medical interventions for addiction in primary … ky 2010...medical interventions for addiction in...
TRANSCRIPT

Medical Interventions for Addiction in Primary CareMedical Interventions for Addiction in Primary CareAddiction in Primary Care SettingsAddiction in Primary Care Settings
R. Douglas Bruce, MD, MA, MScR. Douglas Bruce, MD, MA, MScR. Douglas Bruce, MD, MA, MScAssistant ProfessorYale University School of Medicine
R. Douglas Bruce, MD, MA, MScAssistant ProfessorYale University School of Medicine
March 23, 2010March 23, 2010

NIH Consensus on Drug TreatmentNIH Consensus on Drug Treatment
• Drug Addiction is a disorder of the brain and th f di l di d
• Drug Addiction is a disorder of the brain and th f di l di dtherefore a medical disorder
• Broader access to drug treatment
therefore a medical disorder
• Broader access to drug treatment
• Reduce federal and state barriers impeding access to treatment
• Reduce federal and state barriers impeding access to treatment
• Stressed the importance of providing substance abuse counseling psychosocial therapies and
• Stressed the importance of providing substance abuse counseling psychosocial therapies andabuse counseling, psychosocial therapies, and other supportive services abuse counseling, psychosocial therapies, and other supportive services
March 23, 2010 2

Summary SlideSummary Slide
• Just as medication can help with depression, • Just as medication can help with depression, medication can help in the treatment of alcohol dependence, opioid dependence, medication can help in the treatment of alcohol dependence, opioid dependence, cocaine dependence, nicotine dependence, etc.cocaine dependence, nicotine dependence, etc.
March 23, 2010 3
OutlineOutline
• Neurobiology of addiction
M di i i d
• Neurobiology of addiction
M di i i d• Medication assisted treatment
– Opioids - methadone, buprenorphine,
• Medication assisted treatment
– Opioids - methadone, buprenorphine, naltrexone
– Cocaine – disulfiram
naltrexone
– Cocaine – disulfiram
– Methamphetamine - buproprion
– Alcohol – naltrexone, topiramate
– Methamphetamine - buproprion
– Alcohol – naltrexone, topiramate, p
– Nicotine – NRT, buproprion, varenicline
, p
– Nicotine – NRT, buproprion, varenicline
March 23, 2010 4

NEUROTOXICITYAIDSCANCER
NEUROTOXICITYAIDSCANCER
NeurotoxicityAIDS, CancerMental illness
NeurotoxicityAIDS, CancerMental illness
CANCERMENTAL ILLNESSCANCERMENTAL ILLNESS
Health careHealth careHomelessnessHomelessness
March 23, 2010 5
ProductivityAccidentsProductivityAccidents
HomelessnessCrimeViolence
HomelessnessCrimeViolence

If the societal cost is so high, why do people do drugs?If the societal cost is so high, why do people do drugs?do people do drugs?do people do drugs?
March 23, 2010 6

Common Myths About Drug Abuse…Common Myths About Drug Abuse…
• Drug abuse equates to drug addiction• Drug abuse equates to drug addictionDrug abuse equates to drug addiction
• Alcohol is not a drug
• Addiction is a moral weakness
Drug abuse equates to drug addiction
• Alcohol is not a drug
• Addiction is a moral weakness• Addiction is a moral weakness
• You have to hit rock bottom to recover
• Addiction is a moral weakness
• You have to hit rock bottom to recover
• You have to want treatment for it to be successful
• You have to want treatment for it to be successful
• Drug abuse is more common among minorities
• Drug abuse is more common among minorities
March 23, 2010 7
AddictionAddiction
• A state in which an organism engages in l i b h i
• A state in which an organism engages in l i b h icompulsive behavior
– The behavior is reinforcing (that is,
compulsive behavior
– The behavior is reinforcing (that is, pleasurable or rewarding)
– There is a loss of control in limiting the
pleasurable or rewarding)
– There is a loss of control in limiting the intake of the substanceintake of the substance
March 23, 2010 8

Why Do People Take Drugs in The First Place?Why Do People Take Drugs in The First Place?
To feel goodTo have novel:
f li
To feel better
feelingssensations
experiences
To lessen:anxietyworriesp
ANDto share them
worriesfearsdepressionh lhopelessness
March 23, 2010 9
V l bilitVulnerability
Why do some people become ddi d hil h d ?
March 23, 2010 10
addicted while others do not?

