medical university of south carolina/sc-geriatric education center dental caries. determination....
TRANSCRIPT

Medical University of South Carolina/SC-Geriatric Education Center
Dental caries. Determination. Epidemiology of caries: prevalence and intensity of caries, increase of intensity. Card of epidemiology
examination of WHO. Etiology and cariogenesis. Modern pictures of reasons of origin and theory of development of caries: essence, advantages and failings. Concept of functionally structural
resistence of hard tissues of tooth. Lecturer: as. Yavors’ka-Skrabut I.M.Therapeutic dentistry department

Medical University of South Carolina/SC-Geriatric Education Center
The Epidemiology of Dental Caries in Older Adults

Medical University of South Carolina/SC-Geriatric Education Center
Overview Epidemiology
Epidemiology of dental caries Definition Distribution
By geography, age, gender, race/ethnicity, SES Determinants
Food cariogenicity, diet
Studies of dental caries in older adults
Conclusions
Medical University of South Carolina/SC-Geriatric Education Center
Learning Objectives
At the conclusion of this module, the participant will be able to: Define epidemiology Define dental caries Describe the dental caries index Describe the epidemiology of dental
caries Describe factors related to dental caries

Medical University of South Carolina/SC-Geriatric Education Center
Supplemental Documents
The Pre-Post Test Question with answers, References, and Evaluation Form for this module are found on a separate MS Word document.

Medical University of South Carolina/SC-Geriatric Education Center
Epidemiology1
Epidemiology is the study of the Distribution and Determinants of Disease/health in a population
Definition mnemonic – “3D’s”

Medical University of South Carolina/SC-Geriatric Education Center
Disease: Dental Caries2-4
How to define dental caries? Demineralization of the hard tissues of the
teeth caused by low pH, e.g., bacterial acids http://oralhealth.dent.umich.edu
/CDRAM/Principles.
How to measure dental caries? DMFT and DMFS http://
www.whocollab.od.mah.se/expl/orhdmft.html
Medical University of South Carolina/SC-Geriatric Education Center
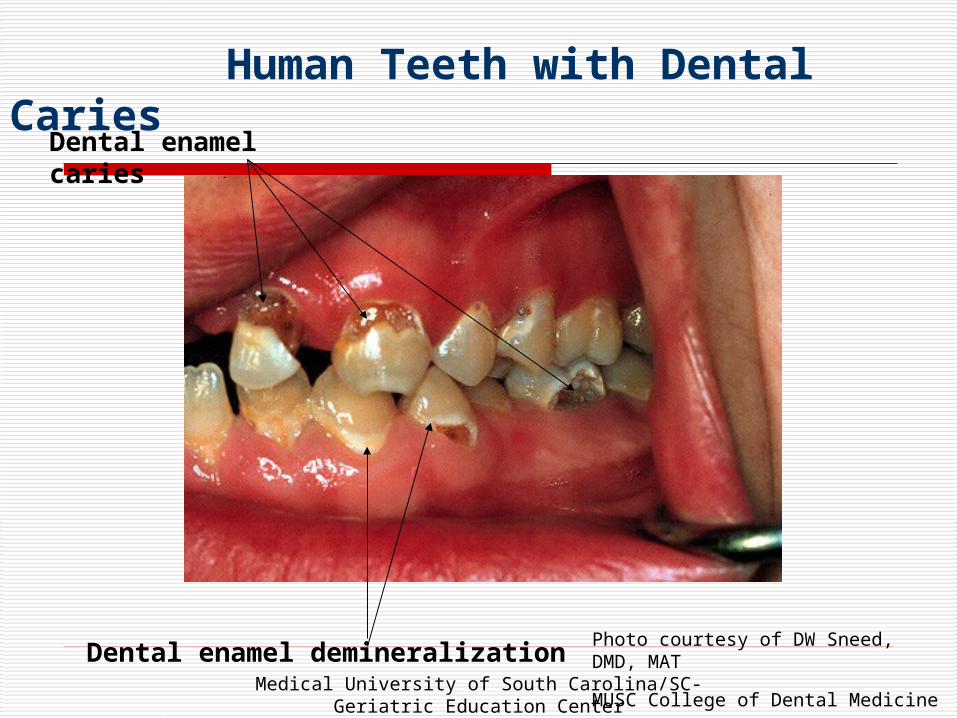
Photo courtesy of DW Sneed, DMD, MAT
MUSC College of Dental Medicine
Human Teeth with Dental Caries
Dental enamel caries
Dental enamel demineralization

