medical conditions complicating pregnancyin+pregnancy... · •pregestational diabetes is generally...
TRANSCRIPT

MEDICAL CONDITIONS
COMPLICATING PREGNANCY
Dr.Badi albaqawi , MD
KFMC-WSH, Riyadh

Objectives
• Common medical diseases affecting pregnant women.
• Course of the disease
• Course of the pregnancy
• Antenatal maternal and fetal surveillance
• Maternal outcome
• Fetal outcome

Introduction
• Diabetes and thyroid disorders are most common.
• How the physiologic changes of pregnancy may
affect the diagnosis and clinical course
• How the disease may affect the pregnancy.

PHYSIOLOGICAL CHANGES OF GLUCOSE
METABOLISM IN PREGNANCY
• Pregnancy is a state of insulin resistance & relative
glucose intolerance
• This is due to placental production of anti-insulin
hormones : hPL, cotisol, and glucagon
• FBS
• Postprandial glucose ↑ ↑
• Insulin production ↑ ↑ 2 folds in N women
• Insulin requirements ↑ ↑ in diabetic women
• renal threshold for glucose glycosuria

DIABETES MELLITUS
• The prevalence of diabetes mellitus has greatly increased
in the last 20 years.
• Range from 6-12% .
• 80-90% of diabetes in pregnant women is gestational, and
about 10% is pregestational.
GDM Pregestational

Gestational diabetes mellitus (GDM)
• Defined as glucose intolerance with onset or first
recognition during pregnancy.
• Human placental lactogen, progesterone,
prolactin, and cortisol
• GDM is considered stress test for future development of
DM .

Pregestational diabetes mellitus
• Diabetes present before pregnancy and may be
either type 1 or type 2 diabetes.
• White classification of diabetes during pregnancy
to assess disease severity and the likelihood of
complications .


EFFECT OF PREGNANCY ON DM
• Insulin requirement ↑ ↑ in pregnancy reaching a max at
term & being at least 2 X the pre-pregnancy requirement
• Pt with diabetic nephropathy deterioration in renal
function with in creatinine clearance & proteinuria
this deterioration in renal function is usually reversed
after delivery

EFFECT OF PREGNANCY ON DM
• 2 X ↑↑ in retinopathy
rapid improvement in glycemic control worsening
retinopathy due to ↑↑ retinal blood flow
• ↑↑ icidence of hypoglycemia
• Ketoacidosis is rare unless associated with hyperemesis,
infections, tocolytic & corticosteroid Rx

EFFECTS OF DM ON PREGNANCY
• ↑ incidence of congenital abnormalities
• The risk is related to the degree of glycemic control 5%
with Hb A1c > 8%
25% with Hb A1c > 10% with ↑↑ risk
of abortions
• Sacral agenesis, congenital heart defects, skeletal
abnormalities & neural tube defects
• Perinatal & neonatal mortality ↑↑ 2-4 X
• Unexplained IUFD at term / more in macrosomic babies

EFFECTS OF DM ON PREGNANCY
• Macrosomia the incidence is ↑↑ with poor diabetic
control
not eliminated by tight control
associated with ↑↑ risk of operative delivery, birth
trauma, & shoulder dystocia
• Hyperglycemia fetal polyuria polyhydramnios
PROM, preterm delivery
• Prematurity pose an added problem as pulmonary
surfactant production is slightly delayed in babies of
diabetic mothers

EFFECTS OF DM ON PREGNANCY
• Postnatally, babies are at risk of hypoglycemia & jaundice
• ↑↑ risk of PET especially in pt with pre-existing
hypertension & nephropathy where it reaches almost 30%

Diagnosis of Gestational Diabetes
Mellitus
• Low risk between 24 and 28 weeks’
• High risk1st antenatal visit.
• High risk previous pregnancy with GDM, a history of
polycystic ovarian disease, obesity, previous IUFD, history
of big baby
• If a first-trimester screen is done and is found to be
negative, it should be repeated at 24 to 28 weeks.
• 50 g OGTT >130mg/dl is +ve.
• If blood glucose >200mg/dl is +ve and no need for 2nd
step.

Diagnosis of Gestational Diabetes
Mellitus
Screening
One step using 75 g
glucose
Two steps using 50 g then
100g glucose


