medication use in pregnancy - prisma health
TRANSCRIPT

4/15/2019
1
DM, HTN, and PTL:Pearls for the Bedside
Berry Campbell, MD
USC School of Medicine
Director, Maternal Fetal Medicine
Berry Campbell, MD
USC School of Medicine
Director, Maternal Fetal Medicine
18 Year Old G1 @ 36 weeks• Presents in labor
• Presumed gastroenteritis (N&V 3 days)
• Ctx q 3 minutes, decreased variability, late decels
• CBC normal
• Routine (limited) prenatal care – negative history
3

4/15/2019
2
What interventions?
• IVF
• Oxygen
• Position change
• Terbutaline

4/15/2019
3
Next Step?
• DELIVERY!!!!!!
• General anesthesia
Primary Cesarean Section• 8 lb 2oz male
• 2/3/5 Apgars
• Cord gas pH 6.9
• Placenta large and edematous; excessive AF upon amniotomy (polyhydramnios)
8
Intra-operative Course
• BP low
• Pulse > 140
• 02 sats < 92%
• Labs → pH 6.9
9

4/15/2019
4
Thoughts??
• Abruptio
• Pulmonary embolus
• Amniotic fluid embolus
• Other?
• Labs: Cr 1.7, K+ 7.2, Na+ 129, HCO3
• Glucose 433
DIAGNOSIS
Diabetic Ketoacidosis!
Missed glucola, never had 3rd trimester labs
Gestational DM?
Pregestational?
Diabetes Mellitus Complications
• Macrosomia, IUGR
• Birth defects
• Stillbirth
• Neonatal hypoglycemia, trauma, polycythemia, jaundice
• HTN, preeclampsia
• Diabetic ketoacidosis
12

4/15/2019
5
DKA
• Maternal mortality
• Perinatal asphyxia, acidosis (ketones)
• Perinatal mortality up to 70%
Diabetic Ketoacidosis• pH < 7.3
• Serum HCO3 - Low
• Serum acetone positive
• BS ≥ 300 (200 in pregnancy)
• Other findings: Elevated K then low, low Na, Cl and HCO3
• Literally, DKA is deficiency of insulin
Insulin
• ↓ FFA release from adipose
• ↓ Liver FFA oxidation and Ketogenesis

4/15/2019
6
DKADecreased Insulin
↓
↑ FFA
↓
↑ Ketone release
↓
Metabolic Acidosis, Respiratory Compensation (Kussmaul breathing)
DKA
Hyperglycemia
↓
Osmotic Diuresis
↓
Excessive Urine Loss of water, Na, K
↓
Volume Contraction
Fetal Death
• Hyperglycemia →
hyperinsulinemia
• Insulin ↑ metabolic rate, ↑oxygen consumption & ↓O2 delivery stillbirth

4/15/2019
7
• Precipitating factors
– Prolonged emesis from any cause
– Infection
– Insulin omission/pump failure
– Non-compliance
– Alcohol/drug use
– Steroids
DKA

4/15/2019
8
DKA TreatmentIV Insulin 0.2-0.4 units/kg – Load
2.0-10.0 units/hour maintenance
Na Cl 0.9% 4-6L first 12 hours1 L first hour
500-1000ml/hr x 4 hours250 ml/hr
D5 NS When glucose 200-250
Potassium elevated initially Replace 20 meq/L when normal
Bicarb 1 Amp/L if pH < 7.1
DKA
Allow in utero resuscitation if possible before delivery
Hypovolemia, acidosis, impaired O2 delivery
↓
Fetal death
Diabetic Ketoacidosis
• Most often in long standing pre-gestational diabetics
• Non-compliance the single most common issue
• Repeated episodes are common, related to higher risk of vascular complications
• History: Ever have DKA? When was last time?

