medicine in oregon - home | oregon medical association in oregon a publication of the oregon medical...
TRANSCRIPT

11740 SW 68th PkwyPortland, OR 97223Return Service Requested
Volume 2, Number 1 • Winter 09
Medicine in Oregon
A publication of the Oregon Medical Association Policy • Community • Practice
Now What?
Transitions: Looking Back, and Preparing to Move Forward
Member Survey Data Will Help OMA Chart the Future

Winter2009• 1

OMA Member Survey Data Will Help OMA
Figure 2:
Figure 4:
Figure 3:
Figure 5:
On Call A poem by Michael Wynn, DO
Back Page
Medicinein Oregon
Volume 2, Number 1 Winter 2009
Policy community Practice
Published quarterly by Oregon Medical Association 11740 SW 68th Pkwy, Ste 100Portland, OR 97223(503) 619-8000 • fax (503) 619-0609www.theOMA.org • [email protected]
Editorial Advisory BoardCarla McKelvey, Physician EditorMonica Wehby Peter BernardoNancy Boutin Evelyn FordMike Crew (of counsel)
OMA StaffJo Bryson Betsy Boyd-FlynnJennifer Nordgaard Reina O’Beck
SubmissionsWe welcome and encourage our members to contribute to Medicine in Oregon.
For more information, contact Betsy Boyd-Flynn at 503-619-8000 or [email protected]
Advertising & Design byLLM Publications, Inc.8201 SE 17th Ave, Portland OR 97202(503) 656-8013 • (800) 647-1511fax (503) 655-0778www.llm.comPresident | Linda PopeGraphic Design | Heather WhiteAdvertising Sales | John Garbett
Joseph Madigan
On the CoverIn the mid-19th century, thousands of Americans headed west-ward across the Plains to Oregon and California. Covered wagons were primar-ily used to transport goods. Since the wagons had no suspension and the roads were rough, many people pre-ferred to walk, unless they had horses to ride.
© 2009 by the Oregon Medical Association. All rights reserved. No part of this publication may be reproduced or transmitted in any form by any means, electronic or mechanical, including photocopy, recording, any information storage or retrieval system, without permission from the publisher.
10page
Now What?PLUS...One physician’s Adventure in Cyberspace
15page
The Technology Issue 6 FrOM ThE DESk OF JO BrySOn
OMA’s Take on Technology: Helping Members Make Sense of It
10 FEATurEThe Doctor is Online: Now What? By Betsy Boyd-Flynn
PluS One Physician’s Adventures in CyberspaceBy Betsy Boyd-Flynn
18 In ThE OFFICETechniques for Harmonizing Clinicians, Patients and the Electronic Health Record By Laurence Baker, PhD and Nan Robertson, RPh
20 ADvOCACy In FOCuSWhat E-Prescribing Can Do for Health CareYour Voice is NeededBy William Pierce, MD
22 On My MInDTwo Perspectives on Technology in Medicine By Evelyn Ford, M3 and Margaret Thompson, MD
25 In hOuSE COunSElTelemedicine: Real Promise for Oregon By Kelly Hagan, JD
Also Inside 4 FrOM ThE PrESIDEnT
Transitions: Looking Back, and Preparing to Move Forward
MEMBErShIP MATTErS5 New and reinstated members
8 Payment Advocacy Corner
9 Upcoming events
15 FEATurEMember Survey Data Will Help OMA Chart the FutureBy Joy Conklin and Jennifer Nordgaard
26 MEDICAl hISTOryMedicine and History in OregonBy Nancy S. Boutin, MD
Chart the Future

Winter2009• 3

As I write this, the OMA is experiencing a significant transition as our long-time Director of Government Affairs and most recently Associate Executive Director, Scott Gallant, prepares others to take on the cause of physicians and patients. His last day with the OMA is slated for Jan. 20, 2009. His career with us contains many lessons that ought to inform our future together.
Scott is recognized for his leadership in health care policy during some of the OMA’s most treacherous fights and monumental victories over a 28 year span. Not only is he respected as a force to be reckoned with in Oregon political circles, he is respected nationally in the world of national politics and policy. At AMA meetings and other national venues, when others discover I am from Oregon, invariably I am asked about Scott Gallant. When I acknowledge that, yes, I do indeed know Mr. Gallant quite well, I am regaled with colorful stories. He is a boundless source of information, knowledge, and energy, foreseeing problems and pitfalls others may overlook, finding solutions others have missed...always with the mission to guide the OMA through the legislative jungles of Salem and Washington, D.C.
When asked what he felt was the most significant transition in medicine during his nearly three decades of service, Scott identified the decline of a close medical community as the largest change over the years. “A uniform
sense of purpose and commitment, and a general belief that physicians should and could lead the state in health care reform or other major policy issues, has certainly changed,” he said.
He believes this change is due to the evolution of the societal approach to community and civic involvement, or perhaps a response by physicians coping with a world that has become more complex as the practice of medicine has become more complex. Regardless, this sense of disempowerment has had a profound impact on physicians, as evidenced by a growing schism between primary care and other medical specialties.
“The OMA has always approached issues on the basis that all physicians and patients do best when all boats rise,” notes Gallant. For example, during the severe recession of the mid-1980s, physicians took a leadership role in developing and passing the Oregon Health Plan, which was controversial at the time and in some respects is still a controversial approach to health care delivery.
Asked to pick out other career landmarks, Gallant said that Oregon physicians have been instrumental in so many key issues during his career that he found it hard to recall them all, but offered a few: Mandatory immunizations, confidentiality of patient records for AIDS patients, motorcycle helmet law, seat belt legislation, passage of the first tobacco
Monica Wehby, MD
Monica Wehby, MD, is president of the Oregon Medical Association. She is a pediatric neurosurgeon in Portland, and has been a member of OMA since 1997.
From the President
Transitionslooking Back, and Preparing to Move Forward Not only is Scott
Gallant respected as
a force to be reckoned
with in Oregon
political circles, he is
respected nationally in
the world of national
politics and policy.
4 •Medicine in Oregon
The naTion and The state face unprecedented times, as does the medical community, which grapples with major changes to the delivery and cost of health care, building over the last three decades. Health care
is facing significant challenges in the future, including payment reform, increasing adoption of electronic health records, electronic prescribing, the evolution of medical homes, coordinated care, and possibly broad-based federal and state health care reform. Historians tell us that in any transition, reflecting on the lessons of the past help to put the possibilities and opportunities for the future in perspective.

Winter2009• 5
tax (through an initiative) to fund the Oregon Health Plan, tax credits for rural medical practices, establishment of the Oregon Health Professionals Program, provision of state liability protection for health care personnel who treat patients during a state emergency, passage of a state and federal patient safety legislation, passage of mental health parity legislation, the patient protection act, the medical staff by-laws statutes, prompt pay legislation, liability reform, creation of the rural health association, the durable power of attorney statute, the living will statute, support for Ron Wyden’s Healthy Americans Act, creating the Wyden Workforce Report, battling innumerable federal and state reimbursement issues …..and that’s the short list.
“It seems a little stark that one’s professional experience can be summarized in a single paragraph,” Gallant mused, “but many of these issues have had a lasting impact on patients and physicians.” Physicians should be proud of the accomplishments that the OMA has and will accomplish on behalf of organized medicine and the patients they serve. Without a doubt, Scott’s efforts on behalf of the OMA have saved lives and improved care for Oregonians.
That spirit of involvement needs to continue. Physicians will play a critical role in any health reform effort. If the plans at the state or federal level don’t take into consideration the critical role
physicians play in the cost, delivery and quality of care patients receive they will have missed an opportunity for reform that will work and will be lasting for the benefit of patients.
Physician workforce issues are often overlooked as a key element for a successful reform plan. Unfortunately, policy makers have not been able to grasp the impact of the physician shortage on quality and access to care. At the same time, medicine has been diversifying into “medical silos,” it is extremely difficult to forge a consensus on major issues within the house of medicine.
As former Governor Kitzhaber has often said, the public and elected officials respect the opinion of medicine. Physicians can, should and will be successful advocates on issues large and small for all patients, regardless of their insurance status. The public and our colleagues expect no less. The future is very bright for the OMA, and presents many opportunities for those of you who become involved in the OMA just as we personally empower ourselves to make a difference in our own lives and that of our patients.
Despite all these challenges, I am convinced the future is very bright for the OMA, and presents many opportunities our members, just as we personally empower ourselves to make a difference in our own lives and that of our patients. Scott’s legacy has been to set a good example for us. We wish him well.
2008 oMa executive committeePresident | Monica Wehby, MDPresident-Elect | Peter Bernardo, MD Immediate Past President | klaus Martin, MDvice President | James hicks, MDSecretary-Treasurer | John Evans, III, MDSpeaker of the house | Carla Mckelvey, MD
vice Speaker | Mary McCarthy, MD
Member-at-large | William Pierce, MD
Member-at-large | Carlos Sanchez, MD
OMA Alliance President | Eva Germaine-Shimotakahara
Joining the circleOMA thanks those members who have paid their 2008 dues, and welcomes the following new members and those who have reinstated their membership with the OMA.
Michele N. Adamcak, DOHarry T. Adamo, MDJonathan S. Alexander, MDBeata J. Anasz-Kopecka, MDBrett M. Andres, MDFrancisco L. Arroyo, MDKatelyn Mae AtkinsThu H. Aung, MDKaryn Marie AustinA. Sharen AzarRobert P. Barlow, MDCarrie A. Baxter, PACharles L. Beck, MDRichard H. Bensimon, MDEmma BenzarAdam BlanchardMarkus Alexander BoinErin S. Bolken, PAMingying Y. Bonner, PA-CJames C. Borowiec, MDJames T. Boyd, MDPrasheeda BremjitValerie J. BrookeJeffery C. Brown, MDSara J. BubenikKim Lan Thi Bui, MDTeresa J. Buracchio, MDCharles Nicholes BuserStacy S. Caldwell, PA-CRobert J. Cantor, MDJessica R. CarlsonStacie L. Carney, MDEmily Hawkins CarterLauralyn B.
Carter-Meletich, DOAlpana Chandra, MDRenee Mclean Chang, MDAmmar ChangeziLynette ChenAndrea H. Chiavarini, MDBryan C. Chitwood, MDJames S. Chong, DOKatelyn Ann ClarkCameron C. Coffee, PAJessica E. Coffman, PAJoseph Anthony Colella, MDDavid M. Collins, MDChristopher M. Colville, MDNicole Marie ConradJohn Carl ConroyLindsay E. Cook, MDF. Michael Cornell, MDWalter Crittenden
Stephanie Erin CrockerTheresa-Huong T.T. Dang, PASonal B. Dave, MDJ. Salvador De La CruzChristopher Clement DentonSharon M. Dickinson, PA-CJohn P. Dohrman, MDJenna M. DonaldsonSheeten B. Doshi, MDNeal Bruce DouglasWendi K. Drummond, DOJohn W. Egar, MDDavid C. Emch, PA-CJustin Flores EstarisLauren E. FaricyNaomie FishmanJennifer E. Flythe, MDEric L. Foote, PARichard G. Foutch, DODavid Glenn FrazerTravis E. Fromwiller, MDKyle I. Fuchs, MDJames L. Gajewski, MDTeresa L. George, PANicole Y. Gesik, DOAndrew J. Gilchrist, MDAdam N. GlaserMark I. Golden, MDLeah Macke GordonCynthia S. Gulick, DOMelissa A. Hahn, MDStephen M. Hale, MDBirgitta Hamann, PAAmanda J.H. Hamilton, MDMegan L. Harless, PAKristine E. Harvey, MDAllan J. Hedges, Jr, MDJohn Thomas HeinemanAnna Lee HemphillJames R. Hills, MDKen K. Hirasaki, MDNazmul Hoque, MDThanh Mai HuynhWilliam P. Irvine, MDBadia Jabbour, MDRobert L. Jacques, MDMichael P. Jaczko, DOTricia T. James, MDTina Jenq, MDSunshine S. John, PA-CJeremiah O. JohnsonTerry L. Jones, PAHeather A. Kahn, MD

