medication reconciliation for the elderly population h. edward davidson, pharmd, mph asst....
TRANSCRIPT
Medication Reconciliation for the Elderly Population
H. Edward Davidson, PharmD, MPHAsst. Professor, Clinical Internal MedicineEastern Virginia Medical SchoolPartner, Insight Therapeutics, LLC
Learning Objectives
To define medication reconciliation and its role in patient-centered care
To illustrate the types of medication related problems associated with transitions of care
To describe a method for health care providers and institutions to evaluate their transition of care processes
“Medications are probably the single most important health care technology in preventing illness, disability, and death in the geriatric population.”
Avorn J. Medication use and the elderly: current status and opportunities. Health Affairs 1995.
Clinical Practice Guidelines, the Elderly, and Multiple Comorbid Conditions
Hypothetical 79-yr-old woman with COPD, Type 2 DM, osteoarthritis, hypertension, and osteoporosis
If followed published CPGs wouldBe prescribed 12 routine medicationsCost of $406/month
Implications in pay-for-performance initiativesIncrease risk of medication related problemsDifferent settings, different goalsPotential for diminished quality of care
Boyd CM et al. JAMA 2005;295:716-24.
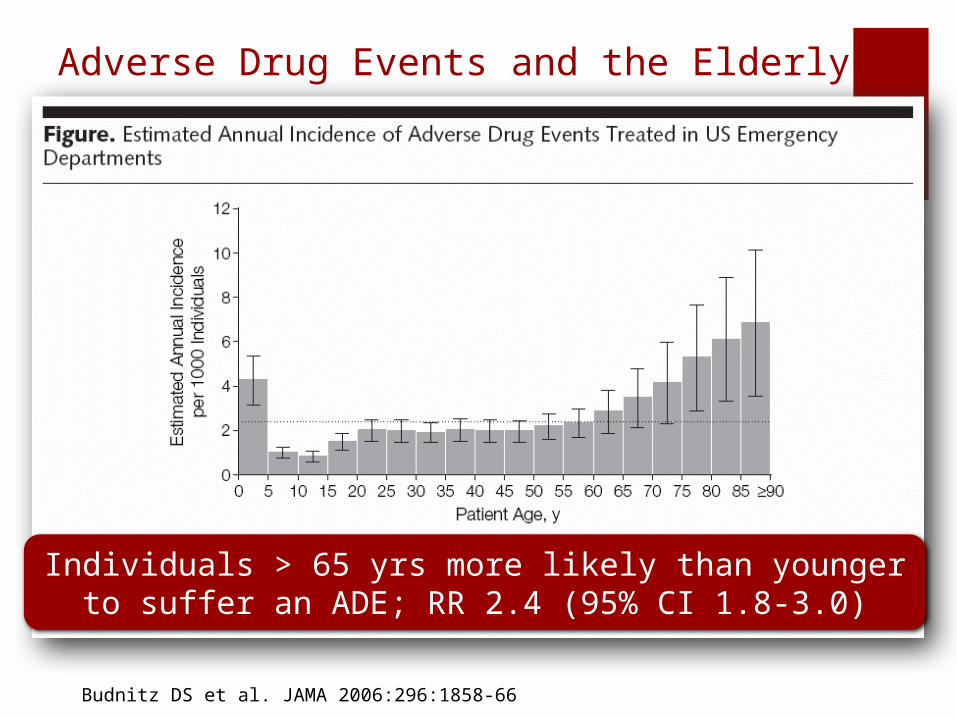
Adverse Drug Events and the Elderly
Individuals > 65 yrs more likely than younger to suffer an ADE; RR 2.4 (95% CI 1.8-3.0)
Budnitz DS et al. JAMA 2006:296:1858-66
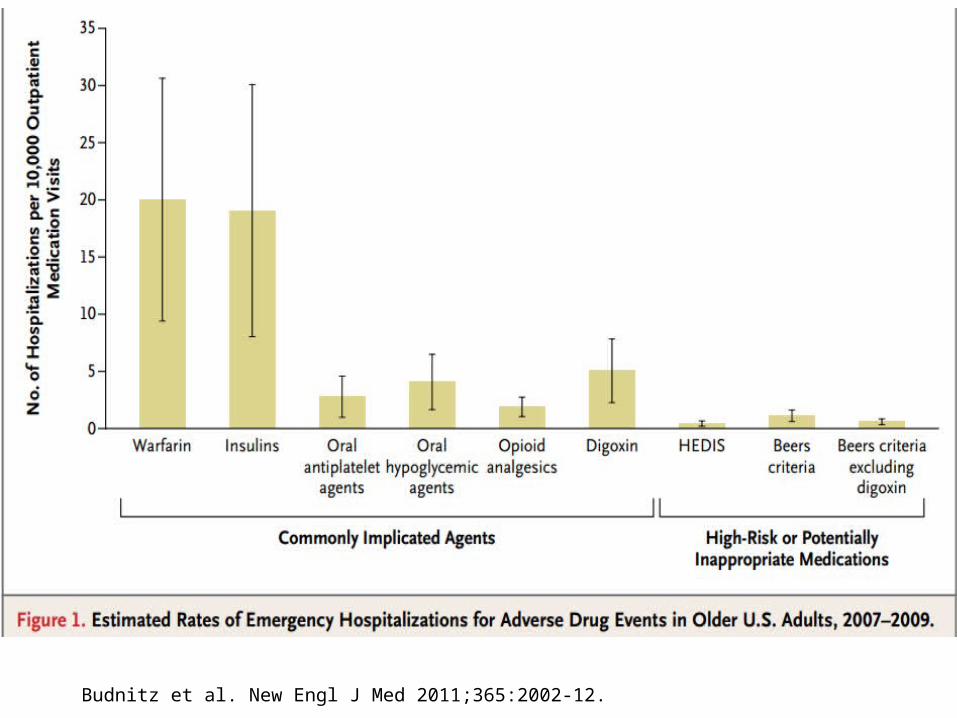
Budnitz et al. New Engl J Med 2011;365:2002-12.
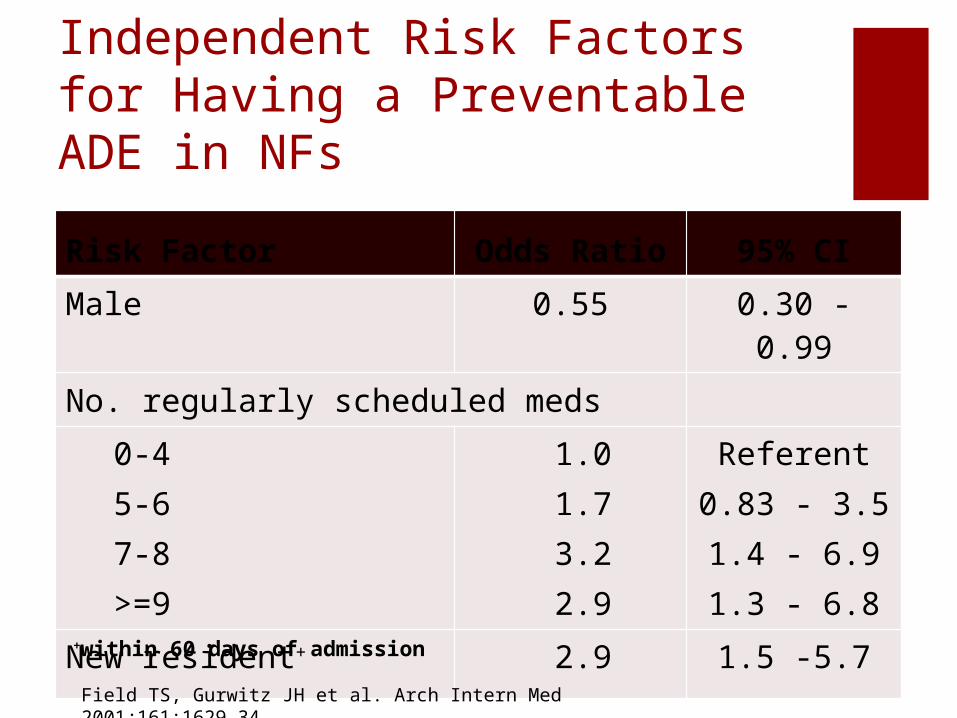
Independent Risk Factors for Having a Preventable ADE in NFs
Risk Factor Odds Ratio 95% CI
Male 0.55 0.30 - 0.99
No. regularly scheduled meds
0-45-67-8>=9
1.01.73.22.9
Referent0.83 - 3.51.4 - 6.91.3 - 6.8
New resident+ 2.9 1.5 -5.7
+within 60 days of admission
Field TS, Gurwitz JH et al. Arch Intern Med 2001;161:1629-34.

