metabolic syndrome and health disparities: addressing unmet needs chief, division of cardiovascular...
TRANSCRIPT
Metabolic Syndrome and Health Disparities:
Addressing Unmet Needs
Metabolic Syndrome and Health Disparities:
Addressing Unmet Needs
Chief, Division of Cardiovascular Medicine
Professor of Clinical MedicineState University of New YorkDownstate Medical Center
Brooklyn, New York
March 30, 2007
Chief, Division of Cardiovascular Medicine
Professor of Clinical MedicineState University of New YorkDownstate Medical Center
Brooklyn, New York
March 30, 2007
Luther T. Clark, MDLuther T. Clark, MD
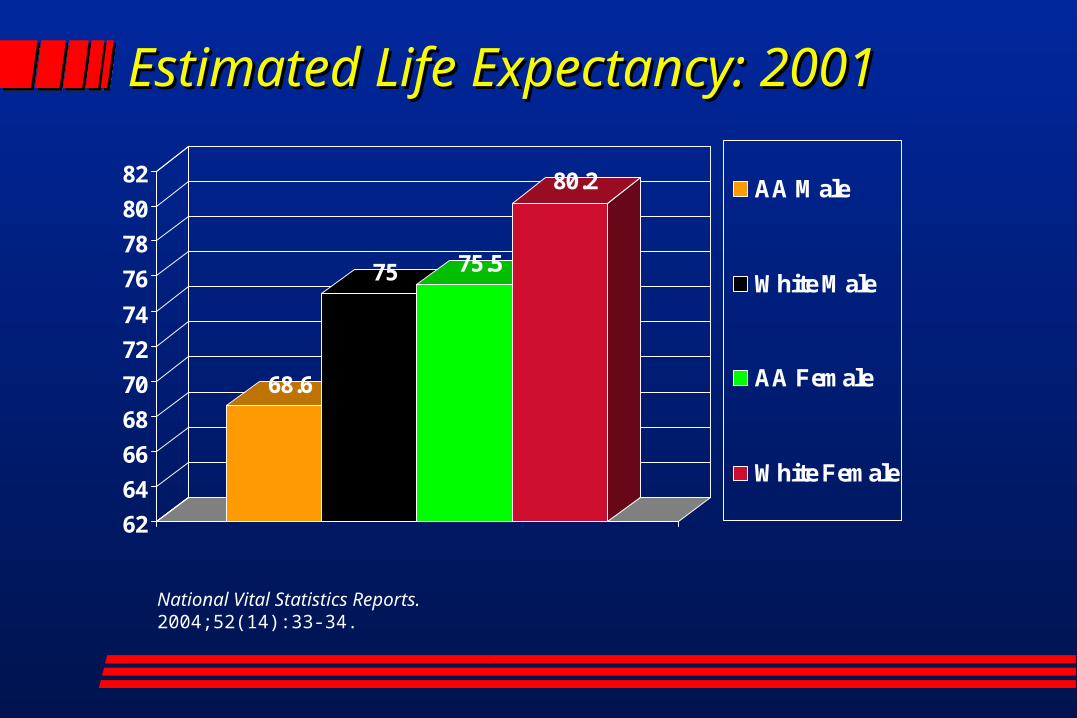
Estimated Life Expectancy: Estimated Life Expectancy: 20012001
68.6
75 75.5
80.2
62
64
66
68
70
72
74
76
78
80
82AA Male
White Male
AA Female
White Female
National Vital Statistics Reports. 2004;52(14):33-34.
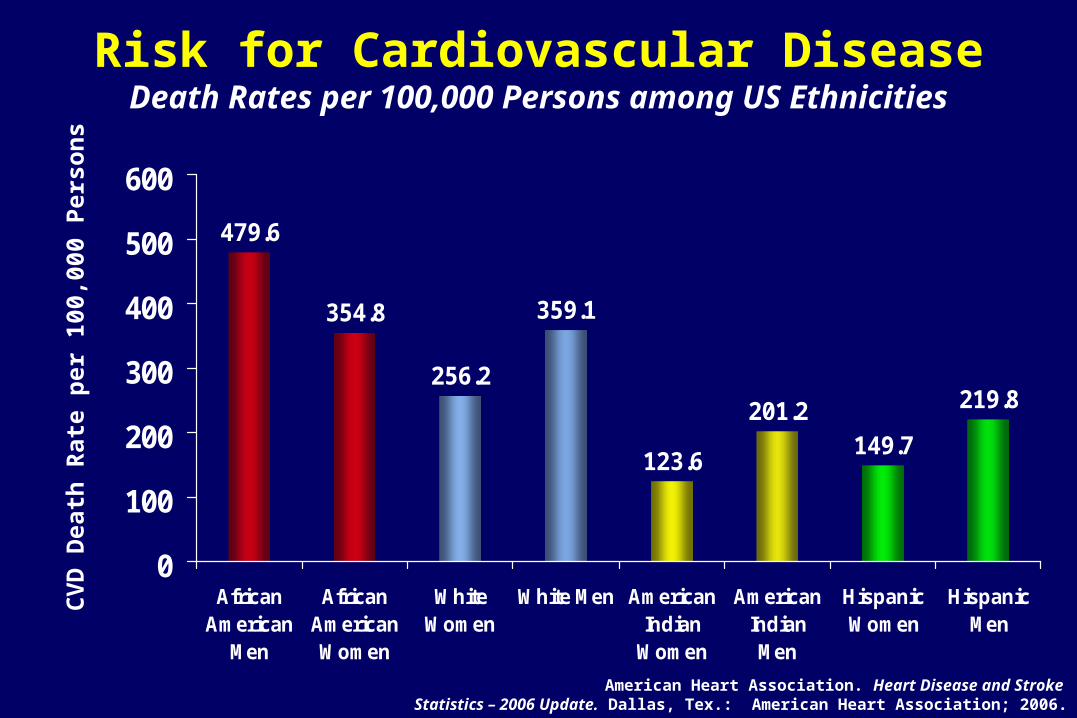
Risk for Cardiovascular DiseaseDeath Rates per 100,000 Persons among US Ethnicities
479.6
256.2
359.1
123.6
201.2149.7
219.8
354.8
0
100
200
300
400
500
600
AfricanAmerican
Men
AfricanAmericanWomen
WhiteWomen
White Men AmericanIndian
Women
AmericanIndianMen
HispanicWomen
HispanicMen
CV
D D
eath
Rat
e p
er 1
00,0
00 P
erso
ns
American Heart Association. Heart Disease and Stroke Statistics – 2006 Update. Dallas, Tex.: American Heart Association; 2006.
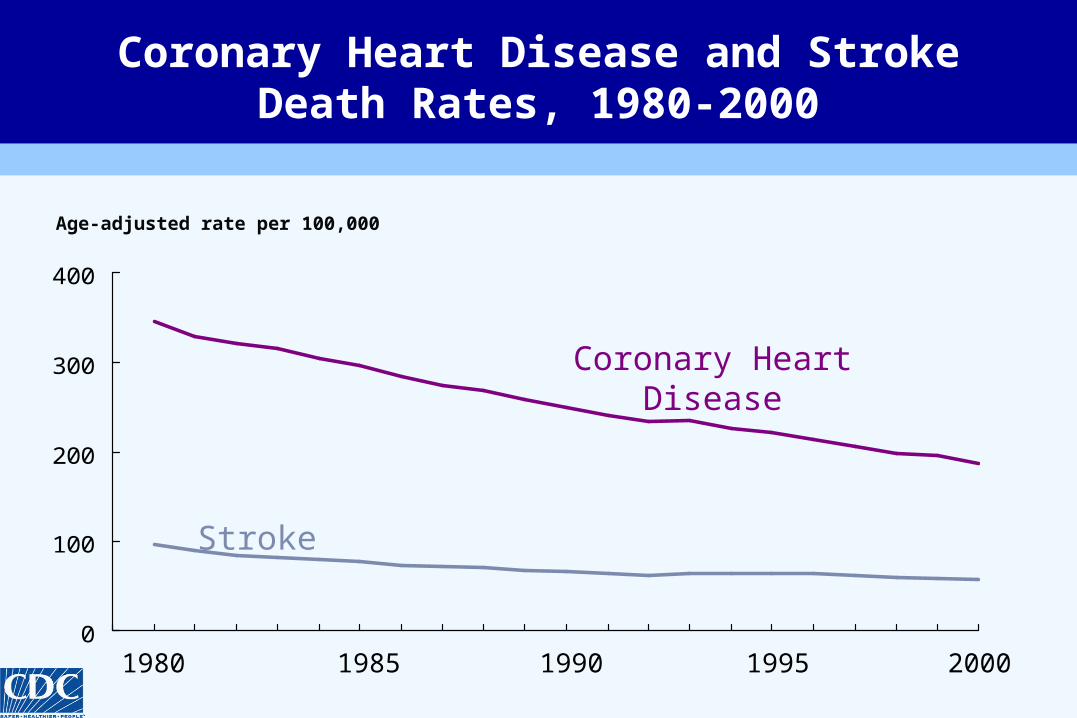
0
100
200
300
400
1980 19901985 20001995
Stroke
Coronary Heart Disease
Coronary Heart Disease and Stroke Death Rates, 1980-2000
Age-adjusted rate per 100,000
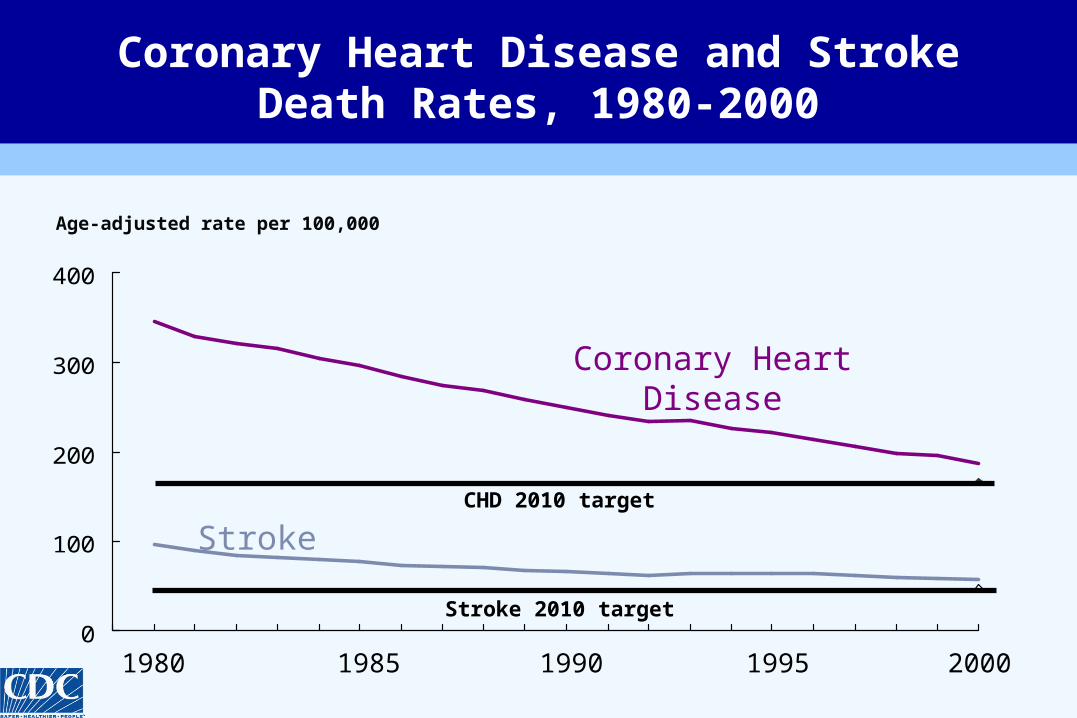
0
100
200
300
400
1980 19901985 20001995
Stroke
Coronary Heart Disease
CHD 2010 target
