medical interporous tm tablets: effectiveness in clinical ... study 1.pdf · stomatitis. the...
TRANSCRIPT
1
MEDICAL INTERPOROUSTM tablets: effectiveness in
clinical and microbial control of the denture biofilm.
Silva-Lovato1, CH; De Wever, B2; Paranhos, HFO1, Watanabe, E1; Pisani, MX1;
Souza, RF1 and Ito, IY.
1: Department of Dental Materials and Prostodontics, School of Dentistry,
University of Sao Paulo, Brazil.
2: MSI Laboratories AG, Vaduz, Liechtenstein.
Publication in preparation

2
INTRODUCTION
Denture-induced stomatitis (atrophic chronic candidiasis) is an inflammatory
lesion of the denture bearing mucosa that affects approximately 50% of patients
wearing complete maxillary dentures (Wilson, 1998) and has a multifactor
aetiology. Factors of particular significance are trauma caused by the denture itself,
infection by Candida, poor denture hygiene, continuous denture wear, and dietary
and systemic factors, including suppressed immuno-competence (Lombardi;
Bustz-Jorgensen, 1992; Webb et al., 1998). Especially elderly people wearing
dentures or patients with metabolic diseases such as diabetics, organ transplant
patients, cancer patients or patients on chronic anti-biotic treatment have an
increased risk for developing oral candidiasis (Kulak-Ozkan et al., 2002).
The presence of denture biofilm is an important etiologic factor for this
disease. Biofilm found on dentures consists of a complex mixture of fungi and
bacteria and desquamated epithelial cells (Radford and Radford 1993). These
biofims act as a protective reservoir for oral micro-organisms and C. albicans and
other species of yeast found in biofilm have been reported as important agents for
the installation, maintenance and exacerbation of denture stomatitis. Scanning
electron microscopic evaluation of dentures retrieved from patients suffering from
denture stomatitis demonstrates that Candida biofilm not only colonizes the surface
but also penetrate the cracks and imperfections of the denture material (Ramage et
al., 2004).
3
In addition to Candida species, also other pathogenic and opportunistic
micro-organisms have been isolated from patient’s dentures which include
staphylococcus species, streptococcus and Pseudomonas species (Glass et al.,
2001). Moreover, the colonization of oral surfaces, including denture-seating
surfaces, could serve as a reservoir for disseminated infections, such as
gastrointestinal infections (Green, 1979; Martin et al., 1994; Nikawa et al., 1998).
Even respiratory pathogens that are uncommon in the oral flora have been isolated
from dentures, including Escherichia Coli, Klebsiella, MRSA or methicillin resistant
st. aureus and Enterobacteria (Rossy et al., 1995; Senpuku et al. 2003; Sumi et al.
2002). For the above described reasons, adequate removal of pathogenic biofilm
should be recommended as a routine practice.
The efficacy of several denture cleansers has been clinically evaluated.
Commercial denture cleansing products are generally not very efficient in denture
biofilm control. In addition some of these cleansers are either corrosive or change
the colour or hardness of the polymer after repeated use (Keyf et al., 2003; Garcia
et al., 2004; Webb et al., 2005). The ideal denture maintenance product must be
effective in the removal of organic and inorganic deposits, have antibacterial and
antifungal biofilm removal properties, be non-toxic to humans, compatible with the
denture materials including metals, easy to handle and also have a low cost
(Nikawa et al., 1999). The aim of this study was to evaluate the clinical
effectiveness of a novel disinfecting cleaning tablet called Medical InterporousTM for
complete denture cleansing, in terms of denture biofilm removal, in denture
wearing patients.
4
MATERIALS AND METHODS
This study was conducted with 40 complete denture wearers (14 men and
26 women) with a mean age of 62.3 ± 9.0 years (range: 45 to 70 years). Dentures
were inserted at least 1 year (mean 5.5 ± 4.8 years) prior to the study and were
made from heat-polymerized acrylic resin. All participants presented adequate
general health conditions. This research project was approved by the institutional
Ethics Committee. Patients were informed of the nature of the investigation, and
written informed consent was obtained prior to enrolment.
Exclusion criteria were: time of denture use less than a year and absence of
biofilm on internal surface of upper dentures during the first examination. This
assessment was conducted by the Additive Index of Ambjørnsen et al. (19). Only
subjects wearing upper complete dentures with scores of “1” or greater were
selected. In other words, a zero in one or more areas of the Index precluded
inclusion.