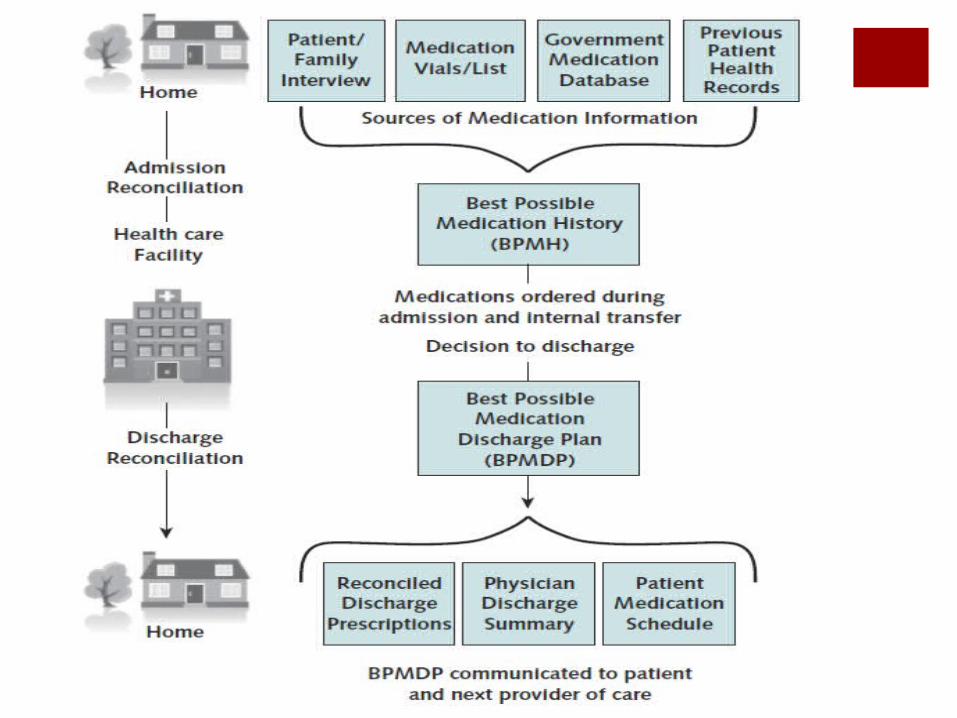
What is Medication Reconciliation?Joint Commission:
The process of comparing a patient's medication orders to all of the medications that the patient has been taking
Reconciliation is done to avoid medication errors such as omissions, duplications, interactions, and the need to continue medications
Provides the patient/resident (or family) with written information on the medications they should take
Explains the importance of managing medication information when he/she leaves the organization’s care

Evolution of Medication Reconciliation
NPSG.03.06.01: Maintain and communicate accurate patient medication information
Implemented 7/2011
NPSG.08.01.01: Accurately and completely reconcile medications across continuum of
care
Implemented 1/2006
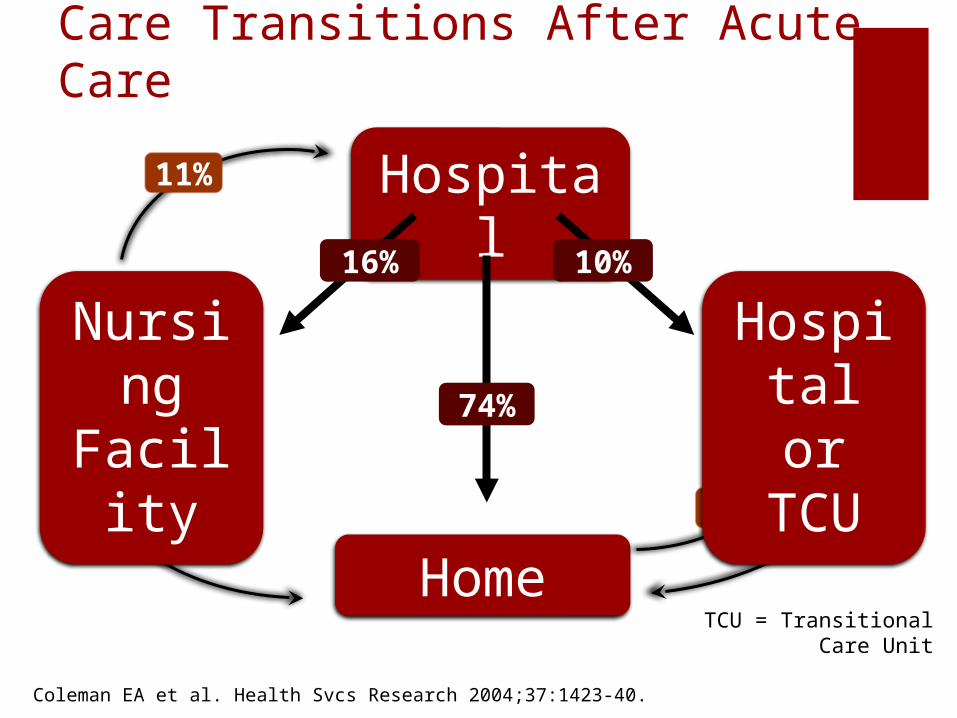
Care Transitions After Acute Care
Hospital
Home64%
77%
13%
11%
Nursing
Facility
Hospital or TCU
16% 10%
74%
TCU = Transitional Care Unit
Coleman EA et al. Health Svcs Research 2004;37:1423-40.

Hospital Admission
On hospital admission, more than 50% of patients have at least one medication discrepancy*
Approximately 40% of those have potential to cause harm
Cornish PL et al. Arch Intern Med 2005;165:424-9.
* Discrepancy defined as error between admission medication orders and patient interview of medication history.

Hospital Discharge
On discharge from the hospital, 30% of patients have at least one medication discrepancy* with the potential to cause possible or probable harm
Kwan Y et al. Arch Intern Med 2007;167:1034-40.
*Most common discrepancy is omission of pre-admit medication.
Adverse Events in Nursing Home Residents Transferred to the Hospital
122 nursing home to hospital transfers98% returned to the nursing homeIn 86% of transfers, at least one medication
order was altered (mean 1.4)65% - discontinued19% - dose changes10% - substitutions
20% of changes resulted in an adverse event
Boockvar KS, Fishman E, Kyriacou CK et al. Arch Intern Med 2004;164:545-50.
