TP groups, and 3.5 hours/d training for the 2 −TP groups. The amount of in-laboratory treatment and participant–therapist interac-tion was thus equivalent between groups. In the +TP groups, participants wore a heavily padded safety mitt on their less affected arm to prevent use of that hand for a target of 90% of waking hours for the entire 14-day treatment period (10 training days plus 4 weekend days). In the −TP groups, par-ticipants wore the safety mitt for only in-laboratory treatment.
ShapingShaping is a training method in which a motor or behavioral objective is approached in small steps by successive approxi-mations (ie, a task is gradually made more difficult with respect to a participant’s motor capabilities). Its principles were explicitly formulated by Skinner,22,23 and they have been applied to the rehabilitation of movement.21,24 A more detailed description of the shaping process is presented in Methods in the online-only Data Supplement.
Repetitive Task PracticeThe same or similar tasks were used with the same sched-ule of administration as in shaping, and the participants were encouraged to keep trying, but no feedback was given, and tasks of increasing difficulty were not introduced.
Transfer PackageThe TP consists of a set of techniques in common use in the behavioral analysis field for the treatment of a variety of con-ditions, but they have not been used systematically in reha-bilitation. The techniques used here are as follows: behavioral contracts, daily home diary, daily administration of the Motor Activity Log (MAL) to track amount and quality of use of the more affected arm in 30 important Activities of Daily Living (ADL), problem solving to overcome perceived bar-riers to more affected arm use in ADL performance, written assignment of practice at home of both tasks performed in the laboratory, and use of the more affected arm in specified ADL, post-treatment home skill practice assignments, weekly tele-phone calls for the first month after laboratory treatment in which the MAL is given, and problem solving performance. The procedures are described in detail in Methods in the online-only Data Supplement.
MeasuresThe MAL is a scripted, structured interview21 that is reliable and valid.25 Evidence for validity of the MAL includes a strong correlation (r, range =0.71–0.91; P≤0.01) with accelerometry, an objective measure of amount of movement in the life situation.26 Participants are asked to rate the quality of movement and amount of use of their more affected arm in daily life on 30 upper-extremity activities over a specified period (eg, past week, yesterday). Only the quality of movement rating, named the Arm Use scale, is reported here because the 2 ratings are highly correlated (r=0.95; P=0.0001), and hence redundant.8,19,20,25 The minimum detectable change on the MAL Arm Use scale is 0.5 points (10% of full scale range).25,26 The test score is the mean of the item scores. The Wolf Motor Function Test (WMFT) is a valid and reliable measure of
by guest on June 22, 2018http://stroke.ahajournals.org/
Dow
nloaded from
Taub et al Transfer Package of CI Therapy 3
in-laboratory motor capacity (ie, maximum ability), when a participant is asked to complete a task with the more affected arm.27,28 Time to complete each of 15 upper-extremity actions or tasks is recorded. The test score is the mean of the item “Performance Time scores” after transforming them into a rate (repetitions per minute).29 The MRI results from the subjects in this study have been reported previously.19
Data AnalysisMixed model, repeated measures ANOVAs were used to test the independent and interdependent effects, if any, of the presence of the TP and type of training on pre- to post-treatment outcomes. Parallel models, which substituted test scores at 1-year follow-up for the post-treatment values, were
used to evaluate the long-term effects of these components of CI therapy. Inspection of the group means and corresponding confidence intervals permitted description of the differences in outcomes between particular groups and testing occasions. The analysis was conducted on a per-protocol basis because the purpose of this components analysis was to identify the contribution of receiving particular components of CI therapy on treatment outcome. Two-tailed tests with an α of 0.05 were used. To control the study-wide inflation of type I error, simple contrasts (eg, comparing individual groups to one another) were only conducted if the relevant omnibus test was significant.30 The f statistic11 was used to index the effect size of the differences in treatment gains between the groups; values ≥0.4 are considered large. The d′ statistic was used
Figure 1. Trial profile. Shaping=training with shaping, repetition=repetitive task practice, +TP=presence of transfer package (TP), −TP=absence of transfer package. MAL indicates Motor Activity Log.
by guest on June 22, 2018http://stroke.ahajournals.org/
Dow
nloaded from

4 Stroke May 2013
to index the effect size of the changes within each group or combination of groups; values 0.57 are considered large.
Trial Profile and Initial Participant CharacteristicsOf 289 candidates screened by telephone, 56 were enrolled. Of this number, 45 were randomized to 1 of the 4 groups in Study 1, and 11 were randomized to the single group in Study 2 (see Study 2: Methods and Results). In Study 1, 89% completed treatment and 80% completed MALs at 1-year follow-up. There was no difference in drop-out between groups at either post-treatment (P=0.793) or 1-year follow-up (P=0.741). Figure 1 shows the trial profile and numbers randomized to and completing treatment in each group, along with reasons for drop-out.
Study 1: ResultsParticipants were, on average, 63 years of age (range =29–88) and 3.9 years after stroke (range =1.0–11.0). Thirty-eight were right dominant before stroke; 16 had paresis on the right side. There were no significant differences at pretreatment between the Study 1 groups on any of the characteristics listed in Table II in the online-only Data Supplement (P, range=0.16–0.36), including expectation of benefit from treatment (P=0.20). Nor were there pretreatment differences on the MAL (P=0.92; Table III in the online-only Data Supplement) or WMFT (P=0.74; Table IV in the online-only Data Supplement).
Changes From Pre- to Post-treatmentTable III in the online-only Data Supplement and Figure 2A show changes at post-treatment on the MAL. Use of the TP, regardless of type of training received, resulted in gains in spontaneous use of the more affected arm in the life situation that were significantly larger than those observed in its absence (mean difference in MAL gains =1.2 points; P<0.01). Type of training received did not affect MAL gains (mean differ-ence =0.2; P=0.495). Inspection of the mean changes in each group reveals that although the −TP groups had MAL gains that were greater than the minimum detectable change on this test (Shaping−TP, mean=0.7; Repetition−TP, mean=0.8), the +TP groups had changes that were more than twice as large (Shaping+TP, mean=1.8; Repetition+TP, mean=2.1).
Table IV in the online-only Data Supplement and Figure 2C show post-treatment changes on the WMFT, which, as noted, measures maximum motor capacity in the laboratory. Use of the TP and training with shaping each made indepen-dent contributions to post-treatment WMFT Performance Rate gains (+TP versus −TP; mean difference =6.4 repeti-tions/min, P<0.05; Shaping versus Repetition, mean differ-ence =5.4, P<0.05). Inspection of the mean changes within each group suggests that effects of these 2 factors were addi-tive. Absence of both the TP and shaping resulted in no gains: Repetition−TP group, mean = −0.3. Presence of the TP or of shaping resulted in similar gains: Repetition+TP group, mean=5.7; Shaping−TP group, mean=4.7. Presence of both factors resulted in gains that were nearly double those when 1 factor alone was present: Shaping+TP group, mean=11.6.
The magnitude of the enhancement in treatment outcome produced by the TP in spontaneous use of the more affected
arm in the real world (MAL) was twice as large as that for maximum motor capacity of that arm (WMFT; f=0.8 vs 0.4; Tables III and IV in the online-only Data Supplement), which is consistent with previous data from this laboratory.5,8,9,21 Notwithstanding the difference between these 2 aspects of motor function in magnitude of treatment gains, there was a moderate correlation between them both before treat-ment (r=0.44; P<0.01) and with respect to treatment change (r=0.55, P<0.001) across all participants.
Changes From Pretreatment to 1 Year After TreatmentAs may be seen from Table III in the online-only Data Supplement and Figure 2B, there was no decrement in MAL scores after treatment ended in any of the 4 groups. Thus, the pattern of findings with respect to real-world outcome was the same at 1-year follow-up as at post-treatment.
Study 2: Methods and ResultsA separate study was performed to assess the effect of a single component of the TP, weekly phone contact with participants for the first month after treatment, and on post-treatment retention. The participants were randomly selected from the same pool of potential participants as used in Study 1 (Figure 1). None of their characteristics were significantly different from those of the participants in Study 1 (Table II and Table V in the online-only Data Supplement). During treatment, they were given repetitive task practice and no TP, just as the Repetition−TP group in Study 1. Figure 3 shows that pre- to post-treatment change on the MAL was virtually the same for these 2 groups. However, the addition of 4 weekly phone contacts for the first month after treatment substantially increased the spontaneous use of the more affected arm in the life situation. Six months after treatment, the MAL gains in this group bridged approxi-mately one half the gap in MAL gains at post-treatment between the repetitive task practice groups with and without the TP. At 1-year follow-up, the MAL score in this group had decreased to the level of the Repetition−TP group at that occasion, suggest-ing that other elements of the TP are needed to sustain MAL gains over the longer-time interval at the higher level.
Overall DiscussionThe current consensus in physical rehabilitation, including the perspective of patients, researchers, clinicians, and health care payers, is that functional activity in the life situation is the most important outcome to pursue.31–33 In the present experi-ment, training in the laboratory/clinic by itself produced a substantial real-world effect. However, the TP was by far more important for inducing transfer of training from the treatment setting to the activities of daily living, increasing real-world treatment effect by a factor of almost 2.5.
The 2 TP groups scored a mean of 1.2 on the MAL Arm Use scale at the beginning of treatment and ended treatment 2 weeks later scoring 3.1. A rating of 3, according to the verbal anchor presented to participants, represents an ability to perform a daily life activity independently. A post-treatment test score of 3.1 indicates that after treatment, participants were performing approximately half the 30 ADLs tracked
by guest on June 22, 2018http://stroke.ahajournals.org/
Dow
nloaded from

