medicare policy and falls prevention · medicare policy and falls prevention ... falls risk...
TRANSCRIPT
1
Medicare Policy and Falls Prevention
American Occupational Therapy Association
June 7, 2010
This report was prepared by the American Occupational Therapy Association under contract with the Centers for Disease Control and Prevention, National Center for Injury Prevention and Control (CDC/NCIPC) an agency of the US. Department of Health and Human Services. The views presented do not necessarily reflect CDC policy.
4720 Montgomery Lane, Bethesda, MD 20814 301-652-2682 www.aota.org
2
Analysis of Medicare Policy in Relation to Preventing Falls Among Older Adults
I. Table of Contents ………………………………………………………………2
II. Executive Summary ………………………………………………………………3
III. Issues Summary ………………………………………………………………8
IV. Introduction ………………………………………………………………………11
V. Falls Among Older Adults: A Snapshot ……………………………………………12
VI. Falls Prevention Defined/Terminology ……………………………..………………………………13
VII. Medical Necessity and Prevention ………...………………………………….16
VIII. Communication Directed to Medicare Beneficiaries ….……………………….16
IX. Medicare Quality Initiatives- Post Acute Care (Skilled Nursing Facilities and Home Health Agencies) ………………..………………….18
A. Skilled Nursing Home Quality Initiative …………………………………………………….18
B. Home Health Quality Initiative …………………………………………………….21
X. Physician Quality Reporting Initiative (PQRI) ………………………...………………….24
XI. Payment Policy and Local Coverage Determinations ………….……………….28
A. Vitamin D ……………………………………………………..……………….28
B. Durable Medical Equipment …………………………………………….28
1. Bathroom Safety Devices ……………..…………………….29
2. Mobility Devices …………………………….……………………….30
C. Local Coverage Determinations …………………………………………….31
XII. Falls & Diagnosis Coding …………………………………………………..………….34
XIII. Coordination Among Healthcare Providers/Coordination with Community-Based Fall Prevention Programs……………………………………………………………….37
A. Coordination of Healthcare Services ………………………………..….37
B. Coordination Between Healthcare Providers and Community-Based Programs …….……………………………………………………………..…38
XIV. Healthcare Reform: New Developments ………………………………………..40
XV. Toward Enhancing Medicare Payment Policy and Utilization: Summary of Findings ……………………………………………………………..42
XVI. References ……………….……………………………………………………..43
XVII. Appendix A: Interview Compendium …………….….…………………………..46
XVIII. Appendix B: Survey of Healthcare Providers …….……………………………..52
XIX. Appendix C: Survey of AOTA members .…………………………………..57
3
Executive Summary
Falls among older adults is a growing national concern due to the social and financial cost of falls, the rapidly increasing older adult population and the expanding body of evidence that falls are preventable and falls risk can be reduced.
The National Falls-Free Action Plan (National Council on Aging, 2005) includes several goals relevant to this issue:
Develop a public policy agenda to promote falls prevention at the national, state, and local levels. (pg 10, 35)
Develop options and approaches for how Medicare and other provider systems should reimburse for physical mobility services and treatment related to falls prevention. (pg 19)
This report intends to identify how current public policy, and in particular Medicare policy, contributes to falls prevention by elucidating the influence of Medicare policy on practitioners who address falls risk, analyzing these policies, and identifying potential areas for policy enhancement or change. Content for this report is grounded in a comprehensive set of interviews with individuals representing Federal government agencies, providers, and other nonprofit organizations concerned with fall prevention in the elderly. The issues identified as policy and other barriers to effective fall prevention activities informed the identification and explication of issues in this report.
As the primary payer for health care for older adults, Medicare bears the greatest share of financial costs. Medicare policy also wields the greatest influence on healthcare services directed toward preventing falls. As both a payer and regulator, Medicare policy can require, permit, incentivize or prohibit provider actions related to falls prevention. Other federal and state policies (e.g., Medicaid) also have influence as do issues such as care coordination, community program accessibility, and research.
Effective falls prevention activities have been identified by research evidence. These activities include assessment and identification of falls risk factors and intervention to address these factors. The recommendations made in the American Geriatrics Society/British Geriatrics Society 2010 Guideline for Prevention of Falls among Older Persons are used in this report to define evidence based fall prevention activities and are frequently referenced as a guide to suggested policy changes.
Other prevention activities that are evidence-based have been identified by the Centers for Disease Control and Prevention (CDC) and are replicated in communities across the nation. The report discusses intersection of these programs and the healthcare systems. Key issues raised in interviews conducted by the project and identified through policy analysis activities can be grouped into the following areas:
Medical Necessity and Communication with Beneficiaries
A fundamental tenet of Medicare coverage policy is the concept of “medical necessity,” defined as items or services “reasonable and necessary for the diagnosis or treatment of illness or injury or to improve the functioning of a malformed body member.” (42 U.S.C. 1395y [a]) Prevention activities do not meet the definition of medical necessity per se and are usually covered by Medicare only when specifically included by law, creating an inherent tension between falls prevention activities and Medicare coverage.
In communications directed to beneficiaries, Medicare policy regarding falls and falls prevention is discussed only in limited ways. The Welcome to Medicare exam (Initial Preventive Physical Exam/IPPE) must include falls risk assessment, but communications to beneficiaries
4
about this benefit do not mention falls and fail to prepare beneficiaries that falls risk will be addressed during this important encounter or to educate them about the importance of considering falls in the overall health evaluation. In communications regarding preventive services and health assessment, specific mention of falls risk can help beneficiaries understand that falls are preventable and that falls are a concern that is appropriately addressed with a health provider.
Quality Initiatives
Quality initiatives in post-acute care settings (skilled nursing facilities [SNF] and home health [HH] agencies) promoted by the Centers for Medicare and Medicaid Services (CMS) have incorporated falls surveillance into mandated assessment and data collection activities. Recent revisions of the federally mandated data collection tools for these settings (Minimum Data Set [MDS] 3.0 and Outcomes and Assessment Information Set [OASIS] Version C) encourage providers to assess falls risk and to plan interventions that may reduce falls risk.
In SNFs, there is the potential to obtain rich data on falls risk and falls intervention, supplementing the limited or inconclusive data available from existing research. However, the mandated Care Area Assessment (CAA) component of the SNF data gathering tool may inadvertently obscure or complicate the process of identifying relevant falls risk factors due to the breadth of potential factors to be considered by the care team. Refining the CAA to more closely align with recognized risk factors would reduce confusion as well as burden. There is also strong evidence that SNF residents at risk of falls benefit from Vitamin D supplementation. Coverage of Vitamin D for SNF residents determined to be at risk of falls should be addressed as part of SNF Part A payment.
There is also potential for more data to be collected regarding falls risk and falls intervention among beneficiaries receiving home healthcare. CMS has announced plans to require home health agencies to publicly report a home health process measure related to falls. This is expected to be implemented in the near future. Monitoring this will further incentivize falls risk intervention by home health agencies. Resources provided to home health agencies by CMS should be updated to incorporate the most current evidence-based practices. Given that outcomes data currently are limited to outcomes achieved at the time of discharge from home health, consideration should be given to monitoring service usage and claims data post-discharge to determine if home health outcomes, including those related to falls, are sustained by the patient beyond the termination of home healthcare. Home health agencies also are a strong point of referral to community-based falls programs; a capacity that should be strengthened.
The Physician Quality Reporting Initiative (PQRI) is a voluntary program that incentivizes providers for consistently implementing specific care processes. Falls risk assessment and a falls risk intervention plan are two PQRI care process measures. However, the care processes that PQRI requires for the falls intervention plan measure are not consistent with current best evidence; because providers are encouraged to follow these processes, this measure may actually promote care processes that are not recommended. The new AGS Guideline had not been published at the time of the development of the falls-related PQRI measures. It is essential that any care processes incentivized by payment be updated so they are consistent with current evidence.
Coverage Policies and Local Coverage Determinations (LCD)
There is strong evidence that Vitamin D supplementation is a powerful intervention to reduce falls risk, among both community-dwelling older adults and those living in residential care settings. Variation across Part D plans has made it more difficult for SNFs to obtain all the
5
medications and supplements prescribed for their residents. Vitamin D is not on the formulary of any Part D plan examined. Given the very low cost of Vitamin D, the significant cost benefit in terms of falls risk reduction, consideration of Part D policies in this regard could promote higher utilization of Vitamin D when appropriate in SNFs or in community dwelling older adults.
Provision of durable medical equipment (DME) may be an appropriate falls prevention intervention either to improve mobility safety (canes, walkers, rollators or wheelchairs) or to modify the environment to reduce risk (bath seats, grab bars, elevated toilet seats) during self-care activities. Medicare covers mobility devices, but restricts how often they may be covered or replaced. Specifically, there is no coverage for a device if another similar device has been paid for in the preceding 5 years, even if the other device is no longer adequate or appropriate. There also is no coverage if the beneficiary needs two different devices (e.g., a cane during the day, a walker at night) to meet the mobility demands of the home environment. Bathroom DME is not covered and is considered not reasonable and necessary. However, given the costs associated with falls in the bathroom, and the undesirable alternatives beneficiaries face when they cannot safely access bathroom fixtures for personal care, a reconsideration of “reasonableness” of bathroom DME coverage is appropriate.
Local coverage determinations (LCD) are interpretations of Medicare policy established by Medicare Administrative Contractors (MACs). They particularly affect Part B outpatient services. There are discrepancies and inconsistencies among LCDs that affect falls intervention. Many restrict the provision of services such as occupational therapy and physical therapy to address falls risk evaluation in the home environment or the provision of these services for an individual who is generally “at risk” for falls but has no particular fall-related diagnosis.
Of particularly concern is one LCD for outpatient occupational therapy that explicitly excludes occupational therapy evaluation from coverage if it is “for” items or services that are non-covered. This means that during an occupational therapy evaluation, practitioner recommendations for a non-covered item, such as a bathing chair or a grab bar, might result in the evaluation being denied as a covered service. Some of the strongest research evidence for modifying the home environment to reduce falls risk is based on intervention protocols that include an occupational therapy assessment in the home and implementation of environmental modifications. Non-coverage of assessment based on the coverage status of a particular piece of equipment poses ethical concerns and may deny beneficiaries information about helpful recommendations for equipment or modifications that may be covered by other payers or that they may choose to purchase out of pocket.
There are also discrepancies among LCDs regarding recognition and use of the ICD-9-CM code for falls history/falls risk (V15.88) as a diagnosis that demonstrates need for occupational therapy, physical therapy, or other services. This restricts access to services and also restricts data gathering capabilities. (See next section.)
Overall, ensuring consistency among and between LCDs is an important issue. Such efforts also should ensure that LCDs reflect current evidence and do not restrict coverage of an evaluation because of what that evaluation or assessment might recommend (e.g., non-covered bath chairs).
Falls Coding
CMS working with CDC’s National Center for Injury Prevention and Control was proactive in the creation of an ICD-9-CM code V15.88 to indicate falls history and elevated falls risk. The code was implemented in 2005, but is not widely known or used by providers. By definition, V15.88 does not indicate a true “diagnosis” or denote “medical necessity” as defined in Medicare statutes, but is important both to identify patients at risk of falls and for surveillance
6
and research activities. Another coding issue is the use of E880 series codes, which are supplemental codes to indicate circumstances of an injury. These codes are used at the discretion of the provider or facility, but are not widely used. Increased efforts to educate providers and to promote use of these codes would assist coordination of care for beneficiaries who are at risk of falls and would support falls surveillance efforts nationwide.
Coordination among Providers and With Community Based Programs
There is currently little coordination among healthcare providers in regard to fall prevention efforts. Coordination too often is little more than a prescription or a referral to other healthcare providers. In some cases, coordination is complicated by regulatory mandates or coverage criteria that differs among settings. For example, emergency care providers often identify falls risk when beneficiaries present to an emergency department after a fall. Emergency providers may initiate referrals for aftercare and follow-up, but such care may require that the individual’s personal or primary physician provide ongoing coordination and oversight of such care. Health care in the home may be preferred by the beneficiary, but beneficiaries will not qualify for the home health benefit if they are not homebound. Part B services, separate from the home health benefit, are by law allowed to be provided in the beneficiary’s home. Many providers, such as hospital outpatient departments, do not allow for provision in the home. These barriers to effective referral and coordination increase the likelihood that beneficiaries who have had a fall may not receive appropriate follow-up to reduce the risk of another fall.
There is a relatively sharp divide between health services delivered by healthcare providers and systems and social or human services delivered by community organizations such as non-profit agencies, aging services networks, governmental entities, and faith communities. There are a growing number of community-based fall prevention programs, based on research evidence, that provide effective, accessible fall-prevention services. However, too often, healthcare providers are unaware of these programs and therefore fail to refer individuals who might benefit. Efforts should be made to educate both providers and beneficiaries about these programs and to encourage providers to refer beneficiaries to such programs when appropriate. Consideration should also be given to incentivizing providers (clinicians and provider organizations) to join local and national falls prevention coalitions, such as the Falls Free Coalition.
New Preventive Benefit
The Patient Protection and Affordable Care Act of 2010 (PPACA) (P.L. 111-148) includes provisions favorable to falls prevention efforts. The PPACA creates a new Medicare preventive benefit, an annual preventive care visit. Section 4103 of PPACA authorizes not only an annual preventive visit, but also requires a personal prevention plan. Other provisions in this section make health risk screening, as well as prevention services, more accessible. There also is a potential for stronger linkages to community programs and community-based service delivery systems.
Summary
Falls prevention is a complex, multifactorial, social and health problem. Fall prevention is not a discrete incident, but rather a process. While a fall itself may be an acute event, falls prevention and falls risk management is largely a self management process that requires self management support, including professional interventions, similar to management of chronic conditions. Policy issues identified by the project and examined in this report are clustered around payment for services under healthcare programs, even as many other policies (community program funding, research priorities, etc.) also affect the status of falls prevention

7
activities. Falls prevention is explicitly or implicitly addressed across a range of Medicare regulations, initiatives, and coverage guidelines.
Ongoing Medicare quality initiatives are providing influence on provider behavior and have potential to further incentivize care processes that incorporate falls risk assessment and falls risk reduction. Because Medicare directives and instructions have such a strong influence on provider behavior, it is essential that such materials be consistent with current evidence and best care practices, such as those in the AGS Guideline. A number of Medicare coverage policies have an impact on efforts to reduce falls risk, though their relationship to falls prevention may not be immediately apparent. Policies related to Vitamin D supplementation, DME, and therapy services appear to restrict intervention in reaction to a problem, and furthermore are based on the assumption that medically necessary interventions must be directed toward body structures and functions rather than behavior or the environment.
Current evidence indicates multiple factors are involved in effective falls risk assessment, addressing biology, behavior, and environment. In light of the cost of falls in health, social, and economic terms, it seems appropriate to reconsider these policies and also to encourage increased coordination with community-based fall prevention efforts. Adoption of a falls risk/falls history ICD-9-CM code to supplement V15.88 benefits those who are at risk and supports surveillance and research. More provider education is needed to promote widespread, consistent use of appropriate codes related to falls. Recent legislation creating a Medicare annual preventive assessment and preventive health plan is a significant positive step toward more accessible, coordinated and effective falls prevention efforts. Provider education also is a key area where policy can have a positive effect in promoting understanding and awareness of all related dimensions of fall prevention, from individual health care, to community planning, to social and related community resources.
8
Issues Summary
Identified Falls Prevention Strengths in Medicare Policy:
Strength 1: Specific inclusion of falls risk assessment in the required elements of the Welcome to Medicare examination (Initial Preventive Physical Exam/IPPE).
Strength 2: Falls risk assessment and intervention is promoted in the recent revision of the Minimum Data Set (MDS) Version 3.0, which is mandated for use in all Medicare-certified skilled nursing facilities.
Strength 3: Falls risk assessment and intervention is promoted in the recent revision of the Outcomes and Assessment Information Set (OASIS) Version C, which is mandated for use by all Medicare-certified home health agencies.
Strength 4: Inclusion of a falls-related patient outcome item on Home Health Compare promotes falls assessment and intervention by Medicare-certified home health agencies.
Strength 5: Inclusion of two falls-related items in the Physician Quality Reporting Initiative (PQRI) promotes and incentivizes physician and other enrolled Medicare providers to implement falls risk assessment and intervention.
Strength 6: Palmetto GBA, a Medicare Administrative Contractor (MAC), has promoted falls prevention by recognizing the falls risk ICD-9CM code (V15.88) in local coverage determinations (LCDs) and has offered guidance to providers to promote falls prevention efforts within the current limitations of Medicare coverage policies. Palmetto’s “Going Beyond Diagnosis” educational initiative, which integrates the International Classification of Functioning, Disability and Health (ICF) (World Health Organization (WHO), 2001) with local coverage policies, offers a rubric for addressing the biological, behavioral and environmental aspects of fall prevention consistent with Medicare coverage requirements.
Identified Issues with Possible Solutions:
Issue 1: In communications directed to beneficiaries, Medicare could improve its emphasis and clarity with regard to policy regarding falls and falls prevention.
Possible Solution: In communications regarding preventive services and health assessment, specific mention of falls risk would better inform and prepare beneficiaries. It is critical that beneficiaries understand that falls are preventable and a concern to be addressed with a health provider. Efforts should be made to increase beneficiary awareness of falls risk and the falls risk assessment included in the Welcome to Medicare visit and, once implemented, the annual wellness visit authorized by the Patient Protection and Affordable Care Act (PPACA).
Issue 2: Many providers are unaware of the importance of fall risk assessment and prevention.
Possible Solutions: Increase provider education to promote awareness and understanding of the importance of falls risk assessment and follow-up with a falls risk intervention plan.
Issue 3: In home health under Medicare, increase emphasis on the importance of establishing a trajectory for the patient and/or family to sustain the outcome (e.g., continue to implement falls risk management strategies) beyond the point at which the home health agency discharges.
Possible Solutions:
9
1) Promote referral to community-based evidence-informed falls prevention programs on discharge from home health;
2) Taper intervention intensity during the home health episode, gradually transferring falls prevention actions to the patient and family; and
3) Include a follow-up or “booster” intervention following home health discharge.
Issue 4: Sustainability of outcomes is an area not addressed by the Home Health Quality Initiative. There is no mechanism to collect data (about falls or any other patient status indicator) after the home health episode ends to determine, for instance, if the self-care and safety interventions provided during the home health episode have been continued or are effective.
Possible Solution: Given that outcomes data currently are limited to outcomes achieved by the time of discharge from home health, consideration should be given to monitoring service usage and claims data post-discharge to determine if home health outcomes, including those related to falls, are sustained by the patient beyond the termination of home health care.
Issue 5: Fall prevention services may appropriately fall under the “medical necessity” requirement for Medicare coverage, but should also be addressed under the category of preventative care. This creates an inherent tension between providing assessment or intervention to prevent falls, whereas medical necessity is based on diagnosis and treatment of an illness, injury, or malformation of a body part.
Possible Solution: Create a falls risk prevention/intervention benefit that includes occupational, physical/therapy, durable medical equipment (DME), vitamin D, and is coordinated with community-based fall prevention programs. The benefit could be triggered by identification of falls risk (V15.88) and would include a list of available services that address the beneficiary’s falls risk factors and would be covered even in the absence of a specific “medically necessary” diagnosis.
Issue 6: There is currently little coordination among healthcare providers in regard to fall prevention efforts. Coordination and follow-up too often is little more than a prescription or a referral to other healthcare providers.
Possible Solutions: Efforts should be made to educate both providers and beneficiaries about the fall prevention programs and resources available in the community. These programs include falls prevention clinics and programs offered by health care facilities and practitioners and community-based lay-led programs. Priority should be to refer to evidence-based programs. Providers should be encouraged to refer beneficiaries to such programs when appropriate. Falls prevention should be a key issue as CMS implements the various care coordination or medical home demonstrations authorized in the PPACA. Of particular concern are referrals from hospital emergency room visits, where the treating physician has no link to the patient after the visit. Wherever evidence-informed or evidence-based fall prevention programs are available, any beneficiary deemed able to participate should be referred to such programs. Consideration should also be given to encouraging providers (clinicians and provider organizations) to join local falls prevention coalitions.
Issue 7: The code indicating fall risk was implemented in 2005, but is not widely known or used by providers. By definition, the code, V15.88, does not indicate a true “diagnosis” or denote “medical necessity” as defined in Medicare statutes, but is important both to identify patients at
10
risk of falls and for surveillance and research activities. E880 series codes are supplemental codes to indicate circumstances of an injury. These codes are used at the discretion of the provider or facility and are also not widely used.
