medical helminthology. roundworms- human parasites iryna pryvrotska
TRANSCRIPT

Medical Medical Helminthology. Helminthology.
Roundworms- human Roundworms- human parasitesparasites
Iryna PryvrotskaIryna Pryvrotska

NematodesNematodes RoundwormsRoundworms with a cylindrical body and with a cylindrical body and
a complete digestive tract including a complete digestive tract including mouth and anus. mouth and anus.
They are They are unsegmented, unsegmented, pseudocoelomatepseudocoelomate worms. worms.
The body is covered with a The body is covered with a noncellular,noncellular, highly resistant coating called a highly resistant coating called a cuticle.cuticle.
Nematodes have Nematodes have separate sexesseparate sexes; the ; the female is usually larger than the male. female is usually larger than the male. The male typically has a The male typically has a coiled tailcoiled tail. .
The medically important nematodes can The medically important nematodes can be divided into 2 categories: be divided into 2 categories: intestinalintestinal and and tissuetissue nematodes.nematodes.

Ascaris lumbricoidesAscaris lumbricoides
causes ascariasis.causes ascariasis. Distribution:Distribution: worldwide. worldwide. Morphology:Morphology: Adult maleAdult male
about 20 cm in length, about 20 cm in length, posterior end is curved posterior end is curved ventrally;ventrally;
AAdult femaledult female about 25- about 25-40 cm in length, 40 cm in length, posterior end is straight. posterior end is straight.
Eggs Eggs are brown, oval, are brown, oval, covered by membranes. covered by membranes. An external membrane is An external membrane is tuberoustuberous

Ascaris lumbricoidesAscaris lumbricoides Mode of transmission:Mode of transmission: fecal-oral fecal-oral
(alimentary). Humans are infected by (alimentary). Humans are infected by eating eggs in soil contaminated with eating eggs in soil contaminated with human feces. human feces.
Ascaris lumbricoidesAscaris lumbricoides Clinical manifestationClinical manifestation: : - Migrating larvae may lead to pneumonia, - Migrating larvae may lead to pneumonia,
eosinophilia.eosinophilia. - Adults may cause intestinal obstruction, - Adults may cause intestinal obstruction,
penetration of the intestinal wall, occlusion of penetration of the intestinal wall, occlusion of the bile duct, the pancreatic duct or the the bile duct, the pancreatic duct or the appendix, toxic effects (nausea, vomiting). Most appendix, toxic effects (nausea, vomiting). Most infections are asymptomatic.infections are asymptomatic.
Laboratory diagnosis Laboratory diagnosis faeces ovoscopy faeces ovoscopy (eggs are oval with an irregular surface); larvae (eggs are oval with an irregular surface); larvae may be found in sputum.may be found in sputum.
Prophylaxis:Prophylaxis: wwashing hands before meals; ashing hands before meals; proper washing of vegetables eaten raw; proper washing of vegetables eaten raw; treatment of patients; proper disposal of feces; treatment of patients; proper disposal of feces; health education.health education.

Enterobius Enterobius vermicularisvermicularis causes enterobiasis.causes enterobiasis.
Distribution:Distribution: worldwide.worldwide.
Morphology:Morphology: Adult Adult female worms are up female worms are up to 10 mm in length, to 10 mm in length, and male worms are and male worms are up to 5 mm. up to 5 mm.
EggsEggs are transparent are transparent and colourless, and colourless, asymmetrical, with asymmetrical, with thin and smooth thin and smooth membrane, 40-60 membrane, 40-60 micro;m.micro;m.
Enterobius Enterobius vermicularisvermicularis
Mode of transmissionMode of transmission: fecal-oral (alimentary). : fecal-oral (alimentary). Infective stageInfective stage: eggs. : eggs. The adult pinworms live in the large intestine The adult pinworms live in the large intestine
approximately 30 days.approximately 30 days. After fertilization female worm migrates from After fertilization female worm migrates from
the anus and releases thousands of fertilized the anus and releases thousands of fertilized eggs on perianal skin.eggs on perianal skin.
Within 6 hours, eggs develop into larvae and Within 6 hours, eggs develop into larvae and become infectious. become infectious.
Reinfection can occur if they are carried to the Reinfection can occur if they are carried to the mouth by fingers after scratching of the itching mouth by fingers after scratching of the itching skin. skin.

