medicare advantage plans - wellcare
TRANSCRIPT

2017 SUMMARY OF BENEFITS
MEDICARE ADVANTAGE PLANS
Georgia Barrow, Bryan, Butts, Chatham, Chattahoochee, Cherokee, Clayton, Cobb, Columbia, De
Kalb, Douglas, Fayette, Forsyth, Fulton, Glynn, Gwinnett, Harris, Henry, Liberty, McIntosh, Meriwether, McDuffie, Muscogee, Newton, Paulding, Richmond, Rockdale, Spalding, Stewart,
Talbot, Walton
H1112
January 1, 2017 - December 31, 2017
WellCare Liberty (HMO SNP) Plan 033
H1112_GA034484_WCM_SOB_ENG CMS Accepted GA7033SOB76272E_0616 ©WellCare 2016 GA_06_16

Summary of Benefits January 1, 2017– December 31, 2017
This booklet gives you a brief overview of what we cover and what you can expect to pay. Itdoesn't list every service we cover or every limitation or exclusion. To get a complete list ofservices we cover, give us a call and ask for the "Evidence of Coverage." You can also find a copyon our website at www.wellcare.com/medicare. To join WellCare Liberty (HMO SNP), you must be entitled to Medicare Part A, be enrolledin Medicare Part B and the Georgia Department of Community Health, and live in our servicearea. Our service area includes the following counties in Georgia: Barrow, Bryan, Butts, Chatham,Chattahoochee, Cherokee, Clayton, Cobb, Columbia, DeKalb, Douglas, Fayette, Forsyth,Fulton, Glynn, Gwinnett, Harris, Henry, Liberty, McDuffie, McIntosh, Meriwether, Muscogee,Newton, Paulding, Richmond, Rockdale, Spalding, Stewart, Talbot, Walton Like all Medicare health plans, we cover everything that Original Medicare covers. And thenwe add some other benefits to help you stay your healthy best. For instance, when you haveurgent health care needs, you can talk to our nurses on call. Our Nurse Advice Line is open tomembers 24 hours every day at 1-800-581-9952. TTY users may call 1-877-247-6272. You can compare the coverage and costs in this booklet with the coverage and costs offered byOriginal Medicare by looking in your current "Medicare & You" handbook. You can view it online at http://www.medicare.gov or get a copy by calling 1-800-MEDICARE (1-800-633-4227),24 hours a day, 7 days a week. TTY users may call 1-877-486-2048. Contact information and hours
1 If you are not a member of this plan, call toll-free 1-866-527-0057 (TTY 1-877-247-6272).1 If you are a member of this plan, call toll-free 1-866-482-3361 (TTY 1-877-247-6272).1 Our website: www.wellcare.com/medicare1 From October 1 to February 14, we're here for you 7 days per week, 8 a.m. to 8 p.m.1 From February 15 to September 30, you can call us Monday–Friday, 8 a.m. to 8 p.m.
Which doctors, hospitals and pharmacies can I use?WellCare Liberty (HMO SNP) has a network of doctors, hospitals, pharmacies and otherproviders. You can save money by using providers in the plan's network. If you use providersthat are not in our network, the plan may not pay for these services. You can see our plan's provider directory and pharmacy directory and our complete plan formulary(list of Part D prescription drugs) at our website: www.wellcare.com/medicare. Or, call us atthe number above and we’ll send you a copy.
Summary of Benefits | 1

Summary of Benefits January 1, 2017– December 31, 2017
For each benefit listed below, you can see what our plan covers in addition to what GeorgiaDepartment of Community Health covers. Medicaid is a joint Federal and state governmentprogram that helps with medical costs for certain people with limited incomes and resources. Medicaid coverage varies depending on the state and the type of Medicaid you have. What youpay for covered services may depend on your level of Medicaid eligibility. Some people withMedicaid get help paying for their Medicare premiums and other costs. Other people may alsoget coverage for additional services and drugs that are covered under Medicaid but not byMedicare. No matter what your level of Medicaid eligibility is, WellCare Liberty (HMO SNP)will cover the benefits as described in the plan’s column. If you have questions about your Medicaideligibility and what benefits you are entitled to call: 1-866-482-3361. Below are the different levels of Medicaid eligibility. Full Benefit Dual Eligible (FBDE): Helps pay Medicare Part A and Part B premiums, andother cost-sharing (like deductibles, coinsurance, and co-payments). Eligible beneficiaries alsoreceive full Medicaid benefits. Qualified Medicare Beneficiary (QMB): Helps pay Medicare Part A and Part B premiums,and other cost-sharing (like deductibles, coinsurance, and co-payments). (Some people withQMB are also eligible for full Medicaid benefits (QMB+).) Specified Low-Income Medicare Beneficiary (SLMB): Helps pay Part B premiums. (Somepeople with SLMB are also eligible for full Medicaid benefits (SLMB+).) Qualifying Individual (QI): Helps pay Part B premiums. Qualified Disabled & Working Individuals (QDWI): Helps pay Part A premiums. This document is available in other formats such as Braille and large print. This document may be available in a non-English language. For additional information, call usat 1-877-374-4056 , TTY 1-877-247-6272
Summary of Benefits | 2