Taub et al Transfer Package of CI Therapy 5
by the MAL without the aid of the less affected arm or an external source. Converting the mean scores to the percentile scale presented to participants, the spontaneous use of the more affected arm compared to before stroke improved from 12% before treatment to 53% after treatment, an increase of 4.4 times due to treatment. This is consistent with previous research from this laboratory.8,34
Improvement on the MAL at post-treatment was 2.4 times greater in the groups that received the TP than in the groups
that did not, even though all groups received more affected arm training of the same duration and intensity. Moreover, this advantage persisted for the entire year of follow-up; there was no decrement in MAL gains in any of the Study 1 groups. The power of TP is further indicated by the fact that the introduction of a single one of its components in Study 2, weekly phone contacts for the first month after treatment, resulted in bridging the performance gap between groups with and without the TP at post-treatment by half, 6 months
Figure 2. Treatment outcome for real-world spontaneous use of more affected arm (Motor Activity Log [MAL]) and the maxi-mum motor capacity of that extremity (Wolf Motor Function Test [WMFT] performance rate). MAL outcomes at post-treatment and 1-year follow-up are graphed in A and B, respectively. WMFT post-treatment outcomes are graphed in C. In all 3 panels, change from pretreatment is plotted. TP indicates transfer package.
Figure 3. Real-world constraint-induced movement (CI) therapy outcome for groups from study 1 with the transfer package (TP; Shaping+TP, Repetition+TP), no TP (Shaping−TP, Repetition−TP), and no TP during treatment but with phone contact in follow-up only (Study 2 participants). Study 2 participants, who did not receive the TP during treatment, had virtually the same pre- to post-treatment Motor Activ-ity Log (MAL) gains as the −TP groups in Study 1, which were less than half of the MAL gains made by +TP groups in Study 1. After treatment, Study 2 participants had 4 weekly phone calls for the first month after treatment in which the MAL and problem solving were performed. Six months after treatment, approximately half the difference in spontaneous use of the more affected arm between the −TP and +TP groups had been bridged. Data is ipsitized (ie, scores at pretreatment are set to zero).
by guest on June 22, 2018http://stroke.ahajournals.org/
Dow
nloaded from