Enterobius Enterobius vermicularisvermicularis
Clinical manifestationClinical manifestation:: Infection is frequent Infection is frequent among children under 12 years of age. Perianal among children under 12 years of age. Perianal pruritus (itching) is most common symptom.pruritus (itching) is most common symptom.
Laboratory diagnosisLaboratory diagnosis:: the the eggs eggs are are recovered from recovered from perianal skinperianal skin by using the by using the “Scotch tape” technique and can be observed “Scotch tape” technique and can be observed microscopically (eggs are not found in the microscopically (eggs are not found in the stools). Seldom adult worms can be found in stools). Seldom adult worms can be found in the stools.the stools.
Prophylaxis:Prophylaxis: keep sanitary condition, keep sanitary condition, treatment of patientstreatment of patients

Trichuris trichiuriaTrichuris trichiuria causes causes trichocephaliasistrichocephaliasis
(whipworm infection). (whipworm infection). Distribution:Distribution: worldwide worldwide, ,
especiallyespecially in in the the tropics. tropics. Morphology:Morphology: Adult Adult female female
worms are up to 5,5 cm in worms are up to 5,5 cm in length, and male are up to 4 length, and male are up to 4 cm. The anterior end of the cm. The anterior end of the body is hairlike. body is hairlike.
The The eggseggs are brown, barrel- are brown, barrel-shaped with a plug at each shaped with a plug at each end, 20-50 micro;m in size.end, 20-50 micro;m in size.

Trichuris trichiuriaTrichuris trichiuria Mode of Mode of
transmission:transmission: fecal- fecal-oral (alimentary). oral (alimentary).
Embryonated eggs Embryonated eggs may be ingested may be ingested through through contaminated water, contaminated water, raw vegetables and raw vegetables and hands.hands.
Infective stageInfective stage: eggs. : eggs.

Trichuris trichiuriaTrichuris trichiuria
Pathogenesis and clinical manifestationPathogenesis and clinical manifestation: Adult : Adult worms burrow their hairlike anterior ends into worms burrow their hairlike anterior ends into the intestinal mucosa. They feed blood. the intestinal mucosa. They feed blood. Trichuris may cause diarrhea, abdominal pain, Trichuris may cause diarrhea, abdominal pain, nausea, acute appendicitis. Most infections are nausea, acute appendicitis. Most infections are asymptomatic.asymptomatic.
Laboratory diagnosisLaboratory diagnosis: microscopic : microscopic examination of feces (finding the typical eggs).examination of feces (finding the typical eggs).
Prophylaxis:Prophylaxis: washing hands before meals; washing hands before meals; proper washing of vegetables eaten raw; proper washing of vegetables eaten raw; treatment of patients; proper disposal of feces; treatment of patients; proper disposal of feces; health education.health education.

TrichinellaTrichinella spiralisspiralis causes causes trichinosistrichinosis. . DistributionDistribution worldwide, especially in eastern Europe and west worldwide, especially in eastern Europe and west
Africa.Africa. Morphology:Morphology: 1) The 1) The adults femaleadults female worms are up to 3-4 worms are up to 3-4 0.6 mm; the 0.6 mm; the adult adult
malemale worms are up to 1.5 worms are up to 1.5 0.04 mm; 0.04 mm; 2) the 2) the incysted larvaeincysted larvae (1 mm)(1 mm) is enclosed in a fibrous cyst is enclosed in a fibrous cyst
wallwall.. Localisation:Localisation: small intestine (adult worms) and striated small intestine (adult worms) and striated
muscles (larvae).muscles (larvae). Any mammal (rat, bear, fox) can be infected, but pigs are the Any mammal (rat, bear, fox) can be infected, but pigs are the
most important reservoirs of human disease.most important reservoirs of human disease.