Summary of Benefits January 1, 2017– December 31, 2017
NOTE: 1 SERVICES UNDER CATEGORIES WITH A 1 MAY REQUIRE PRIOR
AUTHORIZATION. 1 SERVICES UNDER CATEGORIES WITH A 2 MAY REQUIRE A REFERRAL
FROM YOUR DOCTOR.
Monthly Plan Premium
Deductible
Maximum Out-of-Pocket Responsibility (does notinclude prescription drugs)
No Deductible
Inpatient hospital coverage1,2
Doctor Visits1,2
Georgia Department ofCommunity HealthWellCare Liberty (HMO SNP)
Premiums and Benefits
You pay $0.00 You must continue to payyour Medicare Part Bpremium.
$6,700 annually The most you pay for co-pays,coinsurance and other costs for Medicare-covered A and B services for the year. If youreach this limit on out-of-pocket costs, you keepgetting covered hospital andmedical services while we paythe full cost for the rest of the year
$0 co-pay up to 90 days peradmission
For dual-eligible members,Medicaid pays for this serviceif it is not covered byMedicare or when the Medicare benefit is exhausted. $12.50 per admission formembers over age 21.
Summary of Benefits | 3

Georgia Department ofCommunity HealthWellCare Liberty (HMO SNP)
1 Primary
1 Specialists
Preventive care
You pay $0 co-pay per visit
You pay $0 co-pay per visit
You pay nothing for thefollowing
1 Abdominal aortic aneurysm screening
1 Alcohol misuse counseling
1 Bone mass measurement 1 Breast cancer screening
(mammogram)
For dual-eligible members,Medicaid pays for this serviceif it is not covered byMedicare or when the Medicare benefit is exhausted. Cost-based: Cost Based Co-Payment $10.00 or less $0.50 $10.01-$25.00 $1.00 $25.01-$50.00 $2.00 $50.01 or more $3.00 FQHC or RHC $2.00
For dual-eligible members,Medicaid pays for this serviceif it is not covered byMedicare or when the Medicare benefit is exhausted. Cost-based: Cost Based Co-Payment $10.00 or less $0.50 $10.01-$25.00 $1.00 $25.01-$50.00 $2.00 $50.01 or more $3.00 FQHC or RHC $2.00
For dual-eligible members,Medicaid pays for this serviceif it is not covered byMedicare or when the Medicare benefit is exhausted Immunizations (Flu vaccine, Hepatitis Bvaccine - for people with
Summary of Benefits | 4

Georgia Department ofCommunity HealthWellCare Liberty (HMO SNP)
1 Cardiovascular disease (behavioral therapy)
1 Cardiovascular screenings
1 Cervical and vaginalcancer screening
1 Colorectal cancer screenings(Colonoscopy, Fecaloccult blood test,Flexible sigmoidoscopy)
1 Depression screening1 Diabetes screenings1 HIV screening1 Medical nutrition
therapy services1 Obesity screening and
counseling1 Prostate cancer
screenings (PSA)1 Sexually transmitted
infections screening andcounseling
1 Tobacco use cessation counseling (counselingfor people with no signof tobacco-related disease)
1 Vaccines, including Flushots, Hepatitis Bshots, Pneumococcalshots
1 "Welcome to Medicare" preventive visit(one-time)
1 Yearly "Wellness" visit Any additional preventiveservices approved by Medicareduring the contract year willbe covered
Medicare who are at risk,Pneumonia vaccine) Mammograms (AnnualScreening) (for women with Medicareage 40 and older) Pap Smears and PelvicExams (for women with Medicare) Prostate Cancer ScreeningExams (for men with Medicare age50 and older) Welcome to Medicare; andAnnual Wellness Visit – Not Covered Health/Wellness Education • Written health education materials, includingnewsletters • Nutritional Training• Additional SmokingCessation • Other Wellness Benefits Bone Mass Measurement (for people with Medicarewho are at risk)$3.00 co-pay if outpatientbased Colorectal Screening Exams (for people with Medicare age50 and older)$0 co-pay forMedicaid-covered services.
Summary of Benefits | 5

Georgia Department ofCommunity HealthWellCare Liberty (HMO SNP)
Emergency care
Urgently needed services
Diagnostic services/labs/imaging1,2
1 Diagnostic radiologyservice (e.g., MRI)
You pay $0 co-pay per visit If you are admitted to thehospital within 24 hours, youdo not have to pay your shareof the cost for emergency care
You pay $0 co-pay per visit If you are admitted to thehospital within 24 hours, youdo not have to pay your shareof the cost for urgently neededservices
If part of an E&M visit,cost-based: Cost Based Co-Payment$10.00 or less $0.50 $10.01-$25.00 $1.00 $25.01-$50.00 $2.00 $50.01 or more $3.00
For dual-eligible members,Medicaid pays for this serviceif it is not covered byMedicare or when the Medicare benefit is exhausted. $0 co-pay forMedicaid-covered services. *Not covered outside the U.S. except under limitedcircumstances. Contact the plan for more details.
For dual-eligible members,Medicaid pays for this serviceif it is not covered byMedicare or when the Medicare benefit is exhausted.
You pay $0 co-pay whenperformed at a specialist's For dual-eligible members,office or free standing facility Medicaid pays for this serviceand $0 co-pay when if it is not covered byperformed in an outpatient Medicare or when thesetting Medicare benefit is exhausted.
$3.00 co-pay if outpatientbased
Summary of Benefits | 6