6 Stroke May 2013
afterward. In future research, it would be of value to perform components analysis to determine the role of each of the individual elements of the TP.
The question arises as to whether the TP increases treat-ment effect by increasing the amount of practice of more affected arm use. Alternatively, it is possible that the TP pro-motes integration of therapeutic gains achieved in the labo-ratory into real-world activities so that more affected arm use becomes habitual. These 2 possibilities are not mutually exclusive. Addressing this question in future research would be of mechanistic and theoretical interest; however, from the point of view of practical therapeutics, the resolution of this important issue does not really matter. The TP seems to be a means of increasing real-world treatment outcome that does not involve increasing costly therapist time; this would be of considerable value whatever the mechanism by which the TP achieved its effect.
Sources of FundingThis research was supported by grant HD34273 from the National Institutes of Health.
DisclosuresNone.
References 1. Langhorne P, Coupar F, Pollock A. Motor recovery after stroke: a sys-
tematic review. Lancet Neurol. 2009;8:741–754. 2. Hoare B, Wasiak J, Imms C, Carey L. Constraint-induced movement
therapy in the treatment of the upper limb in children with hemiplegic cerebral palsy. Cochrane Database Syst Rev. 2007:Art. No.: CD004149. DOI:004110.001002/14651858.CD14004149.pub14651852.
3. Shaw SE, Morris DM, Uswatte G, McKay S, Meythaler JM, Taub E. Constraint-induced movement therapy for recovery of upper-limb function following traumatic brain injury. J Rehabil Res Dev. 2005;42:769–778.
4. Mark VW, Taub E, Bashir K, Uswatte G, Delgado A, Bowman MH, et al. Constraint-induced movement therapy can improve hemipa-retic progressive multiple sclerosis. Preliminary findings. Mult Scler. 2008;14:992–994.
5. Taub E, Uswatte G, Pidikiti R. Constraint-induced movement therapy: a new family of techniques with broad application to physical rehabilita-tion–a clinical review. J Rehabil Res Dev. 1999;36:237–251.
6. Morris DM, Shaw SE, Mark VW, Uswatte G, Barman J, Taub E. The influence of neuropsychological characteristics on the use of CI ther-apy with persons with traumatic brain injury. NeuroRehabilitation. 2006;21:131–137.
7. Mark VW, Taub E, Uswatte G, Bashir K, Cutter GR, Bryson C, et al. Constraint-induced movement therapy for the lower extremities in multi-ple sclerosis: case series with 4-year follow-up. Arch Phys Med Rehabil. 2013, in press.
8. Taub E, Uswatte G, King DK, Morris D, Crago JE, Chatterjee A. A pla-cebo-controlled trial of constraint-induced movement therapy for upper extremity after stroke. Stroke. 2006;37:1045–1049.
9. Taub E, Uswatte G, Mark VW, Morris DM. The learned nonuse phenomenon: implications for rehabilitation. Eura Medicophys. 2006;42:241–256.
10. Morris D, Taub E, Mark V. Constraint-induced movement therapy (CI therapy): characterizing the intervention protocol Eura Medicophys. 2006;42:257–268. PMID17039224.
11. Cohen J. Statistical Power Analysis for the Behavioral Sciences. Hillsdale, NJ: Lawrence Erlbaum; 1988.
12. Sirtori V, Corbetta D, Moja L, Gatti R. Constraint-induced move-ment therapy for upper extremities in stroke patients (Review). Cochrane Database Syst Rev. 2009:Art. No.: CD004433. DOI: 004410.001002/14651858.CD14004433.pub14651852.
13. Miltner WHR, Bauder H, Sommer M, Dettmers C, Taub E. Effects of constraint-induced movement therapy on chronic stroke patients: a repli-cation. Stroke. 1999;30:586–592. PMID10066856.
14. Kunkel A, Kopp B, Muller G, Villringer K, Villringer A, Taub E, et al. Constraint-induced movement therapy: a powerful new technique to induce motor recovery in chronic stroke patients. Arch Phys Med Rehabil. 1999;80:624–628. PMID10378486.
15. Sterr A, Elbert T, Berthold I, Kölbel S, Rockstroh B, Taub E. Longer versus shorter daily constraint-induced movement therapy of chronic hemiparesis: an exploratory study. Arch Phys Med Rehabil. 2002;83:1374–1377. PMID12370871.
16. Dettmers C, Teske U, Hamzei F, Uswatte G, Taub E, Weiller C. Distributed form of constraint-induced movement therapy improves functional outcome and quality of life after stroke. Arch Phys Med Rehabil. 2005;86:204–209.
17. Uswatte G, Taub E, Morris D, Barman J, Crago J. Contribution of the shaping and restraint components of constraint-induced movement ther-apy to treatment outcome. NeuroRehabilitation. 2006;21:147–156.
18. Ploughman M, Corbett D. Can forced-use therapy be clinically applied after stroke? An exploratory randomized controlled trial. Arch Phys Med Rehabil. 2004;85:1417–1423.
19. Gauthier LV, Taub E, Perkins C, Ortmann M, Mark VW, Uswatte G. Remodeling the brain: plastic structural brain changes produced by dif-ferent motor therapies after stroke. Stroke. 2008;39:1520–1525.
20. Taub E, Uswatte G, Bowman MH, Mark VW, Delgado A, Bryson C, et al. Effect of CI therapy on arm use in chronic stroke patients with plegic hands. Arch Phys Med Rehabil. 2013;94:86–94.
21. Taub E, Miller NE, Novack TA, Cook EW III, Fleming WC, Nepomuceno CS, et al. Technique to improve chronic motor deficit after stroke. Arch Phys Med Rehabil. 1993;74:347–354.
22. Skinner BF. The Behavior of Organisms. New York, NY: Appleton-Century-Crofts; 1938.
23. Skinner BF. The Technology of Teaching. New York, NY: Appleton-Century-Crofts; 1968.
24. Taub E, Crago J, Burgio L, Groomes T, Cook EW, DeLuca S, et al. An operant approach to overcoming learned nonuse after CNS damage in monkeys and man: the role of shaping. J Exp Anal Behav. 1994;61: 281–293. PMC1334416.
25. Uswatte G, Taub E, Morris D, Light K, Thompson PA. The Motor Activity Log-28: assessing daily use of the hemiparetic arm after stroke. Neurology. 2006;67:1189–1194.
26. Uswatte G, Foo WL, Olmstead H, Lopez K, Holand A, Simms LB. Ambulatory monitoring of arm movement using accelerometry: an objective measure of upper-extremity rehabilitation in persons with chronic stroke. Arch Phys Med Rehabil. 2005;86:1498–1501.
27. Wolf SL, Catlin PA, Ellis M, Archer AL, Morgan B, Piacentino A. Assessing Wolf motor function test as outcome measure for research in patients after stroke. Stroke. 2001;32:1635–1639.
28. Morris D, Uswatte G, Crago J, Cook EW, III, Taub E. The reliability of the Wolf Motor Function Test for assessing upper extremity motor func-tion following stroke. Arch Phys Med Rehabil. 2001;82:750–755.
29. Hodics TM, Nakatsuka K, Upreti B, Alex A, Smith PS, Pezzullo JC. Wolf Motor Function Test for characterizing moderate to severe hemipa-resis in stroke patients. Arch Phys Med Rehabil. 2012;93:1963–1967.
30. Keppel G, Zedeck S. Data Analysis for Research Designs: Analysis of Variance and Multiple Regression/Correlation Approaches. New York, NY: W. H. Freeman and Company; 1989.
31. Uswatte G, Taub E. Implications of the learned nonuse formulation for measuring rehabilitation outcomes: lessons from Constraint-Induced Movement therapy. Rehabil Psychol. 2005;50:34–42.
32. Keith RA. Conceptual basis of outcome measures. Am J Phys Med Rehabil. 1995;74:73–80.
33. Granger CV. The emerging science of functional assessment: our tool for outcomes analysis. Arch Phys Med Rehabil. 1998;79:235–240.
34. Taub E, Lum PS, Hardin P, Mark VW, Uswatte G. AutoCITE: auto-mated delivery of CI therapy with reduced effort by therapists. Stroke. 2005;36:1301–1304.
by guest on June 22, 2018http://stroke.ahajournals.org/
Dow
nloaded from

Bowman, Camille Bryson, Adriana Delgado and Staci Bishop-McKayEdward Taub, Gitendra Uswatte, Victor W. Mark, David M. Morris, Joydip Barman, Mary H.
Transfer Package of Constraint-Induced Movement TherapyMethod for Enhancing Real-World Use of a More Affected Arm in Chronic Stroke:
Print ISSN: 0039-2499. Online ISSN: 1524-4628 Copyright © 2013 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Stroke published online March 21, 2013;Stroke.
http://stroke.ahajournals.org/content/early/2013/03/21/STROKEAHA.111.000559World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://stroke.ahajournals.org/content/suppl/2013/03/21/STROKEAHA.111.000559.DC1Data Supplement (unedited) at:
http://stroke.ahajournals.org//subscriptions/
is online at: Stroke Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer process is available in the
Request Permissions in the middle column of the Web page under Services. Further information about thisOnce the online version of the published article for which permission is being requested is located, click
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office.Strokein Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
by guest on June 22, 2018http://stroke.ahajournals.org/
Dow
nloaded from