Infective stage for humans:Infective stage for humans: larva. larva.Mode of transmissionMode of transmission: : alimentary (eating alimentary (eating raw or undercooked meat, usually pork, raw or undercooked meat, usually pork, containing larvae encysted in the containing larvae encysted in the muscle).muscle).

TrichinellaTrichinella spiralisspiralis
Clinical manifestation:Clinical manifestation: initially diarrhea, initially diarrhea, abdominal pain followed by 1-2 weeks later by abdominal pain followed by 1-2 weeks later by fever, muscle pain, periorbital edema, and fever, muscle pain, periorbital edema, and eosinophilia. Death, which is rare, is usually due eosinophilia. Death, which is rare, is usually due to congestive heart failure or respiratory to congestive heart failure or respiratory paralysis. paralysis.
Laboratory diagnosisLaboratory diagnosis:: muscle biopsy muscle biopsy reveals reveals larvae larvae within striated muscle; serologic within striated muscle; serologic test (become positive 3 weeks after infection). test (become positive 3 weeks after infection).
ProphylaxisProphylaxis by properly cooking pork and by properly cooking pork and by feeding pigs only cooked garbageby feeding pigs only cooked garbage; pork ; pork inspection in slaughter houses using a inspection in slaughter houses using a trichinoscopetrichinoscope..

Ancylostoma duodenale and Ancylostoma duodenale and Necator americanus Necator americanus
(hookworms)(hookworms) cause cause ancylostomiasis ancylostomiasis
(hookworm infection).(hookworm infection). Morphology:Morphology:
1) 1) Adult Adult worms about 1 cm in worms about 1 cm in length; length;
2) 2) EggsEggs are translucent, oval are translucent, oval with blunt poles, 40-60 micro;m with blunt poles, 40-60 micro;m in size; in size;
3) the 3) the rhabditiform larvarhabditiform larva is about is about 0.25-0.5 micro;m with 0.25-0.5 micro;m with rhabditiform oesophagus (1/3 rhabditiform oesophagus (1/3 body length), pointed tail end;body length), pointed tail end;
4) the 4) the filariform larvafilariform larva is about is about 0.6-0.7 micro;m with cylindrical 0.6-0.7 micro;m with cylindrical oesophagus (1/4 body length), oesophagus (1/4 body length), sharply pointed tail.sharply pointed tail.

HookwormsHookworms Hosts:Hosts: humans. humans. Mode of transmissionMode of transmission: :
penetration of skin by filariform penetration of skin by filariform larva larva
Infective stage:Infective stage: filariform larva. filariform larva. Clinical manifestation:Clinical manifestation: 1) invasion stage (the larvae 1) invasion stage (the larvae
penetrate the skin): dermatitis penetrate the skin): dermatitis and itching (“ground itch”);and itching (“ground itch”);
2) migration stage: pneumonia 2) migration stage: pneumonia with eosinophilia; with eosinophilia;
3) intestinal stage: anemia, 3) intestinal stage: anemia, diarrhea, abdominal pain, nausea. diarrhea, abdominal pain, nausea.
Laboratory diagnosisLaboratory diagnosis: eggs in : eggs in the stool; blood in the feces is the stool; blood in the feces is frequent finding.frequent finding.
Prophylaxis:Prophylaxis: disposing of disposing of sewage properly and wearing sewage properly and wearing shoes.shoes.

Wuchereria bancroftiWuchereria bancrofti causes filariasis. causes filariasis. This disease occurs in the This disease occurs in the
tropics.tropics.