Volunteers were instructed to clean their dentures according to two
methods:
1) Control: brushing 3 times a day using a Denture brush (Denture - Condor S.A.,
Santa Catarina, Brazil) and tap water following meals (breakfast, lunch and dinner);
2) Experimental: brushing the denture using a Denture brush (Denture - Condor
S.A., Santa Catarina, Brazil) and tap water following meals (breakfast, lunch and
dinner) and treating the denture with Medical InterporousTM Dentures tablets (MSI
Laboratories AG, Vaduz, Liechtenstein), by immersing the denture into 150 ml of
5
lukewarm water and consequently adding one tablet. The denture was then
allowed to soak in the solution for at least 15 minutes. After treatment, the denture
was removed from the solution and rinsed vigorously under running water before
replacing back in the mouth.
The 40 patients had been randomly distributed to each group and received
verbal information and practical demonstration of both control and experimental
techniques. After participants had received their denture maintenance instructions
and hygiene materials, the disclosure of the internal surface of maxillary denture of
each participating denture wearer was assessed using a 1% neutral red solution
(Paranhos et al, 2007). The disclosed dentures were consequently brushed until
complete removal of disclosed biofilm (biofilm free). For evaluation of the
effectiveness in the removal of biofilm, after 21 days of the use of both denture
maintenance methods (control and experimental), the internal surfaces of upper
dentures were disclosed by 1% neutral red solution. The surfaces were then
photographed (digital camera: Canon EOS Digital Rebel EF-S 18-55; and flash:
Canon MR-14 EX, Canon Inc., Tokyo, Japan) with standard film-object distance
and exposure time. The camera was fixed on a stand (CS-4 Copy Stand, Testrite
Inst. Co., Inc., Newark, NJ, USA). After quantification, biofilm was eliminated by
brushing with a specific brush for complete dentures (Denture - Condor S.A., Santa
Catarina, Brazil) and liquid soap (JOB Química, Produtos para limpeza Ltda.,
Monte Alto, SP, Brazil).
Photos were transferred to a computer and the total surface area and areas
corresponding to the stained region were measured using image processing
software (Image Tool 2.02) (Fig. 1). Biofilm percentage was calculated using the
6
relation between biofilm area multiplied by 100, and total surface area of the
denture’s internal base.
The influence of the treatments on the denture biofilm percentage was
assessed with an independent sample t-test. The homogeneity of the variances
was tested with a Levene’s test and normality of the residuals was tested with a
Shapiro-Wilk test (SW). A significance level of p < 0.05 was used. The data were
transformed to their square root to meet the assumptions. In the tables the back-
transformed mean values together with their 95% confidence interval are shown.

7
RESULTS
Table 1 and Figure 1 show the biofilm percentage in the internal surface of
the upper complete denture after the use of the Control method and after the use
of the Medical InterporousTM Dentures tablet (Treatment). The percentage was
obtained from the measurement of the total and disclosed area with biofilm.
Table 1: Total amount of denture biofilm presence (as percentage of total denture
surface area) in the control group (Control) and after treatment (Treatment) with
Medical InterporousTM Dentures tablet (mean ± SD, n=20)
Group Biofilm (%)
Mean 95% CI
Control 37.5 28.2 to 48.1
Treatment 4.7 2.4 to 7.9
The data were transformed to their square root prior to the analysis to obtain
homogeneity of the variances (F1, 38= 1.797, p=0.188) and normality of the
residuals (SW40=0.946, p=0.056). An independent t-test revealed a significant
lower biofilm percentage for the treatment group (2.18 ± 1.36) in comparison with
the control group (mean 37.5, 95% CI 28.2 to 48.1) (t38=7.996, p < 0.001).

8
Figure 1: Denture wearing patients were scored for bio-film presence (red staining)
before (left) and after 21 days of Medical InterporousTM treatment (right). Note the
almost complete reduction of biofilm on the treated dentures.