as ParT of oMa’s long-term strategic goals, we created the Technology Committee three years ago
and charged them to address OMA’s electronic connectivity with members and the public, provide advice regarding the new and emerging issues around the use of electronic health/medical records and evaluate various telecommunications and web products to enhance OMA communications.
With regard to electronic health/medical records, the committee assembled advice and information about EMRs and made it available to OMA members. The goal was not to recommend a particular system, but rather to provide criteria that members could use when selecting a system and that would enable them to make wise decisions and enhance patient care in their practices.
The committee purchased full access to an important website for independent research data on health care IT vendor performance. KLAS is an independent organization that obtains site user responses to help build reports about an electronic health record product thus allowing products to be evaluated alongside one another. Access to this database enables OMA to assist members in monitoring specific vendor performance that leads to system selection, contracting and ongoing relationships.
We continue to strive to find ways to improve how we do business and how we can best communicate with our members through using video conferencing, video streaming, webinars, and other electronic formats. We introduced handheld voting devices for the House of Delegates this year, and are addressing the topic of association membership in the age of social networks and what role that will play in the future of medicine.
Did you know that over 60 million US adults are now using social media
(social networks, blogs, streaming video, etc.) to interact and share their health experiences online? The impact social media is having on medicine is most notable in four areas:
� Patient social networks
� Social search
� Knowledge sources such as Wikipedia
� Physician online communities
Patient social networks are either all purpose communities, such as HealthCentral, MedHelp and RevolutionHealth, or disease focused, such as Patients Like Me (neuro-degenerative diseases and mood disorders), Relief Insite (chronic pain), DiabetesMine (diabetes), I’m Too Young for This (cancer patients from 15–40 years old) and Advanced Breast Cancer Community (offers both an information source and social network for people with breast cancer). Patients are using such communities, which are growing in popularity, to discuss their daily life struggles or to cope with rare diseases.
Online communities offer the benefits of support groups to those who might otherwise be unable or unwilling to participate, including family members and loved ones of the person diagnosed. Physician-patient interaction must be balanced with the continued innovation and growth in consumer-directed healthcare.
When using or recommending social media sites to patients, our member physicians need to focus on the following:
� Become familiar with assessing the quality of patient sites—one resource is a written a report called “The Wisdom of Patients: Health Care Meets Online Social Media” from the California Health Care Foundation’s newsletter, written by Jane Sarasohn-Kahn MHSA of THINK-Health.
oMa’s Take on Technologyhelping Members Make Sense of It We continue to strive
to find ways to improve
how we do business
and how we can
best communicate
with our members...
Joanne k. Bryson, CAE
From the Desk of Jo Bryson
6 •Medicine in Oregon

Winter2009• 7
Magazine submission guidelines
We welcome submissions from our members, including opinion pieces, essays about your practice, or visual art. We do not offer payment for published work, but can provide additional copies of the magazine in which your work appears.
If you are interested in writing but do not have a clear idea or a specific topic in mind, you may wish to contact a member of the editorial advisory board or the staff editor. They may be able to assign you a topic or make suggestions for content we are seeking for a particular issue.
Get a sense of what is planned by viewing the editorial calendar for the year, which is kept up to date on the OMA website at www.theOMA.org/MiO. Submission deadlines and tentative themes for each issue are as follows:
Mar. 5: Spring 2009 issue; Mental Health in OregonJune 5: Summer 2009 issue; Politics and Medicinesept. 5: Fall 2009 issue; Oregon’s Research Hub/Quality & Performance in Practicedec. 1: Winter 2010 issue; topic TBD
Send your submissions electronically to [email protected]. Written submissions should be sent in rich text format or MS Word 2003. Any accompanying photos or illustrations can be sent either on CD or via e-mail. Please note these must be high-resolution files, 300 dpi or higher. We have a 6MB size limitation on e-mail we can receive. Include a brief (25 words or fewer) biographical note, including your specialty, where you practice and (optionally) how long you have been a member of OMA.
Works of visual art can be submitted either via mailed CD or e-mail, or contact Betsy Boyd-Flynn to arrange an in-person meeting.
David H. Kane, MDBarbara L. Keller, MDRobert J. Kershaw, MDGeorge M. Khoury, MDAaron KilberEdsel U. Kim, MDRichard K. Kimani, MDJames D. Kippen, MDBrant Evan KirkCharles B.D.G. Knight, MDEdward J. Lairson, MDSummer R. Lam, MDKyle LambJames M. Leach, PA-CDenise A. Ledbetter, PATim H. Lee, MDMark Allen LundquistAnna Marie Q. Macasa, MDChristine L. Martin, MDElizabeth N. MartinKaitlin Stuart MasarieCarly Mauch, PA-CJonathan McBride, MDMatthew C. McClelland, MDNathaniel K. McCoyKatherine McLean, PA-CAlexandra J. McMenamin, PAKimberly MerschDorothy K. Miner, PA-CTyler MittelstaedtJerrod C. Mitzel, MDTrevor Joseph MoerkerkeKatherine L. J.
Molyneux, PA-CMichelle MonnieGregory A. Moore, MDBrian Blagdon MorganRobert James MorrisonAmy L. Mulcaster, DOMark Luis MunozChristopher M. MurphyEdward N. MurphyLaura K. Murphy, MDDevarshi Nath, MDLynne M. Nguyen, PAEric M. NordstromSarah L. Normandin, MDMike R. OakleyMigdalia E. OrdonezGene PaekAbby K. Parsons, MDDavid S. Partch, PA-CGlen R. Patrizio, MDMelissa PaulissenCharles L. Pederson, MDD. Ann Penaloza, MDMichael Keith PhelpsCristin A. Rettler, PA
Ronald L. Reynoso Hernandez, MD
Bryan A. Richardson, MDErin Rose RiekeDonald P. Robertson, DOKelly E. Robinson, PAIlan J.D. Rothman, MDBethany Tara SamuelsonJenny Marie SatterbergEvan T. Saulino, MDJustin Benjamin SearnsWilliam James SendersLoton ShippeyMark ShwayderGurmant P. Singh, MDMargaret V. Smithpeter, MDCaroline C. Smythe, MDAdam D. Soll, MDSusan K. Sparling, MDAleka Spurgeon-HeinriciAmy Ruth StarrAllison Michele SticklesElizabeth A. Strubel, PA-CYolanda B. Suarez, DOJoel M. Suckow, MDRandy A.
Sussmane-Stubbs, MDAtiq Syed, MDSusan I. Terran, PAChristopher Thoming, MDAshley Xuan-An TranJohn D. Tucker, MDRoberta N. Vandentop, PADaryl G. Vogel, MDTam T. VuongWendy Leigh WalkerChristopher N. Walton, MDAngela E. Watson, PA-CKari S. Wattenbarger, PA-CPhillip T. Weidner, DOH. Edwin Weih, PAMelissa Ashley WelkerAshton S.
Wickramasinghe, MDKirk WillettPatrick S. Williams, MDBradford J. Witman, PALily Jane WittichAnda Karleen B. Yangson, MDKeenan Elizabeth YanitRalph A. Yates, DOSteven Yeh, MDErik J. Young, MDMaggie K. Yu, MDLuai R. ZarourMarc A. Zenoniani, MDYong Zhu, MD
Membership information is available through Beth Cherry at (503) 619-8000 or [email protected].
� Provide patients with criteria for reviewing and selecting appropriate online patient support groups, as well as their potential risks and benefits
� Make sure to visit a website before recommending it; learn about the community and consider becoming a physician contributor
� Warn patients not to make medical decisions based on patient support group advice without input from their physician
Social networks provide patients with both amazing opportunities and new dangers. Physicians can help guide their patients to make wise decisions as they engage and interact with the online world.
To help our leadership better understand social networking and the impact it is having on associations, we have engaged Jeff DeCagna to address the Board of Trustees in January. Jeff is a chief
strategist and founder of Principled Innovation, LLC, located in Reston, Virginia and a member of The Center for Association Leadership board of directors. He recently spoke at the 2008 Annual Conference of the Oregon Society of Association Management about social networking. We hope his insight will help OMA as we continue to evolve the way we interact with our members, and the way our members interact with each other.
We continue to embrace the important role technology will play in the future of medicine, in part because technology has brought us to this point. The future of medicine is driven by technological advances that hope to improve health care, decrease administrative costs and enhance how we communicate with our members. Our ultimate goal is to stay ahead of the curve.

