medical stone management made easy – … stone management made easy ... high acid-ash diet,...
TRANSCRIPT
MEDICAL STONE MANAGEMENT MADE EASY –
PRACTICAL ADVICE
Glenn M. Preminger, M.D.
Comprehensive Kidney Stone Centerat Duke University Medical Center
Durham, North Carolina
UCLA State-of-the Art Urology 02 March 2017
MEDICAL MANAGEMENT OF NEPHROLITHIASISPromoters of Nephrolithiasis
Dietary sodiumDietary calcium / Calcium supplements Changing epidemiologic patterns
High acid-ash diet, obesity, bariatric surgery
Inhibitors of NephrolithiaisPotassium Citrate
Long term treatmentLemonade
RECENT ADVANCES

METABOLIC EVALUATION
Calcareous calculi Non-calcareous calculiHypercalciuria (40-75%) Low urinary pH
Uric acid stones (5%)Hyperuricosuria (10-50%) CystinuriaHyperoxaluria (<5%) Cystine stones (1%)Hypomagesuria (<5%) Infection (urea-splitting)
Struvite stones (15%)Hypocitraturia (10-50%)
* Expressed as percentage of total
CLASSIFICATION
HYPERCALCIURAROLE OF SODIUM
Oral sodium intake is a major determinate of renal calcium excretionAn increased sodium intake of 100 mEq / day will increase urinary calcium 50 mg / dayExcess urinary sodium will also block the hypocalciuric action of thiazides
DIETARY CALCIUM
Early recommendations suggest that low calcium diet will decrease urinary Ca++ excretion, thereby reducing risk of stone formationPotential risk factors involving low calcium diet:
Reduced bone mass Increased urinary oxalate
IMPACT OF LOW CALCIUM DIET

DIETARY CALCIUM
45,600 men, ages 40-75, with no h/o stones97,000 women, ages 34-59,with no h/o stones
4 - 12 year follow-upCa++ intake inversely associated with stone formationLow calcium diet increases the risk for renal stone formation
IMPACT OF LOW CALCIUM DIET
Curhan, et al, 1993Curhan, et al, 1997
DIETARY CALCIUM
Five-year randomized, prospective trial in 120 men with hypercalciura (> 300 mg/day) and recurrent nephrolithiasis
IMPACT OF LOW CALCIUM DIET
Borghi,et al 2002
Low Calcium Diet(400 mg/day)
Normal sodiumNormal protein
Regular Calcium Diet(1200 mg/day)Low sodiumLow protein

DIETARY CALCIUMIMPACT OF LOW CALCIUM DIET
Borghi,et al 2002
440
248
460
236
0
100
200
300
400
500
Calcium(mg/day)
Low Calcium Norm Calcium
Baseline5 Years Rx
* *

DIETARY CALCIUMIMPACT OF LOW CALCIUM DIET
Borghi,et al 2002
227201
241
123
0
50
100
150
200
250
Sodium(meq/day)
Low Calcium Norm Calcium
Baseline5 Years Rx
*

DIETARY CALCIUMIMPACT OF LOW CALCIUM DIET
Borghi,et al 2002
33.1
39.0 37.0
29.0
0
10
20
30
40
Oxalate(mg/day)
Low Calcium Norm Calcium
Baseline5 Years Rx
**

DIETARY CALCIUMIMPACT OF LOW CALCIUM DIET
Borghi,et al 2002
p=0.04
DIETARY ADVICE
Normal calcium intake in most patientsModerate calcium restriction in patientswith absorptive hypercalciuriaModerate dietary intake of oxalate
Spinach, tea, chocolate, nutsLimit dietary sodium intakeLimit red meat intake
RECOMMENDATIONS
CALCIUM SUPPLEMENTS
Initial observations anecdotal
Clinical and physicochemical / physiologic data support this concept
CAUSE OF STONE FORMATION ?
CALCIUM SUPPLEMENTS
Prominent increase in urinary calcium during first month of supplementationLess prominent with continued therapy due to suppressed parathyroid function (↓ Vit D)
PREMENOPAUSAL WOMEN
POSTMENOPAUSAL WOMENCalciuric response is blunted due to impaired intestinal calcium absorption
Probably 20 to reduced Vit D synthesis

CALCIUM SUPPLEMENTS
"Citracal"Over-the-counter preparation
Calcium citrate 950 mgElemental calcium 200 gm
Provides increased intestinal calcium absorptionPrevents supersaturation of stone-forming saltsA more "stone-friendly" calcium supplement
CALCIUM CITRATE
CALCIUM SUPPLEMENTS
Long-term clinical trial in pre-menopausal womenNo significant change in urinary saturation of:
Calcium oxalate Calcium phosphate (brushite)
No increased propensity for crystallization of calcium saltsMainly due to "protective" effects of citrate
CALCIUM CITRATE
Sakhaee & Pak, 2004
CALCIUM SUPPLEMENTS
Check 24-hour urinary calcium 4 months after beginning supplementation
If nomocalciuric - nothing to do
If hypercalciuric - begin thiazides
RECOMMENDATIONS
Dietary changes potentially responsible for increasing incidence and changing trends in calcium oxalate and uric acid stone formation
High acid-ash dietObesity
CHANGING EPIDEMIOLOGIC PATTERNS
NEPHROLITHIASIS
MEDICAL MANAGEMENT OF NEPHROLITHIASIS
Peak incidence age 30 - 60Gender (Male : Female) 3 : 1Family history 3 - fold ↑ riskBody size ↑ risk with ↑ weightRecurrence after first stone:
Year 1 10 - 15%Year 5 50 - 60%Year 10 70 - 80%
NATURAL HISTORY & RISK FACTORS