Before After
Before After
Before After
9
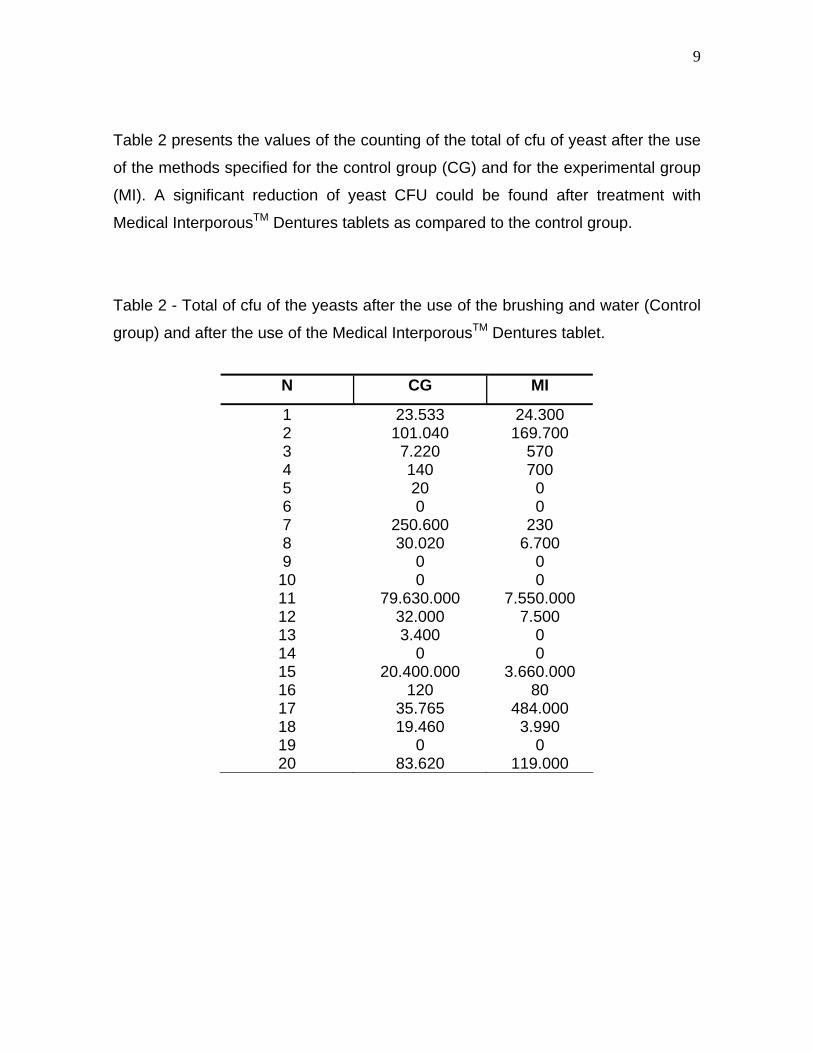
Table 2 presents the values of the counting of the total of cfu of yeast after the use
of the methods specified for the control group (CG) and for the experimental group
(MI). A significant reduction of yeast CFU could be found after treatment with
Medical InterporousTM Dentures tablets as compared to the control group.
Table 2 - Total of cfu of the yeasts after the use of the brushing and water (Control
group) and after the use of the Medical InterporousTM Dentures tablet.
N CG MI
1 23.533 24.300 2 101.040 169.700 3 7.220 570 4 140 700 5 20 0 6 0 0 7 250.600 230 8 30.020 6.700 9 0 0 10 0 0 11 79.630.000 7.550.000 12 32.000 7.500 13 3.400 0 14 0 0 15 20.400.000 3.660.000 16 120 80 17 35.765 484.000 18 19.460 3.990 19 0 0 20 83.620 119.000

10

11
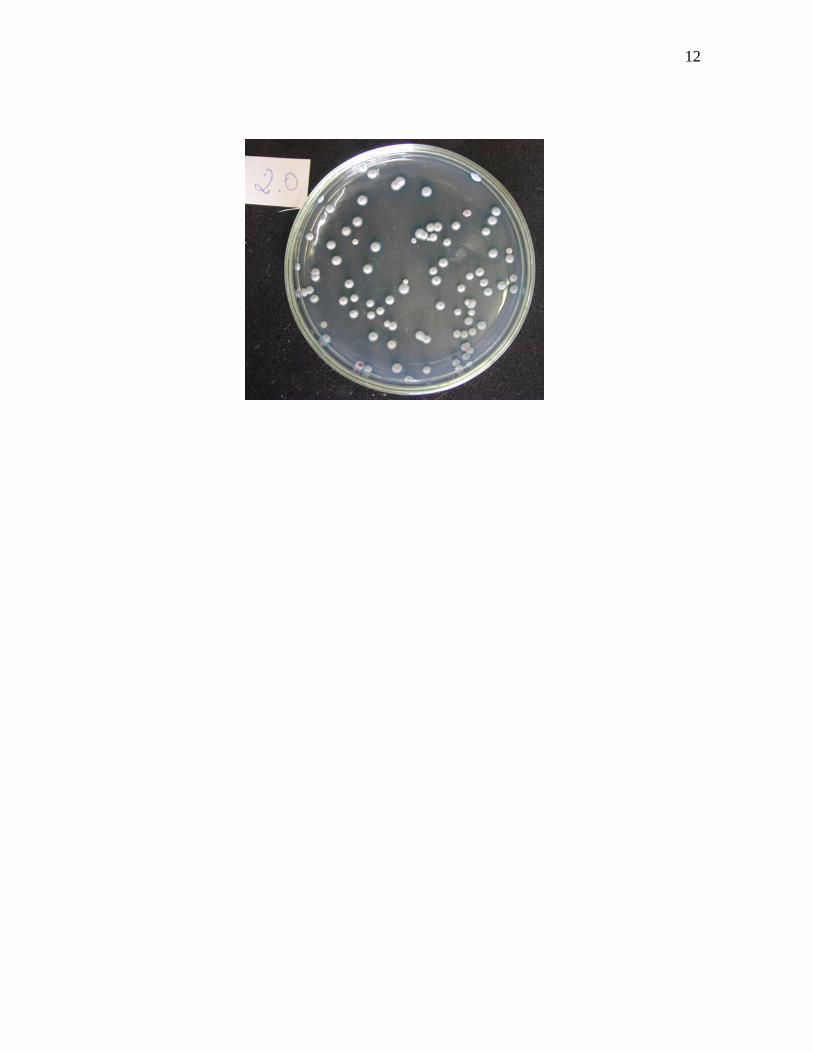
The Figures 1 a 3 show the morphology of the cfu’s of yeast (Candida Albicans)
developed in CHROMagar®
12
13
DISCUSSION
The study of oral hygiene in elderly denture wearers is becoming increasingly
important because of the increasing numbers of elderly people in the world. Today
approximately 600 million people are aged over 60 years, and this number is
estimated to double by 2025, 80% of which live in developing countries. In Brazil,
by 2050 over 100 million people will be old-aged (Petersen et al, 2005). Denture
stomatitis is a common clinical pathology observed in elderly populations. Microbial
plaque on the fitting surface of the denture is one of the principal causes of denture
stomatitis. The correlation between poor denture cleanliness and denture stomatitis
