metabolic and bariatric surgery: expected outcomes, merits philip omotosho, md assistant professor...
TRANSCRIPT

Metabolic and Bariatric Surgery:Expected Outcomes, Merits
Philip Omotosho, MDAssistant Professor of SurgeryRush Medical College

• Review bariatric surgery as a treatment for morbid obesity
• Review the indications for bariatric surgery• Review the impact of bariatric surgery on co-
morbidity resolution
Objectives
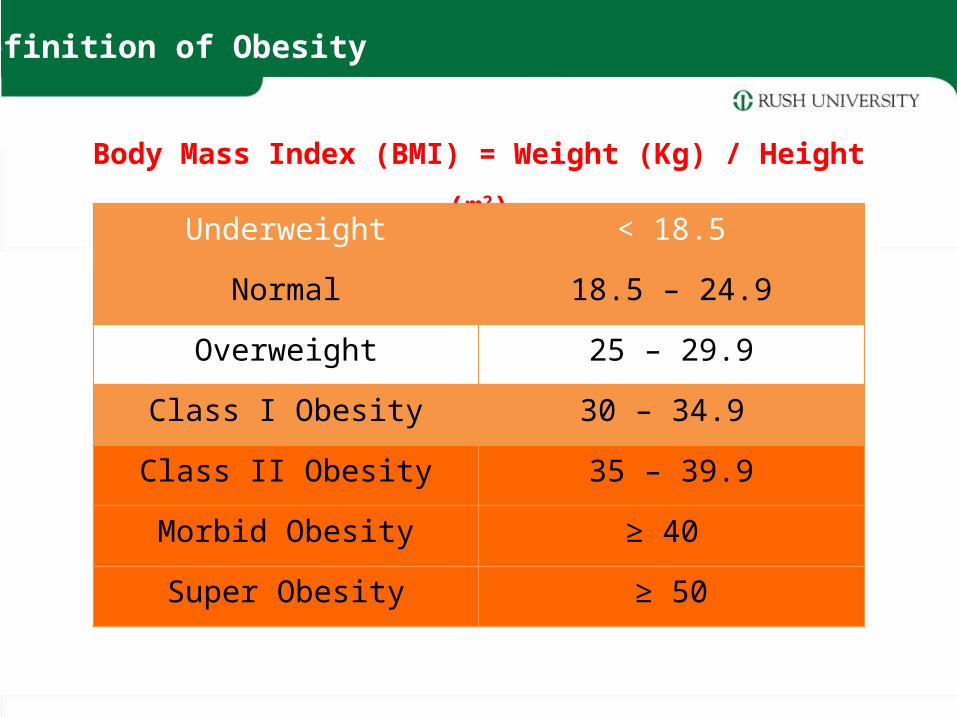
Body Mass Index (BMI) = Weight (Kg) / Height (m2)Underweight < 18.5
Normal 18.5 – 24.9
Overweight 25 – 29.9
Class I Obesity 30 – 34.9
Class II Obesity 35 – 39.9
Morbid Obesity ≥ 40
Super Obesity ≥ 50
Definition of Obesity

Source: Behavioral Risk Factor Surveillance System, CDC.
15%–<20% 20%–<25% 25%–<30% 30%–<35% ≥35%
Prevalence* of Self-Reported Obesity Among U.S. Adults
by State and Territory, BRFSS, 2013*Prevalence estimates reflect BRFSS methodological changes started in 2011. These estimates should not be compared to prevalence estimates before 2011.
CA
MT
ID
NVUT
AZNM
WY
WA
OR
CO
NE
ND
SD
TX
OK
KS
IA
MN
AR
MO
LA
MI
IN
KY
ILOH
TN
MS AL
WI
PA
WV
SC
VA
NC
GA
FL
NY
VT
ME
HI
AK
NHMARICTNJDEMDDC
PRGUAM
• Worldwide obesity has more than doubled since 1980• In 2008, 1.5 billion adults, 20 and older were overweight. Of these
over 200 million men and nearly 300 million women were obese• 65% of the world’s population live in countries where overweight
and obesity kills more people than underweight• Nearly 43 million children under the age of five were overweight in
2010• Obesity is preventable
World Health Organization Fact SheetKey Facts