Biology/genesBiology/genes
E i t
Biology/EnvironmentInteractions
Environment
March 23, 2010 11
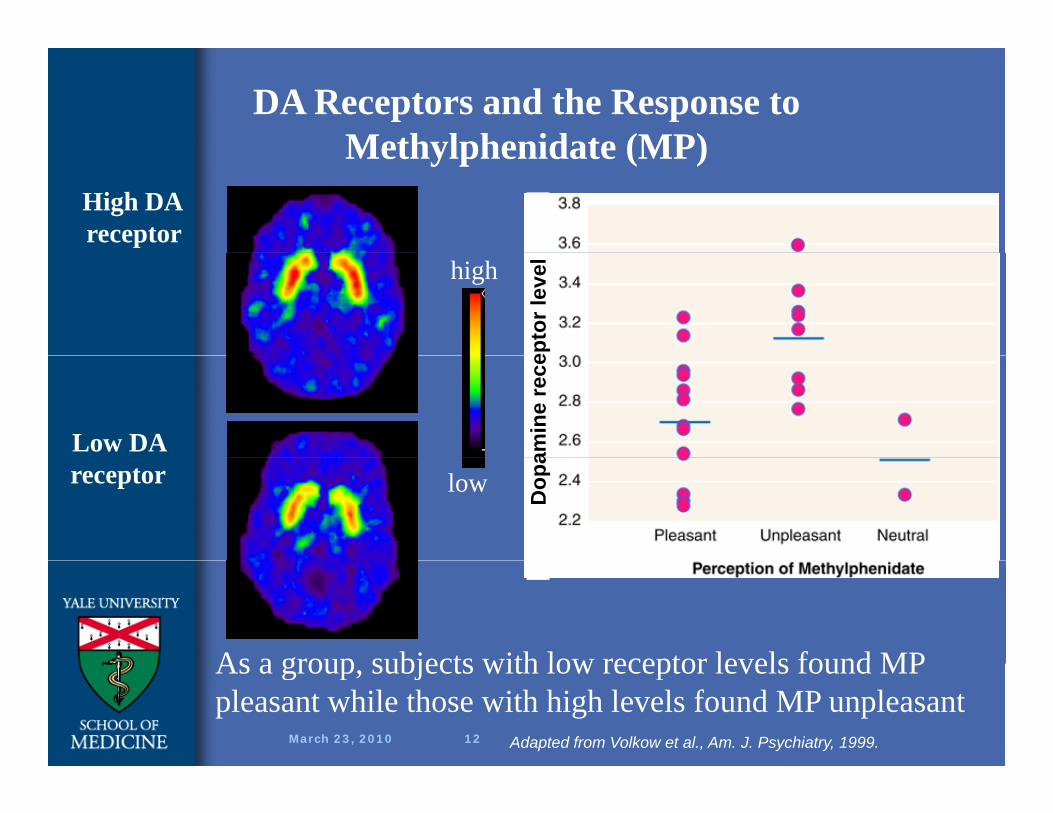
DA Receptors and the Response to Methylphenidate (MP)
High DA receptor
Methylphenidate (MP)
high
epto
r lev
el
Low DA amin
e re
ce
lowreceptor
Dop
a
As a group subjects with low receptor levels found MP
March 23, 2010 12
As a group, subjects with low receptor levels found MP pleasant while those with high levels found MP unpleasant
Adapted from Volkow et al., Am. J. Psychiatry, 1999.
used to be
March 23, 2010 13

