mental health promotion at work … health promotion at work roundtable organised by eurohealthnet...
TRANSCRIPT

MENTAL HEALTH PROMOTION AT WORK
ROUNDTABLE
Organised by EuroHealthNet
Brussels, 19 th May 2015
The scientific base for healthy work environment
Natalia Wege, MD, MPH
Institut of Occupational and Social Medicine,
Center for Health and Society, University of Duesseldorf, Germany

Provides access to a core social role in adult life- Continuous salary, wage (economic independence)
- Social status and socioeconomic security
- Prestige, social identity
Enables meeting of demands- Motivation of agentic self, structuring of time
- Success, self efficacy
- Continuous learning, skill development
Offers reward, recognition, and belonging
- Enlarged social network (beyond family)
- Social support and cooperation
- Recognition of achievement
Work has the potential of maintaining and
promoting mental health!

Continuous automatisation of production
Microelectronic revolution of information and communication technologies
Increase of service and IT sectors within the labour market
High prevalence of psychomental and socio-emotional stress at work
Growth of flexible and precarious employment, work-life imbalance
Job instability and insecurity, forced mobility
High work pressure, often related to economic globalization
Modern working life carries opportunities and
risks for mental health!

Increase of work pressure 2004-2010: European Social Survey, 19 EU member states
Source: Gallie D (Ed.) (2013) ESS Topline Results Series 3, European Social Survey

Increase in perceived job insecurity 2004-2010: European Social Survey, 19 EU member states
Source: Gallie D (Ed.) (2013) ESS Topline Results Series 3, European Social Survey

Challenges
In view of the burden of reduced mental health in
general, and of depression in particular, across
European working populations:
1. What is the role of stressful work in increasing the risk of incident poor mental health?
– How can we identify and define stressful work?
– How can we provide scientific evidence?
2. What are the policy implications of current knowledge for improving mental health at work?

Three complementary theoretical models of
stressful work and their prediction of health risks

Active
Passive
Low-
strain
High-
strain
Psychological Demands
De
cis
ion
la
titu
de
(c
on
tro
l)low high
low
hig
h
The demand-control model(R. Karasek 1979, R. Karasek, T. Theorell 1990)
Source: Karasek: Healthy work, New York: Basic Books, 1990, p. 32.
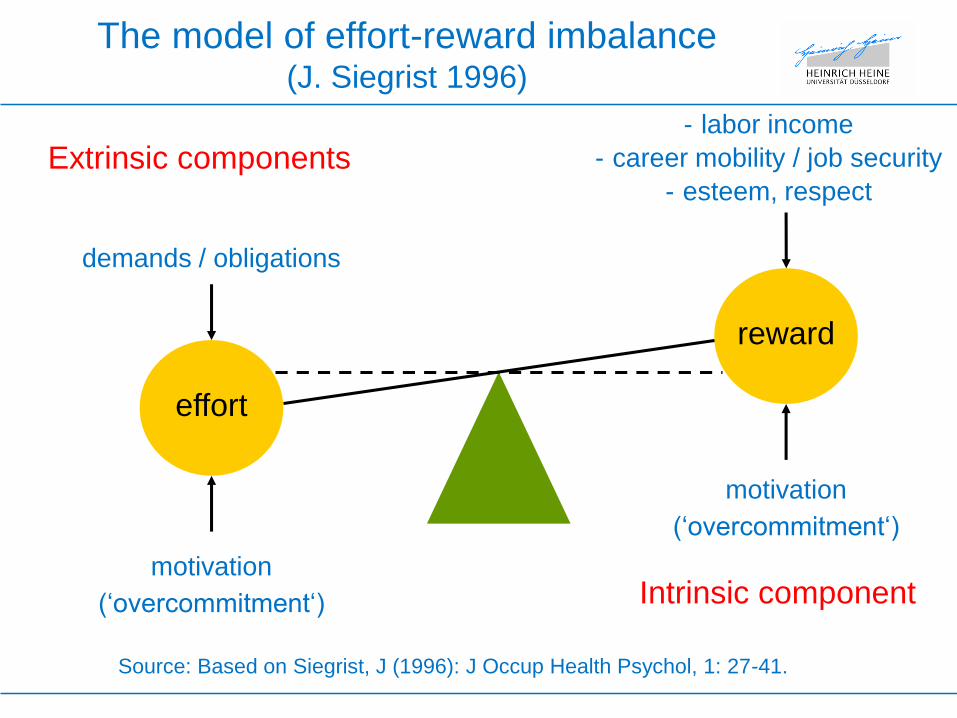
effort
reward
demands / obligations
- labor income
- career mobility / job security
- esteem, respect
motivation
(‘overcommitment‘)
motivation
(‘overcommitment‘)
Extrinsic components
Intrinsic component
The model of effort-reward imbalance (J. Siegrist 1996)
Source: Based on Siegrist, J (1996): J Occup Health Psychol, 1: 27-41.

• Procedural justicePerceptions of consistent, accurate, unbiased and
ethical rules of procedures
• Relational justicePerceptions of polite, fair interactions from
supervisors
• Distributive justicePerceptions of appropriate distribution of job tasks
and gains among employees
The Organizational Justice Model(J. Greenberg et al. 1982; M. Elovainio et al. 2002)

Relevant study design: Prospective observational cohort study
of working populations who are free from mental disorder at
baseline.
Study aim: Demonstrating elevated relative risks/ odds ratios of
mental disorder as a function of exposure to work stress
Additional evidence on pathways:
Experimental and ‘naturalistic’ studies linking work stress with
psychobiological markers related to disorder
Measuring work stress:
Psychometrically validated scales/ questionnaires
www.jcqcenter.org
www.uniklinik-duesseldorf.de/med-soziologie
Scientific evidence on associations with
mental health risks?