Mortality risk associated with morbid obesity
6Gray DS., Med Clin North Am. 1989; 73(1):1–13
2.5
2.0
1.5
1.0
20 25 30 35 40
BMI
MortalityRatio
Moderate VeryLow Low Moderate High Very
High
MenWomen
X

• Although weight may be reduced acceptably with non-surgical means, most patients fail to maintain a reduced weight
• Indications for bariatric surgery:BMI ≥ 40 BMI ≥ 35 plus associated significant obesity-related comorbidityFailure of non-surgical weight loss attempts
1991 NIH Consensus Development Conference on Gastrointestinal Surgery for Severe Obesity

Restrictive Adjustable Gastric Banding
Sleeve Gastrectomy
Combined Modality(Both restrictive and malabsorptive mechanisms)
Roux-en-Y Gastric Bypass
Biliopancreatic Diversion with Duodenal Switch
Classification

• Appetite Control
• Glucose and Lipid Metabolism
• Insulin Homeostasis
• Regulatory Peptides
Surgically-induced changes in the entero–encephalic endocrine axis (Metabolic Surgery)
Beyond Weight Loss
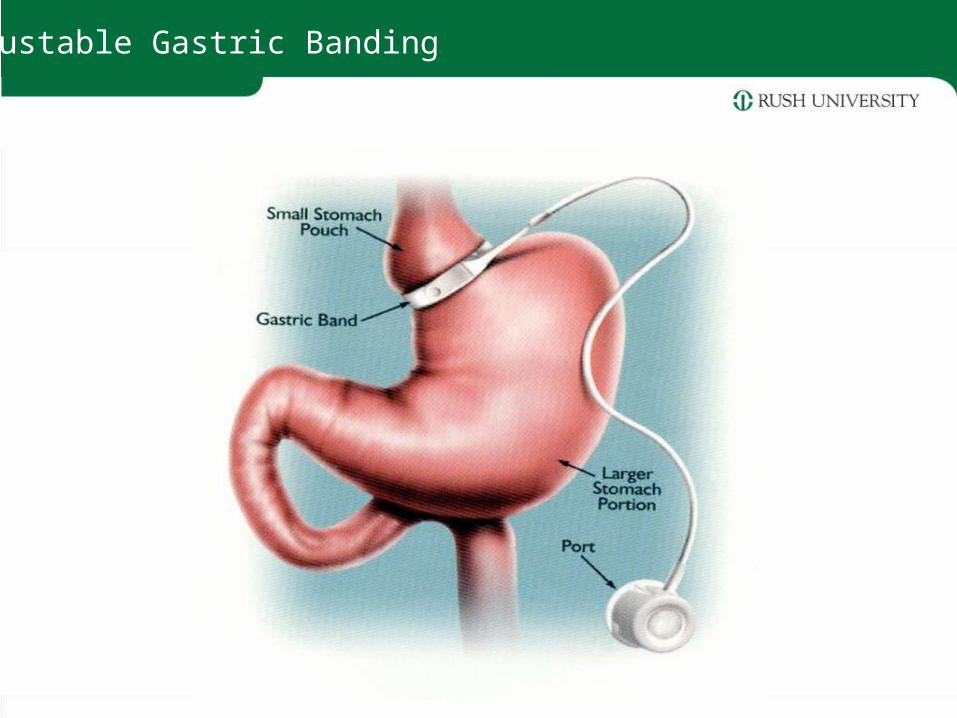
Adjustable Gastric Banding

• FDA approved in 2001 for implantation in the United States
• Non-resectional• Placed just below the esophagogastric
junction, creating a “virtual pouch”• Adjusted via subcutaneous access port
Adjustable Gastric Banding

Subcutaneous Port / Huber needle

Sleeve Gastrectomy

• Originally performed as the restrictive component of the duodenal switch procedure
• Risk management strategy for severely obese or high risk patients
• Substantial improvement in comorbidities in 1-2 yrs followed by a second-stage operation – RYGB or BPD/DS
• Early reports emerged of substantial weight loss with sleeve gastrectomy alone
Sleeve Gastrectomy

Roux-en-Y Gastric Bypass
• Reduced stomach capacity (small pouch)
• Malabsorptive limb• No resection• Weight loss from both
restriction and malabsorption
• Considered the gold standard for bariatric surgery
15

Biliopancreatic Diversion with Duodenal Switch

• Buchwald Meta-analysis 22,094 patients
• Operative mortality – Restrictive procedures 0.1%
– RYGB 0.5%
– BPD/DS 1.1%
Buchwald H, et al: Bariatric Surgery: A systematic review and meta-analysis. JAMA 292:1724-1737, 2004
Surgical Risk – Perioperative Mortality

Surgical outcomes – Risk
18N Engl J Med 2009;361:445-54.