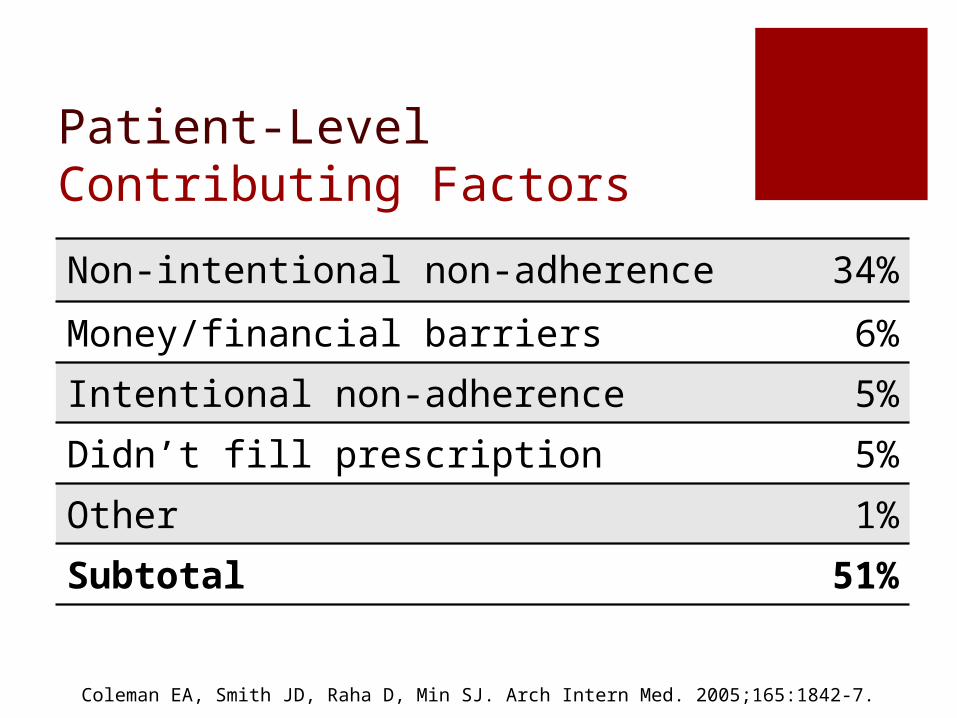
Patient-Level Contributing Factors
Non-intentional non-adherence 34%
Money/financial barriers 6%
Intentional non-adherence 5%
Didn’t fill prescription 5%
Other 1%
Subtotal 51%
Coleman EA, Smith JD, Raha D, Min SJ. Arch Intern Med. 2005;165:1842-7.
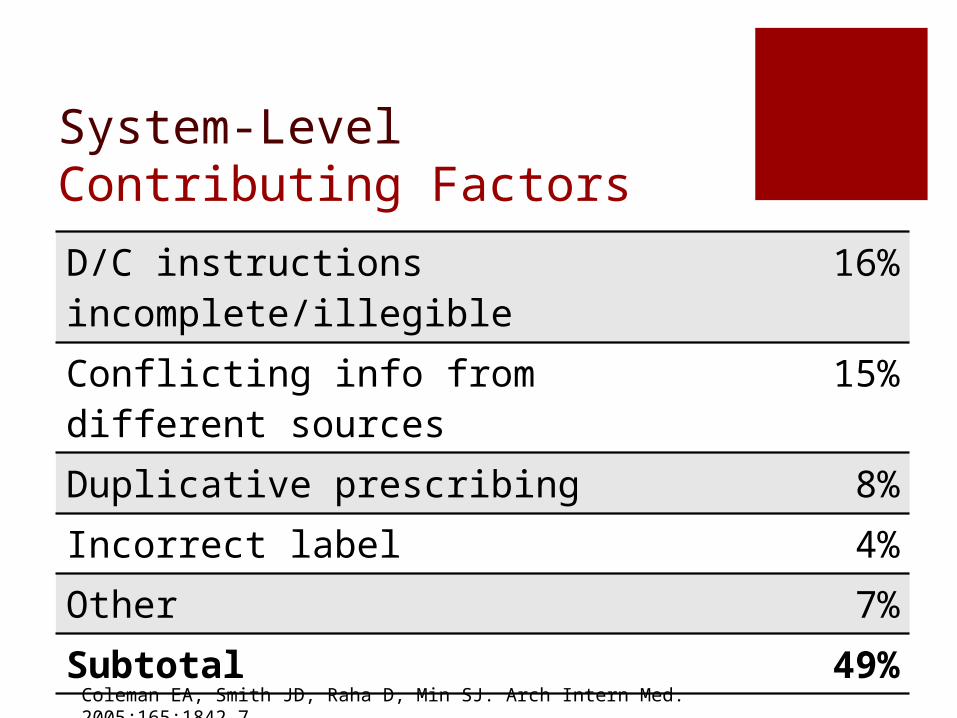
System-Level Contributing FactorsD/C instructions incomplete/illegible 16%
Conflicting info from different sources
15%
Duplicative prescribing 8%
Incorrect label 4%
Other 7%
Subtotal 49%
Coleman EA, Smith JD, Raha D, Min SJ. Arch Intern Med. 2005;165:1842-7.