Georgia Department ofWellCare Liberty (HMO SNP)
You pay $0 co-pay For dual-eligible members,Medicaid pays for this service
Community Health *Not covered: portable X-rayservices; services provided infacilities not meeting thedefinition of an independentlaboratory or X-ray facility;services or procedures referredto another testing facility;services furnished by a Stateor public laboratory; servicesor procedures performed by afacility not certified toperform them.
1 Lab services
if it is not covered byMedicare or when the Medicare benefit is exhausted. $3.00 co-pay if outpatientbased *Not covered: portable X-rayservices; services provided infacilities not meeting thedefinition of an independentlaboratory or X-ray facility;services or procedures referredto another testing facility;services furnished by a Stateor public laboratory; servicesor procedures performed by afacility not certified toperform them.
You pay $0 co-pay for basic For dual-eligible members,1 Diagnostic tests and tests and procedures and $0 Medicaid pays for this serviceprocedures co-pay for advanced tests and if it is not covered by
procedures such as Medicare or when the Echocardiogram Medicare benefit is exhausted.
Summary of Benefits | 7

Georgia Department ofWellCare Liberty (HMO SNP) Community Health $3.00 co-pay if outpatientbased *Not covered: portable X-rayservices; services provided infacilities not meeting thedefinition of an independentlaboratory or X-ray facility;services or procedures referredto another testing facility;services furnished by a Stateor public laboratory; servicesor procedures performed by afacility not certified toperform them.
1 Outpatient x-rays
if it is not covered byMedicare or when the Medicare benefit is exhausted. $3.00 co-pay if outpatientbased *Not covered: portable X-rayservices; services provided infacilities not meeting thedefinition of an independentlaboratory or X-ray facility;services or procedures referredto another testing facility;services furnished by a Stateor public laboratory; servicesor procedures performed by afacility not certified toperform them.
You pay $0 co-pay when For dual-eligible members,1 Therapeutic radiology performed at a specialist's Medicaid pays for this serviceservices office or free standing facility if it is not covered by
You pay $0 co-pay For dual-eligible members,Medicaid pays for this service
Summary of Benefits | 8
Georgia Department ofCommunity HealthWellCare Liberty (HMO SNP)
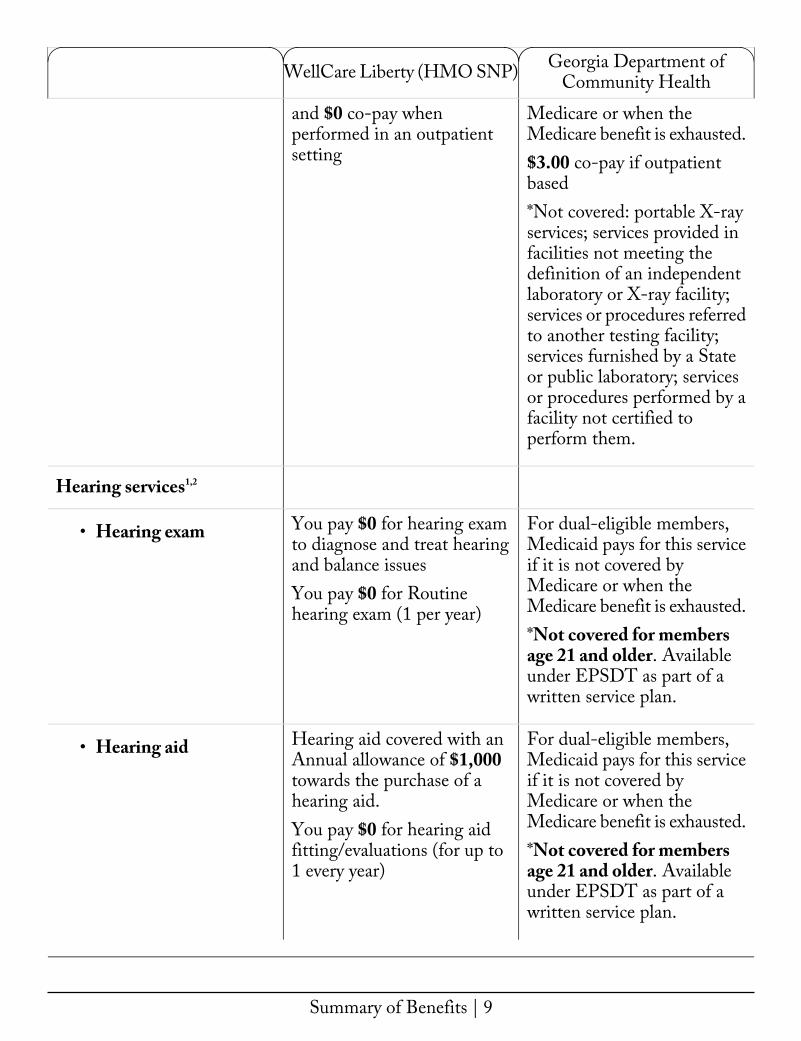
Hearing services1,2
1 Hearing exam
1 Hearing aid
and $0 co-pay whenperformed in an outpatientsetting
You pay $0 for hearing examto diagnose and treat hearingand balance issues You pay $0 for Routine hearing exam (1 per year)
Hearing aid covered with anAnnual allowance of $1,000towards the purchase of ahearing aid. You pay $0 for hearing aidfitting/evaluations (for up to1 every year)
Medicare or when the Medicare benefit is exhausted. $3.00 co-pay if outpatientbased *Not covered: portable X-rayservices; services provided infacilities not meeting thedefinition of an independentlaboratory or X-ray facility;services or procedures referredto another testing facility;services furnished by a Stateor public laboratory; servicesor procedures performed by afacility not certified toperform them.
For dual-eligible members,Medicaid pays for this serviceif it is not covered byMedicare or when the Medicare benefit is exhausted. *Not covered for members age 21 and older. Available under EPSDT as part of awritten service plan.
For dual-eligible members,Medicaid pays for this serviceif it is not covered byMedicare or when the Medicare benefit is exhausted. *Not covered for members age 21 and older. Available under EPSDT as part of awritten service plan.
Summary of Benefits | 9