8 •Medicine in Oregon
Membership Matters
Payment advocacy cornerBy Reina O’Beck
“I was never aware that this OMA service existed and I recommend it to any physicians when they encounter insurance reimbursement issues. I appreciated their quick response and professionalism.” Chong Chang, MD, OMA Member
Medicine in Oregon will now feature a regular column exclusively related to education on physician payment issues.
It will also include real-life advocacy requests submitted by physicians to OMA’s payment advocacy department.
This issue of Medicine in Oregon features an advocacy request submitted by Chong Chang, MD, an
obstetrician with the Willamette Surgical Specialists, LLP. Dr. Chang contacted the OMA because of one of his contracted health plans was continually denying payment for an assistant surgeon on a procedure. Other health plans that he works with have paid for assistant surgeons on this particular procedure.
Dr. Chang submitted appeals for these denials, but the health plan continued to deny payment for the assistant surgeon. Not knowing what to do next, Dr. Chang contacted the Oregon insurance commission, who referred him to the OMA.
The payment advocacy staff consulted the Health Care Finance Committee, one of the OMA’s standing committees composed of physicians either in practice or serving as health plan medical directors, and asked them to review the case and provide feedback. The committee was tasked with deciding as to whether an assistant surgeon was medically necessary for the procedure in question.
After a thorough review of Dr. Chang’s operative and procedure report, the Health Care Finance Committee agreed that an assistant surgeon, in this case, should be allowed and therefore reimbursed. The OMA, on behalf of Dr. Chang, wrote a letter to the
health plan asking them to reconsider their payment denial for an assistant surgeon.
After a short period, the health plan did reconsider the denial and paid the assistant surgeon. Dr. Chang and his office believe that the OMA’s input was the main reason for the positive outcome.
The OMA receives frequent requests from physicians and their staff to resolve payment matters on their behalf. These matters range from claims not being paid in a timely manner, queries about coding, or other more specific matters, such as the above scenario.
If you are experiencing payment, customer service or other issues in working with Medicare, Medicaid, or a commercial health insurance payer, the OMA is available to work with private and public payers to work towards resolving these matters on your behalf.
Submit an advocacy request form, now available online, so we can begin to assist you today. If you need to send Protected Health Information for further documentation, please complete, sign and fax a Business Associate Agreement. To access advocacy request materials, visit www.theOMA.org/advocacyrequest.
For further information on this member service, contact [email protected] or call (503) 619-8000.

Winter2009• 9
uPcoMing eventsnon-oMa eventsLane county Medical society Monthly dinner Meeting
Feb. 3, March 3, April 7; 6 pmHilton Eugene & Conference Center
oregon academy of otolaryngology head and neck surgery, inc. Mid-Winter Meeting
Feb. 13–15, Timberline Lodge
american Lung association of oregon annual chest disease conferenceVisit www.lungoregon.org/ots/cdc.html for more information
Feb. 19–22, Sunriver
oregon Pathologists association dinner/Membership Business Mtg.
Feb. 27; 6:30 pm, OMA Headquarters
oregon Pathologists association scientific seminar
Feb. 28; 9:00 amSt. Vincent Medical Center Souther AuditoriumPortland
oregon academy of family Physicians—advanced Life support in obstetrics (aLso)Visit www.oafp.org for more information
March 6–7, Klamath Falls
oregon Psychiatric association Winter conferenceVisit www.orpsych.org/calendar.htm for more information
March 13–14Crowne Plaza Hotel Portland / Lake Oswego
oregon academy of ophthalmology 2009 Post graduate conventionVisit www.oregoneyephysicians.org for more information
March 13-14 World Forestry Center
oregon section american college of obstetricians and gynecologists (acog) annual clinical MeetingVisit www.acog.org/acog_sections/dist_web.cfm?recno=29 for more information
April 3–5, Sunriver
For more information on OMA workshops, including locations, visit www.theOMA.org/workshops.
audio conference series upcoming government regulations including hIPAA and red Flag rulesVisit www.theOMA.org/hipaaseries to register.
Feb. 10, 17, 24, March 12; 10–11:30 am
coding seriesApril 28–30: OMA Headquarters
hiPaa “how To’s” seriesApril 8: OMA Headquarters
April 17: Bend
April 23: Medford
April 24: Eugene
May 5: OMA Headquarters
Medical collections WorkshopMarch 3; 1–5 pm: OMA Headquarters
March 17; 1–5 pm: Eugene
April 7; 1–5 pm: Salem
April 21; 8:30 am–12:30 pm: Medford
April 22; 8:30 am–12:30 pm: Roseburg
Practice Management seriesMarch 10–11: OMA Headquarters
April 15–16: Bend
workshops
oMa alliance Winter sessionContact Pat Webster at [email protected] for more information.
Feb. 18Salem
oMa executive committee MeetingFeb. 19Salem
day at the capitolVisit www.theOMA.org for more information or to register.
Feb. 19Salem
deadline for oMef grant applicationsVisit www.theOMA.org/omef for more information.
Mar. 25
deadline for oMef Linn Benton scholarship applicationVisit www.theOMA.org/omef for more information.
April 1
oMa/oMaa annual house of delegates
April 24–26Hilton Eugene & Conference Center
oregon Medical education foundation Board Meeting
April 25Eugene
OMA headquarters11740 SW 68th Pkwy, Ste 100, Portland(503) 619-8000 • www.theOMA.org

10 •Medicine in Oregon
There is a parTner in your pracTice that may not have been invited. This new partner is changing the way you relate to your patients, and may be making
significant demands on your time. Who is this upstart? The Internet. It isn’t new, but the way patients, physicians and other health care providers are using it is changing.
Contrary to what many of us might think about the way time-crunched doctors behave online, data from sources as diverse as the AMA and the market research firm Manhattan Research are demonstrating that growing numbers of physicians are online for more than just e-mail. In 2007, the AMA partnered with Sermo, a private online community for physicians, and created multiple groups on the public social networking site Facebook for its younger member demographics. Manhattan Research’s 2007 study found that over 200,000 physicians are participating in
“social media,” whether posting professional content or participating in online communities. And that’s just one part of the picture. (Manhattan Research, 2007)
The same study from Manhattan Research showed that over 500,000 physicians are using video online for various purposes, and over 100,000 are downloading audio files and podcasts. Physicians authoring blogs were not the youngest demographic—in fact they were more often older, more experienced and with “something to say,” while the younger
physicians were more likely to consume information from those sources. (2007)
So if this gives us a sense of how physicians are using the Internet, it should be no surprise that patients are using it, too. In the Information Age, many sources are clambering for your patients’ attention and information, whether it be health information, or more disturbingly, information about their physicians and health care providers.
:\ What is out There about you?Increasingly, physicians are grappling with how their reputations are shaped by what appears online.
David Rothman, a medical librarian for a hospital in Rochester New York, has a highly-regarded blog, www.Davidrothman.net, where he has been discussing medical informatics since 2006. Recent topics on his blog include exploring “infodemiology” projects like “Google Flu,” which analyzes search statistics of users nationwide to track where instances of flu are appearing.
He is well-versed in how the Internet impacts physicians and patient access to information. At the 2008 AMA Medical Communicators conference, Rothman talked about what physicians can—and can’t—do to manage their online reputations.
Now What?By Betsy Boyd-Flynn
and reina o’Beck