Stroke 2010 target
Coronary Heart Disease and Stroke Death Rates, 1980-2000
Age-adjusted rate per 100,000
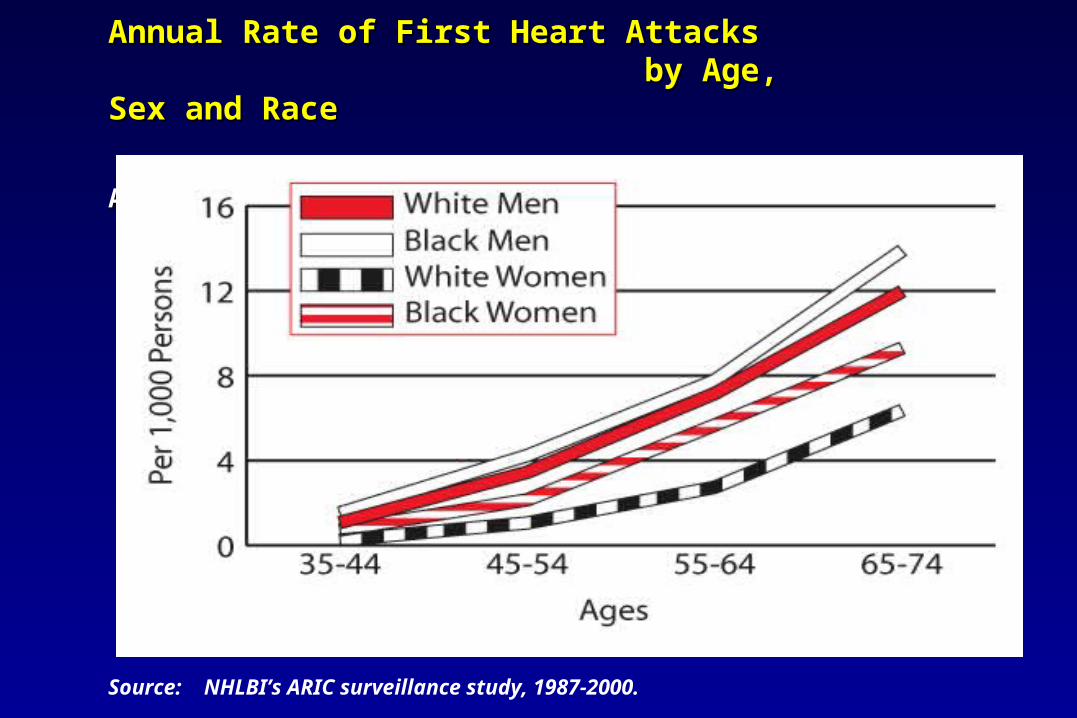
Annual Rate of First Heart Attacks Annual Rate of First Heart Attacks by Age, Sex and Race by Age, Sex and Race
ARIC: 1987-2000ARIC: 1987-2000
Source: NHLBI’s ARIC surveillance study, 1987-2000.
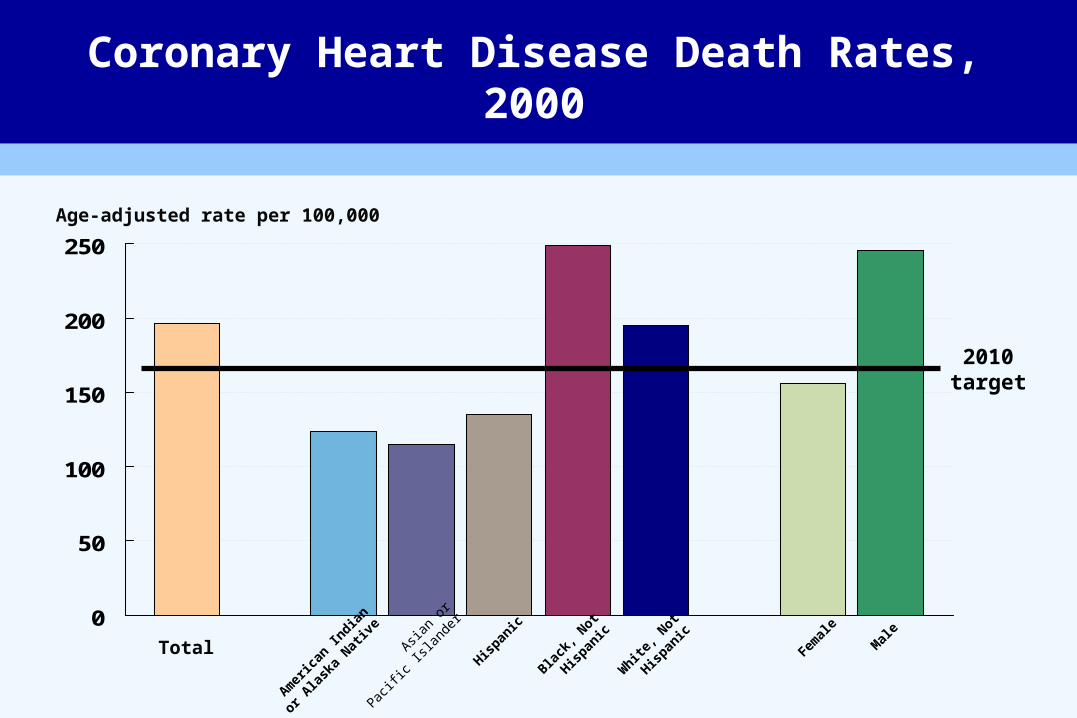
Coronary Heart Disease Death Rates, 2000
0
50
100
150
200
250
TotalBla
ck, N
ot
Hispan
ic
Hispan
ic
Asian
or
Pac
ific Is
lande
r
Amer
ican
India
n
or Ala
ska
Nativ
e
White
, Not
Hispan
ic Mal
e
Femal
e
2010target
Age-adjusted rate per 100,000

“Disparities in the health care delivered to racial and ethnic minorities are real and are associated with worse outcomes in many cases, which is unacceptable.”
-- Alan Nelson, retired physician, former president of the American Medical Association and chair of the committee that wrote the Institute of Medicine report, Unequal Treatment: Confronting Racial and Disparities in Health Care
IOM Report, 2002: Assessing the Quality of Minority Health Care
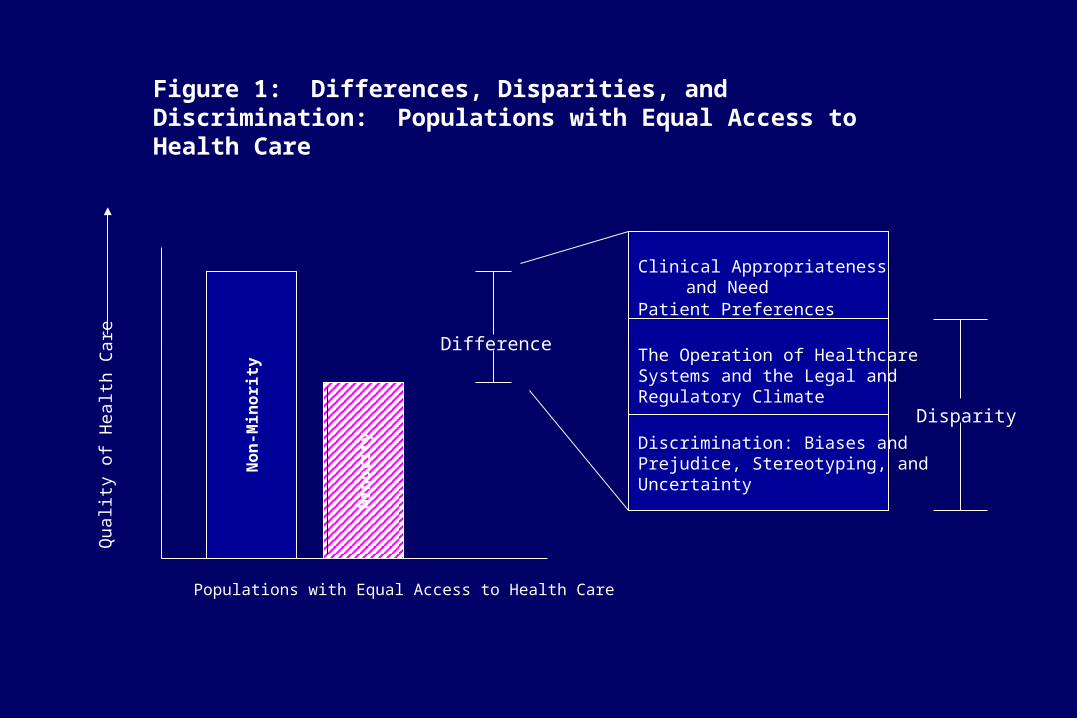
Non
-Min
orit
y
Min
orit
yDifference
Clinical Appropriateness and Need
Patient Preferences
The Operation of Healthcare Systems and the Legal and Regulatory Climate
Discrimination: Biases andPrejudice, Stereotyping, andUncertainty
Disparity
Qua
li ty
o f H
e al th
Car
eFigure 1: Differences, Disparities, and Discrimination: Populations with Equal Access to Health Care
Populations with Equal Access to Health Care

Cardiac Care: The Weight of the Evidence
“Of all forms of inequality in our society, injustice in health care is the most shocking
and the most inhumane.”