MEDICAL MANAGEMENT OF NEPHROLITHIASIS
Peak incidence age 30 - 60Gender (Male : Female) 1.3 : 1Family history 3 - fold ↑ riskBody size ↑ risk with ↑ weightRecurrence after first stone:
Year 1 10 - 15%Year 5 50 - 60%Year 10 70 - 80%
NATURAL HISTORY & RISK FACTORS

MEDICAL MANAGEMENT OF NEPHROLITHIASIS
CHANGING EPIDEMIOLOGYUsing nationally representative data, an updated estimate the prevalence of kidney stones in the United States was performedNational Health and Nutrition Examination Survey (NHANES) queried participants about kidney stones
1994 20071 in 20 1 in 11
Scales, et al, 2012
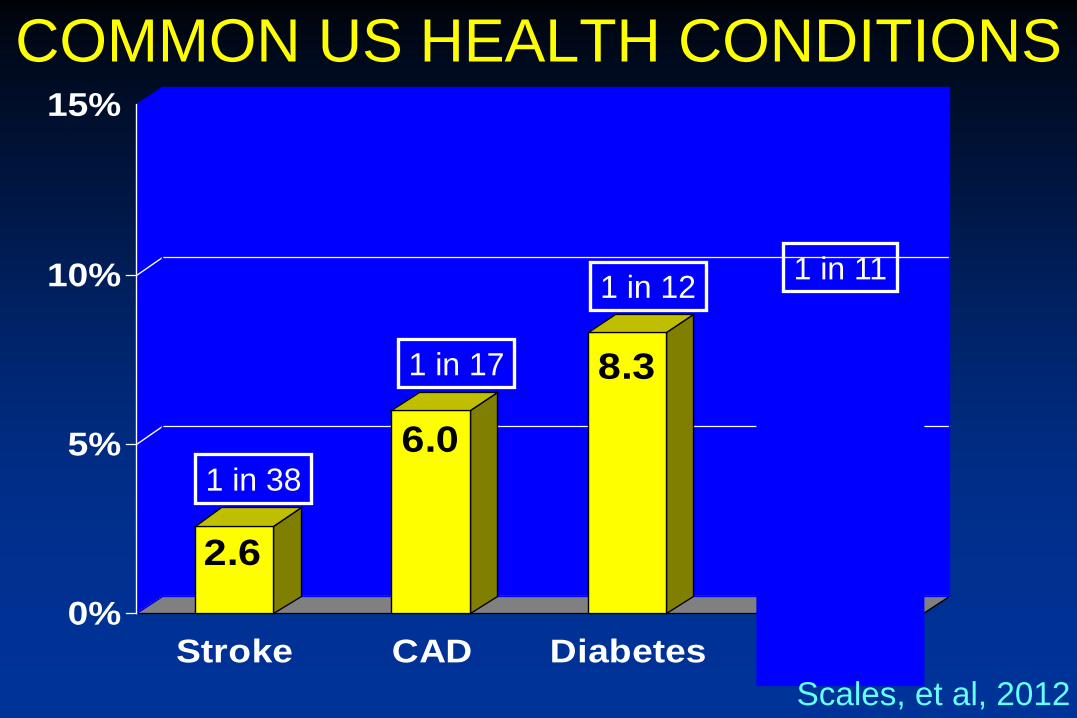
COMMON US HEALTH CONDITIONS
2.6
6.0
8.3 8.8
0%
5%
10%
15%
Stroke CAD Diabetes Stones
1 in 38
1 in 17
1 in 12 1 in 11
Scales, et al, 2012