SUPPLEMENTAL MATERIAL
Supplemental Methods
Shaping
For rehabilitation, shaping involves a) providing immediate and very frequent feedback
concerning improvements in the quality of movement, b) selecting tasks that are tailored to
address the motor deficits of individual participants, c) modeling, prompting, and cuing of task
performance, and d) systematically increasing the difficulty level of the task performed in small
steps when improvement is present for a period of time. A battery of over 120 tasks with a
shaping plan for each has been developed by the CI Therapy Research Group. The principles for
use as guidelines for shaping to induce recovery of motor function are presented in 1 (Appendix
1); 3 sample shaping tasks with shaping plans are also presented there. Training with adult
participants is carried out in sets of 10 discrete 30 sec trials with 1 min rests between trials and
longer rests between sets of trials as needed to reduce fatigue. Approximately twenty-five trials
are given per hour; higher functioning participants sometimes need to be slowed down to equate
amount of training between patients with different levels of motor ability. Task performance is
timed by stopwatch and a written record of performance times is kept; it is referred to frequently
and the time is reported to the participant at the end of each trial. This is typically highly
motivating, encouraging the participants to keep trying to improve on their “personal best” in the
manner of a video game. In this laboratory shaping has two distinct levels. The first level is
directed toward improving the speed and quality of movement from trial to trial within a task
with frequent feedback and encouragement being given. The second level involves introducing a
new task that is similar to but more difficult than the one being used when motor performance
improves to the point where the therapist feels that it can be accomplished by the participant
1

(e.g., picking up and moving as many standard checker game counters as possible in 30 sec,
followed after skill acquisition by use of slick round glass marbles). When the emphasis is on the
between-level task modification process, the procedure is sometimes referred to as “adaptive task
practice.”2 The procedure employed here involves use of both levels of shaping but focuses more
attention on improving within-level task performance.
Component Procedures of the Transfer Package
Behavioral Contract. At the outset of treatment, the therapist negotiates a contract with the
participant and separately with the caregiver, if one is available, in which they agree that the
participant will use his or her more impaired arm as much as possible outside the laboratory and
wear the restraint device whenever it is safe for up to 90% of waking hours. Specific activities
during which the participant can practice using the more impaired arm are discussed and written
down. At the end of this process, the negotiated document is signed by the patient (or caregiver),
the therapist, and a witness to emphasize the character of the document as a contract.
Daily home diary. During treatment, the participants catalog how much they have used the more-
affected arm for the activities specified in the behavioral contract and worn the restraint device.
The diary is kept for the part of the day spent outside the laboratory and is reviewed in detail
each morning with the therapist.
Daily administration of the Motor Activity Log (MAL). The MAL collects information about use
of the more-affected arm in 30 important and commonly performed ADL. The daily repetition of
“how well” participants complete the activities in this detailed report is probed and verified in a
number of ways3 and serves to keep participants’ attention on use of the more-affected arm
outside the laboratory.
2

Problem Solving. Daily during treatment and in four weekly phone contacts following treatment,
the therapist helps participants to think through any barriers to using their more impaired arm
and ways to overcome it. For example, if a participant is concerned about spilling liquid from a
glass, the therapist may suggest only filling the glass half way. If a participant is embarrassed by
clumsiness in use of the more-affected arm in feeding themselves in a restaurant (many of the
laboratory’s patients are from out of town), the therapist may suggest eating in the hotel room.
Home skill assignments during treatment. Participants are assigned on a written check-off sheet
10 specific ADL tasks in which the more-affected arm should be used, with 5 easy tasks for that
participant and 5 more difficult (e.g., carrying the mail, sorting the mail, opening the curtains,
making the bed, feeding a pet). Alternately, the participants might be assigned 6 tasks daily
similar to ones carried out in the laboratory (3 easy and 3 more difficult) on a written check-off
sheet to be performed repetitively with their more-affected arm. The tasks typically use materials
that are commonly available (e.g., transferring dried beans on a spoon from one bowl to another)
and are chosen for practice to improve the participant’s most significant movement deficits.
When answers to the MAL or check-off lists indicate a lack of performance, the therapist can
then inquire into the reasons for this and problem solve with the participant/caregiver on how to
reverse this trend.
Home skill assignments after treatment. Toward the end of treatment, a written individualized
post-treatment home skill practice program is developed and given to the patient. There are 7
separate lists, one for each day of the week, that are to be repeated weekly. Each list contains 3
repetitive tasks to be carried out for 15-30 minutes and 7 ADL in which the participant is asked
to use the more-affected hand selected from a list of approximately 400 developed by the
laboratory.
3

Post-treatment telephone contacts. Participants are contacted weekly for the month after
treatment by telephone. During each contact the How Well and How Often Scales of the MAL
are administered and problem solving is carried out.
The strategies used in the CI therapy transfer package are in common use in behavioral
interventions for treating such problems as disruptive classroom behaviors, drug addiction, and
medication adherence; but they have not been employed in a systematic way in physical
neurorehabilitation.4
Self-monitoring is one of the most commonly used strategies and involves asking
participants to observe and document their target behaviors.5-12 For example, Rhode et al.
showed the importance of self-monitoring in transferring behavior treatment gains from a
resource room to regular classroom situation.13 When self-monitoring interventions were utilized
in the resource room only, children's behavior improved only in this setting. However, when
these same interventions were implemented in the classroom, behavior gains generalized to the
classroom setting and were persistent even after termination of the intervention.13 Just the act of
monitoring a target behavior is thought to be effective because it helps patients attend to
appropriate stimuli and is self-reinforcing. In CI therapy, for example, recording instances when
the more-impaired arm is used in a daily diary may help participants to immediately notice small,
gradual improvements in use of their arm that participants would not notice otherwise until later
in treatment when improvements are more pronounced. The MAL carried out in interaction with
the therapist also has an important self-monitoring function.
Contracting, i.e. negotiating specific behaviors that participants agree to do, has also been
shown to be efficacious in promoting behavior change. Contracting indicates the behaviors that a
participant agrees to carry out and those that are not acceptable. Positive findings for contracting
4

have been observed in treatment of cocaine-dependent outpatients 14 and adherence to behavior
modification training for parents of children with behavior problems.15 The CI therapy transfer
package uses contracting with both participants and caregivers to increase compliance with
home-based portions of the therapy. For the participant, this includes attempting to use the more-
impaired arm at home, wearing the restraint device on the less-impaired arm, and doing home
skill practice exercises; for the caregiver the behavioral contract might involve agreement to
assist in the performance of certain activities in a gradually diminishing fashion, but often more
importantly to provide less help for the participant in carrying out other activities with the more-
impaired arm. The behavioral contract is frequently renegotiated part-way through treatment as
the participant’s motor ability improves.
Telephone contacts are also a means of increasing treatment compliance. They have been
successful at promoting behavior change in a variety of areas, such as increasing fruit and
vegetable consumption,16 reducing HbAlc levels in diabetics,17 increasing physical activity,18 and
complying with mammography recommendations.19 Mixed results have been obtained in studies
employing telephone interventions to promote compliance with pharmacological management of
hypertension 20, 21 and to reduce coronary disease.22 However, the interventions used varied
widely between studies, possibly accounting for the array of findings. In C1 therapy, the 4
weekly follow-up phone calls in the first month after treatment, which include administration of
the MAL, is thought to be effective in increasing adherence to CI therapy at home by extending
therapist-reinforcement of increased more-impaired arm use into the post-treatment period. The
follow-up phone calls also provide an opportunity for therapists to continue to model problem-
solving for participants.
5

