med. j. ivory exostosis of the skull
TRANSCRIPT
POSTGRAD. MED. J. (1965), 41, 277
IVORY EXOSTOSIS OF THE SKULL
PETER G. BULLOUGH, M.B., Ch.B.,The Nuffield Department of Orthopcedic Surgery, University of Oxford.
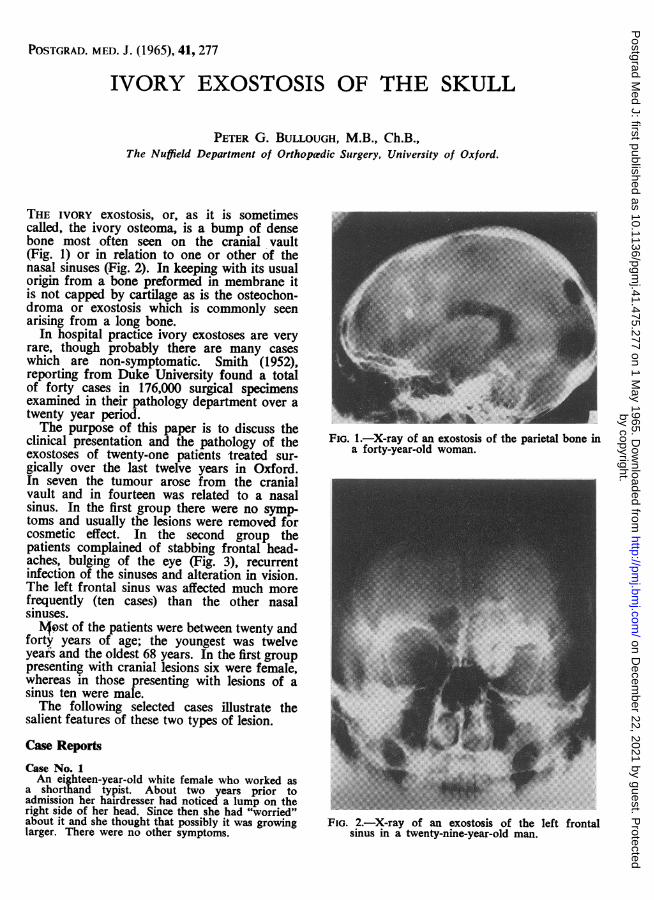
THE IVORY exostosis, or, as it is sometimescalled, the ivory osteoma, is a bump of densebone most often seen on the cranial vault(Fig. 1) or in relation to one or other of thenasal sinuses (Fig. 2). In keeping with its usualorigin from a bone preformed in membrane itis not capped by cartilage as is the osteochon-droma or exostosis which is commonly seenarising from a long bone.
In hospital practice ivory exostoses are veryrare, though probably there are many caseswhich are non-symptomatic. Smith (1952),reporting from Duke University found a totalof forty cases in 176,000 surgical specimensexamined in their pathology department over atwenty year period.The purpose of this paper is to discuss the
clinical presentation and the pathology of theexostoses of twenty-one patients treated sur-gically over the last twelve years in Oxford.In seven the tumour arose from the cranialvault and in fourteen was related to a nasalsinus. In the first group there were no symp-toms and usually the lesions were removed forcosmetic effect. In the second group thepatients complained of stabbing frontal head-aches, bulging of the eye (Fig. 3), recurrentinfection of the sinuses and alteration in vision.The left frontal sinus was affected much morefrequently (ten cases) than the other nasalsinuses.Most of the patients were between twenty and
forty years of age; the youngest was twelveyears and the oldest 68 years. In the first grouppresenting with cranial lesions six were female,whereas in those presenting with lesions of asinus ten were male.The following selected cases illustrate the
salient features of these two types of lesion.
Case ReportsCase No. 1An eighteen-year-old white female who worked as
a shorthand typist. About two years prior toadmission her hairdresser had noticed a lump on theright side of her head. Since then she had "worried"about it and she thought that possibly it was growinglarger. There were no other symptoms.
