mechanisms of resistance
DESCRIPTION
mekanisme antibiotikTRANSCRIPT

Antibiotic Resistance:
An Introduction to Mechanisms
T. Mazzulli, MD, FRCPC, FACP
Microbiologist & Infectious Disease Consultant
Mount Sinai Hospital/University Health Network

Antibiotic
Mechanisms of Action and Resistance
Objectives1. Understand the factors affecting the interaction
between antimicrobial agents and infecting organisms
2. Recognize and explain (with examples) the phenotypic and genotypic mechanisms of resistance
3. Understand some key concepts related to mechanism of action and resistance of common antimicrobial agents


Mechanisms of Antimicrobial Resistance
1. Phenotypic
2. Genotypic

Phenotypic Mechanisms of Antimicrobial
Resistance
Mechanism Example
Enzymatic inactivation/inactivation of the drug Impermeable cell wall Efflux Target modification Target by-passing
Beta-lactamases Aminoglycoside-modifying enzymes Glycopeptides vs. Gram-negatives Imipenem-resistance in P. aeruginosa Most tetracycline resistance in Gram-negatives Multi-drug efflux in P. aeruginosa Quinolone resistance in S. aureus Glycopeptide resistance in enterococci Penicillin-resistance in pneumococci Methicillin-resistance in S. aureus Most anti-folate resistance
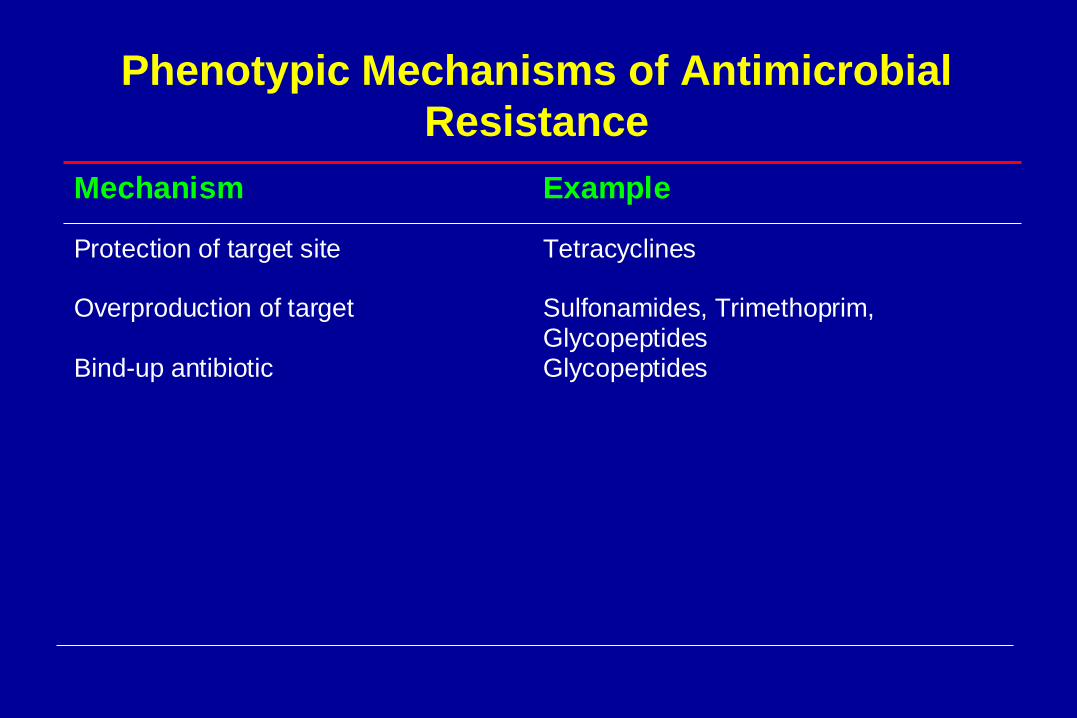
Phenotypic Mechanisms of Antimicrobial
Resistance
Mechanism Example
Protection of target site Overproduction of target Bind-up antibiotic
Tetracyclines Sulfonamides, Trimethoprim, Glycopeptides Glycopeptides

Genotypic Mechanisms of Antimicrobial
Resistance
2 key mechanisms:
1. Intrinsic (Primary)
2. Acquired (Secondary)