Surgical outcomes
Surgery decreases long-term mortality, morbidity, and healthcare use in morbidly obese patients
Total direct healthcare cost for control patients was 45% HIGHER than for bariatric surgery patients
• 5-year mortality rates
– 0.68% bariatric surgery patients
– 6.17% control patients
19
Christou et al. Ann Surgery 2004
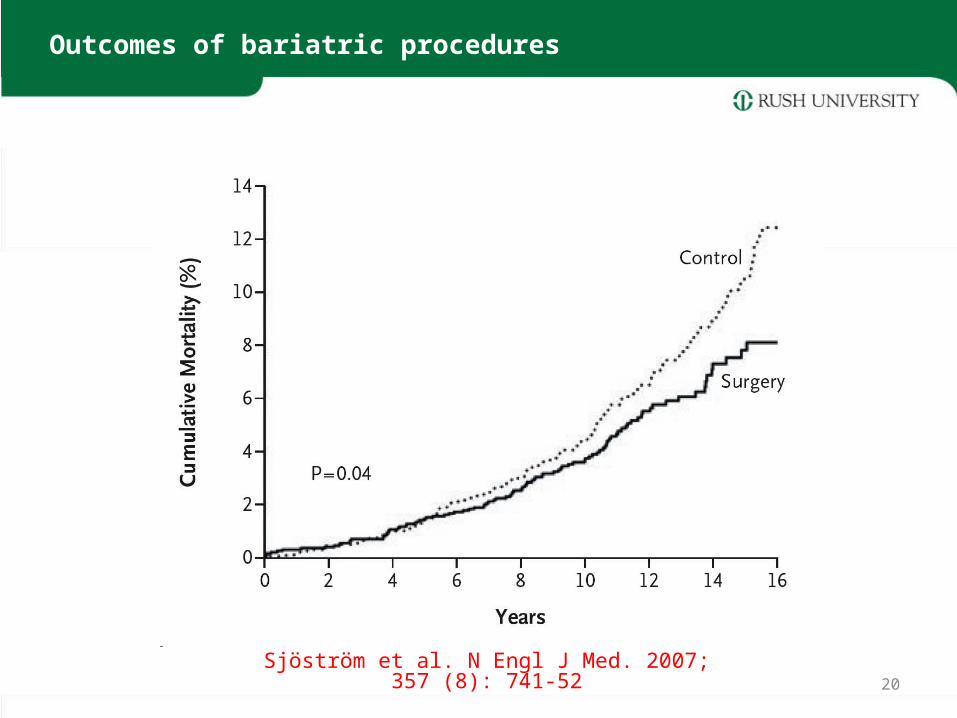
Outcomes of bariatric procedures
20
Sjöström et al. N Engl J Med. 2007; 357 (8): 741-52