BoneIncreased Ca resorption
IntestineIncreased Ca absorption
KidneyDecreased Ca reabsorptionDecreased Citrate synthesisIncreased tubular citratereabsorption
IMPACT OF ACIDOSIS
CHANGING TRENDSIN NEPHROLITHIASIS
Hypercalciuria & negative
Ca++ balance
Hypocitraturia
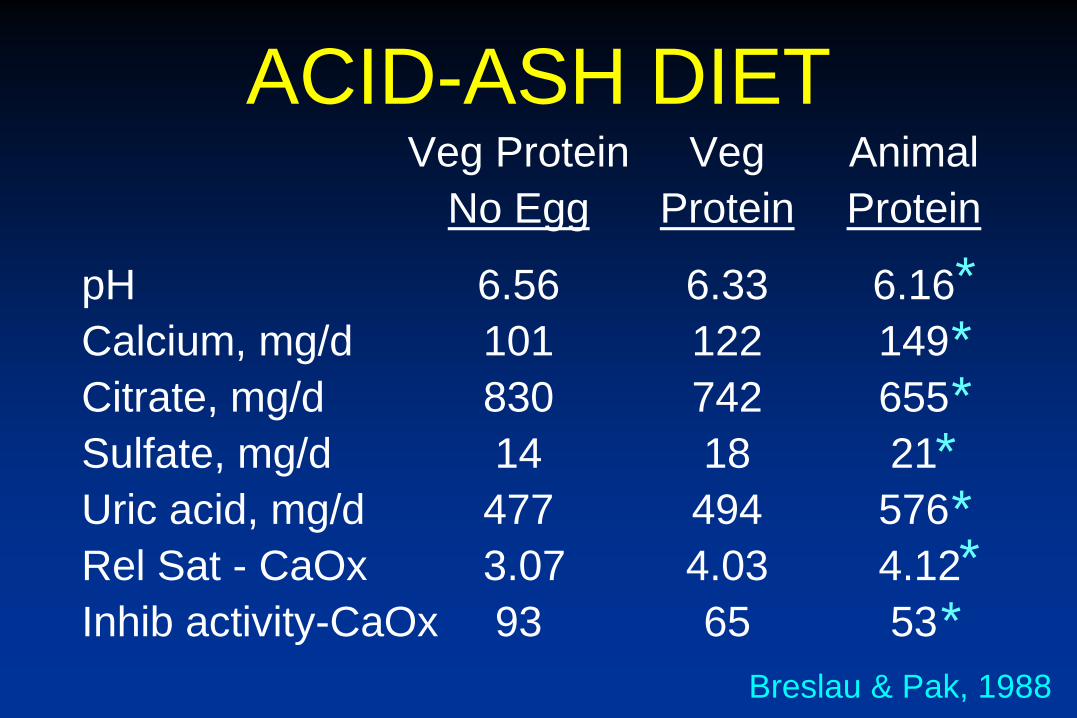
ACID-ASH DIETVeg Protein Veg Animal
No Egg Protein Protein
pH 6.56 6.33 6.16Calcium, mg/d 101 122 149Citrate, mg/d 830 742 655Sulfate, mg/d 14 18 21Uric acid, mg/d 477 494 576Rel Sat - CaOx 3.07 4.03 4.12Inhib activity-CaOx 93 65 53
Breslau & Pak, 1988
*
*
***
*
*
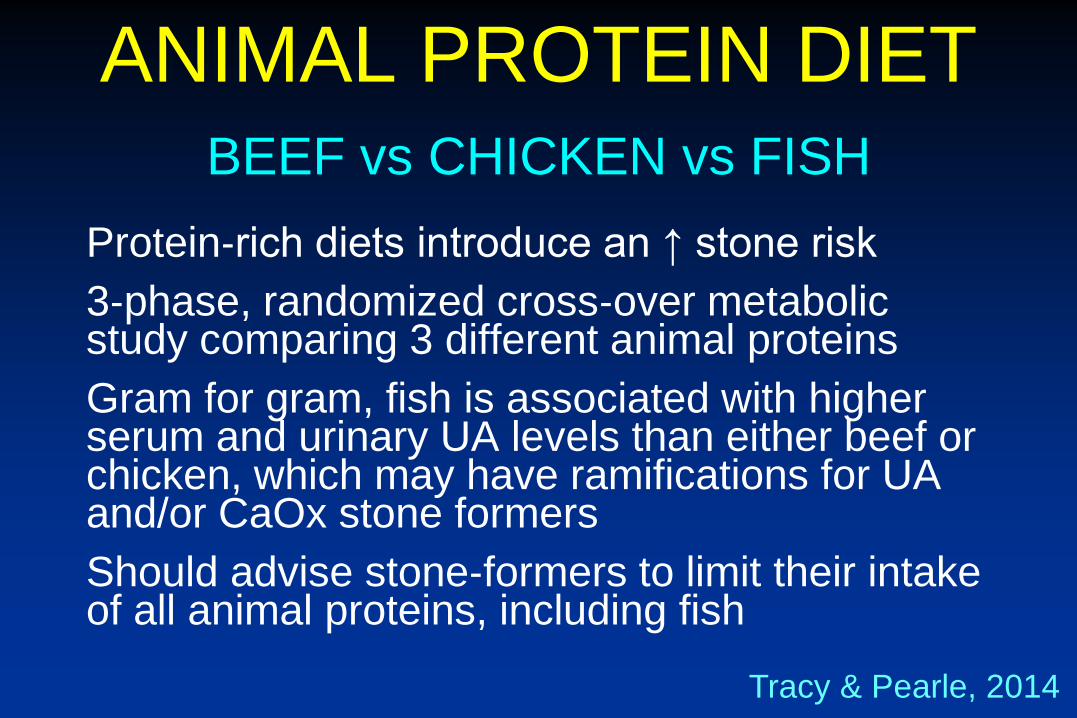
Protein‐rich diets introduce an ↑ stone risk3‐phase, randomized cross‐over metabolic study comparing 3 different animal proteinsGram for gram, fish is associated with higher serum and urinary UA levels than either beef or chicken, which may have ramifications for UA and/or CaOx stone formers Should advise stone‐formers to limit their intake of all animal proteins, including fish
BEEF vs CHICKEN vs FISH
ANIMAL PROTEIN DIET
Tracy & Pearle, 2014

NEPHROLITHIASISEFFECT OF ANIMAL PROTEIN DIET
Calcium pH
Sulfate Citrate
Uric acidAll increased risk factors for recurrent stone formation