Problem-solving interventions can also be effective for overcoming barriers to behavior
change. Problem-solving interventions teach individuals to identify obstacles that hinder them,
generate potential solutions, select a solution to implement, evaluate the outcome, and choose
another solution if needed.6, 11, 21, 23 Problem-solving interventions have been associated with
positive health behavior changes such as managing diabetes,24 compliance with rheumatoid
arthritis treatment,25 and relief of anxiety/depression symptoms.26 In CI therapy, therapists help
participants to find solutions to apparent obstacles to use of their more-impaired arm that
participants raise when reviewing the daily diary or completing the MAL. It is thought that by
modeling appropriate problem-solving behavior during CI therapy and in the follow-up MAL
telephone contacts, the therapists stimulate participants to effectively solve new problems that
arise in using their more-impaired arm after in-person contact with therapists has ended.
Function of the Transfer Package
In most rehabilitation regimens, the participant is required to carry out exercises guided
by a therapist primarily during treatment sessions. The TP makes the patient a more active
participant in their own improvement, not only during the treatment sessions but also at home.
The TP provides a systematic means of specifying explicitly what the participant is expected to
do when outside the treatment setting, monitoring what in fact is done, and providing a structure
within which to solve apparent barriers to carrying out treatment goals. Thus, the TP permits
participants to be immersed in a therapeutic environment for a meaningful portion of their day.
Therapy is not confined to the limited period that the current reimbursement system permits. It
has been recognized by many therapists from the outset of the rehabilitation field that optimal
therapy would be carried out “24/7”. Application of the TP may represent an initial step in this
direction. Finally, it should be noted that the TP can be used in conjunction with many other
6

7
physical rehabilitation regimens and can be carried out in a relatively brief period of time.
Therefore, it might be possible to employ it with other rehabilitation treatments to increase their
outcome.
ONLINE SUPPLEMENT Supplemental Tables
8

Table S1. Schema for Classifying More-affected Arm Impairment in People with Upper-extremity Hemiparesis* Severity of Impairment
Minimum Active Range of Motion Required
Shoulder
Elbow
Wrist
Fingers
Thumb
Grade 2
Flexion ≥45° and Abduction ≥45°
Extension ≥20° from a 90° flexed starting position
Extension ≥20° from a fully flexed starting position
Extension of all MCP and IP (either PIP or DIP) joints ≥10°†
Extension or abduction of thumb ≥10°
Grade 3
Flexion ≥45° and Abduction ≥45°
Extension ≥20° from a 90° flexed starting position
Extension ≥10° from a fully flexed starting position
Extension ≥10° MCP and IP (either PIP or DIP) joints of at least 2 fingers†
Extension or abduction of thumb ≥10°
Grade 4
Flexion ≥45° and Abduction ≥45°
Extension ≥20° from a 90° flexed starting position
Extension ≥10° from a fully flexed starting position
Extension of at least 2 fingers >0° and <10°‡
Extension or abduction of thumb ≥10°
Grade 5A§
At least one of the following: Flexion ≥30° abduction ≥30° scaption ≥30°
Initiation of extension| |
Must be able to either initiate extension of the wrist or initiate extension of one digit
Grade 5B§
At least one of the following: Flexion ≥30° abduction ≥30° scaption ≥30°
Extension ≥20º from a 90º flexed starting position
No active movement required for the wrist, fingers, or thumb
*In this system, people are placed in the highest grade at which they can meet or exceed each minimum movement criterion for each joint 3 times in 1 minute. Anybody who cannot meet the minimum movement criterion for Grade 5A or 5B is placed in Grade 6. Importantly, placement in any of the Grades also requires a substantial deficit in use of the more-affected arm as documented by a score of less than 2.5 on MAL (see Measures) and a minimum degree of passive ROM. For Grades 2-4 the minimum passive ROM criteria are: shoulder flexion and abduction of at least 90° and shoulder external rotation of at least 45°, elbow extension to within 30° of the normal limit, forearm supination to at least 45°, forearm pronation to at least 45° from neutral, wrist extension to at least neutral, and MCP joint extension to within 35° of the normal limit. For Grades 5A and 5B, the passive ROM criteria are the same, except for the following relaxations of the requirements: a) forearm supination to neutral instead of to 45° and b) wrist extension to within 45° of
9