Circuits Involved In Drug Abuse and Addiction
All of these must be consideredAll of these must be considered
March 23, 2010 14
All of these must be consideredin developing strategies to effectively treat addiction
All of these must be consideredin developing strategies to effectively treat addiction
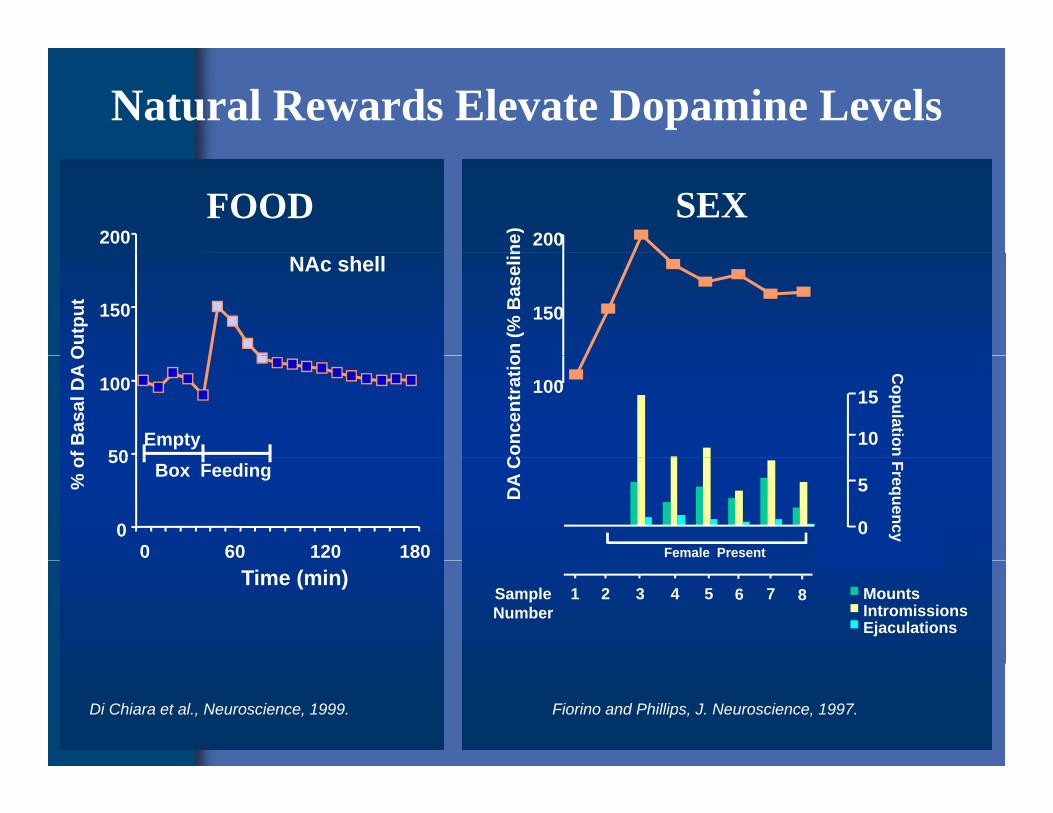
Natural Rewards Elevate Dopamine Levels
200FOOD
200ne)
SEX
150
Out
put
NAc shell
150
on (%
Bas
elin
50
100
of B
asal
DA
O
Empty
100
Con
cent
ratio
15
10
Copulation
0
50
0 60 120 180
% o Box Feeding
DA
C0
5
Frequency
Female PresentMarch 23, 2010March 23, 2010Time (min)
MountsIntromissionsEjaculations
SampleNumber
1 2 3 4 5 6 7 8
Di Chiara et al., Neuroscience, 1999. Fiorino and Phillips, J. Neuroscience, 1997.
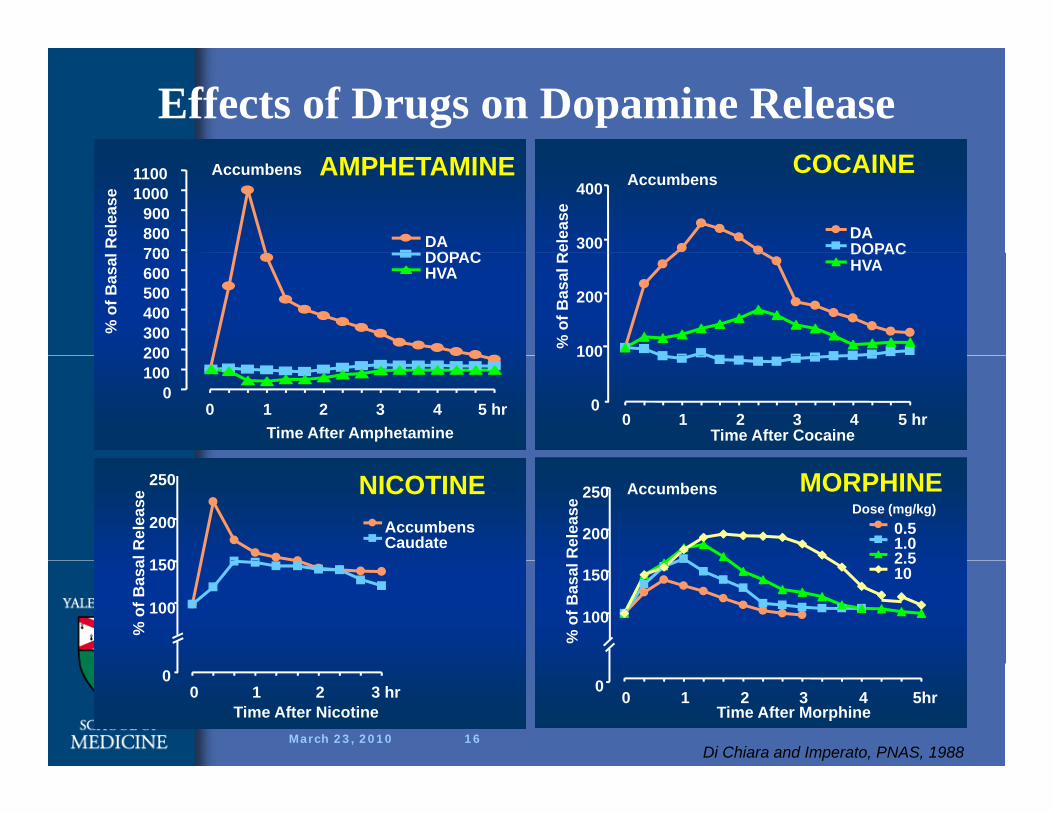
Effects of Drugs on Dopamine Release