Medical University of South Carolina/SC-Geriatric Education Center
Photo courtesy of DW Sneed, DMD, MAT
MUSC College of Dental Medicine
Close-up Photograph of Root CariesDental enamel
Root
surface
Root caries

Medical University of South Carolina/SC-Geriatric Education Center
Disease: Dental Caries5-8
How to count dental caries for a population?U.S. National Surveys
NHANES, HHANES, NOHSShttp://www.cdc.gov/nchs/nhanes.htmhttp://www.cdc.gov/nohss/sealants/surveys.htm
NIDCR/CDC Dental, Oral, and Craniofacial Data Resource Centerhttp://drc.nidcr.nih.gov/default.htm

Medical University of South Carolina/SC-Geriatric Education Center
A Brief History of Dental Caries9
Evidence from human skulls 400’s – 1500’s
occlusal dental caries relatively uncommon attrition outpaced occlusal caries
root caries predominate
1600’s – 1800’s more refined foods, sugar new dental caries pattern
generally begin in pits & fissures of teeth later on proximal surfaces (between teeth) well-established by end of 1800’s in most developed
countries

Medical University of South Carolina/SC-Geriatric Education Center
Brief History of Dental Caries9
Throughout most of 1900’s Dental caries experience
seen primarily in high-income countries low prevalence in low-income world likely related to diet
Late 1900’s Dental caries experience
increase in some (not all) low-income countries decrease in high-income countries among
children young adults

Medical University of South Carolina/SC-Geriatric Education Center
Distribution: Dental Caries
Geographic Age
Gender
Race / ethnicity
Socioeconomic status
Familial patterns

Medical University of South Carolina/SC-Geriatric Education Center
Distribution: Geographic10
By Countryhttp://www.whocollab.od.mah.se/countriesalphab.html#TopVariation among countries

Medical University of South Carolina/SC-Geriatric Education Center
Distribution: Geographic
By Region in the US: Variation within country DMFS generally
highest in Northeast, lowest in West, and intermediate in Midwest and South
less distinct differences today than 50 years ago impact of fluorides and water fluoridation

Medical University of South Carolina/SC-Geriatric Education Center
Distribution: Age
DMF scores increase with increasing age DMF index is cumulative
(Decayed can become Filled, and then Missing through time)
Whole tooth missing due to dental caries is equal to a count of 4 or 5 surfaces in the DMFS index
Cohort effect