Georgia Department ofCommunity HealthWellCare Liberty (HMO SNP)
Dental services1,2
Vision services1,2
1 Vision exams
You pay nothing for the The following Dental Servicesfollowing preventive dental are a benefit of Georgiaservices: Medicaid:
*Preventive, diagnostic and1 Cleaning (for up to 1 treatment services provided toevery six months) Members under age 21.1 Dental x-ray(s) (for up Emergency Services only forto 1 every 12 to 36 Members age 21 and older.months)1 Oral exam (for up to 1 Members under 21 years of
every six months) age:1 Fluoride treatment (for $0 co-pay per visit — Services
up to 1 every year) include exams, cleanings,X-rays, fillings, dentures, oralOur plan pays up to $1000 surgery and orthodonticevery year for most dental treatment.services. Additional
comprehensive dental services Members 21 years of age andyou will pay nothing for older: (emergency only):include one of the following: $0 co-payone Endodontic procedure peryear,one Periodonticsprocedure every 6 to 36months or one Extraction peryear. Also included is oneProsthodontic procedure every12 to 60 months, one OralMaxillofacial procedure every60 months or other services every 6 to 24 months.
You pay $0 for The following Vision ServicesMedicare-covered diabetes are a benefit of Georgiaretinopathy screening and you Medicaid: pay $0 for all other Medically necessary diagnosticMedicare-covered eye exams services may be covered.
Services may only be coveredif performed for medicalreasons and not for refractive
Summary of Benefits | 10

Georgia Department ofCommunity HealthWellCare Liberty (HMO SNP)
You pay $0 co-pay forRoutine vision exam (1 peryear) You pay nothing forMedicare-covered Glaucoma screenings.
Our plan pays up to $200 every year for up to 1 pair ofContact lenses, Eyeglasses(frames and lenses), EyeglassFrames or Eyeglass lenses.
purposes for members 21 yearsof age or older. Cost-based: Cost Based Co-Payment $10.00 or less $0.50 $10.01-$25.00 $1.00 $25.01-$50.00 $2.00 $50.01 or more $3.00 *Not covered for members age21 and older: routine refractive services and opticaldevices.
The following Vision Servicesare a benefit of GeorgiaMedicaid: Medically necessary diagnosticservices may be covered.
1 Eyewear
You pay nothing for eyeglasses Services may only be coveredor contact lenses after cataract if performed for medicalsurgery. reasons and not for refractive
purposes for members 21 yearsof age or older. Cost-based: Cost Based Co-Payment $10.00 or less $0.50 $10.01-$25.00 $1.00 $25.01-$50.00 $2.00
Summary of Benefits | 11

Georgia Department ofCommunity HealthWellCare Liberty (HMO SNP)
Mental health services1,2
$0 co-pay up to 90 days per1 Inpatient visit admission
You pay $0 co-pay per1 Outpatient group or outpatient therapy visitindividual therapy visit
$50.01 or more $3.00 *Not covered for members age21 and older: routine refractive services and opticaldevices.
For dual-eligible members,Medicaid pays for this serviceif it is not covered byMedicare or when the Medicare benefit is exhausted. $12.50 per admission formembers over age 21. *(This is dependent upon themember’s demographiclocation).
For dual-eligible members,Medicaid pays for this serviceif it is not covered byMedicare or when the Medicare benefit is exhausted. $3.00 co-pay is required on allnon-emergency outpatienthospital visits. *Community Mental HealthRehabilitation services are only available as part of awritten service plan. Pregnant women, membersunder 21 years of age, nursingfacility members, communitycare participants, QualifiedMedicare
Summary of Benefits | 12

