mechanisms of action of antiseizure drugs and the
TRANSCRIPT

Mechanisms of Action of Antiseizure Drugsand the Ketogenic Diet
Michael A. Rogawski1, Wolfgang Loscher2, and Jong M. Rho3,4,5
1Department of Neurology, University of California, Davis, Sacramento, California 958172Department of Pharmacology, Toxicology, and Pharmacy, University of Veterinary Medicine,Hannover, Germany
3Department of Pediatrics, University of Calgary, Calgary, Alberta, Canada4Department of Clinical Neurosciences, University of Calgary, Calgary, Alberta, Canada5Department of Physiology and Pharmacology, University of Calgary, Alberta, Canada
Correspondence: [email protected]; [email protected]; [email protected]
Antiseizure drugs (ASDs), also termed antiepileptic drugs, are the main form of symptomatictreatment for people with epilepsy, but not all patients become free of seizures. The ketogenicdiet is one treatment option for drug-resistant patients. Both types of therapy exert theirclinical effects through interactions with one or more of a diverse set of molecular targetsin the brain. ASDs act by modulation of voltage-gated ion channels, including sodium,calcium, and potassium channels; by enhancement of g-aminobutyric acid (GABA)-medi-ated inhibition through effects on GABAA receptors, the GABA transporter 1 (GAT1) GABAuptake transporter, or GABA transaminase; through interactions with elements of the syn-aptic release machinery, including synaptic vesicle 2A (SV2A) and a2d; or by blockade ofionotropic glutamate receptors, including a-amino-3-hydroxy-5-methyl-4-isoxazole-propi-onate (AMPA) receptors. The ketogenic diet leads to increases in circulating ketones, whichmay contribute to the efficacy in treating pharmacoresistant seizures. Production in the brainof inhibitory mediators, such as adenosine, or ion channel modulators, such as polyunsat-urated fattyacids, mayalso playa role. Metabolic effects, including diversion from glycolysis,are a further postulated mechanism. For some ASDs and the ketogenic diet, effects onmultiple targets may contribute to activity. Better understanding of the ketogenic diet willinform the development of improved drug therapies to treat refractory seizures.
Antiseizure drugs (ASDs), often referred to asantiepileptic drugs or anticonvulsant drugs,
are administered chronically with the intent ofpreventing the occurrence of epileptic seizuresin a person at risk. Although limited resultsfrom animal studies or uncontrolled clinicalstudies suggest that some ASDs might have anti-epileptogenic actions (Kaminski et al. 2014),
there is insufficient evidence to conclude thatany ASD can produce clinically useful diseasemodification. The symptomatic relief from sei-zures that ASDs provide occurs through inter-actions with a variety of cellular targets. Theactions on these targets can be categorizedinto four broad groups: (1) modulation of volt-age-gated ion channels, including sodium, cal-
Editors: Gregory L. Holmes and Jeffrey L. Noebels
Additional Perspectives on Epilepsy: The Biology of a Spectrum Disorder available at www.perspectivesinmedicine.org
Copyright # 2016 Cold Spring Harbor Laboratory Press; all rights reserved; doi: 10.1101/cshperspect.a022780
Cite this article as Cold Spring Harb Perspect Med 2016;6:a022780
1
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
Press on December 16, 2021 - Published by Cold Spring Harbor Laboratoryhttp://perspectivesinmedicine.cshlp.org/Downloaded from

cium, and potassium channels; (2) enhance-ment of g-aminobutyric acid (GABA) inhibi-tion through effects on GABAA receptors, theGAT1 GABA transporter or GABA transami-nase; (3) direct modulation of synaptic releasethrough effects on components of the releasemachinery, including synaptic vesicle protein2A (SV2A) and the a2d subunit of voltage-gated calcium channels; and (4) inhibition ofsynaptic excitation mediated by ionotropic glu-tamate receptors, including a-amino-3-hydroxy-5-methyl-4-isoxazole-propionate (AMPA) re-ceptors (Table 1). The result of the interactionsat these diverse targets is to modify the intrinsicexcitability properties of neurons or to alter fastinhibitory or excitatory neurotransmission.These actions reduce the probability of seizureoccurrence by modifying the bursting proper-ties of neurons (reducing the capacity of neu-rons to fire action potentials at high rate) andreducing synchronization in localized neuronal