1999OBESITY TRENDS AMONG U.S. ADULTS
2008
1990
No Data <10% 10%–14% 15%–19% 20%–24% 25%–29% ≥30%
PREVALENCE OF OBESITY

1999GLOBAL OBESITY TRENDS
2008
1990
No Data <10% 10%–14% 15%–19% 20%–24% 25%–29% ≥30%
PREVALENCE OF OBESITY

IMPACT OF OBESITY
Stone patient population: 1021
Obese patients with stones: 140 (14%)
Obese patients with complete 83metabolic evaluation receiving medical therapy
RETROSPECTIVE REVIEW
Ekeruo, et al, 2004
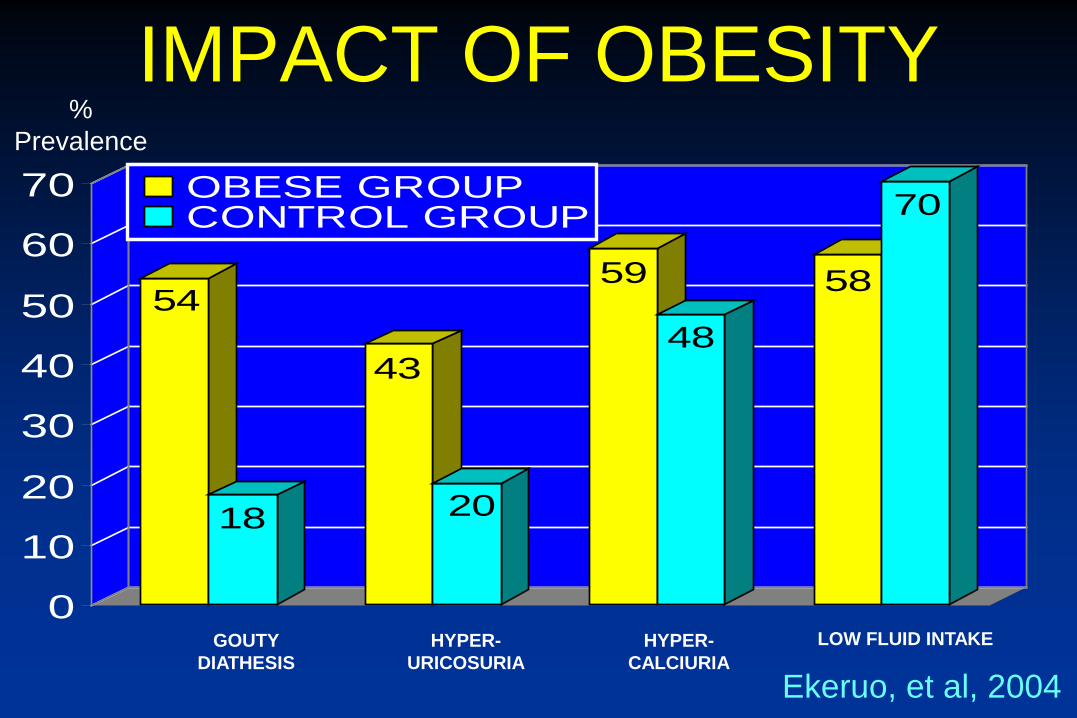
54
18
43
20
59
48
58
70
0
10
20
30
40
50
60
70 OBESE GROUPCONTROL GROUP
GOUTYDIATHESIS
HYPER-URICOSURIA
HYPER-CALCIURIA
LOW FLUID INTAKE
% Prevalence
Ekeruo, et al, 2004
IMPACT OF OBESITY