Winter2009• 11
Rothman talks about two aspects physicians should consider: the degree to which it’s important for a physician practice or clinic to have a presence on the web for marketing purposes, and the work physicians need to do to manage their reputations generated by patients through sites like Angie’s list, which lists physicians as a “service” and allows members to rank them in similar ways to how they rank plumbers. When patients without identities or restrictions are allowed to post opinions online, doctors can learn—too late—that misinformation is spreading about them virally, and it may be far more damaging than old-fashioned gossip.
Two articles published in 2007 in Medical Economics offered shared experience and advice to physicians who found themselves in such a situation. Contacting the administrators of a web site where inaccurate or slanderous information is posted is the first course. Asking your lawyer to draft a cease-and-desist letter can be a next step, and some physicians may even want to escalate to a lawsuit if the situation is grave enough. (Meyer, 2007; Rice, 2007)
But with physicians already so busy, how can they add the task of tracking every online mention of their name or practice to their to-do list? It could be a full-time job for a staff member to root out and quash any damaging or inaccurate references about physicians across the Internet, especially when many sources invite inflammatory comments as a way to drive drama and site traffic.
Rothman suggests that even asking that question is the wrong place to start. “The question is: How did it come to be that the first search engine result is negative?” What you can do, and really all most physicians should try to do, is make sure the first result a patient sees when he or she searches for you in Google is accurate, reliable information you control, that you, or someone you paid, created.
Although building your online presence can be time-consuming, it is a much more manageable task (see sidebar: “One Physician’s Adventures in Cyberspace”) than combating negative or inaccurate information. The first place to start is to make certain you have a website, though it doesn’t need to be very complex. Rothman suggests it needs to do the following “list all practice participants, offer users dynamic directions to get there, and provide basic biographical information, including major publication links.”
Once you build the site, you still have a marketing job ahead of you to make sure people can find it, and find it first. For this, you may want to call in an expert in what’s called search engine optimization—a process of creating your pages so that they include the search terms and technical items search engines are looking for. You can study this yourself, or consider whether hiring a company or contractor is a
good idea. Whatever you do, Rothman says, make sure you get references for whoever you work with. Achieving good search engine rankings can be done in a lot of ways, and not all of them are legitimate.
:\ new space, old BehaviorRothman’s key message is that what patients are doing online is not new, it’s just an evolution of how they have always behaved. Patients have always talked to their friends and neighbors to offer referrals to physicians they love, and cautions about physicians they don’t. “People have always used networks, and this is a new way of doing that,” says Rothman. “Doctors are accustomed to the idea of the human-to-human grapevine—it’s just harder for them to see that it’s moved online.”
Eventually, says Rothman, search algorithms will be refined to include deep volumes of data that match patients with physicians along many dimensions, not just location or specialty, and it will happen through sites with multiple purposes, like Craigslist or Facebook. The challenge for the companies who want to get into this business will be ensuring they are a trusted source of information. The good news is those companies will need the cooperation of physicians in order to achieve that trust.
:\ online payer rankings are coming
The trend to place physician practice data online for public access is inexorable. The OMA has been working with several insurers already to help shape the profiling process, and will be promoting legislation in the 2009 session so as to place some parameters on what those ranking programs will do. Joy Conklin, OMA’s Director of Socioeconomic Affairs, says the need for the legislation is quite clear.
“We know of cases where the data is wrong, or a physician’s identity is wrong in the ranking system,” says Conklin. OMA’s legislation stipulates that the data collected and published will be statistically valid; in order for a data point to be tracked and made public, a physician must have a sufficient number of patients for whom that data applies. Importantly, the law also provides that physicians will have an opportunity to review their data and correct errors before it is made public.
Also critical, the legislation stipulates that patients will be informed about how the data is acquired and how they
When patients without identities or restrictions are allowed to post opinions online, doctors can learn—too late—that misinformation is spreading about them virally

should interpret it. “Patient usage of this kind of data is low at this point, but it will grow over time,” says Conklin.
“Right now, profiling is based on claims data rather than clinical data; as more physicians put EMRs into place, accuracy of these systems will improve. Until then, the parameters in the bill will help ensure patients get data that makes sense, and physicians aren’t impacted by inaccurate information.”
:\ Treating the “Worried Well”According to the Pew Internet & American Life project’s research on Internet technology and medicine, 80% of patients are looking for health information online.
One of the people who hopes to help your patients come to the exam room better informed is Ash Damle, CEO of www.Medgle.com, a health information site where patients can enter symptoms and other data anonymously—by body part, match to an image, age, gender, duration of condition, and more. Through a powerful algorithm that sorts the queries, patients are presented with a list of possibilities to discuss with their doctor. It’s not meant to replace a physician, but rather to help patients decide whether to seek out medical care, and provide them with a starting point for a conversation with a clinician.
MiO:\ Compared to most physicians, would you describe yourself as technically savvy?Dr. Miller:\ Well, I have structured my practice so that I have the ability to incorporate technology into it. I take an integrative medicine approach, and in that respect I do things differently than most physicians do. Part of the integrative approach is accepting the Internet into my practice. Patients will often e-mail me their blood pressure results, and I really like it. It’s a secure Internet channel for them, and sometimes it’s much easier for me to answer emails at the end of the day than try to return phone calls. By and large, patients don’t abuse that access. The patients I see are people who are interested in their health—they e-mail me information that’s important.
MiO:\ how are you able to make time for connecting with your patients in this way?
I started this practice about three years ago because I didn’t like 10-minute visits. So I stopped taking
insurance, and opted out of Medicare. I spend one and a half hours with new patients, and a half-hour follow up. Once I decide on a course of treatment, I present them with a superbill, and then they bill their insurance.
MiO:\ What do you do when people come in with printouts from the Internet?
I have the time to talk to them about it—if I only had 10 minutes, I admit it would bother me. When a new patient comes in, I do a comprehensive history and physical, and we talk about what I think will help them, then we talk about what they’re willing to do. Some people are more comfortable with herbal treatments, some with traditional, and they often get their treatment information from the Internet. Most of it is familiar, and sometimes I learn from them, but if I’m in with a patient and I want to look up something online, I do it with them there and we discuss it together.
When they self-diagnose, they’re right about 60% of the time. I believe what we learn in medical school is true—99% of what’s wrong with a person is in their history. The way I’ve set things up, I have time to explore it with them.
MiO:\ how else are you using the Internet to connect with your patients?
I am a health expert for a couple of websites: www.lifescripts.com and www.tbd.com. For many of us in medicine who want to make sure people are doing the right things, writing online is a great way to educate people and keep them from doing the wrong things. I answer questions, and I get a great sense of what people are learning about and hearing.
We have created a blog for our book because we wanted to distribute the most up-to-date information possible, so we created the website, and that way readers can stay updated with the
one physician’s adventures in cyberspaceBy Betsy Boyd-Flynn
The Doct
or is
on line,
cont.
An MIT graduate with double degrees in math, electrical engineering and computer science, Damle attended the AMA’s Medical Communicators conference in April 2008 and discussed with attendees the way a user-driven search like his can help improve, rather than disrupt, the physician-patient relationship.
“If a patient can come into a doctor visit with the most likely causes of their problem, and understand what they might be, the tone of that first patient visit can change for the better,” says Damle. Well-sourced online information, he continued, can help patients feel like “a participant in their care, and more likely to follow through on what they need to do.”
He suggests physicians look at the Internet as a partner, and see the benefits and risks in that. “In the end, the physician is hoping for the best outcome for the patient, in the most efficient manner possible. Through judicious use of the Internet, they really can enable their patients to be more effective and improve communication and connection with their patients.”
Indeed, the possibility is that increasing physician engagement with the Internet can improve health care more broadly. Susannah Fox, the Pew researcher who authored the latest study about “e-patients,” published in October 2008, suggested at a conference that experts agree that “engaging large numbers of providers in the world of

online communication with and between patients about health issues is the best way…to craft a new model of higher quality medical care.” (Fox, 2008) That model right now includes mostly white, college-educated adults, and that’s a problem for rural and minority populations who are already underserved.
While skepticism about health information available on the Internet is high, perhaps especially among physicians, Fox’s research suggests that the number of patients who report bad outcomes due to information gathered online is actually quite low—just 3%. Literature reviews suggest similar low instances of problems. But for certain inflammatory issues, like the disproved yet widely-touted association of autism and vaccines, the Internet can prove a springboard for wider-spread controversy that can potentially harm public health. All the more reason for physicians to be online providing credible information.
Rothman puts it this way: “Having a blog is brilliant because it gives physicians a human voice. People respond to individuals much better than they respond to credentials.”
:\ What’s in the future?Increasingly, the Internet is becoming user-created and controlled, and access to it will be ever more integrated in daily life. The volume of information is likely to explode,
and physicians will need to reckon with the impacts on their practice if they are to thrive.
Aside from helping physicians take better care of their patients, the technology might possibly expand to people who don’t have access right now. Fox, the Pew researcher, sees the expansion of Internet usage on cell phones and mobile devices as one way the technology gap between whites and non-whites can be bridged, allowing many more people to have access to the health information on the Internet. Damle sees the potential for the marriage of television and Internet to bridge that same gap, and points to the growth of technology in case management as a way to reduce costs and ease the burden on an overtaxed health care system. “Necessity is the mother of invention,” says Damle, “and there is a lot of necessity right now.”
references
Fox, S. (2008) Recruit doctors. Let e-patients lead. Go mobile. Presented by Pew Internet & American Life Project at the Health 2.0 conference in San Diego, CA. Retrieved on Dec. 17, 2008 from www.pewinternet.org/pdfs/Fox_Health_March_2008.pdf
Manhattan Research. (2007). Physicians and the web 2.0: Five things you should know about the evolving online landscape. Retrieved on Dec. 17, 2008 from www.manhattanresearch.com/files/PRESS/Physicians_and_Web_2.0_from_Manhattan_Research.pdf.
Meyer, C. (2007) My web rating: oh no! Medical Economics, 84(19), 51, 55
Rice, B. (2007) Trashed on the web? Now what? Medical Economics 84(1), 32-4, 36-7
newest information. It’s impossible to be current when you publish a book, but the blog extends the life of the information.
I believe the Internet and technology will be a growing part of practice—it will just be normal. The people younger than us are used to this. iPhones and texting are part of life for them; interacting with their physicians this way will just be normal.
MiO:\ What surprises you about how you’re using the Internet these days?
I’m surprised I am on a laptop all the time. Years ago, people would tell me we’d have palm-sized computers, and I never thought I would be into it. Now, I have a laptop in my exam room. I have an
EMR and type all my own notes and generate my own superbills with it.
MiO:\ What would you say to physicians who are interested in getting into this way of communicating?
Start small. Go in with a positive attitude — I wouldn’t go in if I did not have a positive attitude about the Internet. You might start with a website for your practice, and post weekly tips. Before you know it, you have pages of tips, and that’s good. It’s essential to make sure your e-mail is secure, of course. Physicians have to go with their own comfort level. I look at it as a way to be creative in medicine, and many of us need to be. I’ve enjoyed finding different ways to get my message across and
have fun. The bottom line is, if you don’t like the Internet, don’t do it.
MiO:\ Do you feel like technology can help improve health literacy?
I think physicians should use technology to educate patients, but tell them not to count on it for everything, and give them simple ground rules. I tell my patients “Don’t count on me to catch this every day. Don’t e-mail me that you’re having a heart attack.” But using the Internet for simple things like tracking blood pressure or answer quick questions will save them a lot of time in the end—you can answer that at any time—even while you’re watching TV.
Robin Miller, MD is a family physician in private practice in Medford, Oregon who understands the Internet’s capacity to shape her practice and her other professional ventures. Recently, she and Janet Horn, MD, co-authored a book called The Smart Woman’s Guide to Midlife and Beyond. Medicine in Oregon spoke to her to discuss her experiences using technology to connect with her patients and the public. Dr. Miller can be reached at [email protected].