Best Practices: Medication ReconciliationPharmacist involvement
Inpatient setting on intake and dischargePost-discharge assessment/follow-upIn-home review
Prioritize effortsHigh-risk patients (number of medications,
disease conditions (e.g., COPD, MI, heart failure)
High-risk medications; opioids, insulin, anticoagulants/antiplatelets, digoxin, oral hypoglycemic agents

Medication List Toolkit
www.patientsafety.org/page/109587/

Why Evaluation?
Evaluation
Improvement
Opportunities
Did process improve
the outcome
?
Performance as
expected over time
Evaluation is the conscious reflection on what we do
Evaluation ResearchMore rigorous than basic QI methods
Involves developing an evaluable model A collective effort of all stakeholders
Use of a measurement chart to identify variables
Usually involves assessing baseline performance and comparing to a post-intervention period (quasi-experimental research designs)

Evaluation Scenario
Rationale: Vulnerable elders OIG scrutiny (Medicare costs) Significant problems documented
Nursing Home
Hospital/ED
Environmental Scan For MeasuresJoint Commission
National Quality Forum
Institute for Healthcare Information
ACOVE
CMS
AHRQ
Identify Process Nodes
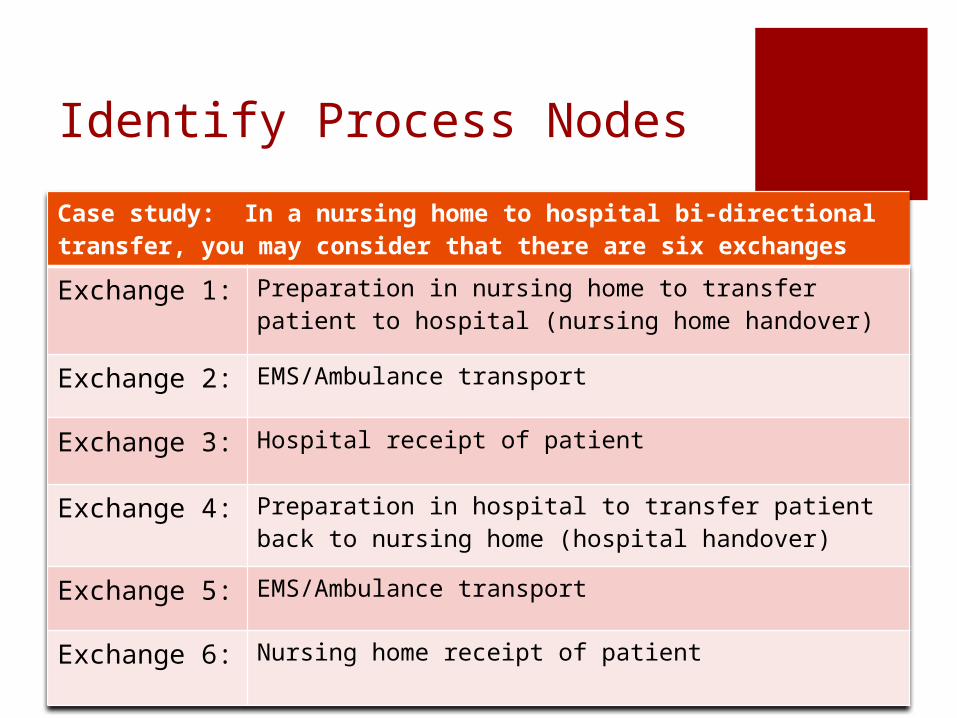
Case study: In a nursing home to hospital bi-directional transfer, you may consider that there are six exchanges
Exchange 1: Preparation in nursing home to transfer patient to hospital (nursing home handover)
Exchange 2: EMS/Ambulance transport
Exchange 3: Hospital receipt of patient
Exchange 4: Preparation in hospital to transfer patient back to nursing home (hospital handover)
Exchange 5: EMS/Ambulance transport
Exchange 6: Nursing home receipt of patient
Determine Evaluation Questions
Q 1
• Is the appropriate information being communicated to the ED/hospital by nursing home staff?