ensembles. In addition, ASDs inhibit the spreadof abnormal firing to adjacent and distant brainsites. This occurs through strengthening of theinhibitory surround, a function predominantlyof GABA released from interneurons acting onGABAA receptors, and by inhibition of gluta-mate-mediated excitatory neurotransmissionwithin the network of principal (relay) neurons.Some seizures, including typical generalized ab-sence seizures, result from elevated thalamo-cortical synchronization. ASDs effective againstthese seizure types interfere with the rhythm-generating mechanisms that underlie synchro-nized activity in the thalamocortical circuitry.In this review, we consider each of the principaltargets of ASDs and discuss how, to the extentknown, these agents affect the activity of thesetargets. The goal of epilepsy therapy is the com-plete elimination of seizures. This objective isnot achievable for many patients. When ASDsare not able to control seizures, some patients
Table 1. Molecular targets of clinically used ASDs
Molecular target ASDs that act on target
Voltage-gated ion channelsVoltage-gated sodium channels Phenytoin, fosphenytoin,a carbamazepine, oxcarbazepine,b
eslicarbazepine acetate,c lamotrigine, lacosamide; possiblytopiramate, zonisamide, rufinamide
Voltage-gated calcium channels (T-type) EthosuximideVoltage-gated potassium channels (Kv7) Ezogabine
GABA inhibitionGABAA receptors Phenobarbital, primidone, benzodiazepines, including
diazepam, lorazepam, and clonazepam; possiblytopiramate, felbamate, ezogabine
GAT1 GABA transporter TiagabineGABA transaminase VigabatrinSynaptic release machinerySV2A Levetiracetama2d Gabapentin, gabapentin enacarbil,d pregabalin
Ionotropic glutamate receptorsAMPA receptor PerampanelMixed/unknown Valproate, felbamate, topiramate, zonisamide, rufinamide,
adrenocorticotrophin
From Rogawski and Cavazos 2015; adapted, with permission.
GABA, g-Aminobutyric acid; GAT1, g-aminobutyric acid transporter 1; SV2A, synaptic vesicle protein 2A; AMPA,
a-amino-3-hydroxy-5-methyl-4-isoxazole-propionate.aFosphenytoin is a prodrug for phenytoin.bOxcarbazepine serves largely as a prodrug for licarbazepine, mainly S-licarbazepine.cEslicarbarbazepine acetate is a prodrug for S-licarbazepine.dGabapentin enacarbil is a prodrug for gabapentin.
M.A. Rogawski et al.
2 Cite this article as Cold Spring Harb Perspect Med 2016;6:a022780
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
Press on December 16, 2021 - Published by Cold Spring Harbor Laboratoryhttp://perspectivesinmedicine.cshlp.org/Downloaded from

may benefit from dietary therapies. The keto-genic diet is the most widely used and best val-idated such treatment approach. Here, we re-view a variety of theories to explain the actionof the ketogenic diet in the treatment of epilepsyranging from the view that the antiseizure ac-tivity relates to ketone bodies or the productionof inhibitory mediators, such as adenosine, tothe hypothesis that it is a result of shifts in in-termediary metabolism.
VOLTAGE-GATED ION CHANNELS
Voltage-Gated Sodium Channels
Voltage-gated sodium channels play an essentialrole in the initiation and propagation of actionpotentials in neurons (Mantegazza et al. 2010).Neuronal depolarizations by only a few mil-livolts, which ordinarily result from activa-tion of synaptic glutamate receptors (mainlyAMPA receptors, but also N-methyl-D-aspartate[NMDA] receptors), cause sodium channels toopen and enable influx of sodium along its elec-trochemical gradient. These channels then inac-tivate within milliseconds. The influx of sodiumions during the brief time that sodium channelsare open generates the depolarizing component(upstroke) of the action potential. Althoughnearly all sodium channels inactivate on depo-larization, �1% of the sodium current is non-inactivating, resulting in a small persistent so-dium current (INaP), which is carried by thesame channels as the fast transient current.INaP facilitates epileptic burst firing by reducingthe threshold for action potential generation,sustained repetitive firing, and augmentationof depolarizing synaptic currents (Stafstrom2007). Some ASDs, most notably phenytoin, in-hibit INaP, an action that is believed to contrib-ute to their efficacy (Mantegazza et al. 2010).
Voltage-gated sodium channels are multi-meric protein complexes, composed of a largea-subunit that forms four subunit-like homol-ogous domains (designated I–IV) and one ormore smallerb subunits (Meldrum and Rogaw-ski 2007). The ion-conducting pore is containedwithin the a-subunit, as are the elements of thechannel that mediate its fundamental physio-
logical properties, including rapid inactivation.The a subunits alone are able to form a func-tional sodium channel, but b subunits (b1–b4are known) can modulate the kinetics and traf-ficking of the channel (Patino and Isom 2010).Of the 10 known a subunits, using the channeland receptor nomenclature of Alexander et al.(2013), Nav1.1, Nav1.2, Nav1.3, and NaV1.6are the four most abundantly expressed sub-units in the brain (Yu and Catterall 2003; Vacheret al. 2008). Mutations in voltage-gated sodiumchannels have been associated with various ge-netic forms of epilepsy (Oliva et al. 2012).