neutral instead of to neutral. †Informally assessed by being able to pick up and drop a tennis ball. ‡Informally assessed by being able to pick up and drop a washcloth. §Grade 5B is distinguished from 5A by the absence of any active extension at the wrist, fingers, or thumb on the more-affected hand. However, greater active extension of the elbow is required for Grade 5B than 5A. Without a greater degree of movement at the elbow to compensate for the lack of any movement at the hand, the movement capacity specified by Grade 5B would be too low to permit training with even rudimentary functional tasks. Note that people who meet the Grade 5A hand and Grade 5B elbow criteria would be placed in Grade 5A. People who meet the Grade 5B hand criterion but fail to meet the Grade-5B elbow criterion, even though they exceed the Grade 5A elbow criterion, would fall into Grade 6. | | Initiation is defined here as minimal movement, i.e., below the level that can be measured reliably by goniometry. CIMT=Constraint-Induced Movement therapy. MCP= metacarpophalangeal; IP=interphalangeal. PIP=proximal interphalangeal. DIP=distal interphalangeal. ROM=range of motion. MAL=Motor Activity Log.
10
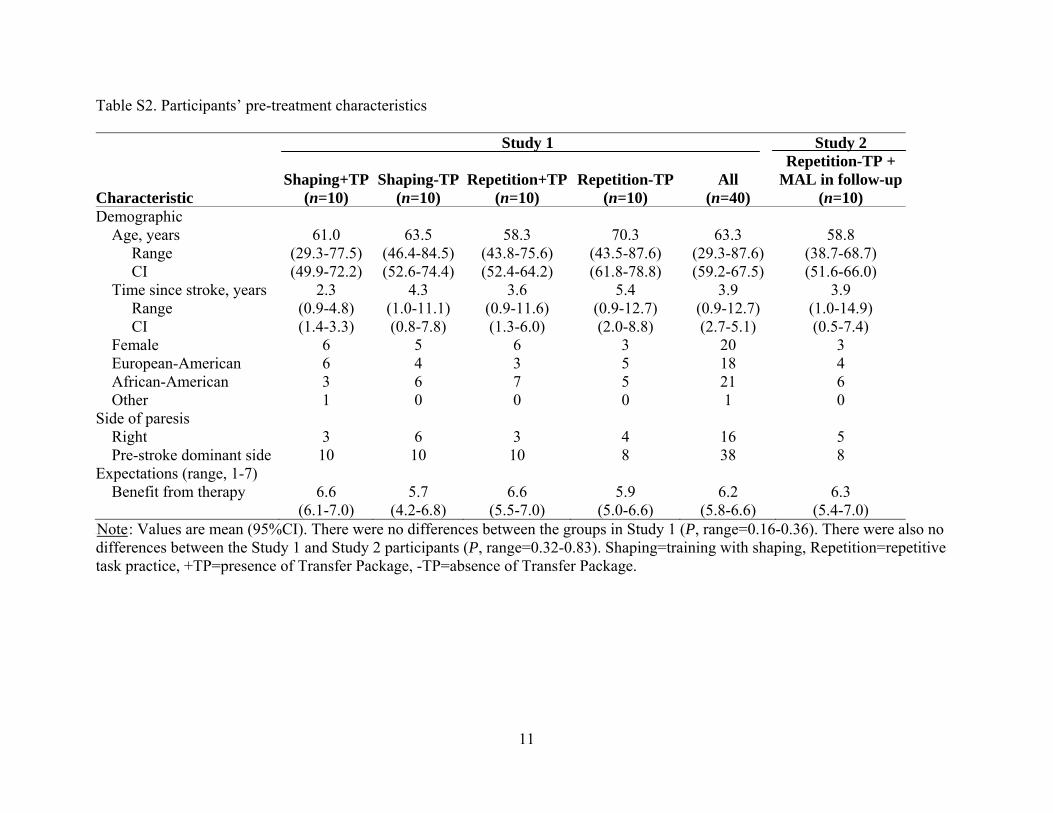
Table S2. Participants’ pre-treatment characteristics
Characteristic
Study 1 Study 2
Shaping+TP(n=10)
Shaping-TP(n=10)
Repetition+TP(n=10)
Repetition-TP(n=10)
All (n=40)
Repetition-TP + MAL in follow-up
(n=10) Demographic Age, years Range CI
61.0 (29.3-77.5) (49.9-72.2)
63.5 (46.4-84.5) (52.6-74.4)
58.3 (43.8-75.6) (52.4-64.2)
70.3 (43.5-87.6) (61.8-78.8)
63.3 (29.3-87.6) (59.2-67.5)
58.8 (38.7-68.7) (51.6-66.0)
Time since stroke, years Range CI
2.3 (0.9-4.8) (1.4-3.3)
4.3 (1.0-11.1) (0.8-7.8)
3.6 (0.9-11.6) (1.3-6.0)
5.4 (0.9-12.7) (2.0-8.8)
3.9 (0.9-12.7) (2.7-5.1)
3.9 (1.0-14.9) (0.5-7.4)
Female 6 5 6 3 20 3 European-American 6 4 3 5 18 4 African-American 3 6 7 5 21 6 Other 1 0 0 0 1 0 Side of paresis Right 3 6 3 4 16 5 Pre-stroke dominant side 10 10 10 8 38 8 Expectations (range, 1-7) Benefit from therapy 6.6
(6.1-7.0) 5.7
(4.2-6.8) 6.6
(5.5-7.0) 5.9
(5.0-6.6) 6.2
(5.8-6.6) 6.3
(5.4-7.0) UNoteU: Values are mean (95%CI). There were no differences between the groups in Study 1 (P, range=0.16-0.36). There were also no differences between the Study 1 and Study 2 participants (P, range=0.32-0.83). Shaping=training with shaping, Repetition=repetitive task practice, +TP=presence of Transfer Package, -TP=absence of Transfer Package.
11
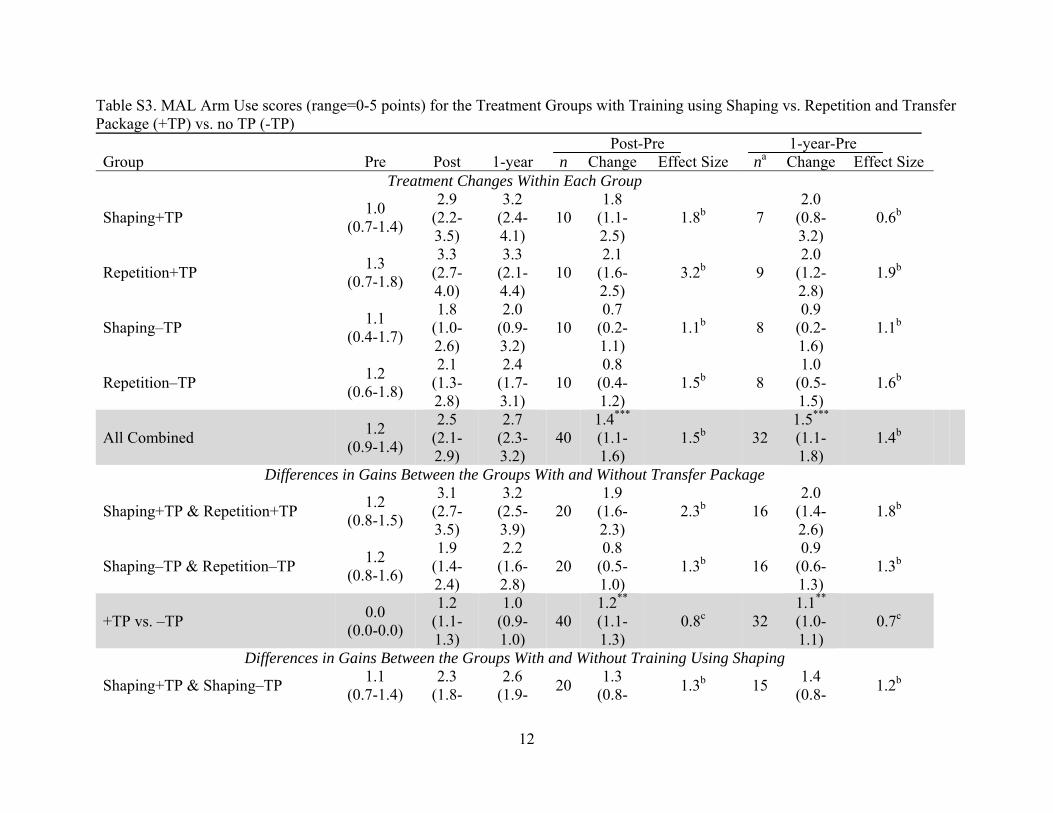
Table S3. MAL Arm Use scores (range=0-5 points) for the Treatment Groups with Training using Shaping vs. Repetition and Transfer Package (+TP) vs. no TP (-TP) Post-Pre 1-year-Pre Group Pre Post 1-year n Change Effect Size na Change Effect Size
Treatment Changes Within Each Group
Shaping+TP 1.0 (0.7-1.4)
2.9 (2.2-3.5)
3.2 (2.4-4.1)
10 1.8
(1.1-2.5)
1.8b 7 2.0
(0.8-3.2)
0.6b
Repetition+TP 1.3 (0.7-1.8)
3.3 (2.7-4.0)
3.3 (2.1-4.4)
10 2.1
(1.6-2.5)
3.2b 9 2.0
(1.2-2.8)
1.9b
Shaping–TP 1.1 (0.4-1.7)
1.8 (1.0-2.6)
2.0 (0.9-3.2)
10 0.7
(0.2-1.1)
1.1b 8 0.9
(0.2-1.6)
1.1b
Repetition–TP 1.2 (0.6-1.8)
2.1 (1.3-2.8)
2.4 (1.7-3.1)
10 0.8
(0.4-1.2)
1.5b 8 1.0
(0.5-1.5)
1.6b
All Combined 1.2 (0.9-1.4)
2.5 (2.1-2.9)
2.7 (2.3-3.2)
40 1.4*** (1.1-1.6)
1.5b 32 1.5*** (1.1-1.8)
1.4b
Differences in Gains Between the Groups With and Without Transfer Package
Shaping+TP & Repetition+TP 1.2 (0.8-1.5)
3.1 (2.7-3.5)
3.2 (2.5-3.9)
20 1.9
(1.6-2.3)
2.3b 16 2.0
(1.4-2.6)
1.8b
Shaping–TP & Repetition–TP 1.2 (0.8-1.6)
1.9 (1.4-2.4)
2.2 (1.6-2.8)
20 0.8
(0.5-1.0)
1.3b 16 0.9
(0.6-1.3)
1.3b
+TP vs. –TP 0.0 (0.0-0.0)
1.2 (1.1-1.3)
1.0 (0.9-1.0)
40 1.2** (1.1-1.3)
0.8c 32 1.1** (1.0-1.1)
0.7c
Differences in Gains Between the Groups With and Without Training Using Shaping
Shaping+TP & Shaping–TP 1.1 (0.7-1.4)
2.3 (1.8-
2.6 (1.9- 20 1.3
(0.8- 1.3b 15 1.4 (0.8- 1.2b
12