is statistically significant according to Kulak-Ozkan et al., 2002. Removal of the
denture plaque by means of good denture hygiene is important in the prevention of
the denture stomatitis, in aesthetic aspects and in the maintenance of a healthy
mucosa (Arendorf & Walker, 1987). Efficient plaque control by mechanical or
chemical denture cleansing has produced significant resolution of this oral disease
(Berge, Silness & Sorheim, 1987), however the incidence of denture stomatitis is
still significant affecting 11-67% of denture wearers (Jeganathan et al, 1992) and
recent studies indicate that 1 in 3 removable denture wearers in the United States
suffers from denture stomatitis (Shulman et al, 2005).
A variety of chemical denture cleansing products are commercially available.
These type denture cleansers can be divided into five groups: alkaline peroxides,
alkaline hypochlorite, diluted organic and inorganic acids, disinfectants and
enzymes (Butdtz-Jorgensen, 1979; Moore et al., 1984). While chemical plaque
control is a useful and appropriate procedure, such treatment should always be
accompanied by mechanical control of plaque in the fitting surface of the denture

14
(Paranhos et al., 2007; Chan et al, 1991; Cobargas et al., 1997; Lee et al, 1985),
and brushing the fitting surface of the prosthesis should be indicated as essential
technique of hygiene, at least for patients with motors disabilities. Because of this
evidence, the association of both methods was used in this present study in the
experimental group (brushing and immersion in Medical InterporousTM for 15
minutes).