700800900
10001100
Rel
ease
DADOPAC
Accumbens AMPHETAMINE
300
400
Rel
ease
DADOPAC
AccumbensCOCAINE
200300400500600700
% o
f Bas
al DOPAC
HVA
100
200
% o
f Bas
al R
DOPACHVA
0100200
0 1 2 3 4 5 hrTime After Amphetamine
0
100
0 1 2 3 4 5 hrTime After Cocaine
200
250
Rel
ease
Accumbens
0.51.02 5
Dose (mg/kg)MORPHINE
150
200
250
al R
elea
se
AccumbensCaudate
NICOTINE
100
150%
of B
asal
2.510
100
150
% o
f Bas
a
March 23, 2010 16
00 1 2 3 4 5hr
Time After Morphine
00 1 2 3 hr
Time After Nicotine
Di Chiara and Imperato, PNAS, 1988
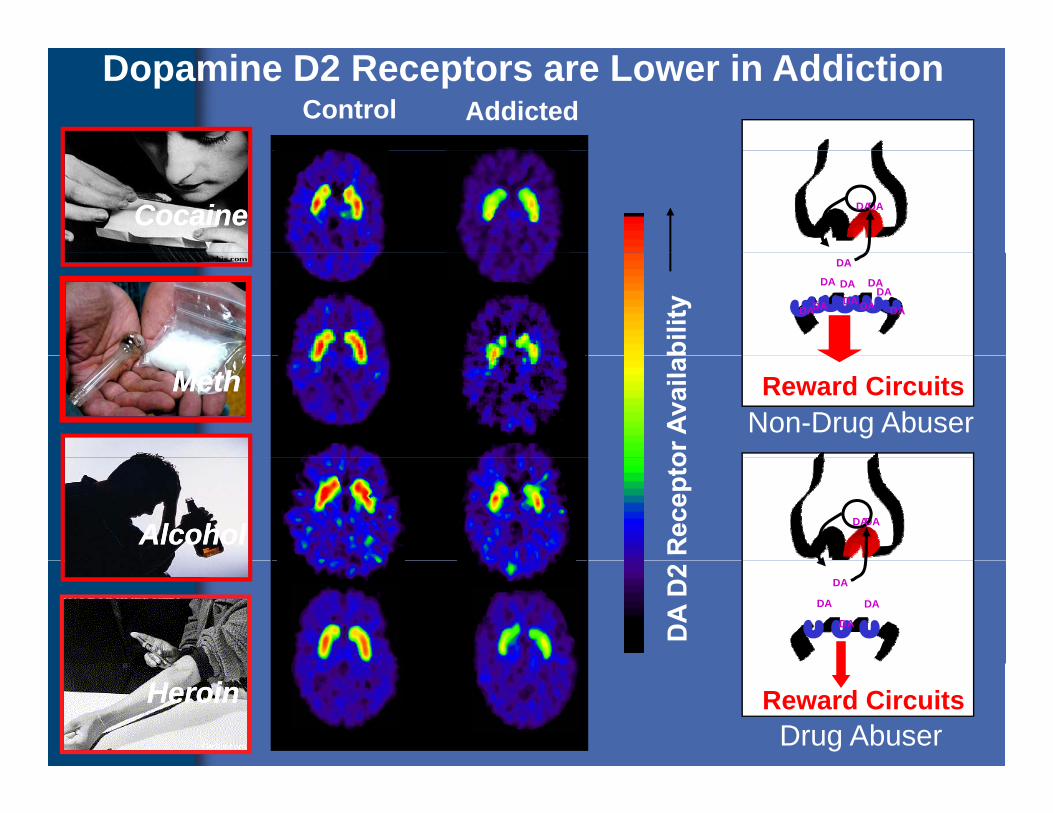
Control AddictedDopamine D2 Receptors are Lower in Addiction
CocaineCocaine DADA
DA
DA DADA
DADA DADA
DA DA
Reward CircuitsNon-Drug Abuser
MethMeth
AlcoholAlcohol DADA
DA
DA
DA DA
March 23, 2010 17
Reward CircuitsDrug Abuser
HeroinHeroin

