mental health services executive clinical leadership
TRANSCRIPT

Mental Health Services Executive Clinical Leadership
Program Project Overview– Running
Away Causes Delay
June 2017 Tanya Dugard
Quality Manager Mental Health Services, MNCLHD

Quality Project Overview
Reducing absconding events in CHAMHU
MHS Absconding Report, June 2017 Page 1
Table of Contents No. Page Executive Summary 2 1. Background 3 2. Aim and SMART checklist 4 3. Rationale and Purpose 5 4. Deliverables and Constraints 6 5. Work plan 8 6. Stakeholder Communication 9 7. Team Members 10 8. Resources 1 9. Evaluation 12 10. Reporting 15 11. Sustainability and Spread 15 Appendices
One – Action plan 16
Two – Driver Diagram 17 Three –Patient Stories - example 18
ABBREVIATIONS
Title Abbreviation Mid North Coast Local Health District MNCLHD
Mental Health Services MHS
Clinical Excellence Commission CEC
Ministry of Health MOH
Specialty Health Network SHN
High Dependency Unit HDU
Low Dependency or Open Area LDU

Quality Project Overview
Reducing absconding events in CHAMHU
MHS Absconding Report, June 2017 Page 2
EXECUTIVE SUMMARY OUTLINE This report provides a summary of the Quality Project – Running Away Causes Delay – reducing absconding incidents in Coffs Harbour Mental Health Inpatient Unit. This was facilitated via the Executive Clinical Leadership Program Cohort 17 BACKGROUND As a result of a number of incidents of patients absconding from mental health inpatient units, a safety notice was issued to Local Health Districts and Specialty Health Networks (LHDs and SHNs) in June 2016 in conjunction with results from the MNCLHD Mental Health Clinical Incident Trending report indicated that 17% of all admissions resulted in an absconding event. Of those events Coffs Harbour mental health inpatient unit accounted for 49% of all absconding events for the July 2015 to June 2016 period. OUTCOMES TO DATE Completion of Capitol works to the Inpatient unit which included removal of trees,
raising and lowering of fences, installation of airlock facility
Multidisciplinary Team Clinical Reviews recommenced
Supervision in courtyards
Flexible Visiting Hours introduced
Leave included in Clinical Handover
Patient stories commenced
Participation in Smoke free working party – who now attend the group program
Leave procedure finalised for global consultation
Process for including alerts of absconders to be embedded into Complex care
procedure
RESULTS
21% Decrease in Absconding rates
100% of all Mental Health Consumers are involved in multidisciplinary team review
100% of all Clinical Handovers include Leave
40% visitations to the Coffs Harbour mental health inpatient unit occurred outside
of the recommended visiting hours
53% of consumers who were identified as a smoker was provided the appropriate
processes to commence smoking cessation
10% of those who absconded were repeat absconders
56% events were absconding Type 1 (directly from the unit) (50% in 2015/2016)
o 42% absconded via the courtyard (68% in 2015/16)
o 57% absconded via the door (31% in 2015/2016)
Quality Project Overview
Reducing absconding events in CHAMHU
MHS Absconding Report, June 2017 Page 3