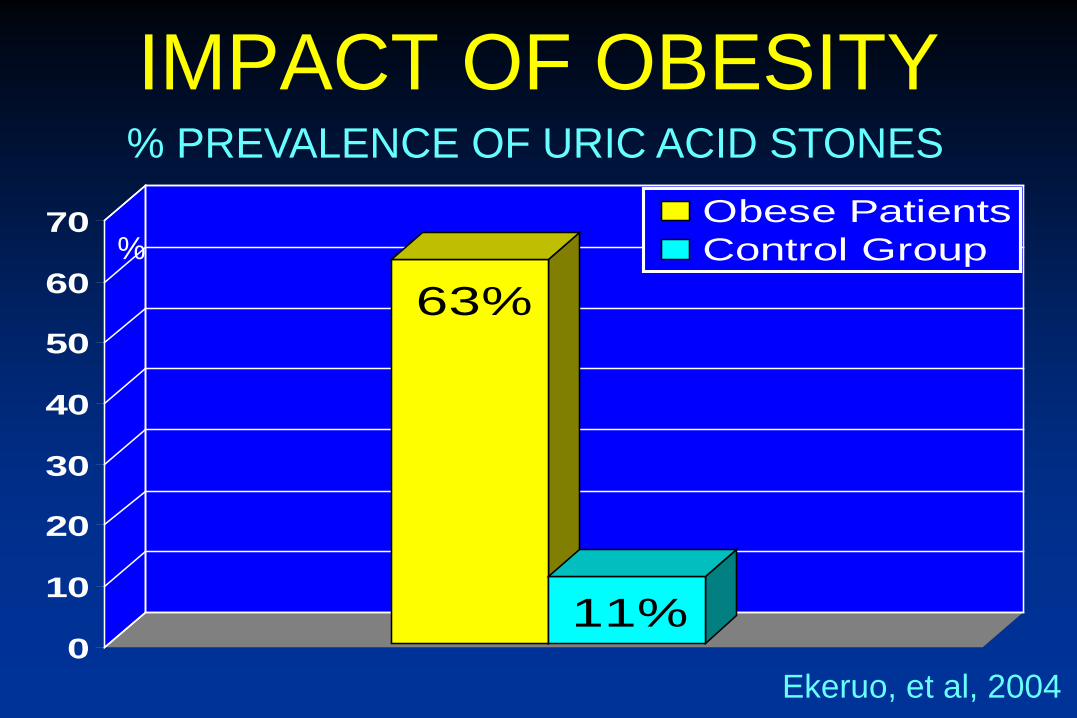
63%
11%0
10
20
30
40
50
60
70 Obese PatientsControl Group
% PREVALENCE OF URIC ACID STONES
%
Ekeruo, et al, 2004
IMPACT OF OBESITY
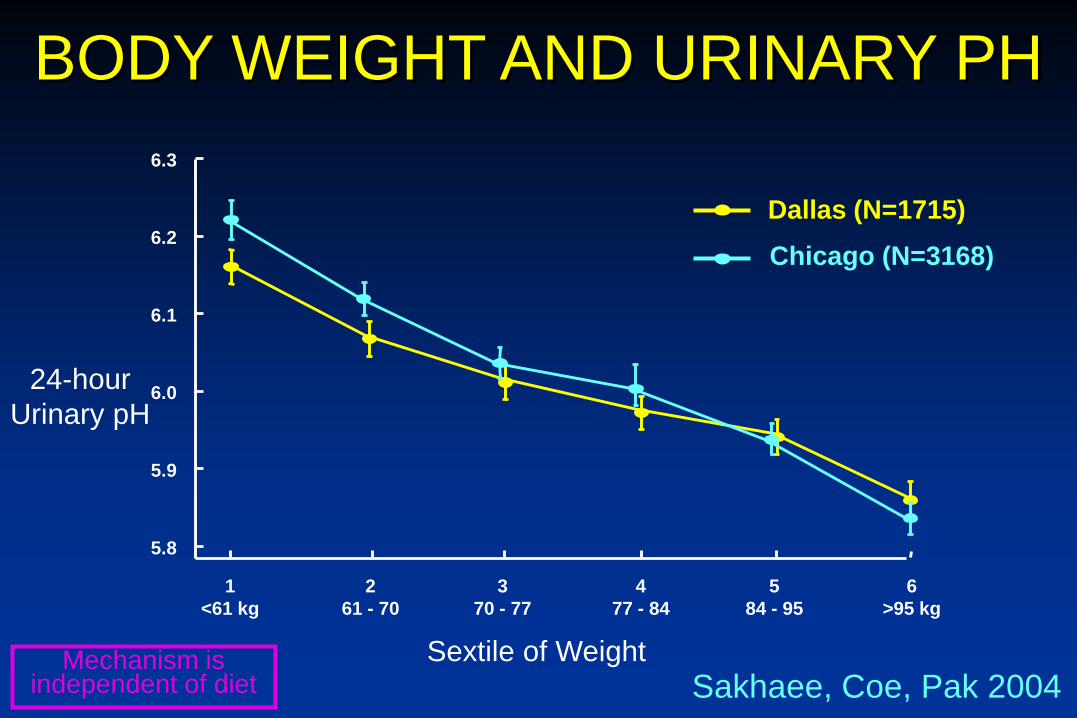
Sextile of Weight
24-hour Urinary pH
5.8
5.9
6.0
6.1
6.2
6.3
Dallas (N=1715)Chicago (N=3168)
1<61 kg
261 - 70
370 - 77
477 - 84
584 - 95
6>95 kg
BODY WEIGHT AND URINARY PH
Mechanism is independent of diet Sakhaee, Coe, Pak 2004
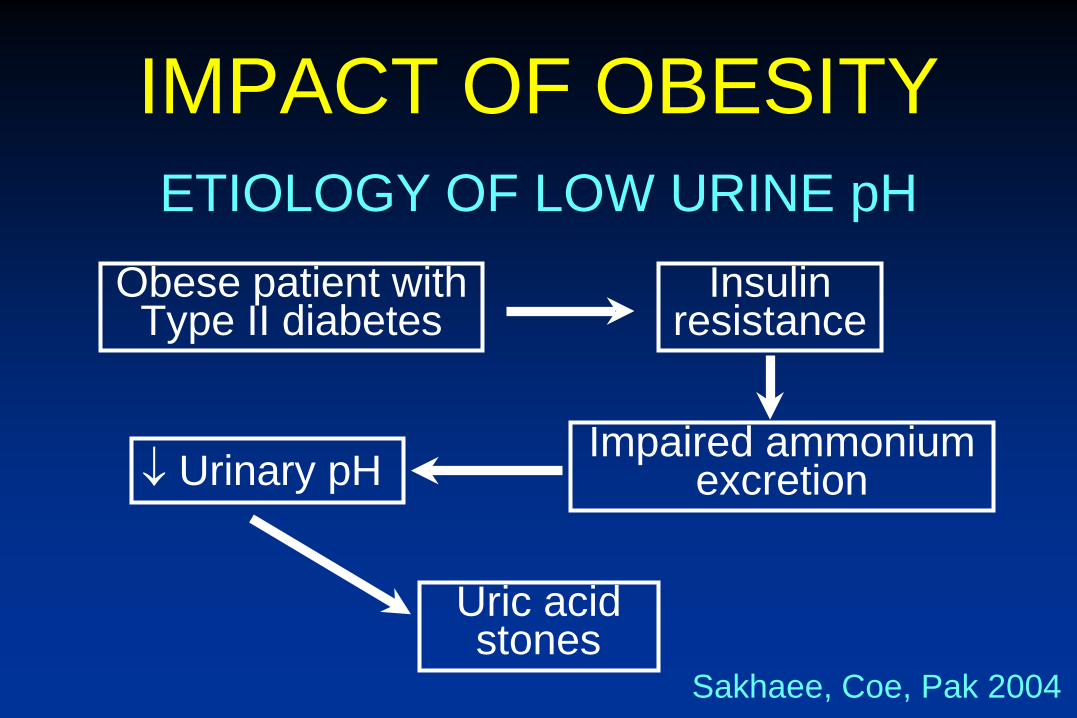
IMPACT OF OBESITY
Obese patient withType II diabetes
ETIOLOGY OF LOW URINE pH
Sakhaee, Coe, Pak 2004
Impaired ammonium excretion
Insulinresistance
↓ Urinary pH
Uric acidstones