Wuchereria bancroftiWuchereria bancrofti
Mode of Mode of transmissiontransmission.. Humans are Humans are infected when the infected when the female mosquito female mosquito (especially (especially Anopheles Anopheles and and Culex Culex species)species) deposits infective deposits infective larvae on the skin larvae on the skin while biting. while biting.
Wuchereria bancroftiWuchereria bancrofti
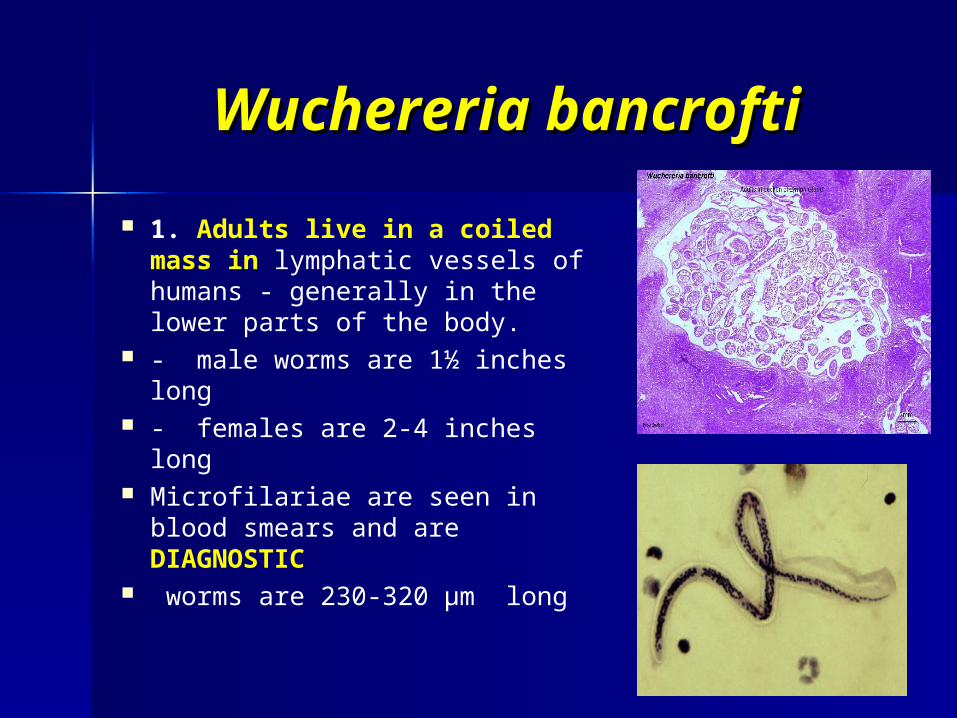
1. Adults live in a coiled mass in lymphatic vessels of humans - generally in the lower parts of the body.
- male worms are 1½ inches long
- females are 2-4 inches long Microfilariae are seen in blood
smears and are DIAGNOSTIC worms are 230-320 µm long

Life Cycle ofLife Cycle of Wuchereria Wuchereria bancroftibancrofti
2. Females produce thousands of Microfilariae that are released into the lymph and move into peripheral blood

Life Cycle ofLife Cycle of Wuchereria Wuchereria bancroftibancrofti
Microfilariae are ingested when night-biting mosquito takes blood meal.
Microfilariae migrate to the mosquito muscles and molt

Life Cycle ofLife Cycle of Wuchereria Wuchereria bancroftibancrofti
Larva migrate to the mouth parts of the mosquito and enter human skin when the mosquito bites.
larva enter small lymphatic vessels and move to the large lymphatic vessels
- molt 2x to become adults
- adults take up to a year to mature and produce microfilariae

Microfilariae of Microfilariae of Wuchereria Wuchereria bancroftibancrofti
Nocturnal periodicity of microfilariae

Pathology of Pathology of Wuchereria Wuchereria bancroftibancrofti
Pathology caused by Wuchereria Wuchereria bancroftibancrofti included 3 clinical phases
1. Takes time between infection with L3 after a mosquito bite and maturation of adults (usually a year) - no symptoms