Drugs Are Usurping Drugs Are Usurping Brain CircuitsBrain Circuits
and and Motivational Motivational PrioritiesPrioritiesPriorities Priorities
March 23, 2010 18

Addiction Changes Brain Circuits
Non-Addicted Brain Addicted Brain
Control Control
DriveSaliency NOT Drive GOSaliency DriveSaliencyGO
MMemory Memory
March 23, 2010 19
Source: Adapted from Volkow et al., Neuropharmacology, 2004.
This is why addicts can’t just quit
This is why treatment is essentialThis is why treatment is essential
March 23, 2010 20

Treatment for Addiction Includes:
1. Pharmacological (medications)2 Behavioral Therapies2. Behavioral Therapies3. Medical treatment for the
complications of addiction (e.g., HIV, HCV therapy), py)
4. Social Services
March 23, 2010 21

Pharmacology in Primary Care: Pharmacology in Primary Care: Opioids = buprenorphineOpioids = buprenorphine
March 23, 2010March 23, 2010

HeroinHeroin
Heroin is a short-acting, semisynthetic opioid produced from opium that can be smoked, sniffed, or injected
Heroin euphoria begins shortly after injection and lasts ~ 1 hour, followed by 1-4 hours of sedation; withdrawal symptoms or cra ing begin se eral ho rs lateror craving begin several hours later.
Most heroin dependent individuals inject 2-4 times per day. M di t d ti ff t b i j ti ll t fMany mediate sedating effects by injecting a small amount of cocaine, if available (not in Russia or Asia), known as a "speedball." Sometimes crack is smoked as a substitute.
Unsterile use, unpredictable concentrations in street samples, adulterants in injection mixture, lifestyle necessary to procure [].
March 23, 2010 23
drugs are responsible for most heroin-associated medical complications.
Bi di
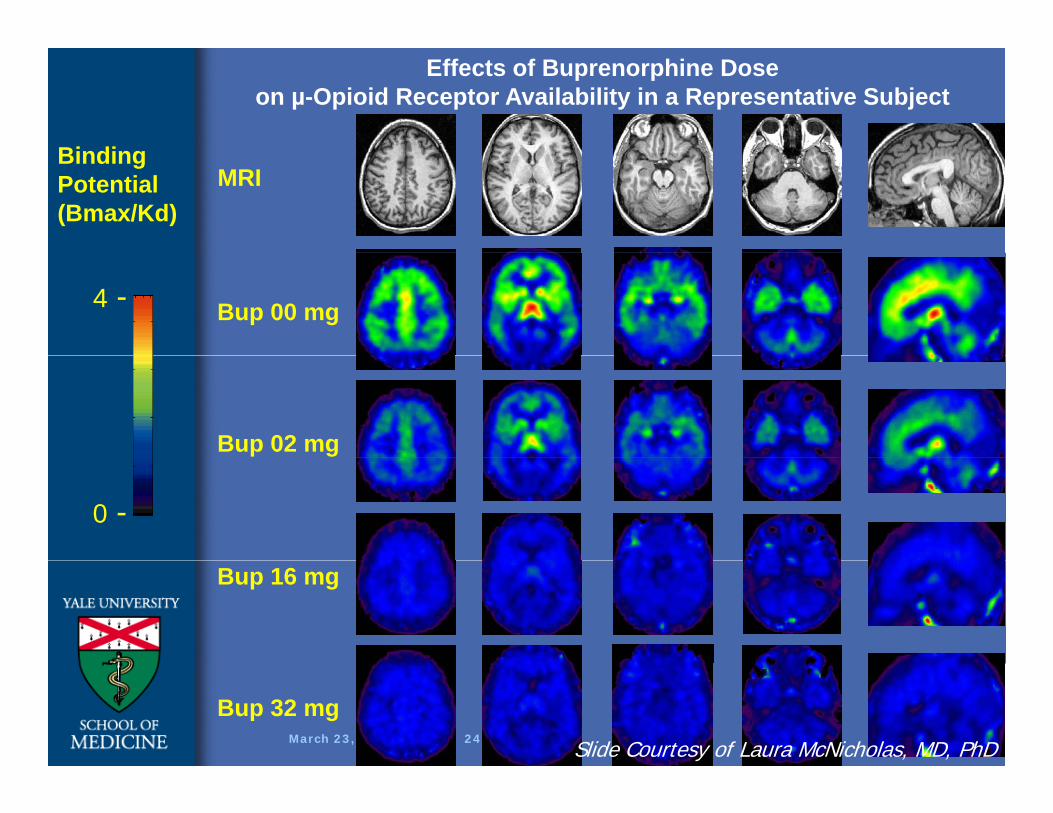
Effects of Buprenorphine Dose on µ-Opioid Receptor Availability in a Representative Subject
MRIBindingPotential(Bmax/Kd)
Bup 00 mg4 -
Bup 02 mg
0 -
Bup 16 mg
March 23, 2010 24
Bup 32 mgSlide Courtesy of Laura McNicholas, MD, PhD
Medication Assisted Treatment -OpioidsMedication Assisted Treatment -OpioidsOpioidsOpioids
• Rationale
– Cross-tolerance
• Rationale
– Cross-tolerance
• prevent withdrawal
• relieve craving for opioids– Narcotic blockade
• prevent withdrawal
• relieve craving for opioids– Narcotic blockade
• block or attenuate euphoric effect of exogenous opioids
• Pharmacotherapy
• block or attenuate euphoric effect of exogenous opioids
• Pharmacotherapy Pharmacotherapy
– Buprenorphine
– MethadoneLAAM
Pharmacotherapy
– Buprenorphine
– MethadoneLAAM– LAAM
– Naltrexone– LAAM– Naltrexone
March 23, 2010 25
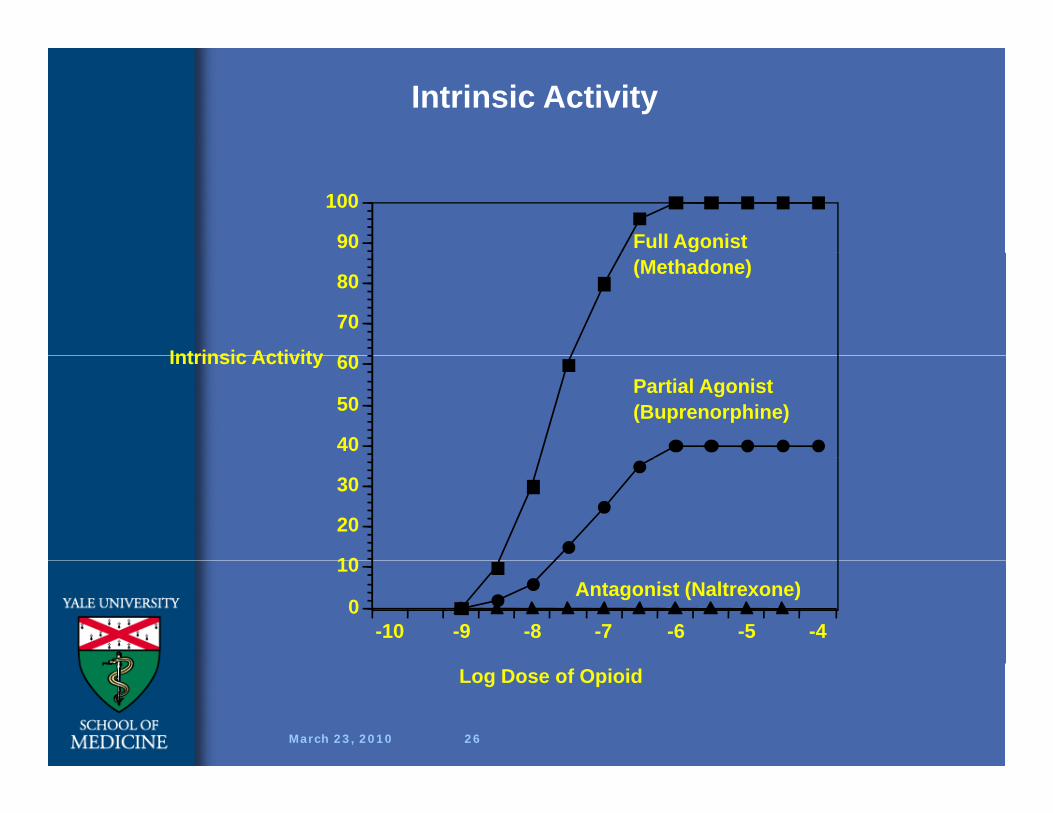
Intrinsic Activity
90
100
Full Agonist
60
70
80
Intrinsic Activity
(Methadone)
40
50
60Intrinsic ActivityPartial Agonist(Buprenorphine)
10
20
30
-10 -9 -8 -7 -6 -5 -40
10Antagonist (Naltrexone)
March 23, 2010 26
Log Dose of Opioid