1. Background As a result of a number of incidents of patients absconding from mental health inpatient units, a safety notice was issued to Local Health Districts and Specialty Health Networks (LHDs and SHNs). Chief Executives had to ensure that a rigorous process is in place to support the safe and appropriate assessment of involuntary patients prior to the approval of leave being granted from a mental health inpatient unit. A number of tasks were allocated to each LHD which included 1. Distribute this notice to all stakeholders and all mental health inpatient units. 2. Undertake a safety audit of the physical environment of all mental health inpatient units in the LHD/SHN to identify any requirements to reduce the risk of patients absconding and report to the Ministry by 1 August 2016. 3. Review any absconding incidents to identify areas for improvement of risk management and report to the Ministry by 1 August 2016. 4. Audit and revise the current procedures for leave from mental health inpatient units with a view to reducing absconding incidents and to better assess and manage the risk of harm to self or others. This is to include a review of risk assessment protocols, including the patient’s past history of absconding and current absconding risk. This is to be reported to the Ministry by 1 August 2016. 5. Ensure that any leave decisions be considered by a multidisciplinary team, and the outcomes documented, with regard to improved management of the risk of harm to self or others from patients prior to approval by the treating psychiatrist. The patient’s leave plan must include written advice to the family/carer concerning measures to manage risks during leave, including risk of harm to self or others, and the provision of a crisis plan if difficulties arise during leave. This, and written advice and information, must be provided to the family/carer prior to the leave. As part of the project, that despite the results of each of the actions required further information would be sought by the project team to identify further innovative areas of improvement

Quality Project Overview
Reducing absconding events in CHAMHU
MHS Absconding Report, June 2017 Page 4
2. Aim and SMART
SMART CHECKLIST Specific An agreed and identified problem that Mental Health Services
is trying to solve? Reducing Absconding Rates in Coffs Harbour Mental Health Inaptient Unit by 50%
Yes
Measurable How will you know if the problem has been solved? Reduction in Absconding rates
Changes to process and Balance measures
Yes
Achievable Resources allocated to address problem? Budget for capitol works $80K
Project management for smoke free
Team allocated for project
Yes
Realistic Is it likely that the desired outcome really will be achieved? Major changes to unit and processess within
Yes
Time-based Clear and appropriate start and finishing dates for the implementation of the work
June 2017
3. Rationale and Purpose Results from the MNCLHD Mental Health Clinical Incident Trending report indicated that 17% of all admissions resulted in an absconding event. Of those events Coffs Harbour mental health inpatient unit accounted for 49% of all absconding events. Further data indicated the following • 84% (n=39) of the inpatients were involuntary • 58% (n=23) were involuntary patients absconded directly from the unit (Absconding Type 1) • The most common form of absconding was over the fence 20% (n=8) including one incident where the patient absconded over the High Dependency Unit (HDU) fence. • 17% were patients on trial leave to the low dependency unit from HDU • 1% were recently transferred to Low Dependency Unit (LDU) from HDU • Out of the Five repeat absconders four patients absconded more than twice during a single admission • 30% (n=12) had noted in the incident that there was a history of absconding • 23% (n=9) returned to the unit within 48 hours • 20% of all admissions during July 2015 to June 2016 included an absconding event