2.8) 3.3) 1.7) 2.0)
Repetition+TP & Repetition–TP 1.2 (0.9-1.6)
2.7 (2.1-3.2)
2.9 (2.2-3.5)
20 1.5
(1.0-1.9)
1.7b 17 1.5
(1.0-2.0)
1.5b
Shaping vs. Repetition 0.2 (0.1-0.3)
0.4 (0.3-0.5)
0.3 (0.2-0.3)
40 0.2
(0.1-0.3)
0.1c 32 0.1
(0.1-0.2)
0.1c
Note. *P<0.05, **P<0.01, ***P<0.001. The interaction effect (Type of Training x Presence of Transfer Package) was not significant at post-treatment (P=.795) or at 1-year follow-up (P=.365). Hence, no simple contrasts were conducted. In other words, statistical testing was only conducted for the 3 rows shaded in grey. The first of which presents data that are the basis for the omnibus test of the effect of treatment on MAL scores, regardless of presence or absence of the TP and type of training. The data in the second and third rows shaded in grey are the basis for the omnibus tests of the main effects of presence of the TP and type of training, respectively. Since statistical testing was not conducted for the data in the other rows, the absence of a symbol marking a P value <0.05 does not indicate that the change observed was not statistically significant. aReasons for missing data are given in the trial profile in Figure 1. As noted in Study 1: Methods, there was no difference in incidence of missing data across groups. Furthermore, the post-treatment MAL scores of the 20% of participants without data at 1-year were not significantly different from the post-treatment scores of those with 1-year data, which suggests that dissatisfaction with small treatment gains was not the reason that the participants had missing 1-year data (P=0.508). bCohen’s d' is a repeated measures index of effect size (large d' =.57); it is the mean pre- to post-treatment change divided by the SD of the change.27 cCohen’s f is a measure of effect size (large f = 0.4); it indexes the magnitude of the difference in pre- to post-treatment change between the two groups being compared. For example, for the test of the effect of type of training, it is the variance in MAL scores accounted for by type of training (shaping vs. repetition) x testing occasion (pre, post) interaction divided by the error variance for this factor.27 MAL=Motor Activity Log. No sex-based or racial/ethnic-based differences were present.
13

Table S4. WMFT Performance Rate Scores (repetitions/minute) for the Treatment Groups with Training using Shaping vs. Repetition and Transfer Package (+TP) vs. no TP (-TP) Group Pre Post Change Effect Size
Pre- to Post-treatment Changes Within Each Group
Shaping+TP 29.3 (21.2-37.5)
40.9 (29.4-52.4)
11.6 (3.3-19.9) 1.0a
Repetition+TP 36.2 (26.0-46.4)
41.9 (31.0-52.8)
5.7 (1.2-10.1) 0.9a
Shaping–TP 32.4 (19.3-45.5)
37.1 (23.2-50.9)
4.7 (1.6-7.8) 1.1a
Repetition–TP 34.5 (25.1-43.9)
34.2 (23.8-44.5)
-0.3 (-5.3-4.6) -0.1a
All Combined 33.1 (28.6-37.7)
38.5 (33.4-43.7)
5.4*** (2.7-8.2) 0.6a
Differences in Gains Between the Groups With and Without Transfer Package
Shaping+TP & Repetition+TP 32.8 (26.7-38.9)
41.4 (34.3-48.6)
8.6 (4.2-13.1) 0.9a
Shaping–TP & Repetition–TP 33.5 (26.2-40.7)
35.6 (27.8-43.5)
2.2 (-0.7-5.1) 0.4a
+TP vs. –TP 0.7 (0.0-1.4)
5.8 (5.0-6.6)
6.4* (6.0-6.8) 0.4b
Differences in Gains Between the Groups With and Without Training Using Shaping
Shaping + TP & Shaping – TP 30.9 (23.9-37.9)
39.0 (30.9-47.2)
8.1 (3.8-12.5) 0.9a
Repetition + TP & Repetition – TP 35.4 (29.1-41.6)
38.0 (31.0-45.1)
2.7 (-0.7-6.0) 0.4a
Shaping vs. Repetition 4.5 (3.8-5.2)
1.0 (0.2-1.8)
5.4* (5.0-5.8) 0.3b
Note. *P<0.05, **P<0.01, ***P<0.001. The interaction effect (Type of Training x Presence of Transfer Package) was not significant (P=.858). Hence, no simple contrasts were conducted. In other words, statistical testing was only conducted for the 3 rows shaded in grey. The first of which presents data that are the basis for the omnibus test of the effect of treatment on WMFT scores, regardless of presence or absence of the TP and type of training. The data in the second and third rows shaded in grey are the basis for the omnibus tests of the main effects of presence of the TP and type of training, respectively. Since statistical testing was not conducted for the data
14

in the other rows, the absence of a symbol marking a P value <0.05 does not indicate that the change observed was not statistically significant. There were no missing data at post-treatment. However, 1-year follow-up data are not reported for the WMFT because about half of the participants lived out of town and did not return to the laboratory on this testing occasion. Only 20% of the data were missing for the MAL because this instrument can be administered over the telephone if necessary. aCohen’s d' is a repeated measures index of effect size (large d' =.57); it is the mean pre- to post-treatment change divided by the SD of the change.27 cCohen’s f is a measure of effect size (large f = 0.4); it indexes the magnitude of the difference in pre- to post-treatment change between the two groups being compared. For example, for the test of the effect of type of training, it is the variance in WFMT scores accounted for by type of training (shaping vs. repetition) x testing occasion (pre, post) interaction divided by the error variance for this factor.27 WMFT=Wolf Motor Function Test.
15

