medicaid services and part c april 26, 2006 early intervention conference hotel roanoke
TRANSCRIPT

MedicaidMedicaidServices Services
and and Part CPart CApril 26, 2006
Early Intervention ConferenceHotel Roanoke

Overview of Overview of Maternal and Child Health ServicesMaternal and Child Health Services
Relationship between MCH services– EPSDTEPSDT– BabyCareBabyCare– Schools Schools – FAMIS– Family Planning
Waiver
Collaboration with VDH, DSS and DMHMRSAS– Part CPart C– Head StartHead Start– WICWIC– LeadLead– Vaccines for Vaccines for
ChildrenChildren– Resource MothersResource Mothers
MCH Division changes

Definitions of Benefit PlansDefinitions of Benefit Plans
FAMIS 133% < 200% FPL– MCO (no MCO? = Fee for
Service)– FAMIS for children under 19
Medicaid < 133% FPL– FAMIS Plus = Children’s Medicaid
(under age 19)– MCO vs Fee For Service

Medicaid and FAMISMedicaid and FAMIS
Get detailed information service criteria and limitations via the
internet at…
www.dmas.virginia.gov
www.famis.org
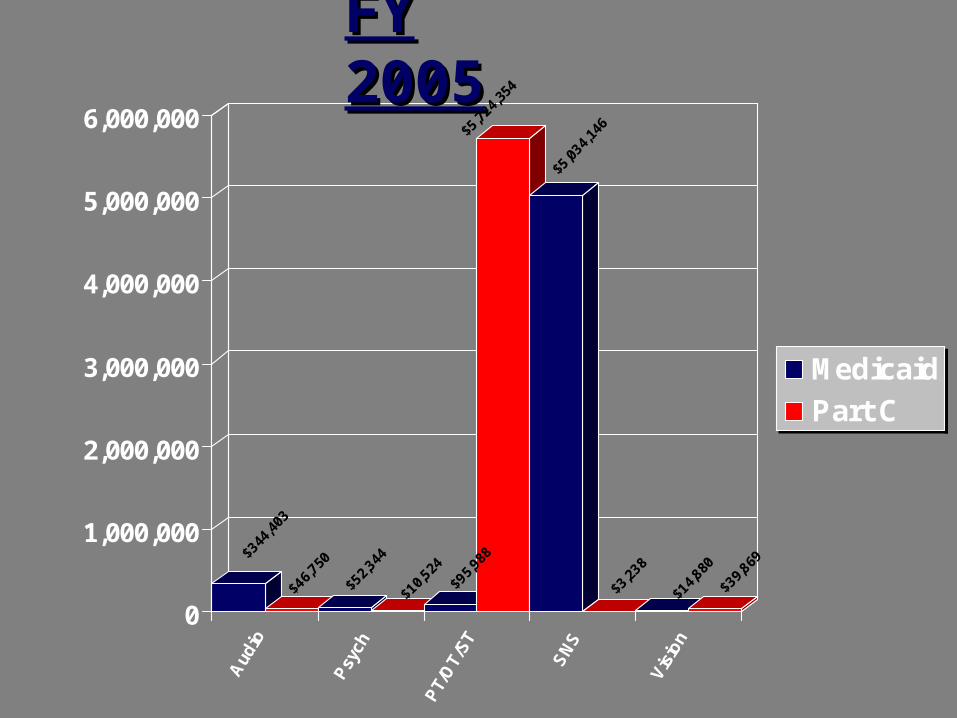
$344
,403
$46,7
50
$52,3
44
$10,5
24
$95,9
88
$5,72
4,35
4
$5,03
4,14
6$3
,238
$14,8
80
$39,8
69
0
1,000,000
2,000,000
3,000,000
4,000,000
5,000,000
6,000,000
Aud
io
Psy
ch
PT/
OT/
ST
SN
S
Vis
ion
Medicaid
Part C
FY 2005FY 2005

Early and Periodic Screening, Early and Periodic Screening, Diagnosis, and Treatment Diagnosis, and Treatment
ServicesServices(EPSDT)(EPSDT)

What is EPSDT? What is EPSDT?
A Medicaid program for children up to the age of 21 with a preventive treatment approach
Diagnosis or screening services are the backbone of the program
EPSDT criteria must be considered within existing state plan service reviews
Referrals for treatment services occur during well child or other as needed screenings

Who is Eligible for EPSDT?Who is Eligible for EPSDT?
Children under the age of 21 who receive Medicaid through Medicaid/FAMIS Plus, or a MCO are eligible to receive the full scope of Medicaid/EPSDT services
FAMIS children who are not enrolled with a Managed Care Organization
MCO enrolled FAMIS children receive Well Child services through their MCO but are not eligible for the full scope of EPSDT