Pathology of Pathology of Wuchereria Wuchereria bancroftibancrofti
2. Inflammation phase
- females release microfilariae
- infiltration of white blood cells
- intense inflammation of lymphatic vessels and lymph nodes
Pathology of Pathology of Wuchereria Wuchereria bancroftibancrofti
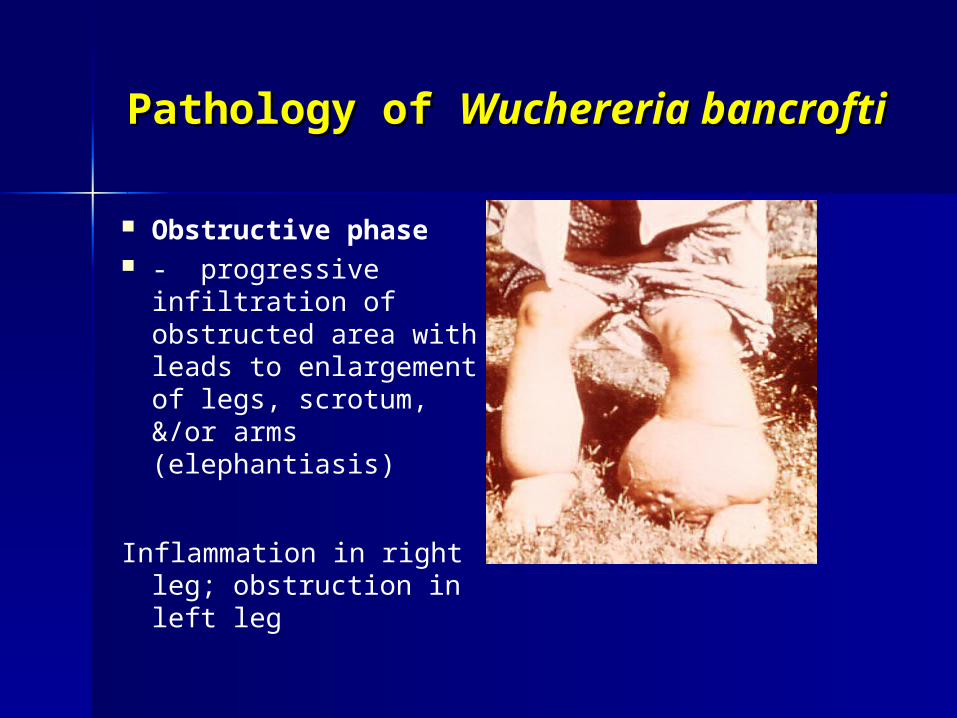
Obstructive phase - progressive
infiltration of obstructed area with leads to enlargement of legs, scrotum, &/or arms (elephantiasis)
Inflammation in right leg; obstruction in left leg

Obstructive phase photos
Prevention involves mosquito control with insecticides and the use of protective clothing, mosquito netting, and repellents.
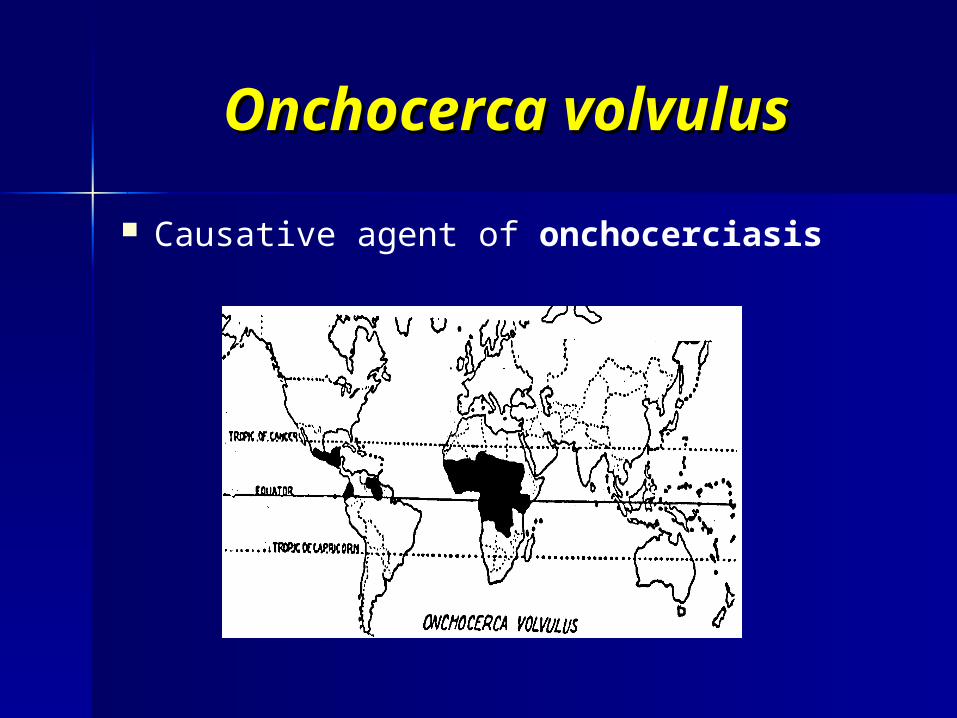
Onchocerca volvulusOnchocerca volvulus
Causative agent of onchocerciasis