Quality Project Overview
Reducing absconding events in CHAMHU
MHS Absconding Report, June 2017 Page 5
4. Deliverables and Constraint CHANGES
Recommendations Endorsed by Director of reports submitted to MOH –
August 2016
Environment
Review of all fenced courtyards
Removal of trees in courtyards near the fence
Increased supervision in courtyards by staff
Reduction of access to IPU
Review of establishing an air lock in the front door
Absconding Report July 2016
Increase in supervision
Post debriefing with consumers who have absconded
All inpatient services review and explore opportunities to implement improved
smoke free activities
Patients sent out on time out of High Dependency units are to remain on
15/60 observations
Use of eMR to identify high risk absconders through alert system
Use the Trauma informed care and Practice Organisation Toolkit to assess
Mental health services commitment to Trauma informed care
Procedure Review
Mental Health Leave procedure finalised
Care level procedure to include auditing requirements of patients on care
level 3 to remain under nurse escort
Ongoing training regarding risk assessment in eMR and improvement of
documentation thereof
Management of Consumers In Mental Health High Dependency Units
completed
Clear documentation requirements pertaining to leave and care levels
Deliverables
Increased supervision of patients
More time with the patients
More patient centred care approach
Better Communication processes in the identification of high absconding
risks
Less absconding incidents
Improved Communication between clinicians and consumers
Improved understanding of rules and responsibilities in the unit
Improved insight to the reasons why consumers abscond

Quality Project Overview
Reducing absconding events in CHAMHU
MHS Absconding Report, June 2017 Page 6
Other
Project Team through brainstorming via driver diagram
Meet with project team to further identify more innovative ideas to improve
Work in conjunction with Productive MH wards to release time to care
Proposed outcome is to have closer governance and engagement of patients
in their care and improve treatment plans at commencement of admission by
the provision of alerts in the Electronic Medical Record
Constraints
Reluctance by Staff to engage with increased supervision in courtyards
Enough time to implement all the recommendations as well as consideration
for new ones
Quality Project Overview
Reducing absconding events in CHAMHU
MHS Absconding Report, June 2017 Page 7
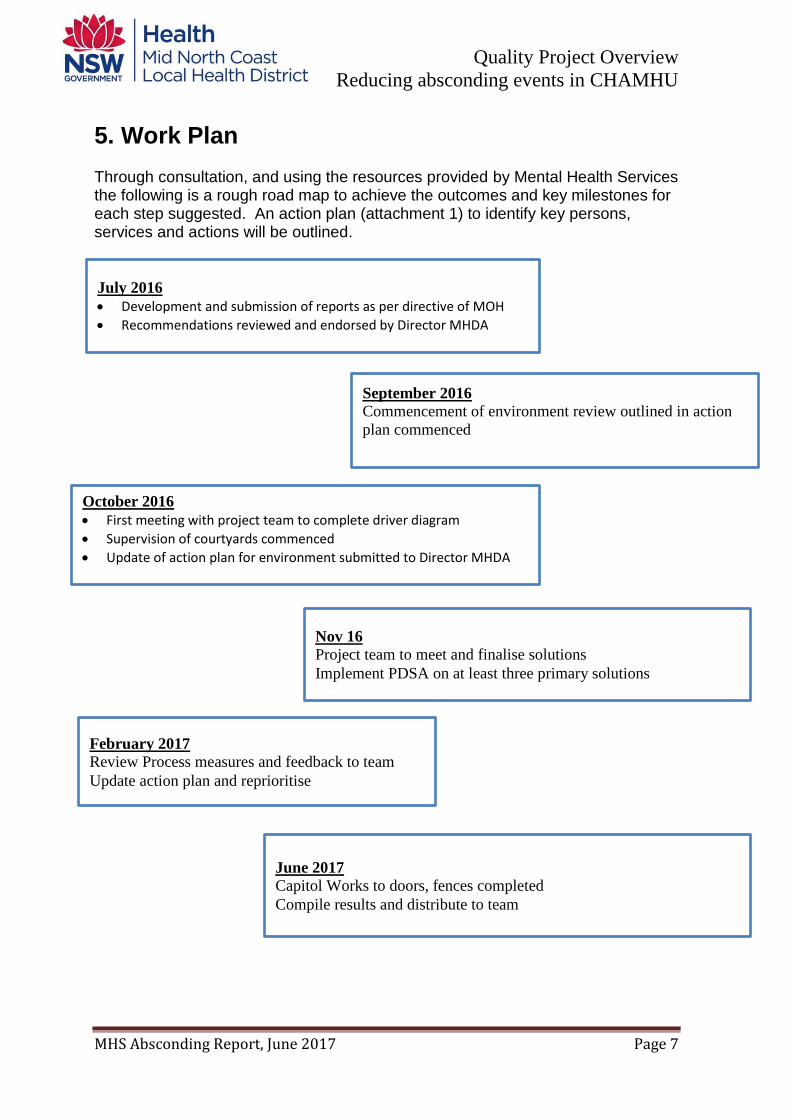
5. Work Plan Through consultation, and using the resources provided by Mental Health Services the following is a rough road map to achieve the outcomes and key milestones for each step suggested. An action plan (attachment 1) to identify key persons, services and actions will be outlined.