Social gradient of work stress
0
5
10
15
20
25
30
35
40
Effort-Reward Imbalance Low control
Perc
en
t h
igh
str
essed
Very low
Low
Medium
High
Very high
Source: Wahrendorf M et al. (2013) European Sociological Review 29: 792-802
The social gradient of work stress in the European
workforce (age 50-64): SHARE-study


Psychosocial stress at work and depressive symptoms: 13.128
employed men and women 50-64 yrs. from 17 countries in three
continents (SHARE, ELSA, HRS, JSTAR)
0
0,5
1
1,5
2
2,5
USA (N=1560) Europa (N=10342) Japan (N=1226)
ERI
Low control
Source: J. Siegrist et al (2012) Globalization and Health 8:27.
* *
*
* *

Stronger effect of work stress (effort-reward imbalance (ERI)) on
depression among workers with low socioeconomic positions
(SEP) (Denmark; N=1729)
n OR (%95 CI)
ERI low / SEP high 652 1 (Reference)
ERI low / SEP low 611 1,45 (0,72 -2,92)
ERI high / SEP high 313 1,26 (0,59 - 2,70)
ERI high / SEP low 153 2,43 (1,07 - 5,53)
Logistic regression analysis. Adjusted for age, sex, family status, health behavior,
sleep distiurbance, subkjective health and depression at baseline
Source: R Rugulies et al. (2013) Eur J Public Health 23: 415-420

Source: Juvani A et al. (2014): Scand J Work Environ Health, 40: 266-277.
Cumulative hazard curves of disability pension due to
depression by quartiles of work stress
effort-reward imbalance) in Finland (n =51.874)

Reduced fatigue and depression is associated with labour
market exit (GAZEL-study, France; N=14.104)
Source: Westerlund H et al (2010) BMJ 341:c6149.

Personal level: Stress prevention programs
Interpersonal level: Leadership training;
communication skills;
Structural level: Organizational/personnel
development (based on work stress models)
Job enrichment/ enlargement (autonomy, control, responsibility)
Skill utilization / active learning
Participation / team work and social support
Culture of recognition
Fair wages/ gain-sharing
Continued qualification/ promotion prospects
What can be done to reduce unhealthy work
and promote workers‘ health?

Variable
Demand
Control
Social support
Reward
Effort-reward imbal.
Work-rel. burnout
Means at t2 adj. for t0
experimental - control hospital p
11.9
70.0
23.7
31.2
1.0
43.2
12.6
68.7
23.0
30.2
1.1
48.3
.008
.051
.011
.003
.001
.003
Source: R. Bourbonnais et al. (2011), Occup Environ Med, 68: 479-486.
Organizational intervention in a Canadian hospital vs.
control hospital*
*36 month-follow-up, two Canadian hospitals, N=248 (intervention) vs. 240 (control
hospital) (ANCOVA, adj. for baseline values)

Source: T. Theorell et al. (2001), Psychosom Med, 63: 724-733.
Intervention group Control group
Baseline
390.4
6.2
After 1 year
345.2
6.1
Mean Cortisol
(nmol/l)
Mean decision
latitude
(range 2-8)
Interaction group X time: *p = .05, **p = .02
Baseline
387.2
6.0
After 1 year
391.3
5.7
**
*
Interpersonal level: Leadership training of managers
and stress hormone excretion in subordinates

Mean score of stressful work and extent of implementation of national
labour market integration policy (EU-funded DRIVERS Project, based
on SHARE data)
Source: Wahrendorf M, Siegrist J. (2014) BMC Public Health 14: 849

Odds ratios of depressive symptoms by work stress:
mitigation of effect by distinct labour policies?
Source: Lunau T. et al. (2013), BMC Public Health, doi:10.1186/1471-2458-13-1086
Based on
SHARE, HRS,
ELSA; n =
5650, m/w
aged 50-64.
13 countries

Conclusions
• Robust scientific evidence that unhealthy work (DC, ERI,
OJ) is associated with an almost twofold elevated
relative risk of poor mental health (depression).
• Overall, every fifth working person is exposed to
unhealthy work, with higher prevalence among those
with low SEP.
• These important human and economic costs can be
tackled by strengthening evidence-based prevention at
the level of companies and of national/international labor
and social policies.
»

Policy implications 1:
Organizational and personnel development
• Provide shared commitment from management and
employees
• Provide available expertise (e.g. occupational safety &
health)
• Monitor working conditions and employees‘ health, with
special emphasis on social inequalities
• Develop and implement programmes, invest in
improvements, consult models of best practice
• Ensure continuity, evaluate outcomes, build networks

Policy implications 2:
National/international initiatives
• Apply legal frameworks (national, international)
• Enforce fair work standards in trade contracts
• Promote voluntary agreements between employers and
trade unions
• Support social movements (e.g. EU: Corporate Social
Responsibility)
• Maintain and develop distinct national labor and social
policies
Welfare regimes securing basic social and economic protection,
access to health care, further education, etc.