Possible Solutions: Promote use of the V code among all health care providers. Promoting the use of E falls codes, especially by emergency, urgent, and primary care providers which can aide in research and tracking.
Issue 8: There are discrepancies and inconsistencies between and among LCDs that affect falls intervention. There also are discrepancies in LCDs regarding recognition and use of the ICD-9-CM code for falls history/falls risk.
Possible Solutions: Efforts should be made to ensure consistency among and between LCDs. Such efforts should also ensure that LCDs reflect current evidence and do not base coverage of an evaluation on the possible outcomes of such assessment.
Issue 9: Variation across Medicare Part D plans has made it more difficult for skilled nursing facilities (SNF) to obtain all the medications prescribed for their residents. Vitamin D is not on the formulary of any Part D plan examined. Part A does not pay for vitamin supplementation.
Possible Solution: Given the very low cost of Vitamin D and the significant cost benefit in terms of falls risk reduction, policies should be considered that would ensure that SNF residents have access to Vitamin D and promote availability of Vitamin D for community-dwelling beneficiaries.
Issue 10: Classifying DME such as grab bars and bath benches as “presumptively nonmedical” may not be cost beneficial when considered from a falls prevention perspective.
Possible Action: Consider a change in coverage policy to include these items as covered DME. It is important to note that some of these items (bath seats, transfer benches, grab bars, and raised toilet seats) have been assigned Health Care Common Procedure Codes (HCPCS) and are covered by Medicaid in a number of states (e.g. North Carolina, New York, Hawaii). The DME component could include mobility devices regardless of prior receipt and would also include bathroom safety devices that have assigned HCPCS codes.
Issue 11: Mobility devices are covered by Medicare, but with restrictions on how often they are covered, meaning there is no coverage for a device if another device has been paid for in the preceding 5 years, even if the other device is no longer adequate or appropriate.
Possible Solution: Adjust reimbursement to allow for issues such as changing weight or height to allow for replacement or the need for more than one device. In addition, appropriate initial and follow-up instructions are needed to ensure that device use is integrated well into routines and habits and do not inadvertently increase falls risk.
Issue 12: Emergency Department (ED) physicians make home health referrals to initiate intervention after an older adult presents to an ED having fallen, but without serious injury requiring hospitalization. In some cases, services may not be provided due to home health benefit requirements (e.g., homebound status).
Possible Solution: Encourage home health and other providers to offer Part B outpatient therapy services in home settings, as allowed under current law, for follow-up after other episodes of care.
11
Introduction
In the early 1990s, a television commercial featured an older woman lying on the floor calling “Help! I’ve fallen and I can’t get up.” The advertisement was for a personal emergency response system. But instead of calling attention to either the problem or the product, the catchphrase became part of popular culture, mocking frailty associated with aging and suggesting helplessness or hopelessness.
In the first decade of the 21st Century, falls among older adults have drawn more serious attention from healthcare professionals, policy makers, public health authorities, social service providers, families and caregivers of older adults, and older adults themselves. Several factors have contributed to this increased attention: the growing number of older adults who wish to remain independent, the increasing social and economic costs of falls, and a growing body of evidence indicating that falls are preventable and not a normal aspect of aging. Attention to falls has contributed to the formation of a National Falls Free Coalition, the passage of the Safety of Seniors Act of 2007 (P.L.110-102), and inclusion of falls risk screenings or assessments in preventive Medicare benefits authorized by the Medicare Improvements for Patients and Providers Act of 2008 (PL-110-102) and the Patient Protection and Affordable Care Act of 2010 (PL 111-148).
The purpose of this document is to identify and analyze Federal policy issues in relation to falls prevention and treatment services. As the primary insurer for nearly all older adults in the US and the single largest purchaser of health care, Medicare has a considerable influence on how falls are addressed. Medicare is both a payer and a regulator, so policies include not solely whether a given service or device is covered, but also what provider actions are required, permitted, incentivized or prohibited. The analysis begins with communications from Medicare directed to beneficiaries, as these frame the beneficiary’s understanding of his or her benefits. The analysis continues with quality initiatives incorporated in regulatory or payment policy and finally, coverage policies.
Here is a brief overview of the problem of falls among older adults. Further, issues of coordination within the healthcare system and between the healthcare system and community-based falls prevention services will also be analyzed.
12
Falls Among Older Adults: A Snapshot
More than one third of adults 65 and older fall each year in the United States (Hausdorff, Rios, & Edelberg, 2001; Hornbrook, et al., 1994).
Among older adults, falls are the leading cause of injury deaths. They are also the most common cause of nonfatal injuries and hospital admissions for trauma (Centers for Disease Control and Prevention [CDC], 2005).
In 2005, 15,800 people 65 and older died from injuries related to unintentional falls; about 1.8 million people 65 and older were treated in emergency departments for nonfatal injuries from falls, and more than 433,000 of these patients were hospitalized (CDC, 2005).
Outcomes Linked to Incidence of Falls
Twenty percent to 30% of people who fall suffer moderate to severe injuries such as bruises, hip fractures, or head traumas. These injuries can make it hard to get around and limit independent living. They also can increase the risk of early death (Alexander, Rivara, & Wolf, 1992; Sterling, O'Connor, & Bonadies, 2001).
Falls are the most common cause of traumatic brain injuries, or TBI (Jager, Weiss, Coben, & Pepe, 2000). In 2000, TBI accounted for 46% of fatal falls among older adults (J. Stevens, Corso, Finkelstein, & Miller, 2006).
Most fractures among older adults are caused by falls (Bell, Talbot-Stern, & Hennessy, 2000).
The most common fractures are of the spine, hip, forearm, leg, ankle, pelvis, upper arm, and hand (Scott, 1990).
Many people who fall, even those who are not injured, develop a fear of falling. This fear may cause them to limit their activities, leading to reduced mobility and physical fitness, and increasing their actual risk of falling (Vellas, Wayne, Romero, Baumgartner, & Garry, 1997).
Cost of Falls in Older Adults
In 2000, direct medical costs totaled $0.2 billion ($179 million) for fatal falls and $19 billion for nonfatal fall injuries ( Stevens, et al., 2006). Direct costs are what patients and insurance companies pay for treating fall-related injuries. These costs include fees for hospital and nursing home care, doctors and other professional services, rehabilitation, community-based services, use of medical equipment, prescription drugs, changes made to the home, and insurance processing.
Direct costs do not account for the long-term effects of these injuries such as disability, dependence on others, lost time from work and household duties, and reduced quality of life.
The preceding information was taken directly from the CDC Fact Sheet: Falls Among Older Adults: An Overview, available on the CDC website: http://www.cdc.gov/HomeandRecreationalSafety/Falls/adultfalls.html. Given that Medicare is the primary insurer for nearly all older adults over the age of 65, Medicare bears the greatest share of the direct medical costs for falls, further straining its resources when preventive actions could help to reduce costs.
13
Fall Prevention Defined/Terminology
Current research on falls and falls prevention indicates that falls are multi-factorial. There is a growing body of research to identify factors contributing to falls, to assess or screen for individual falls risk, and to identify effective falls prevention services or interventions. As awareness of the falls problem increases, so too does the number of devices and services being promoted to prevent falls. In order to analyze current policies in relation to falls, the first question to be asked is “what constitutes fall prevention?”
For the purposes of this report, “fall prevention activities” are defined as items, services or programs for which there is credible evidence that application or implementation reduces falls risk. The recently released American Geriatric Society (AGS)/British Geriatric Society (BGS) Clinical Practice Guideline: Prevention of Falls in Older Persons (2010) was used primary resource to identify such fall prevention activities and provides a framework for this analysis.
The 2010 AGS/BGS Guideline updated an earlier guideline published in 2001 (American Geriatrics Society, British Geriatrics Society & American Academy of Orthopedic Surgeons) and included research conducted on falls prevention since the earlier guideline. A preliminary draft of the 2010 Guideline was peer reviewed by the American Academy of Family Physicians, American Academy of Home Care Physicians, American Academy of Ophthalmology, American Academy of Otolaryngology, American Academy of Physical Medicine and Rehabilitation, American College of Emergency Physicians, American College of Physicians, American Medical Association, American Occupational Therapy Association, American Physical Therapy Association, British Association for Emergency Medicine, Chartered Society of Physiotherapists, College of Occupational Therapists (UK), National Association for Home Care and Hospice, Gerontological Advanced Practice Nurses Association, Royal Pharmaceutical Society of Great Britain, Society for Academic Emergency Medicine, and the Society for General Internal Medicine.
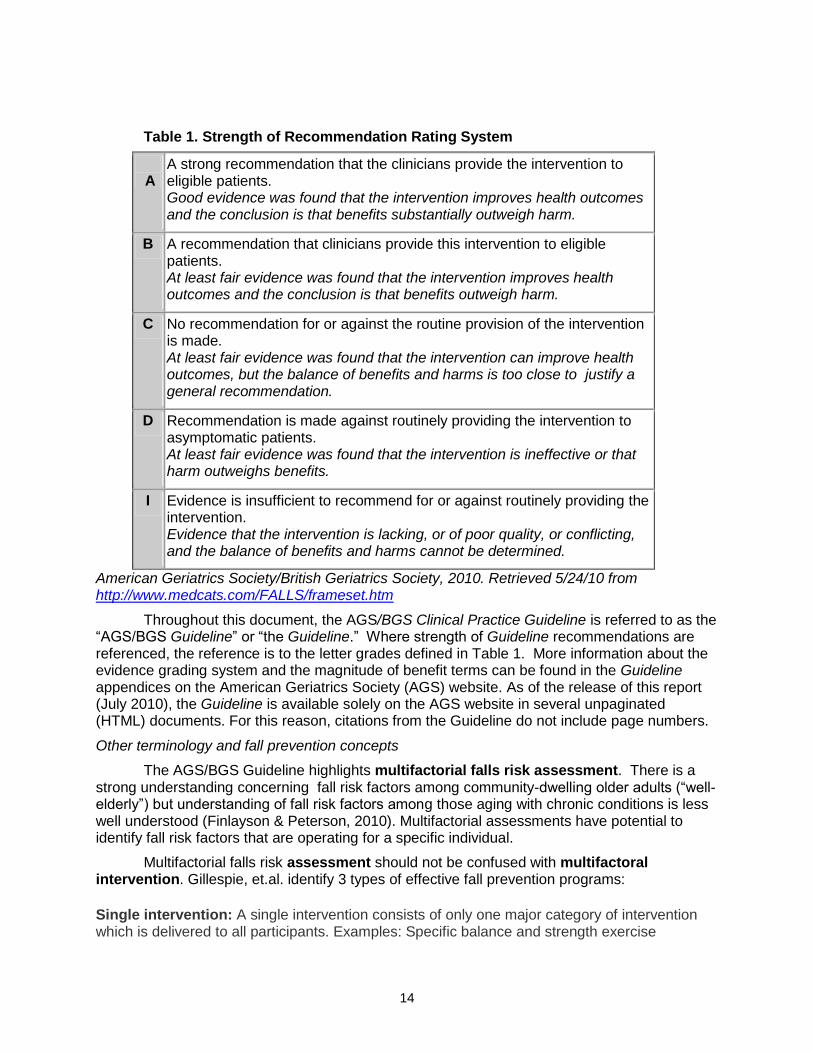
The panel used a standardized format for grading the strength of recommendations, based on an evidence rating system used by the US Preventive Services Task Force (USPSTF) (Harris, et al., 2001), to critically analyze the research literature and grade the evidence. The grade for the strength of a recommendation is based on both the overall quality of the evidence and on the magnitude of net benefit. The grades are defined in the following table:
14
Table 1. Strength of Recommendation Rating System
A
A strong recommendation that the clinicians provide the intervention to eligible patients. Good evidence was found that the intervention improves health outcomes and the conclusion is that benefits substantially outweigh harm.
B A recommendation that clinicians provide this intervention to eligible patients. At least fair evidence was found that the intervention improves health outcomes and the conclusion is that benefits outweigh harm.
C No recommendation for or against the routine provision of the intervention is made. At least fair evidence was found that the intervention can improve health outcomes, but the balance of benefits and harms is too close to justify a general recommendation.
D Recommendation is made against routinely providing the intervention to asymptomatic patients. At least fair evidence was found that the intervention is ineffective or that harm outweighs benefits.
I Evidence is insufficient to recommend for or against routinely providing the intervention. Evidence that the intervention is lacking, or of poor quality, or conflicting, and the balance of benefits and harms cannot be determined.
American Geriatrics Society/British Geriatrics Society, 2010. Retrieved 5/24/10 from http://www.medcats.com/FALLS/frameset.htm
Throughout this document, the AGS/BGS Clinical Practice Guideline is referred to as the “AGS/BGS Guideline” or “the Guideline.” Where strength of Guideline recommendations are referenced, the reference is to the letter grades defined in Table 1. More information about the evidence grading system and the magnitude of benefit terms can be found in the Guideline appendices on the American Geriatrics Society (AGS) website. As of the release of this report (July 2010), the Guideline is available solely on the AGS website in several unpaginated (HTML) documents. For this reason, citations from the Guideline do not include page numbers.
Other terminology and fall prevention concepts
The AGS/BGS Guideline highlights multifactorial falls risk assessment. There is a strong understanding concerning fall risk factors among community-dwelling older adults (“well-elderly”) but understanding of fall risk factors among those aging with chronic conditions is less well understood (Finlayson & Peterson, 2010). Multifactorial assessments have potential to identify fall risk factors that are operating for a specific individual.
Multifactorial falls risk assessment should not be confused with multifactoral intervention. Gillespie, et.al. identify 3 types of effective fall prevention programs:
Single intervention: A single intervention consists of only one major category of intervention which is delivered to all participants. Examples: Specific balance and strength exercise

15
programs, services of an occupational therapist or physical therapist, vitamin D supplementation.
Multifactorial intervention: An intervention made up of a set of interventions that are selected and offered to an individual to address the specific risk factors identified through a multifactorial fall risk assessment.
Multicomponent intervention: A set of interventions addressing more than one intervention domain or category offered to all participants in a program. Examples: Matter of Balance, Stepping On. (2009).
16
Medical Necessity and Prevention
The Social Security Act specifies that “medical necessity” is a prerequisite for Medicare to cover any service. Medical necessity is defined in Sec. 1862. [42 U.S.C. 1395y] (a)
Notwithstanding any other provision of this title, no payment may be made under part A or part B for any expenses incurred for items or services—(1) (A) which, except for items and services described in [a succeeding] subparagraph, are not reasonable and necessary for the diagnosis or treatment of illness or injury or to improve the functioning of a malformed body member (emphasis added).
Prevention activities do not meet the definition of medical necessity per se and are usually covered by Medicare only when specifically included by law, creating an inherent tension between falls prevention activities and Medicare coverage. The only exceptions to this policy are specifically identified in statute. In recent years Congress authorized specific exceptions for vaccines for influenza and pneumonia and screening procedures for cancers of the cervix, prostate, breast, and colon and for cardiovascular or endocrine conditions. However, the passage of the Medicare Improvements for Patients and Providers Act of 2008 (MIPPA) established a broader context for coverage of preventive services. MIPPA for the first time authorized the Secretary of Health and Human Services (HHS) to extend coverage to additional preventive services through the national coverage determination process if:
The Secretary determines them to be reasonable and necessary for the prevention or early detection of an illness or disability;
They are recommended with a grade of A or B by the United States Preventive Services Task Force (USPSTF), a task force of the Agency for Healthcare Research and Quality); and
They are appropriate for individuals entitled to benefits under Medicare Part A or enrolled under Part B. (Centers for Medicare & Medicaid Services, 2008a).
Falls prevention is not a singular service, so is not as easily defined as a vaccine or a screening procedure. Falls prevention is a process and a set of services or activities that depend on the specific falls risk profile of the individual and may take place over time, much as the management of chronic illness is provided. At this time, the Welcome to Medicare examination (Initial Patient Preventive Physical Exam [IPPE]) is the only Medicare-covered service that addresses falls risk solely as a preventive measure. In the recent Patient Protection and Affordable Care Act (P.L. 111-148), commonly known as PPACA, a “wellness visit” has been added to Medicare that includes a statutory reference to falls prevention. But all other services fall under the “medical necessity” requirement; therefore, providing assessment or intervention to prevent falls is somewhat restricted when medical necessity is based strictly on diagnosis and treatment of an illness, injury, or malformation of a body part.
Communications Directed to Medicare Beneficiaries
Key communications directed to Medicare beneficiaries include the Medicare.gov website (www.medicare.gov) and the Medicare and You (CMS, 2010a) guide, a publication mailed to all Medicare beneficiaries every year. As referenced above, beneficiaries have access to the IPPE/ “Welcome to Medicare” examination. This benefit is available during the first 12 months after enrolling in part B. Guidance from CMS to providers states that falls risk assessment is a mandated component of the IPPE (CMS, 2010b). However, the information provided to recipients about the IPPE does not mention this aspect of the assessment (Medicare, n.d.).

17
Evidence suggests that some older adults do not perceive falls as preventable, but instead as either an inevitability of aging or as a personal failing. Some older adults deny experiencing falls, fearing that to do so concedes loss of independence (Stevens, Noonan & Rubenstein, 2010). Information about falls risk and falls prevention is not included in the IPPE preparatory materials and in the Medicare & You handbook. The lack of mention of falls and falls risk in the Medicare beneficiary materials may leave beneficiaries feeling confronted or vulnerable when asked about falls during the IPPE. Further these materials miss an opportunity to prepare or to educate beneficiaries that falls risk will be addressed during the important encounter as well as educating them about the importance of consideration of falls in overall health evaluation. Providing this information in the handbook would prepare beneficiaries for this aspect of the exam. Including information about falls in these communications would reframe falls as preventable, not inevitable, and as a concern that is appropriately addressed with a health provider.
18
Medicare Quality Initiatives in Post-Acute Care (Skilled Nursing Facilities and Home Health Agencies)
Medicare has mandated tools to be incorporated into patient assessment in certain post- acute care settings as a condition of participation in the Medicare program. These tools are used for multiple purposes, but one important purpose is to provide data that reflects or is a proxy for care quality. These efforts are known as quality initiatives. Quality initiatives and the behaviors they promote have a powerful influence on clinicians’ perceptions of best clinical practice. Currently, reports on quality measures are available to provider organizations (their own and national comparison data) and to state surveyors who examine compliance with Medicare and state regulations. In addition, a small number of measures are reported publicly to provide Medicare beneficiaries, their families, and their providers with information about the quality of care provided in Medicare-certified skilled nursing facilities (Nursing Home Compare: www.medicare.gov/nursinghomecompare) and home health agencies (Home Health Compare: www.medicare.gov/homehealthcompare). These publicly available reports allow users to compare providers in their community based on the providers’ performance on a select set of patient outcome measures. In skilled nursing facilities, the data collection tool is the Resident Assessment Instrument (RAI), including the Minimum Data Set (MDS). In home health agencies, the tool is the Outcomes and Assessment Information Set (OASIS). These data sets and resulting quality indicators have directed provider attention to falls risk among patients and recognition of prevention of falls as a key quality indicator.