ASDs that protect against seizures throughan interaction with voltage-gated sodium chan-nels are commonly referred to as “sodium chan-nel blockers” (Fig. 1). They are among the mostfrequently used drugs in the treatment of bothfocal and primary generalized tonic–clonic sei-zures. Such drugs include phenytoin, carba-mazepine, lamotrigine, oxcarbazepine (as wellas its active metabolite licarbazepine), rufina-mide, and lacosamide. ASDs that interact withvoltage-gated sodium channels also show acharacteristic “use-dependent” blocking actionso that they inhibit high-frequency trains of ac-tion potentials much more potently than theyattenuate individual action potentials or firingat low frequencies. Because they also show a“voltage-dependence” to their blocking action,sodium-channel-blocking ASDs are more po-tent at inhibiting action potentials superim-posed on a depolarized plateau potential ascharacteristically occurs with seizures. Thus,importantly, sodium-channel-blocking ASDspreferentially inhibit seizure discharges in rela-tion to normal ongoing neural activity. By vir-tue of their ability to inhibit the action potentialinvasion of nerve terminals, sodium-channel-blocking ASDs inhibit the release of diverse neu-rotransmitters, including glutamate; whetherthis is responsible for the therapeutic activityof the drugs remains uncertain (Waldmeieret al. 1995).
The binding site for sodium on sodium-channel-blocking ASDs is believed to overlapwith the binding site of local anesthetics, whichis within the pore of the channel and is formedby the S6 segments of domains I, II, and IV.
Antiseizure Drugs and the Ketogenic Diet
Cite this article as Cold Spring Harb Perspect Med 2016;6:a022780 3
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
Press on December 16, 2021 - Published by Cold Spring Harbor Laboratoryhttp://perspectivesinmedicine.cshlp.org/Downloaded from

Sodium-channel-blocking ASDs bind withhigher affinity to this site when the channel isin the inactivated state, and, when such a drug isbound, the channel is stabilized in the inactivat-ed state (Mantegazza et al. 2010). When neu-rons are depolarized and firing rapidly, sodiumchannels spend a greater amount time in theinactivated state and are able to accumulatebound drug so that they become trapped inthe inactivated state. This accounts for the use-and voltage-dependent blocking action thatthey show. Phenytoin, carbamazepine, and la-motrigine are considered “classical” sodium-channel-blocking ASDs. Lacosamide is also be-lieved to induce its therapeutic effects by inter-acting with sodium channels (Rogawski et al.2015). However, unlike other sodium-channel-blocking ASDs, lacosamide does not inhibithigh-frequency repetitive spike firing on thetime scale of hundreds of milliseconds. It does,however, inhibit spike firing in long trains ofspikes on the time scale of 1–2 sec. It has been
proposed that the very slow action of lacos-amide is caused by an enhancement of a distinctand poorly understood form of inactivation,referred to as “slow inactivation.” An alterna-tive explanation is that lacosamide binds moreslowly to fast-inactivated sodium channels thando the other sodium-channel-blocking ASDs.In any case, the unusually slow developmentof block produced by lacosamide during high-frequency activity could allow lacosamide tobetter discriminate between seizure-like patho-logical firing and normal network activity.
T-Type Voltage-Gated Calcium Channels
Low-voltage-activated (T-type) calcium chan-nels play a major role in the intrinsic thalamo-cortical oscillations that underlie the spike-wavedischarges of generalized absence seizures (Avoliet al. 2001; Huguenard 2002; Lambert et al.2014). There are three T-type Ca2þ channel iso-forms encoded by separate genes, denoted as
Perampanel
Levetiracetam
Voltage-gatedNa+ channel
Phenytoin, carbamazepine,lamotrigine, lacosamide,zonisamide, oxcarbazepine
Glutamate
SV2A
Felbamate
Gabapentin,pregabalin
α2δ subunitof P/Q-typeCa2+ channel
Ezogabine
Ezogabine
Presynaptic terminalof glutamate neuron
Postsynapticneuron
KV7 K+
channel
KV7 K+
channel
K+
K+
Na+ (Ca2+)
Na+
Na+ (Ca2+)
NMDAreceptor
AMPAreceptor
Figure 1. Diverse molecular targets for antiseizure drugs (ASDs) at excitatory glutamatergic synapses. Seizureprotection can be conferred by effects on voltage-gated sodium channels, M-type voltage-gated potassiumchannels (Kv7), and voltage-gated calcium channels located in presynaptic terminals. Additional presynaptictargets include the synaptic vesicle protein SV2A and the a2d accessory subunit of voltage-gated calciumchannels. These presynaptic targets may act to diminish glutamate release. Postsynaptic targets include iono-tropic glutamate receptors of the N-methyl-D-aspartate (NMDA) and a-amino-3-hydroxy-5-methyl-4-isoxa-zole-propionate (AMPA) types.