Sjöström et al. 357 (8): 741, NEJM ; August 23, 2007
Long-term Weight Loss Outcomes: SOS Study
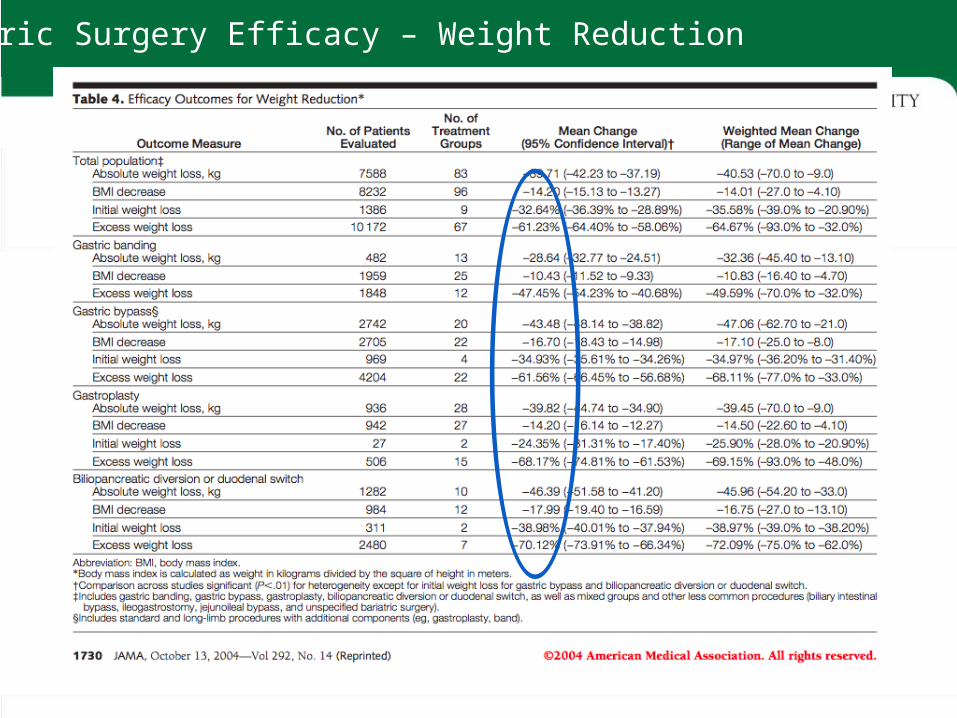
Bariatric Surgery Efficacy – Weight Reduction
• 50-60% EWL at 1 year– Some studies report EWL ~ 80% at 1 year (Schauer)
• Long term results?– 84% EWL | 3yrs | Boza et al. Mean preop BMI 37– 55% EWL | 5 years | Bohdjalian et al. Mean preop BMI 48.2
– 48% EWL | 8 years | Eid et al. Mean preop BMI 66
Sleeve Gastrectomy

Hutter MM et al. Ann Surg 2011; 254:410-20
Reduction in BMI

Obesity and Diabetes RiskObesity and Diabetes Risk
0
20
40
60
80
100
<20 20-25 25-30 30-35 35-40 >40
BMI Levels
Incidence of New Casesper 1000 Persons/Year
-
Knowler WC et al. Am J Epidemiol 1981
Overweight
19
Obese
30
Morbidly Obese
45-65

Classic Pathogenesis of Type II Diabetes
26
1 •Excess Energy Intake•Diminished Energy Expenditure
2 •Increase Body Weight•Increase Insulin Resistance
3 •Type II Diabetes

Evidence Based Pathogenesis of Type II
Diabetes
27
Perturbation of energy/glucose homeostasis
Behavior
Genetic
Environment
Obesity Diabetes
Surgical Treatment of Diabetes
Ann Surg 1987; 206(3):316-23
- Cohort of 42 pts with Type 2 DM- Post-operative normalization of fasting blood glucose,
fasting insulin, and HbA1c- Improvement in insulin release, insulin resistance
and utilization of glucose

Buchwald, H. et al. 2004
Bariatric surgery: a systematic review and meta-analysis
989
% Resolution (95% Confidence Interval)
0 20 40 60 80 100
98.9 (96.8, 100.0)
47.9 (29.1, 66.7)
83.8 (77.3, 90.1)
Duodenal Switch
Gastric Bypass
Gastric Banding205
288
Type 2 DM Remission

Surgery (N=30) Control (N=30)
Remission in % (N) 73% (22/30) 13% (4/30)
Achieving A1C < 6.2% in % 80% (N=24) 20% (N=6)
Medication use (N) 4 28
Weight loss (mean±SD) in % 20±9.4 1.4±4.9
Excess wt loss (mean±SD) % 62.5 4.3
Change in BMI (kg/m2) - 7.4 - 1.5Dixon, JB et al. JAMA 2008;299:316-323
LAGB: Weight Loss and Diabetes Remission

N Engl J Med 2012. Copyright © 2012 Massachusetts Medical Society.

Schauer P. et al.

Schauer P. et al.

Schauer P. et al.