Onchocerca volvulusOnchocerca volvulus VectorsVectors of Onchocerca of Onchocerca
volvulus (blackflies) volvulus (blackflies) develop in rivers and develop in rivers and people who live along people who live along those rivers are affected. those rivers are affected. Infection rates are often Infection rates are often over 80% in endemic over 80% in endemic areas. areas.
Mode of transmissionMode of transmission.. Humans are infected Humans are infected when the when the female female blackfly blackfly SimuliumSimulium deposits infective larvae deposits infective larvae on the skin while biting. on the skin while biting.

Onchocerca volvulusOnchocerca volvulus The larvae enter the The larvae enter the
wound and migrate into wound and migrate into the subcutaneous tissue, the subcutaneous tissue, where they differentiate where they differentiate into adults, usually into adults, usually within within dermal nodules.dermal nodules.
The female produces The female produces microfilariae.microfilariae.
The microfilariae The microfilariae develop into infective develop into infective larvae in the fly to larvae in the fly to complete the cycle. complete the cycle. Humans are the only Humans are the only definitive hosts.definitive hosts.
Microfilariae of Onchocerca NEVER invade the bloodstream.

Skin nodule cut open to reveal adults coiled together
Microscopic section showing adults and scar tissue reaction around them forming the nodule
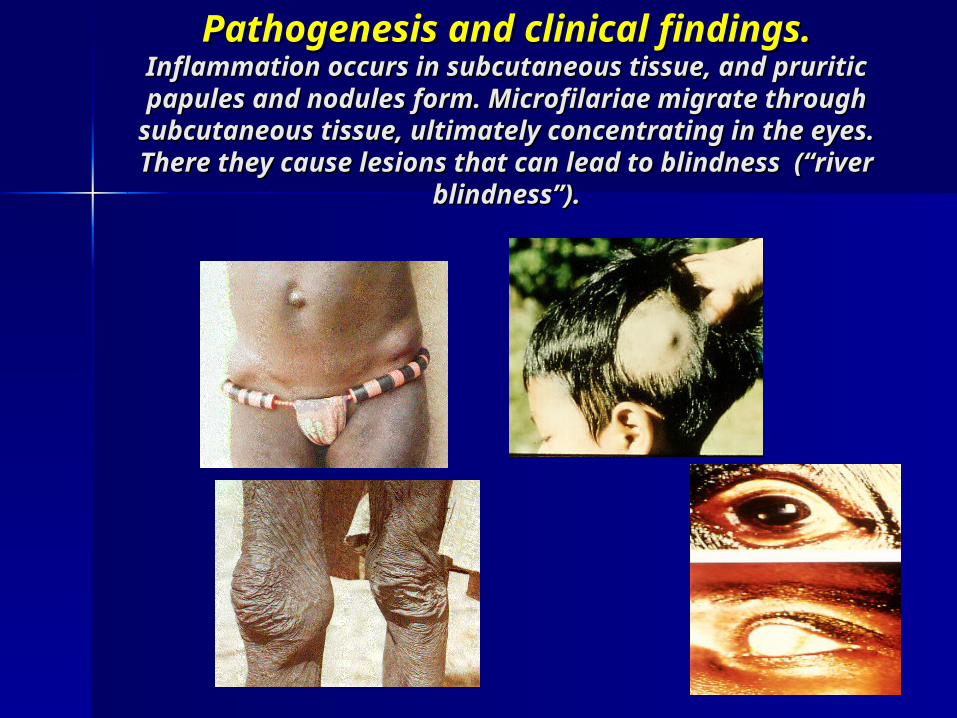
Pathogenesis and clinical findings.Pathogenesis and clinical findings. Inflammation occurs in subcutaneous tissue, and Inflammation occurs in subcutaneous tissue, and pruritic papules and nodules form. Microfilariae pruritic papules and nodules form. Microfilariae migrate through subcutaneous tissue, ultimately migrate through subcutaneous tissue, ultimately
concentrating in the eyes. There they cause concentrating in the eyes. There they cause lesions that can lead to blindness (“river lesions that can lead to blindness (“river
blindness”).blindness”).