Genotypic Mechanisms of Antimicrobial
Resistance
1. Intrinsic Resistance:– Usually related to structural features
e.g. permeability of cell wall or target modification
– Chromosomally mediated
e.g. Pseudomonas aeruginosa, S. maltophilia, Enterococci, others
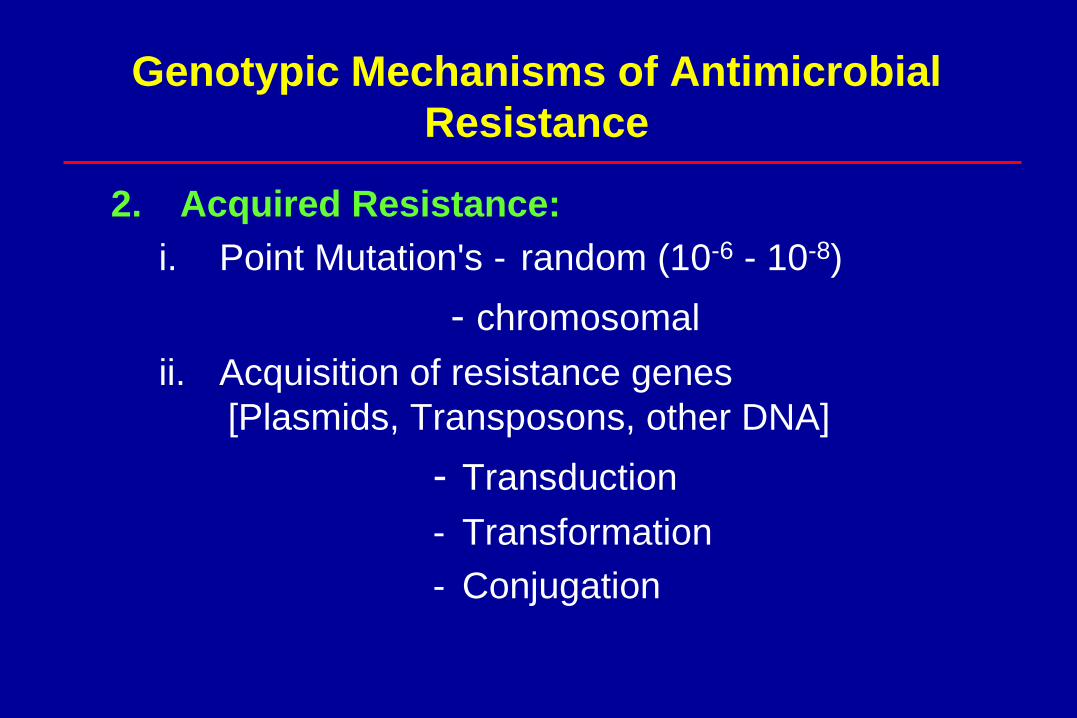
Genotypic Mechanisms of Antimicrobial
Resistance
2. Acquired Resistance:
i. Point Mutation's - random (10-6 - 10-8)
- chromosomal
ii. Acquisition of resistance genes
[Plasmids, Transposons, other DNA]
- Transduction
- Transformation
- Conjugation
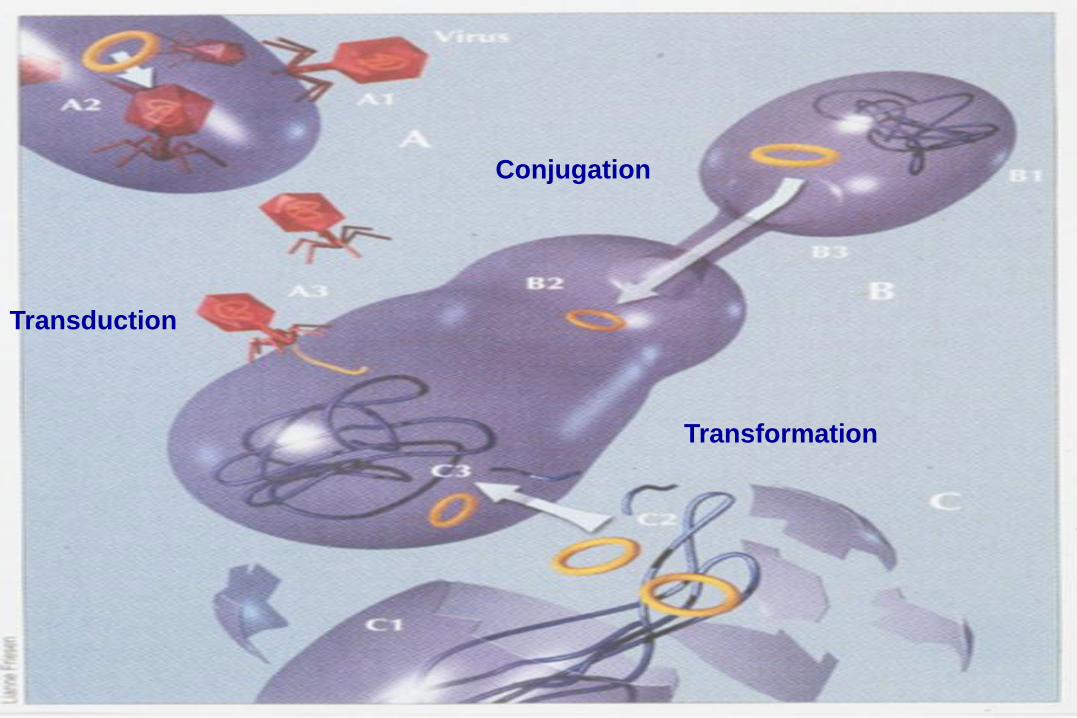
Transduction
Transformation
Conjugation
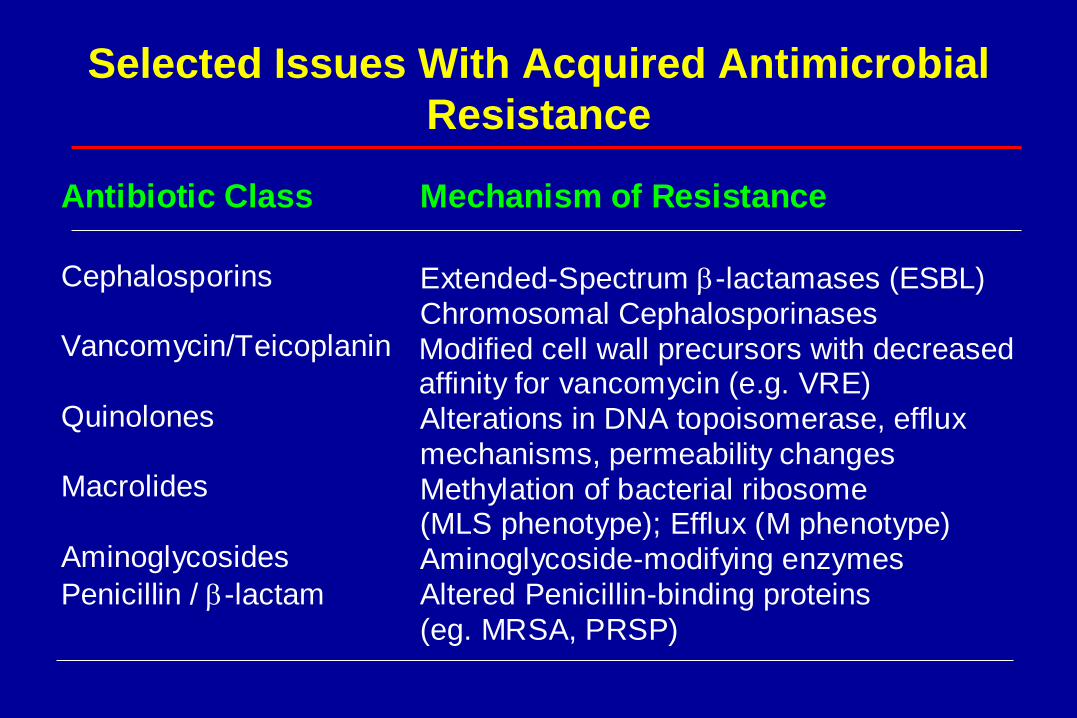
Selected Issues With Acquired Antimicrobial
Resistance
Antibiotic Class Mechanism of Resistance
Cephalosporins Vancomycin/Teicoplanin
Quinolones Macrolides Aminoglycosides
Penicillin / -lactam
Extended-Spectrum -lactamases (ESBL) Chromosomal Cephalosporinases Modified cell wall precursors with decreased affinity for vancomycin (e.g. VRE)
Alterations in DNA topoisomerase, efflux mechanisms, permeability changes Methylation of bacterial ribosome (MLS phenotype); Efflux (M phenotype) Aminoglycoside-modifying enzymes
Altered Penicillin-binding proteins (eg. MRSA, PRSP)