14 •Medicine in Oregon

A recurrent theme among these younger physicians is the need to find balance between their professional and personal lives. OMA is also examining ways to balance the needs of our “core” members who have been in practice for many years, with the expectations and perspectives of physicians who have recently graduated and are interested in a new or different mode of practice.
OMA’s committees, leaders and staff are using the information obtained in the survey to develop and refine programs and services that will most effectively serve the needs of our members in the coming year and beyond. The data highlighted here gives an overview of what members value, how they view OMA’s organizational performance and future issues of concern.
Membership We asked members to provide information regarding their participation in the OMA and other professional organizations.
In response to an open-ended question, one-third of members indicated they are a member of the OMA because it is the “thing to do/to support organized medicine”. Other reasons given, in descending order, were as follows:
� Advocacy/political support (30.2%)
� CNA/malpractice insurance (25%)
� Information/keeping up on issues (12.6%)
� Member benefits (10.3%)
� Employer pays or requires it (7.5%)
� Advice/support on medical-legal/practice issues (5.6%)
Advocacy remains a primary reason physicians belong to the association as reported by one third of respondents. One quarter cited the need to belong to OMA in order to be eligible for CNA Insurance. Moving forward, a top priority for the association will be to identify and communicate the value of OMA membership in a meaningful way to all members.
According to the survey, less than a quarter of OMA’s members under 40 reported that joining OMA was “the thing to do.” Advocacy and political support ranked highest among members 49 or younger. An indication of the volunteer time and resources younger physicians have to devote to organized medicine may well depend on family obligations, a greater awareness of social responsibility, and the fact that as more physicians are employed, they may receive benefits and resources through their employer that have traditionally been provided by the state medical association.
By Joy Conklin and Jennifer Nordgaard
In early 2008, OMa conducted an extensive survey of all active, active-limited and active first-
year members in order to gather information about its members, how they practice, and their opinions regarding OMA programs, services and the profession of medicine. A total of 4,934 questionnaires were mailed, with 1,057 completed and returned. A comprehensive membership survey of this nature had not been conducted in nearly a decade. The demographics of respondents generally reflected the overall demographic make-up of OMA’s membership.
As noted in previous surveys, OMA’s members continue to age along with the overall physician population. Two-thirds of our members are age 50 and older and about 60 percent of members have been in practice for more than 20 years. As the OMA considers products and services that benefit members, we also look at trends in medicine and how to respond to these changes.
OMA has fewer young physician members (age 45 and younger), more members practicing in groups, and a larger number of employed physicians than we did a decade ago. Additionally, the percentage of male to female physician members has remained constant, even though there are a greater percentage of females in medical school and entering the physician workforce.
About one-fourth of OMA members consider themselves employed. Almost half of our current members under 40 indicated that they are employed.
Chart the Future Member Survey Data Will Help OMA
Winter2009• 15

Members were asked to rate various organizations on a 5-point scale of 1 = no value to 5 = great value. National specialty societies received the highest average rating (4.1%). OMA was second with an average rating of 3.6%, followed by state specialty society and primary hospital medical staff (both rated at 3.2%), and then county medical society (2.7%) followed by AMA with an average rating of 2.6 (see Figure 1). More than 60 percent of respondents rated OMA as a great or good value.
These ratings do not differ from the 1999 survey.
Organizational PerformanceWe asked members to provide us with ratings of our various organizational components.
Members rated OMA’s success in accomplishing various tasks on a 4-point scale (see Figure 2). The average ratings were as follows.
� Manage OMA’s business affairs effectively – 3.1%
� Act as a wise steward of OMA resources – 3.1%
� Provide leadership for the profession – 3%
� Protect and strengthen the viability of medical practices in Oregon – 2.9%
� Enhance the unified voice of Oregon medicine – 2.9%
� Ensure success in legislative and regulatory activities to improve the environment in which physicians practice – 2.8%
A large number of physicians felt that OMA was successful or very successful in providing leadership to the medical profession, as well as managing OMA’s business affairs effectively and acting as a wise steward of OMA resources. This is important information as Oregon and the rest of the country face hard economic times and a critical shortage of physicians and other medical professionals. OMA is poised to continue its leadership role in helping
physicians maintain successful practices through this challenging climate.
Members were also asked to identify their level of agreement with several selected statements (see Figure 3). The average ratings on a 4-point scale were as follows.
� OMA is an influential player in the state health care arena – 3.0%
� OMA understands the needs of most Oregon physicians – 2.8%
� OMA’s policies are generally consistent with my beliefs – 2.8%
� OMA is an effective community partner – 2.8%
� My views and opinions can influence OMA’s decision making process – 2.5%
� OMA is an influential player in the national health care arena – 2.3%
Though this question was phrased differently in the 1999 membership survey, comparison data shows that fewer members now feel their views and opinions influence OMA’s decision making process than it has in the past. Physicians do, however, continue to view OMA as an influential player in the state health arena.
Figure 1 Value of Organizations
Figure 1:
Figure 2:
Figure 2 Success in accomplishing Tasks
Figure 3 agreement with Statements
Figure 3:
Chart the Future Cont.
16 •Medicine in Oregon
No Value
Little Value
Some Value
Good Value
Great Value
American Medical Association
Oregon Medical Association
County medical society
National specialty society
State specialty society
Primary hospital medical staff
Local IPA
0% 20% 40% 60% 80% 100%
0% 20% 40% 60% 80% 100%
0% 20% 40% 60% 80% 100%
0=No Opinion
1=Very Unsuccessful
2=Unsuccessful
3=Successful
4=Very Successful
0=No Opinion
1=Strongly Disagree
2=Disagree
3=Agree
4=Strongly Agree
Protect/strengthen the viability of practices
Success in legislative and regulatory activities
Provide leadership for the profession
Enhance unified voice of Oregon medicine
Manage OMA’s business affairs effectively
Act as a wise steward of OMA resources
My views/opinions can influence OMAUnderstands needs of physicians
Policies consistent with my beliefsInfluential player in state health care
Influential player in national health careEffective community partner
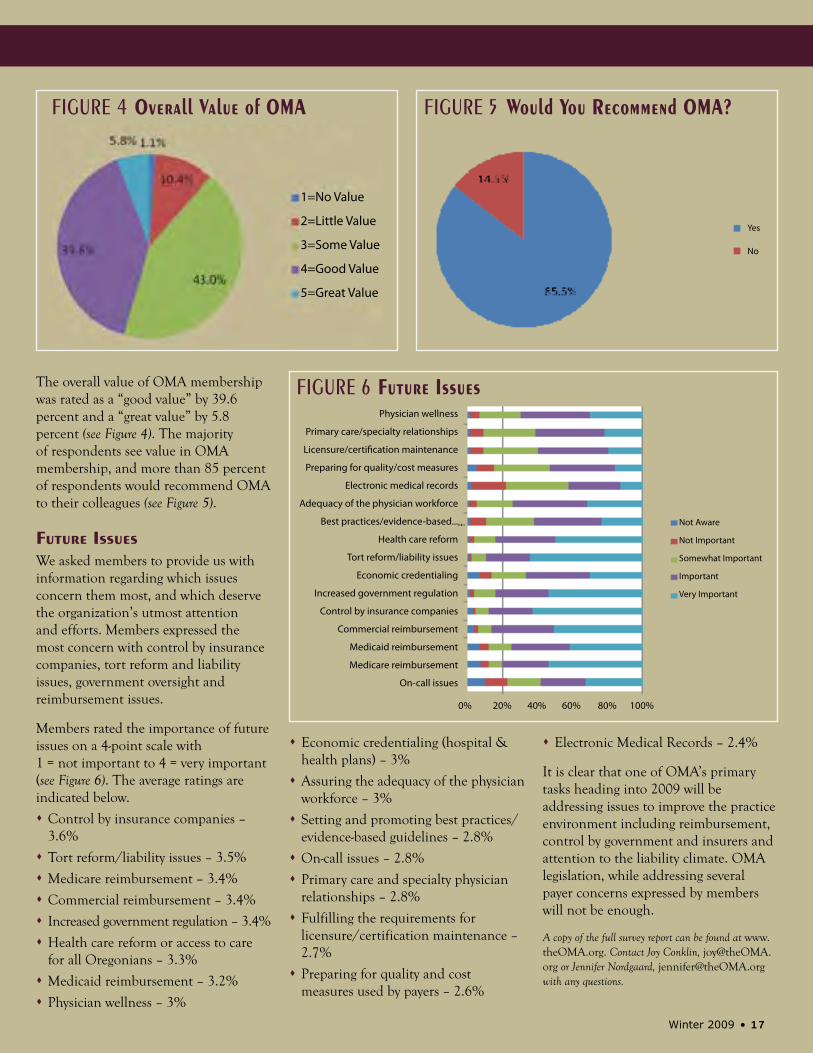
The overall value of OMA membership was rated as a “good value” by 39.6 percent and a “great value” by 5.8 percent (see Figure 4). The majority of respondents see value in OMA membership, and more than 85 percent of respondents would recommend OMA to their colleagues (see Figure 5).
Future IssuesWe asked members to provide us with information regarding which issues concern them most, and which deserve the organization’s utmost attention and efforts. Members expressed the most concern with control by insurance companies, tort reform and liability issues, government oversight and reimbursement issues.
Members rated the importance of future issues on a 4-point scale with 1 = not important to 4 = very important (see Figure 6). The average ratings are indicated below.
� Control by insurance companies – 3.6%
� Tort reform/liability issues – 3.5%
� Medicare reimbursement – 3.4%
� Commercial reimbursement – 3.4%
� Increased government regulation – 3.4%
� Health care reform or access to care for all Oregonians – 3.3%
� Medicaid reimbursement – 3.2%
� Physician wellness – 3%
Figure 6 Future Issues
� Economic credentialing (hospital & health plans) – 3%
� Assuring the adequacy of the physician workforce – 3%
� Setting and promoting best practices/evidence-based guidelines – 2.8%
� On-call issues – 2.8%
� Primary care and specialty physician relationships – 2.8%
� Fulfilling the requirements for licensure/certification maintenance – 2.7%
� Preparing for quality and cost measures used by payers – 2.6%
� Electronic Medical Records – 2.4%
It is clear that one of OMA’s primary tasks heading into 2009 will be addressing issues to improve the practice environment including reimbursement, control by government and insurers and attention to the liability climate. OMA legislation, while addressing several payer concerns expressed by members will not be enough.
A copy of the full survey report can be found at www.theOMA.org. Contact Joy Conklin, [email protected] or Jennifer Nordgaard, [email protected] with any questions.
Figure 4 Overall Value of OMa
Figure 4:
Winter2009• 17
Figure 5 Would you recommend OMa?
Figure 5:
Not Aware
Not Important
Somewhat Important
Important
Very Important
1=No Value
2=Little Value
3=Some Value
4=Good Value
5=Great Value
Yes
No
Physician wellness
Primary care/specialty relationships
Licensure/certification maintenance
Preparing for quality/cost measures
Electronic medical records
Adequacy of the physician workforce
Best practices/evidence-based...
Health care reform
Tort reform/liability issues
Economic credentialing
Increased government regulation
Control by insurance companies
Commercial reimbursement
Medicaid reimbursement
Medicare reimbursement
On-call issues
0% 20% 40% 60% 80% 100%