Martin Luther King, Jr.Second National Convention of the
Medical Committee for Human RightsChicago, March 25, 1966
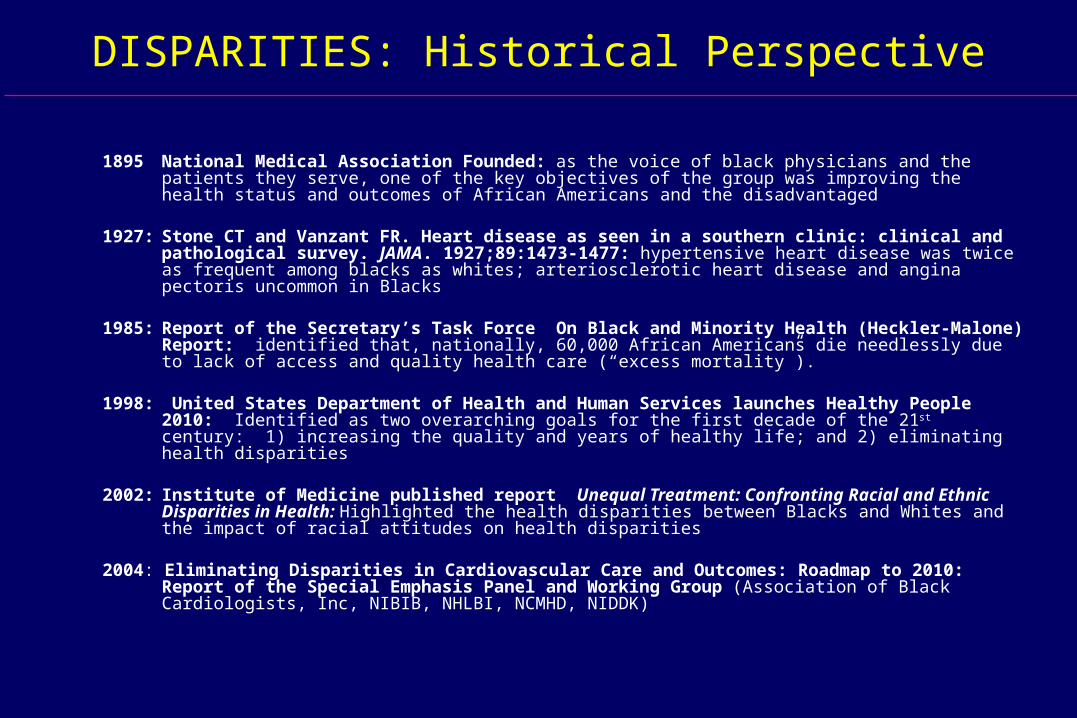
DISPARITIES: Historical Perspective
1895 National Medical Association Founded: as the voice of black physicians and the patients they serve, one of the key objectives of the group was improving the health status and outcomes of African Americans and the disadvantaged
1927: Stone CT and Vanzant FR. Heart disease as seen in a southern clinic: clinical and pathological survey. JAMA. 1927;89:1473-1477: hypertensive heart disease was twice as frequent among blacks as whites; arteriosclerotic heart disease and angina pectoris uncommon in Blacks
1985: Report of the Secretary’s Task Force On Black and Minority Health (Heckler-Malone) Report: identified that, nationally, 60,000 African Americans die needlessly due to lack of access and quality health care (“excess mortality”).
1998: United States Department of Health and Human Services launches Healthy People 2010: Identified as two overarching goals for the first decade of the 21st century: 1) increasing the quality and years of healthy life; and 2) eliminating health disparities
2002: Institute of Medicine published report Unequal Treatment: Confronting Racial and Ethnic Disparities in Health: Highlighted the health disparities between Blacks and Whites and the impact of racial attitudes on health disparities
2004: Eliminating Disparities in Cardiovascular Care and Outcomes: Roadmap to 2010: Report of the Special Emphasis Panel and Working Group (Association of Black Cardiologists, Inc, NIBIB, NHLBI, NCMHD, NIDDK)

Although there have been tremendous scientific achievements in terms of improvement in overall
health status for the general population, significant health inequities persist among African Americans
and other minorities.
A Continuing National Paradox
Although there have been tremendous scientific achievements in terms of improvement in overall
health status for the general population, significant health inequities persist among African Americans
and other minorities.
A Continuing National Paradox
1985 Secretary of Health and Human Services Report on Black and Minority Health
Excess CVD Morbidity and Mortality among African Americans
Excess burden of risk factors Patient delay in seeking medical care Under-treatment of high risk individuals
Under-utilization of primary and secondary risk reduction strategies Limited access to modern/invasive/high tech services: thrombolytics,
cath, percutaneous coronary interventions (PCI), bypass surgery Under-treatment of chronic cardiac conditions (ie heart failure)
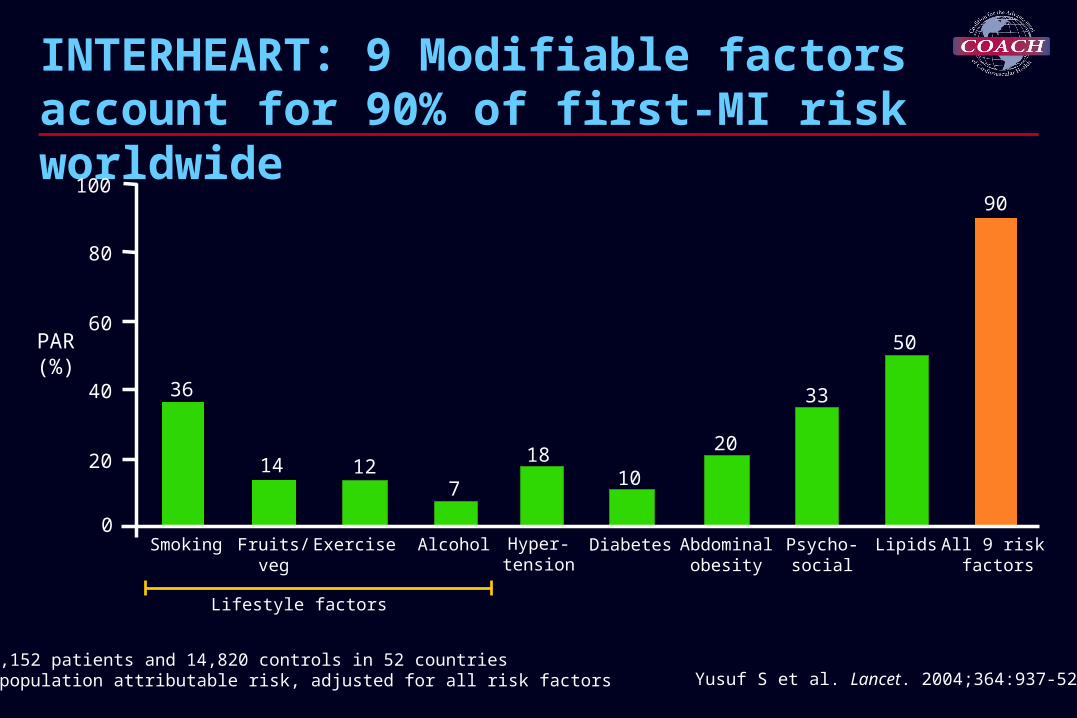
INTERHEART: 9 Modifiable factors account for 90% of first-MI risk worldwide
Yusuf S et al. Lancet. 2004;364:937-52.N = 15,152 patients and 14,820 controls in 52 countriesPAR = population attributable risk, adjusted for all risk factors
36
127 10
20
33
0
20
40
60
80
100
Smoking Fruits/veg
Exercise Alcohol Psycho-social
Lipids All 9 risk factors
PAR(%)
14 18
50
90
Diabetes Abdominalobesity
Hyper-tension
Lifestyle factors
Risk Factors More Prevalent inAfrican-Americans than Whites
• Associated with Increased Risk – Hypertension– Type 2 diabetes mellitus– Obesity– Cigarette smoking– Physical inactivity– Left ventricular hypertrophy
• Associated With Decreased Risk– Higher high-density lipoprotein cholesterol
• Association with CHD risk unclear– Higher Lp(a)
More Prevalent in Non-Hispanic More Prevalent in Non-Hispanic Blacks than NHWBlacks than NHW
– Hypertension– Type 2 diabetes mellitus– Obesity– Metabolic Syndrome
(females)– Cigarette smoking– Physical inactivity
– Type 2 diabetes mellitus– Obesity– Lower HDL-Cholesterol
(females)– Elevated Triglycerides– Metabolic Syndrome– Physical Inactivity
More Prevalent in Hispanics More Prevalent in Hispanics than NHWthan NHW
CHD risk factors in Hispanics and African Americans CHD risk factors in Hispanics and African Americans compared to Non-Hispanic Whitescompared to Non-Hispanic Whites
Clark LT. Med Clin NA. 2005;89 (5):977-1001.Liao, et al J Am Coll Cardiol 30: 1200–1205, 1997
Ford, et al. JAMA. 2002;287:356-359.