MCO and EPSDTMCO and EPSDT
MCO’s have responsibility to provide EPSDT diagnostic and treatment services according to Federal Criteria American Academy of Pediatrics (AAP) guidelines

What are EPSDT Services?What are EPSDT Services?
EPSDT services include: Screening/Well Child check-ups,
lead testing and immunizations
Other treatment services to correct a medical condition, make it better, or prevent the child’s health status from worsening

EPSDT Required ServicesEPSDT Required Services
Preventive screenings Preventive Laboratory Services Developmental/Behavioral
Assessment Lead testing at 12 and 24 months Immunizations Referral to a dentist at age 3
All children should receive these services

EPSDT ScreeningsEPSDT Screenings

EPSDT ScreeningsEPSDT Screenings
EPSDT screenings must: – Be regularly scheduled according
to AAP/Bright Futures Guidelines (refer to periodicity chart for detail)
– Contain certain elements to be considered an EPSDT screening

EPSDT Screening TypesEPSDT Screening Types
There are 4 types of EPSDT screenings
1. Medical 2. Dental3. Vision 4. Hearing

EPSDT ScreenersEPSDT Screeners
Physician
Certified Nurse Practitioner

Types of ScreeningsTypes of Screenings
AAP recommended screenings:
– These are typical “well child care” – They are conducted according to
the DMAS periodicity schedule

Types of ScreeningsTypes of Screenings
Inter-periodic or partial screenings:
These are intermittent physician encounters or “sick visits”
Problem-focused screening

Screening and TreatmentScreening and Treatment
Periodic, Inter-periodic or partial screenings may be used to document the need for EPSDT treatment
Any caregiver or professional who comes in contact with the EPSDT enrollee may request an inter-periodic screening

Mandated Screening ElementsMandated Screening Elements1. A Comprehensive health and developmental
history (including assessment of both physical and mental health development);
2. A comprehensive unclothed physical exam; 3. Age appropriate (if needed) immunizations
scheduled according to the: Advisory Committee on Immunization Practices (ACIP) guidelines: http://www.cdc.gov/nip/recs/child-schedule.htm

More More Screening ElementsScreening Elements
4. Laboratory tests (including lead blood level assessment at 12 and 24 or when new patient with unknown history up to 72 months or as appropriate for age and risk factors); AND
5. Health Education- Anticipatory Guidance and problem focused guidance and counseling.

EPSDT Periodicity Schedule EPSDT Periodicity Schedule
– States must provide screenings at intervals which meet reasonable standards of medical and dental practice, for pediatric vaccines
– Virginia uses the American Academy of Pediatrics (AAP) guidelines to develop its EPSDT periodicity schedule

Screening and Long Term CareScreening and Long Term Care
Referrals should be made to agencies who help with accessing Long Term Care/Community Based Waiver Programs
More information accessing waiver services may be found by calling the DMAS Long Term Care Division at
804-786-1465

Possible Referrals to ProgramsPossible Referrals to Programs
Mental Health Services Specialized Therapies/Rehabilitative
Services to manage developmental disabilities
EPSDT Nursing, Personal Care, Medical and adaptive equipment
Residential Treatment, facility and hospital services
Other medically necessary care

The EPSDT DifferenceThe EPSDT Difference
Mandatory Lead Testing is the exception where EPSDT screenings exceed Well Child Care
The EPSDT difference is in the scope of EPSDT treatment

Lead Testing Lead Testing RequirementsRequirements
The Centers for Medicare and Medicaid Services (CMS) requires that all Medicaid enrolled children receive a blood lead test at 12 months and 24 months of age.

Lead Testing Lead Testing RequirementsRequirements
Children enrolled in Medicaid between the ages of 24 months and 72 months of age must also receive a blood lead test if they have not been previously screened for lead poisoning or if the current medical record is insufficient to prove that a lead test has been performed on the child

Lead Testing Lead Testing RequirementsRequirements
Testing may be performed by venipuncture or capillary blood sample. Filter paper methods are also acceptable.
Confirm elevated capillary blood lead levels ≥10 μg/dL.
A second capillary sample for confirmation is allowable if performed within 12 weeks (84 days) of the original capillary sample.
A venous sample is considered “confirmed”. A venous sample is required for an environmental investigation at levels above 15 μg/dL.