4/15/2019
9
4/15/2019
10
24 year old G1P0 @ 28 weeks• C/O HA, visual spots
• BP 140/90; 1 + protein
• Fetal size CWD, normal fluid and BPP
• No history HTN
Management
• Admit obs
• Labs: LFT’s, CBC, Cr, 24 hour urine
• Treat HA
• Consider Steroids
• No change in status, BP and symptoms disappear, no protein
• Diagnosis?
• HTN in pregnancy (gestational HTN)
• Management?
• Outpatient obs with no BP meds; ?steroids?
4/15/2019
11
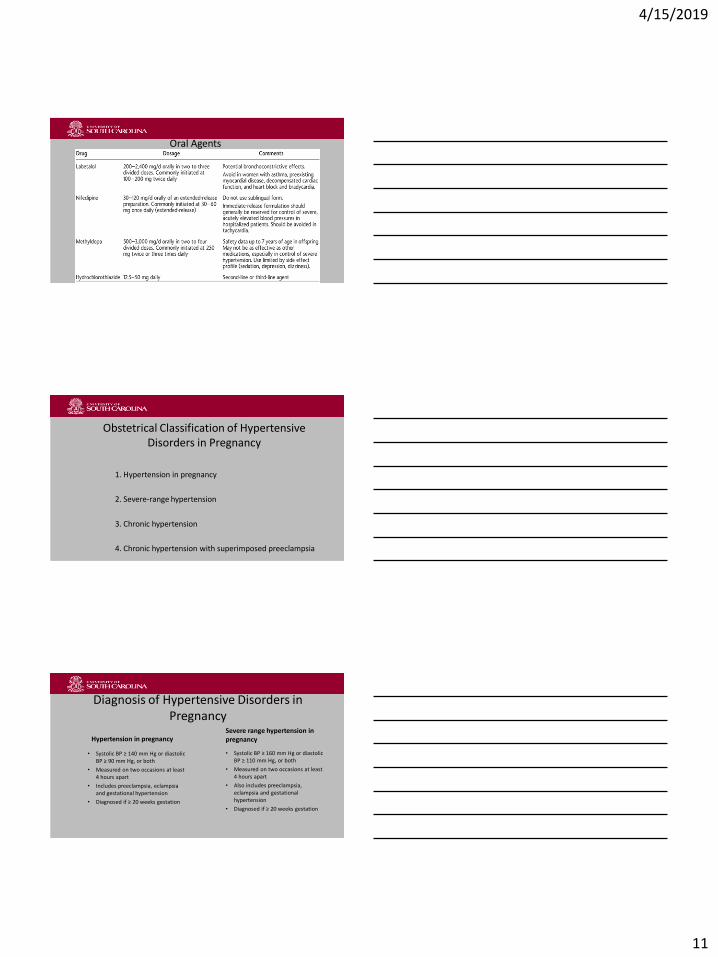
Oral Agents
Obstetrical Classification of Hypertensive Disorders in Pregnancy
1. Hypertension in pregnancy
2. Severe-range hypertension
3. Chronic hypertension
4. Chronic hypertension with superimposed preeclampsia
Diagnosis of Hypertensive Disorders in Pregnancy
Hypertension in pregnancy
• Systolic BP ≥ 140 mm Hg or diastolic BP ≥ 90 mm Hg, or both
• Measured on two occasions at least 4 hours apart
• Includes preeclampsia, eclampsia and gestational hypertension
• Diagnosed if ≥ 20 weeks gestation
Severe range hypertension in pregnancy
• Systolic BP ≥ 160 mm Hg or diastolic BP ≥ 110 mm Hg, or both
• Measured on two occasions at least 4 hours apart
• Also includes preeclampsia, eclampsia and gestational hypertension
• Diagnosed if ≥ 20 weeks gestation

4/15/2019
12
Diagnosis of Hypertensive Disorders in Pregnancy
Chronic hypertension
• Hypertension diagnosed or present before pregnancy or before 20 weeks gestation
• Also hypertension diagnosed for the 1st time in pregnancy and that does not resolve in the postpartum period
Chronic hypertension with superimposed preeclampsia
• Preeclampsia in any woman with chronic hypertension
Same patient………but now
• BP 180/110; 1 + protein; O2 sats 92%
• LFT’s normal Cr 1.1
• Hb 12.3 plt 142k
• HA and visual changes improve
• NST Rx
• Management?
35
• BP management
• CXR, consider BNP
• Strict I&Os
• Weight
• IVF, magnesium sulfate, steroids
• Oxygen