Resistance Due to Antibiotic Selection
Spontaneous
mutation occurs
in the absence
of drug
selection in a
sensitive
population
Drug
treatment
Mutant is selected
for by drug
treatment as
sensitive strains
die off
Resistant
clone grows
within what
used to be a
sensitive
population
Sensitive
bacteria
Resistant
bacteria
Resistant clone
becomes dominant
(may be multi-drug
resistant)
Dissemination of Resistant Bacteria
Resistant clone
spreads to other
patients &
contacts
Resistant clone
spreads to the
environment
Resistant clone results in
failure of therapy or re-
infection/relapse in the same
patient
Controlling Antimicrobial Resistance
• Reducing colonization and infection
• Reducing volume of antimicrobial use
• When decision made to treat
– Use right drug
– Right dose
– Right duration
Controlling Antimicrobial Resistance
Antimicrobial Stewardship Infection Control

Mechanisms of Antibiotic Resistance
1. Enzymatic inactivation:
• Beta-lactamases
• Aminoglycoside-modifying enzymes


Ambler Classification of Beta-Lactamases
Class Active Site Enzyme Type Substrates
A Serine Penicillinases
Broad Spectrum Pen. (all), Narrow Ceph.
ESBL Above plus 3rd Gen. Ceph, Aztreonam
Carbapen’ase Above plus Cephamycins,
Carbapenems
B Met-B-Lac (Zn2+) Carbapen’nase Above plus Cephamycins,
Carbapenems
C Serine Cephalosp’nase Extend. Spectrum + Cephamycins
D Serine Oxacillinases
Broad Spectrum Pen. (all), Narrow Ceph.
Extend. Spectrum Broad Spectrum + Monobactam
Carbapen’nase Extended Spectrum + Cephamycins,
Carbapenems
Jacoby GA et al. NEJM 2005;352

Bush-Jacoby-Medeiros Functional Classification of Beta-Lactamases
Group Enzyme Type Inhibited by Clavulanate Molecular Class
1 Cephalosporinase No C
2a Penicillinases Yes A
2b Broad Spectrum Yes A
2be Extended Spectrum Yes A
2br Inhibitor-Resistant Diminished A
2c Carbenicillinases Yes A
2d Cloxacillinase Yes D or A
2e Cephalosporinase Yes A
2f Carbapenemase Yes A
3 Carbapenemase No B
4 Penicillinase No A
Jacoby GA et al. NEJM 2005;352