IMPACT OF OBESITY
Dietary modification & weight loss
POSSIBLE SOLUTIONS
Reverse insulin resistance
Normal urinary acidity
Alkali therapy
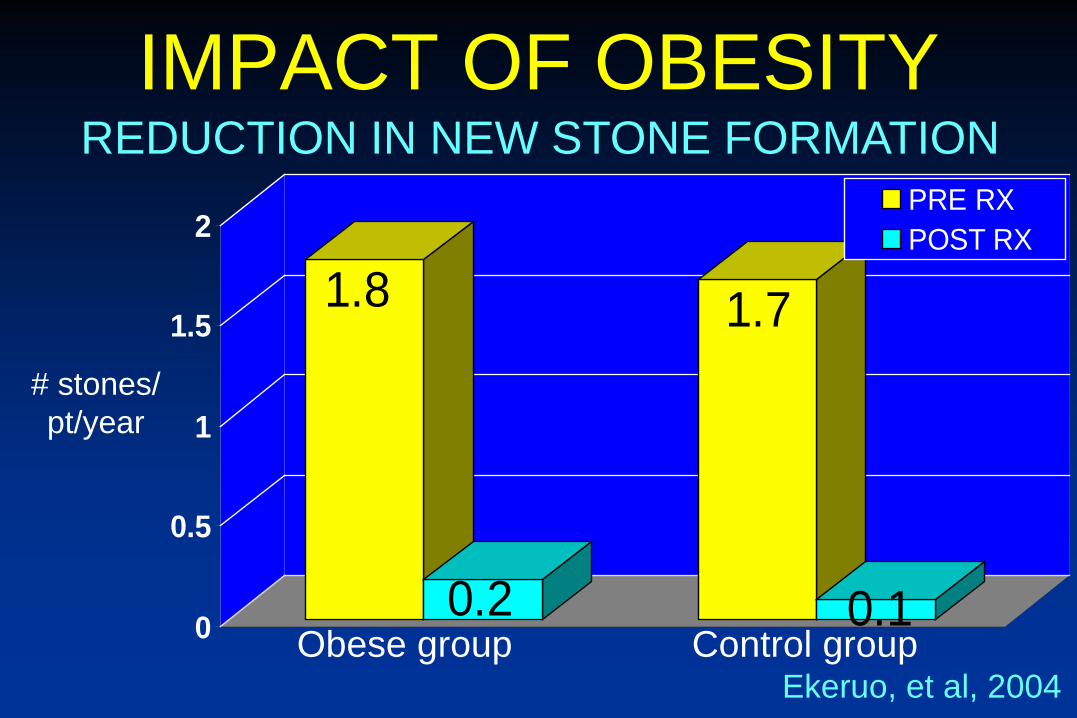
1.8
0.2
1.7
0.10
0.5
1
1.5
2PRE RXPOST RX
Obese group Control group
REDUCTION IN NEW STONE FORMATION
# stones/pt/year
Ekeruo, et al, 2004
IMPACT OF OBESITY
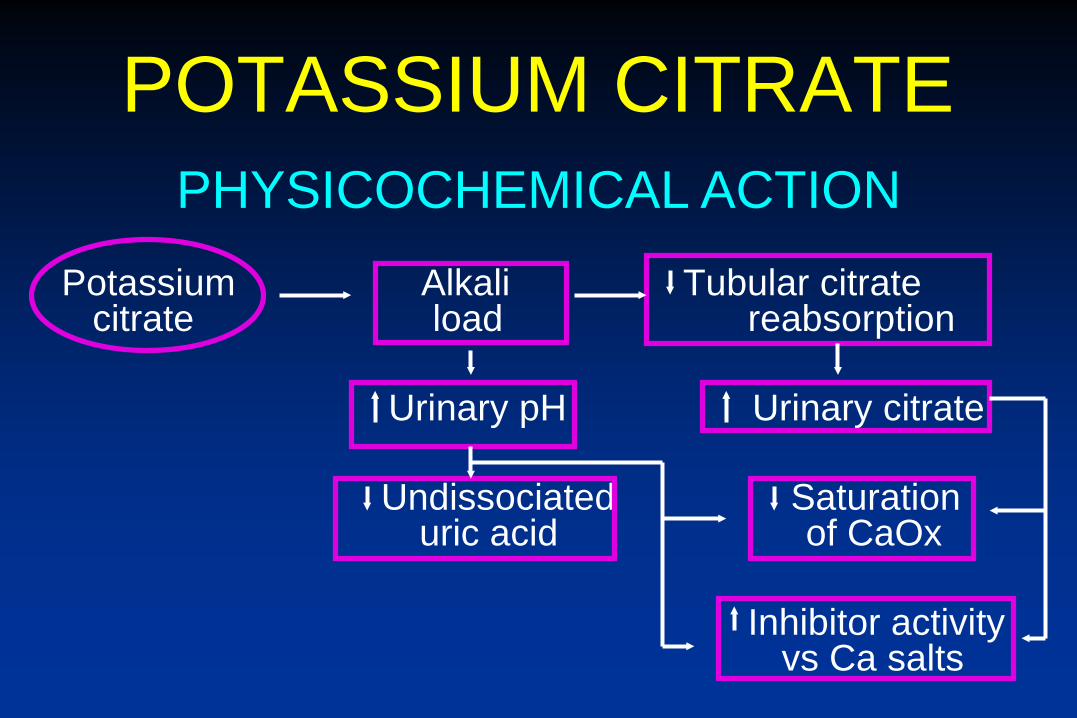
POTASSIUM CITRATE
Potassium Alkali Tubular citratecitrate load reabsorption
Urinary pH Urinary citrate
Undissociated Saturationuric acid of CaOx
Inhibitor activityvs Ca salts
PHYSICOCHEMICAL ACTION