4/15/2019
13
Intrapartum Management: Medications for Acute-onset, Severe BP
• ***Goal is NOT to normalize BP, but a mild hypertensive BP range (140-150/90-100 mm Hg)***
• First line medication management choices include: IV labetalol, IV hydralazine, OR immediate release oral nifedipine
• Magnesium sulfate is NOT used as an antihypertensive medication but is the drug of choice for seizure prophylaxis
Loading dose 4-6 g over 15 min IV, then 1-2 g/hr
Target serum concentration 4-8 mg/dL
Toxicity corrected with calcium gluconate, IVF, loop diuretics or hemodialysis
Intrapartum Management: Medications for Acute-onset, Severe BP
• Suggested protocols (just pick one):
1. Initial 1st line management with immediate release oral nifedipine
2. Initial 1st line management with IV hydralazine
3. Initial 1st line management with IV labetalol
HOWEVER: Clinical situation may benefit a specific choice over others!
• CXR increased interstitial markings
• BNP 442
• What BP med?

4/15/2019
14
PREECLAMPSIA
Vasospasm …….↑ BP
↓
Endothelial Injury…….. Edema,
Platelet
consumption,
Proteinuria
PreeclampsiaOrgan System Involvement
• Renal - GFR, Cr, Protein spill
• Liver – Fibrin deposits with LFT’s
• Hematologic – Low platelets, Hct, coagulopathy
• CNS - HA, visual changes, seizures
• Respiratory – Pulmonary Edema
BP Management with Pulmonary Edema
• Prefer after-load reduction (vasodilator)
• Choices:
Hydralazine
Procardia

4/15/2019
15
Hydralazine
Nifedipine
24 year old G1P0 @ 28 weeks• Same as before, severe HTN
• BUT………….
• Fetal weight 5% tile
• FHT reassuring
• Doppler flow abnormal (IRDF)
45

4/15/2019
16
46
BP Management?
• Remember, fetus is teetering on the edge!
• High BP may be the only thing perfusing placenta (UPI)
• SLOWLY decrease BP, maybe slower admin of meds
• Extreme care if use Procardia (other IV choices better as can titrate starting with lower doses)
Labetalol