Medical University of South Carolina/SC-Geriatric Education Center
Average Number of Dental Caries on Permanent Teeth Surfaces (DMF), Among Dentate Persons by Age11
01020
30405060
708090
'18-19 '20-29 '30-39 '40-49 '50-59 '60-69 '70+
Age
Mea
n D
MF
S
Medical University of South Carolina/SC-Geriatric Education Center
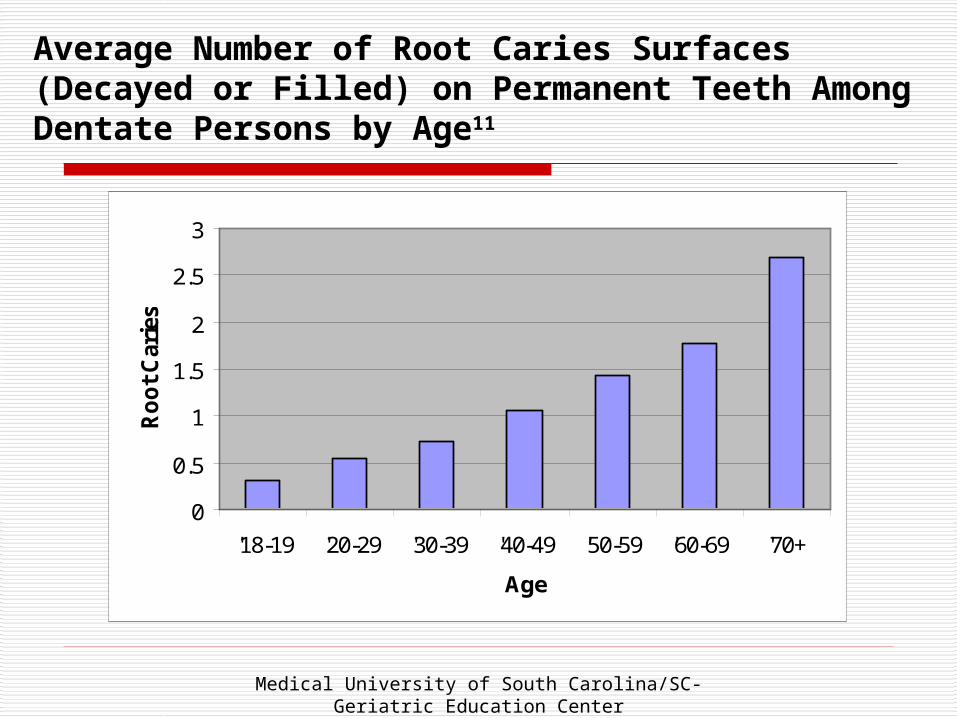
Average Number of Root Caries Surfaces (Decayed or Filled) on Permanent Teeth Among Dentate Persons by Age11
0
0.5
1
1.5
2
2.5
3
'18-19 '20-29 '30-39 '40-49 '50-59 '60-69 '70+
Age
Ro
ot
Car
ies

Medical University of South Carolina/SC-Geriatric Education Center
Distribution: Gender
Females generally have higher DMF scores
Probable treatment effect females usually have higher “Filled”
component Earlier tooth eruption among females Cannot say females are more
susceptible to dental caries

Medical University of South Carolina/SC-Geriatric Education Center
Average Number of Coronal Caries on Permanent Teeth Surfaces, DMF, Among Dentate Persons by Gender and by Age11
0102030405060708090
'Mal
e
'Fem
ale
'Mal
e
'Fem
ale
'Mal
e
'Fem
ale
'Mal
e
'Fem
ale
'Mal
e
'Fem
ale
'Mal
e
'Fem
ale
'Mal
e
'Fem
ale
'18-19
'18-19
'20-29
'20-29
'30-39
'30-39
'40-49
'40-49
'50-59
'50-59
'60-69
'60-69
'70+ '70+
Mea
n D
MF
S
Age (years) by Gender

Medical University of South Carolina/SC-Geriatric Education Center
Distribution: Race-Ethnicity
Little evidence for inherent differences in dental caries susceptibility across race-ethnicity.
Differences in socioeconomic status associated with race-ethnicity in the U.S. are probably more important.

Medical University of South Carolina/SC-Geriatric Education Center
Distribution: Socioeconomic Status
SES relates to a person’s background-values Education Income Occupation
Most recent data suggest that DMFS scores are inversely related to SES

Medical University of South Carolina/SC-Geriatric Education Center
Socioeconomic Status and Age Groups
15-24 years 35-44 years 55-64 years
Average DMFS Scores for Adults in Three Socioeconomic Levels, 1988-949,11
0
1020
30
40
5060
70
80
Low Middle High Low Middle High Low Middle High
Average DMFS
DecayedMissingFilled
9,11

Medical University of South Carolina/SC-Geriatric Education Center
Percentage of adults aged 50 years and older with 21 or more teeth by race-ethnicity and federal poverty level10,11
• Age standardized to the year 2000 U.S. population.
4.2.3

Medical University of South Carolina/SC-Geriatric Education Center
Distribution : Familial Patterns9
“My family has bad teeth”
May be a function of Bacterial transmission Family habits/ culture
diet behavioral traits
Genetics (e.g., salivary flow, composition)
Additional research is needed

Medical University of South Carolina/SC-Geriatric Education Center
Determinants: Dental Caries
Host (teeth) Substrate (fermentable
carbohydrates) Flora (bacteria) Time

Medical University of South Carolina/SC-Geriatric Education Center
Determinants: Cariogenicity12
‘Cariogenicity’ is suggested to apply to gram-to-gram cariogenic potential for comparisons
‘Effective cariogenicity’ includes both the gram-to-gram cariogenic potential and the frequency and duration of exposure of the teeth
Fruits, in general, have very low or no cariogenic potential.