LONG TERM RX WITH POTASSIUM CITRATE
1480 patients were reviewed in the Duke Stone Center Database 954 patients had ≥ two 24-hour urinary profiles515 patients were included in the analysisMean Duration of KCit therapy
41 months (range 6 – 168 months)
METHODS
Robinson, et al, 2008

CHANGE IN pH BY DURATION
p < 0.0001
Robinson, et al, 2008
Pre-Rx 6–12 mo 12–24 mo 24–36 mo > 36 mo
LONG TERM K-CITRATE

CHANGE IN CITRATE BY DURATION
Pre-Rx 6–12 mo 12–24 mo 24–36 mo > 36 mo
p < 0.01
Robinson, et al, 2008
LONG TERM K-CITRATE

STONE FORMATION RATE
2.34
0.580.0
0.5
1.0
1.5
2.0
2.5
3.0
ston
es/y
ear
p < 0.0001
Pre-Rx Post-Rx
LONG TERM K-CITRATE

CONCLUSIONSKCit provides a significant alkali and citraturic response during both short and long term therapyUrinary metabolic profiles are sustained for as long as 14 yearsLong term KCit therapy significantly reduces stone formation rates
LONG TERM RX WITH POTASSIUM CITRATE
Robinson, et al, 2008
POTASSIUM CITRATE
Liquid / crystals - Citra–K crystals(generic)
Slow-release pills - Urocit K® / genericUrocit K® - 15
CURRENT PREPARATIONS
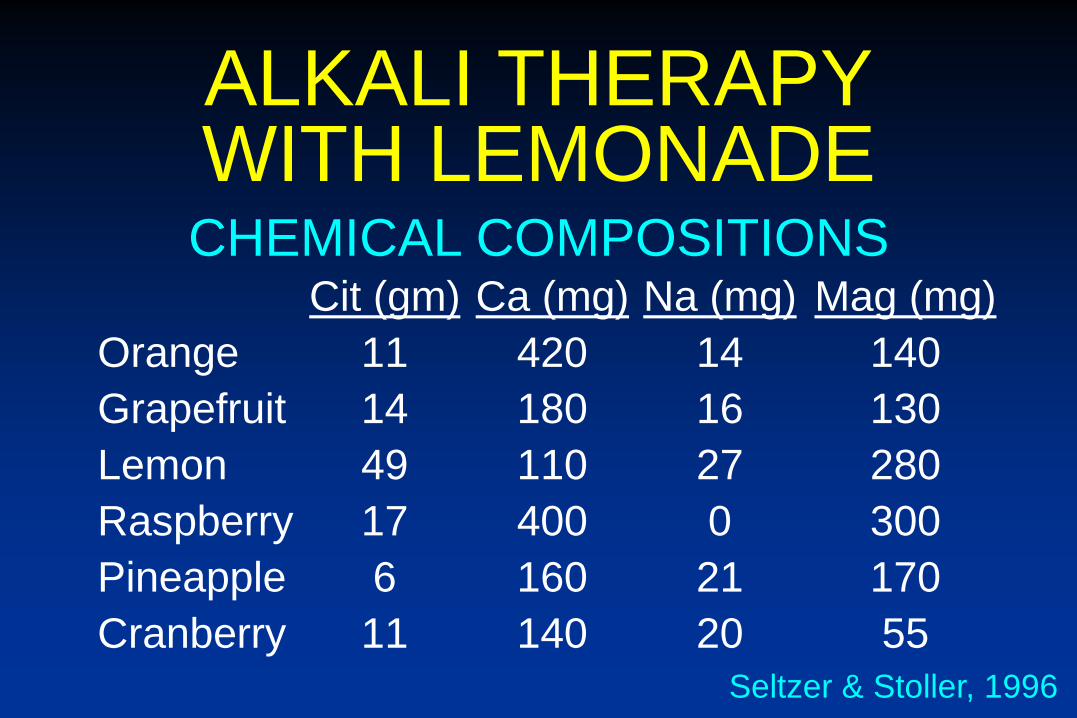
ALKALI THERAPYWITH LEMONADE
Cit (gm) Ca (mg) Na (mg) Mag (mg)Orange 11 420 14 140Grapefruit 14 180 16 130Lemon 49 110 27 280Raspberry 17 400 0 300Pineapple 6 160 21 170Cranberry 11 140 20 55
CHEMICAL COMPOSITIONS
Seltzer & Stoller, 1996
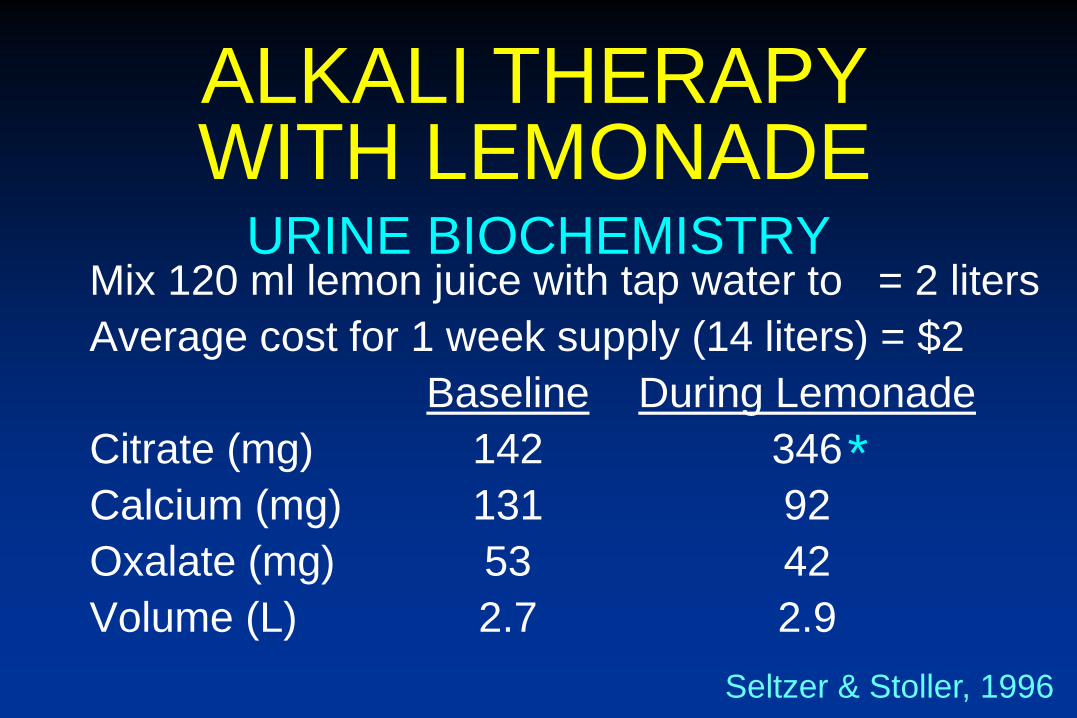