Dentures are made of poly-methyl metacrylate (PMMA) and all of them become
quickly colonized by various micro-organisms once they are being placed in the
mouth. These micro-organisms, including bacteria, fungi and viruses initially
adhere to the surface of the denture material and subsequently penetrate into the
dentures via a complex of pores and tracks formed by the release of gases during
the construction polymerization process (Chau et al., 1995; Lin et al., 1999). In
another study, Jeganathan et al., in 1997 suggested that the increasing occurrence
of stomatitis in some of the analyzed prosthesis wearing patients may be related to
the age of the denture: the denture may become traumatic because of old age and
the surface may have altered porosities that make it more difficult to keep clean.
This may partially explain the varying number of CFUs of Candida albicans in the
experimental group in this present study.
The overall objective of immersing a denture in a cleaning maintenance solution is
to obtain a clean but also decontaminated prosthesis through the destruction of
micro-organisms by means of the chemical actions including the effervescency
properties of the cleanser. (Asad, Watkinson e Hugget, 1992). Its has been shown
previously that 24 hour accumulations can be removed moderately effectively after
15 minutes of immersion and completely with overnight soaking.(Hutchins-Parker,
15
1973). In this present study the percentage of biofilm in the experimental group has
diminished substantially (from 37.5% to 4.7%) in comparison to the control group
after 15 minutes of immersion in Medical InterporousTM. Hence, regular overnight
soaking in this product may increase the antimicrobial potential even further, clean
the denture completely and leave polished and shiny surfaces. According to Shay
et al., 2000, some cleansers were more effective when used overnight.
In addition to the usual instructions in oral hygiene that should be given to patients
wearing prosthesis, the use of disclosing solutions to identify plaque accumulations
was demonstrated. Since mature plaque is much more resistant to removal than
the 24 hour plaque (Hutchins-Parker, 1973.), the quantification of the plaque can
be regarded as a good outcome measurement for denture hygiene. The use of
neutral red solution is justified by its high affinity to oral biofilms and the ease of
removal. (Silva C.H. et al., 2002) In addition, photography (Ambjorsen E. et al.,
1984) combined with quantitative analysis (Paranhos H.F.O. et al., 2004) was
employed to standardize an objective evaluation method. A limitation of most
biofilm measurement techniques, including the present method is the two
dimensional nature of the recording. The use of a disclosing method appears to
present no disadvantage when compared with the biofilm weight (MacCraken GI,
et al., 2006). Furthermore, biofilm staining is the most commonly used technique
for denture biofilm quantification (Nikawa, H. et al., 1999), and hence, provides a
more efficient method if data need to be compared with previous studies. The
analysis used in this study was based on the biofilm quantification of the internal
surface of the upper complete denture, in accordance with the studies of Paranhos
et al., 2007; Keng et al., 1996; Tarbet et al., 1984; Sheen et al., 2000; Mc Cabe et
16
al., 1996. This surface has greater potential for build-up of pathogenic micro-
organisms and the consequent development of denture stomatitis. As suggested
by Paranhos H.F.O., et al., 2007 we did not measure the external surface, since it
accumulated much less biofilm.
The ideal denture cleanser should be efficient in removal of organic and inorganic
depositions, non toxic, low cost, ease to use and reduce the amount of plaque,
stain and food of the dentures surface. We observed a significant difference
between the control group and the experimental group in reduction in Candida spp
however with some variability. This could be related to the variability in the number
of CFUs of Candida ssp, between the period of study and the subjects, as was
previously described by with Gornitsky et al., 2002.
Medical InterporousTM tablets contain NitrAdineTM, a disinfecting formula that
demonstrated high in vitro biofilm removal activity against a variety of micro-
organisms including Candida Albicans, Ps. Aeruginosa, st. aureus including the
MRSA type and viruses (Glass et al, 2003, Van de Vannet et al, 2007, De Prijck et
al 2007) The effectiveness of the Medical InterporousTM in reducing the biofilm
percentage may also be due to the presence of sodium lauryl sulfate (SLS) in its
formula, Moore T.C. et al., 1984, noticed that in a group of six cleansers alkaline
peroxide cleansers, only two of them had a superior performance against yeasts,
maybe because of the presence of SLS. SLS is a detergent used to solubilise
protein in microbiology laboratories.
Dills et al., 1988 showed that brushing combined with soaking treatment removed
significantly more organisms than brushing alone: the level of micro-organisms
recovered from the prosthesis were significantly lower, which confirms the results

17
from our current study. In this same study Dills affirms that the denture cleansers
tested were not selective in its antimicrobial action, and that denture cleanser soak
treatment displayed a broad spectrum activity in eliminating gram negative
anaerobic rods, gram positive facultative cocci, and gram negative anaerobic cocci.