July 2016
Development and submission of reports as per directive of MOH
Recommendations reviewed and endorsed by Director MHDA
September 2016
Commencement of environment review outlined in action
plan commenced
October 2016
First meeting with project team to complete driver diagram
Supervision of courtyards commenced
Update of action plan for environment submitted to Director MHDA
Nov 16
Project team to meet and finalise solutions
Implement PDSA on at least three primary solutions
February 2017
Review Process measures and feedback to team
Update action plan and reprioritise
June 2017
Capitol Works to doors, fences completed
Compile results and distribute to team

6. Stakeholder Communications Worksheet
Stakeholder name Communication Approach (from
Power/interest grid)1
Key interests and issues Current status
2
Desired support
3
Desired Actions Messages to convey
Action and communication
Director Mental Health, Drug and Alcohol
Monitor
Progress on recommendations Monthly reports
Advocate High Drive change
Information
Senior Executive Team Alan Pretty
Monitor
Monthly reports
Advocate High Drive Change Supply infomration action plan update on environmental changes
MHS Workforce Keep informed Supervision of consumers Care levels Provision of reports
Critic: Blocker Medium Implement change progress with project
Official Visitors Keep Satisfied Supervision in courtyards Supporter low support change Progress with Project
Facility Managers Keep informed Action plans and implementation thereof
Support High Implement Change Progress with project
Patients and carers
Keep satisfied Leave arrangements debriefing tool
Neutral low Receive /participate Change and feedback
information
Project Team Keep Informed progress of PDSA Cycles and results of data
Advocate HIGH Develop change methods
Support and implement change
Patient safety and quality Committee
Monitor Results of audits advocate High Endorse change Update on progress
1 Manage closely; keep satisfied; keep informed; monitor
2 Advocate (actively helping success); Supporter; Neutral; Critic; Blocker
3 What support do you require from them? High / medium / low

7. Team Members Project Sponsor – Alan Pretty, General Manager Mental health Services
Team Lead – Tanya Dugard, Quality Manager, Mental Health Services
Nurse Unit Manager – Coffs Harbour Mental Health Inpatient unit –
Paul Gover
Clinical Nurse Consultant level 3
(Senior MH Nurse) – Kim Edwards
Social Worker Michelle Donges