16
Table S5. MAL Arm Use and WMFT Performance Rate Scores for Study 2 Participants Change from Pre to Pre Post 1-month 6-month 1-year Post 1-month 6-month 1-year MAL Arm Use scale (range=0-5 points) Mean 95% Confidence Interval Effect Sizea
1.3 (0.6-1.9)
2.0 (0.9-3.1)
2.5 (1.5-3.6)
3.0 (1.7-4.2)
2.1 (1.0-3.1)
0.7* (0.2-1.3)
0.9
1.3** (0.7-1.8)
1.7
1.5**
(0.8-2.1) 1.8
0.8** (0.3-1.3)
1.5 N 10 10 8 8 WMFT Performance Rate (repetitions/minute) Mean 95% Confidence Interval Effect Sizea
27.4 (12.8-42.0)
35.9 (17.8-53.9)
na na na 8.5** (3.1-13.9)
1.1
na na na
N 10 Note. *P<0.05, **P<0.01. Study 2 participants received repetitive task practice without a TP during treatment and the MAL component of the TP weekly for 4-weeks afterwards. Their pre-treatment MAL and WMFT scores were not significantly different from the corresponding scores for all Study 1 participants (Ps≥0.67). WMFT data were not collected at the 1- and 6-month follow-ups. As in the case of Study 1, one-year follow-up data are not reported for the WMFT because about half of the participants did not return to the laboratory on this testing occasion. Only 20% of the data were missing for the MAL because this instrument can be administered over the telephone if necessary. aCohen’s d' is a repeated measures index of effect size (large d' =.57); it is the mean pre- to post-treatment change divided by the SD of the change.27 MAL=Motor Activity Log, WMFT=Wolf Motor Function Test, na=not available. TP=transfer package

Supplemental References
1. Taub E, Uswatte G, King DK, Morris D, Crago J, Chatterjee A. A placebo-controlled trial of Constraint-Induced Movement therapy for upper extremity after stroke. Stroke. 2006;37:1045-1049
2. Winstein CJ, Miller JP, Blanton S, Taub E, Uswatte G, Morris D, et al. Methods for a multisite randomized trial to investigate the effect of Constraint-Induced movement therapy in improving upper extremity function among adults recovering from a cerebrovascular stroke. Neurorehabil Neural Repair. 2003;17:137-152
3. Uswatte G, Taub E, Morris D, Light K, Thompson P. The Motor Activity Log-28: assessing daily use of the hemiparetic arm after stroke. Neurology. 2006;67:1189-1194
4. Zinn S. Patient adherence in rehabilitation. In: Bosworth H, Oddone E, Weinberger M, eds. Patient treatment adherence: Concepts, interventions, and measurement. Mahway, New Jersey: Lawrence Erlbaum Assoc; 2006.
5. Friedman RH. Automated telephone conversations to assess health behavior and deliver behavioral interventions. J Med Syst. 1998;22:95-102
6. Hallam J, Petosa R. A worksite intervention to enhance social cognitive theory constructs to promote exercise adherence. Am J Health Promot. 1998;13:4-7
7. Martin JE, Dubbert PM, Katell AD, Thompson JK, Raczynski JR, Lake M, et al. Behavioral control of exercise in sedentary adults: studies 1 through 6. J Consult Clin Psychol. 1984;52:795-811.
8. Noland MP. The effects of self-monitoring and reinforcement on exercise adherence. Res Q Exerc Sport. 1989;60:216-224
9. Oldridge NB, Jones NL. Improving patient compliance in cardiac rehabilitation: effects of written agreement and self-monitoring. J Cardiopulm Rehabil. 1983;3:257-262
10. Owen N, Lee C, Naccarella L, Haag K. Exercise by mail: a mediated behavior-change program for aerobic exercise. J Sports Psychol. 1987;9:346-357
11. Rejeski WJ, Brawley LR, Ambrosius WT. Older adults with chronic disease: benefits of group-mediated counseling in promotion of physical active lifestyles. Health Psychol. 2003;22:414-423
12. Stoffelmayr BE, Mavis BE, Stachnik T, Robison J, Rogers M, VanHuss W, et al. A program model to enhance adherence to work-site-based fitness programs. J Occup Med. 1992;34:156-161
13. Rhode G, Morgan DP, Young KR. Generalization and maintenance of treatment gains of behaviorally handicapped students from resource rooms to regular classrooms using self-evaluation procedures. J Appl Behav Anal. 1983;16:171-182
14. Higgins ST, Budney AJ, Bickel WK. Outpatient behavioral treatment for cocaine dependence: one-year outcome. In: Marlatt GA, VandenBos GR, eds. Addictive behaviors: readings on etiology, prevention, and treatment. Washington, DC: American Psychological Association; 1997:629-645.
15. Eyberg SM, Johnson SM. Multiple assessment of behavior modification with families: effects of contingency contracting and order of treated problems. J Consult Clin Psychol. 1974;42:594-606
16. Marcus AC, Heimendinger J, Wolfe P, Fairclough D, Rimer BK, Morra M, et al. A randomized trial of a brief intervention to increase fruit and vegetable intake: a replication study among callers to the CIS. Prev Med. 2001;33:204-216
17

18
17. Sacco WP, Morrison AD, Malone JI. A brief, regular, proactive telephone "coaching" intervention for diabetes: rationale, description, and preliminary results. J Diabetes Complications. 2004;18:113-118
18. Oden MP. The relationship between awareness of cardiac risk factors, physical activity level, telephone intervention, and health behavior change in African-American women. Diss Abstr Int A Hum Soc Sci. 2005;66:101
19. Saywell RM, Champion VL, Skinner CS, Menon U, Daggy J. A cost-effectiveness comparison of three tailored interventions to increase mammography screening. J Womens Health. 2004;13:909-918
20. Bosworth HB, Olsen MK, Gentry P. Nurse administered telephone intervention or blood pressure control: a patient-tailored multifactorial intervention. Patient Educ Couns. 2005;57:5-14
21. The Writing Group for the Activity Counseling Trial Research Group. Effects of physical activity counseling in primary care: the Activity Counseling Trial: a randomized controlled trial. JAMA. 2001;286:677-687
22. Castro CM, King AC, Brassington GS. Telephone versus mail interventions for maintenance of physical activity in older adults. Health Psychol. 2001;20:438-444
23. Kind AC, Pruitt LA, Phillips W, Oka R, Rodenburg A, Haskell WL. Comparative effects of two physical activity programs on measured and perceived physical functioning and other health-related quality of life outcomes in older adults. J Gerontol A Biol Sci Med Sci. 2000;55:M74-M83
24. Glasgow RE, Toobert DJ, Barrera M. Assessment of problem-solving: a key to successful diabetes self-management. J Behav Med. 2004;27:477-490
25. DeVellis BM, Blalock SJ, Hahn PM. Evaluation of a problem-solving intervention for patients with arthritis. Patient Educ Couns. 1988;11:29-42
26. Wade SL, Michaud L, Brown TM. Putting the pieces together: preliminary efficacy of a family problem-solving intervention for children with traumatic brain injury. J Head Trauma Rehabil. 2006;21:57-67
27. Cohen J. Statistical Power Analysis for the Behavioral Sciences. Hillsdale NJ: Lawrence Erlbaum; 1988.