These results support the need to use of a denture disinfectant in addition to
brushing the prosthesis for proper denture hygiene.
Since most elderly people do not know how to keep dentures clean, knowledge
about the efficacy of different denture maintenance protocols is of importance to
improve the quality of life of denture wearing patients (Paranhos H.F.O. et al.,
2007), but also the durability of the dentures. Medical InterporousTM tablets prove
to be very efficient in the elimination of biofilm from removable dentures in denture
patients. Additional studies are currently ongoing to address the physico-chemical
properties of the Medical InterporousTM as well as its mechanism of action in the
prevention of denture stomatitis symptoms.

18
CONCLUSION
Denture biofilm counts were higher for the control method, when compared with
the treatment based on denture brushing and the immersion in Medical
InterporousTM tablets. This present study suggests that these disinfecting cleaning
tablets are efficient in removal of denture biofilm, and should therefore be
recommended as a routine method for the prevention of the development of
microbial biofilm induced denture stomatitis.
ACKNOWLEDGEMENTS
We like to thank Dr. Els Adriaens for performing the statistical analysis of the data
and Dr. Bart Vande Vannet for critical review of the paper’s content.

19
References
1. Green SL. Anaerobic pleuro-pulmonary infections. Post Grad Med
1979;65:62-66.
2. Lombardi T, Budtz-Jørgensen E. Treatment of denture-induced stomatitis: a
review. Eur J Prosthodont Restor Dent 1993;2:17-22.
3. Martin BJ, Corlew MM, Wood H, Olson D, Golopol LA, Wingo M, Kirmani N.
The association of swallowing dysfunction and aspiration pneumonia. Dysphagia
1994;9:1-6.
4. Nikawa H, Hamada T, Yamamoto T. Denture plaque – past and recent
concerns. J Dent 1998;26:299-304.
5. Nikawa H, Hamada T, Yamashiro H, Kumagai H. A review of in vitro and in
vivo methods to evaluate the efficacy of denture cleansers. Int J Prosthod
1999;12:153-159.
6. Webb BC, Thomas CJ, Willcox MDP, Harty DWS, Knox KW. Candida-
associated denture stomatitis. Aetiology and management: A review. Part 2. Oral
diseases caused by Candida species. Aust Dent J 1998;43:160-166.
7. Wilson J. The aetiology, diagnosis and management of denture stomatitis.
Brit Dent J 1998;185:380-384.
8. Kulak-Ozkan Y, Kazazoglu E., Arikan A. Oral hygiene habits, denture
cleanliness, presence of yeast and stomatitis in elderly people. J. Oral Rehabilit.
2002; 29: 300-304.
9. Radford DR., Radford JR. A SEM study of denture plaque and oral mucosa
of denture related stomatitis. J. Dent 1993; 21:87-93.

20
10. Ramage G., Tomsett K., Wickles BL. Loez-Ribot JL. Denture stomatitis, a
role for Candida biofilms. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2004;
98: 53-59.
11. Glass T., Bullard J., Hadley C., Mix E., Conrad R. Partial spectrum of
microorganisms found in dentures and possible disease implications. JAOA 2001;
101:92-94.
12. Rossi T., Laine J., Eerola E., Kotilainen P., Pettonen R. Denture carriage of
methicillin resistant Staphylococcus aureus. The Lancet 1995; 345:1577.
13. Senpuku H., Sogame A., Inoshita E., Tsuha Y., Miyazaki H., Hanada N.
Systemic diseases in association with microbial species in oral biofilm from elderly
requiring care. Gerodontology 2003; 49: 301-309.
14. Sumi Y., Miura H., Sunakawa M., Michiwaka Y., Sakagami N. Colonization
of denture plaque by respiratory pathogens in dependent elderly. Gerondontology
2002; 19: 25-29.
15. Keyf F., Güngor T. Comparison of effects of bleach and cleansing tablet on
reflectance and surface changes of a dental alloy used for removable partial
dentures. J. Biomaterials Applications. 2003; 18: 5-14.
16. Garcia R., De Souza Junior J., Rached R., Del Bel Cury A. Effect of denture
cleansers on the surface roughness and hardness of a microwave-cured acrylic
resin and dental alloys. J. of Prosthodontics 2004; 13:3:173-178.