Clinical Nurse Educator
Allyson Wilson
Occupational Therapist
Jaclyn Cansdell
Health Security Assistant
Kathy Brazel
Consumer Representative
Nicholas Kosseris
Clinical Director – Dr Afraz Zaman
Clinical Educator Lynn Davies

8. Resources
Date Resources Cost
12/2016 Environmental audit conducted with recommendations and Quotes to physically change inpatient unit structure
$88K
06/2016 Participation in executive Clinical Leadership program including flights and accommodation
$10K

Quality Project Overview
Reducing absconding events in CHAMHU
MHS Absconding Report, June 2017 Page 3
9. Evaluation
The following are the tools to determine the effectiveness of the work plan:
OUTCOME MEASURE (Measured at end of period September 2016 – May 2017) Total Absconding Events in same measurement period September 2016 - May 2017 and compare to previous measured period Results
A 21% decrease in absconding events measured over the same period
25 absconding events compared to 32 from the previous year % Consumers who abscond more than once in the measured time frame
Quality Project Overview
Reducing absconding events in CHAMHU
MHS Absconding Report, June 2017 Page 4
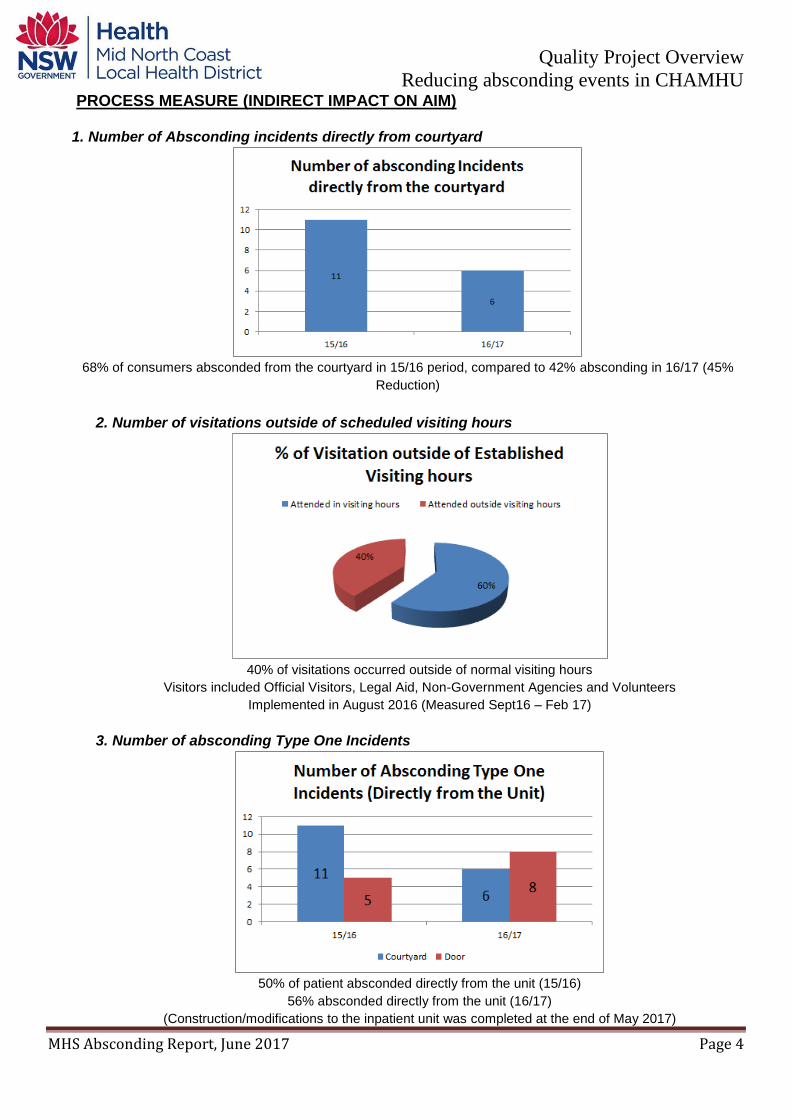
PROCESS MEASURE (INDIRECT IMPACT ON AIM)
1. Number of Absconding incidents directly from courtyard
68% of consumers absconded from the courtyard in 15/16 period, compared to 42% absconding in 16/17 (45%
Reduction)
2. Number of visitations outside of scheduled visiting hours
40% of visitations occurred outside of normal visiting hours
Visitors included Official Visitors, Legal Aid, Non-Government Agencies and Volunteers
Implemented in August 2016 (Measured Sept16 – Feb 17)
3. Number of absconding Type One Incidents
50% of patient absconded directly from the unit (15/16)
56% absconded directly from the unit (16/17)
(Construction/modifications to the inpatient unit was completed at the end of May 2017)

Quality Project Overview
Reducing absconding events in CHAMHU
MHS Absconding Report, June 2017 Page 5
4. Number of leave prescriptions in eMR (Measurement taken on 23/6/17) Measurements taken on 23 mental health consumers in Coffs Harbour Mental Health Inpatient unit in the open area. 100% of all consumers had a leave prescription 5. % Use of leave in clinical handover Measurements taken on 23 electronic medical records to locate clinical handover sign of mechanism. 100% had leave arrangements documented in the handover tool.