Georgia Department ofCommunity HealthWellCare Liberty (HMO SNP)
Skilled Nursing Facility1,2
Rehabilitation services1,2
1 Cardiac (heart) rehabservices
1 Occupational therapyvisit
You pay nothing per day fordays 1 through 20 $0 co-pay per day for days 21through 100 Our plan covers up to 100days in a SNF
You pay $0 co-pay
You pay $0 co-pay
Beneficiary (QMB), andhospice care participants arenot subject to the co-payment.When the outpatientcost-based settlements are made for hospital services, theco-payment plus Medicaidpayment will be compared tothe allowable cost to determine the amount of final settlement.
For dual-eligible members,Medicaid pays for this serviceif it is not covered byMedicare or when the Medicare benefit is exhausted.
Covered if medically necessaryfor dual-eligible members,Medicaid pays for this serviceif it is not covered byMedicare or when the Medicare benefit is exhausted.
For dual-eligible members,Medicaid pays for this serviceif it is not covered byMedicare or when the Medicare benefit is exhausted. $3.00 co-pay per visit *Not covered for Members age21 and older. Available under EPSDT as part of a writtenservice plan.
Summary of Benefits | 13

Georgia Department ofCommunity HealthWellCare Liberty (HMO SNP)
You pay $0 co-pay1 Physical therapy and
speech and languagetherapy visit
You pay $0 co-payAmbulance1
Transportation You pay nothing for 36One-way trips every year.These are shared trips to planapproved locations.
For dual-eligible members,Medicaid pays for this serviceif it is not covered byMedicare or when the Medicare benefit is exhausted. $3.00 co-pay per visit *Not covered for Members age21 and older. Available under EPSDT as part of a writtenservice plan.
For dual-eligible members,Medicaid pays for this serviceif it is not covered byMedicare or when the Medicare benefit is exhausted. $0 co-pay per visit ifemergent $3.00 co-pay per visit will beimposed if the condition is notan emergent medicalcondition.
The following TransportationServices are a benefit of Georgia Medicaid: Non-emergencytransportation – NET services are defined as medicallynecessary transportation foranymember (and escort, ifrequired,) who has no othermeans of transportationavailable to any Medicaidreimbursable service for the purpose of receivingtreatment, medical evaluation,
Summary of Benefits | 14

Georgia Department ofCommunity HealthWellCare Liberty (HMO SNP)
Foot care (podiatryservices)1,2
You pay $0 co-pay1 Foot exams and
treatment
Not Covered1 Routine foot care
obtaining prescription drugsor medical equipment. For dual-eligible members,Medicaid pays for this serviceif it is not covered byMedicare or when the Medicare benefit is exhausted.
For dual-eligible members,Medicaid pays for this serviceif it is not covered byMedicare or when the Medicare benefit is exhausted. Cost-based: Cost Based Co-Payment $10.00 or less $0.50 $10.01-$25.00 $1.00 $25.01-$50.00 $2.00 $50.01 or more $3.00 *Not covered: services for flatfoot; subluxation; routinefoot care, supportive devices;vitamin B-12 injections.
For dual-eligible members,Medicaid pays for this serviceif it is not covered byMedicare or when the Medicare benefit is exhausted. Cost-based: Cost Based Co-Payment $10.00 or less $0.50 $10.01-$25.00 $1.00
Summary of Benefits | 15

Medical equipment/supplies1
Georgia Department ofWellCare Liberty (HMO SNP) Community Health $25.01-$50.00 $2.00 $50.01 or more $3.00 *Not covered: services for flatfoot; subluxation; routinefoot care, supportive devices;vitamin B-12 injections.
1 Diabetes supplies
if it is not covered byMedicare or when the Medicare benefit is exhausted. $1.00 or $3.00 co-pay (servicebased)
You pay nothing For dual-eligible members,1 Diabetic Therapeutic Medicaid pays for this serviceShoes and Inserts if it is not covered by
For dual-eligible members,Medicaid pays for this service
You pay nothing1 Durable medical
equipment (e.g.,wheelchairs, oxygen) if it is not covered by
Medicare or when the Medicare benefit is exhausted. $1.00 or $3.00 co-pay (servicebased)
You pay $0 co-pay For dual-eligible members,Medicaid pays for this service1 Prosthetics (e.g.,
braces, artificial limbs) if it is not covered byMedicare or when the Medicare benefit is exhausted. $1.00 or $3.00 co-pay (servicebased)
For dual-eligible members,Medicaid pays for this service
You pay nothing
Summary of Benefits | 16

Georgia Department ofCommunity HealthWellCare Liberty (HMO SNP)
Wellness Programs1
1 Fitness
1 Additional Routine Annual Physical
1 Nurse Advice Line – 24 hours
Medicare Part B Drugs1
1 Chemotherapy drugs
You pay nothing
You pay nothing
You pay nothing
You pay $0 for Part B drugsobtained in a pharmacy and$0 for all other medical settings
Medicare or when the Medicare benefit is exhausted. $1.00 or $3.00 co-pay (servicebased)
For dual-eligible members,Medicaid pays for this serviceif it is not covered byMedicare or when the Medicare benefit is exhausted. $0 co-pay forMedicaid-covered services.
For dual-eligible members,Medicaid pays for this serviceif it is not covered byMedicare or when the Medicare benefit is exhausted. $0 co-pay forMedicaid-covered services.
For dual-eligible members,Medicaid pays for this serviceif it is not covered byMedicare or when the Medicare benefit is exhausted. $0 co-pay forMedicaid-covered services.
Not Applicable
Summary of Benefits | 17