4/15/2019
17
BP Management
• Same patient with serum Cr 1.8, poor UOP?
• Procardia shown to improve renal perfusion, UOP
Same case• c/o HA with loss of vision
• Seizure begins!
• Supportive: Airway, O2 sats
• Magnesium sulfate IV (continue or start)
• BP meds
• FHR monitoring
50
Management• Seizure recovers
• Continue Magnesium sulfate
• Move to delivery
• Induction vs. CS
51
4/15/2019
18
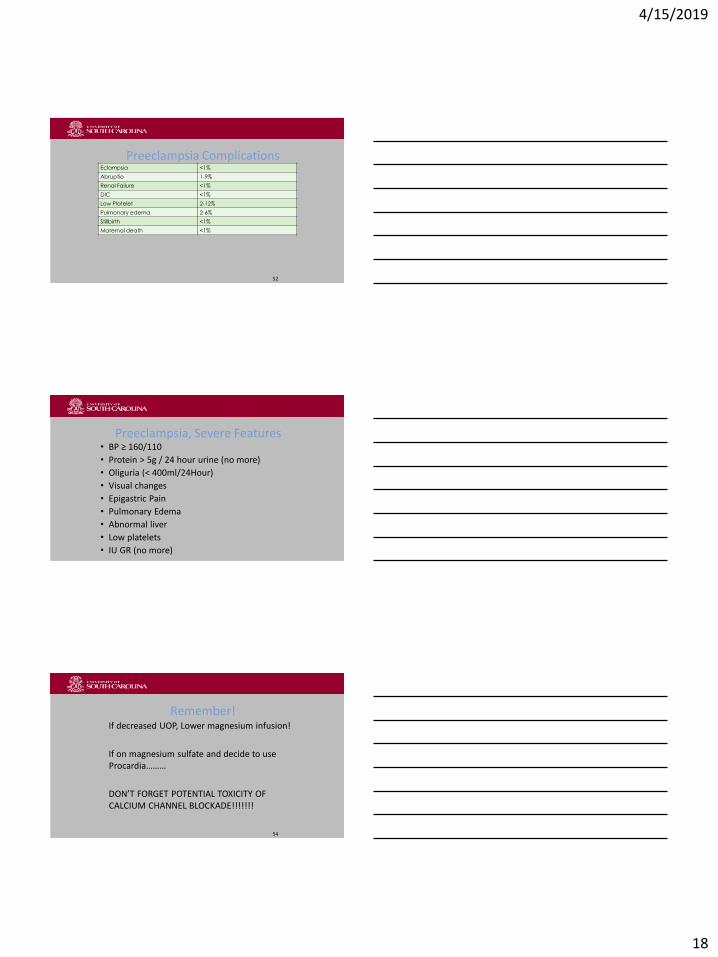
Preeclampsia ComplicationsEclampsia <1%
Abruptio 1-9%
Renal Failure <1%
DIC <1%
Low Platelet 2-12%
Pulmonary edema 2-6%
Stillbirth <1%
Maternal death <1%
52
Preeclampsia, Severe Features• BP ≥ 160/110
• Protein > 5g / 24 hour urine (no more)
• Oliguria (< 400ml/24Hour)
• Visual changes
• Epigastric Pain
• Pulmonary Edema
• Abnormal liver
• Low platelets
• IU GR (no more)
Remember!If decreased UOP, Lower magnesium infusion!
If on magnesium sulfate and decide to use Procardia………
DON’T FORGET POTENTIAL TOXICITY OF CALCIUM CHANNEL BLOCKADE!!!!!!!
54
4/15/2019
19
Hypertensive Emergencies• Require immediate control of BP; defined as SBP > 180 mmHg or
DBP > 120 mmHg and/or acute target organ damage; ICU admission
• Present with cerebral infarction, pulmonary edema, hypertensive encephalopathy, CHF
• Esmolol load 0.25-0.5 mg/kg IVP over 1 minute, then 0.05-0.1 mg/kg/min IV for 4 minute
• Nicardipine IV infusion at 5 mg/hr and titrated by 2.5 mg/hr every 5 min to max rate of 15 mg/hr
• Nitroglycerin IV infusion at 5 µg/min increased every 3-5 min until max dose of 100 µg/min
• Sodium nitroprusside IV infusion at 0.25 to 5.0 µg/kg/min; onset immediate w/ short half-life (extreme cases only)
• Epidural analgesia can be helpful for reduction in SVR
Hypertensive Emergencies
***Goal to reduce SBP by max of 25% in 1st hour, then aim for 160/100 over next 2-6 hours, then cautiously titrate to normal over next 24-48 hours
*Key to hypertension in pregnancy; have an established action plan / protocol in place before actual event. In other words, know what you know and if you don’t know get help
Prevention of Preeclampsia

4/15/2019
20
• 38 yo G1 at 28 weeks
• Presents with uterine contractions, spotting, watery mucous discharge
• IVF pregnancy
• Uncomplicated course to this point
• FHT reactive, ctx every 3-5 minutes
• Palpate moderate intensity
• Pelvic no ROM
• Cervix digitally 4cm/70%/-1

4/15/2019
21
Management??
• IV Fluids
• Betamethasone
• Rule/out infection (UTI, GC, etc)
• Transfer/keep (NICU capabilities)
• Tocolytics?
• Magnesium sulfate: Ca channel blocker. SE: toxicity (resp)
• Indomethacin: NSAID. SE: renal, GI, bleeding
• Terbutaline: Betamimetic. SE: cardiac, ↑BS
• Procardia (short acting): Ca channel blocker. SE: HA, cardiac
Preterm Labor
• IV magnesium sulfate 4-6 g bolus then 2-3 g/hr
• SQ terbutaline 0.25 q 30 min up to 3 doses with pulse < 130
• Indocin 25-50 mg po q 4; nifedipine 10-20 mg po q 4
63