6. % of consumers who smoke offered NRT upon admission
Documentation Audit conducted in April 2017 indicated that 53% of consumers who were
identified as a smoker was provided the appropriate processes to commence smoking
cessation
7. Number of Patient stories = 2
o Themes identified – issues with not being listened to, medication not helping and
misinterpreting information due to psychosis
BALANCING MEASURE Side Effect Number of Patients readmitted within 28/7 who had absconded prior
A vast reduction in the readmission rates
Quality Project Overview
Reducing absconding events in CHAMHU
MHS Absconding Report, June 2017 Page 6
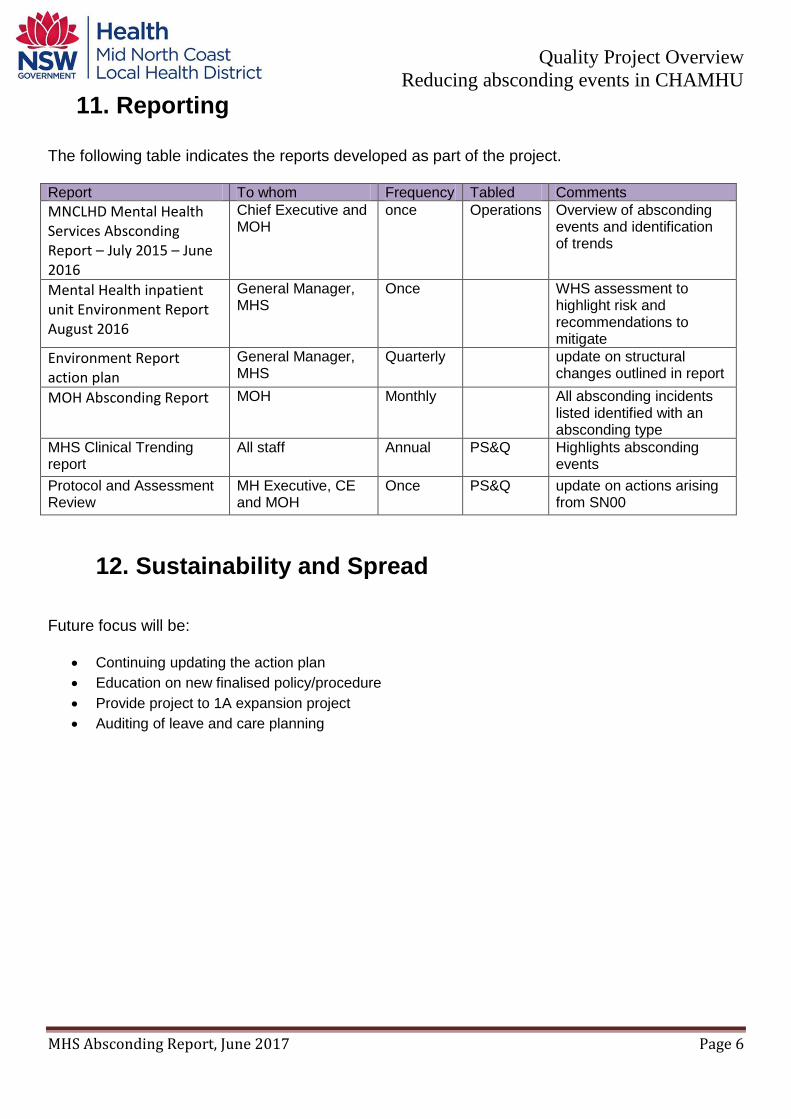
11. Reporting The following table indicates the reports developed as part of the project. Report To whom Frequency Tabled Comments
MNCLHD Mental Health Services Absconding Report – July 2015 – June 2016
Chief Executive and MOH
once Operations Overview of absconding events and identification of trends
Mental Health inpatient unit Environment Report August 2016
General Manager, MHS
Once WHS assessment to highlight risk and recommendations to mitigate
Environment Report action plan
General Manager, MHS
Quarterly update on structural changes outlined in report
MOH Absconding Report MOH Monthly All absconding incidents listed identified with an absconding type
MHS Clinical Trending report
All staff Annual PS&Q Highlights absconding events
Protocol and Assessment Review
MH Executive, CE and MOH
Once PS&Q update on actions arising from SN00
12. Sustainability and Spread
Future focus will be:
Continuing updating the action plan
Education on new finalised policy/procedure
Provide project to 1A expansion project
Auditing of leave and care planning

Appendix One: Action Plan
Mental Health Services, MNCLHD
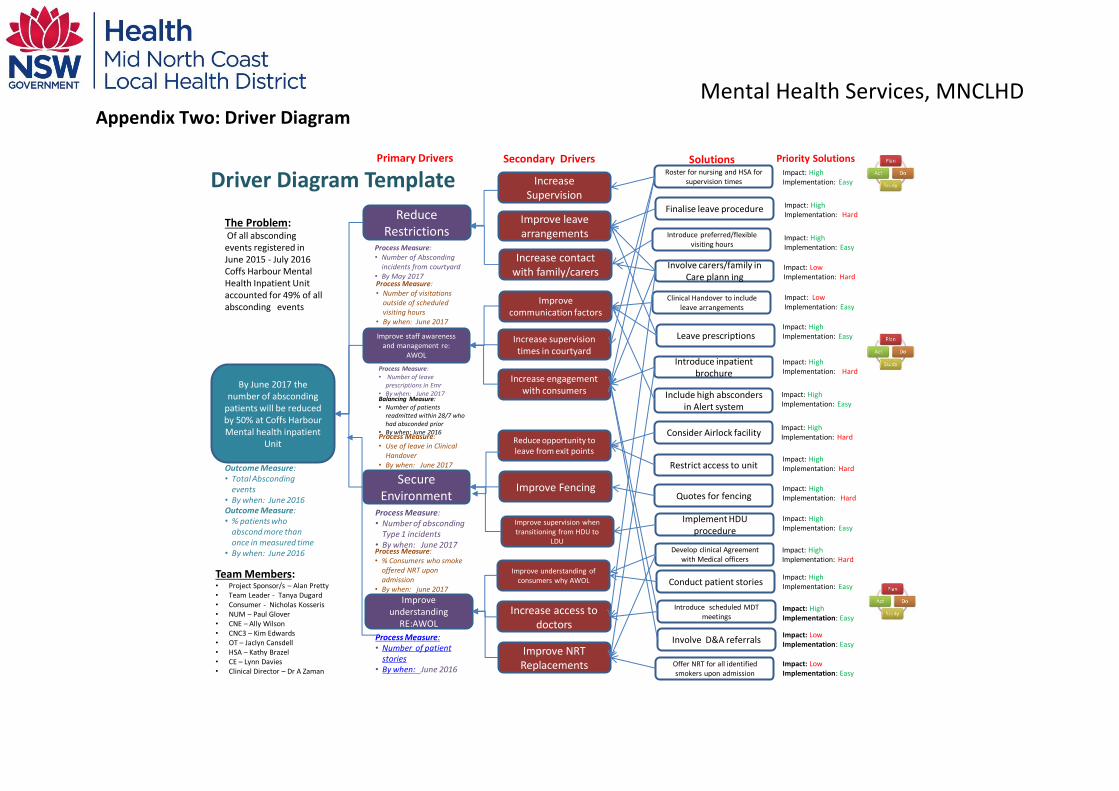
Appendix Two: Driver Diagram
Driver Diagram Template
By June 2017 the number of absconding
patients will be reduced by 50% at Coffs HarbourMental health inpatient
Unit
Outcome Measure: • Total Absconding
events• By when: June 2016
Reduce Restrictions
Process Measure: • Number of Absconding
incidents from courtyard• By May 2017
Process Measure: • Number of leave