Skilled Nursing Home Quality Initiative
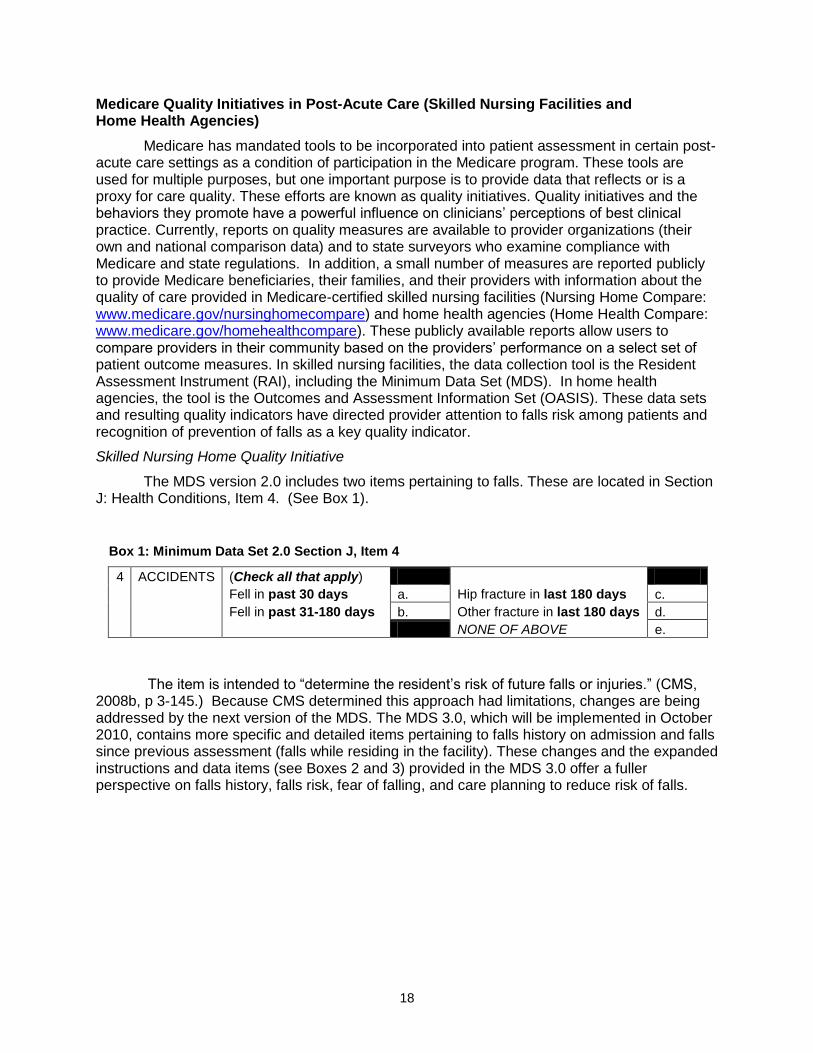
The MDS version 2.0 includes two items pertaining to falls. These are located in Section J: Health Conditions, Item 4. (See Box 1).
The item is intended to “determine the resident’s risk of future falls or injuries.” (CMS, 2008b, p 3-145.) Because CMS determined this approach had limitations, changes are being addressed by the next version of the MDS. The MDS 3.0, which will be implemented in October 2010, contains more specific and detailed items pertaining to falls history on admission and falls since previous assessment (falls while residing in the facility). These changes and the expanded instructions and data items (see Boxes 2 and 3) provided in the MDS 3.0 offer a fuller perspective on falls history, falls risk, fear of falling, and care planning to reduce risk of falls.
Box 1: Minimum Data Set 2.0 Section J, Item 4
4 ACCIDENTS (Check all that apply)
Fell in past 30 days a. Hip fracture in last 180 days c.
Fell in past 31-180 days b. Other fracture in last 180 days d.
NONE OF ABOVE e.
19
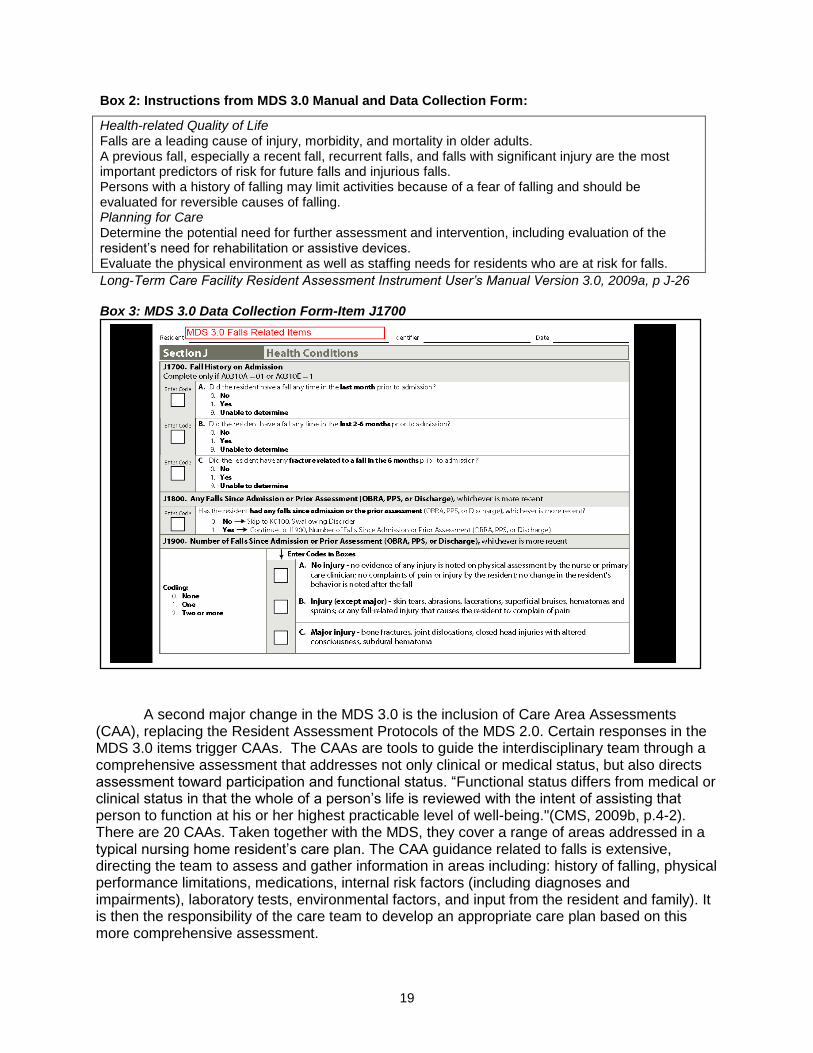
A second major change in the MDS 3.0 is the inclusion of Care Area Assessments (CAA), replacing the Resident Assessment Protocols of the MDS 2.0. Certain responses in the MDS 3.0 items trigger CAAs. The CAAs are tools to guide the interdisciplinary team through a comprehensive assessment that addresses not only clinical or medical status, but also directs assessment toward participation and functional status. “Functional status differs from medical or clinical status in that the whole of a person’s life is reviewed with the intent of assisting that person to function at his or her highest practicable level of well-being."(CMS, 2009b, p.4-2). There are 20 CAAs. Taken together with the MDS, they cover a range of areas addressed in a typical nursing home resident’s care plan. The CAA guidance related to falls is extensive, directing the team to assess and gather information in areas including: history of falling, physical performance limitations, medications, internal risk factors (including diagnoses and impairments), laboratory tests, environmental factors, and input from the resident and family). It is then the responsibility of the care team to develop an appropriate care plan based on this more comprehensive assessment.
Box 2: Instructions from MDS 3.0 Manual and Data Collection Form:
Health-related Quality of Life Falls are a leading cause of injury, morbidity, and mortality in older adults. A previous fall, especially a recent fall, recurrent falls, and falls with significant injury are the most important predictors of risk for future falls and injurious falls. Persons with a history of falling may limit activities because of a fear of falling and should be evaluated for reversible causes of falling. Planning for Care Determine the potential need for further assessment and intervention, including evaluation of the resident’s need for rehabilitation or assistive devices. Evaluate the physical environment as well as staffing needs for residents who are at risk for falls.
Long-Term Care Facility Resident Assessment Instrument User’s Manual Version 3.0, 2009a, p J-26 Box 3: MDS 3.0 Data Collection Form-Item J1700
20
Although attention to the issue of falls is appropriate, the CAA for falls is five pages long and includes 49 potential factors contributing to falls. The extensive list may encourage the care team to consider falls from a multifactor perspective. However, the requirement to investigate and analyze so many factors in so many domains also may obscure or complicate the process of identifying relevant falls risk factors. Refining the CAA to more closely align with recognized risk factors would reduce confusion as well as burden. The broad and non-prioritized list of potential risk factors provided in the CAA contrasts sharply with the limited AGS/BGS Guideline recommendations for falls reduction in long-term care facilities. The CAA list is not prioritized, nor is there guidance that supports evidence-based decision making. If the CAA process is to better inform care planning, consideration should be given to prioritizing the CAA tool based on current evidence regarding risk factors and risk reduction interventions.
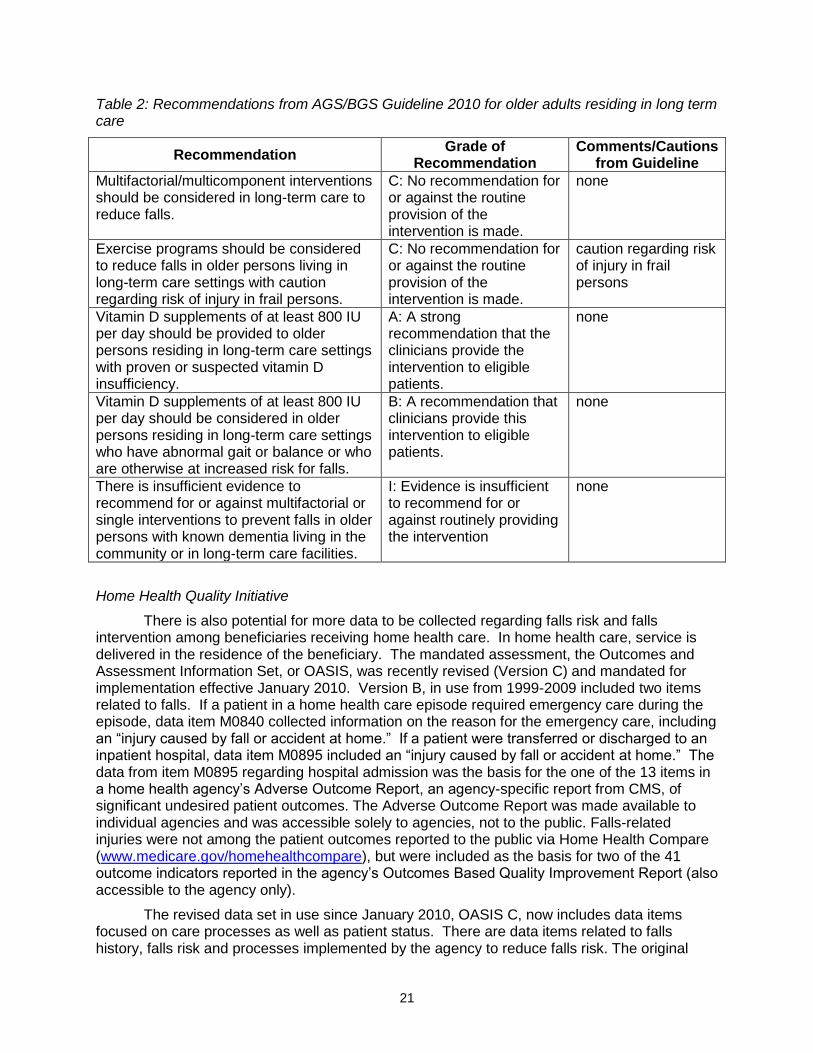
For example, Vitamin D supplementation is recommended strongly for long term care residents with an identified Vitamin D insufficiency. Vitamin D supplementation is also recommended for long term care residents with abnormal gait, balance deficits or other identified falls risks. Yet “vitamin D deficiency” is listed in the CAA list on page 4, at the end of a list of “intrinsic factors,” which the care team is to consider. There is no indication that points out that this is an evidence-based significant risk factor or that Vitamin D supplementation is an intervention supported by best available evidence. Table 2 summarizes the AGS/BGS Guideline 2010 recommendations pertaining to falls assessment and prevention targeted to older adults living in long term care facilities.
The revised MDS 3.0 and the introduction of the CAA may contribute to a better understanding and increased utilization of fall prevention activities by nursing facilities and staff because they come from an important source, Medicare. The large repository of data that will be generated by the revised MDS 3.0, including the refined data items related to falls history and falls risk, may provide data on falls risk factors and falls risk reduction factors effective for residents in long term care settings. This potential for skilled nursing facilities to obtain rich data on falls risk and falls intervention could be extremely helpful, supplementing the limited or inconclusive data available from existing research.
21
Table 2: Recommendations from AGS/BGS Guideline 2010 for older adults residing in long term care
Recommendation Grade of
Recommendation Comments/Cautions
from Guideline
Multifactorial/multicomponent interventions should be considered in long-term care to reduce falls.
C: No recommendation for or against the routine provision of the intervention is made.
none
Exercise programs should be considered to reduce falls in older persons living in long-term care settings with caution regarding risk of injury in frail persons.
C: No recommendation for or against the routine provision of the intervention is made.
caution regarding risk of injury in frail persons
Vitamin D supplements of at least 800 IU per day should be provided to older persons residing in long-term care settings with proven or suspected vitamin D insufficiency.
A: A strong recommendation that the clinicians provide the intervention to eligible patients.
none
Vitamin D supplements of at least 800 IU per day should be considered in older persons residing in long-term care settings who have abnormal gait or balance or who are otherwise at increased risk for falls.
B: A recommendation that clinicians provide this intervention to eligible patients.
none
There is insufficient evidence to recommend for or against multifactorial or single interventions to prevent falls in older persons with known dementia living in the community or in long-term care facilities.
I: Evidence is insufficient to recommend for or against routinely providing the intervention
none
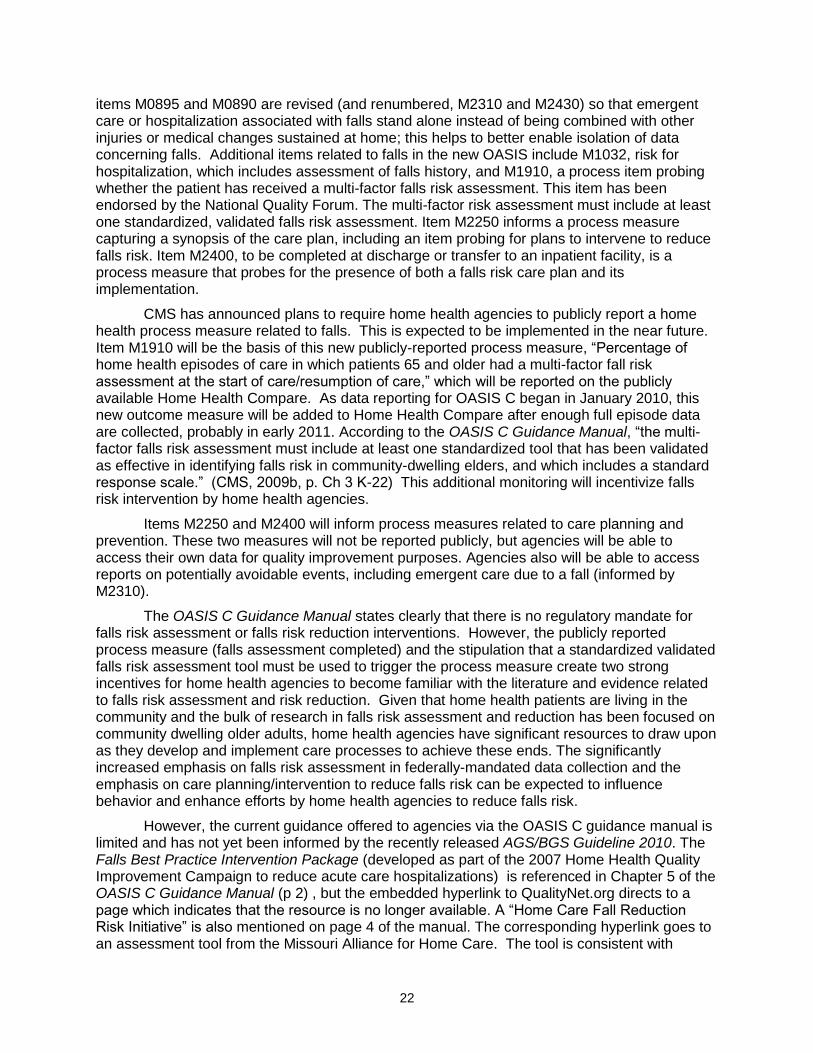
Home Health Quality Initiative
There is also potential for more data to be collected regarding falls risk and falls intervention among beneficiaries receiving home health care. In home health care, service is delivered in the residence of the beneficiary. The mandated assessment, the Outcomes and Assessment Information Set, or OASIS, was recently revised (Version C) and mandated for implementation effective January 2010. Version B, in use from 1999-2009 included two items related to falls. If a patient in a home health care episode required emergency care during the episode, data item M0840 collected information on the reason for the emergency care, including an “injury caused by fall or accident at home.” If a patient were transferred or discharged to an inpatient hospital, data item M0895 included an “injury caused by fall or accident at home.” The data from item M0895 regarding hospital admission was the basis for the one of the 13 items in a home health agency’s Adverse Outcome Report, an agency-specific report from CMS, of significant undesired patient outcomes. The Adverse Outcome Report was made available to individual agencies and was accessible solely to agencies, not to the public. Falls-related injuries were not among the patient outcomes reported to the public via Home Health Compare (www.medicare.gov/homehealthcompare), but were included as the basis for two of the 41 outcome indicators reported in the agency’s Outcomes Based Quality Improvement Report (also accessible to the agency only).
The revised data set in use since January 2010, OASIS C, now includes data items focused on care processes as well as patient status. There are data items related to falls history, falls risk and processes implemented by the agency to reduce falls risk. The original
22
items M0895 and M0890 are revised (and renumbered, M2310 and M2430) so that emergent care or hospitalization associated with falls stand alone instead of being combined with other injuries or medical changes sustained at home; this helps to better enable isolation of data concerning falls. Additional items related to falls in the new OASIS include M1032, risk for hospitalization, which includes assessment of falls history, and M1910, a process item probing whether the patient has received a multi-factor falls risk assessment. This item has been endorsed by the National Quality Forum. The multi-factor risk assessment must include at least one standardized, validated falls risk assessment. Item M2250 informs a process measure capturing a synopsis of the care plan, including an item probing for plans to intervene to reduce falls risk. Item M2400, to be completed at discharge or transfer to an inpatient facility, is a process measure that probes for the presence of both a falls risk care plan and its implementation.
CMS has announced plans to require home health agencies to publicly report a home health process measure related to falls. This is expected to be implemented in the near future. Item M1910 will be the basis of this new publicly-reported process measure, “Percentage of home health episodes of care in which patients 65 and older had a multi-factor fall risk assessment at the start of care/resumption of care,” which will be reported on the publicly available Home Health Compare. As data reporting for OASIS C began in January 2010, this new outcome measure will be added to Home Health Compare after enough full episode data are collected, probably in early 2011. According to the OASIS C Guidance Manual, “the multi-factor falls risk assessment must include at least one standardized tool that has been validated as effective in identifying falls risk in community-dwelling elders, and which includes a standard response scale.” (CMS, 2009b, p. Ch 3 K-22) This additional monitoring will incentivize falls risk intervention by home health agencies.
Items M2250 and M2400 will inform process measures related to care planning and prevention. These two measures will not be reported publicly, but agencies will be able to access their own data for quality improvement purposes. Agencies also will be able to access reports on potentially avoidable events, including emergent care due to a fall (informed by M2310).
The OASIS C Guidance Manual states clearly that there is no regulatory mandate for falls risk assessment or falls risk reduction interventions. However, the publicly reported process measure (falls assessment completed) and the stipulation that a standardized validated falls risk assessment tool must be used to trigger the process measure create two strong incentives for home health agencies to become familiar with the literature and evidence related to falls risk assessment and risk reduction. Given that home health patients are living in the community and the bulk of research in falls risk assessment and reduction has been focused on community dwelling older adults, home health agencies have significant resources to draw upon as they develop and implement care processes to achieve these ends. The significantly increased emphasis on falls risk assessment in federally-mandated data collection and the emphasis on care planning/intervention to reduce falls risk can be expected to influence behavior and enhance efforts by home health agencies to reduce falls risk.