Increase in numbers of Group 1, 2 and 3 β-
lactamases from 1970 to 2009
Group 1/class C cephalosporinases
Group 2/class A and class D β-lactamases
Group 3/class B metallo-
β-lactamases
Bush K and Jacoby G. AAC 2010

Group 1 (Class C) - Amp C -lactamases
• Cephalosporinases; chromosomally mediated; Inducible
• Typically found in Enterobacter, C. freundii, certain
indole-positive Proteae, Serratia, P. aeruginosa (not
Klebsiella or Salmonella spp.) - “SPICE” organisms
• Hydrolyzes penicillins, cephlalosporins, monobactams,
and cephamycins
• Resistant to -lactamase inhibitors
• Only carbapenems and cefepime are active (but
carbapenems and cefoxitins are strong inducers)
• May move onto plasmids and become constitutive

Group 1 (Class C) - Amp C -lactamases
• In E. coli, constitutive over expression of AmpC
β-lactamases can occur because of:
– mutations in the promoter and/or attenuator region
(AmpC hyperproducers)
– the acquisition of a transferable ampC gene on a
plasmid or other transferable elements (plasmid-
mediated AmpC β-lactamases)
Group 1 (Class C) - Amp C -lactamases
Laboratory implications:
• MICs > 8 ug/ml
• Easily identified in lab if expressed
– No “inducibility” test
Group 2 (Class A) -lactamases
• Dozens of enzymes; may be plasmid (constitutive)
or chromosomal (inducible)
• Non-essential enzymes
1. Broad Spectrum:
– PC1 in Staphylococcus aureus:
• Due to PC1
• Prevalence >95% worldwide
• Beta-lactamase stable penicillins (e.g. cloxacillin, nafcillin) and
beta-lactamase inhibitors are effective
• Hyperproduction results in “Borderline Oxacillin resistant S.
aureus” (BORSA) with MIC=4ug/ml; do not have the same
infection control implications as MRSA
Group 2 (Class A) -lactamases
1. Broad Spectrum:
– H. influenzae:
• Due to TEM-1 (90%) and ROB-1 (10%) beta-
lactamase
• Prevalence now 25-40% worldwide
• Initially more prevalent in serotype b strains
– M. catarrhalis:
• prevalence now >95% worldwide
• BRO-1 (predominates) and BRO-2 enzymes differing
by one amino acid
• Readily transferred by conjugation

Group 2 (Class A) -lactamases
1. Broad Spectrum:
– Most common -lactamases found in E. coli and K.
pnuemoniae are plasmid mediated TEM-1, TEM-2,
SHV-1
• Responsible for ampicillin resistance in E. coli &
ampicillin-cephalothin resistance in K.
pnuemoniae
• Susceptible to -lactamase inhibitors

Group 2 (Class A) -lactamases
2. Extended Spectrum (ESBLs):
– >20 derivatives of TEM; 6 derivatives of SHV; others
• Rapidly increasing are CTX-M -lactamases which were acquired
via plasmids from the chromosomal Amp C enzymes of Kluyvera
spp. (environmental gram negatives)
– Amino acid substitutions in area of -lactamases capable of
accommodating bulkier side chains of newer
cephalosporins & aztreonam
– Resistant to all penicillins, most inhibitor/drug combinations,
cephalosporins and aztreonam
– Carbapenems and cephamycins (cefotetan, cefoxitin) are
active in vitro
– Multi-resistant to other classes of drugs

Group 2 (Class A) -lactamases
2. Extended Spectrum (ESBLs):
– Predominant bugs: E. coli & K. pnuemoniae
– Occasionally found in K. oxytoca, K. ozaenae,
Serratia marcescens, Enterobacter, Salmonella,
Proteus, Citrobacter, Morganella morganii
Extended Spectrum Beta-lactamases (ESBLs)
Laboratory implications:
• Modest increase in MICs (1 to 8 ug/ml)
• Difficulty in detecting them if only screening
with a single 3rd generation cephalosporin
(e.g. cefotaxime)
• New CLSI guidelines

Enterobacteriaceae: Breakpoints revised
Agent
CLSI 2009 CLSI 2010
S I R S I R
Cefazolin ≤8 16 ≥32 ≤1 2 ≥4
Cefotaxime ≤8 16-32 ≥64 ≤1 2 ≥4
Ceftriaxone ≤8 16-32 ≥64 ≤1 2 ≥4
Ceftazidime ≤8 16 ≥32 ≤4 8 ≥16
Aztreonam ≤8 16 ≥32 ≤4 8 ≥16
Cefipime ≤8 16 ≥32 ≤8 16 ≥32

Group 2 (Class A) -lactamases
3. Carbapenemases:
– KPC-1, KPC-2, KPC-3 in K. pneumoniae are most
prevalent:
• Now reported in many other gram negatives – E. coli,
Citrobacter, Enterobacter, Salmonella, Serratia, P. aeruginosa
• KPC enzymes are transferable on plasmids
– Hydrolyze carbapenems, broad-spectrum penicillins,
oxymino-cephalosporins, and cephamycins
– Not inhibited by -lactamase inhibitor combinations
– Subgroup 3b contains smaller group of MBLs that
preferentially hydrolyze carbapenems
• IMP & VIM enzymes most frequently in non-fermentative
bacteria but also in Enterobacteriaceae