prescriptions in Emr• By when: June 2017
Process Measure: • Number of absconding
Type 1 incidents• By when: June 2017
Secure Environment
Improve staff awareness and management re:
AWOL
Improve understanding
RE:AWOL
Process Measure: • Number of patient
stories• By when: June 2016
Increase Supervision
Improve leave arrangements
Increase contact with family/carers
Improve communication factors
Increase supervision times in courtyard
Increase engagement with consumers
Reduce opportunity to leave from exit points
Improve Fencing
Improve supervision when transitioning from HDU to
LDU
Improve understanding of consumers why AWOL
Increase access to doctors
Improve NRT Replacements
Roster for nursing and HSA for supervision times
Finalise leave procedure
Introduce preferred/flexible visiting hours
Involve carers/family in Care plann ing
Clinical Handover to include leave arrangements
Leave prescriptions
Introduce inpatient brochure
Include high absconders in Alert system
Consider Airlock facility
Restrict access to unit
Quotes for fencing
Implement HDU procedure
Develop clinical Agreement with Medical officers
Conduct patient stories
Introduce scheduled MDT meetings
Involve D&A referrals
Offer NRT for all identified smokers upon admission
Impact: High Implementation: Easy
Impact: High Implementation: Hard
Impact: High Implementation: Hard
Impact: High Implementation: Hard
Impact: High Implementation: Easy
Impact: High Implementation: Hard
Impact: High Implementation: Easy
Impact: High Implementation: Easy
Impact: LowImplementation: Easy
Impact: LowImplementation: Easy
Impact: LowImplementation: Hard
Impact: LowImplementation: Easy
Impact: High Implementation: Easy
Impact: High Implementation: Hard
Impact: High Implementation: Easy
Impact: High Implementation: Hard
Impact: High Implementation: Easy
Team Members:• Project Sponsor/s – Alan Pretty• Team Leader - Tanya Dugard• Consumer - Nicholas Kosseris• NUM – Paul Glover• CNE – Ally Wilson• CNC3 – Kim Edwards• OT – Jaclyn Cansdell• HSA – Kathy Brazel• CE – Lynn Davies• Clinical Director – Dr A Zaman
The Problem: Of all absconding events registered in June 2015 - July 2016 Coffs Harbour Mental Health Inpatient Unit accounted for 49% of all absconding events