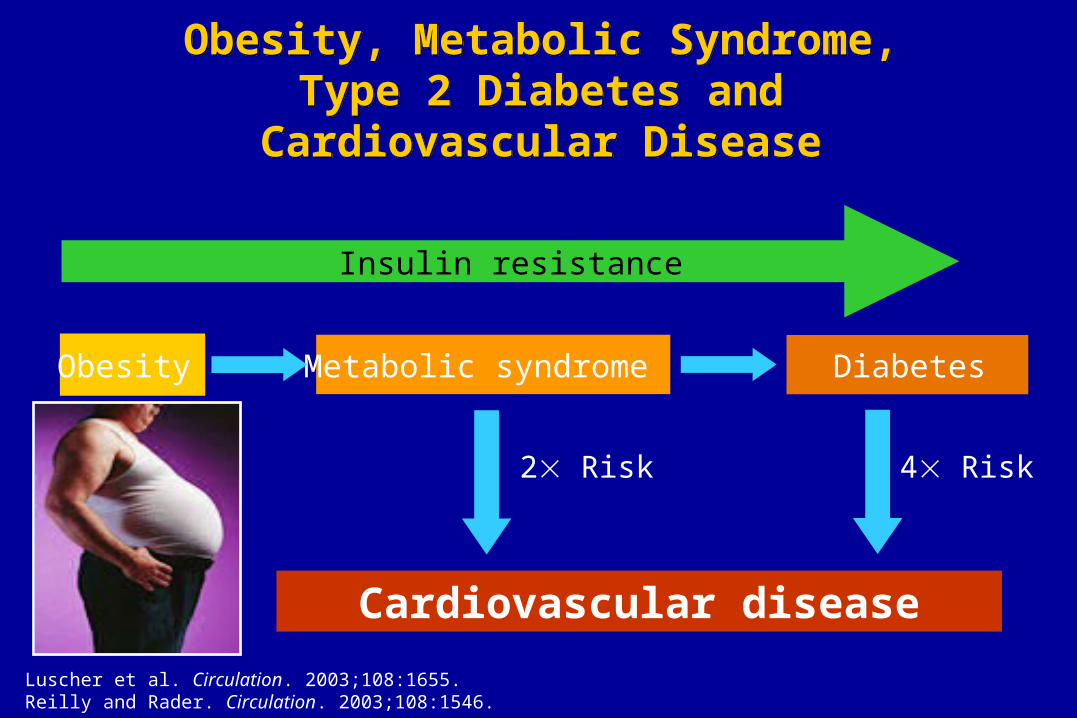
Obesity, Metabolic Syndrome, Type 2 Diabetes and
Cardiovascular Disease
Obesity, Metabolic Syndrome, Type 2 Diabetes and
Cardiovascular Disease
Obesity
Cardiovascular disease
Metabolic syndrome
Insulin resistance
2 Risk 4 Risk
Luscher et al. Circulation. 2003;108:1655.Reilly and Rader. Circulation. 2003;108:1546.
Diabetes
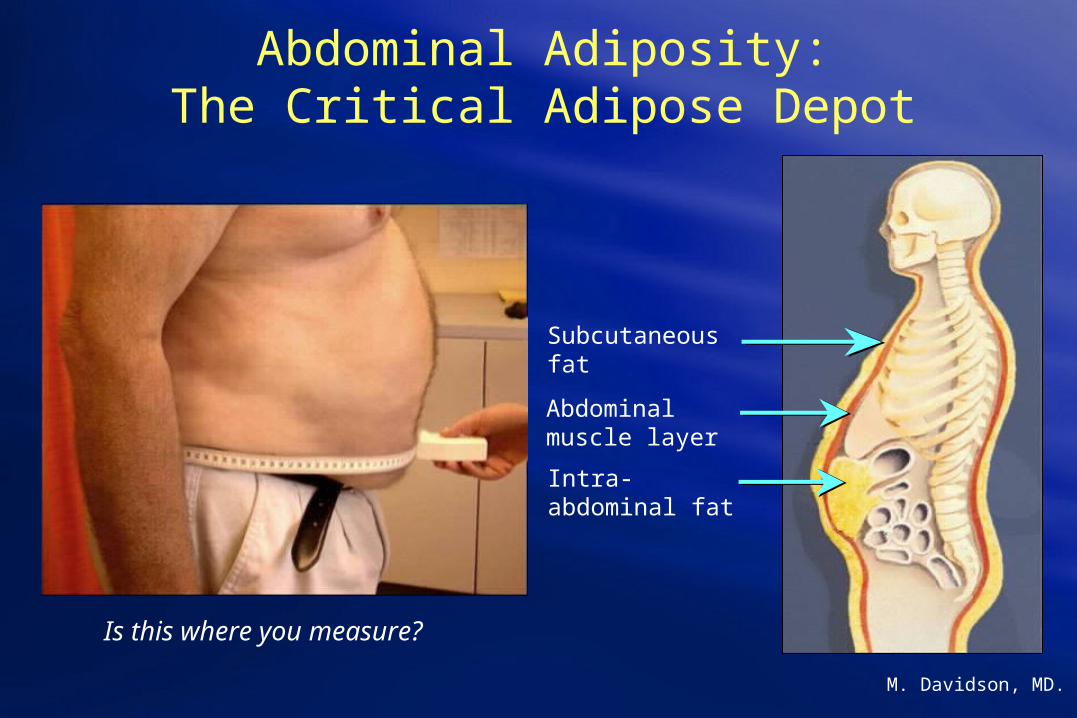
Subcutaneous fat
Abdominal muscle layer
Intra-abdominal fat
Abdominal Adiposity:The Critical Adipose Depot
M. Davidson, MD.
Is this where you measure?
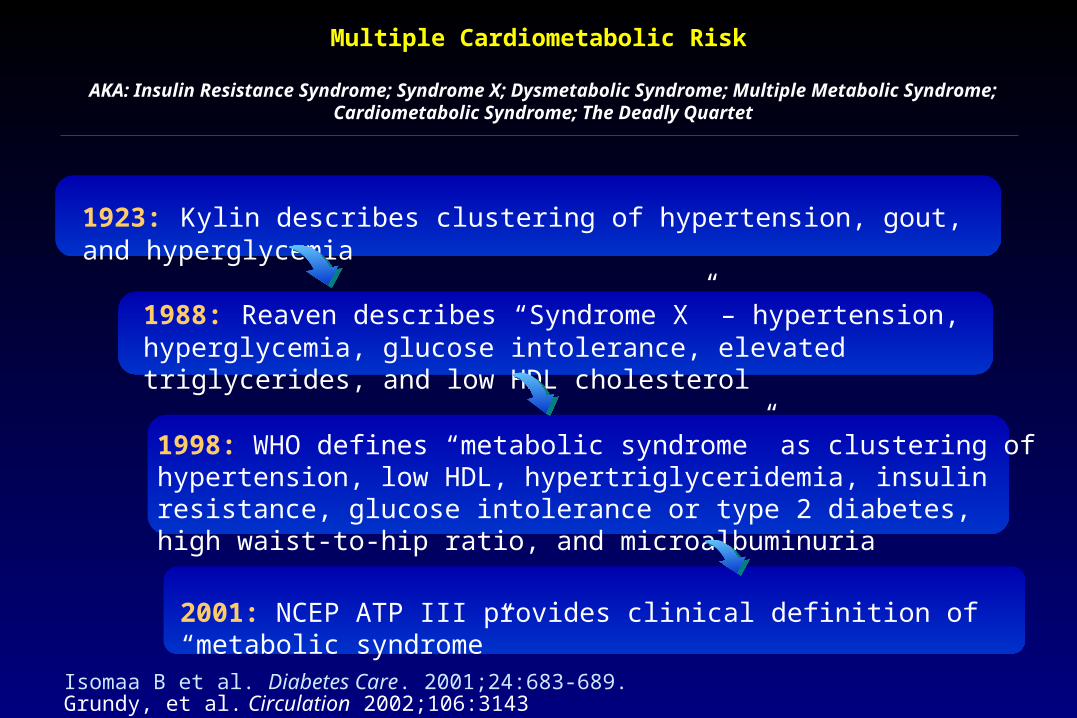
Multiple Cardiometabolic Risk
Isomaa B et al. Diabetes Care. 2001;24:683-689.Grundy, et al. Circulation 2002;106:3143
AKA: Insulin Resistance Syndrome; Syndrome X; Dysmetabolic Syndrome; Multiple Metabolic Syndrome; Cardiometabolic Syndrome; The Deadly Quartet
1923: Kylin describes clustering of hypertension, gout, and hyperglycemia
1988: Reaven describes “Syndrome X” – hypertension, hyperglycemia, glucose intolerance, elevated triglycerides, and low HDL cholesterol
1998: WHO defines “metabolic syndrome” as clustering of hypertension, low HDL, hypertriglyceridemia, insulin resistance, glucose intolerance or type 2 diabetes, high waist-to-hip ratio, and microalbuminuria
2001: NCEP ATP III provides clinical definition of “metabolic syndrome”

Clinical Identification of the Metabolic Syndrome*Clinical Identification of the Metabolic Syndrome*
Risk Factor Defining Level • Abdominal obesity (waist circumference) Men > 102 cm (>40 in) Women > 88 cm (>35 in)• Triglycerides 150 mg/dl• HDL Cholesterol Men < 40 mg/dl Women < 50 mg/dl• Blood pressure 130/ 85 mm Hg• Fasting glucose 100 mg/dl
Circulation. 2002;106:3143.Circulation. 2005;112: 2735-2752.