18 •Medicine in Oregon
There are Three Barriers to electronic health record (EHR) adoption by physicians
(DesRoches, et al, 2008): cost, concern about reduced productivity, and concern that the patient-physician relationship cannot be maintained if a computer is introduced into the exam room experience. Improving patient satisfaction with health care, enhancing the physician-patient relationship, and supporting clinician adoption of the EHR can be achieved through the use of targeted communication skills and EHR techniques. In the current economic crisis, when margins for medical practices are shrinking, a smooth transition to an EHR is increasingly important.
The EHR will soon be a reality for most doctors, nurses, physician assistants and all clinicians who interact with patients. Currently over 50% of clinicians in Oregon use an EHR every day, when seeing their patients. The EHR was a feature of both major presidential candidates’ health care reform packages. Pay for performance and
Techniques for harmonizing Clinicians, Patients,
and the Electronic health recordBy Laurence Baker, PhD and Nan Robertson, RPh
In the Office
The clinician should make eye contact with the patient every 30–60 seconds.
M U S EMake a personal connection at the beginning of each visit,
Understand the patient’s reasons for the visit and their priority,
Sit, see, and share the screen with the patient,
Enlist your patients as partners in their care.
increases in reimbursement rates by the Center for Medicare and Medicaid Services for e-prescribing are programs on the horizon that will depend on EHR adoption.
Despite these incentives, some clinicians are reluctant to use an EHR, even if their organization has adopted one. One of the most frequently cited reasons for avoiding the EHR is concern that using the EHR during the patient encounter will interfere with the clinician patient relationship (Linder, et al, 2006). Both clinician adoption of the EHR and patient satisfaction can be achieved with the application of communication skills summarized in the MUSE model. Research demonstrates that patients are more satisfied with their physician when computerized information is shared with them during the visit (Hsu, et al, 2005).
MUSE reminds us to think of four areas of the clinician-patient relationship:
� Make a personal connection at the beginning of each visit,
� Understand the patient’s reasons for the visit and their priority,
� Sit, see, and share the screen with the patient,
� Enlist your patients as partners in their care.
Making a personal connection involves a warm greeting, introducing yourself while making eye contact, introducing
the EHR to the patient, acknowledging the patient’s companions and negotiating confidentiality, and using electronic information (e.g., recent appointments, allergies, hobbies, etc.) to indicate you know the patient.
Understanding the patient’s reasons for the visit involves actively collaborating with the patient to establish the agenda for the visit and asking the patient the most important thing they want to get from the visit.
Sitting down while you work with the patient and the EHR and turning the screen so that both you and the patient can see the screen is key to both involving the patient in their care and efficiently using time. Health data, such as blood sugars, can be graphically displayed and shared with the patient.

Winter2009• 19
The EHR is a powerful tool for enlisting the patient as a partner in care. When sharing health data, ask the patient what their thoughts are about the meaning of the data for their health. When pharmacy screens provide you with choices, invite the patient to make these choices with you.
Sharing the screen is one of the most powerful things a clinician can do. Consider positioning the EHR screen and the patient so that the three of you form a “MUSE Triangle.” Seated in the triangle, the clinician can use the EHR and enter information while the patient sees the screen. The patient can also see the clinicians’ front torso, even though the clinician’s eyes may be gazing at the screen. The clinician should make eye contact with the patient every 30–60 seconds. Pause and make eye contact whenever the
patient discloses some emotional information. Much of the documentation can be done while the patient is in the room. Simply ask, “I want to make notes of our visit in your record. Would you like to stay and sit with me while I do that?”
While the EHR may present new challenges for clinicians, using the MUSE techniques can support a strong and satisfying relationship for both patients and clinicians.
Laurence Baker, PhD is a Senior Consultant with The Robertson Group LLC. He can be reached at [email protected]. Nan Robertson, RPh, is the Principal at The Robertson Group LLC. She can be reached at [email protected].
referencesDesRoches CM, et al, Electronic health records in ambulatory
care – A national survey of physicians. N Engl J Med; 2008; 359: 50-60.
Linder JA, Schnipper JL, Tsurikova R, Melnikas AJ, Volk LA, Middleton B. Barriers to electronic health record use during patient visits. AMIA Annu Symp Proc. 2006; 499-503.
Hsu J, Huang J, Fung V, Robertson N, Jimison H, Frankel R. Health information technology and physician-patient interactions: impact of computers on communication during outpatient primary care visits. J Am Med Inform Assoc. 2005 Jul-Aug;12(4):474-80. Epub 2005 Mar 31.

20 •Medicine in Oregon
What ‘E-PrESCrIBInG’ Can Do for health Care
Advocacy in Focus
Much of The focus following medicine’s huge victory last summer regarding Medicare
physician payments centered on steep cuts that were replaced by a continuation of a 0.5 percent update through 2008 and an additional 1.1 percent update for 2009. One aspect of the Medicare Improvements for Patients and Providers Act, the new law that staved off the cuts and set the positive updates, that hasn’t received as much attention is the financial incentive tied to electronic prescribing, also known as “e-prescribing.”
The law established a federal program through which physicians who prescribe electronically this year and in 2010 will be eligible for a 2 percent Medicare payment bonus. That will be phased down to 1 percent in 2011 and 2012 and 0.5 percent in 2013. Penalties for physicians who still prescribe using paper would take effect in 2012.
Physicians are eligible for incentive payments if at least 10 percent of their Medicare-allowed charges are associated with prescriptions. These physicians are the only ones who would face penalties down the road. To obtain the payments, eligible physicians need to report applicable e-prescribing measures established under the Physician Quality Reporting Initiative (PQRI) for their patients with Medicare Part D plans.
While the AMA does not support the penalties, it’s important to note that physicians who e-prescribe could—combined with the 1.1 percent payment update in place for 2009 and 2 percent PQRI bonus—see a more than 5 percent positive payment update this year.
An aspect of health care that is rapidly increasing in importance, e-prescribing allows physicians to transmit prescriptions electronically to a pharmacy’s computer system. It also allows doctors to view potential drug interactions and side effects, see prescription drug coverage and insurance information, receive electronic notification about the need to authorize refills or approve generic substitutions and share simultaneous access to prescription histories and allergies with pharmacies.
E-prescribing can play a significant role in health care by helping to improve patient safety, enhance care coordination among physicians and health care providers and reduce administrative burdens that keep physicians from their patients. “The benefits of what this technology can provide are real,” AMA Trustee Steven Stack, MD, said during an educational session on e-prescribing as part of the Interim Meeting of the AMA House of Delegates. “It’s the on ramp to the superinformation highway for health care.”
While some physicians are fortunate enough to work in health care communities that have gained a head start on e-prescribing, many aren’t so lucky and are just trying to make ends meet. Physician practices will need to redesign their work processes to maximize the benefits of e-prescribing, and the AMA is working with others to develop resources, which will be available soon, that will help educate and provide guidance for physicians who are interested in this technology.
Last year when Congress began considering legislation on e-prescribing, the AMA asked lawmakers to consider ways to help physicians pursue this technology, such as grants, loans, tax credits and other economic incentives. Physicians need adequate financial support to cover the costs—both direct and indirect—of buying, implementing and operating an e-prescribing system, and communities must have the necessary technical infrastructure and connectivity to support it (by all prescribers to dispensers).
The AMA also asked Congress to direct the US Department of Health and Human Services to establish national e-prescribing technical standards by the end of next year. The AMA remains optimistic that this timeline will be met, and it would be an important step; final standards would help interoperability among systems and are necessary to assure physicians and other stakeholders that their investments in e-prescribing software will not be rendered obsolete overnight.
The AMA recognizes the potential for improvements in patient safety and advances in care coordination that e-prescribing holds and will continue to collaborate with all stakeholders and Congress toward the most effective, efficient adoption and implementation of e-prescribing systems. A key to achieving this, however, is working together.
To join the AMA or renew your membership, visit www.ama-assn.org or call AMA Member Relations at (800) 262-3211.