N Engl J Med 2012. Copyright © 2012 Massachusetts Medical Society.

Mingrone G. et al

Bariatric Surgery Efficacy – Hyperlipidemia

Bariatric Surgery Efficacy – Obstructive Sleep Apnea

Sugerman, H. et al. Ann Surg 1999; Vol. 229(5): 634–642
Efficacy – Pseudotumor Cerebri

Malik SM et al. World J Diabetes 2012; 3(4): 71-79
“Bariatric surgery should be considered along with other medical and life-style alterations as first line therapy in PCOS women with obesity and MS.”
Bariatric Surgery Efficacy – PCOS


Torquati et al. J Am Coll Surg 2007;204:776–783
Efficacy – Cardiovascular Morbidity

Torquati et al. J Am Coll Surg 2007;204:776–783
Efficacy – Cardiovascular Morbidity

,
Anatomic Modifications Result in Alteration of GI Hormone Activity

The Foregut Theory– Exclusion of the duodenum
results in inhibition of a putative signal that is responsible for insulin resistance and/or abnormal glycemic control (T2DM)
Rubino et.al, Ann Surg, 2006
The Entero-Insular Axis
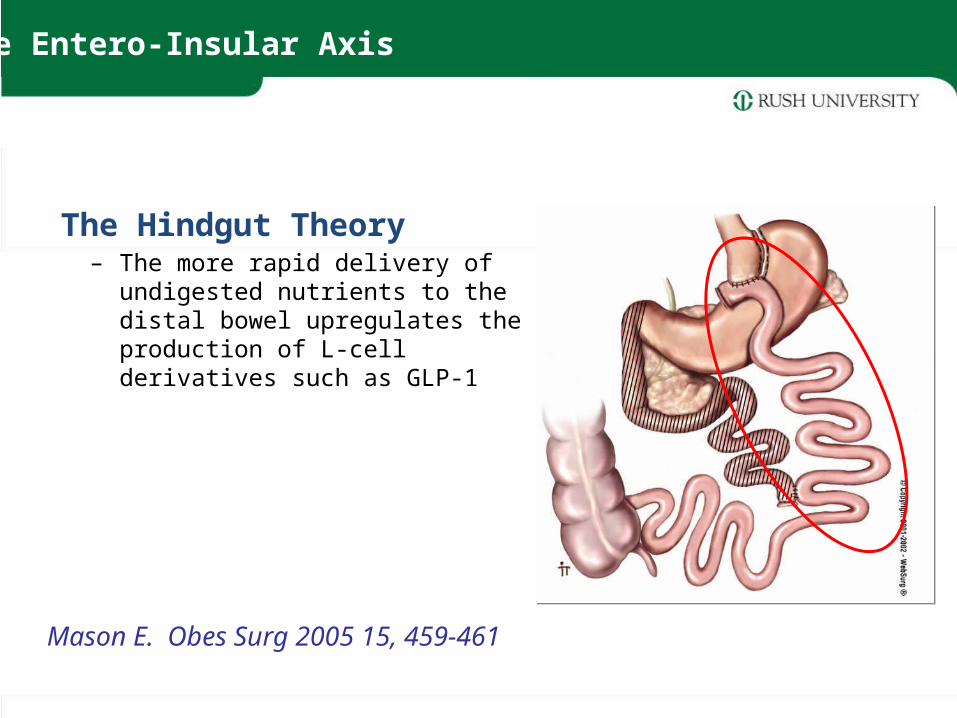
The Hindgut Theory– The more rapid delivery of undigested
nutrients to the distal bowel upregulates the production of L-cell derivatives such as GLP-1
Mason E. Obes Surg 2005 15, 459-461
The Entero-Insular Axis

‘…Reflects the enormous positive effects of bariatric surgery on the metabolic complications of severe obesity, including type 2 diabetes mellitus, sexual hormone dysfunction in both men and women (polycystic ovarian syndrome), non-alcoholic liver disease, and lipid metabolism (both cholesterol and triglycerides), but maintains in its name the positive effect of weight loss on pressure-related phenomenon (baros or bariatric) such as joint disease, GERD, urinary incontinence, obesity hypoventilation, venous stasis disease, and pseudotumor cerebri.’
Harvey Sugerman, MD
Conclusion