FIG. 1.-X-ray of an exostosis of the parietal bone ina forty-year-old woman.
FIG. 2.-X-ray of an exostosis of the left frontalsinus in a twenty-nine-year-old man.
by copyright. on D
ecember 22, 2021 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.41.475.277 on 1 May 1965. D
ownloaded from

POSTGRADUATE MEDICAL JOURNAL
FIG. 3.-Clinical photograph of a twenty-six-year-oldwoman complaining of recurrent rhinitis anddiplopia. A large exostosis was removed fromthe right frontal sinus.
FIG. 4.-Macro-photograph of an exostosis removedfrom the right parietal bone of an eighteen-year-old girl. (H. & E. x4).
On examination there was slight tenderness overthe bump, the skin moved freely over it and X-rayexamination revealed an ivory osteoma of the parietalbone. Histologic examination revealed dense corticalbone but no other abnormality (Fig. 4).Case No. 2A seventeen-year-old white male working as a farm
labourer. Five years prior to admission he firstnoticed bulging of the left eye and at about the sametime he started to experience stabbing pains over theleft eye. His local doctor diagnosed the condition asmigraine and treated him with phenobarbitone. Aftersix months the pains ceased and did not return untiltwo months prior to admission. He had never hadfits.On examination the left eye was protuberant by
five millimetres. All the movements of the left eyewere slightly limited and there was diplopia at theextremes of gaze in all directions. An X-ray pictureof the skull showed a radio-opaque lesion of the leftethmoid sinus encroaching on the left orbit. Atoperation the tumour had eroded the orbital plateand the outer layer of the dura mater so that thearachnoid was in contact with the tumour. Thehistology of the lesion is illustrated in Figs. 6-10.
FIG. 5.-Photograph of the tumour removed fromthe left frontal sinus of a fifty-year-old man withrecurrent sinusitis.
FIG. 6.-Macrophotograph of an exostosis removedfrom the left ethmoid sinus of a seventeen-year-old boy complaining of headaches and bulgingof the left eye for approximately five years.(H. & E. x4).
278 May, 1965by copyright.
on Decem
ber 22, 2021 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.41.475.277 on 1 M
ay 1965. Dow
nloaded from

BULLOUGH: Ivory Exostosis of the Skull
-;*aT-" ^x*Krt^ -*;- t, ,,,"" r
. -*- ....
:-i-.b: o :,:..":
>*':'.
(a) (b)
FIGS. 7a & b.-Photomicrograph of the edge of the lesion shown in Fig. 5. There is a verymild chronic inflammatory infiltrate beneath the respiratory epithelium lining the sinus.Fig. 7b taken of the same field by polarized light shows the non-lamellar patttern of thecollagen in the bone matrix. (H. & E. x400).
Case No. 3A thirty-five-year-old white farmer. Two months
prior to admission he noticed that in order to keepthe sun out of his eyes it had become necessary totip his hat more and more. At the same time he hadnoticed some slight pain around the eye. At the eyehospital he was told that there was a slight displace-ment of the eye. Study of photographs taken twoyears before the onset of symptoms showed inretrospect that even then there had been somedisplacement.On examination it was found that there was a hard,
non-tender, bony lump in the supero-medial part ofthe right orbit. The proptometer reading was fifteenmillimetres on the right and thirteen millimetres onthe left. The X-ray picture showed a lobulatedradio-opaque mass filling the right frontal sinus.At operation the lesion had eroded through the duramater. Histologic examination revealed an essentiallysimilar picture to the previous case except that thelaying down of lamellar bone in the central part ofthe lesion had proceeded somewhat further. He wasadmitted to hospital for a second time six monthslater with almost complete ptosis of the right eyelidand pain over the eye. An X-ray picture revealed thata good deal of the lesion still remained in the sinusand he was re-explored and the rest of the lesionremoved.
FIG. 8.-Photomicrograph of the central area of thelesion shown in Fig. 6. There is active osteo-clastic resorption of the non-lamellar bone in theupper right hand corner of the picture andreplacement by vascular fibrous tissue in whichlamellar bone trabeculae are being formed.(H. & E. xlOO).