4/15/2019
22
• Don’t forget—
• Age risks.
• IVF risks.
Preterm Labor
• Betamethasone 12mg IM x 2 doses, 24 hours apart
• Goal: attain 48 hours from 1st dose—lowers risk of RDS, ICH, NEC
• Precipitating/associated factors: UTI, other infections, previa, abruptio, prior PTL, twins, smoking, drug abuse
65
• Cervix 6cm/100%/0 station
• 1 hour ground transport
• Transfer/ keep?
• Presentation make any difference?

4/15/2019
23
Preterm Labor (<37 weeks)
• Contractions
• Cervical change or >2cm/50% on 1st exam with contractions
• Early preterm <34 weeks
• Late preterm 34-36w 6d
67
Thank You!!

4/15/2019
24
• Potassium
• Deficit often 5 – 10 mEq/kg
• Do not replace in during the first 2-4 hours
– Levels usually normal to mildly elevated at outset
– As acidosis corrected, levels fall quickly due to intracellular shift ---H+/K+ transporter
• Replacement
– 40 mEq/h when serum K<3
– 30 mEq/h if between 3 and 4
– 20 mEq/h if between 4 and 5
– No replacement if >5
• Monitor UOP carefully, may use KCl, KPhos
DKA
• The Basics
– Patient transferred to ICU
– Fetal monitoring if at viable gestational age
– Detailed flow chart
• Dates/times
• Serial glucose measurements
• Serum ketones
• Electrolytes
• ABGs
• AG
• Insulin
• I/Os
DKA

4/15/2019
25
• Diagnosis in pregnancy
– Serum pH <7.30
– Serum bicarbonate < 15
– Serum ketones > 1:2 dilution
– Any glucose level (non-pregnant needs to be >300)
• Often leukocytosis present, not necessarily indicative of infection, look for left shift
• AG in DKA often >15 [Na-(Cl+HCO3)]
• Serum osmolality correlates with mental status
– [2(Na+K)+serum glucose/18], value >320 mOsm/L significant, coma > 340
DKA
• Clinical presentation
– Develops over 3-7 days
– Polyuria, polydipsia, blurred vision, anorexia, nausea/vomiting, abdominal pain, weight loss
– Abdominal symptoms from elevated ketones
– May have mental status changes, Kussmaul breathing, fruity odor, dry mucous membranes
– Sinus tachycardia and orthostatic hypotension
DKA
• Ketones
– Moderately strong acids
– Body reacts to correct the metabolic acidosis
• Respiratory
– Kussmaul breathing – increase respiratory rate and depth
– Blow-off CO2
– Compensatory “respiratory alkalosis”
• Bicarbonate declines
• Hyperglycemia osmotic diuresis
DKA

4/15/2019
26
Preeclampsia• 7% incidence
• Nulliparous, family history, multiples, Renal Disease, HTN, IDDM, previous preeclampsia, African Americans
HELLP• Hemolysis
• Elevated Liver
• Low Platelet
• 2-12% of preeclampsia
HELLP• Epigastric Pain
• Nausea/Vomiting
• HTN, Edema, Proteinuria

4/15/2019
27
Preeclampsia Management
• Supportive care
• Magnesium sulfate – seizure prophylaxis
• Betamethasone if < 34 weeks
• Delivery
Eclampsia
• Think ABCs
• Magnesium sulfate
• Stabilize
• Deliver if pregnant once stable
DiagnosisMagnesium Toxicity
Loss reflex 8-10 mg%
Slurred speech 10-12mg%
Muscle paralysis, respiratory difficulty 15-17mg%
Cardiac arrest 30-35mg%
81

4/15/2019
28

4/15/2019
29