URINE BIOCHEMISTRYMix 120 ml lemon juice with tap water to = 2 litersAverage cost for 1 week supply (14 liters) = $2
Baseline During LemonadeCitrate (mg) 142 346Calcium (mg) 131 92Oxalate (mg) 53 42Volume (L) 2.7 2.9
ALKALI THERAPYWITH LEMONADE
Seltzer & Stoller, 1996
*
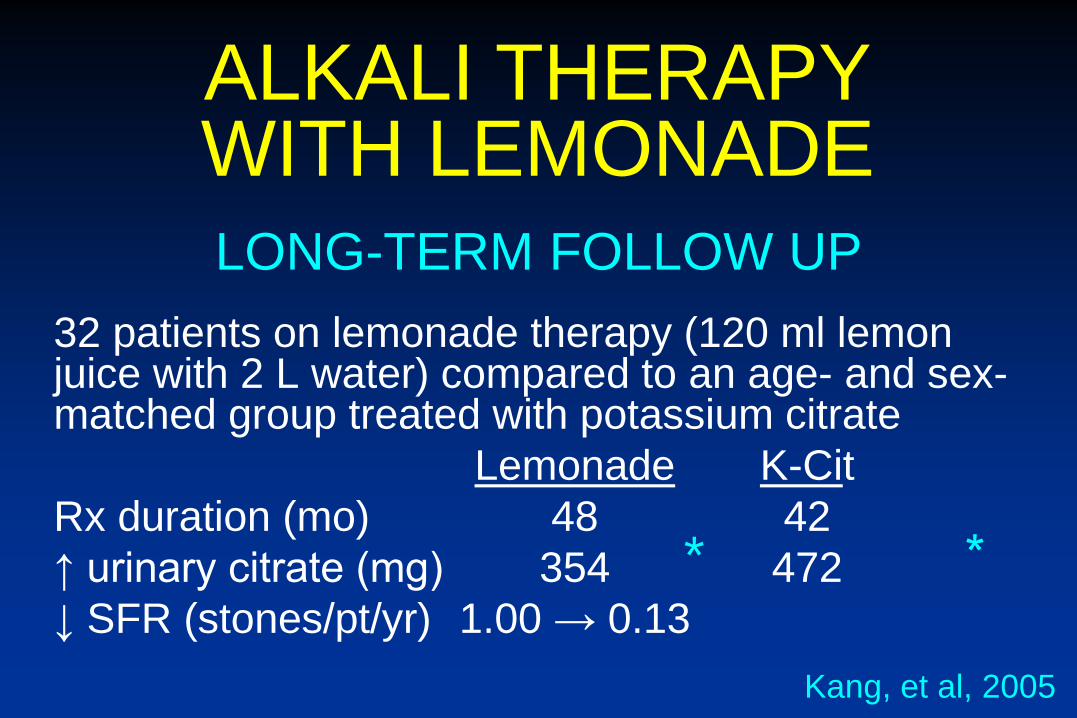
LONG-TERM FOLLOW UP32 patients on lemonade therapy (120 ml lemon juice with 2 L water) compared to an age- and sex-matched group treated with potassium citrate
Lemonade K-CitRx duration (mo) 48 42↑ urinary citrate (mg) 354 472↓ SFR (stones/pt/yr) 1.00 → 0.13
ALKALI THERAPYWITH LEMONADE
Kang, et al, 2005
*

ALTERNATIVES TO K-CIT60 mEq/day of NaBic provided an equivalent and significant increase in urinary citrate and pH(1300 mg / BID)NaBic led to a significant ↑ in sodium excretion without concomitant ↑ in urinary calcium This short-term study suggests that NaBic may be an effective alternative for the treatment of hypocitraturia in patients who cannot tolerate or afford the cost of KCitNaBic is not ideal in patients with pure uric acid stones and high urate excretion
ALKALIZATION WITH NA+ BICARB
Pinheiro & Heilberg, 2013

MEDICAL MANAGEMENT OF NEPHROLITHIASIS
Dietary ModificationNormal calcium, low salt, low protein
New MedicationsPotassium magnesium citrate
Enteric TherapyOxalobactor formigenes
Genetic TherapyHypercalciuriaCystinuria
FUTURE DIRECTIONS