Active Lead Testing Active Lead Testing LaboratoriesLaboratories
Environmental investigations are a service offered by Medicaid through Lead Safe Virginia. Environmental Investigations are reimbursed to DMAS enrolled health departments. Medicaid funds are not available for testing of environmental substances such as water, paint or soil. Please consult with your local health department or contact Lead-Safe Virginia to see if your patient qualifies for a risk assessment

DMAS Enrolled LabsDMAS Enrolled Labs
MCO enrolled providers will use the labs as designated in their provider contracts
DMAS labs who currently provide pediatric lead testing can be found on the DMAS website www.dmas.virginia.gov by contacting the provider help-line and by email at [email protected]

Lead-Safe Virginia provides clinical guidance
Free Medical "hotline" at 866-767-5323 (866-SOS-LEAD).
The hotline is within the University of Virginia and it is available 24 hours a day seven days a week.
Lead Safe VirginiaLead Safe Virginia
DMAS Birthday CardsDMAS Birthday Cards
DMAS/EPSDT birthday cards include lead testing requirements for children under the age of 6 and information about upcoming well child appointments.
The cards are sent to all Medicaid- eligible recipients, including those in Managed Care Organization
Follow up notices go to the providers to remind them that a test is required

Bright FuturesBright Futures
Developed in conjunction with CMS, AAP, and HRSA to promote EPSDT
More information and family guidance is provided at www.brightfutures.org
Bright futures materials mirror the AAP guidelines

Tools for FamiliesTools for Families
Tools for practices
Tools for social workers
A tool for Medicaid programs

Bright FuturesBright Futures
Bright Futures guidelines address the new health risks that threaten children and families today. Bright futures discusses chronic conditions such as: – asthma, – obesity and – complications of early sexual
activity.

Bright FuturesBright Futures
Bright futures discusses healthcare issues that affect many Medicaid families such as:
poverty and limited access to
health care, prenatal risks and low birth-weight
babies, nutrition and school performance,
substandard housing and lead poisoning.

Bright Futures Web Based Bright Futures Web Based Training ModuleTraining Module
http://www.vahealth.org/brightfutures/

Bright Futures VirginiaBright Futures Virginia
http://www.vahealth.org/brightfutures/
The web course is divided into six segments, and can be completed in about seven hours.
One section teaches participants how to apply Bright Futures Guidelines to their practices and is particularly helpful for those who serve high-risk families

Bright Futures VirginiaBright Futures Virginia
Other segments include an overview of Bright Futures, developmental assessments, medical assessment, immunization and screening, and tools to help put Bright Futures into practice

Take 5Take 5

Scope of ServicesScope of Services Individualized health care, diagnostic services,
and “treatment” as listed in the Federal Medicaid statute, must be provided when medically necessary to correct and ameliorate physical and mental conditions discovered during screening services whether or not included in the state plan
The program does not cover services that are experimental or investigational
Must be services that are considered either mandated or optional services by CMS

EPSDT TreatmentEPSDT Treatment
If a health condition is discovered during an EPSDT screening the physician will refer the individual for evaluation to recommend treatment for the condition.
When these services are included in the Virginia State Plan, they are considered treatment services
When these services are not services that are included in the Virginia State Plan, they are considered specialized services

MCO and EPSDTMCO and EPSDT
MCOs provide EPSDT treatment services through their provider network
Certain Medicaid services such as Community Mental Health Rehabilitation and Personal Care are accessed directly through DMAS upon referral from the MCO enrolled physician

Medical NecessityMedical Necessity
All services must be deemed medically necessary to correct or ameliorate a health or mental health conditions
Determined on a case-by-case basis according to EPSDT criteria

EPSDTEPSDTSpecialized ServicesSpecialized Services
Periodic, Inter-periodic or partial screenings may be used to document the need for EPSDT treatment
Any caregiver or professional who comes in contact with the EPSDT enrollee may request an inter-periodic screening

Federally MandatedFederally MandatedMedicaid ServicesMedicaid Services
Inpatient Hospital Services
Emergency Hospital Services
Outpatient Hospital Services
Nursing Facility Care Rural Health Clinic
Services Federally Qualified
Health Center Clinic Services
Lab and X-Ray Services Physician Services Home Health Services EPSDT Family Planning Nurse-Midwife Services Transportation Medicare Premiums (Part
A) - Hospital; (Part B) - Supplemental Ins. For Categorically Needy

Optional Medicaid ServicesOptional Medicaid Services Other Clinic Services Skilled Nursing Facility
Services for Individuals under 21 years of age
Podiatrist Services Optometrist Services Clinical Psychologist
Services Certified Pediatric Nurse
and Family Nurse Practitioner Services
Home Health: PT, OT, and Speech Therapy
Dental Services for Persons under 21
Physical Therapy & Related Services
Prescribed Drugs Case Management Services Prosthetics Mental Health Services Mental Health Clinic Services Hospice Services Medicare Part B Premiums for the
Medically Needy PACE