Implications of B-lactamases in Gram Negatives
• ESBLs - consider all pencillins, cephalosporins & aztreonam as resistant; ? Beta-lactamase inhibitors
• AmpC - Enterobacter, Citrobacter & Serratia spp. -may develop resistance to 3rd Gen. Ceph within 3 to 4 days of therapy
• Salmonella & Shigella spp. should always be considered resistant to 1st & 2nd Gen. Ceph.
• For enterobacteriaceae: Cephalothin R = Cephalexin R but not Cefazolin R

Implications of B-lactamases in Gram Negatives
• 1st Gen. Ceph. - R: Citrobacter, Enterobacter,
Morganella, Providencia, Serratia, Proteus vulgaris,
Yersinia
• Ampicillin - R: Above plus Klebsiella
• 2nd Gen. Ceph. - R: Citrobacter, Enterobacter,
Serratia, (P. vulgaris - cefuroxime)
• Amox/Clav. - R: Citrobacter, Enterobacter, Serratia

Mechanisms of Antibiotic Resistance
1. Enzymatic inactivation:
• Beta-lactamases
• Aminoglycoside-modifying enzymes


Enterococcal Aminoglycoside-Modifying Enzymes
Organism Enzyme STREP GENT TOBRA AMIK
E. faecalis & faecium
6-AAD
+
-
-
-
3’-APH - - - +
2”-APH/ 6’-AAC
- + + +
E. faecium 6’-AAC* - - + +
4”-AAD - - + +
+ = synergy NOT achievable; - = synergy achievable with cell wall agent
*Intrinsic, chromosomally-mediated
Aminoglycoside
Mechanisms of Antibiotic Resistance
2. Target modification:
• Penicillin resistance in pneumococci (PRSP)
• Vancomycin resistant enterococci (VRE)
3. Target by-passing:
• Methicillin-resistance in S. aureus (MRSA)
-lactam Antimicrobials
Mechanism of Action:
• Target: penicillin binding proteins (PBP)
• PBPs are essential enzymes
(carboxypeptidases, transpeptidases &
transglycosylases) for building the bacterial
cell wall
• Multiple PBPs in different organisms

Glycopeptide Antimicrobials
Mechanism of Action:
– Exact mechanism of action not known
– Binds to terminal D-ala-D-ala residues of
cell wall components and prevents
incorporation of the subunit into the
growing peptidoglycan


-lactams Antimicrobials
2. Altered Target (Remodeling):
• S. pneumoniae: slow remodeling of PBPs (3 of
the 6 PBPs are altered - 1a, 2x, & 2b)
• Due to transformation of PBP genes via
scavenging of genetic material– Gradual increase in MICs (<0.06 to 0.5 / 1.0)
» 3 of 6 altered PBPs for Pen Resistance
» 2 of 6 altered PBPs for Ceph Resistance
• High Level resistance when MIC >4 ug/ml
• Concomitant resistance to other unrelated
classes of antibiotics (~10 to 15% are MDR)

Lab Implication of Penicillin Resistance
in S. pneumoniae
Source of isolate and
mode of therapy
Susceptibility
category
(MICs: µg/ml)
S I R
Meningitis isolates ≤0.06 .12 -1 ≥2
Non-meningitis isolates, oral ≤0.06 .12 -1 ≥2
Non-meningitis isolates,
parenteral
2 4 8
CLSI 2008. Performance Standards for Antimicrobial Susceptibility Testing;
Eighteenth Informational Supplement (M100-S18)
-lactams Antimicrobials
3. Target By-passing (Novel PBP):
• S. aureus- synthesis of a novel PBP 2a
(capable of continuing cell wall synthesis)
MRSA (encoded for by chromosomal mecA
gene)
• Hospital MRSA (multi-drug resistant) vs
Community MRSA (less drug resistant)

Classification of MRSA
US PFGE Canadian strain SCCmec Type PVL
USA 100 2 II -
USA 200 3 – 6 II -
USA 300 10 IVa +
USA 400 7 IVa +
USA 500 5 – 9 IV -
USA 600 1 II -
USA 700 - IV -
USA 800 2 IV -
USA 1000 - IV +
USA 1100 - IV +
Mechanisms of Antibiotic Resistance
4. Target modification and efflux:
• MLS antibiotics

MLS Antibiotics
• Macrolides - Erythromycin
- Azithromycin
- Clarithromycin
• Ketolides - Telithromycin
• Lincosamides - Clindamycin
• Streptogramins - Quinipristin /
Dalfopristin

Mechanism of Action & Resistance
• Interact with 50S ribosomal subunit (mainly with
23sRNA)
– Inhibition of bacterial protein synthesis
• Macrolides bind strongly to Domain V and weakly to
Domain II, whereas ketolides bind strongly to both
domains
• Do not induce target resistance nor are they
affected when it has been induced by others;
(Telithromycin not affected by efflux mechanism)

Mechanisms of Macrolide Action & Resistance
Cytoplasm
Ribosomes
50
30
50
30
50
30
Bacteria alter macrolide binding site
(ermAM gene, MLSB phenotype)
Macrolide unable to block protein synthesis
Macrolide
Bacteria activate efflux pumps
(mefE gene, M phenotype)
Macrolide excreted from cell