Buprenorphine, Methadone, LAAM: T t t R t tiBuprenorphine, Methadone, LAAM: T t t R t tiTreatment RetentionTreatment Retention
100
ned 80 73% Hi Meth
nt R
etai
40
60 58% Bup
53% LAAM
Per
cen
20
40 53% LAAM
01 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17
20% Lo Meth
March 23, 2010 27
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17Study Week

Buprenorphine, Methadone, LAAM:Opioid Urine ResultsBuprenorphine, Methadone, LAAM:Opioid Urine Results
All Subjects80
100at
ive
Bup
LAAM
60
80
49%
% N
ega Bup
Hi Meth
40
6040%
%
Mea
n Lo Meth
2019%
39%
1 3 5 7 9 11 13 15 170
19%
March 23, 2010 28
Study Week1 3 5 7 9 11 13 15 17
BuprenorphineBuprenorphine
• Every physician treating HIV-infected drug users should have an X waiver and
• Every physician treating HIV-infected drug users should have an X waiver and drug users should have an X waiver and be ready to prescribe.
• The 1 2 3 of BUP:
drug users should have an X waiver and be ready to prescribe.
• The 1 2 3 of BUP:• The 1, 2, 3 of BUP:
– 1. It is easier than HIV/HCV treatment.
2 It is safer than prescribing oxycodone for
• The 1, 2, 3 of BUP:
– 1. It is easier than HIV/HCV treatment.
2 It is safer than prescribing oxycodone for– 2. It is safer than prescribing oxycodone for pain or alprazolam for anxiety.
– 3 It is desperately needed to expand access to
– 2. It is safer than prescribing oxycodone for pain or alprazolam for anxiety.
– 3 It is desperately needed to expand access to3. It is desperately needed to expand access to treatment.3. It is desperately needed to expand access to treatment.
3/23/2010 29
Pharmacology in Primary Care : Pharmacology in Primary Care : Cocaine = DisulfiramCocaine = Disulfiram
March 23, 2010March 23, 2010
CocaineCocaineC i h d hl id i l bl l hi h i i j dCocaine hydrochloride is a water-soluble salt which is injected
or taken by nasal inhalation, “snorted”.
Although cocaine hydrochloride is destroyed by heat it mayAlthough cocaine hydrochloride is destroyed by heat, it may be chemically converted to a free-base ("crack") cocaine, which can be smoked. Pulmonary absorption of “crack” is as rapid as IV injectionrapid as IV injection.
Cocaine’s half-life is short, resulting in the need for frequent administration; active cocaine users may inject or inhale ; y jcocaine as many as 20 times a day.
Cocaine induces feelings of elation, omnipotence and i i ibili d i h l il b h i d id d linvincibility and with volatile behavior and rapid development of dependence.
Cocaine use is associated with high risk sexual behavior
March 23, 2010 31
Cocaine use is associated with high risk sexual behavior.
Site of Cocaine BindingSite of Cocaine Binding
March 23, 2010 32

DisulfiramDisulfiram
• Increases dopamine in the brain by inhibiting dopamine beta hydroxylase
• Increases dopamine in the brain by inhibiting dopamine beta hydroxylaseinhibiting dopamine beta hydroxylase.
• 6 RCTs have demonstrated efficacy in treating cocaine dependence
inhibiting dopamine beta hydroxylase.
• 6 RCTs have demonstrated efficacy in treating cocaine dependencetreating cocaine dependence.
• Dosage: 250 mg/day
• No studies in HIV/HCV populations so
treating cocaine dependence.
• Dosage: 250 mg/day
• No studies in HIV/HCV populations so • No studies in HIV/HCV populations so need to watch AST/ALT
• Problem remains adherence Works well
• No studies in HIV/HCV populations so need to watch AST/ALT
• Problem remains adherence Works well • Problem remains adherence. Works well with the motivated patient or the patient who is administered it with methadone.
• Problem remains adherence. Works well with the motivated patient or the patient who is administered it with methadone.
3/23/2010 33

Pharmacology in Primary Care : Pharmacology in Primary Care : Methamphetamine = BuproprionMethamphetamine = Buproprion
March 23, 2010March 23, 2010