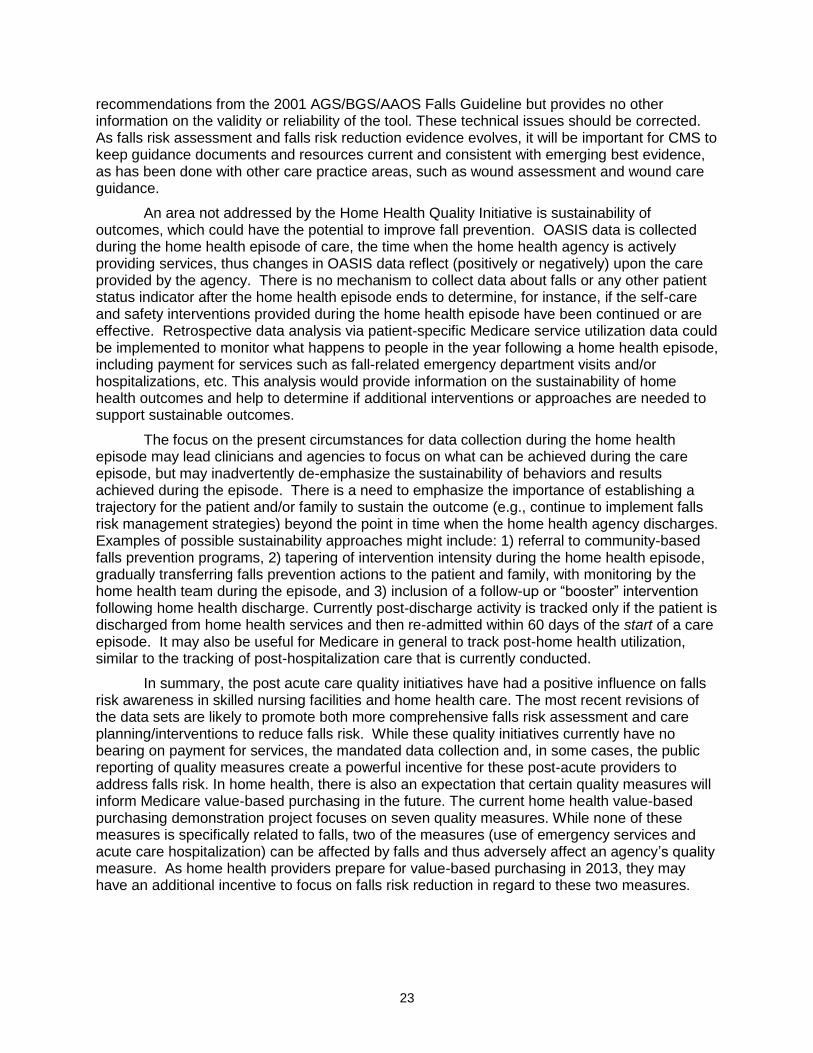
However, the current guidance offered to agencies via the OASIS C guidance manual is limited and has not yet been informed by the recently released AGS/BGS Guideline 2010. The Falls Best Practice Intervention Package (developed as part of the 2007 Home Health Quality Improvement Campaign to reduce acute care hospitalizations) is referenced in Chapter 5 of the OASIS C Guidance Manual (p 2) , but the embedded hyperlink to QualityNet.org directs to a page which indicates that the resource is no longer available. A “Home Care Fall Reduction Risk Initiative” is also mentioned on page 4 of the manual. The corresponding hyperlink goes to an assessment tool from the Missouri Alliance for Home Care. The tool is consistent with
23
recommendations from the 2001 AGS/BGS/AAOS Falls Guideline but provides no other information on the validity or reliability of the tool. These technical issues should be corrected. As falls risk assessment and falls risk reduction evidence evolves, it will be important for CMS to keep guidance documents and resources current and consistent with emerging best evidence, as has been done with other care practice areas, such as wound assessment and wound care guidance.
An area not addressed by the Home Health Quality Initiative is sustainability of outcomes, which could have the potential to improve fall prevention. OASIS data is collected during the home health episode of care, the time when the home health agency is actively providing services, thus changes in OASIS data reflect (positively or negatively) upon the care provided by the agency. There is no mechanism to collect data about falls or any other patient status indicator after the home health episode ends to determine, for instance, if the self-care and safety interventions provided during the home health episode have been continued or are effective. Retrospective data analysis via patient-specific Medicare service utilization data could be implemented to monitor what happens to people in the year following a home health episode, including payment for services such as fall-related emergency department visits and/or hospitalizations, etc. This analysis would provide information on the sustainability of home health outcomes and help to determine if additional interventions or approaches are needed to support sustainable outcomes.
The focus on the present circumstances for data collection during the home health episode may lead clinicians and agencies to focus on what can be achieved during the care episode, but may inadvertently de-emphasize the sustainability of behaviors and results achieved during the episode. There is a need to emphasize the importance of establishing a trajectory for the patient and/or family to sustain the outcome (e.g., continue to implement falls risk management strategies) beyond the point in time when the home health agency discharges. Examples of possible sustainability approaches might include: 1) referral to community-based falls prevention programs, 2) tapering of intervention intensity during the home health episode, gradually transferring falls prevention actions to the patient and family, with monitoring by the home health team during the episode, and 3) inclusion of a follow-up or “booster” intervention following home health discharge. Currently post-discharge activity is tracked only if the patient is discharged from home health services and then re-admitted within 60 days of the start of a care episode. It may also be useful for Medicare in general to track post-home health utilization, similar to the tracking of post-hospitalization care that is currently conducted.
In summary, the post acute care quality initiatives have had a positive influence on falls risk awareness in skilled nursing facilities and home health care. The most recent revisions of the data sets are likely to promote both more comprehensive falls risk assessment and care planning/interventions to reduce falls risk. While these quality initiatives currently have no bearing on payment for services, the mandated data collection and, in some cases, the public reporting of quality measures create a powerful incentive for these post-acute providers to address falls risk. In home health, there is also an expectation that certain quality measures will inform Medicare value-based purchasing in the future. The current home health value-based purchasing demonstration project focuses on seven quality measures. While none of these measures is specifically related to falls, two of the measures (use of emergency services and acute care hospitalization) can be affected by falls and thus adversely affect an agency’s quality measure. As home health providers prepare for value-based purchasing in 2013, they may have an additional incentive to focus on falls risk reduction in regard to these two measures.
24
Physician Quality Reporting Initiative (PQRI)
Beginning in 2005, Medicare implemented a voluntary reporting initiative for physicians and non-physician providers focusing on key care process measures. This initiative differed from the two post-acute care initiatives mentioned above in two respects: 1) it was (and is currently) voluntary, and 2) participants in the initiative are eligible to receive a “bonus payment percentage” on all Medicare claims based on meeting certain measure benchmarks in the preceding reporting year. This initiative was known first as PVRP (physician voluntary reporting program) and, starting in 2007, PQRI. Screening for future falls risk was a measure included in 2007 and 2008:
“Percentage of patients aged 65 years and older who were screened for future fall risk (patients are considered at risk for future falls if they have had 2 or more falls in the past year or any fall with injury in the past year) at least once within 12 months.”
For 2009 and ongoing, this measure was renamed (#154: Falls: Risk Assessment) and a second fall-related measure, falls risk plan, was added:
“#155: Falls: Plan of Care: Percentage of patients aged 65 years and older with a history of falls who had a plan of care for falls documented within 12 months.”
According to the 2010 Physician Quality Reporting Initiative Measure Specifications Manual, Measure #154 is based on the following two definitions:
Fall – A sudden, unintentional change in position causing an individual to land at a lower level, on an object, the floor, or the ground, other than as a consequence of sudden onset of paralysis, epileptic seizure, or overwhelming external force.
Risk Assessment – Comprised of balance/gait AND one or more of the following: postural blood pressure, vision, home fall hazards, and documentation on whether medications are a contributing factor or not to falls within the past 12 months. (p.340)
The rationale for this measure states:
Screening for specific medical conditions may direct the therapy. Although the clinical guidelines and supporting evidence calls for an evaluation of many factors, it was felt that for the purposes of measuring performance and facilitating implementation this initial measure must be limited in scope. For this reason, the work group defined an evaluation of balance and gait as a core component that must be completed on all patients with a history of falls as well as four additional evaluations – at least one of which must be completed within the 12 month period. (p.341)
The “workgroup” referenced is the Geriatrics Work Group of the AGS/Physician Consortium for Performance Improvement (AGS/PCPI) which included many of the leading experts in falls research. The measure specification includes Clinical Recommendations Statements. Some of these statements are taken verbatim from the 2001 AGS/BGS/AAOS Guideline. However, other statements are inconsistent with both the 2001 Guideline and the newer AGS/BGS Guideline 2010. The original form of the measure is found on the National Quality Measures Clearinghouse website (http://www.qualitymeasures.ahrq.gov/summary/summary.aspx?doc_id=12668&string=falls). Dated 2008, this version of the measure indicates that the additional Clinical Guidance Recommendations were taken verbatim from the “soon to be released” AGS revised guideline. However, the 2008 recommendations include statements not supported or included in the 2010
25
Guideline, such as screening for depression, as this was determined by AGS not to have an impact on falls.
The clinical actions specifically addressed in the measure’s definition of falls risk assessment are consistent with current best evidence. The measure raises the awareness of physicians and other practitioners and prompts them to assess falls risk. However, the Clinical Recommendations Statements include both out-of-date and unsupported recommendations. Keeping measures and other items up to date with current research is challenging but should be considered as a priority to keep these systems valuable.
Measure #154 is paired with measure #155, Falls: Plan of Care. The Measure Specifications Manual explains that “this measure should be reported if CPT II code 1100F “Patient screened for future falls risk; documentation of two or more falls in the past year or any fall with injury in the past year” is submitted for Measure #154.” (p.343) Measure #155 is based on the following definitions:
Plan of Care – Must include: 1) consideration of appropriate assistance device(s) AND 2) balance, strength, and gait training.
Consideration of Appropriate Assistance Device – Medical record must include: documentation that an assistive device was provided or considered OR referral [was made] for evaluation for an appropriate assistance device
Balance, Strength, and Gait Training – Medical record must include: documentation that balance, strength, and gait training/instructions were provided OR referral to an exercise program, which includes at least one of the three components: balance, strength or gait. (p.344)
and the following Clinical Recommendation Statements:
Among community-dwelling older persons (i.e., those living in their own homes), multifactorial interventions should include:
gait training and advice on the appropriate use of assistive devices (Grade B)
review and modification of medication, especially psychotropic medication (Grade B)
exercise programs, with balance training as one of the components (Grade B)
treatment of postural hypotension (Grade B)
o modification of environmental hazards (Grade C)
o treatment for cardiovascular disorders (Grade D) (AGS/BGS/AAOS) (pp.34-345)
As indicated in the final statement, the recommendations are taken (verbatim) from the 2001 AGS/BGS/AAOS Guideline (p.667). Neither the content of the recommendations nor the strength of the recommendations matches the recently released 2010 AGS/BGS Guideline. The 2010 AGS/BGS Guideline states that the components most commonly included in efficacious interventions were: [with recommendation grade]
a. Adaptation or modification of home environment (A)
b. Withdrawal or minimization of psychoactive medications (B)
26
c. Withdrawal or minimization of other medications (C)
d. Management of postural hypotension (C)
e. Management of foot problems and footwear (C)
f. Exercise, particularly balance, strength, and gait training (A). (AGS, 2010)
The AGS/BGS Guideline 2010 identifies an additional grade A recommendation for intervention that is absent from the Measure #155 criteria or Clinical Recommendation Statements: Vitamin D supplements of at least 800 IU per day should be provided to older adults with proven Vitamin D deficiency.
The 2010 version also includes the following grade A recommendations:
The health professional or team conducting the fall risk assessment should directly implement the intervention or should assure that the interventions are carried out by other qualified healthcare professionals.
All older adults who are at risk of falling should be offered an exercise program incorporating balance, gait and strength training.
An exercise program that targets strength, gait and balance, such as Tai Chi or physical therapy, is recommended as an effective intervention to reduce falls.
The Balance, Strength and Gait Training component of the measure states that documentation may indicate that “instruction was provided OR referral to an exercise program, which includes at least one of the three components: balance, strength or gait.” It appears that instruction regarding an exercise program would meet the balance, strength, and gait training requirement of this Measure, yet fall far short of the recommendations related to exercise. Similarly, referral to an exercise program may meet the requirement, but falls short of the recommendation that the health professional should assure that the interventions are carried out. In addition, the measure does not reference referral to covered Medicare services, such as occupational therapy or physical therapy, for assessment and intervention if the patient meets the medical necessity criteria for those services.
The other required component of the measure, consideration of, or provision of an assistive device, is also inconsistent with the current AGS/BGS Guideline. Nowhere in the 2010 Guideline are assistive devices recommended. While such a device may be provided as part of gait training, there is some evidence that provision of a device without appropriate training in its use may be counterproductive, increasing falls risk (Stevens, Thomas, Teh & Greenspan, 2009). Provision of a prescription for an assistive device without follow-up is inconsistent with the strong (grade A) recommendation from the AGS/BGS 2010 that “the health professional or team conducting the fall risk assessment should directly implement the interventions or should assure that the interventions are carried out by other qualified healthcare professionals.” The recommendation of a health professional should assure that the interventions are carried out. For this measure, the option of “instruction” regarding exercise and the required consideration of assistive devices may actually divert attention from interventions that specifically address identified falls risk factors. It might also be possible to provide the two required aspects of the measure but not follow-up to ensure that interventions provided are effective or if there is compliance or sustainability by the patient.
While PQRI participation currently is voluntary, the bonus payment and the recent legislation that PQRI will become mandatory in a few years are both strong incentives for providers to participate. It is important that PQRI measures pertaining to falls be feasible to measure and appropriate to facilitate implementation, but also that any such changes should be
27
consistent with and supported by the best available evidence. It appears that that the current measures may incentivize assessment and care planning that is not multifactorial, does not ensure follow-up, and may mislead both the provider and the patient to believe that falls risk has been effectively addressed. The content of these two PQRI measures should be revised and updated to be consistent with the recommendations of the AGS/BGS Guideline 2010.
28
Payment Policies and Local Coverage Determinations
Medicare is known primarily as a payer, the largest purchaser of healthcare services in the country. Medicare payment policies have a powerful influence on the care received by beneficiaries. This is true even if beneficiaries have other (secondary) health insurance. If Medicare does not cover a given item or service, then beneficiaries are unlikely to have coverage for these items or services through their secondary insurance. But Medicare coverage policies have influence that extends beyond the provisions found in coverage manuals. Medicare policies—what is covered and what is not—also inform the clinical decision making of providers. This “pragmatic reasoning” (Schell, 2009) develops as providers deal with Medicare beneficiaries and Medicare policies on a day-to-day basis, even though they may seldom consult a coverage manual. Given both the explicit and the tacit influence of Medicare policy on both providers and practice, it is essential that coverage policies be clear, consistent, and, to the extent possible, based on best clinical evidence. The multiple factors associated with falls risk and falls risk reduction touch on many different aspects of Medicare policy and Medicare coverage.
Vitamin D
Vitamin D deficiency is a risk factor for falls and falls-related fractures. Research indicates that Vitamin D supplementation of at least 800 IU per day has benefit that strongly outweighs risk for older adults with documented Vitamin D deficiency or for older adults with suspected Vitamin D deficiency and heightened risk for falls. The AGS/BGS Guideline 2010 recommends Vitamin D supplementation for community dwelling older adults and also for older adults living in long term care facilities. For the latter population, this recommendation is the only falls risk intervention that meets the criteria for an A or B grade recommendation. Yet because Vitamin D is available over the counter and is administered orally, it is not covered under any Medicare Part D plan examined, even when prescribed. While the retail price of Vitamin D is relatively low (approximately 10 cents per 1000 IU tablet), the lack of coverage means Vitamin D may be the first prescription not filled by beneficiaries facing financial challenges.
In skilled nursing facilities (SNF), the issue is more complex. Vitamin D deficiency is common among residents living in long term care facilities (Drinka, Krause, Nest & Goodman, 2007). Before the implementation of Medicare Part D, long term care facilities and their pharmacies were in control of the medications dispensed to their residents. Part D introduced wide variation in formularies and medication-related management processes for residents at the facility level, and an additional burden on clinical and pharmacy staff (Stevenson, Huskamp & Newhouse, 2008). Given the challenges posed for facilities to obtain prescribed medications ordered for each resident, the recommendation to provide non-Part D covered vitamin supplementation may be overlooked or ignored. It appears that a coverage policy change is needed, either in requiring Vitamin D to be in the formulary for all Part D plans or, at a minimum, to enable skilled nursing facilities to dispense Vitamin D to all residents for whom it is prescribed, regardless of their Part D coverage. The very minimal cost of Vitamin D is far outweighed by the evidence that Vitamin D supplementation reduces falls risk among long term care residents (Cameron, Murray, Gillespie, Robertson, Hill, Cumming & Kerse, 2010).
Durable Medical Equipment (DME)
The Medicare Benefit Policy Manual defines DME as “equipment which:
Can withstand repeated use;
Is primarily and customarily used to serve a medical purpose;
29
Generally is not useful to a person in the absence of an illness or injury; and
Is appropriate for use in the home.
All requirements of the definition must be met before an item can be considered to be durable medical equipment.” (CMS, n.d., Chapter 15 §110.1) Addressing the medical purpose requirement, the manual refers to equipment that is presumptively non medical:
Equipment which basically serves comfort or convenience functions or is primarily for the convenience of a person caring for the patient, such as elevators, stairway elevators, and posture chairs, do not constitute medical equipment. Similarly, physical fitness equipment (such as an exercycle), first-aid or precautionary-type equipment (such as preset portable oxygen units), self-help devices (such as safety grab bars), and training equipment (such as Braille training texts) are considered nonmedical in nature. (CMS, n.d., Chapter 15 §110.1 (B) (1)) (Emphasis added.)
In addition to safety grab bars, Medicare does not cover DME items such as bath seats, transfer tub benches and elevated toilet seats as they are considered self-help devices or personal convenience items and thus non-medical. This section of the Benefit Policy Manual also elaborates on “necessary and reasonable”:
1. Necessity for the Equipment Equipment is necessary when it can be expected to make a meaningful contribution to the treatment of the patient’s illness or injury or to the improvement of his or her malformed body member. In most cases the physician’s prescription for the equipment and other medical information available to the DMERC [Durable Medical Equipment Regional Carrier) will be sufficient to establish that the equipment serves this purpose.
2. Reasonableness of the Equipment Even though an item of DME may serve a useful medical purpose, the DMERC or intermediary must also consider to what extent, if any, it would be reasonable for the Medicare program to pay for the item prescribed.
The following considerations should enter into the determination of reasonableness:
1. Would the expense of the item to the program be clearly disproportionate to the therapeutic benefits which could ordinarily be derived from use of the equipment?
2. Is the item substantially more costly than a medically appropriate and realistically feasible alternative pattern of care?
3. Does the item serve essentially the same purpose as equipment already available to the beneficiary? (CMS, n.d., Chapter 15 §110.1) (Emphasis added)
Bathroom Safety Devices:
The AGS/BGS Guideline 2010 includes a strong recommendation for adaptation or modification of the home environment to reduce falls. Many of the studies that underpin this recommendation included modifications in the bathroom to reduce falls, such as installation of grab bars or use of a seat during bathing. These items are used to compensate for impairments such as weakness, poor balance, and limited activity tolerance that could otherwise lead to a fall. From this perspective, these items clearly meet the medical necessity requirement. In terms of reasonableness, however, the cost/benefit analysis implied in the Benefit Policy Manual is particularly relevant. Bath seats, grab bars and raised toilet seats typically cost less
30
than $100, while transfer benches cost less than $150. A 1998 study found that the average healthcare cost (hospital, emergency room, home health care, and emergency care) for a fall related injury sustained by an adult 72 years old and older was approximately $20,000, not including physician charges (Rizzo, Friedkin, Williams, Nabors, Acampora & Tinetti, 1998). Given the minimal cost of the equipment in comparison to the significant cost of care from falls or other resulting problems, application of the first test of reasonableness could support coverage of these items.
The second and third tests point out the lack of other alternatives. Older adults whose impairments affect their ability to perform bathing and toileting have no “feasible alternatives.” They may persist with efforts to bathe or toilet despite the risk, or their hygiene and skin integrity may decline as they curtail these activities in an effort to reduce falls risk.
Classifying these items as “presumptively nonmedical” (see definition above) appears arbitrary when considered from a falls prevention perspective. The medical consequences of non-coverage and the cost savings associated with coverage should be considered in this policy decision. Given these issues, a change in coverage policy is called for to include these items as covered DME. It is important to note that some of these items (bath seats, transfer benches, grab bars and raised toilet seats) have been assigned Health Care Common Procedure Codes (HCPCS) and are covered by Medicaid in a number states (e.g., North Carolina, New York, Hawaii).