Onchocerca volvulusOnchocerca volvulus
Laboratory diagnosisLaboratory diagnosis.. Biopsy of Biopsy of the affected skin reveals the affected skin reveals microfilariae.microfilariae.
PreventionPrevention involves control of involves control of the blackfly with insecticides.the blackfly with insecticides.

Loa loaLoa loa causes loiasis. causes loiasis.
The disease is The disease is found only in found only in tropical central tropical central and west and west Africa, the Africa, the habitat of the habitat of the vector vector Chrysops.Chrysops.

Loa loaLoa loa Mode of transmission.Mode of transmission.
Humans are infected by the Humans are infected by the bite of the bite of the deer fly deer fly (mango (mango fly),fly), ChrysopsChrysops,, which which deposits infective larvae on deposits infective larvae on the skin.the skin.
The larvae enter the bite The larvae enter the bite wound, wander in the body, wound, wander in the body, and develop into adults. and develop into adults.
The females release The females release microfilariae that enter the microfilariae that enter the blood, particularly during blood, particularly during the day. the day.
The microfilariae are taken The microfilariae are taken up by the fly during a blood up by the fly during a blood meal and differentiate into meal and differentiate into infective larvae, which infective larvae, which continue the cycle when the continue the cycle when the fly bites the next person.fly bites the next person.

Pathogenesis and clinical Pathogenesis and clinical findings.findings.
Adults cause localized inflammatory reactions in the skin called Calabar swellings.
Eye swells when worms migrate through.
Laboratory diagnosis.Laboratory diagnosis. Diagnosis is made by Diagnosis is made by visualization of the visualization of the microfilariae in a blood microfilariae in a blood smear.smear.
PreventionPrevention.. Control of Control of the fly by insecticides the fly by insecticides can prevent the disease.can prevent the disease.

Dracunculus medinensisDracunculus medinensis (guinea fire worm) (guinea fire worm)
causes dracunculiasis. causes dracunculiasis. The disease occurs over large areas of The disease occurs over large areas of
tropical Africa, the Middle East, and tropical Africa, the Middle East, and India.India.

Dracunculus Dracunculus medinensismedinensis
Adult females are largest nematodes of humans – reach length of up to 4 feet.
Male is smaller - 4 cm.
HOSTS - humans and many other mammals (dogs, cats, cattle, horses, monkeys)