MLS Antibiotics – Mechanisms of Resistance
1. Target modification (erm genes):
• Inducible - S. pneumo - all MLS
- S. aureus - only M
• Constitutive
• Acquisition of a gene; one step
• MIC increases from < 0.5 to > 8.0
mg/L
MLS Antibiotics – Mechanism of Resistance
2. Efflux pump (mef genes):
• S. aureus - MS phenotype
• S. pneumo - MLS phenotype
• Rare in S. aureus
3. Inactivation:
• Rare in S. aureus
• Not seen in S. pneumoniae

0
10
20
30
40
50
No
. o
f S
train
s
Erythromycin MIC (g/mL)
mefE +ermB
ermB
mefE
None
Correlation Between Erythromycin
MIC and Resistance Mechanisms

MLS Resistance in S. pneumoniae
Cross-Resistance
Mechanism % of Macrolide
Resistance
Clindamycin Streptogramin
Altered target Efflux pump
45
55
Yes
No
Yes
No

MLS Resistance in S. aureus
Cross-Resistance
Mechanism % of
Macrolide
Resistance
Clindamycin Streptogramin
Altered target
Efflux pump
>98
Rare
Yes
No
Yes
Yes

Clinical Implications of MLS Resistance
• Macrolide Resistant / Clindamycin Sensitive:
• S. aureus - do not use clindamycin
(inducible resistance)
• S. pneumoniae - could use clindamycin
(efflux pump - no cross-resistance)

Mechanisms of Antibiotic Resistance
5. Target Modification:
– Fluoroquinolone resistance in S. pneumoniae
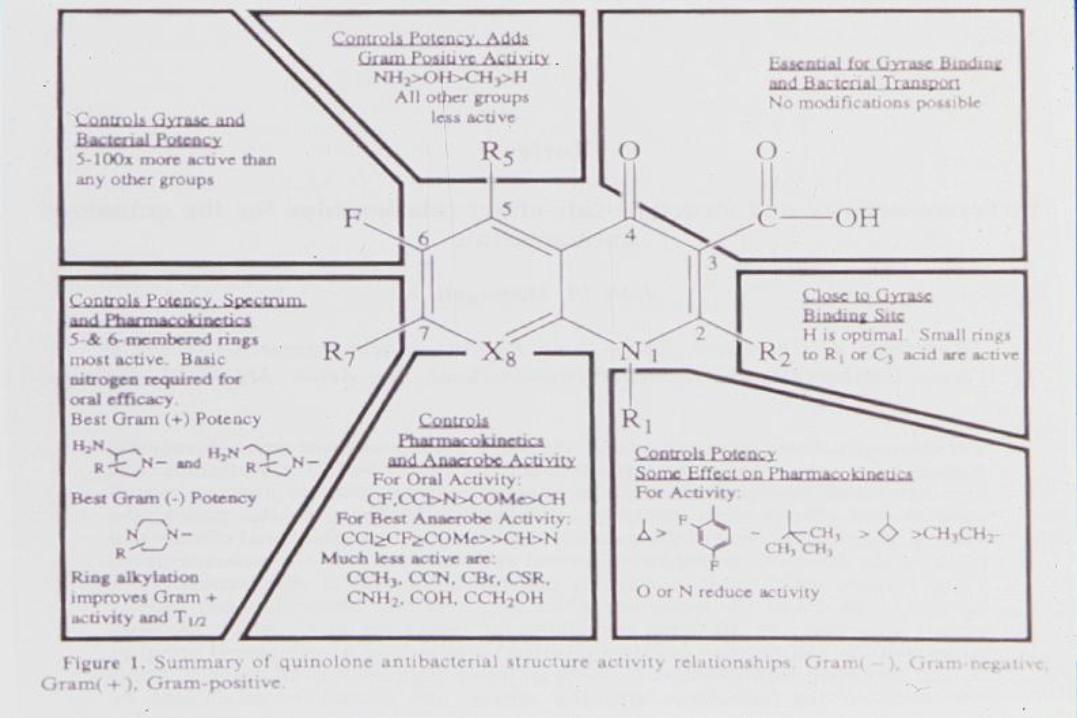

Fluoroquinolones
Mechanism of Action:
• Bind to 2 essential enzymes
• DNA gyrase (topoismerase II)
• Topoisomerase IV
• Results in termination of nucleic acid synthesis
and replication
• Bactericidal - kill both multiplying and resting
bacteria

Fluoroquinolones
Mechanism of Action:
• DNA gyrase (gyr A / gyr B)
• 10 target in gram neg
• 20 target in gram pos
• Topoisomerase IV (par C / par E)
• 10 target in gram pos
• 20 target in gram neg

Topoisomerases
• Enzymes which alter the number of times one
single strand of DNA duplex winds around its
complimentary strand
• Essential enzymes
• DNA replication, recombination, transcription
• Role in partitioning replicated chromosomes
Fluoroquinolones
Mechanism of Resistance:
1. Decreased permeability - low level resistance
2. Energy dependent efflux - low level resistance
3. Target modification - high level resistance
– Point mutations of gyr A & par C
– No plasmid (transferable) resistance until recently
Fluoroquinolones
Mechanism of Resistance:
• 1st / 2nd generation agents
• single mutations required for clinically
relevant resistance
• 3rd / 4th generation agents
• two mutations required for clinically
relevant resistance
Vancomycin Resistance
• Enterococcus
• S. aureus