Mobility Devices:
A recent analysis was conducted of falls associated with the use of walkers or canes (Stevens, Thomas, Teh & Greenspan, 2009). The authors concluded
Although falls associated with walkers and canes represented just 2.6% of older adult fall injuries treated in EDs [emergency departments], the population affected was the frailest and most vulnerable older adults. The majority of these injuries happened at home, and 21% to 35% occurred while the person was walking. Research is needed to understand the physical and cognitive demands that walking aids place on users. Additional studies are needed to identify potential design problems so as to improve walkers and reduce the incidence of fall injuries in this high-risk population. (pp.1468-69)
Canes and walker are covered as Medicare Part B DME. However, in practice, many beneficiaries do not obtain these devices from DME vendors, but instead “inherit” or “borrow” the items from friends or family members. Others purchase these items at pharmacies, mass merchandisers or second-hand stores without accessing the Medicare benefit or related services covered under Medicare. However, canes and walkers must be fitted appropriately to the stature and mobility needs of the user in order to be used safely and effectively. A handsome wooden cane designed for a tall person will provide no support or stability for a short person. A walker with a standard capacity of 250 pounds will not adequately support a beneficiary weighing 300 or more pounds.
Even though these devices appear relatively simple, cane or walker use is not intuitive for most individuals. Use of these devices requires increased cognitive demands that in some situations necessitate instruction to safely integrate use of the device into daily routines and environments. It appears simple to use a walker when traversing an open room. However, when the user must negotiate narrow doorways, open locked doors, or carry items, the walker may be abandoned. Rollator walkers have a seat that is to be used only when the rollator is stationary with wheels locked. However, many users attempt to use the seat as a “rolling chair.” Such use exceeds the structural capacity of the device and may lead to catastrophic device
31
failure and injury to the user seated on the device. Appropriate instruction, and follow-up instruction if needed, is necessary to ensure that device use is integrated into routines and habits and that those devices do not inadvertently increase falls risk.
Current coverage for these items may also unintentionally contribute to misuse or unsafe use. Medicare pays for only one mobility-assist item at a time. During the time period for which that item is covered (usually 5 years), Medicare will not pay for another mobility device. This limitation does not take into consideration the environmental barriers that beneficiaries encounter in their homes, which may require use of more than one device. For example, the study of falls associated with walkers and canes noted that few falls associated with walkers occurred in the bathroom. This makes sense given that residential bathroom doorways are two feet wide and that most bathroom entries do not allow a user to negotiate a walker (or wheelchair) through the bathroom doorway and into the room. An alternative would be to have a walker or a cane in the bathroom to provide mobility support once in the bathroom, but neither of these items would be covered by Medicare. (Nor would grab bars installed in the bathroom to provide support.) Similarly, a walker-user living in a two-level home is unlikely to be able to carry the walker up or down a flight of steps. A simple solution would be to have a walker on both levels and to use railings on the stairs for support between levels, but the current benefit does not cover two devices simultaneously.
Furthermore, significant changes in physical status or cognitive ability may necessitate a new device earlier than the expected “lifetime” of given item. While a cane or walker may be expected to last 5 years under normal use, the 5-year “lifetime” assumes that a beneficiary’s mobility skills will remain unchanged for that same period of time. If a beneficiary receives a cane, walker, or rollator (walker with four wheels and seat) that is not appropriate (provides inadequate support, is not suitable for home environment, cognitive or physical demands of the device exceed capabilities), or becomes inappropriate, the likely consequence is either a reduction in mobility and activity or a heightened risk of injury. It seems arbitrary to withhold coverage for another device for 5 years when replacement by a more appropriate device may reduce falls risk while sustaining functional mobility. Few providers are aware of the 5-year lifetime and thus may not consider the beneficiary’s physical and cognitive skills projected over 5 years when they prescribe or issue a device. To adequately improve falls risks associated with these devices, the current policy should be highlighted through increased provider education, care coordination, and publicizing of appeal or review rights so that beneficiaries whose mobility needs exceed their current device are not forced to wait the lifetime of the device to obtain one that is more appropriate.
Given the data regarding falls associated with walkers and canes and the common features of residential construction, it seems reasonable to revise the current coverage policy for these devices by eliminating the coverage restriction of one mobility device in circumstances where the beneficiary needs more than one device to manage mobility related activities of daily living in the home or to safely enter/exit the home. It also seems reasonable to educate both prescribers and beneficiaries on the importance of having a cane or walker appropriately fitted and to receive training in safe use so the device can be integrated into daily routines and to ensure that any related cognitive issues are addressed. There is a PQRI Measure related to prescribing or issuing an assistive device that is separate from the falls measures; this should require that the prescription should include training or instruction to fit, adjust, and integrate the device for safe use.
Local Coverage Determinations
“A Local Coverage Determination (LCD) . . . is a decision by a fiscal intermediary or carrier [administrative contractor] whether to cover a particular service on an intermediary-wide
32
or carrier-wide basis in accordance with Section 1862(a)(1)(A) of the Social Security Act (i.e., a determination as to whether the service is reasonable and necessary).” (Center for Medicare & Medicaid Services, 2010). Since 2003, Medicare contractors have established a number of LCDs with implications for falls prevention. Those that most directly relate to falls prevention and to implementation of the AGS/BGS Guideline 2010 recommendations pertain to coverage of occupational therapy and physical therapy.
In Medicare education materials, if the findings of the Welcome to Medicare physical or a subsequent provider encounter indicate that a beneficiary has a significant falls risk, the provider is encouraged to refer the beneficiary to other services to address the falls risk, including occupational therapy and physical therapy. Such referrals also are consistent with the research informing the AGS/BGS Guideline 2010 recommendations. However, occupational therapy or physical therapy services will be covered only if they are consistent with applicable LCDs. Most commonly, the LCDs include lists of diagnoses that “support medical necessity” for these services. However, a beneficiary may be at risk of falls without having a diagnosis or without having a diagnosis listed in the LCD. For example, a beneficiary may have difficulty with balance affecting control during position change such as transfers. There is no diagnosis in the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) which accurately describes this problem. “Abnormality of gait “(781.2) may also be present, but it is not uncommon for an individual to experience balance problems without exhibiting an abnormal gait. In these circumstances, the beneficiary may seek out or be referred to a physical or occupational therapist, and the therapist may address the problem through remedial or compensatory strategies. However, the lack of a diagnosis will likely result in denial of the therapy claim.
LCDs are specific to the jurisdiction of the carrier, intermediary, or administrative contractor, so there are also variations and inconsistencies geographically. For example, the LCD for occupational therapy issued by Cahaba Government Benefit Administrators (L30007) applies to outpatient occupational therapy provided in Alabama, Georgia, and Tennessee. This LCD imposes a limitation on occupational therapy evaluation (not reasonable and necessary), stating that “CPT 97003 - An evaluation by a therapist is non-covered when the evaluation is for a non-covered service (e.g., wheelchair ramp).” An evaluation by an occupational therapist is a process of assessment to identify strengths and needs prior to identifying interventions; an evaluation by definition is not “for” a specific intervention. Thus denying coverage for an evaluation that, for instance, recommends the use of a bath chair that is not covered by Medicare could be denied under this LCD.
More importantly, research underpinning the AGS/BGS Guideline 2010 recommendations includes several randomized controlled trials involving occupational therapy assessment in the home leading to modifications of the home environment with a concurrent reduction in falls risk (Close, Ellis, Hoper, Glucksman, Jackson & Swift, 1999, Cumming, et.al., 1999, Clemson, Cumming, Kendig, Swann, Heard & Taylor, 2004). Limiting coverage for such an evaluation is inconsistent with current best evidence. Furthermore, this arbitrary limit does not take into consideration that, for a beneficiary with dual eligibility, a grab bar or transfer bench may not be covered by Medicare but may be covered by Medicaid. It may be the beneficiary’s decision, upon receiving such recommendations, to pay for the devices or modifications out of pocket to reduce his/her falls risk. Moreover, the limitation on suggesting appropriate equipment or other modifications creates an ethical dilemma for occupational therapists. If the findings of an occupational therapy evaluation indicate that the beneficiary may benefit from (non-covered) home modifications or equipment to reduce falls risk and/or to improve function, the therapist faces the choice of documenting these findings and communicating them to the
33
beneficiary, knowing that this carries a risk of having the claim for the evaluation denied, or withholding information from the beneficiary.
In contrast, the 2010 LCD for outpatient occupational therapy issued by Palmetto Government Benefit Administrators (L1149) contains no such limitation on evaluation. Further, Palmetto GBA has developed an educational piece for providers, “Falls Evaluation: Translating Evidence-Based Interventions into Your Practice”, which states:
Evidence-based falls evaluations are encouraged by Medicare. Although the importance of falls evaluations has been recognized by the research community for many years, there has been a lag in the translation of this knowledge to the clinical community. Falls evaluations are components of existing quality improvement efforts for Medicare Part A providers. (Palmetto GBA, 2010)
The tool goes on to address the complexity of addressing falls risk under a system that is based on medical necessity. It concludes by stating:
To allow for falls evaluations in Part A environments, Palmetto GBA has therefore included the V15.88 code in its Part A Local Coverage Determinations (LCDs) addressing North Carolina Outpatient Physical Therapy (PT) (L1166) and South Carolina Outpatient Physical Therapy (PT) (L10214) and South Carolina Outpatient Occupational Therapy (OT) (L12642) and North Carolina Outpatient Occupational Therapy (OT) (L1149). The code will also be included in Physical Therapy for Home Health PT (L282) and Home Health-OT (L12643) LCDs. (See the following for more information on the V15.88 code).
This disparity between LCDs means disparities and inconsistencies in what is covered and available to beneficiaries who are at risk of falls. Ironically, these two LCDs apply to neighboring states; beneficiaries separated by a few miles or even a few blocks may be subject to very different coverage policies. The Cahaba LCD does not take into consideration that occupational therapists may identify interventions that may improve beneficiaries’ function and reduce their risk, even if the interventions are not covered and have no impact on Medicare spending. More importantly, this LCD disregards the right of the beneficiary to be made aware of such interventions. In contrast, the Palmetto LCDs, taken with the “Falls Evaluation: Translating Evidence-based Interventions into Your Practice” piece and its provider education tools for Going Beyond Diagnosis, seek to engage the expertise of the provider to optimize the health and function of the beneficiary, even while staying within current Medicare parameters.
34
Falls and Diagnosis Coding
The International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) is based on the World Health Organization's Ninth Revision, International Classification of Diseases (ICD-9). ICD-9-CM is the official system of assigning codes to diagnoses associated with healthcare utilization in the United States. Four organizations, the American Hospital Association (AHA), the American Health Information Management Association (AHIMA), the Centers for Medicare and Medicaid Services, and the National Center for Health Statistics, are the “cooperating parties” responsible for maintenance and revision of the ICD 9-CM. In 2004, CMS and the National Center for Injury Prevention and Control (NCIPC) at CDC requested that a new ICD-9-CM code be established to recognize a history of falls. The rationale for the request stated:
Currently there is no ICD-9-CM diagnosis code that conveys a history of falling. Introduction of such a code can be used to identify patients at risk, conduct epidemiological research, measure quality of care, and help justify a provider’s decision to order preventive evaluation or services. The data on interventions is clearer for the elderly when a timeframe of the past 6-12 months is used. However, this code could also be used to identify associations between a history of falls and injuries in other age groups as well using different timeframes. External Cause of Injury codes (E codes) do not provide the same information since they are captured at the time of an acute injury. Many of the falls that elderly patients report, when asked, did not result in injury or a healthcare encounter.
The following new code is being proposed:
TABULAR MODIFICATION
V15 Other personal history presenting hazards to health
V15.8 Other specified personal history presenting hazards to health
New code V15.88 History of fall (ICD-9-CM Coordination and Maintenance Committee, 2004, p.16)
The request was approved by the ICD-9-CM Coordination and Maintenance Committee and was officially included in the October 1, 2005 revision of the ICD-9-CM. Both “personal history of falls” and “at risk for falls” were approved as inclusion terms for this code.
Since the time the code was adopted, some parties have assumed that recognition or use of the code would equate falls risk with “medical necessity.” For example, advertising directed at health providers for a computerized clinical device focusing on balance improvement includes the following statement:
New ICD-9 Code: V15.88 Personal History of Fall The Centers for Disease Control and Prevention (CDC) and Centers for Medicare and Medicaid Services (CMS) have created a code, V15.88 History of Fall, on the list of diagnostic codes implemented on October 1, 2005. They also listed At Risk for Fall as an inclusion term. . . . A specific fall code should heighten healthcare provider awareness of the importance of falling as a manageable medical problem, and enhance the likelihood that fall risk evaluation and management services would be considered medically reasonable and necessary services, and therefore covered. (Biodex Medical Systems, 2009.)
35
This statement captures the assumption succinctly: diagnosis equals medical necessity. However, the nature of the code and the rules and guidelines for coding do not support the assumption.
The ICD-9-CM Official Guidelines for Coding and Reporting
are a set of rules that have been developed to accompany and complement the official conventions and instructions provided within the ICD-9-CM itself. The instructions and conventions of the classification take precedence over guidelines. These guidelines are based on the coding and sequencing instructions in Volumes I, II and III of ICD-9-CM, but provide additional instruction. Adherence to these guidelines when assigning ICD-9-CM diagnosis and procedure codes is required under the Health Insurance Portability and Accountability Act (HIPAA). (CMS, 2009, p 1)
In regard to V codes, the coding guidelines state: “The Supplementary Classification of Factors Influencing Health Status and Contact with Health Services (V01.0 - V89.09) is provided to deal with occasions when circumstances other than a disease or injury (codes 001-999) are recorded as a diagnosis or problem.” (p 67) V15.88 is a V code indicating “circumstances or problems influence a person’s health status but are not in themselves a current illness or injury.” (p 67, emphasis added). Thus, by definition, the code V15.88 does not indicate a disease or injury and cannot convey medical necessity.
The rationale included in the request for the V15.88 code alluded to “external causes of injury” codes. These are “E codes,” another category of ICD-9-CM codes that is supplemental. There is an entire series of E codes (E880-E888) related to falls, where the differences in the codes reflect the physical circumstances and proximate cause of the fall. For example, E880 codes refer to falls from stairs or steps, where E880.0 indicates an accidental fall on or from an escalator, but E880.1 indicates a fall on or from a sidewalk or curb. The E885 codes indicate an accidental fall on same level from slipping, tripping, or stumbling, while E886 codes indicate an accidental fall on same level from collision pushing or shoving by or with other person. When no additional information about the circumstances is available, the code E888.8 other accidental fall, or E888.9 unspecified accidental fall, may be used.
The coding guidelines address E codes to ensure standardization in how they are used. These guidelines state:
External causes of injury and poisoning codes (categories E000 and E800-E999) are intended to provide data for injury research and evaluation of injury prevention strategies. . . . E codes capture how the injury, poisoning, or adverse effect happened (cause), the intent (unintentional or accidental; or intentional, such as suicide or assault), the person’s status (e.g. civilian, military), the associated activity and the place where the event occurred. (p. 84).
The coding guidelines also state that an E code can never be a principal (first listed) diagnosis. Under the current coding rules and guidelines, the value of V15.88 is to identify the patient’s risk of falls and, potentially, for surveillance and research. The value of the E code is surveillance and research. However, since the adoption of the V15.88 code, relatively few practitioners are aware of and have adopted use of the code. Furthermore, the supplemental status of the E codes means use is at the discretion of the practitioner or setting. Wider awareness and use of both codes across settings would have two outcomes: 1) increase provider awareness of a given patient’s risk of falls and 2) provide research and surveillance data on falls risk, falls injury, and effectiveness of prevention efforts within the population. The V15.88 code might also be used to denote a need for preventive services, but such use would require modification to

36
current coding rules and guidelines.
37
Coordination among Healthcare Providers/ Coordination with Community-Based Fall Prevention Programs
Two of the strongest recommendations in the AGS/BGS Guideline 2010 pertain to intervention and coordination:
The multifactorial fall risk assessment should be followed by direct interventions tailored to the identified risk factors, coupled with an appropriate exercise program.
The health professional or team conducting the fall risk assessment should directly implement the interventions or should assure that the interventions are carried out by other qualified healthcare professionals (2010).
Yet current policies and circumstances do not promote coordination and follow-up, especially once falls risk is identified.
Coordination of Healthcare Services
As mentioned previously, current PQRI policy may incentivize certain providers to conduct falls risk assessments, but it does not incentivize multifactorial falls risk assessment (PQRI measure requires assessment of only two factors) nor does it promote coordinated or comprehensive follow-up. Coordination and effective care transitions must occur to ensure that an older adult with a falls history or falls risk receives multifactorial fall risk assessment followed by appropriate intervention.
When an older adult presents to an urgent care center or emergency department after a fall, current policies make it difficult for coordinated follow-up in situations where the beneficiary is not hospitalized. Presenting to urgent or emergency care for a fall clearly identifies an individual as being at risk of additional falls. An emergency care provider may refer the patient back to a primary care physician for follow-up or may make a referral for follow-up care in the home. However, the emergency care provider is not in a position to provide ongoing coordination. The primary provider may or may not be notified of the emergency encounter, and the beneficiary may or may not follow up with the primary provider. The emergency care provider or the primary provider can refer to outpatient therapy for a home safety assessment or gait and balance training, but certain restraints exist.
If referral to home care is made, current home health regulations require that a physician certify and provide ongoing oversight of any homecare services, which is often unfeasible when the referral is initiated by an emergency care provider. If the beneficiary is not homebound, then the home health agency may be unable to provide services. Referral to outpatient therapy may be an alternative, but most outpatient therapy providers are not equipped to conduct assessments or to provide services in or about the home. Medicare Part B does allow for the provision of outpatient therapy services in the beneficiary’s home.
One option to make in-home assessment and intervention more available would be for more home health agencies to be Part B therapy providers. Home health agencies have the allowance under law and the infrastructure to deliver therapy evaluation and intervention in the home. The Part B therapy benefit requires a provider certification, but requires less coordination burden than the Part A home health benefit. Nor does it require that the beneficiary be homebound in order to receive the services in the home. Increased education to home health providers regarding Part B therapy service provision could increase the availability of follow-up when falls risk is identified, and would create more options for follow-up by providers such as emergency care physicians whose ability to provide or coordinate services is limited. The PPACA recently passed includes many efforts to demonstrate and test various approaches to
38
coordination of care (e.g., accountable care organizations, medical home). Attention to falls within these efforts would be an important factor for measuring success.
Coordination between Healthcare Providers and Community-Based Programs
One of the challenges to effective fall prevention is the separation between healthcare services and services or programs offered through social or human services and aging networks. Health services are provided one-on-one by physicians, nurses, pharmacists, therapists, and others, while social or human services are provided by area agencies on aging (AAA), senior centers, faith communities, non-profit organizations, and municipal or county-level social service or aging programs. These programs usually provide services to groups or populations. Older patients and their families conclude that healthcare providers deal with “medical” concerns and senior centers or AAAs deal with “social” concerns such as transportation, social contact, and activity.
At a national level, the Falls Free® Coalition is a group of national organizations and state coalitions working to reduce the growing number of falls and fall-related injuries among older adults. Nationally and at a local level, the coalition includes both healthcare provider organizations and social/aging service providers. The national coalition was established through the leadership of the National Council on Aging (NCOA) Center for Healthy Aging, with support from the Archstone Foundation and Home Safety Council (Falls Free® Coalition website, n.d). The Coalition has developed resources and spotlighted best practices for community- based fall prevention initiatives.
The CDC, through the National Center for Injury Prevention and Control (NCIPC), is involved in state and local fall prevention efforts to translate falls prevention research into evidence-based practice at the community level. Through an interagency agreement between the CDC and the Administration on Aging (AoA), AoA currently provides 24 states with three-year grants designed to mobilize the aging, public health, and non-profit networks at the state and local level. Four evidence-based or evidence-informed fall prevention models are being implemented: Matter of Balance; Stepping On; Tai Chi, and Step by Step. (CDC, 2008)
CDC, under this interagency agreement, is conducting three activities related to falls prevention:
Supporting the efforts of the Falls Free Coalition.
Assessing the long-term impact of Matter of Balance.
Estimating the average [program] implementation and maintenance costs and comparing these costs across three AoA-funded fall prevention programs: Matter of Balance, Moving for Better Balance, and Stepping On. (CDC, 2008)
As a result of the efforts of the CDC, NCOA, AoA and the Coalition, a growing number of communities have evidence-based falls prevention programs available to the older adults living in those communities.
But integration between health and community systems is still lacking. The divide between health services and aging/social services means health providers and institutions may be unaware of the services and resources of the community system. While CMS policies such as PQRI and other quality initiatives may increase health providers’ awareness of falls and falls risk, healthcare providers are often unaware of the services provided through the local aging network, including evidence-based falls prevention programs. It is essential that healthcare providers recognize that community-based, lay-led or professionally-led programs (that are evidence-based or evidence-informed) are an important part of the intervention “toolbox” for reducing falls risk and preventing falls among older adults. Similarly, community-based

39
programs must be aware of the services to address falls risk that can be offered only by a qualified healthcare provider.