Accessing Accessing Specialized Services (cont.)Specialized Services (cont.)
EPSDT requests for state plan services will be rejected and referred to the existing Medicaid program
Service denials in other programs should be appealed as appropriate
EPSDT is not always an option for service or waiver denials

Is it on The List?Is it on The List?
All EPSDT or other treatment services provided through Medicaid must be defined in the
Social Security Act 1905 (a) The Social Security Act defines
which services that states may offer through their Medicaid program

Specialized ServicesSpecialized Services
The following Services are not covered under the State Plan and are covered only under EPSDT– Substance Abuse Treatment Services – Hearing Aids– Assistive Technology– Personal Care– Private Duty Nursing

Accessing Specialized Services Accessing Specialized Services
Fax Specialized Services requests to EPSDT Coordinator @ (804)786-5799
EPSDT Requests must contain the following:– Request form (DMAS-412 or 351)– Letter of Medical need (DMAS-352 or 353)– Evaluation from specialist (discipline specific)– Treatment plan (from relevant provider)– Description of service requested and why
established programs do not meet this need
Medical NecessityMedical Necessity
The medical justification for a service must accompany the request for EPSDT treatment services.
Certain services may not be covered by EPSDT– Respite– Environmental Modifications– Vocational– Educational

EPSDT and MedicaidEPSDT and MedicaidProgram Criteria ExamplesProgram Criteria Examples
When services for children are reviewed in any state plan service such as the DME program then EPSDT program criteria is used to determine medical necessity
Programs that are exempt from EPSDT criteria:– Eligibility criteria for HCBC waivers– Eligibility criteria for inpatient psychiatric– Eligibility criteria are not required to
change the program criteria for individual needs (EG: Autism and IIH)
Take 5Take 5

EPSDT is Part of the Early EPSDT is Part of the Early Intervention NetworkIntervention Network
By learning how to access all available Medicaid services, Early Intervention can be provided efficiently to children by using Medicaid resources
Even using EPSDT Medicaid cannot pay for services that are not eligible for CMS reimbursement

What Fits?What Fits?
Part C is related to IDEA Medicaid cannot not pay for
services available through IDEA Virginia Medicaid does not enroll
Special Educators as health service providers

Services: Part C Services: Part C What does Medicaid cover?What does Medicaid cover?
Assistive Technology Audiology Health Services/Nursing Services Medical Services (= EPSDT!!) Nutrition Services

OT PT Psychological Services (limited)
– Home Based Psych Services/Parent Training (Collaborative)
ST Transportation (covered to Medicaid
covered services)– Mileage is not reimbursable
Vision- Screenings and Glasses, OT visits are covered in Medicaid
Services: Part C Services: Part C What does Medicaid cover? Cont.What does Medicaid cover? Cont.

What is Part C Funded?What is Part C Funded?
Family Training, Counseling and Home visits
Respite Care Service Coordination Social Work Special Instruction (some exceptions
with therapies) Transportation to non-Medicaid
Services

EPSDTEPSDTSpecialized ServicesSpecialized Services
Periodic, Inter-periodic or partial screenings may be used to document the need for EPSDT treatment
Any caregiver or professional who comes in contact with the EPSDT enrollee may request an inter-periodic screening

Accessing Specialized Services Accessing Specialized Services
Fax Specialized Services requests to EPSDT Coordinator @ (804)786-5799
EPSDT Requests must contain the following:– Request form (DMAS-351)– Letter of Medical need– Evaluation from specialist (discipline specific)– Treatment plan (from relevant provider)– Description of service requested and why
established programs do not meet this need

Accessing Accessing Specialized Services (cont.)Specialized Services (cont.)
EPSDT requests for state plan services will be rejected and referred to the existing Medicaid program
Service denials in other programs should be appealed as appropriate
EPSDT is not always an option for service or waiver denials
Specific Program Specific Program GuidelinesGuidelines

Specialized ServicesSpecialized Services
The following Services are not covered under the State Plan and are covered only under EPSDT– Substance Abuse Treatment Services – Hearing Aids– Assistive Technology– Personal Care– Private Duty Nursing

Substance Abuse Substance Abuse Treatment ServicesTreatment Services

EPSDT Substance Abuse EPSDT Substance Abuse Treatment Services Treatment Services
Substance abuse treatment may be provided exclusively through EPSDT to eligible persons under age 21 who have demonstrated a medical need for clinically appropriate substance abuse treatment.

Referral ProcessReferral Process
MD authorization is mandatory
A clinical assessment by a licensed mental health professional is necessary to evaluate the need for treatment and develop a clinically appropriate treatment plan.