Georgia Department ofWellCare Liberty (HMO SNP) Community Health You pay $0 for Part B drugs Not Applicable
1 Part B drugs obtained in a pharmacy and$0 for all other medical settings.
Summary of Benefits | 18

WellCare Liberty (HMO SNP)
Part D Information Part D Cost Shares
Initial Coverage You pay the following until your total yearly drug costs reach$3,700. Total yearly drug costs are the total drug costs paid byboth you and our Part D plan. You may get your drugs atnetwork retail pharmacies and mail service pharmacies.
Retail 30-Day Supply
Generics: You pay $0 or $1.20Tier 1: Preferred Generic You pay $0 or $3.30Drugs
Generics: You pay $0 or $1.20 or $3.30Tier 2: Generic Drugs Brands: You pay $0 or $3.70 or $8.25Tier 3: Preferred Brand
DrugsTier 4: Non-Preferred Drugs
Generics: You pay $0 or $1.20Tier 5: Specialty Drugs Not Covered or $3.30
Brands: You pay $0 or $3.70 or $8.25
Preferred Mail Order 90-Day Supply
Initial Coverage (After youpay your deductible, ifapplicable)
If you reside in a long term care (LTC) facility, you pay the same as a retail pharmacy. Whenyou move from one phase of the Part D benefit to another, your cost-sharing may changeas well. For more information on the additional pharmacy specific cost-sharing and thephase of the benefit, please call us or access our Evidence of Coverage online.
Coverage Gap Most Medicare drug plans have a coverage gap (also called the"donut hole"). This means that there's a temporary change inwhat you will pay for your drugs. The coverage gap begins afterthe total yearly drug cost (including what our plan has paidand what you have paid) reaches $3,700. This stage does not apply to you
Catastrophic Coverage After your yearly out-of-pocket drug costs (not including whatthe plan has paid, but including drugs you purchased through
Summary of Benefits | 19

WellCare Liberty (HMO SNP)
your retail pharmacy and through Mail Service order) reach$4,950, you pay nothing.
Georgia Department ofWellCare Liberty (HMO SNP) Community Health Benefits Continued
Prescription Drug
if it is not covered byMedicare or when the Medicare benefit is exhausted. Cost-based: Drug Cost Co-Payment$10.00 or less $0.50 $10.01-$25.00 $1.00 $25.01-$50.00 $2.00 $50.01 or more $3.00 *Not covered: certain outpatient drugs pursuant toSection 1927(d) of the SocialSecurity Act. Additionally,certain over the counter (OTC) drugs must beincluded, pursuant to theGeorgia State Policies andProcedures Manual.
You pay $0 co-pay For dual-eligible members,1 Ambulatory surgical Medicaid pays for this servicecenter if it is not covered by
Medicare or when the Medicare benefit is exhausted. $3.00 Co-Pay per visit w/regular exclusions
For dual-eligible members,Please see the Part D Medicaid pays for this serviceinformation above
Outpatient Surgery1,2
Summary of Benefits | 20

Chiropractic care1,2
Georgia Department ofWellCare Liberty (HMO SNP) Community Health For dual-eligible members,
1 Outpatient hospital Medicaid pays for this serviceif it is not covered byMedicare or when the Medicare benefit is exhausted. $3.00 Co-Pay per visit w/regular exclusions
Renal dialysis
if it is not covered byMedicare or when the Medicare benefit is exhausted.
Hospice You pay nothing for hospice For dual-eligible members,care from a Medicare-certified Medicaid pays for this service
You pay nothing
Not CoveredNot CoveredAcupuncture
Not CoveredYou pay $0 co-pay1 Medical chiropractic
services
Not CoveredNot Covered1 Routine chiropractic
services
Our plan will pay up to $40Over-the-Counter items Not Covered every month for the purchaseof covered over-the-counter items. Please visit our website to see our list of covered over-the-counter items.
For dual-eligible members,Medicaid pays for this service
You pay nothing.Home health
if it is not covered byMedicare or when the Medicare benefit is exhausted.
For dual-eligible members,Medicaid pays for this service
You pay nothing.
Summary of Benefits | 21

Georgia Department ofWellCare Liberty (HMO SNP) Community Health if it is not covered byMedicare or when the Medicare benefit is exhausted.
Federal qualified healthcenter services
if it is not covered byMedicare or when the Medicare benefit is exhausted. *Ambulatory services such asdental services are subject toany limitations applicable tothe specific ambulatoryservice. $2.00 co-pay
hospice. You may have to paypart of the cost of drugs andrespite care. Hospice iscovered outside of our plan.Please contact us for more details.
The following FamilyYou pay nothing for MedicareFamily planning Planning Services are a benefitcovered services of Georgia Medicaid:Medicaid covers some Familyplanning services and supplies. For dual-eligible memberscoverage for services andsupplies for the purpose offamily planning are coveredregardless of sex or maritalstatus. $0 co-pay forMedicaid-covered services.
For dual-eligible members,You pay nothing for MedicareMedicaid pays for this servicecovered services
Private duty nursing Not Covered For dual-eligible members,Medicaid pays for this service
Summary of Benefits | 22