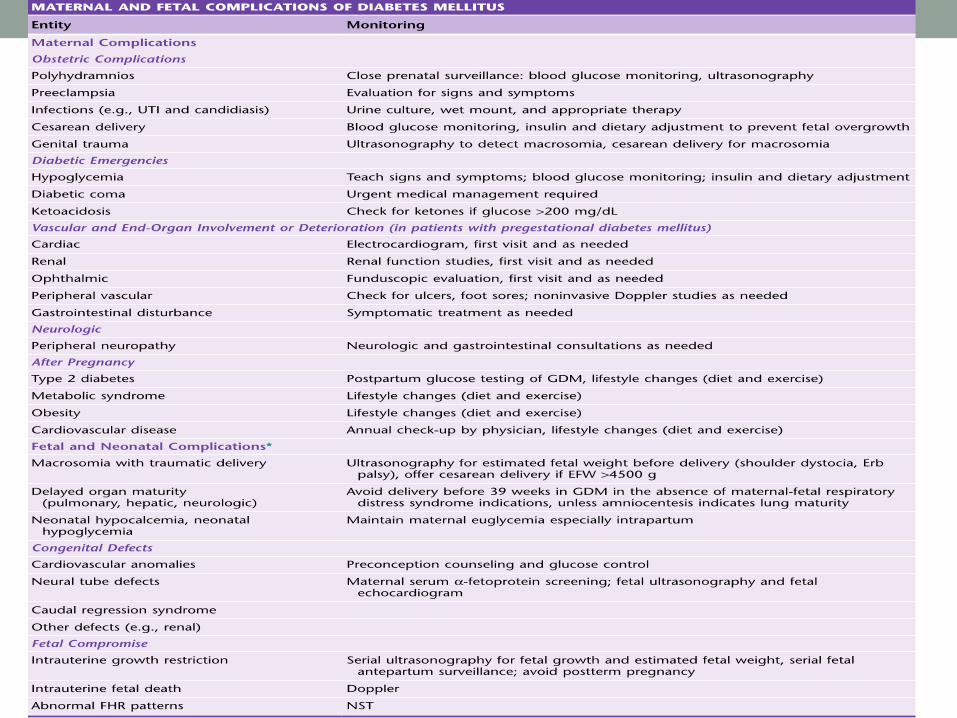
Complications
• Most fetal and neonatal effects are attributed to the
consequences of maternal hyperglycemia
• Fetal hyperglycemia during the period of embryogenesis
is teratogenic.
• direct correlation between birth defects in diabetic
pregnancies and increasing glycosylated hemoglobin A1C
(HbA1C)
• Fetal demise due to acidosis, hypotension from
osmotic diuresis, or hypoxia from increased metabolism,
coupled with inadequate placental oxygen transfer.

Hyperglycemia
Maternal hyperglycemia
Fetal hyperglycemia
Fetal pancreatic beta-cell hyperplasia
Fetal hyperinsulinaemia
Macrosomia,organomegaly, polycythaemia, hypoglycemia,
RDS

• Pregestational diabetes is generally associated with a
higher rate of maternal and fetal complications
Preexisting DM in Pregnancy
Effect of preexisting DM on pregnancy (Maternal)
1. increase risk of miscarriage
2. increase risk of preclampsia
3. increase risk of infection eg vaginal candidiasis, UTI,
endometrial or wound infection
4. increase LSCS rate

Preexisting DM in Pregnancy
Fetal
1. increase risk of congenital abnormalities
sacral agenesis, congenital heart disease,
neural tube defects
Hba1c level Risk
normal not increased
<8% 5%
>10% 25 %

Preexisting DM in Pregnancy
2. Perinatal mortality (excluding congenital abnormality ) 2
fold increased
3. Increase risk of sudden unexplained intrauterine fetal
death.

Complications of pregnancy in pre-
existing DMMaternal:
Increase insulin requirment’Hypoglycemia
Infection
Ketoacidosis
Deterioration in retinopathy’Increased proteinuria+
edema
Miscarriage
Polyhydramnios
Shoulder dystocia
Preeclampsia
Increased caesarean rate
Fetal:
Congenital abnormalities
Increased neonatal and perinatal mortality
Macrosomia
Late stillbirth
Neonatal hypoglycemia
Polycythemia
jaundice
Management
• a team approach
• education and counseling,
• ACHIEVING EUGLYCEMIA : FBS <95 mg/dl and 2hr pp is
< 120 mg/dl.
DIET EXERCISE
PHARMACOLOGIC THERAPY.

Diet
• 30-35 kcal/kg /day
• The diet is composed of about 45-50% carbohydrate, 20-
25% protein, and 20-25% fat.
• Contain a generous amount of fiber.
• Caloric intake is divided into 20% at breakfast, 30% at
lunch, 30% at dinner, and 20% at a bedtime snack.

PHARMACOLOGIC THERAPY
• Metformine.
• Oral hypoglycemic agent (glyburide) .
• Insulin .
• Insulin is the medication of choice to maintain eu-
glycemia in pregnancy and is the recommended therapy
in women with pregestational diabetes.

Antepartum Obstetric Management
• Multidisciplinary team including obstetricians, endocrinologists, dieticians, & midwives optimize outcome
• Preconception councelling
• To achieve normoglycemia
• Dietary advice on a low sugar, low fat, high fiber diet
• Regular capillary glucose series

Antepartum Obstetric Management
• Regular assessment of Hb A1c
• Ophthalmologic examination & Rx of retinopathy
• Regular monitoring of renal function in Pt with diabetic
nephropathy
• Detailed U/S screening for congenital malformations in
the 2nd trimester (20wk) to exclude NTD, sacral
agenesis, & cardiac defects
• Frequency of antenatal visits needs to be individualized

The timing of delivery
• depends on fetal and maternal status and the degree
of glucose control.
• Well-controlled GDM without other complications,
spontaneous onset of labor at term may be awaited.
• Earlier intervention is indicated if these conditions are not
met.
• For macrosomic babies, increased birth trauma to both
mother and fetus should be avoided. Cesarean delivery
may be elected for large fetuses (>4500 g).

Intrapartum Management
• Establishment of maternal euglycemia during labor.
• continuous infusion of regular insulin is given.
• Plasma glucose level between 80 and 120 mg/dL.
• Fetal heart rate monitoring is recommended for all
patients with diabetes.

Postpartum Period
• Insulin requirements drop sharply because the placenta .
• Plasma glucose levels should be monitored and lispro or
regular insulin given when plasma glucose levels are
elevated.
• Women with GDM should undergo a 75-g OGTT at 6 to
12 weeks postpartum.
• If the mother is breastfeeding, 500 calories/day should be
added to the prepregnancy diet.
• Contraception counseling