American Society of American Society of Addictions Medicine (ASAM)Addictions Medicine (ASAM)
DMAS currently uses ASAM patient placement criteria to determine clinical treatment levels and determine “medical necessity”

ASAM (cont.)ASAM (cont.)
DMAS uses ASAM criteria to guide the level of services that are pre authorized by DMAS
The ASAM guide has easy to use charts to describe clinically appropriate treatment per usage pattern and age

Substance Abuse TreatmentSubstance Abuse TreatmentPre AuthorizationPre Authorization
Services may be received until the pre authorization threshold is reached. The following is needed when requesting pre authorization:– DMAS-351– DMAS 412– Use the DMAS 352 or the 353 EPSDT screening
form for the MD referral– Clinical Assessment of need from LMHP– Treatment Plan from counselor– Provider identification number

Hearing/Audiology Hearing/Audiology ServicesServices

Covered Covered HearingHearing Services Services
Require MD referral and authorization by an audiologist
Analog and digital hearing aids are covered
FM systems are covered as necessary– Batteries are covered through the
DME program Cochlear implants are covered
through the surgical program-not EPSDT

Referral ProcessReferral Process MD referral to Otarlaryngologist or
Audiologist Items must be MD ordered using the
CMN DMAS-352 Preauthorization is required for digital
hearing aids, FM systems, and cochlear implants
Preuathorization is not required for analog hearing aids

Hearing ServicesHearing Services PA Forms PA Forms
DMAS 351 Request form DMAS 352/DMAS 353 is the CMN Audiogram DMAS 352/DMAS 353 Detailed description of item(s) Itemized quote/invoice cost

Assistive TechnologyAssistive Technology

Assistive TechnologyAssistive Technology
Request through KEPRO under the durable medical equipment (DME) program
DMAS 351 is the request form DMAS 352 denotes MD order Evaluation from relevant therapist Itemized quote/invoice cost Detailed description of item(s) Description of functional benefits

Personal CarePersonal Care

Personal CarePersonal Care
The services will be provided to those individuals who have documented medical necessity for such care as a means to assist in maintaining and/or improving health status. Services are based on medical necessity and will not take the place of informal support systems.

Personal Care CriteriaPersonal Care Criteria
ADL dependency in three areas is mandatory to require personal care
Care need is not solely due to normal developmental milestones

Personal Care Personal Care ReferralsReferrals
MD referral documents need for personal care services
DMAS-7 used for initial assessment Send completed DMAS 7 to EPSDT
Coordinator Parents/caregivers will select a
personal care provider from available providers in the area

Personal Care Personal Care Pre- Auth FormsPre- Auth Forms
DMAS 351 A DMAS 7 (refer to handouts) is
needed to demonstrate the medical necessity
UAI from VDH screening team (if denied waiver services) or
LOF if on MR/DD waitlist

Personal CarePersonal Care Forms (cont) Forms (cont)
Need 97A/B from provider (Plan of Care) Need 99A/B from provider (nursing
Assessment of need) Submit detailed schedule outlining specific
times and duties of aide including other active services for the child
*A waiver denial is not necessary to initiate personal care services

EPSDT NursingEPSDT Nursing

EPSDT NursingEPSDT Nursing
EPSDT nursing is defined as continuous nursing deemed necessary by the attending physician for assessing and monitoring the primary medical condition, providing interventions, and communicating with the physician regarding changes in the individual's medical status.

EPSDT NursingEPSDT Nursing
Persons who are eligible for nursing services are individuals who:– Require the skilled intervention or medical
monitoring from a medical professional in order to maintain physical health or to prevent imminent physical harm.
– Do not meet criteria to receive nursing via Home Health Program or HCBS Waivers

EPSDT NursingEPSDT Nursing
Children who are eligible nursing via one of the HCBS Waivers will be informed about the availability of those services
The MD will decide whether to refer for home health or EPSDT nursing services

EPSDT Nursing EPSDT Nursing Pre Auth FormsPre Auth Forms
DMAS 351 is the request form Physician-signed nursing plan of care Plan of care must be signed within 10 of
requested start date. Send EPSDT nursing assessment or MD
orders on a CMS 485 or equivalent Assess primary insurance as appropriate
for nursing care Include schedule of services that are
currently active.