Life CycleLife Cycle
Humans are Humans are infected when infected when tiny tiny crustaceans crustaceans (copepods)(copepods) containing containing infective infective larvae are larvae are swallowed in swallowed in drinking drinking water.water.
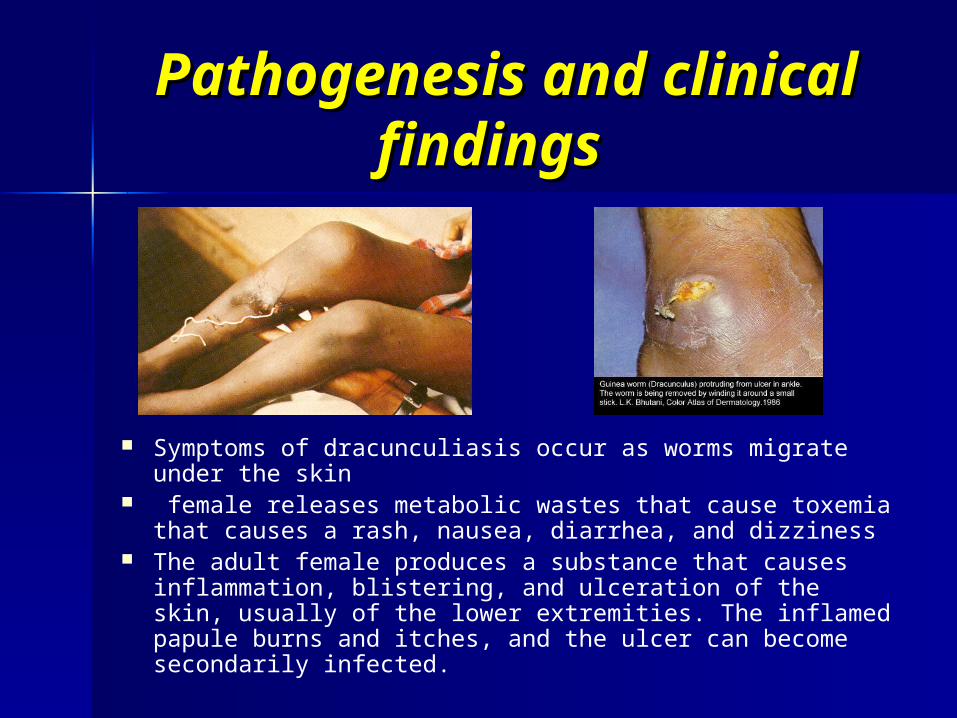
Pathogenesis and Pathogenesis and clinical findingsclinical findings
Symptoms of dracunculiasis occur as worms migrate under the skin
female releases metabolic wastes that cause toxemia that causes a rash, nausea, diarrhea, and dizziness
The adult female produces a substance that causes inflammation, blistering, and ulceration of the skin, usually of the lower extremities. The inflamed papule burns and itches, and the ulcer can become secondarily infected.

Dracunculus Dracunculus medinensismedinensis
Laboratory diagnosisLaboratory diagnosis.. Diagnosis is usually made Diagnosis is usually made clinically by finding the head of clinically by finding the head of the worm in the skin ulcer.the worm in the skin ulcer.
PreventionPrevention consists consists of filtering of filtering or boiling of drinking water.or boiling of drinking water.

Toxocara canisToxocara canis causes visceral larva migrans. Visceral larva migrans causes visceral larva migrans. Visceral larva migrans
occurs worldwide. Young children are primarily affected.occurs worldwide. Young children are primarily affected. Life cycle.Life cycle. Infective stage:Infective stage: eggs. eggs. The definitive host for Toxocara canis is the dog.The definitive host for Toxocara canis is the dog. Eggs soil human (small intestine) internal Eggs soil human (small intestine) internal
organsorgans(the liver, brain, and eyes). (the liver, brain, and eyes). The larvae eventually are encapsulated and die. The larvae eventually are encapsulated and die. The life cycle is not completed in humans. Humans are The life cycle is not completed in humans. Humans are
therefore accidental, dead-end hosts.therefore accidental, dead-end hosts. Pathogenesis and clinical findingsPathogenesis and clinical findings.. Pathology is Pathology is
related to the granulomas that form around the dead related to the granulomas that form around the dead larvae. The most serious clinical finding is blindness due to larvae. The most serious clinical finding is blindness due to retinal involvement. Fever, hepatomegaly, and retinal involvement. Fever, hepatomegaly, and eosinophilia are common.eosinophilia are common.
Laboratory diagnosis:Laboratory diagnosis: serologic tests.serologic tests. Prevention.Prevention. Dogs should be dewormed, and children Dogs should be dewormed, and children
should be prevented from eating soil. should be prevented from eating soil.

Thank you for Thank you for attention!attention!