May, 1965 279by copyright.
on Decem
ber 22, 2021 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.41.475.277 on 1 M
ay 1965. Dow
nloaded from
POSTGRADUATE MEDICAL JOURNAL
(hi
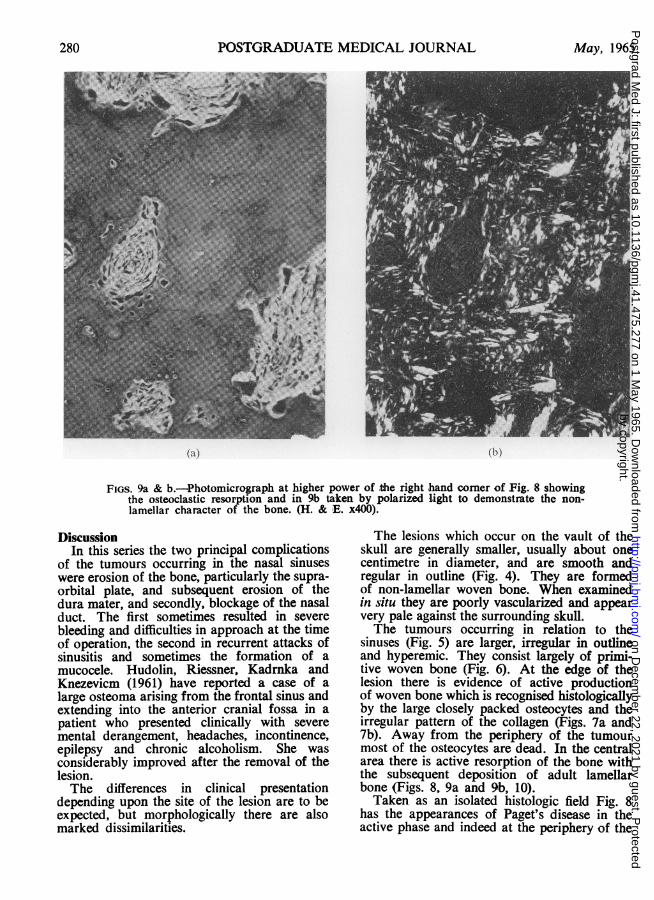
FIGS. 9a & b.-Photomicrograph at higher power of the right hand corner of Fig. 8 showingthe osteoclastic resorption and in 9b taken by polarized light to demonstrate the non-lamellar character of the bone. (H. & E. x400).
DiscussionIn this series the two principal complications
of the tumours occurring in the nasal sinuseswere erosion of the bone, particularly the supra-orbital plate, and subsequent erosion of thedura mater, and secondly, blockage of the nasalduct. The first sometimes resulted in severebleeding and difficulties in approach at the timeof operation, the second in recurrent attacks ofsinusitis and sometimes the formation of amucocele. Hudolin, Riessner, Kadrnka andKnezevicm (1961) have reported a case of alarge osteoma arising from the frontal sinus andextending into the anterior cranial fossa in apatient who presented clinically with severemental derangement, headaches, incontinence,epilepsy and chronic alcoholism. She wasconsiderably improved after the removal of thelesion.The differences in clinical presentation
depending upon the site of the lesion are to beexpected, but morphologically there are alsomarked dissimilarities.
The lesions which occur on the vault of theskull are generally smaller, usually about onecentimetre in diameter, and are smooth andregular in outline (Fig. 4). They are formedof non-lamellar woven bone. When examinedin situ they are poorly vascularized and appearvery pale against the surrounding skull.The tumours occurring in relation to the
sinuses (Fig. 5) are larger, irregular in outlineand hyperemic. They consist largely of primi-tive woven bone (Fig. 6). At the edge of thelesion there is evidence of active productionof woven bone which is recognised histologicallyby the large closely packed osteocytes and theirregular pattern of the collagen (Figs. 7a and7b). Away from the periphery of the tumourmost of the osteocytes are dead. In the centralarea there is active resorption of the bone withthe subsequent deposition of adult lamellarbone (Figs. 8, 9a and 9b, 10).Taken as an isolated histologic field Fig. 8
has the appearances of Paget's disease in theactive phase and indeed at the periphery of the