Medical University of South Carolina/SC-Geriatric Education Center
Determinants: Diet & Dental Caries9
The intake of refined carbohydrates, especially refined sugars, is a risk factor for caries,e.g., animal models human studies
Cooked or milled starches can be broken down by salivary amylase and then serve as a substrate for cariogenic bacteria
Uncooked / lightly cooked vegetables are considered virtually noncariogenic

Medical University of South Carolina/SC-Geriatric Education Center
Dental Caries Experience in Older Adults13
Four large cohort studies of adults aged 50 years or older Iowa North Carolina Ontario South Australia
Reports of coronal and root caries At least a 3 year follow-up period

Medical University of South Carolina/SC-Geriatric Education Center
Incidence and Increments of Coronal and Root Caries in Older Adults13
Number at follow-up
Observation period (years)
Coronal Caries Root Surface Caries Both Combined
Study Incidence Increment Incidence Increment Increment
Iowa 338 3 56% 2.4 (0.8)* 44% 1.1 (0.4) 3.5 (1.2)
North Carolina
3
Blacks 234 45% 1.6 (0.5) 29% 0.6 (0.2) 2.2 (0.7)
Whites 218 59% 2.1 (0.7) 39% 0.8 (0.3) 2.9 (1.0)
Ontario 493 3 57% 1.9 (0.6) 27% 0.6 (0.2) 2.5 (0.8)
South Australia
528 5 67% 2.7 (0.5) 59% 2.2 (0.4) 4.9 (1.0)
•Parentheses contain the annualized increment, computed by dividing the combined caries increment by the number of years of follow-up, then rounding the result to 1 decimal place

Medical University of South Carolina/SC-Geriatric Education Center
Risk Factors for Caries Development in Older Adults13
Coronal caries No common risk factors Suggested factors include low SES, and severity
of periodontal attachment loss at baseline
Root caries Common risk factor was partial denture wearing Other suggested factors include periodontal
problems and age

Medical University of South Carolina/SC-Geriatric Education Center
Caries in Swedish Older Adults14
Methods 10-year incidence study 55, 65, and 75 years old at baseline Measured coronal and root caries
Results Higher incidence of coronal caries in youngest
age group (65 years old at conclusion of study) Higher incidence of root caries in oldest age
group (85 years old at conclusion of study)
Medical University of South Carolina/SC-Geriatric Education Center
A State of Decay: The Oral Health of Older Americans15
September 2003: publication of an Oral Health America Special Grading Project
http://www.oralhealthamerica.org/pdf/StateofDecayFinal.pdf
Overall National Grade: D
Vast majority of older Americans do not have dental insurance coverage No Medicare dental coverage Most state Medicaid programs only cover emergency-only
dental benefits: D+ 71-80% do not have private dental insurance: D

Medical University of South Carolina/SC-Geriatric Education Center
Conclusions As the number of missing teeth increase with
increased age, so do the number of surfaces affected by dental caries
Older adults suffer from the accumulation of coronal and root caries over their lifetimes
Older adults have less dental insurance (Medicare does not cover usual dental services), make fewer dental visits, and use more medication that may lead to decreased saliva (xerostomia)

Medical University of South Carolina/SC-Geriatric Education Center
BiographySusan G. Reed, DDS, MPH, DrPH is an Assistant Professor of Stomatology, Director of the Dental Public Health & Oral Epidemiology Section at the College of Dental Medicine. Her joint appointment is with the Department of Biometry, Bioinformatics & Epidemiology. Her dental degree is from Case Western Reserve University and she is a 1996 graduate of the University of Michigan, School of Public Health where she completed her MPH, Residency in Dental Public Health, and was an NIH fellow for her doctorate in oral epidemiology. Dr. Reed is Board Certified in Dental Public Health. Her research interests include the epidemiology of oral cancer in SC, and oral Chlamydia trachomatis research.