17. Webb B., Thomas C., Whittle T. A 2-year study of Candida-associated
denture stomatitis treatment in aged care subjects. Gerondontology 2005; 22: 168-
176.
21
18. Paranhos H, Da Silva C., Venezian G., Macedo L and De Souza R.
Distribution of biofilm on internal and external surfaces of upper complete dentures:
the effect of hygiene instruction. Gerodontology, 2007, 24, 3, 162-168.
19. Petersen P and Yamamoto T. Improving the oral health of older people:the
approach of the WHO oral health programme. Community Dent. Oral Epidemiol.,
2005, 33, 81-92.
20. Jeganathan S and Lin C. Denture stomatitis: a review of the aetiology,
diagnosis and management. Aust. Dent. J., 1992, 37, 107-114.
21. Shulman J, Rivera-Hidalgo F. and Beach M. One in 3 removable denture
users in the United States has denture stomatitis. J.Evid Based Dent Pract 2006, 6,
197-198.
22. Glass R., Bullard J., Conrad R., Blewet E. Evaluation of the sanitization
effectiveness of a denture-cleansing product on dentures contaminated with known
microbial flora. An in vitro Study. Quintessence Intl. 2004, 35, 3, 194-199.
23. Van de Vannet B., De Prijck K., Coenye T., Nelis H. Elimination of candida
albicans biofilms from removable orthodontic appliances. 2007, Poster presented
at the European Orthodontic Society, Berlin.
24. Coenye T., De Prijck K., De Wever B., Nelis H. Use of the modified Robbins
Device to study the in vitro biofilm removal efficacy of NitrAdine, a novel
disinfecting formula for the maintenance of oral medical devices. 2007, J. Applied
submitted for publication.
25. Butdtz-Jorgensen E. Materials and Methods for cleaning dentures. 1979, J.
Prosthet. Dent. 42, 6,: 619-623.
22
26. Lin J., Cameron S., Runyan D., Craft D. Disinfection of denture base acrylic
resin. 1999, J. Prosthet. Dent., 81, 2, 202-206.
27. Jeganathan S. Thean H., Thong K., Chan Y., Singh M. A clinically viable
index for quantifying denture plaque.1996, Quintes. Intl. 27, 8, 569-573.
28. Asad T., Watkinson A., Huggett R. The effect of disinfection procedures on
flexural properties of denture base acrylic resins. 1992, J. Prosthet. Dent. 68, 1,
191-195.
29. Hutchins D. and Parker W. A clinical evaluation of the ability of denture
cleaning solutions to remove dental plaque from prosthetic devices. 1973, NY
State Dent J. 39, 6, 363-367.
30. Shay K. Restorative considerations in the dental treatment of the older
patient. 2000, Gen Dent., 48, 5, 550-554.
31. Silva C., Paranhos H., Ito Y. Biofilm disclosing agents in compleate denture:
clinical and antimicrobial evaluation. 2002, Pesqui Odontal Bras. 16, 3, 270-275.
32. Keng S. Lim M., Denture plaque distribution and the effectiveness of a
perborate containing denture cleanser.1996, Quintescence Intl. 27, 5, 341-345.
33. Tarbet W., Axelrod S., Minkoff S., Fratarcangelo P. Denture cleansing: a
comparison of two methods. 1984, J. Prosthet. Dent. 51, 3, 322-325.
34. Sheen S., Harisson A. Assessment of plaque prevention on dentures using
an experimental cleanser. 2000, J. Prosthet. Dent., 84, 6, 594-601.
35. Mc Cabe J., Murray I., Laurie J., Kelly P. A method for scoring denture
plaque. 1996, Eur. J. Prostodont. Restor. Dent. 4, 2, 59-64.

23
36. Gornitsky M., Paradis I., Lalaverde G., Lano A., Velly A. A clinical and
microbiological evaluation of denture cleansers for geriatric patients in long term
care institutions. 2002, J. Can. Dent. Assoc., 68, 1, 39-45.
37. Dills S., Olshan A., Goldner S., Brogdon C., Comparison of the
antimicrobial capacity of an abrasive paste and chemical soak for denture
cleansers. 1988, J. Prosthet. Dent. 60, 4, 467-470.
38. Maccracken G., Preshaw P., Steen I., Swan M., DeJager M., Haesman P.
2006, J. Clin. Periodontol. 33, 3, 172-176.