* Diagnosis requires three or more criteria present
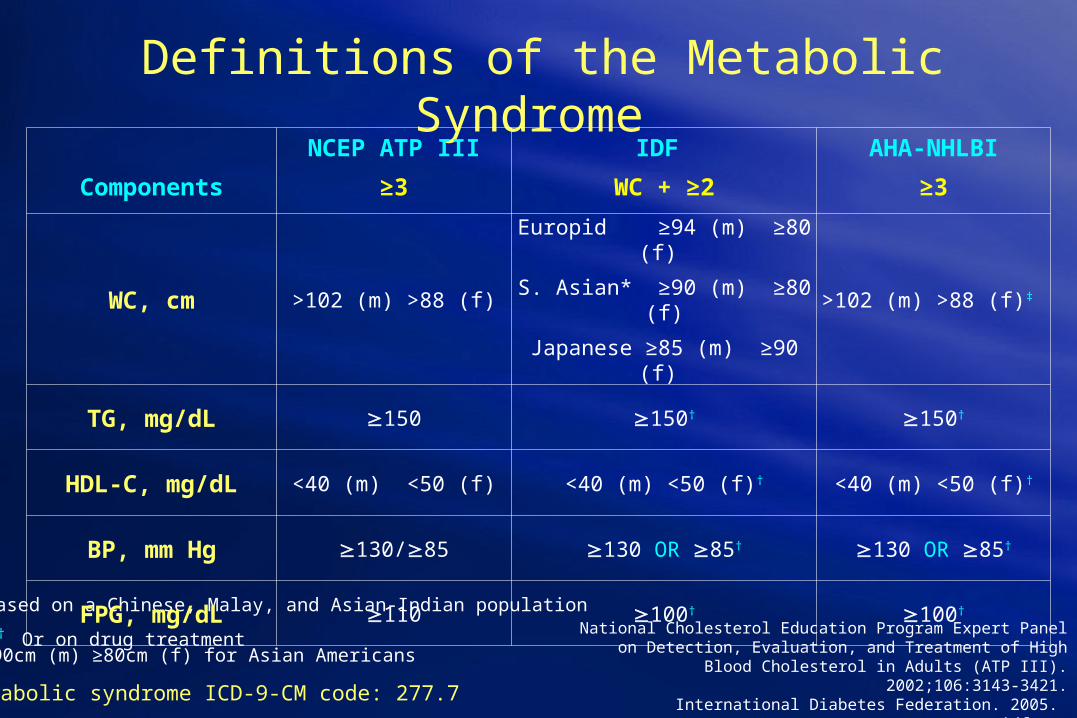
Definitions of the Metabolic Syndrome
National Cholesterol Education Program Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (ATP
III). 2002;106:3143-3421.International Diabetes Federation. 2005. www.idf.orgGrundy SM, et al. Circulation. 2005;112:2735-2752.
* Based on a Chinese, Malay, and Asian-Indian population
† Or on drug treatment
Metabolic syndrome ICD-9-CM code: 277.7
Components
NCEP ATP III
≥3
IDF
WC + ≥2
AHA-NHLBI
≥3
WC, cm >102 (m) >88 (f)
Europid ≥94 (m) ≥80 (f)
S. Asian* ≥90 (m) ≥80 (f)
Japanese ≥85 (m) ≥90 (f)
>102 (m) >88 (f)‡
TG, mg/dL 150 150† 150†
HDL-C, mg/dL <40 (m) <50 (f) <40 (m) <50 (f)† <40 (m) <50 (f)†
BP, mm Hg 130/85 130 OR 85† 130 OR 85†
FPG, mg/dL 110 100† 100†
‡ ≥90cm (m) ≥80cm (f) for Asian Americans
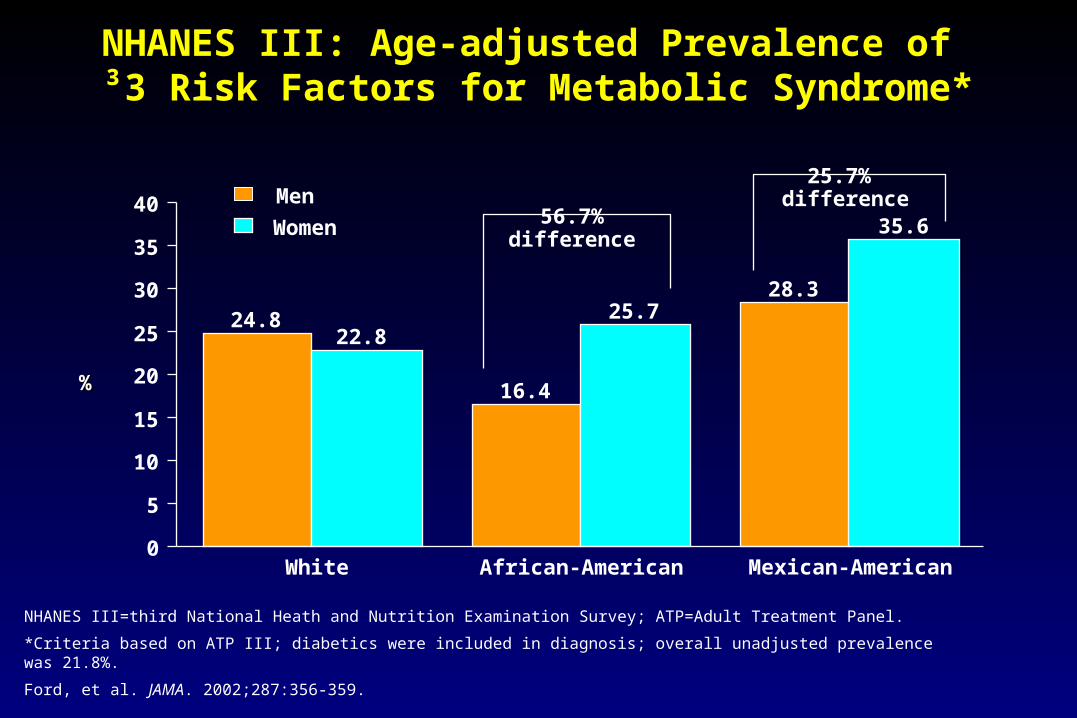
NHANES III: Age-adjusted Prevalence of ³3 Risk Factors for Metabolic Syndrome*
NHANES III=third National Heath and Nutrition Examination Survey; ATP=Adult Treatment Panel.
*Criteria based on ATP III; diabetics were included in diagnosis; overall unadjusted prevalence was 21.8%.
Ford, et al. JAMA. 2002;287:356-359.
%%
24.8
16.4
28.3
22.825.7
35.6
0
5
10
15
20
25
30
35
40
White African-American Mexican-American
Men
Women
25.7% difference
56.7%difference
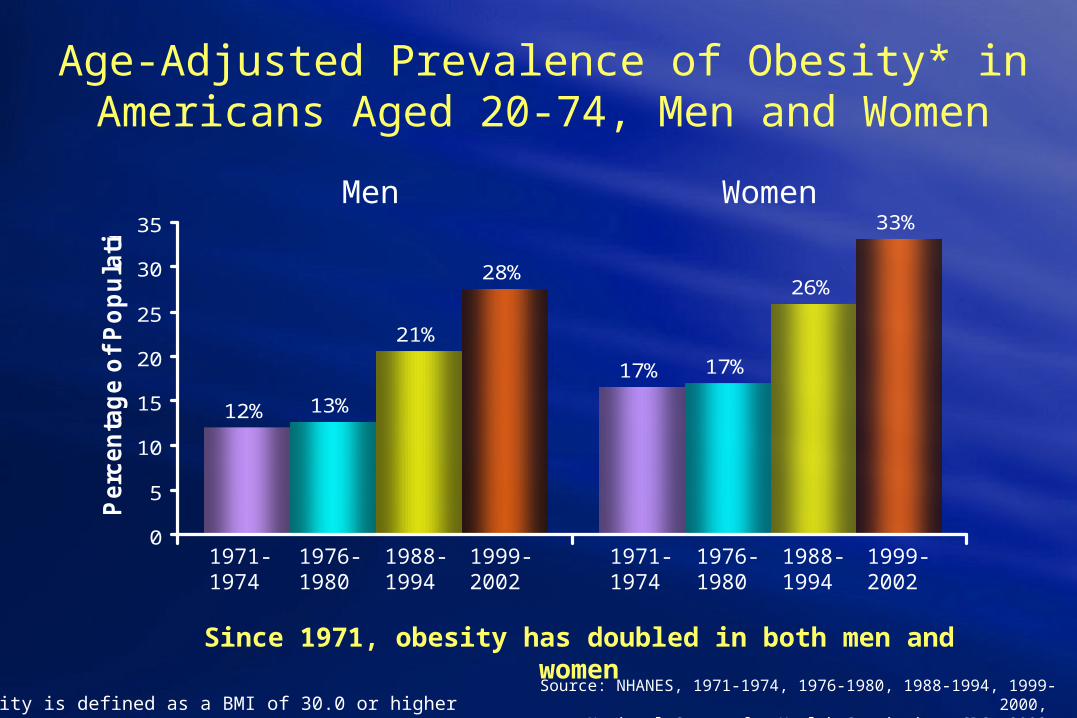
Source: NHANES, 1971-1974, 1976-1980, 1988-1994, 1999-2000, National Center for Health Statistics, CDC, 2002.