Take 5Take 5

BabyCareBabyCare
Spring 2006Spring 2006
Department of Medical Assistance Services
BabyCareBabyCareOverview Overview PurposePurposeEligibilityEligibilityDefinitionsDefinitionsProvidersProvidersFAMIS MOMSFAMIS MOMSManaged Care Organization High Risk Maternity Managed Care Organization High Risk Maternity and Infant Programsand Infant ProgramsCovered ServicesCovered Services Maternal Infant Care Coordination (MICC)Maternal Infant Care Coordination (MICC) Expanded Prenatal ServicesExpanded Prenatal Services
Fit with Part CFit with Part C

Overview of BabyCareOverview of BabyCare
High risk pregnant mothers and high risk infants High risk pregnant mothers and high risk infants may receive intensive case management may receive intensive case management services which will be referred to as Maternal services which will be referred to as Maternal and Infant Care Coordination (MICC).and Infant Care Coordination (MICC).
Pregnant mothers (regardless of enrollment in Pregnant mothers (regardless of enrollment in MICC) are eligible for additional services called MICC) are eligible for additional services called “Expanded Prenatal Services”. Infants do not “Expanded Prenatal Services”. Infants do not qualify for expanded prenatal services. qualify for expanded prenatal services.

The Purpose of BabyCareThe Purpose of BabyCare
To reduce infant mortality and morbidity,To reduce infant mortality and morbidity,
To ensure provision of comprehensive To ensure provision of comprehensive services to pregnant women and infants services to pregnant women and infants up to age two, andup to age two, and
To assist pregnant women and To assist pregnant women and caretakers of infants in receiving wrap-caretakers of infants in receiving wrap-around services that affect their well-around services that affect their well-being and that of their families.being and that of their families.

Who can provide BabyCare?Who can provide BabyCare?
Community Health Community Health CentersCenters
Local Health Local Health DepartmentsDepartments
Rural Health ClinicsRural Health Clinics
Home Health Home Health AgenciesAgencies
Personal Care Personal Care AgenciesAgencies
PhysiciansPhysicians
Outpatient HospitalsOutpatient Hospitals
Local Departments of Local Departments of Social ServicesSocial Services
Community Service Community Service BoardsBoards
Providers who have signed an agreement with DMAS. Providers may include but not limited to:

BabyCare EligibilityBabyCare Eligibility
Fee for service eligible:Fee for service eligible: Pregnant Women up to 60 days Pregnant Women up to 60 days
postpartumpostpartum
Must be pregnant at enrollmentMust be pregnant at enrollment
Infants up to age 2Infants up to age 2

Check Medicaid Eligibility!Check Medicaid Eligibility!Providers must verify eligibility at each Providers must verify eligibility at each point of service.point of service.
Managed Care Organizations may not Managed Care Organizations may not reimburse for services not authorized by reimburse for services not authorized by non-participating providers.non-participating providers. http://virginia.fhsc.comhttp://virginia.fhsc.com MediCallMediCall
1-800-884-97301-800-884-9730
1-800-772-99961-800-772-9996

FAMIS MOMSFAMIS MOMSEffective August 1, 2005.Effective August 1, 2005.
Provides coverage for pregnant Provides coverage for pregnant women whose income is above women whose income is above 133% of poverty up through 150%.133% of poverty up through 150%.
Provides enrollees the same Provides enrollees the same coverage that pregnant women coverage that pregnant women currently receive from the Virginia currently receive from the Virginia Medicaid Program, including Medicaid Program, including BabyCare.BabyCare.
Providers use same billing codes Providers use same billing codes and procedures.and procedures.

FAMIS MOMSFAMIS MOMS
The main difference between FAMIS The main difference between FAMIS MOMS and Medicaid is that the infant is MOMS and Medicaid is that the infant is not automatically enrolled in Medicaid and not automatically enrolled in Medicaid and an application MUST be completed in the an application MUST be completed in the month they were born.month they were born. If not completed within birth month, the baby’s If not completed within birth month, the baby’s
hospitalization is not covered.hospitalization is not covered.

Managed Care Organizations Managed Care Organizations (MCOs)(MCOs)
andandBabyCareBabyCare

MCOsMCOs
MCOs have their own high risk maternal and MCOs have their own high risk maternal and infant programs; however, may contract out infant programs; however, may contract out with other agencies to provide services.with other agencies to provide services.
MCOs are required to provide or arrange for MCOs are required to provide or arrange for services for pregnant women and children up services for pregnant women and children up to age 2 which are comparable to DMAS’s to age 2 which are comparable to DMAS’s BabyCare program as described in Virginia BabyCare program as described in Virginia Administrative Code.Administrative Code.

MCOsMCOs
Not all MCOs have the same program. Not all MCOs have the same program. They have flexibility to administer it in They have flexibility to administer it in different ways. different ways.
DMAS’s BabyCare providers may not DMAS’s BabyCare providers may not bill Medicaid for services if recipient is bill Medicaid for services if recipient is enrolled in a MCO, unless the provider enrolled in a MCO, unless the provider has contracted with the MCO. has contracted with the MCO.