Enterococci - Instrinsic Resistance (“Low level”)
• Penicillins and glycopeptides inhibit but do
not kill (MICs of 1 - 2 mg/L)
• Cephalosporins - uniformly resistant
• Vancomycin (Van C) - all E. flavescens, E.
casseliflavus, E. gallinarum; not transferable
• Aminoglycosides - poor drug uptake (MIC = 8
-256 mg/L)

Enterococci - Acquired Resistance (“High Level”)
• Beta-lactams - altered PBPs; MIC >128 mg/L
- beta-lactamase; plasmid, similar to
S. aureus (rare)
• Aminoglycosides - plasmid-mediated inactivating
enzymes; MIC >500 mg/L
• Vancomycin (& Teicoplanin) - Van A (transposon)
& Van B (chromosomal but
transferable by conjugation)
Implications of Enterococcal Resistance
• All cephalosporins are resistant
• High level aminoglycoside R - no synergy
• Quinapristin/dalfopristin (Synercid) - active against
E. faecium but not E. faecalis
• Linezolid active against both including VRE
• Nitrofurantoin for VRE in urine
• Altered PBPs also resistant to carbapenems

Classes of Vancomycin Resistance in
Enterococcus spp. & S. aureus
Vancomycin Teicoplanin
Class MIC ug/ml MIC ug/ml Inducible Location Species
A 64 to >500 (R) >32 (R) Yes P, C E. faecalis
E. faecium S. aureus
B >16-1024 (I,R)
<8 (S) Yes P, C E. faecalis
E. faecium
C 2 - 32 (I,R) 0.5 – 2 (S) No/Yes C E. galinarum
E. casseliflav
D 64 – 128 (R) 4 – 64 (S,I,R)
No C E. faecium
E 16 (I) 0.5 (S) Yes C E. faecalis
G 12 – 16 (I) 0.5 (S) ? C E. faecalis

Vancomycin Resistance
• Due to target alteration:
– D-ala-D-lac: Van A, B, D
– D-ala-D-ser: Van C, E, G
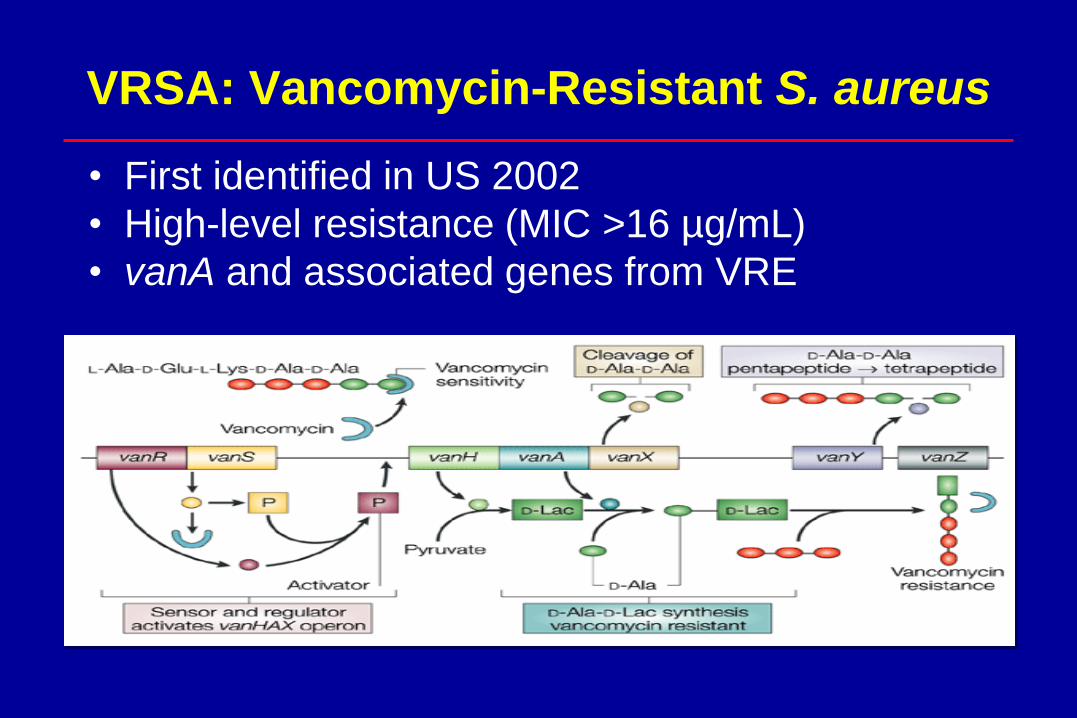
VRSA: Vancomycin-Resistant S. aureus
• First identified in US 2002
• High-level resistance (MIC >16 µg/mL)
• vanA and associated genes from VRE