if it is not covered byMedicare or when the Medicare benefit is exhausted. $0 for Medicaid-covered services.
For dual-eligible members,Medicaid pays for this serviceif it is not covered byMedicare or when the Medicare benefit is exhausted.
Georgia Department ofCommunity HealthWellCare Liberty (HMO SNP)
$2.00 co-pay
For dual-eligible members,Medicaid pays for this serviceif it is not covered byMedicare or when the Medicare benefit is exhausted.
For dual-eligible members,Medicaid pays for this serviceif it is not covered byMedicare or when the Medicare benefit is exhausted. * Covered for pregnantwomen under age 21 andother pregnant women at riskfor adverse outcomes; infantsand toddlers with established risk for developmental delay.
For dual-eligible members,Medicaid pays for this serviceif it is not covered byMedicare or when the Medicare benefit is exhausted. *Not covered for Members age21 and older: heart, lung andheart/lung transplants.
Rural health clinic services You pay nothing for Medicarecovered services
Swing bed services You pay nothing for Medicarecovered services
Targeted case management Offered by the plan if youmeet qualifications
Transplants You pay nothing for Medicarecovered services
Summary of Benefits | 23

Y0070_NA030775_ WCM_INS_MLT CMS Accepted 08052015 NA6MLTINS69044M 69044 ©WellCare 2015 NA 07 15 CCP
Multi-Language Insert
Multi-language Interpreter Services
English: We have free interpreter services to answer any questions you may have about our health or drug plan. To get an interpreter, just call us at 1877-374-4056. Someone who speaks English/Language can help you. This is a free service.
Spanish: Tenemos servicios de interprete sin costo alguno para responder cualquier pregunta que pueda tener sobre nuestro plan de salud o medicamentos. Para hablar con un interprete, por favor llame al 1-877-3744056. Alguien que hable espanol le podra ayudar. Este es un servicio gratuito.
Chinese Mandarin: iX:{l'l1~{~%'ffl:B"Jl:JlEM~~, :m@1~~~~::*:rfmm!.XBJ4'0{:lf:~B"JH:{PJ~
rJ=iJ o Po*1~~~rttl~1~ij~~, iF!JfJ:EE! 1-877-374-40560 iX:{[']Er99=rJtI{'f AI7HlUk~:m@1~ o E~~:rJf!%'ffl:ij~~ o
Chinese Cantonese:您對我們的健康'或藥物保險可能存有疑問,為此我們提供免費的翻譯
服務。 如需翻譯服務,請致電1-877-374-4056。我們講中文的人員將樂意為您提供幫助。
這是一項免費服務。
Tagalog: Mayroon kaming libreng serbisyo sa pagsasaling-wika upang masagot ang anumang mga katanungan ninyo hinggil sa aming planong pangkalusugan o panggamot. Upang makakuha ng tagasaling-wika, tawagan lamang kami sa 1-877-374-4056. Maaari kayong tulungan ng isang nakakapagsalita ng Tagalog. Ito ay libreng serbisyo.
French: Nous proposons des services gratuits d'interpretation pour repondre a toutes VOS questions relatives a notre regime de sante OU d'assurancemedicaments. Pour acceder au service d'interpretation, ii vous suffit de nous appeler au 1-877-374-4056. Un interlocuteur parlant Franc;ais pourra vous aider. Ce service est gratuit.
Vietnamese: Chung toi c6 dich Vl,J thong dich mi@n phf de tra loi cac cau h6i ve chu'dng sue kh6e va chu'dng tr1nh thuoc men. Neu quf vi can thong dich vien xin gc;>i 1-877-374-4056 se c6 nhan vien n6i tieng Vi~t giup do quf vi. Day la dich v1,J mi@n phf .
German: Unser kostenloser Dolmetscherservice beantwortet Ihren Fragen zu unserem Gesundheits- und Arzneimittelplan. Unsere Dolmetscher