Q 2
• Is there documentation in the nursing home medical record of communication with the primary care physician about the ED/hospital transfer?
• Is there documentation in the nursing home medical record of communication with family/caregiver about transfer of the resident?
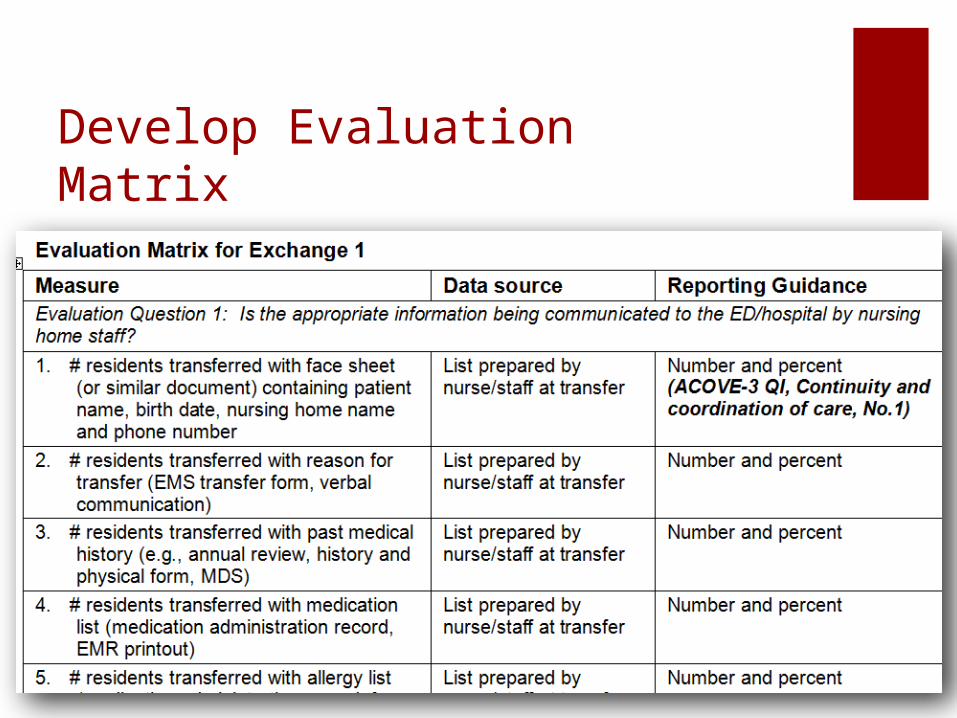
Develop Evaluation Matrix

Collect Data
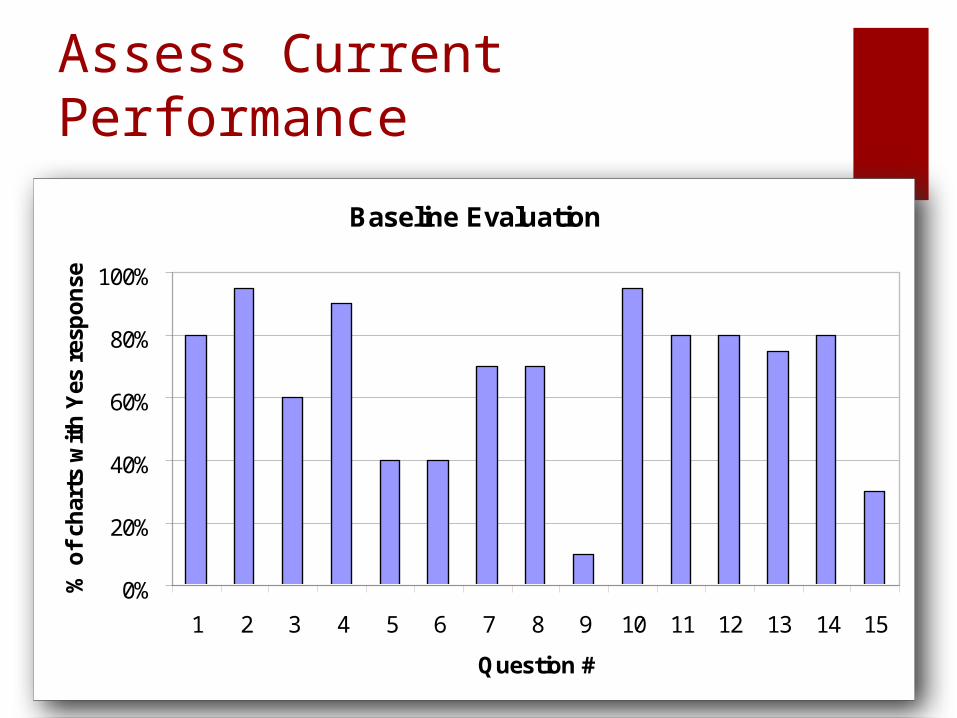
Assess Current Performance
Baseline Evaluation
0%
20%
40%
60%
80%
100%
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15
Question #
% o
f ch
arts
wit
h Y
es r
esp
on
se
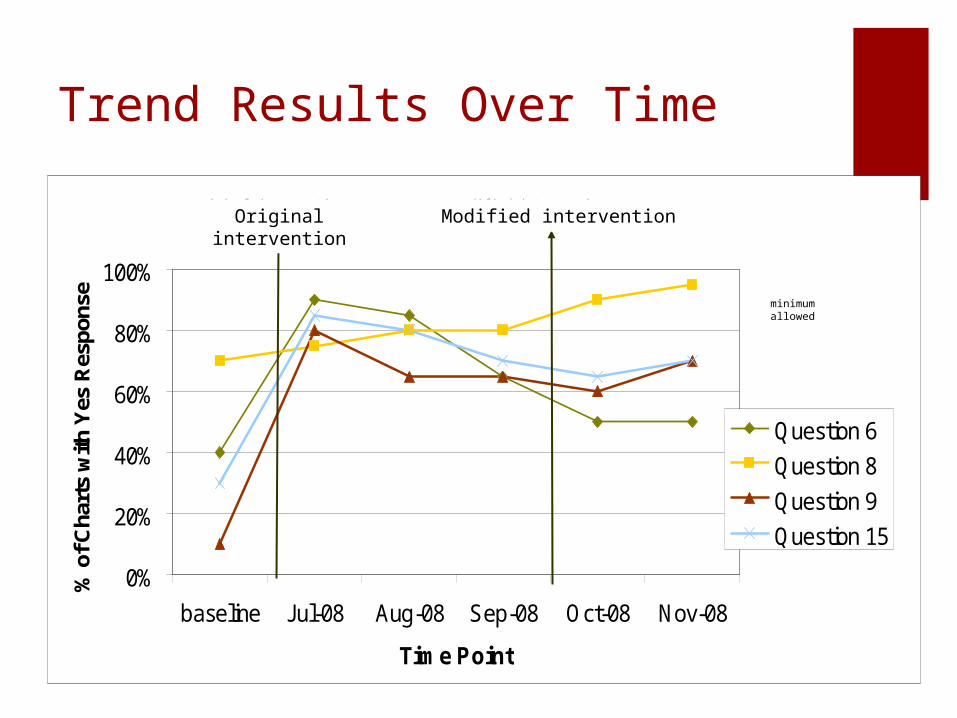
Trend Results Over Time
0%
20%
40%
60%
80%
100%
baseline Jul-08 Aug-08 Sep-08 Oct-08 Nov-08
Time Point
% o
f Cha
rts
with
Yes
Res
pons
e
Question 6
Question 8
Question 9
Question 15
minimum allowed
original intervention modified interventionOriginal intervention Modified intervention

Web-based Evaluation Tool
What Can We Do?Evaluate our own practice settingsSeek guidance of others:
Example - www.ntocc.org, www.cfmc.org/integratingcare/toolkit.htm
Assure patient has: An updated medication list at each encounter An understanding of treatment plan An understanding of their role in care
Assure providers have: An understanding of patient and caregiver preferences Knowledge of practice environment – policies, IT, etc. Access to tools to assist in improving care transitions, and hence,
communication of an accurate medication list