Winter2009• 21
your voice is neededBy William Pierce, MD
Advocacy in Focus
PoLiTicaL advocacy and The practice of medicine have many similarities. Every day, physicians are advocates for their patients’ health care, either by arguing with
patients about why they need to stop smoking, or debating a surgery authorization with an insurance carrier. The definition of an advocate is a person who supports someone to make their voice heard, or ideally helps others to speak for themselves. We are advocates.
As health care issues loom large in the 2009 legislative session in Salem and Washington, we need more than ever for all physicians to come together to advocate and have their voices heard.
Oregon and the nation are living through a very difficult time, and during this legislative session, our elected officials will be making tough decisions. We may not all agree on the party principals of the majority or minority party, however we can agree that the issues surrounding the delivery of quality health care to Oregonians knows no party.
This legislative session we will be facing many contentious issues. Taxes on providers will be discussed. Scope of practice issues will be debated. Liability reform will be approached, again. The need for attracting more physicians to Oregon, especially rural Oregon, will be a theme running throughout the session.
We must stand as one to deliver a message to our lawmakers. A message that access to insurance does not equate access to quality care. A message that health care cost can and should be addressed and one of those costs is defensive medicine. A message that Oregon needs medical liability reform. A message that Oregon physicians need fair contracting and fair reimbursements rates. These messages transcend primary care versus specialty care or rural versus urban.
Oregon physicians will need to stand as one as we try to raise our voices through the thousands of other interest groups lining up to speak to their elected officials. So how do OMA members do just that?
� FIRST, members must stay connected with the OMA. Make sure we have your current e-mail address—that is the fastest and most cost efficient way to communicate.
� SECOND, members need to stay informed and make it a priority to know what is happening in Salem. Log on to the OMA website, and check STAT and PRN for information as it evolves.
� THIRD, commit to being active in the process. Respond to OMA Action Alerts using our quick and easy e-mail program. Your message will get to your lawmakers.
Finally, and most importantly, join the OMA and OMA Alliance for our Day at the Capitol on Thursday, February 19. Register at the OMA website, www.theOMA.org. It’s not too late to commit to taking action and having your voice heard.
William “Bud” Pierce is an oncologist in Salem, and an OMA Executive Committee Member-at-Large.
“Decisions are made by those who show up.”
–Aaron Sorkin, writer and creator of the West Wing

22 •Medicine in Oregon
Two Perspectives on Technology in Medicine
What technologies do you use/rely on the most?EvElyn FOrd: I know as much about medicine as a your average penguin does about flying; I rely heavily on my favorite databases to guide me in the right direction. I have ISI Web of Knowledge, a compendium of Medline and other evidence collections, bookmarked in my web browser and I automatically sign in to My EndNote Web to help me keep articles organized. In the rural village I work with in Zimbabwe, the most essential technology in place is the newly reconstructed well. All the antibiotics in the world cannot make up for a clean water supply.
MArgArET ThOMpSOn: I am 66, and while I am hardly a Luddite, I am certainly a dinosaur, utilizing technology grudgingly rather than with a passionate embrace. In fact, when we got our first treatment planning computer which the physicians would be using along with the dosimetrists, I sat in on the technologist orientation. I found myself so stressed that I developed pimples and diarrhea, an eloquent statement from my body.
That said, our field may be one of the most dependent on technology. Radiation treatment, “the invisible knife,” has long been viewed as a Star Wars approach to cancer treatment. It was on the verge of the diabolical, associated with atomic weaponry and radiation poisoning, suspect for any ill a patient might suffer from that date onward. Fortunately, modern physics and technology have led to more control in beam penetration and distribution. Coupled with modern imaging, we can greatly increase tumor dose while sparing normal tissues in large part, and accomplish more cures. Laboratory technology and research, as well as clinical trials, have led the way to combined irradiation and chemotherapy for yet more progress.
What technologies do you wish we relied on less?FOrd: I wish we relied less on urgent imaging, urgent labs, and our emergency care infrastructure in general. These systems and our use of technology within them are absolutely necessary and save lives every day. The physicians who coordinate our uses of this technology do so brilliantly, even under the most intense time limitations. However, we need to consider the costs of our decision to relegate our country’s only form of universal access to our emergency departments. The state-of-the-art technologies here, and the entire “standby” systems which house them, are both elegant and expensive.
ThOMpSOn: The main technology-related stumbling blocks which we run into cur-rently are in transfer and organization of information. It can be tremendously useful when it works smoothly, and we come to a complete standstill when it’s on the fritz. For example, the office computer which man-ages all of our scheduling, or the hospital electronic medical record, or electronic access to imaging where there is no longer hard copy in films. I understand the VA Hospital is doing a good job in providing uniform EMRs, and I wonder if the private health care system in this land of innovation and choice will ever achieve compatibility.
What technologies do you hope we’ll rely on more as time goes on?FOrd: Technologies of distribution and delivery. We need to improve uptake of preventive care services and screening technology in the US. Globally, we must ensure delivery of essential medicines and other patient care resources to which we’ve had access for decades. Some barriers we must overcome are structural. For example, across Zimbabwe and in many rural African regions, fuel shortages interfere with delivery of everything from vaccines to food; other barriers are legal. Patent law
was engineered to facilitate sharing of ideas and inventions; ironically, it is now used to circumscribe access to life-saving therapy.
ThOMpSOn: The most exciting emerging technology is in diagnostic laboratory and pathology, achieving increasingly refined definition of tumors and earlier detection. Would that we had an ultrasensitive PSA-like test for each malignancy. Likewise, targeted biologic agents have produced some cures, many regressions, with fewer side effects than conventional chemotherapy. Current laboratory methods are predicting which breast cancer patients would benefit from chemotherapy, and we hope to see individual tumors tested for sensitivity to an array of chemotherapy agents in vitro prior to clinical application.
What is the role of technology in your medical education/ continuing education?FOrd: Technology is the foundation of my medical education. Most of my reading resources, including my textbooks, are online. In my preclinical years, in addition to standardized patients, I also had the opportunity to learn from SIM-Man; although no great conversationalist, he’s certainly more amenable to medical students’ intubations than our volunteer actors. At the time of this writing I’ve completed no more than about 25% of my clinical curriculum, and have already had the chance to witness a stunning array of diagnostic and patient care technologies in action, including surgical, pharmacologic, imaging, and many others. This is an exciting time to be entering an increasingly powerful field of medicine.
ThOMpSOn: Continuing medical education has been greatly aided by availability of CD notes, DVD or live streaming video courses. I have personally been underwhelmed by the efficacy of computer searches of the medical literature in my own field. It seems more like a
On My Mind
Evelyn Ford, an Ms3 student at OHSU and Margaret Thompson, a now-retired radiation oncologist answer five questions about how technology is impacting medicine.

Winter2009• 23
scattershot gathering of articles, many in a foreign language with only the abstract translated, known articles on a topic conspicuously absent. I have been better served by a 40 year accumulation of index cards of abstracts and some personal notes derived from major journals in my field plus relevant articles noted in surveys and digests. This I have organized in a practical manner with subcategories pertinent to our decision tree, and I can quickly research a question or go on to original articles. I only use Medline when I am researching something unfamiliar, and library texts are not current enough.
is there any aspect of medicine which cannot be replaced by technology?FOrd: Yes, doctors! In the United States today, our access to technology is unparalleled in human history. Human, physician-caliber creativity is now required in order to achieve delivery of our technologies to those who need them most, both within and beyond our borders. Physician compassion can never be replaced by technology, and it is compassion that guides physicians to and through a life of medical practice. Equally, compassion should guide our own use, development and delivery of technology. As physicians and future physicians, it is our responsibility to harness technology to improve outcomes: for our individual patients, for our health care system, for our world.
ThOMpSOn: Obviously, all this is to no avail if there is not a well trained individual to apply the knowledge to an individual situation, and one hopes, with compassion. There are few greater joys than to see someone on the street enjoying recovery from an illness and to know you were privileged to have a part in this. Or to know that even when cure was not possible, physical and emotional comfort were enhanced by your efforts.
Evelyn Ford is a third year medical student at Oregon Health & Science University. In her free time, she helps direct programming and research for Africa AIDS Response.
Margaret J. Thompson, MD, is a recently-retired radiation oncologist in Salem. She worked full time at Salem Hospital for 25 years, and has been doing locum tenens work around Oregon for the past 10.