Healthcare provider awareness of lay-led community programs can be increased through a variety of approaches, including: 1) Identifying state or local falls coalitions in communications to providers by Medicare; 2) educating providers regarding the evidence-informed and evidence-based programs being promulgated under the CDC-AoA agreement; and 3) identifying referral to community-based falls programs as an option in the falls prevention interventions identified in the PQRI measures and in the OASIS process measure and plan of care item. An additional strategy would be to incentivize healthcare providers (as individuals or organizations) to join and participate in their state or local falls prevention coalitions or to establish fall prevention coalitions if none exist in their area. Educational materials to providers (such as those provided through the Medicare Learning Network) could be more direct in linking falls prevention and risk reduction to community options. A Medicare demonstration project might be developed focusing on coordination of falls prevention efforts between healthcare providers and evidence-based community programs.
40
Healthcare Reform: New Developments
Section 4103 of the Patient Protection and Affordable Care Act of 2010 (P.L. 111-148) (PPACA) establishes a new Medicare preventive service benefit that has implications for falls prevention. The benefit is an annual wellness visit providing a personalized prevention plan. A personalized prevention plan service is defined as:
the creation of a plan for an individual that includes a health risk assessment . . .and that (i) takes into account the results of the health risk assessment; and (ii) may contain these elements:
The establishment of, or an update to, the individual’s medical and family history.
A list of current providers and suppliers that are regularly involved in providing medical care to the individual (including a list of all prescribed medications)
A measurement of height, weight, body mass index (or waist circumference, if appropriate), blood pressure, and other routine measurements.
Detection of any cognitive impairment.
The establishment of, or an update to, the following:
o A screening schedule for the next 5- to-10 years, as appropriate, based on recommendations of the United States Preventive Services Task Force and the Advisory Committee on Immunization Practices, and the individual’s health status, screening history, and age-appropriate preventive services covered under this title.
o A list of risk factors and conditions for which primary, secondary, or tertiary prevention interventions are recommended or are underway, including any mental health conditions or any such risk factors or conditions that have been identified through an initial preventive physical examination (as described under subsection (ww)(1)), and a list of treatment options and their associated risks and benefits.
‘The furnishing of personalized health advice and a referral, as appropriate, to health education or preventive counseling services or programs aimed at reducing identified risk factors and improving self-management, or community-based lifestyle interventions to reduce health risks and promote self management and wellness, including weight loss, physical activity, smoking cessation, fall prevention, and nutrition.
Any other element determined appropriate by the Secretary (of HHS). (Emphasis added)
For the purposes of this new benefit, a health professional is a physician, physician assistant, nurse practitioner, clinical nurse specialist, a medical professional (including a health educator, registered dietitian, or nutrition professional) or a team of medical professionals, as determined appropriate by the Secretary, under the supervision of a physician. (Section 4103(B) and (C))
41
Not later than one year from enactment, the HHS secretary shall establish publicly available guidelines for health risk assessments to be part of this Annual Wellness Visit, developed in consultation with relevant groups and entities. Health risk assessments shall:
1) identify chronic diseases, injury risks, modifiable risk factors, and urgent health needs of the individual; and 2) may be furnished—
through an interactive telephonic or web-based program that meets the standards to be established;
during an encounter with a healthcare professional;
through community-based prevention programs; or
through any other means the Secretary determines appropriate to maximize accessibility and ease of use by beneficiaries, while ensuring the privacy of such beneficiaries.
The Secretary of HHS may coordinate with community-based entities (including State Health Insurance Programs, Area Agencies on Aging, Aging and Disability Resource Centers, and the Administration on Aging) to ensure that health risk assessments are accessible to beneficiaries and provide appropriate support for the completion of health risk assessments by beneficiaries.
This new benefit builds on the general intent of the IPPE, not only in making the preventive service annual, but also by focusing on the individual preventive services plan, emphasizing steps to reduce risk and optimize health. Falls risk is explicitly identified as an element of the plan. In addition, PPACA recognizes a wide range of providers and intervention strategies to conduct screenings and interventions, explicitly identifying community networks and the Administration on Aging. What is not explicit is whether preventive services included in the personalized preventive services plan will be covered if they are not currently covered by Medicare.
The provisions of the PPACA have many implications for the policy issues previously identified, especially when combined with the Medicare Improvements for Patients and Providers Act of 2008(P.L. 110-275) (MIPPA) provisions that modified the process for authorizing covered preventive services. The establishment of coverage for an annual wellness visit means beneficiaries can receive a covered falls risk assessment annually, rather than the single “Welcome to Medicare” physical currently covered. The requirement for a personalized prevention plan, including a health risk assessment, means that beneficiaries found to be at risk for falls will receive a plan with information and recommendations based on their individual risks and needs. The provisions of section 4103 also build stronger linkages to community-based programs and service delivery methods that are community-based rather than facility/institution-based.
42
Toward Enhancing Medicare Payment Policy and Utilization: Summary of Findings
One of the challenges of addressing payment and policy issues to promote falls prevention is that falls prevention is not a singular service. Falls prevention is a process and a set of services or activities which depend on the specific falls risk profile of the individual and require both ongoing monitoring and change to accommodate new circumstances in health, mobility and living situation. The AGS/BGS Guideline 2010 recommendations, drawn from best available research evidence, indicate that falls risk assessment, identification of the risk factors specific to an individual, and intervention directed to those risk factors can prevent falls among community dwelling older adults. Steps toward enhancing Medicare payment policy and utilization to address falls prevention include:
Increasing beneficiary awareness of falls risk and the falls risk assessment included in the Welcome to Medicare visit and, once implemented, the annual wellness visit authorized by PPACA;
Increasing provider awareness and understanding of the importance of falls risk assessment and follow-up with a falls risk intervention plan;
Ensuring that both guidance and requirements associated with the quality initiatives is consistent with current and emerging evidence related to falls prevention;
Provider education to promote consistent and widespread use of the falls risk code, V15.88, so that beneficiaries identified at risk of falls are identified as such in their healthcare records;
Provider education to increase coordination with community-based fall prevention programs, possibly including incentives for meaningful provider participation in national or local falls-free coalitions;
Resolution of inconsistencies across LCDs as they pertain to assessments and intervention related to falls risk and consideration of a national coverage determination on this issue;
Creation of a falls risk prevention/intervention benefit which includes occupational and physical therapy, DME, and vitamin D, and coordinated with community based fall prevention programs. The benefit could be triggered by identification of falls risk (V15.88) and would include services from those listed which address the beneficiary’s falls risk factors and would be covered even in the absence of a specific “medically necessary” diagnosis. The DME component would include mobility devices regardless of prior receipt and would also include bathroom safety devices which have assigned HCPCS codes. Where evidence-based fall prevention programs are available, any beneficiary deemed able to participate would be referred to such programs;
Inclusion of additional services in the benefit upon emergence of grade A or B recommendations of such interventions for falls risk reduction;
Promoting use of the V code denoting falls risk among all healthcare providers. Promoting the use of E falls codes, especially by emergency, urgent, and primary care providers;
Review of usage/claims data to monitor falls-related service utilization by beneficiaries who have received the falls prevention benefit.
43
References Alexander BH, Rivara FP, & Wolf ME.(1992). The cost and frequency of hospitalization for fall–
related injuries in older adults. American Journal of Public Health,82(7):1020–3. American Geriatrics Society & British Geriatrics Society (2010). Prevention of Falls in Older
Person: Clinical Practice Guidelines. Retrieved 5/24/10 from http://www.medcats.com/FALLS/frameset.htm
American Geriatrics Society, British Geriatrics Society & American Academy of Orthopedic Surgeons Panel on Falls Prevention. (2001). Guideline for the prevention of falls in older persons. Journal of the American Geriatrics Society, 49, 664-672.
Bell, A.J., Talbot-Stern, J.K. & Hennessy, A. (2000). Characteristics and outcomes of older patients presenting to the emergency department after a fall: a retrospective analysis. Medical Journal of Australia 173(4):176–7.
Biodex Medical Systems. (2009). Retrieved 5/14/10 from http://www.biodex.com/rehab/balance/balance_300feat.htm
Cahaba Government Benefit Administrators. (2009). LCD for Medicine: Occupational Therapy - Outpatient (L30007). Retrieved 5/24/10 from http://www.cms.gov/mcd/viewlcd.asp?lcd_id=30007&lcd_version=22&basket=lcd%3A30007%3A22%3AMedicine%3D%3D++Occupational+Therapy+%2D+Outpatient%3AMAC+%2D+Part+A%3ACahaba+Government+Benefit+Administrators%7C%7C+LLC+%2810201%29%3A
Cameron, I.D., Murray, G.R., Gillespie, L,D., Robertson, M.C, Hill, K.D., Cumming, R.G. & Kerse, N. (2010). Interventions for preventing falls in older people in nursing care facilities and hospitals. Cochrane Database of Systematic Reviews 2010, (1).
Centers for Disease Control and Prevention, National Center for Injury Prevention and Control. Web–based Injury Statistics Query and Reporting System (WISQARS) [online]. (2005) Retrieved 5/24/2010 from http://www.cdc.gov/injury/wisqars/index.html.
Centers for Disease Control and Prevention. (2008). CDC Fall Prevention Activities. Retrieved from : http://cdc.gov/HomeandRecreationalSafety/Falls/FallsPreventionActivity.html on 5/7/10
Centers for Disease Control and Prevention. (2009). Falls Among Older Adults: An Overview. Retrieved 3/18/10 from http://www.cdc.gov/HomeandRecreationalSafety/Falls/adultfalls.html.
Centers for Disease Control and Prevention. (n.d.) CDC Fall Prevention Activities. Retrieved 4/5/10 from http://www.cdc.gov/HomeandRecreationalSafety/Falls/FallsPreventionActivity.html.
Centers for Medicare & Medicaid Services (2008a). Fact Sheet: Implementation of Payment Related Provisions in the Medicare Improvements for Patients and Providers Act of 2008. Retrieved 5/16/10 from http://www.cms.gov/apps/media/press/factsheet.asp?Counter=3332&intNumPerPage=10&checkDate=&checkKey=&srchType=1&numDays=3500&srchOpt=0&srchData=&keywordType=All&chkNewsType=6&intPage=&showAll=&pYear=&year=&desc=false&cboOrder=date
Centers for Medicare & Medicaid Services. (2008b). Revised Long-Term Care Facility Resident Assessment Instrument User’s Manual Version 2.0. Baltimore, MD: Author.
Centers for Medicare & Medicaid Services. (2009a). Long-Term Care Facility Resident Assessment Instrument User’s Manual Version 3.0. Baltimore, MD: Author.
Centers for Medicare & Medicaid Services. (2009b). OASIS C Guidance Manual. Baltimore, MD: Author.
Centers for Medicare & Medicaid Services. (2010a). Medicare & You 2010. Baltimore: Author. Centers for Medicare & Medicaid Services. (2010b). Medicare preventive services quick
reference information: The ABCs of providing the initial preventive physical examination.
44
Medicare Learning Network. ICN 006904. Retrieved 5/7/10 from https://www.cms.gov/MLNProducts/downloads/MPS_QRI_IPPE001a.pdf .
Centers for Medicare & Medicaid Services. (2010c). 2010 Physician Quality Reporting Initiative Measure Specifications Manual for Claims and Registry Reporting of Individual Measures. Author: Baltimore.
Centers for Medicare & Medicaid Services. (2010d). Local Coverage Determinations. Retrieved 7/03/10 from http://www.cms.gov/DeterminationProcess/04_LCDs.asp
Centers for Medicare & Medicaid Services. (n.d.). Medicare Benefit Policy Manual, Publication 100-02. Retrieved 5/24/10 from http://www.cms.gov/Manuals/IOM/itemdetail.asp?filterType=none&filterByDID=-99&sortByDID=1&sortOrder=ascending&itemID=CMS012673&intNumPerPage=10
Centers for Medicare & Medicaid Services/National Center for Health Statistics. (2009). ICD-9-CM Official Guidelines for Coding and Reporting. Retrieved 5/18/10 from http://www.cdc.gov/nchs/data/icd9/icdguide09.pdf
Clemson, L., Cumming, R.G., Kendig, H., Swann, M., Heard, R., & Taylor, K. (2004). The effectiveness of a community-based program for reducing the incidence of falls in the elderly: A randomized trial. Journal of the American Geriatrics Society, 52, 1487-1494.
Close, J., Ellis, M., Hooper, R., Glucksman, E., Jackson, S & Swift, C. (1999.) Prevention of falls in the elderly trial (PROFET); a randomised controlled trial. Lancet, 353, 93-97.
Cumming, R.G., Thomas, M., Szonyi, G, Salkeld, G. O’Neill, E. Westbury, C. & Frampton, G. (1999.) Home visits by an occupational therapist for assessment and modification of environmental hazards: a randomized trial of falls prevention. J. American Geriatric Society, 47, 1397-1402.
Drinka, P.J., Krause, P.F., Nest, L.J. & Goodman, B.M. (2007). Determinants of vitamin D levels in nursing home residents. Journal of the American Medical Directors Association, 8(2), 76-79.
Falls Free Coalition website. (n.d.) Retrieved 5/18/10 from http://www.healthyagingprograms.org/content.asp?sectionid=113.
Finlayson, M. & Peterson, E. (2010). Falls, aging and disability. Physical Medicine and Rehabillitation Clinics of North America, 21, 357-373.
Gillespie, L.D., Robertson, M.C., Gillespie, W.J., Lamb, S.E., Gates, S., Cumming, R.G., et al. (2009). Interventions for preventing falls in older people living in the community. Cochrane Database of Systematic Reviews, 2, CD007146.
Harris, R.P., Helfand, M., Woolf, S.H., Lohr, K.N., Mulrow, C.D., Teutsch, S.M. & Atkins, D. (2001). Current methods of the US Preventive Services Task Force: A review of the process. American Journal of Preventive Medicine, 20, 21–35.
Hausdorff, J.M,. Rios, D.A. & Edelber, H.K. (2001). Gait variability and fall risk in community–living older adults: a 1–year prospective study. Archives of Physical Medicine and Rehabilitation, 82(8):1050–1056.
Hornbrook, M.C., Stevens, V.J., Wingfield, D.J., Hollis, J.F., Greenlick, M.R. & Ory M.G.(1994). Preventing falls among community–dwelling older persons: results from a randomized trial. The Gerontologist 34(1), 16–23.
ICD-9-CM Coordination and Maintenance Committee. October 7-8, 2004. Diagnosis Agenda. Retrieved 5/18/10 from http://www.cdc.gov/nchs/data/icd9/agendaoct04.pdf.
Jager ,T.E., Weiss, H.B., Coben,J.H. & Pepe, P.E. (2000). Traumatic brain injuries evaluated in U.S. emergency departments, 1992–1994. Academic Emergency Medicine,7(2):134–140.
National Council on Aging (2005). National Falls Free Action Plan. Retrieved on 7/03/10 from
http://www.healthyagingprograms.org/content.asp?sectionid=69&ElementID=220 Medicare Improvements for Patients and Providers Act of 2008. P.L. 110-275.
45
Medicare.gov. (n.d.) Welcome to Medicare Physical Exam. Retrieved 4/5/10 from http://www.medicare.gov/health/physicalexam.asp.
Palmetto GBA. (2009). Part A Intermediary: Falls evaluation: Translating evidence-based interventions into your practice. Retrieved 5/7/10 from http://www.palmettogba.com/palmetto/providers.nsf/docsCat/Providers~Part%20A%20Intermediary~Articles~General~Falls%20Evaluation%20Translating%20Evidence-based%20Interventions%20into%20Your%20Practice?open
Palmetto GBA. (2010). LCD for Outpatient Occupational Therapy (L1149) Retrieved 5/7/10 from http://www.cms.gov/mcd/viewlcd.asp?lcd_id=1149&lcd_version=89&show=all
Patient Protection and Affordable Care Act of 2010. P.L. 111-148. Preventive Services: One-time "Welcome to Medicare" Physical Exam,
http://www.medicare.gov/health/physicalexam.asp, retrieved 4/5/10. Rizzo, J.A., Friedkin, R., Williams, C.S., Nabors J., Acampora, D. & Tinetti, M.E. (1998). Health
care utilization and costs in a Medicare population by fall status. Medical Care 36(8), 1174–1188.
Safety of Seniors Act of 2007. P.L. 110-202. Schell, B.A.B. (2009). Pragmatic reasoning. In Clinical and Professional Reasoning in
Occupational Therapy. BAB Schell & JW Schell, Eds.) Philadelphia, PA: Lippincott, Williams & Wilkins.
Scott JC. Osteoporosis and hip fractures. (1990). Rheumatic Diseases Clinics of North America, 16(3): 717–740.
Social Security Act of 1965. Exclusions from coverage and Medicare as secondary payer. Sec. 1862. [42 U.S.C. 1395y] (a).
Social Security Act of 1965. Exclusions from coverage and Medicare as secondary payer. Sec. 1862. [42 U.S.C. 1395y] (a).
Sterling, D.A., O'Connor, J.A. & Bonadies, J. (2001). Geriatric falls: injury severity is high and disproportionate to mechanism. Journal of Trauma–Injury, Infection and Critical Care, 50(1):116–119.
Stevens, J.A., Corso, P.S., Finkelstein, E.A.& Miller, T.R.(2006). The costs of fatal and nonfatal falls among older adults. Injury Prevention,12, 290–295.
Stevens, J.A., Noonan, R.K, & Rubenstein, L.Z. (2010). Older adult fall prevention: Perceptions, beliefs and behaviors. American Journal of. Lifestyle Medicine, 4. 16-20.
Stevens, J.A., Thomas, K., Teh, L., & Greenspan, A.I. (2009). Unintentional fall injuries associated with walkers and canes. Journal of the American Geriatrics Society, 57, 1464–1469.
Stevenson, D.G., Huskamp, H. A. & Newhouse, J.P (2008). Medicare Part D and the nursing home setting. The Gerontologist, 48(4), 432-441.
The Medicare Improvements for Patients and Providers Act of 2008. P.L. 110-275. World Health Organization. (2001). International Classification of Functioning, Disability and
Health. Author: Geneva. Vellas, B.J., Wayne, S.J., Romero, L.J., Baumgartner, R.N. & Garry, P.J. (1997). Fear of falling
and restriction of mobility in elderly fallers. Age and Ageing, 26, 189–193.
46
Appendix A: Interview Compendium
FALL PREVENTION POLICY
Compilation of Common Themes
Identified through Interviews With Individuals and Representatives of Organizations
At the request of the Centers for Disease Control and Prevention (CDC), during March and April 2010, the American Occupational Therapy Association conducted interviews with individuals and organizational representatives who have a strong interest in the issue of fall prevention among the elderly. Interviews were conducted with seven individual experts and with representatives of a wide range of organizations (listed below), representing Federal government agencies, providers, and other nonprofit organizations concerned with fall prevention in the elderly. An overview of those interviews begins on next page.
ORGANIZATIONS PARTICIPATING IN INTERVIEW SESSIONS
1. Administration on Aging 2. Agency for Healthcare Research and Quality 3. American Academy of Family Practitioners 4. American Association of Homes and Services for the Aging 5. American Bar Association, Medicare Advocacy Project 6. American College of Physicians 7. American College of Surgeons Committee on Trauma 8. American Medical Association 9. American Optometric Association 10. American Physical Therapy 11. American Public Health Association 12. American Society of Consultant Pharmacists 13. Home Safety Council 14. Missouri Alliance for Home Care 15. National Academy of Home Care Physicians 16. National Association of Area Agencies on Aging 17. National Association of Community Health Centers 18. National Association of Directors of Nursing Administration in Long Term Care 19. National Association for Home Care and Hospice 20. National Association of Professional Geriatric Care Managers 21. National Association of State Medicaid Directors 22. National Council on Aging 23. National Safety Council 24. Programs of All-inclusive Care for the Elderly (PACE®) 25. Rebuilding Together 26. Staying Healthy through Education and Prevention (STEP) 27. Visiting Nurse Service of New York 28. Visiting Nurse Associations of America
47
OVERARCHING ISSUES
1. Use health care reform’s focus on prevention as an opportunity to make fall prevention a national priority.
2. Create a dedicated funding stream for fall prevention and ensure CDC funding for evidence-based programs.
3. Create consistent policy language across all funding streams.
4. Consider fall prevention a chronic rather than acute condition to be treated over a lifetime.
5. Create a multi-disciplinary approach to fall prevention with seamless coordination of all health and services providers—clinical and nonclinical--who care for at-risk elderly
6. Link providers across the spectrum with aging services and evidence-based community programs.
7. Reimburse for prevention, maintenance of function, and all medically necessary equipment and home modification related to falls.