Age-Adjusted Prevalence of Obesity* in Americans Aged 20-74, Men and Women
12%
17%
13%
17%
21%
26%28%
33%
0
5
10
15
20
25
30
35
Perc
en
tag
e o
f P
op
ula
tio
n
1971-1974
1976-1980
1988-1994
1999-2002
1971-1974
1976-1980
1988-1994
1999-2002
Since 1971, obesity has doubled in both men and women
*Obesity is defined as a BMI of 30.0 or higher
Men Women
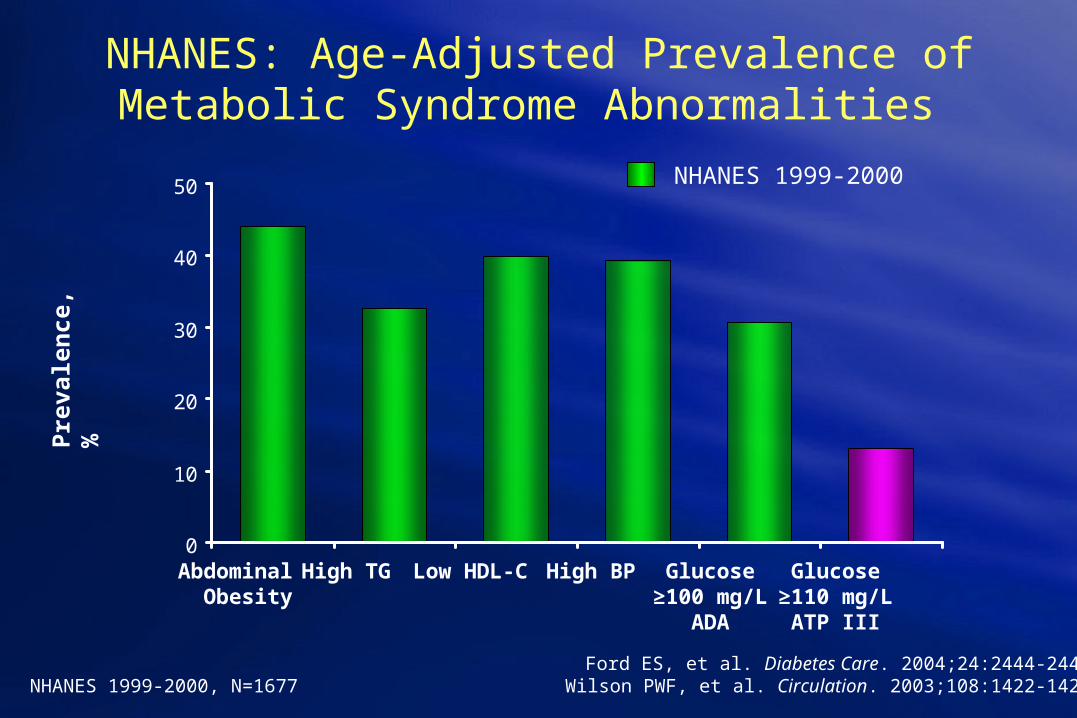
NHANES: Age-Adjusted Prevalence of Metabolic Syndrome Abnormalities
NHANES 1999-2000, N=1677Ford ES, et al. Diabetes Care. 2004;24:2444-2449.
Wilson PWF, et al. Circulation. 2003;108:1422-1425.
0
10
20
30
40
50
Abdominal High TG Low HDL-C High BP Glucose Glucose Obesity ≥100 mg/L ≥110 mg/L
ADA ATP III
Pre
vale
nce
, %
NHANES 1999-2000
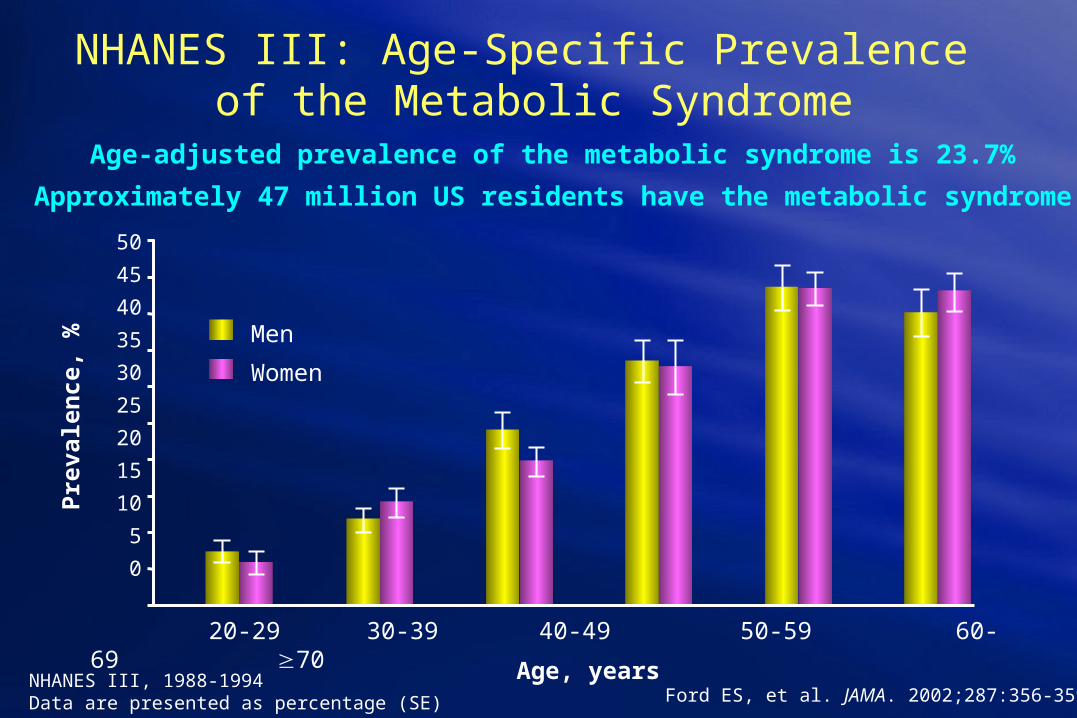
NHANES III: Age-Specific Prevalence of the Metabolic Syndrome
NHANES III, 1988-1994Data are presented as percentage (SE)
20-29 30-39 40-49 50-59 60-69 70
Age, years
50
45
40
35
30
25
20
15
10
5
0
Pre
vale
nce
, %
Men
Women
Ford ES, et al. JAMA. 2002;287:356-359.
Age-adjusted prevalence of the metabolic syndrome is 23.7%
Approximately 47 million US residents have the metabolic syndrome
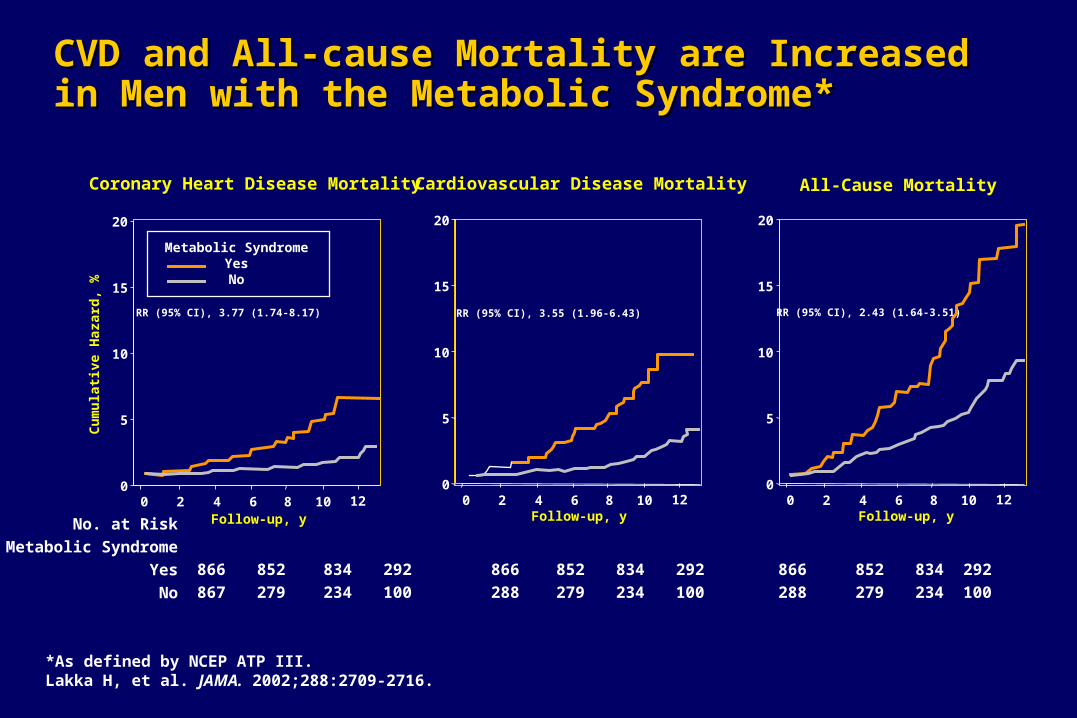
CVD and All-cause Mortality are Increased in Men CVD and All-cause Mortality are Increased in Men with the Metabolic Syndrome*with the Metabolic Syndrome*
Coronary Heart Disease Mortality Cardiovascular Disease Mortality All-Cause Mortality
RR (95% CI), 3.77 (1.74-8.17) RR (95% CI), 3.55 (1.96-6.43) RR (95% CI), 2.43 (1.64-3.51)
Follow-up, y Follow-up, y Follow-up, y
Cu
mu
lati
ve H
azar
d, %
No. at Risk
Metabolic Syndrome
Yes
No
866 852 834 292 866 852 834 292 866 852 834 292
867 279 234 100 288 279 234 100 288 279 234 100
0
5
10
15
20
0 2 4 6 8 10 120
5
10
15
20
0 2 4 6 8 10 120
5
10
15
20
0 2 4 6 8 10 12
Metabolic SyndromeYesNo
*As defined by NCEP ATP III.Lakka H, et al. JAMA. 2002;288:2709-2716.
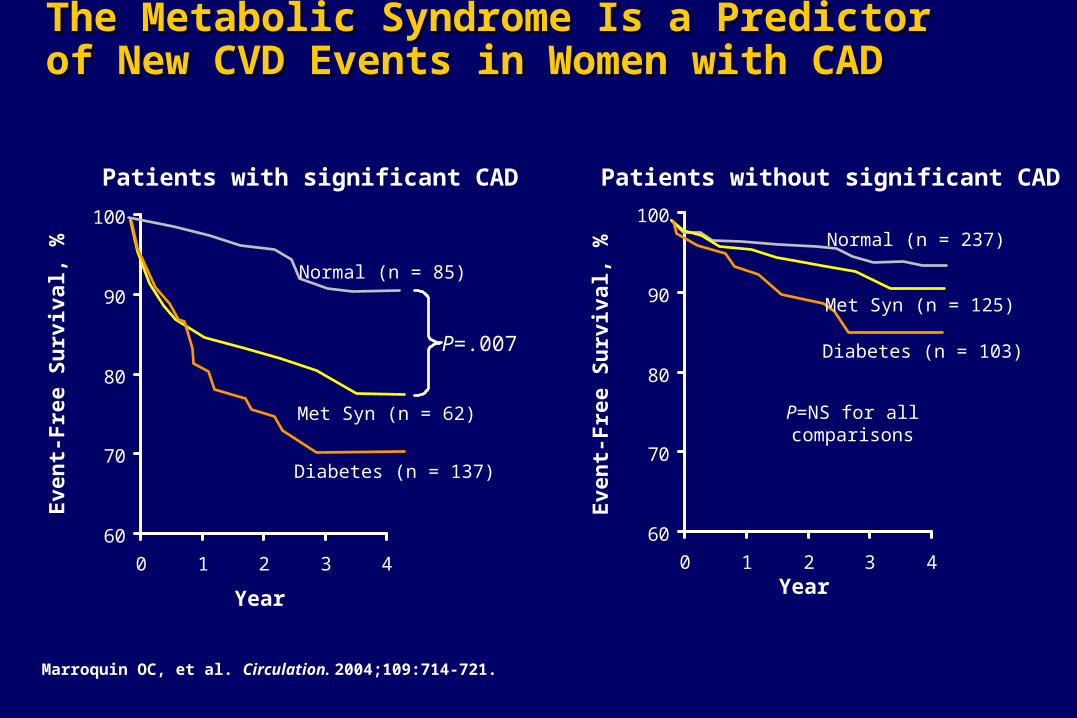
The Metabolic Syndrome Is a Predictor of New The Metabolic Syndrome Is a Predictor of New CVD Events in Women with CADCVD Events in Women with CAD
Marroquin OC, et al. Circulation. 2004;109:714-721.