280 May, 1965by copyright.
on Decem
ber 22, 2021 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.41.475.277 on 1 M
ay 1965. Dow
nloaded from

May, 1965 BULLOUGH: Ivory Fxostosis of the Skull 281
'jj(C5 ;t-hIwwES-i
A|l '
FIG. 10.-Photomicrograph at higher power of thetrabeculk being laid down in the vascular fibroustissue illustrated in Fig. 8 to show the lamellarcharacter of the bone being formed. (H. & E.x400).
hypervascular fibrous zone there is even amosaic appearance. It is because of thisappearance that the lesion has been interpretedas fibrous dysplasia, localised leontiasis ossea*and Pagetoid bone. But in fact the histologicappearances are consistent with what we knowof the remodelling and replacement of wovenbone by lamellar bone in other situations, forexample, myositis ossificans circumscripta, orfracture callus (Collins and Curran, 1959).The hyperactive periosteum lays down a
bump of woven or non-lamellar bone whichacts as a calcified scaffold upon which thevascularized fibrous tissue can build the lamellarbone. The lesion therefore follows a generalrule that lamellar bone is only laid down ona pre-existing calcified framework, eithercalcified cartilage, calcified woven bone, or fociof dystrophic calcification.
In the ivory exostosis of the cranial vaultthe growth is probably very slow and the
substitution of the woven bone by lamellarbone occurs at a steady pace. Thus theselesions show mostly a lamellar pattern withonly occasional fragments of non-lamellar bone.On the other hand the lesions occurring inrelation to the sinuses have a more rapidgrowth and depending on the speed of growthand the age of the lesion will show differentproportions of the two types of bone. Becauseof their position the lesions of the sinuses willalso tend to draw attention to themselves muchsooner than the calvaral lesions.Both types of the tumour probably have
their origin in stimulation of the periosteumwhich lays down a non-lamellar type of bone.The stimulation is probably due to a develop-mental abnormality, trauma or possiblyinfection. Maxwell (1946) has suggested thatthe tumours found in relation to the paranasalsinuses are the result of a chronic proliferativeosteomyelitis secondary to sinus infection. Inthe cases reported here, however,- infection didnot seem to be a predisposing factor and thiswas also the experience of Andrew (1956).
Summary1. Twenty-one cases of exostosis of the
skull are presented. Fourteen cases were foundin relation to one or other of the paranasalsinuses, most frequently the left frontal sinus,and seven were on the cranial vault.
2. Depending upon the site the clinicalpresentation of the tumour differs.
3. The pathological appearance of thelesions also differs, both on gross and micro-scopic examination.
4. Despite the superficial dissimilaritiesevidence is presented to support the view thatthe exostosis of the cranial vault and of theparanasal sinuses are basically similar.
REFERENCESANDREW, J. (1956): Osteomata of the Paranasal
Sinuses, Brit. J. Surg., 43, 489.COLLINS, D. H., and CURRAN, R. C. (1959): Patho-
logical Ossification and Osseous Metaplasia inMan in 'Modern Trends in Pathology'; Chapter 15;London: Butterworth.
HUDOLIN, V., RIESSNER, D., KADRNKA, S., andKNEZEVICM (1%1): Osteoma in the AnteriorCranial Fossa, J. Neurol. Neurosurg. Psychiat.,24, 80.
MAXWELL, J. H. (1946): Chronic ProliferativeOsteomyelitis of the Skull, Ann. Otol. (St. Louis),55, 719.
SMITH, A. G., and ZAVALETA, A. (1952): Osteoma,Ossifying Fibroma, and Fibrous Dysplasia ofFacial and Cranial Bones, A.M.A. Arch. Path.,54, 507.
by copyright. on D
ecember 22, 2021 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.41.475.277 on 1 May 1965. D
ownloaded from