8. Optimize role of vision care in falls prevention.
9. Energize communities to take the lead in providing a safe environment.
10. Demonstrate the cost benefit of fall prevention, including the value of shortening acute episodes and preventing nursing home admissions.
11. Create national outreach and education to achieve common understanding and goals for departments of public health, families, residents, providers, and CMS of how dramatically falls affect people.
TARGETED AUDIENCES FOR RECOMMENDED ACTIONS
CONGRESS
1. Educate Congress that the issue of older adult falls is a health crisis.
2. Create public awareness by making the first day of Fall “Annual Fall Awareness Day.”
FEDERAL OR STATE AGENCIES
3. Designate fall prevention as a top DHHS priority.
4. Provide strong funding for fall prevention activities in communities and throughout health services systems.
5. Create additional partnerships among government agencies to support national initiatives (similar to approach used with influenza immunization initiatives).
6. Support use of taxonomy of ICF rather than ICD to promote better surveillance regarding falls for research, reimbursement of service, and policy development.
7. Improve surveillance and data collection on falls. Many falls currently go unreported, which causes difficulty in conducting falls research.
8. Improve surveillance on intervention outcomes.
9. Improve reporting issues:
a. Define what constitutes a fall;
b. Develop fall prevention criteria;
48
c. Develop state descriptors for fall prevention.
10. Develop guidelines for public funding of fall prevention programs; limit funding to evidence-based programs.
11. Fund professionally led, multidisciplinary evidence- and community-based programs that include all disciplines including psychiatric and other mental health providers, and follow patients into nursing homes and hospitals.
12. Promote optimum use of professional registered nurses, OTs and PTs in community programs demonstrating evidence of need for these professionals.
13. Conduct large professional and public education programs.
14. Raise public and professional awareness about complexity of falls.
15. Demonstrate that fall prevention creates savings for the health care system, and plow savings back into fall prevention.
16. Focus evaluation of fall prevention programs on percentages of the elderly for whom health and wellness was improved rather than the number of fall prevention programs conducted.
17. Create demonstration programs to provide complete understanding of what is medically necessary, including attention to factors such as depression and social isolation, and the broad range of services needed to achieve full knowledge of actual cost savings.
SPECIFIC DISCIPLINES
A. Occupational therapy: Increase role for occupational therapists to:
18. Conduct in-home assessments;
19. Watch patients do daily activities to understand how they function at home;
20. Help patients appreciate and manage their own capacities;
21. Demonstrate that equipment is medically necessary;
22. Train patient aides and families on proper use and maintenance of equipment;
23. Open in-home health cases without delays that currently exist;
24. Better understand existing reimbursement policies, measures, and opportunities in providing home health care;
25. Link patients to information and local community resources
26. Explore opportunities for state Medicaid waivers that allow reimbursement for OT and PT that is not otherwise reimbursable.
B. Physical Therapy:
27. Allow reimbursement for patients to get direct access to physical therapy without delay or a physician order.
28. Reimburse PT for falls screening, and for evaluation and care after screening
29. Allow for preventive PT therapy for at risk patients.
30. Address caps, which affect all Medicare patients.
49
C. Vision Care:
31. Integrate eye health into all programs and policies that affect health and make it part of any health prevention activity, as eye problems are one major cause of falls.
32. Reimburse for attention to asymptomatic eye disease, to allow intervention at the optimum time for correction.
D. Pharmacy
33. Eliminate differences between pharmacist definition of Medication Therapy Management and the legislative definition.
34. Conduct research on medications suitable for frail elderly
35. Reimburse pharmacists for conducting medication reviews and providing other education that can help prevent falls.
E. Family Physicians and Geriatricians
36. Educate physicians about community programs.
37. Provide education opportunities about falls, including evidence-based information, to improve identification of falls risk and falls interventions.
LOCAL/COMMUNITY
38. Examine causative factors for falls in the community, including street, sidewalks, walking paths, pedestrian intersections and lighting design.
39. Involve the whole communities in making environment safe.
40. Examine building codes and zoning requirements and other restrictions that are barriers for establishing community exercise activities and promoting mobility.
41. Set policies that encourage universal design.
42. Examine transportation needs and alternatives.
FUNDING AND RESEARCH ISSUES
FUNDING
43. Consider and reimburse for fall risk as a chronic disease to be addressed over the lifetime, rather than an acute incident.
a. Provide a continuum of care for maintenance after a patient plateaus for fulfilling active life;
b. Revise “improvement standard” that stops reimbursement when patient plateaus;
c. Promote ways to enhance quality of life.
44. Address Medicare therapy caps, which affect all patients including those who have fallen.
45. Reimburse for fall prevention screening at annual medical visit. (Note: This issue was addressed in recent health care reform law PPACA which added an annual wellness visit to Medicare benefits.)
46. Monitor research and evidence that provision of patient education as well as sufficient amounts of physical therapy, occupational therapy or other services provided for certain individuals provides benefits to warrant reimbursement for these services at appropriate interims even after the patient is no longer improving under the current coverage guideline.
50
47. Align payment policy with evidence-based home care services to promote more uniform interventions to promote long-term affect on incidence of falls.
48. Discontinue limitations on use of physical therapy (PT)/occupational therapy (OT) staff for home safety evaluations recommending equipment that is not paid for by Medicare.
49. Reimburse for all durable equipment needed at discharge from nursing homes, including ramps, bath chairs, etc.
50. Ensure that wheelchairs provided actually fit personal physical capability of patient and residence requirements.
51. Provide coverage for evaluating need for as well as buying and installing needed safety equipment of patient, including needs of bariatric-sized patients.
52. Enact policies to reflect family and caregiver needs to better understand and manage cognitive issues as they affect safety.
53. Remove home-bound status criteria limit in Medicare home health benefit so that people with chronic disease who still participate in the community can obtain appropriate services.
54. Create multifactorial policy that broadly expects all providers to work together seamlessly, including physicians, therapists, psychiatrists, eye care specialists, pharmacists, etc.
55. Reimburse for preventive eye care to allow identification of problems at the asymptomatic stage, the optimum time for correction.
56. Reimburse for continuing services that would benefit patients after they leave a fall prevention program to sustain function.
57. Reimburse for patient education about provider recommendations related to fall prevention (e.g., exercise programs, referral to community programs).
58. Create consistent incentives for providers to conduct fall prevention assessments and develop and implement a plan of care.
59. Balance pay-for-performance approach which encourages aggressive control of a specific disease but may also contribute to falls; for example, medication used for aggressive blood pressure control may contribute to falls.
60. Create incentives for postural blood pressure checks.
61. Improve provider understanding and competence about reimbursable services and how to accurately document for those services.
62. Reimburse for training caregivers about how to better protect patients from fall risks.
63. Cover home modification for both medical and quality of life enhancement.
64. Better educate public and caregivers about how to appeal a denial of Medicare coverage.
65. Eliminate inconsistencies among states in Medicaid reimbursements related to fall prevention (i.e., reimbursement for in-home safety equipment.)
66. Educate providers about community-based fall prevention options, especially in relation to fulfilling falls items under PQRI.
RESEARCH AND DATA COLLECTION NEEDS
67. Analyze and publicize home health OASIS assessment data to provide a baseline as to any emergency room visits or inpatient hospitalization related to falls.
51
68. Collect data on if and how providers are proactively using V codes.
69. Collect data on use of PQRI fall prevention measures.
70. Determine cost effectiveness of fall prevention activities.
71. Develop tracking mechanism for collecting data on Medicaid’s share of the cost of falls.
72. Determine length of stay due to fall-related injury and in-hospital falls.
73. Study fear of fall programs to determine impact on reducing the rate of falls.
74. Fund initial studies and clinical trials that take place in setting in which they would ultimately be deployed, for example, in patient homes, assisted living facilities, and nursing homes; collaborate with various settings to improve translation opportunities.
75. Study frail population that has sustained multiple falls in a controlled trial to determine what is effective in preventing further falls and to improve cost savings and health and wellness.
76. Study how intervening earlier with ambulatory individuals living in the community might help prevent later injuries and associated costs.
77. Conduct research on medications suitable for frail elderly.
52
APPENDIX B
SURVEY OF HEALTH CARE PROVIDERS
Fall Prevention Policy
In conjunction with its initiative to examine policy related to fall prevention in the elderly, the Centers for Disease Control and Prevention (CDC) contracted with the American Occupational Therapy Association (AOTA) (Contract No. (200-2009-M31264) to conduct a survey with nine providers in geriatric health care to examine their experiences related to this topic. The CDC and AOTA agreed that nine different specialties would be included, and AOTA identified nine individuals representing those specialties who agreed to complete the survey. The nine disciplines included:
1. Geriatrics
2. Internal medicine
3. Physical therapy
4. Occupational therapy
5. Home Health Nursing
6. Physician’s assistant
7. Community pharmacy
8. Optometry
9. Homecare Medicine
Major findings identified by the survey respondents are reported below. It is important to note that many providers advocate and recommend fall prevention interventions for their client, but they identify the lack of coverage as a major barrier to their implementation, and therefore, their effectiveness. This survey identified a number of needs, including more provider and patient education on fall prevention, adequate reimbursement especially in preventative care and safety devices, and public awareness of the role of these providers in fall prevention.
MAJOR FINDINGS
Screening:
Most responding providers (5/9) screen their patients over the age of 65 at every encounter and if the patient mentions or has been injured in a fall (6/9)
Most screened with by eliciting a falls history (8/9) or a mobility and gait assessment (6/9), while some used various other assessments (4/9). These other assessments included:
o Medication review for fall-risk meds; o Obtaining fall history from family; o Identification of other clinical factors that may increase an individual’s risk for falls
(i.e. diagnoses, frailty, incontinence, poly-pharmacy); o Timed Up and Go test o Activities-Specific Balance Confidence or ABC Scale o Tinetti Balance Test; and o Berg Balance Scale.
The majority of respondents identify patients who have had a previous history of falls (8/9), and use of a mobility device (7/9) as risk factors for falls. Other factors identified include:
53
o Being a senior patient; o Having a fall with injury; o The presence of dizziness or vertigo; o Low vision; o Cognitive impairment o Cluttered living space o Fear of falling; o Poly-pharmacy; and o Low blood pressure.
Although many respondents did not identify constraints that prevented a fall screening, a few (2/9) practitioners identified limited time with the patient and unfamiliarity with the screening tools/process as keeping them from evaluating every patient.
Many of the responding practitioners (7/9) documented fall risks in the narrative of their notes while a few (3/7) use ICD-9 codes such as V15.88 or 781.2. 1
Intervention:
Interventions that had the most recommendations included balance/strengthening training, use of a mobility device, use of a personal emergency response unit 2 , and implementation of environmental modifications. Of the respondents who reported recommending other interventions, all supported modification to patient’s medication regimen, reduction or elimination of medications associated with fall risk, home safety assessment. In addition, six said they recommend alternative footwear. (Refer to Graph 1)
Other professions that were recommended or referred to patients in need of fall prevention intervention were: physical therapy, occupational therapy, podiatry, or a combination of professionals including OT, PT, and podiatry, as well as optometry, community exercise programs, dietetics, and pharmacy. (Refer to Graph 2)
All respondents reported referring to other disciplines but 2 of 9 reported that when they did not refer it was due to time constraints and lack of familiarity with other disciplines.
Some (4/9) practitioners referred to community or non-medical fall prevention programs such as community senior center programs, YMCA programs, county senior health programs, or a community exercise program. Most respondents did not identify a community resource that they used (5/9).
Provision of printed educational materials generated a mixed in respondents (5 yes, 4 No). Some sources of fall prevention literature identified include: o Mayo Clinic resources; o Web links; o CDC; o American Geriatrics Society information; o Agency for Healthcare Research and Quality; o New Hampshire Falls Risk Reduction Task Force ; and o Home Safety Council
Most practitioners reported that they coordinated a follow-up on their recommended intervention (7/9), but many of these were not consistent (5/9).
1 The code 871.2 indicates abnormality of gait rather than a falls risk.
2 The personal emergency response is not a fall prevention devise per se, but rather is designed to help an individual
call for assistance in an emergency.
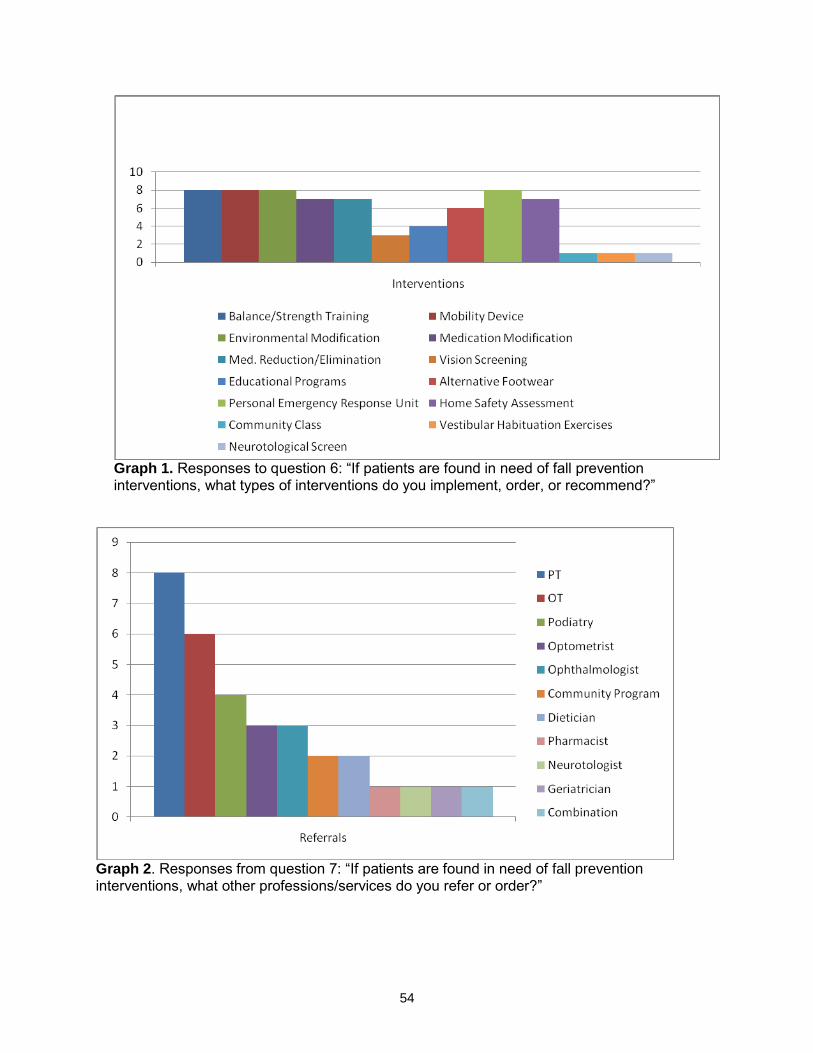
54
Graph 1. Responses to question 6: “If patients are found in need of fall prevention interventions, what types of interventions do you implement, order, or recommend?”
Graph 2. Responses from question 7: “If patients are found in need of fall prevention interventions, what other professions/services do you refer or order?”
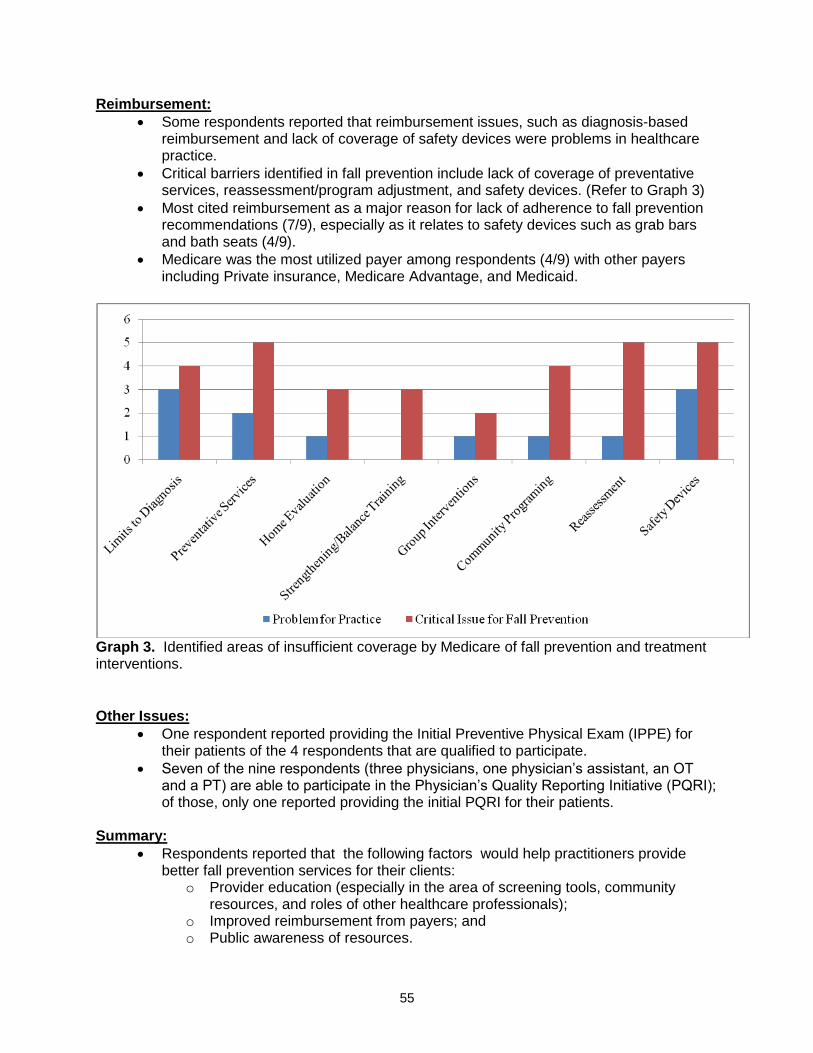
55
Reimbursement:
Some respondents reported that reimbursement issues, such as diagnosis-based reimbursement and lack of coverage of safety devices were problems in healthcare practice.
Critical barriers identified in fall prevention include lack of coverage of preventative services, reassessment/program adjustment, and safety devices. (Refer to Graph 3)
Most cited reimbursement as a major reason for lack of adherence to fall prevention recommendations (7/9), especially as it relates to safety devices such as grab bars and bath seats (4/9).
Medicare was the most utilized payer among respondents (4/9) with other payers including Private insurance, Medicare Advantage, and Medicaid.
Graph 3. Identified areas of insufficient coverage by Medicare of fall prevention and treatment interventions.
Other Issues:
One respondent reported providing the Initial Preventive Physical Exam (IPPE) for their patients of the 4 respondents that are qualified to participate.
Seven of the nine respondents (three physicians, one physician’s assistant, an OT and a PT) are able to participate in the Physician’s Quality Reporting Initiative (PQRI); of those, only one reported providing the initial PQRI for their patients.
Summary:
Respondents reported that the following factors would help practitioners provide better fall prevention services for their clients:
o Provider education (especially in the area of screening tools, community resources, and roles of other healthcare professionals);
o Improved reimbursement from payers; and o Public awareness of resources.

56
Additional comments about ways to improve fall prevention services for older patients include:
o “Objective measures of deficits contributing to risk of fall (lower extremity weakness, gait speed, Timed Up and Go or Dynamic Gait Index (DGI) scores, etc.) satisfy the justification for need of services and plan of care addressing the deficits. “(Physical Therapist)
o “For those living independently, a home safety evaluation as a service that could be requested by family, social workers, or physical therapists independent of physicians, combined with some way to implement recommendations.” (Home Health Practitioner)
o “I think emphasis years earlier on physical fitness, obesity, etc would help. Many of the falls occur when patients try to do things in their home-change a light bulb, etc. Often trip because of rushing, not necessarily unsafe condition.” (Internist)
o All visually impaired patients, especially seniors, should have slip and fall prevention therapy. We are working towards this with a better OT model.” (O.D.)