Vancomycin and S. aureus Resistance
1. Vancomycin Intermediate S. aureus (VISA) &
Heteroresistant-VISA (hVISA):
• 1st case of VISA reported in Japan in 1997
• hVISA is a precursor of VISA:
– Heterogeneous pop’n of S. aureus with MIC of <2 ug/ml but
with non-susceptible subpopulations (MIC >4 ug/ml)
– 2.16% of MRSA and 0.05% MSSA strains (range 0% to
74%)
2. Vancomycin MIC Creep:
• Pop’n shift in MICs over time

S. aureus with Reduced Susceptibility to
Vancomycin
VISA: vancomycin-intermediate S. aureus
• Japan 1997 (Mu50)
• MIC 8 to 16 µg/mL
• Linked to cell wall thickening
hVISA: vancomycin heteroresistant
• Japan 1997 (Mu3)
• Subpopulations of cells in intermediate range
• MIC ≥4 µg/mL
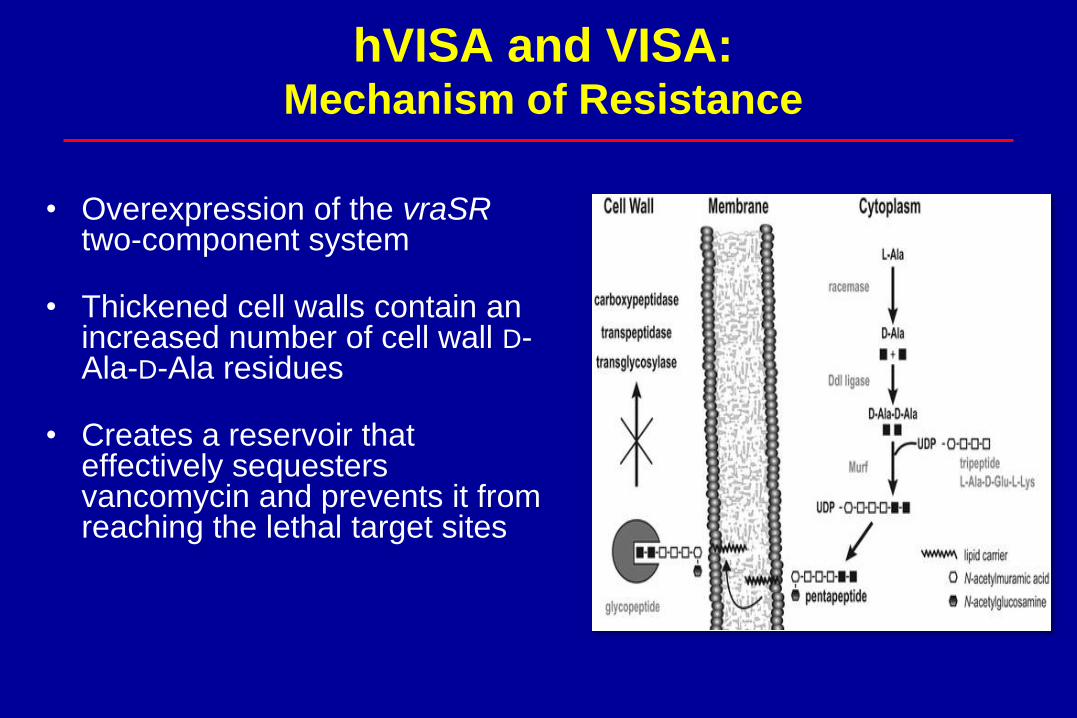
hVISA and VISA: Mechanism of Resistance
• Overexpression of the vraSRtwo-component system
• Thickened cell walls contain an increased number of cell wall D-Ala-D-Ala residues
• Creates a reservoir that effectively sequesters vancomycin and prevents it from reaching the lethal target sites

Vancomycin Breakpoints for S. aureus
• April 2008, FDA set new breakpoints for Vancomycin and are
consistent with those set by the CLSI in 2006
– Based on increasing reports of treatment failures, greater ability to detect
heterogeneously resistant isolates and reports of upward trend of vancomycin
MIC values in S. aureus
Drug
S, I, R Breakpoints (µg/ml)
CLSI (2006) FDA (Pre-2008)
Oxacillin ≤2, -, ≥4 ≤2, -, ≥4
Vancomycin ≤2, 4-8, ≥16 ≤4, 8-16, ≥32

Vancomycin Therapeutic Guidelines
• Vancomycin displays concentration-independent activity against S. aureus,
• AUC/MIC of 400 is the target
• A loading dose of 25–30 mg/kg should be considered
• Trough serum vancomycin concentrations
• Should be obtained just before the 4th dose
• 15–20 mg/L are recommended
• Dosages of 15–20 mg/kg q8–12h are required for most patients with normal renal function if MIC is <1 µg/mL
• If MIC >1 µg/mL, alternative agent recommended
Antibiotics - Summary
• Understanding mechanism of action / resistance should
allow selection of appropriate empiric therapy
• Pharmacokinetic / Pharmacodynamic properties important in
understanding how antibiotics work and implications of
resistance
• Low level resistance may be overcome with higher doses
(e.g. PRSP) or combination therapy (e.g. amp + gent)
• Co-resistance may or may not be predictable
• Susceptibility does not predict clinical success, but
resistance may increase likelihood of failure

Thank you for your attention!