Y0070_NA030775_ WCM_INS_MLT CMS Accepted 08052015 NA6MLTINS69044M ©WellCare 2015 NA 07 15 CCP
erreichen Sie unter 1-877-374-4056. Man wird Ihnen dort auf Deutsch weiterhelfen. Dieser Service ist kostenlos.
Korean: 1%A} ~ .£1 li _!:! ~ EE~ Q.{% _!:! ~ ~l -{!-~ ~~~l 1J-i>~ E-~ :JL~} -1¥-li ~~
Ai Bl A~ ~11 i?--O} jl ~J~ 11 i:::}. ~~ Ai Bl A~ 0 1-§--0}?11?! ~~ 1-877-374-4056\l}_Q_s_
~.£1-5~ 2f'-{:J/,l_2_. ~~~ ~ -0}~ 18-1%A}7}_s=__<;l}E__~ ~~11i:::}. 0 1Ai Bl A~ -1f-ii_s_
-8:- 08~114.
Russian: Ecn111 y sac B03Hll1KHYT BOnpOCbl OTHOCll1TenbHO CTpaxosoro 111n111 Me,[l,1t1KaMeHTHOro nnaHa, Bbl MO}l{eTe BOCnOnb30BaTbC51 HaWll1Mll1 6ecnnaTHblMll1 ycnyraMll1 nepeBO,lJ,4111KOB. LIT06bl BOCnOnb30BaTbC51 ycnyraMll1 nepeBO,lJ,4111Ka, n03BOHll1Te HaM no TenecpoHy 1-877-374-4056. BaM OKa}l{eT nOMOW,b c0Tpy,[1,H1t1K, KOTOpb1ill rosop111T no-pyccK111. ,[J,aHHafl ycnyra 6ecnnaTHafl.
Arabic:
. \.li.l\ ~ ~ ~3 ,::.'-j\ J _J h • _J l ~Li • ~ ..:L-:-: ~\ t.? l r..JC · ~b)IJ •• ' tib..J\ ~ • t.?J~ -~'I ~~ .-:_I\ wl..i~ f' .::.ij \jj\' L.i ~f'~ . 1-877-374-4056 .)c ~ JL...::i:i'll (.$y.;i ~ ~'!.?_)_;.~fa .)c Jy..=JJ ~yJI o~~~ ~~ o~ .~.::.c.~.
Hindi:~~~<::!" <:IT~~ 'll~'51Ci11~~"tr3ff% ~ 3-11 >l"~Ci""I" ~~~~~~
tfR1~~~~3q(>16ltr6. "Q'Cf)~~m"C(l~~~,~~ 1-877-374-4056
~tnTa=rct1t.~c'llRa~~~6~~~~6.~"QCt1~~6.:>
.
Italian: Edisponibile un servizio di interpretariato gratuito per rispondere a eventuali domande sul nostro piano sanitario e farmaceutico. Perun interprete, contattare ii numero 1-877-374-4056. Un nostro incaricato che parla Italianovi fornira l'assistenza necessaria. Eun servizio gratuito.
Portugues: Dispomos de servic;os de interpretac;ao gratuitos para responder a qualquer questao que tenha acerca do nosso piano de saude ou de medicac;ao. Para obter um interprete, contacte-nos atraves do numero 1877-374-4056. Ira encontrar alguem que fale o idioma Portugues para o ajudar. Este servic;o e gratuito.
French Creole: Nou genyen sevis entepret gratis pou reponn tout kesyon OU ta genyen konsenan plan medikal oswa dwog nou an. Pou jwenn yon entepret, jis rele nou nan 1-877-374-4056. Yon moun ki pale Kreyol kapab ede w. Sa a se yon sevis ki gratis.
Polish: Umozliwiamy bezp~atne skorzystanie z us~ug Uumacza ustnego, kt6ry pomoze w uzyskaniu odpowiedzi na temat planu zdrowotnego lub dawkowania lek6w. Aby skorzystac z pomocy Uumacza znajq_cego j~zyk
69044

Y0070_NA030775_ WCM_INS_MLT CMS Accepted 08052015 NA6MLTINS69044M ©WellCare 2015 NA 07 15 CCP
polski, nalezy zadzwonic pod numer 1-877-374-4056. Ta us~uga jest bezp~atna.
Japanese: ':131ltt0fmff}t fmff}t{:lf:~~ c~db ~)]~7°7 / ~;_: ~T ~ C::'1'{Fp~~;: Ji~.Z T ~ t~60 ~;_:
, ~t40w~,R-it~E7-,7J"&) 0 i-tc::'-2''1;,i-fo w~Rtc::'JtJii'd::?J:-~~::t:t, 1-877-374
4056~:: ;B~gll < ft_' 2 v'o B,:;tgi% t gllT A~ iJ"R~v' t~ Li To ~ tLli ~;,f']j.C)-1)-~ C' A
-C'To
69044

WellCare (HMO SNP) is a Medicare Advantage organization with a Medicare contract and acontract with the Georgia Medicaid program. Enrollment in WellCare (HMO SNP) dependson contract renewal. We Cover Part D drugs. In addition, we cover Part B drugs such aschemotherapy and some drugs administered by your provider. You must continue to pay yourMedicare Part B premium. If you meet certain eligibility requirements for both Medicare andMedicaid, your Part B premiums may be covered in full. WellCare uses a formulary. Theformulary, pharmacy network, and/or provider network may change at any time. You will receivenotice when necessary. This information is not a complete description of benefits. Contact theplan for more information. Limitations, co-payments and restrictions may apply. Benefits,premiums and/or co- payments/coinsurance may change on January 1 of each year. You havethe choice to sign up for automated mail service delivery. You can get prescription drugs shippedto your home through our network mail service delivery program. You should expect to receiveyour prescription drugs within 7–10 business days from the time that the mail service pharmacyreceives the order. If you do not receive your prescription drugs within this time, please contactus at 1-866-892-9006 (TTY 1-866-507-6135), 24 hours a day, seven days a week, or visitwww.wellcare.com/medicare/mail_order_pharmacy_coverage. Some plans are available to thosewho have medical assistance from both the state and Medicare. Premiums, co-pays, coinsuranceand deductibles may vary based on the level of Extra Help you receive. Please contact WellCarefor details.
This information is available for free in other languages. Please call our customer service numberat 1-877-374-4056 (TTY 1-877-247-6272), Monday-Friday, 8 a.m. to 8 p.m. Between October1 and February 14, representatives are available Monday-Sunday, 8 a.m. to 8 p.m.
www.wellcare.com/medicare
7627
2