Contact the individual MCO for Contact the individual MCO for specific information on their specific information on their
high risk maternalhigh risk maternal
and infant program.and infant program.

Fee-for-Service (FFS)Fee-for-Service (FFS)(Medicaid, Medallion, FAMIS and(Medicaid, Medallion, FAMIS and
FAMIS MOMS)FAMIS MOMS)
Maternal Infant Care Coordination Maternal Infant Care Coordination (MICC)(MICC)

What is MICC?What is MICC?Maternal Infant Care Coordination is the Maternal Infant Care Coordination is the intensive care coordination/case intensive care coordination/case management program with goals to management program with goals to improve birth outcomes by ensuring improve birth outcomes by ensuring pregnant women and infants receive all pregnant women and infants receive all the services they need. the services they need.

What is MICC?What is MICC?Service elements include the risk screen, Service elements include the risk screen, assessment, service planning, assessment, service planning, coordination and referral, follow-up and coordination and referral, follow-up and monitoring, and education and support monitoring, and education and support services.services.
(Assessment packet provided as (Assessment packet provided as handout)handout)

Primary Care ProvidersPrimary Care Providers
All providers must be enrolled as a All providers must be enrolled as a Medicaid provider:Medicaid provider:
PhysicianPhysician
Nurse PractitionerNurse Practitioner
Certified Nurse MidwifeCertified Nurse Midwife
Coming soon…Coming soon…Physician AssistantsPhysician Assistants
Role of theRole of thePrimary Care ProviderPrimary Care Provider
ID potential or existing problemsID potential or existing problems Maternal Risk Screen DMAS 16Maternal Risk Screen DMAS 16 Infant Risk Screen DMAS 17Infant Risk Screen DMAS 17
(Primary Care Provider is responsible for (Primary Care Provider is responsible for completing the risk screen.)completing the risk screen.)
Referral to a MICC programReferral to a MICC program
Assist in the development of the service Assist in the development of the service plan as neededplan as needed

MICC Care CoordinatorMICC Care CoordinatorServices are provided by:Services are provided by:
Registered Nurse – must be licensed in VA Registered Nurse – must be licensed in VA and have a minimum of 1 year experience and have a minimum of 1 year experience in community health nursingin community health nursing
Social Worker – B.S.W. or M.S.W. and a Social Worker – B.S.W. or M.S.W. and a minimum of 1 year experience in a health minimum of 1 year experience in a health care settingcare setting
Both RN and SW must have 1 year Both RN and SW must have 1 year experience working with women and infants experience working with women and infants
Agencies must be enrolled as BabyCare Agencies must be enrolled as BabyCare ProviderProvider

MICC ServicesMICC Services
Care Coordination/Case ManagementCare Coordination/Case Management
NutritionNutrition Both pregnant mother and infant should be referred to Both pregnant mother and infant should be referred to
Women, Infant, and Children (WIC)Women, Infant, and Children (WIC)
Assist with complianceAssist with compliance
Refer maternal patients with high risk conditions to Refer maternal patients with high risk conditions to expanded prenatal services expanded prenatal services
Refer high risk infants to EPSDTRefer high risk infants to EPSDT
MICC ServicesMICC Services
Patient EducationPatient Education Education about the PregnancyEducation about the Pregnancy
Education about Infant CareEducation about Infant Care

Discharges from MICCDischarges from MICC
60 days 60 days postpartumpostpartum
Infant reaches Infant reaches age 2age 2
Individual enters Individual enters MCOMCO
Reasons for ending MICC eligibility (not limited too):
Goals met (no longer need for service)Drop out of programNo longer meet criteria

Expanded Medicaid Expanded Medicaid ServicesServices
for Pregnant Womenfor Pregnant Women

Expanded Medicaid ServicesExpanded Medicaid Servicesfor Pregnant Womenfor Pregnant Women
Patient EducationPatient Education
Nutrition ServicesNutrition Services
Homemaker ServicesHomemaker Services
Substance Abuse TreatmentSubstance Abuse Treatment

Patient EducationPatient Education
Patient EducationPatient Education
Childbirth classes (limit 6 per pregnancy)Childbirth classes (limit 6 per pregnancy)
Smoking cessation (limit 6 per pregnancy)Smoking cessation (limit 6 per pregnancy)
Parenting classes (limit 6 per pregnancy)Parenting classes (limit 6 per pregnancy)
Instruction must be rendered by Medicaid Instruction must be rendered by Medicaid certified providers who have appropriate certified providers who have appropriate education, license, or certification. education, license, or certification.