24 •Medicine in Oregon

Winter2009• 25
TeLeMedicine real Promise for Oregon By Kelly Hagan, JD
In house Counsel
The WaLL sTreeT JournaL’s special insert of October 20, 2008 told of miraculous advances in healthcare
information technology, a “Prescription for Change.” One section of this long feature article was entitled, “The Offshore Doctor Will See You Now,” as if this reality were right around the corner. It left one to wonder, “What’s going on back there in New York City?”
The promise of healthcare information technology is not to be underestimated. But the healthcare system is a long way from embracing an international, interoperable future. Practical obstacles still abound. The cost is significant, and a return on investment may be difficult to observe or measure, particularly for practitioners. State and federal governments have been stingy with reimbursement for telemedical services, generally restricting payment to circumstances involving rural or underserved populations, and “interactive” services. Efforts to loosen regulatory restrictions under the Anti-Kickback and Stark Laws have generally fallen flat, as the uncertainty displaced by “safe harbors” has been replaced with dissatisfaction with the financial obligations imposed by these reforms.
And as for that offshore doctor, don’t count on anyone paying for those services any time soon. The most recent guidance on teleradiology reimbursement from the Centers for Medicare and Medicaid Services clearly excludes reimbursement for remote services from foreign soil.
“Payment may not be made for a medical service (or a portion of it)
that was subcontracted to another provider or supplier located outside the United States. For example, if a radiologist who practices in India analyzes imaging tests that were performed on a beneficiary in the United States, Medicare would not pay the radiologist or the US facility that performed the imaging test for any of the services that were performed by the radiologist in India.”1
In part for that reason, Nighthawks, one group of American-trained radiologists located overseas who provide immediate diagnostic interpretation of CT images obtained in emergency rooms after hours, now offer “final” reads performed by physicians in the US.
faster PossibilitiesBut telemedicine marches on. In a state like Oregon, with its remote communities and numerous underserved areas, there is need not only for telemedicine, but for much greater speeds of transmission. Most Medicare reimbursement is reserved for “interactive” real-time connections between the patient and the remote provider. And anyone who has waited for a T1 line to download an MRI study knows that the current system is underpowered.
Enter the Rural Health Care Pilot Program. Taking advantage of funding from the Federal Communication Commission, a coalition of more than a 150 Oregon telemedicine advocates sponsored a proposal in 2007 for a regional broadband network. Dubbed the “Oregon Health Network,” the
organization will receive in excess of $20 million dollars over three years to deliver broadband connectivity to healthcare providers throughout Oregon. First will be connections among existing networks, and then ever more remote clinics and facilities. Depending on the services being rendered, these services may be covered by governmental or private payers.
A collateral benefit of the Oregon Health Network is its economic development potential. As it expands into rural Oregon, the huge capacity of fiber optic lines, which far outstrip the needs of rural healthcare providers, will bring with it plenty of excess bandwidth. Rural communities hoping to connect to knowledge-based industries, and telecommunication vendors looking for new markets and sales, will find unexpected ways to exploit this connectivity. Now that would be a happy marriage of policy objectives.
While the telemedicine mavens in New York see transcontinental physical exams in our future, practical telemedicine is already at work in Oregon. With a little help from Congress, and the FCC, it is quickly changing the way healthcare is delivered to Oregonians.
Kelly Hagan is a shareholder in the Portland office of Schwabe, Williamson & Wyatt, P.C., where he specializes in advising healthcare providers on business and regulatory matters. He can be reached at [email protected].
1 CMS MLM Matters, dated 2/23/07; see also CMS Manual Pub. 100-02, Transmittal 66, Change Request 5427, implementation date 4/2/07 (“This Change Request clarifies that payment may not be made for a medical service (or portion of it) that was subcontracted to another provider or supplier located outside the United States”).

26 •Medicine in Oregon
EvEry fifth-gradE studEnt in our state knows that John McLoughlin, the
“father of Oregon,” practiced medicine before he became the Hudson’s Bay Company lead agent on the West Coast, its Chief Factor. Governor John Kitzhaber blended patients and politics for much of his career, and continues to do so as head of the Archimedes Movement. Health care analysts around the country recognize Oregon as an in-novator, willing to explore controversial initiatives like the Oregon Health Plan, Physician-Assisted Suicide, and medi-cal marijuana.
Given the role of medicine in Oregon’s history, two OMA participants with a penchant for history—retired Chief Operat-ing Officer Jim Kronenberg and educational video contractor Matt Simek of Pacific Standard Television—collaborated in 2001 on a concept for bringing the rich history of medicine in Oregon to the state’s citizens through an innovative television series. Kronenberg recalls, “After witnessing Matt’s enor-mous talent and energy in the production of malpractice loss prevention education videos for 30 years, I got the idea for some kind of medical history. It was triggered when I watched a video of one of my true heroes [longtime OHSU associate dean] J.S. ‘Dutch’ Reinschmidt’s reminiscences and thought how terrible it would be to miss recording stories of other senior physicians and public figures who have fundamentally affected health care in Oregon while they were still alive to tell them.”
With the financial support of the Oregon Medical Educa-tion Foundation and a steering committee chaired initially by Dr. Harold Osterud and more recently by Dr. Roy Payne and currently by Dr. George Waldmann, the project sought to examine the history of medicine in Oregon as a three-part television series. The project soon won the additional help of OHSU’s long-standing Oral History Program. For more than a decade, interviewers have captured personal recol-lections from doctors, nurses, and other key players whose careers have influenced medicine in Oregon as well as many other parts of the world.
With support from the OMEF and the OHSU Oral History Program, the project undertook to interview more than 50 senior physicians and others “closely related to health care” for their recollections, insights, and perspectives.
The project has evolved beyond excerpts of “talking heads” to something more meaningful both to physicians and to the general public. Weaving the resulting raw video into a layered tapestry, Simek intends to illustrate the history of medicine in our state from the days of Native healers, through Lewis & Clark and John McLoughlin, the founding of one of the first medical schools west of the Mississippi, the Chinese herbalists of John Day, contributions like the Starr-Edwards heart valve, the imaging revolution, and the advent of interventional radiology, to the present day.
Simek says he feels the press of time, knowing that precious resources could be silenced at any moment. “Fortunately, we interviewed George Saslow, Harold Osterud, Eddie Wah, Ed Press, Ken Swan, and Rod Beals before they passed away. It would have been a terrible loss to miss their stories. We haven’t been so lucky with a few others. These men and women have seen so much change, lived through so much history . . . and it isn’t just them. They learned from doctors who extend the line back to the turn of the 20th century.”
In some ways, Simek has been faced with an embarrassment of riches. Throughout the state, doctors in their 80s and 90s vividly remember the rise of antibiotics, the explosion in medical technology, and the changes brought by the creation of Medicare and Medicaid. To help narrow the field and identify prospective interviewees, Simek and Kronenberg pulled together a steering committee “drawn from the OMA, OHSU, and the general public based on an interest in medi-cal history and in this proposal in particular.” They have also enjoyed the assistance of the Oregon Historical Society, the Foundation for Medical Excellence, and independent historians and researchers.
Medicine and history in OregonBy Nancy S. Boutin, MD
Medical history
A

Winter2009• 27
A project like this could grow to gargantuan proportions, but, as with most projects, funding remains a rate-limiting step. The lion’s share of financial support has come in nearly equal amounts from the OMEF and OHSU, with in-kind donations from many of the organizations listed above. Additional funding required to complete the series is sought from the health care industry and related organizations, the broadcast industry, and trusts and foundations. Individual tax-deductible contributions can be made to the OMEF, a 501(c)(3) charitable educational foundation.
Oregon Public Broadcasting is exploring the possible state-wide distribution of “The History of Medicine in Oregon,” and the project was accepted in 2007 as a partner project of Oregon 150, the organization planning the celebration of Oregon’s sesquicentennial. Whether or not the program makes it to prime time, the steering committee and produc-tion staff intend to distribute the documentary widely for the interest and enjoyment of both medical and general audiences.
“There’s an old canard that those who fail to learn from history are doomed to repeat the mistakes of the past,” says Kronenberg. “And so it is with medicine and health care in our state. There is a great deal to learn from what has gone before from the perspective of those who experienced it.”
For more information, contact Matt Simek, [email protected].
A: Surgical theater, Multnomah County Hospital.
B: U of O Medical School graduate (1904) Herbert M. Greene, MD, on a house call in LaCrosse, Washington, before returning to Portland.
C: X-Ray unit at the People’s Institute and Portland Free Dispensary, 1920s.
D: First Board of Medical Examiners in Oregon, 1889: (L-R) James Dixon, James Brown, O.P.S. Plummer.
E: General Electric Procedure Lab, 1966, used for applied research by Drs. Charles Dotter and Melvin P. Judkins.
F: Tonsillectomy under way at Doernbecher Memorial Hospital for Children.
G: Faculty and students, United States Army Medical Service 46th General Hospital, drill on Marquam Hill, ca. 1941.
h: People’s Institute and Portland Free Dispensary, 1920s.
All photos courtesy OHSU Historical Collections & Archives, Sara Piasecki, Head
B
C
D
E
F G h

On CallBy Michael Wynn, DO
Later than I can describestanding outside with the phonemurmuring to someoneI do not know.
Lavish starsindifferent jewels.
Crickets thrum for lovers.Furred silence crosses the patio.
Late summer air slips insidemy robe falling open.
Exhausted.
If I drop the robe, lift my head,look up at the inexhaustible,the voice would never know.
Send your “Creative Outlets” to Betsy Boyd-Flynn at [email protected].
See complete submission information on page 7.
Dr. Michael Wynn practices Neurology in Salem and Corvallis. His poetry has been published in The Cortland Review, JAMA, and Neurology.

Have HIPAA Questions?
OMA HAs Answers
For complete details, visit
www.theOMA.org/workshops
Updated HIPAA policies, procedures, and templates are now available on the HIPAA section of the OMA website.
These great office tools and resources provide an overview of the HIPAA policies as well as customizable templates and forms for your office.
Developed by Chris Apgar for OMA, a nationally-respected expert on HIPAA, these tools help physicians ensure they meet the HIPAA requirements.
Visit www.theOMA.org/hipaa to access this exclusive member benefit. You will need a member login to access this section of the OMA website. For login instructions, visit www.theOMA.org or contact Stephanie at stephanie@theOMAorg or (503) 619-8000 for further login information.
Audioconferences Start This Month!
1.5 hour courses you can take from the convenience of your office; multiple staff can listen in for one registration fee!
HIPAA-related topics covered include: Changes to electronic transactions and Code Sets, and CMS Compliance Audits, Red Flag Rules and Claims Attachments. To register or to read audio-conference descriptions, visit www.theOMA.org/hipaaseries.
In-Person Workshops Start in April!
HIPAA How To’s will be offered in Portland, Bend, Eugene and Medford during April. These workshops are a great way to find out about the most common areas where practices are having difficulty or are not fully HIPAA compliant. Participants will also learn how to prepare for a CMS audit. Meet Chris Apgar and talk to other offices that are experiencing similar issues.
Web-based course available any time.
The OMA offers a HIPAA online training course that provides the latest information and instruc-tion on HIPAA Privacy, Electronic Security, Electronic Transactions, and Enforcement. If you would like to learn more about this course-ware, visit www.hccs.com/docs/brochures/hipaa_brochure.pdf or to register for this course, click on the “Online HIPAA Training-Register Today” link on the OMA homepage at www.theOMA.org.
3 ways to Learn More...Over the Phone In Person Online