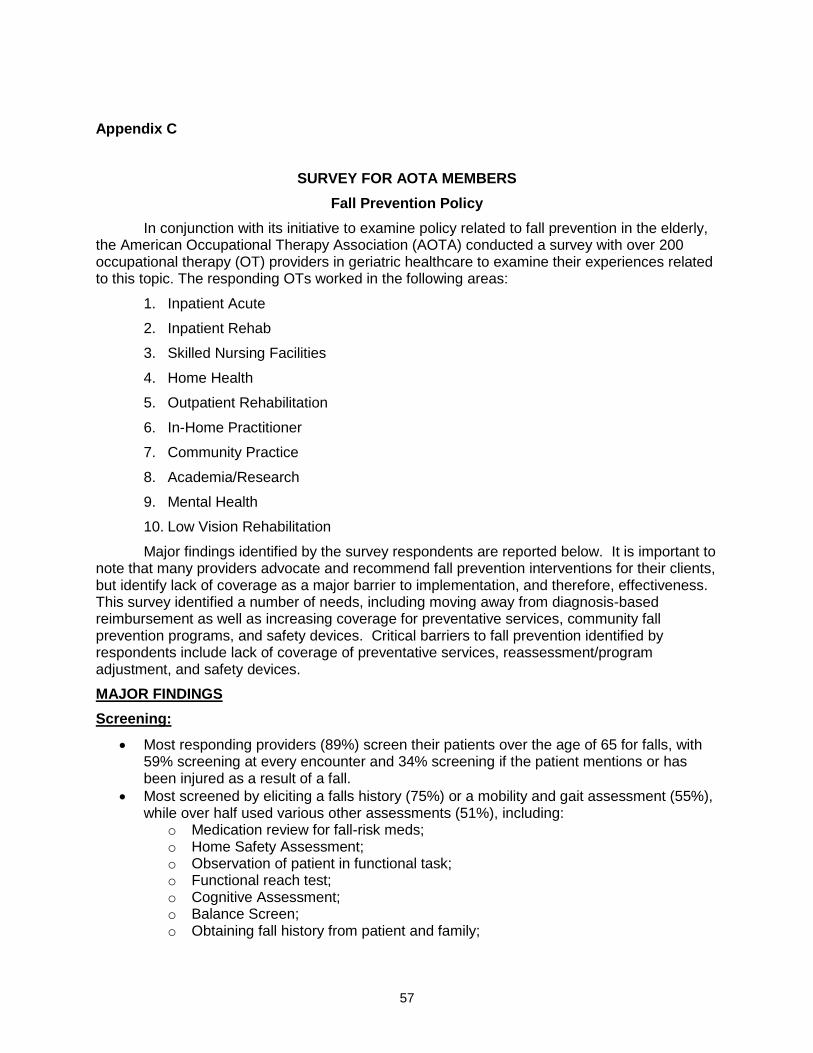
57
Appendix C
SURVEY FOR AOTA MEMBERS
Fall Prevention Policy
In conjunction with its initiative to examine policy related to fall prevention in the elderly, the American Occupational Therapy Association (AOTA) conducted a survey with over 200 occupational therapy (OT) providers in geriatric healthcare to examine their experiences related to this topic. The responding OTs worked in the following areas:
1. Inpatient Acute
2. Inpatient Rehab
3. Skilled Nursing Facilities
4. Home Health
5. Outpatient Rehabilitation
6. In-Home Practitioner
7. Community Practice
8. Academia/Research
9. Mental Health
10. Low Vision Rehabilitation
Major findings identified by the survey respondents are reported below. It is important to note that many providers advocate and recommend fall prevention interventions for their clients, but identify lack of coverage as a major barrier to implementation, and therefore, effectiveness. This survey identified a number of needs, including moving away from diagnosis-based reimbursement as well as increasing coverage for preventative services, community fall prevention programs, and safety devices. Critical barriers to fall prevention identified by respondents include lack of coverage of preventative services, reassessment/program adjustment, and safety devices.
MAJOR FINDINGS
Screening:
Most responding providers (89%) screen their patients over the age of 65 for falls, with 59% screening at every encounter and 34% screening if the patient mentions or has been injured as a result of a fall.
Most screened by eliciting a falls history (75%) or a mobility and gait assessment (55%), while over half used various other assessments (51%), including:
o Medication review for fall-risk meds; o Home Safety Assessment; o Observation of patient in functional task; o Functional reach test; o Cognitive Assessment; o Balance Screen; o Obtaining fall history from patient and family;
58
o Identification of other clinical factors that may increase an individual’s risk for falls (i.e. diagnoses, frailty, incontinence, poly-pharmacy);
o Timed Up and Go test; o Activities-Specific Balance Confidence or ABC Scale; o Tinetti Balance Test; and o Berg Balance Scale.
The majority of respondents identify patients who have had a previous history of falls (72%), and use of a mobility device (62%) as high risk factors for falls. Other factors identified include: o Being a senior client; o Having a fall with injury; o The presence of dizziness or vertigo; o Low vision; o Cognitive impairment; o Environmental hazards; o Fear of falling; o Multiple medical diagnosis; o Neurological impairment; o Report of difficulty in ADLs or IADLs; o Lives alone; o Poly-pharmacy; o Low blood pressure.
Although most respondents did not identify constraints that prevented a fall screening, 17% of responding OTs identified time constraints with the patient while 23% identified the lack of a brief, reliable tool to screen for falls as impeding the evaluation of every patient.
Many of the responding practitioners (91%) documented fall risks in the narrative of their notes, 22% used a flag system in the client’s record, while (18%) use ICD-9 codes such as V15.88. Other reporting methods included reports during weekly team meetings, inclusion in the falls assessment results, and in the OASIS C.
Intervention:
Interventions that had the most recommendations included balance/strengthening training, home safety assessment, alternative footwear, and implementation of environmental modifications. (Refer to Graph 1)
Other professions that were recommended or referred to patients in need of fall prevention intervention were: physical therapy, occupational therapy, optometry, and a community exercise program. (Refer to Graph 2)
Those OT practitioners that do not refer to other professions cite lack of ability to refer, pressure to only utilize resources within the facility, and lack of knowledge of community resources as reasons.
Nearly half (49%) of occupational therapy practitioners referred to community or non-medical fall prevention programs such as community senior center programs, YMCA programs, county senior health programs, or a community exercise program.
The majority (79%) of respondents offer printed educational material about fall prevention to their clients. Sources of this information include: o American Occupational Therapy Association (AOTA); o Centers for Disease Control and Prevention (CDC); o AGS/BGS Guidelines; o Matter of Balance; o Area Agency on Aging;
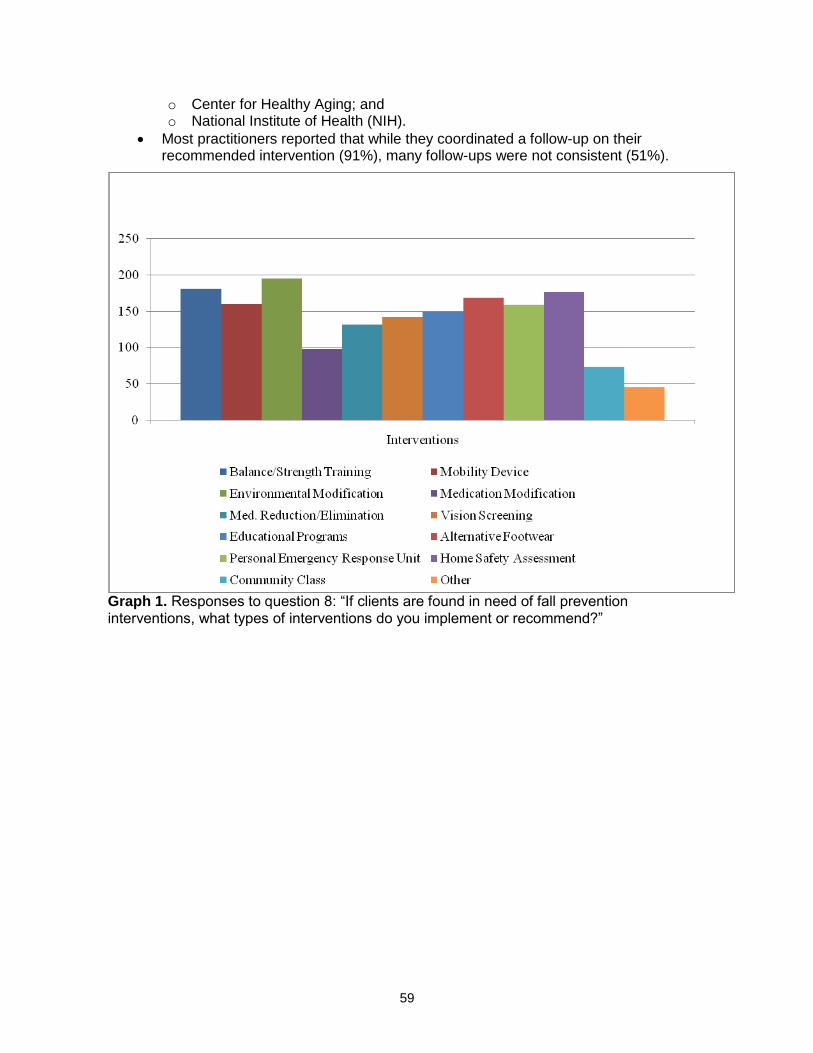
59
o Center for Healthy Aging; and o National Institute of Health (NIH).
Most practitioners reported that while they coordinated a follow-up on their recommended intervention (91%), many follow-ups were not consistent (51%).
Graph 1. Responses to question 8: “If clients are found in need of fall prevention interventions, what types of interventions do you implement or recommend?”
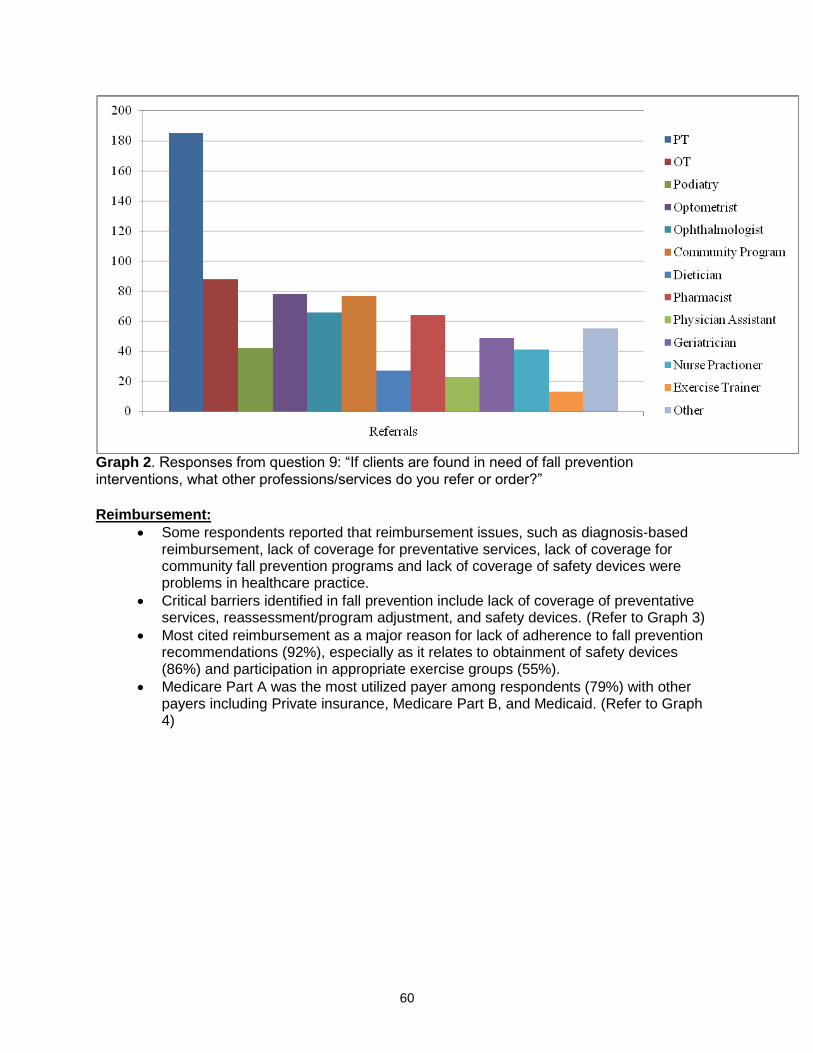
60
Graph 2. Responses from question 9: “If clients are found in need of fall prevention interventions, what other professions/services do you refer or order?”
Reimbursement:
Some respondents reported that reimbursement issues, such as diagnosis-based reimbursement, lack of coverage for preventative services, lack of coverage for community fall prevention programs and lack of coverage of safety devices were problems in healthcare practice.
Critical barriers identified in fall prevention include lack of coverage of preventative services, reassessment/program adjustment, and safety devices. (Refer to Graph 3)
Most cited reimbursement as a major reason for lack of adherence to fall prevention recommendations (92%), especially as it relates to obtainment of safety devices (86%) and participation in appropriate exercise groups (55%).
Medicare Part A was the most utilized payer among respondents (79%) with other payers including Private insurance, Medicare Part B, and Medicaid. (Refer to Graph 4)
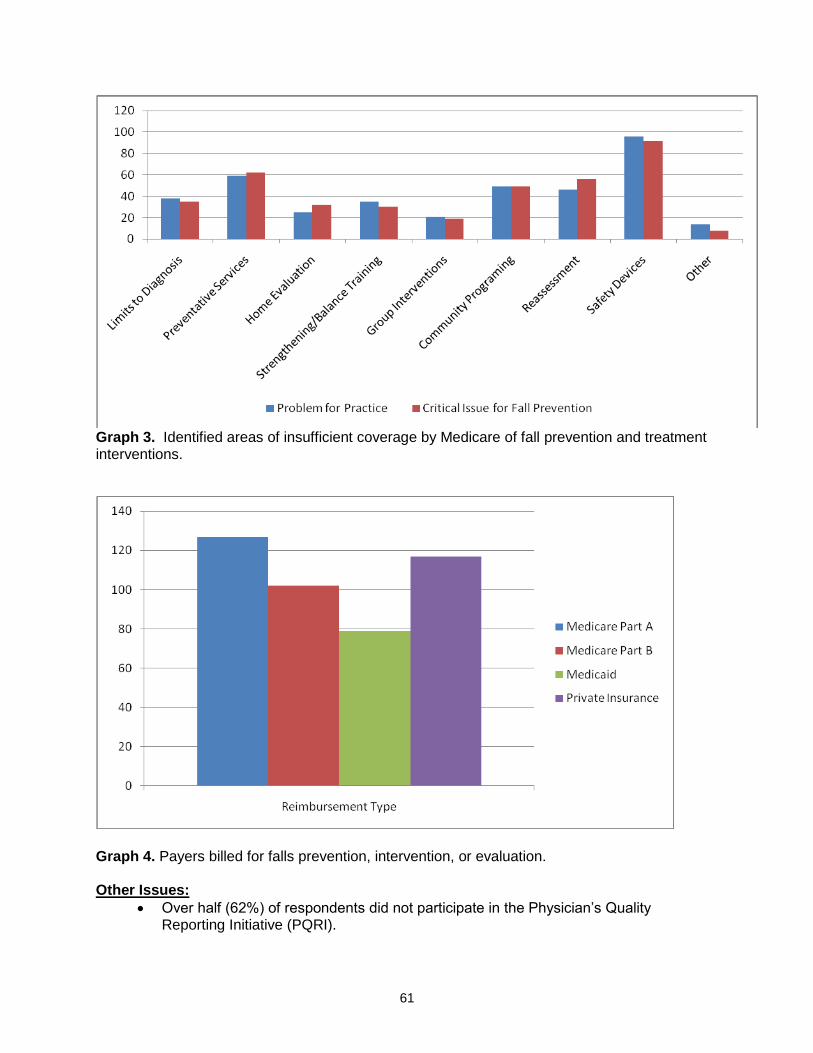
61
Graph 3. Identified areas of insufficient coverage by Medicare of fall prevention and treatment interventions.
Graph 4. Payers billed for falls prevention, intervention, or evaluation. Other Issues:
Over half (62%) of respondents did not participate in the Physician’s Quality Reporting Initiative (PQRI).
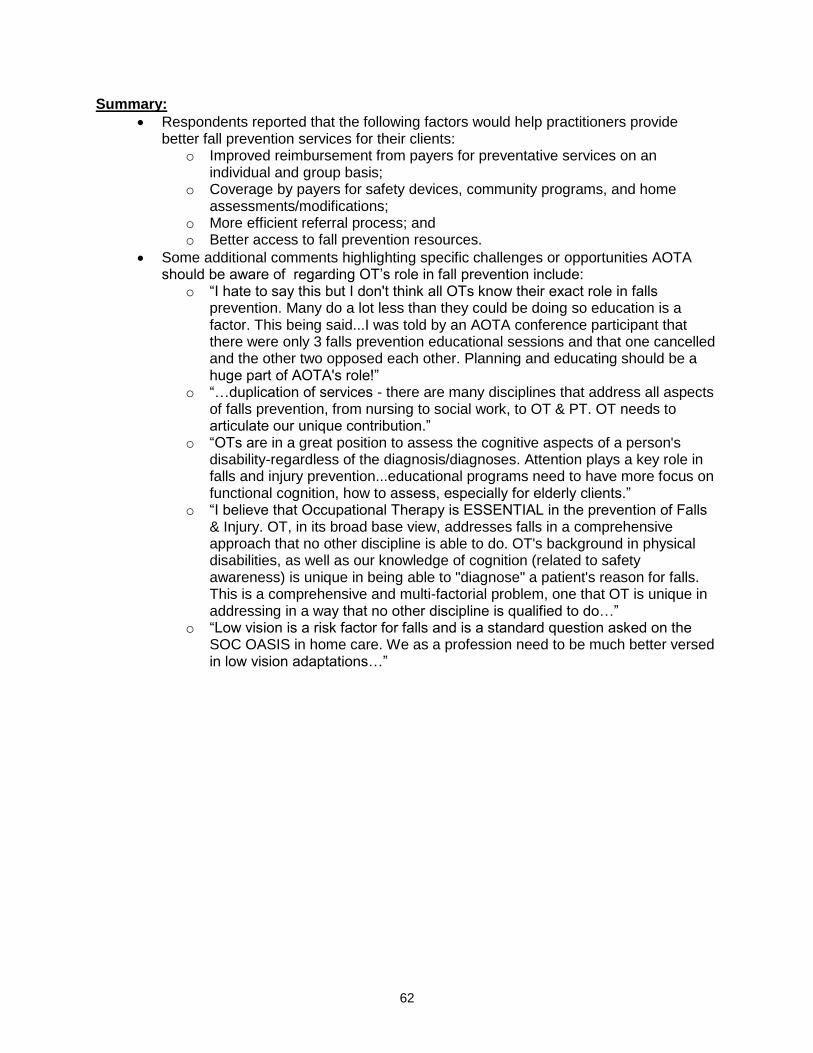
62
Summary:
Respondents reported that the following factors would help practitioners provide better fall prevention services for their clients:
o Improved reimbursement from payers for preventative services on an individual and group basis;
o Coverage by payers for safety devices, community programs, and home assessments/modifications;
o More efficient referral process; and o Better access to fall prevention resources.
Some additional comments highlighting specific challenges or opportunities AOTA should be aware of regarding OT’s role in fall prevention include:
o “I hate to say this but I don't think all OTs know their exact role in falls prevention. Many do a lot less than they could be doing so education is a factor. This being said...I was told by an AOTA conference participant that there were only 3 falls prevention educational sessions and that one cancelled and the other two opposed each other. Planning and educating should be a huge part of AOTA's role!”
o “…duplication of services - there are many disciplines that address all aspects of falls prevention, from nursing to social work, to OT & PT. OT needs to articulate our unique contribution.”
o “OTs are in a great position to assess the cognitive aspects of a person's disability-regardless of the diagnosis/diagnoses. Attention plays a key role in falls and injury prevention...educational programs need to have more focus on functional cognition, how to assess, especially for elderly clients.”
o “I believe that Occupational Therapy is ESSENTIAL in the prevention of Falls & Injury. OT, in its broad base view, addresses falls in a comprehensive approach that no other discipline is able to do. OT's background in physical disabilities, as well as our knowledge of cognition (related to safety awareness) is unique in being able to "diagnose" a patient's reason for falls. This is a comprehensive and multi-factorial problem, one that OT is unique in addressing in a way that no other discipline is qualified to do…”
o “Low vision is a risk factor for falls and is a standard question asked on the SOC OASIS in home care. We as a profession need to be much better versed in low vision adaptations…”