Nutritional ServicesNutritional ServicesAll pregnant women are expected to receive All pregnant women are expected to receive
basic nutrition information from their medical basic nutrition information from their medical care providers or the WIC programcare providers or the WIC program
Specialized Nutritional Services include:Specialized Nutritional Services include: Nutritional Assessment (1)Nutritional Assessment (1) Nutritional Counseling (1)Nutritional Counseling (1) Counseling Follow Up (1)Counseling Follow Up (1)
Provider must be Registered Dietician (R.D.) Provider must be Registered Dietician (R.D.) or person with a masters degree in nutrition or or person with a masters degree in nutrition or clinical dieteticsclinical dietetics

Homemaker ServicesHomemaker Services
Homemaker ServicesHomemaker Services Includes those services necessary to Includes those services necessary to
maintain household routine for pregnant maintain household routine for pregnant women, primarily in third trimester, who women, primarily in third trimester, who need bed rest (as ordered by Physician)need bed rest (as ordered by Physician)
Aides may include companion, Aides may include companion, homemaker, nursing assistant or home homemaker, nursing assistant or home health aide (RN or LPN must provide health aide (RN or LPN must provide supervision) supervision)

Substance Abuse Treatment for Substance Abuse Treatment for Pregnant and Postpartum WomenPregnant and Postpartum Women
Residential and Day Treatment Services Residential and Day Treatment Services include services for Substance Abuse include services for Substance Abuse Treatment for Pregnant and Postpartum Treatment for Pregnant and Postpartum WomenWomen
Community Mental Health Rehabilitative Community Mental Health Rehabilitative Services Manual, Chapter IVServices Manual, Chapter IV

Assessments to determine level of Assessments to determine level of need shall use the need shall use the American Society American Society of Addiction Medicine (ASAM), of Addiction Medicine (ASAM), Patient Placement Criteria for the Patient Placement Criteria for the Treatment of Substance-Related Treatment of Substance-Related Disorders, Disorders, Second Edition, as Second Edition, as amended.amended.
Level of NeedLevel of Need

Substance Abuse Substance Abuse Residential Treatment Residential Treatment
for Pregnant Women (H0018-HD)for Pregnant Women (H0018-HD)
Comprehensive intensive intervention Comprehensive intensive intervention services in residential facilities, OTHER services in residential facilities, OTHER than inpatient facilities, for pregnant & than inpatient facilities, for pregnant & postpartum women with serious postpartum women with serious substance abuse problemssubstance abuse problems

Residential Treatment Residential Treatment LimitationsLimitations
Limit of 300 days per Limit of 300 days per pregnancy, not to exceed 60 pregnancy, not to exceed 60
days postpartum.days postpartum.

Substance AbuseSubstance Abuse Day Treatment Day Treatment
for Pregnant Women (H0015-HD)for Pregnant Women (H0015-HD)
Intervention services in a central location Intervention services in a central location lasting two or more consecutive hours per day, lasting two or more consecutive hours per day, which may be scheduled multiple times per which may be scheduled multiple times per week for pregnant and postpartum women with week for pregnant and postpartum women with serious substance abuse problems. serious substance abuse problems.

Day Treatment: LimitationsDay Treatment: Limitations
A billing UNIT is a minimum of A billing UNIT is a minimum of 2, but less than 4 hours.2, but less than 4 hours.
Limit of 400 UNITS per Limit of 400 UNITS per pregnancy, not to exceed 60 pregnancy, not to exceed 60 days postpartum.days postpartum.

BabyCare and Part CBabyCare and Part CHow do they fit?How do they fit?
Targeted Case ManagementTargeted Case Management BabyCareBabyCare
MICCMICC Community Mental Health Rehab ServicesCommunity Mental Health Rehab Services
Serious Emotional DisturbanceSerious Emotional Disturbance Birth through age 17Birth through age 17
At Risk of Serious Emotion DisturbanceAt Risk of Serious Emotion Disturbance Birth through age 7Birth through age 7
Service may be provided simultaneously, Service may be provided simultaneously, however must have clear documentation of however must have clear documentation of unduplicated services.unduplicated services.Communication with your local agencies!Communication with your local agencies!

ContactsContacts
CMHCMH
Candice ChavisCandice Chavis
804-786-2160804-786-2160
[email protected]@dmas.virginia.gov
William O’BierWilliam O’Bier
804-225-4050804-225-4050
[email protected]@dmas.virginia.gov

ContactsContacts
BabyCareBabyCare
Ashley BartonAshley Barton
804-371-7824804-371-7824
[email protected]@dmas.virginia.gov