Patients with significant CAD
60
70
80
90
100
0 1 2 3 4
P=.007
Normal (n = 85)
Met Syn (n = 62)
Diabetes (n = 137)
Year
Eve
nt-
Fre
e S
urv
ival
, %
60
70
80
90
100
0 1 2 3 4
Patients without significant CAD
Normal (n = 237)
Met Syn (n = 125)
Diabetes (n = 103)
Year
P=NS for allcomparisons
Eve
nt-
Fre
e S
urv
ival
, %
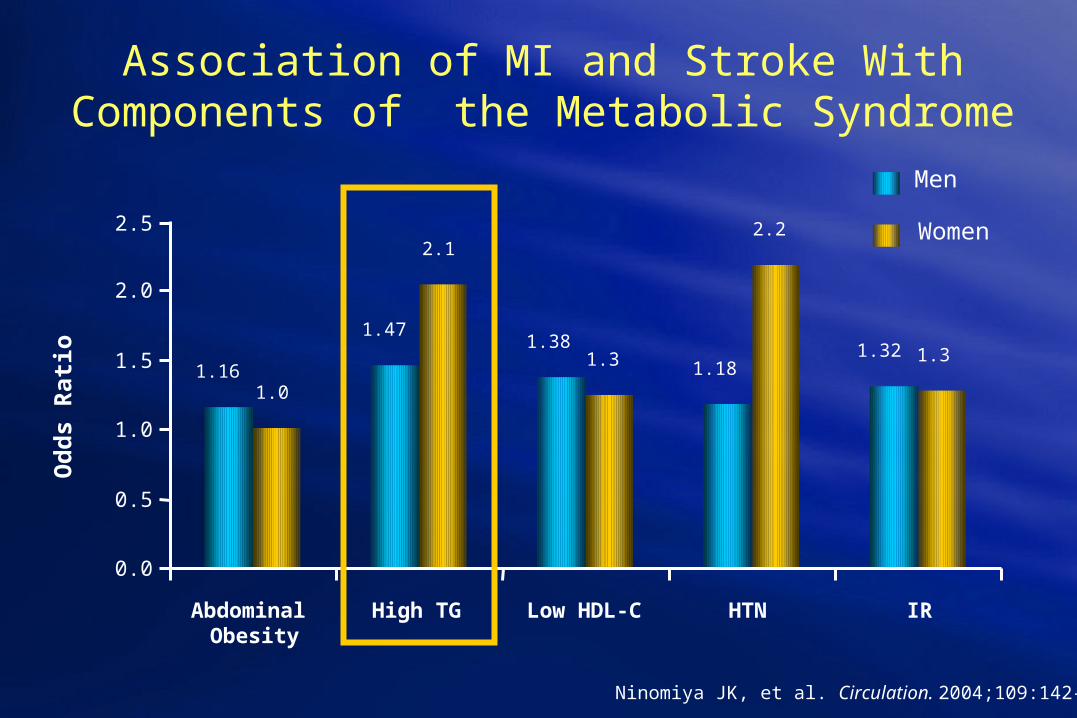
Association of MI and Stroke With Components of the Metabolic Syndrome
Ninomiya JK, et al. Circulation. 2004;109:142-46.
1.16
1.471.38
1.181.32
1.0
2.1
1.3
2.2
1.3
0.0
0.5
1.0
1.5
2.0
2.5
Abdominal Obesity
High TG Low HDL-C HTN IR
Od
ds
Rat
io
Men
Women
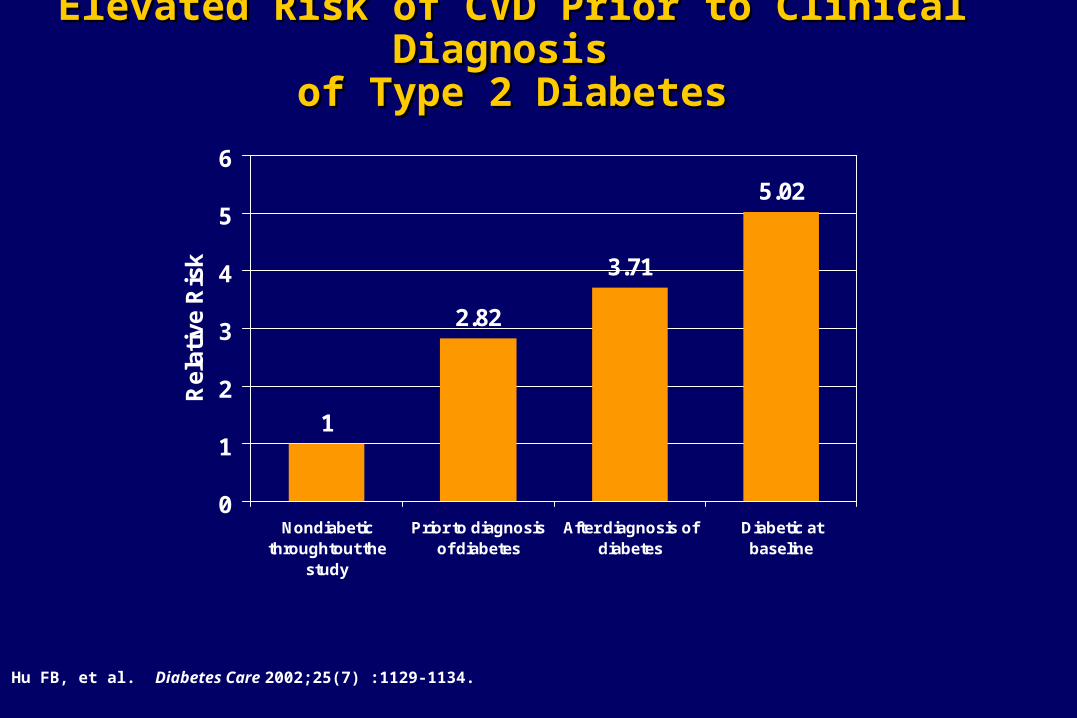
Elevated Risk of CVD Prior to Clinical Diagnosis Elevated Risk of CVD Prior to Clinical Diagnosis of Type 2 Diabetesof Type 2 Diabetes
Hu FB, et al. Diabetes Care 2002;25(7) :1129-1134.
1
2.82
3.71
5.02
0
1
2
3
4
5
6
Nondiabeticthroughtout the
study
Prior to diagnosisof diabetes
After diagnosis ofdiabetes
Diabetic atbaseline
Rel
ativ
e R
isk

4329
194
159144
104
264
208
0
50
100
150
200
250
300
Previous MI and Diabetes are Strong Predictors of Previous MI and Diabetes are Strong Predictors of Mortality (MRFIT; N = 9434)Mortality (MRFIT; N = 9434)
MRFIT, Multiple Risk Factor Intervention Trial*Median 25 years of follow-up, age-adjusted rate per 10,000 person-years
Mo
rtal
ity
Rat
e*
Vaccaro O, et al. Arch Intern Med. 2004;164:1438:1443.
All CVD Death CHD Death
No DM DM
No MI
MI
No DM DM
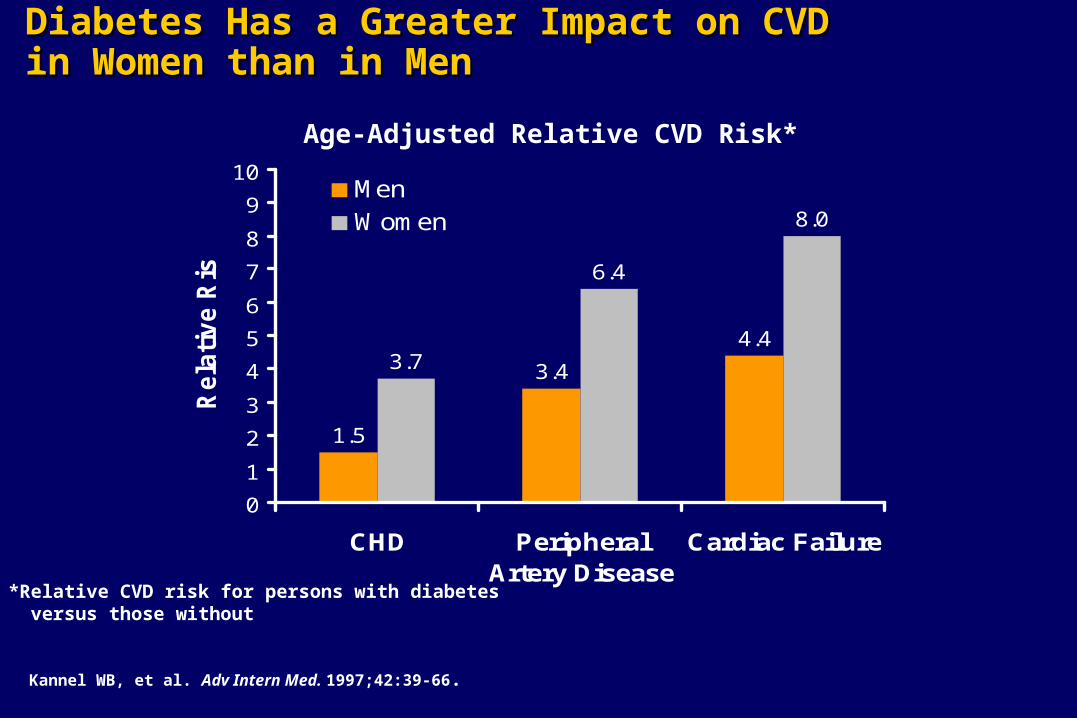
Diabetes Has a Greater Impact on CVD Diabetes Has a Greater Impact on CVD in Women than in Menin Women than in Men
Kannel WB, et al. Adv Intern Med. 1997;42:39-66.