Methamphetamine (MA)Methamphetamine (MA)• MA is a psychostimulant similar in chemical
structure to amphetamine with more profound effects on the CNS and can be smoked snorted
• MA is a psychostimulant similar in chemical structure to amphetamine with more profound effects on the CNS and can be smoked snortedeffects on the CNS and can be smoked, snorted, injected, or administered rectally.
• Produces stimulation and feelings of euphoria d h l d ti f ti (6 t 8 h
effects on the CNS and can be smoked, snorted, injected, or administered rectally.
• Produces stimulation and feelings of euphoria d h l d ti f ti (6 t 8 hand has a long duration of action (6 to 8 hours
after a single dose)• Tolerance develops rapidly and escalation of
d d f i i d
and has a long duration of action (6 to 8 hours after a single dose)
• Tolerance develops rapidly and escalation of d d f i i ddose and frequency is required.
• As with cocaine, MA use is associated with high risk sexual behavior (especially in MSM)
dose and frequency is required.• As with cocaine, MA use is associated with
high risk sexual behavior (especially in MSM)g ( p y )• Neurocognitive effects of MA use worse in
HIV positive patients..
g ( p y )• Neurocognitive effects of MA use worse in
HIV positive patients..
March 23, 2010 35
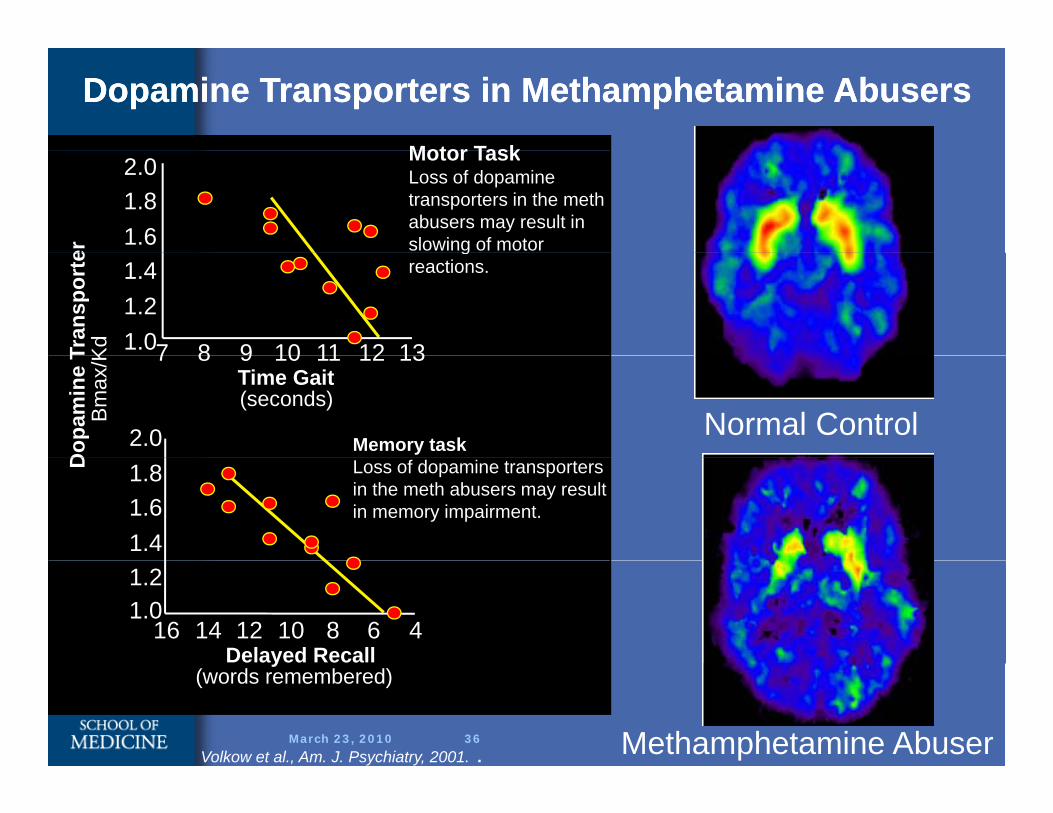
Dopamine Transporters in Methamphetamine AbusersDopamine Transporters in Methamphetamine AbusersMotor TaskMotor TaskLoss of dopamine transporters in the meth abusers may result in slowing of motor 1.6
1.82.0
er greactions.
7 8 9 10 11 12 131.01.21.4
Tran
spor
teK
d
Normal ControlMemory task
7 8 9 10 11 12 13Time Gait(seconds)
2.0
Dop
amin
e T
Bm
ax/K
Loss of dopamine transporters in the meth abusers may result in memory impairment.
1.41.61.8D
468101214161.01.2
Delayed Recall
March 23, 2010 36 Methamphetamine Abuser
y(words remembered)
Volkow et al., Am. J. Psychiatry, 2001. .

TreatmentsTreatments
• Bupropion 150 mg twice daily has shown some reduction in use among mild
• Bupropion 150 mg twice daily has shown some reduction in use among mild some reduction in use among mild methamphetamine users (Shoptaw DAD 2008)
some reduction in use among mild methamphetamine users (Shoptaw DAD 2008))
• Counseling remains the mainstay
)
• Counseling remains the mainstay
3/23/2010 37
Pharmacology in Primary Care: Pharmacology in Primary Care: Alcohol = NaltrexoneAlcohol = Naltrexone
March 23, 2010March 23, 2010

Alcohol Main PointsAlcohol Main Points
• Disinhibition that leads to increased risk taking behaviors and poor adherence to all
• Disinhibition that leads to increased risk taking behaviors and poor adherence to alltaking behaviors and poor adherence to all treatmentsWithd l i
taking behaviors and poor adherence to all treatmentsWithd l i• Withdrawal seizures
• The drug that really is frightening because it i i d l HCV di
• Withdrawal seizures• The drug that really is frightening because it
i i d l HCV diis neurotoxic and accelerates HCV disease progressionis neurotoxic and accelerates HCV disease progression
• CAGE Questions• CAGE Questions
March 23, 2010 39