Outcome Measure: • % patients who
abscond more than once in measured time
• By when: June 2016
Process Measure: • Number of visitations
outside of scheduled visiting hours
• By when: June 2017
Process Measure: • Use of leave in Clinical
Handover• By when: June 2017
Process Measure: • % Consumers who smoke
offered NRT upon admission
• By when: june 2017
Primary Drivers Secondary Drivers Solutions Priority Solutions
Balancing Measure: • Number of patients
readmitted within 28/7 who had absconded prior
• By when: June 2016

Appendix Three: Sample Patient Story
BIN
DIN
G M
AR
GIN
– N
O W
RIT
ING
FAMILY NAME MB MRN
GIVEN NAME □ MALE □ FEMALE
Facility:
D.O.B / / . M.O.
ADDRESS
Mental Health Services Post Incident Debrief Tool
LOCATION/WARD
COMPLETE DETAILS OR AFFIX PATIENT LABEL HERE
“PLEASE”- Engage/Analyse/Summarise DATE CONDUCTED = 9/3/17
E = Engage - “How do you feel about what happened?” The consumers experience of the event, from the consumers’ perspective. Provide information to the consumer and carer about the event (assisting in understanding), provide emotional support, validate the consumer’s feelings associated with the event and repair or improve rapport
Felt labelled
Freaked me out
Paranoid about telephone lines
Went over the fence and walked into town and went home and partner drove him back
Po
st In
cid
en
t De
brie
f To
ol
A - Analysis What are the triggers that causes these actions?: (What sets off the aggression/anger/disturbed behaviour?)
I told the doctor about a peodophile experience and he asked me if I thought I would become one
I was totally psychotic and could not deal with what the doctor said to me so I left the unit
What do you notice in yourself when the triggers are brought on? (What physical signals of distress are there? What is noticed by
the consumer and staff?)
More tolerant now these days
What are some strategies you can use to help you manage stress? (What are some individual and specific strategies to manage or minimise
stress)
Summarise the review Consumer Care Plan Updated in eMR
(Adapted from the PLEASE© Debrief Model iSim Centre)
Page 1 of 2