1.5
3.4
4.43.7
6.4
8.0
0
1
2
3
4
5
6
7
8
9
10
CHD PeripheralArtery Disease
Cardiac Failure
Rela
tive R
isk
MenWomen
Age-Adjusted Relative CVD Risk*
*Relative CVD risk for persons with diabetes versus those without
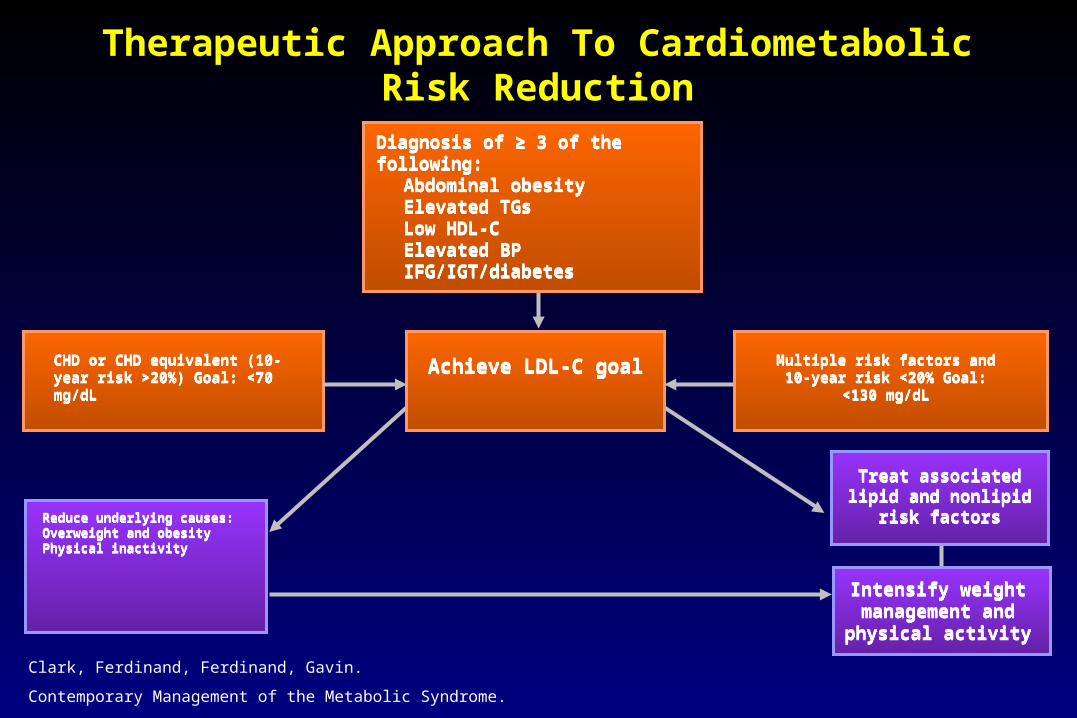
Treat associated lipid and nonlipid risk
factors
Treat associated lipid and nonlipid risk
factors
Intensify weight management and physical activity
Intensify weight management and physical activity
Reduce underlying causes:Overweight and obesityPhysical inactivity
Reduce underlying causes:Overweight and obesityPhysical inactivity
Therapeutic Approach To Cardiometabolic Risk Reduction
CHD or CHD equivalent (10-year risk >20%) Goal: <70 mg/dLCHD or CHD equivalent (10-year risk >20%) Goal: <70 mg/dL
Achieve LDL-C goalAchieve LDL-C goal Multiple risk factors and 10-year risk <20% Goal: <130 mg/dL
Multiple risk factors and 10-year risk <20% Goal: <130 mg/dL
Diagnosis of ≥ 3 of the following:Abdominal obesityElevated TGsLow HDL-CElevated BPIFG/IGT/diabetes
Diagnosis of ≥ 3 of the following:Abdominal obesityElevated TGsLow HDL-CElevated BPIFG/IGT/diabetes
Clark, Ferdinand, Ferdinand, Gavin.
Contemporary Management of the Metabolic Syndrome.

Therapeutic Approach To Cardiometabolic Risk Reduction
IFG/IGT/diabetesIFG/IGT/diabetesProthrombotic stateProthrombotic stateElevated BPElevated BPLow HDL-CLow HDL-CElevated TGsElevated TGs
Weight loss, increased physical activity, counseling. Drug therapy not routinely recommended. If diabetic, optimized
glycemic control
Weight loss, increased physical activity, counseling. Drug therapy not routinely recommended. If diabetic, optimized
glycemic control
Antiplatelet therapy (ASA ± clopidogrel)
Antiplatelet therapy (ASA ± clopidogrel)
Achieve BP goal:<130/80 mm Hg
Achieve BP goal:<130/80 mm Hg
LDL-C is the primary target. Emphasize weight loss and increasing physical activity. Consider
drug therapy in high-risk patients (CHD/CHD equivalents)*
LDL-C is the primary target. Emphasize weight loss and increasing physical activity. Consider
drug therapy in high-risk patients (CHD/CHD equivalents)*
Achieve non-HDL-C goal (LDL-C goal +30)
Achieve non-HDL-C goal (LDL-C goal +30)
*Drug therapy should not be routinely used in patients with IFG/IGT or to prevent diabetes pending the results of ongoing clinical trials.ASA, aspirin; BP, Blood pressure; CHD, coronary heart disease; HDL-C, high density lipoprotein cholesterol; IFG, impaired fasting glucose; IGT, impaired glucose tolerance; LDL-C, low-density lipoprotein cholesterol; TG, triglycerides(Clark, Ferinand: Cardiology Special Edition, 2003)
Intensify weight management and physical
activity
Intensify weight management and physical
activity
Diagnosis of the metabolic syndrome: ≥ 3 of the following:
Abdominal obesityElevated TGsLow HDL-CElevated BPIFG/IGT/diabetes
Diagnosis of the metabolic syndrome: ≥ 3 of the following:
Abdominal obesityElevated TGsLow HDL-CElevated BPIFG/IGT/diabetes
Treat associated lipid and nonlipid risk factors
Treat associated lipid and nonlipid risk factors
Reduce underlying causes:Overweight and obesityPhysical inactivity
Reduce underlying causes:Overweight and obesityPhysical inactivity
CHD or CHD equivalent (10-year risk >20%) Goal: <70 mg/dLCHD or CHD equivalent (10-year risk >20%) Goal: <70 mg/dL
Achieve LDL-C goalAchieve LDL-C goal Multiple risk factors and 10-year risk <20% Goal: <130 mg/dL
Multiple risk factors and 10-year risk <20% Goal: <130 mg/dL
Clark, Ferdinand, Ferdinand, Gavin.
Contemporary Management of the Metabolic Syndrome.
Cardiometabolic Risk:Strategies for Treatment
• Professionals/Patients– Patients with CMR should increase their physical activity level,
lose weight (if overweight) and have their BP and lipid abnormalities treated to recommended goals
– If one cardiometabolic risk factor is present, others should be looked at
– Information on obesity, HBP, and metabolic risk factors for CVD and diabetes should be widely disseminated
– Information on the benefits of physical activity and nutrition should be widely disseminated
– A special campaign to prevent and control childhood obesity should be carried out
Cardiometabolic Risk:Strategies for Treatment
• Professional/lay education– Targeted health promotional programs for various population
groups at cardiometabolic risk
– Partner with CBO for information dissemination
– Integration of individual risk factors for patients with multiple risk factors

Cardiometabolic Risk:Strategies for Treatments
• Research – Addition of metabolic syndrome as an end point in clinical trials
– Assess the benefits of interventions targeting multiple RF in clinical trials
– Randomized clinical trials to assess the effects of treatment of the metabolic syndrome on clinical events and survival
– Improved strategies for management of multiple RF
Unanswered Questions
• What is the incremental risk added by CV risk factors not in the FHS (obesity, elevated TG, IFG)?
• What are the treatment goals (beyond LDL) in patients with multiple risk factors (BP, IFG/IGT, low HDL-C, high TG, overweight/obese)?
• Are there gene-gene and/or gene-environment interactions that predict metabolic syndrome or other clusters of RF and CV risk?
Conclusions
CVD is the leading cause of morbidity/mortality in African Americans
Disparities in cardiovascular health continue to exist, due to: Excessive risk factor burden Patient delays in seeking medical care Under-recognition and under-treatment of high risk individuals Lack of access to routine and modern cardiac medical/procedural care
Prevention of CVD, improving outcomes and decreasing disparities in AA maybe difficult but is not a mystery
A high prevalence of modifiable RF provides great opportunity for prevention
Increase physician awareness of racial disparities in health care Improve compliance and adherence to evidence-based treatment
guidelines Increase educational programs to improve knowledge concerning
cultural competency and sensitivity in clinical settings Increase patient educational programs to
improve knowledge of CVD and available therapies Decrease delays in seeking medical care
Identify and address barriers that limit access to appropriate cardiac services (institutional, provider, health care coverage, etc)
Improve efforts to make cardiovascular care available, accessible,affordable, and acceptable
Increase training of minority clinicians and investigators
Conclusions: Addressing Unmet Needs