ETOH TreatmentETOH Treatment• Naltrexone –
– FDA approved and standard of care
• Naltrexone –
– FDA approved and standard of carepp
– Watch for hepatotoxicity (black box warning)
pp
– Watch for hepatotoxicity (black box warning)g)
– Dosages: 100 mg per day (based on COMBINE study)
g)
– Dosages: 100 mg per day (based on COMBINE study)y)
• Acamprosate
– FDA approved, but inferior to naltrexone
y)
• Acamprosate
– FDA approved, but inferior to naltrexonepp ,
• Disulfiram
– FDA approved, but inferior to naltrexone
pp ,
• Disulfiram
– FDA approved, but inferior to naltrexoneFDA approved, but inferior to naltrexoneFDA approved, but inferior to naltrexone
3/23/2010 40
TopiramateTopiramate
• Not FDA approved for ETOH dependence
• 8 papers showing efficacy of topiramate
• Not FDA approved for ETOH dependence
• 8 papers showing efficacy of topiramate • 8 papers showing efficacy of topiramate for ETOH dependence
• Doses varied by trial but typically
• 8 papers showing efficacy of topiramate for ETOH dependence
• Doses varied by trial but typically • Doses varied by trial, but typically patients were started low (25 mg daily) and titrated up to a max of 300 mg over
• Doses varied by trial, but typically patients were started low (25 mg daily) and titrated up to a max of 300 mg over and titrated up to a max of 300 mg over 6 weeks.
• Important choice because:
and titrated up to a max of 300 mg over 6 weeks.
• Important choice because:p
1.Can give to patients on opioids
2.Moderates symptoms of withdrawal
p
1.Can give to patients on opioids
2.Moderates symptoms of withdrawal2.Moderates symptoms of withdrawal2.Moderates symptoms of withdrawal
3/23/2010 41
Pharmacology in Primary Care:Pharmacology in Primary Care:Nicotine = NicotineNicotine = Nicotine
3/23/20103/23/2010
42
The 5 A’sThe 5 A’s
• Ask about tobacco use
• Advise smokers to quit
• Ask about tobacco use
• Advise smokers to quit• Advise smokers to quit
• Assess willingness to quit
A i t ith itti
• Advise smokers to quit
• Assess willingness to quit
A i t ith itti• Assist with quitting
• Arrange follow-up
• Assist with quitting
• Arrange follow-up
• Brief advice to quit does make a difference!
• Brief advice to quit does make a difference!
3/23/2010 43

PharmacotherapyPharmacotherapy
• Nicotine replacement helps
• Buproprion doubles quit rates (but is
• Nicotine replacement helps
• Buproprion doubles quit rates (but is • Buproprion doubles quit rates (but is metabolized by CYP 2B6 so possible interactions with NFV RTV and EFV)
• Buproprion doubles quit rates (but is metabolized by CYP 2B6 so possible interactions with NFV RTV and EFV) interactions with NFV, RTV, and EFV). Doses 150 mg to 300 mg effective.
• Varenicline – better than buproprion and
interactions with NFV, RTV, and EFV). Doses 150 mg to 300 mg effective.
• Varenicline – better than buproprion and Varenicline better than buproprion and nicotine in comparison trials – watch for suicidality and exacerbation of
Varenicline better than buproprion and nicotine in comparison trials – watch for suicidality and exacerbation of neuropsychiatric symptoms. Slow upward titration to minimize side effects.neuropsychiatric symptoms. Slow upward titration to minimize side effects.
3/23/2010 44

Continuum of InterventionsContinuum of Interventions
Knowing the PiecesKnowing the Pieces
March 23, 2010March 23, 2010
Range of TreatmentsRange of Treatments
• Risk (Harm) ReductionDecrease frequency of adverse events related to
• Risk (Harm) ReductionDecrease frequency of adverse events related to– Decrease frequency of adverse events related to a behavior
– Change in use behavior – e g Changing from
– Decrease frequency of adverse events related to a behavior
– Change in use behavior – e g Changing fromChange in use behavior e.g., Changing from injection use to sniffing
• Risk (Harm) Removal
Change in use behavior e.g., Changing from injection use to sniffing
• Risk (Harm) Removal( )– Cessation of substance abuse– Abstinence based – 12 Steps
( )– Cessation of substance abuse– Abstinence based – 12 Stepsp– Agonist based – buprenorphine, methadone
p– Agonist based – buprenorphine, methadone
March 23, 2010 46
Harm reduction is critical because drug addiction is a chronic illness with relapse rates i il t th f h t i di b t d
Harm reduction is critical because drug addiction is a chronic illness with relapse rates i il t th f h t i di b t dsimilar to those of hypertension, diabetes, and
asthmasimilar to those of hypertension, diabetes, and asthma
March 23, 2010 47
McLellan et al., JAMA, 2000.

Relapse Rates Are Similar for Drug p gAddiction & Other Chronic Illnesses
100
708090
Rel
apse
506070
ient
s Who
203040
to 6
0%to
60%
to 5
0%to
50%
to 7
0%to
70%
to 7
0%to
70%
ent o
f Pat
i
Drug Type I0
1020
Hypertension Asthma
40 t
40 t
30 t
30 t
50
50
50
50
Perc
March 23, 2010 48
gAddiction
Type I Diabetes
Hypertension Asthma
McLellan et al., JAMA, 2000.

DAT R
[C-11]d-threo-methylphenidate
DAT Recoverywith prolongedb ti fabstinence from
methamphetamine high
Normal Control
lowMethamphetamine Abuser
(1 month detoxification)There is hope!!
March 23, 2010 49 Volkow et al., J. Neuroscience, 2001.
Methamphetamine Abuser (14 month abstinent)