M.A. Rogawski et al.
4 Cite this article as Cold Spring Harb Perspect Med 2016;6:a022780
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
Press on December 16, 2021 - Published by Cold Spring Harbor Laboratoryhttp://perspectivesinmedicine.cshlp.org/Downloaded from

Cav3.1 (a1G), Cav3.2 (a1H), and Cav3.3 (a1I).All three T-type calcium channel isoforms areexpressed in thalamocortical circuits (Talleyet al. 1999). Cav3.1 is prominently expressedin thalamic relay neurons in the dorsal thala-mus, which plays a key role in absence seizures;Cav3.2—and to a lesser extent Cav3.3—areprominently expressed in thalamic reticularneurons. All three T-type calcium channel iso-forms are expressed in the cortex, with Cav3.2mainly localized to layer V. In non-REM sleep,including when d waves, sleep spindles, andK-complexes occur, the thalamocortical circuitswitches from a tonic to oscillatory mode offiring, but in absence epilepsy, this switchingcan occur inappropriately, even during wakeful-ness (Crunelli et al. 2014; Powell et al. 2014).T-type calcium channels in the thalamus andcortex contribute to the abnormal behaviorof the circuit. These channels generate low-threshold spikes, leading to burst firing and os-cillatory behavior (Suzuki and Rogawski 1989).GABAergic neurons of the thalamic reticularnucleus are also critically involved in absenceseizures as they hyperpolarize thalamic relayneurons, which de-inactivate T-type calciumchannels, allowing the channels to generateburst firing and the propagation of spike-wavedischarges in the thalamocortical circuit (Da-nober et al. 1998).
Ethosuximide, which is highly efficacious inthe treatment of absence seizures—but not oth-er seizure types—is thought to act by inhibitionof T-type calcium channels in the thalamo-cortical circuit (Coulter et al. 1989; Broicheret al. 2007; Goren and Onat 2007). At clinicallyrelevant concentrations (20–40 mg/ml), somebut not all investigators have observed a partial(20%–30%) reduction of T-type calcium cur-rent by ethosuximide. Notwithstanding thisdiscrepancy, studies with recombinant T-typecalcium channels have confirmed that ethosux-imide blocks all three channel types (Gomoraet al. 2001). The block increases when the cur-rent is activated from more depolarized poten-tials and when T-type calcium channels areinactivated, as occurs especially during high-frequency activation, so that the drug hasselectivity for pathological behavior in the tha-
lamocortical circuit, which is associated withneuronal depolarization and inactivation ofT-type calcium channels. Effects on other mem-brane currents, including INaP, calcium-activat-ed potassium current (Broicher et al. 2007), andinward rectifier potassium current (Huang andKuo 2015), may contribute to the efficacy ofethosuximide in absence epilepsy. Remarkably,results in animal models indicate that earlytreatment with ethosuximide can have disease-modifying (i.e., antiepileptogenic) effects, caus-ing a persistent reduction in seizures and miti-gation of behavioral comorbidities (Blumenfeldet al. 2008; Dezsi et al. 2013). These actions maybe caused by epigenetic modifications. A studyshowing that children with absence epilepsywho receive ethosuximide are more likely thanthose who receive valproate to achieve long-term remission is consistent with the disease-modifying actions observed in animal studies(Berg et al. 2014).
The efficacy of some other ASDs may alsodepend, at least in part, on actions at T-typecalcium channels. Zonisamide, in addition toeffects on voltage-gated sodium channels, mayalso block T-type voltage-gated calcium chan-nels (Powell et al. 2014), thus accounting forits likely efficacy in absence epilepsy (Hughes2009). Similarly, there is evidence that val-proate, a drug of choice in absence epilepsy,may also inhibit T-type calcium channels(Broicher et al. 2007).
Kv7 Voltage-Gated Potassium Channels
Voltage-gated potassium channels open in re-sponse membrane depolarization, permittingefflux of potassium ions, thus driving the mem-brane potential toward a hyperpolarized level.This serves to repolarize depolarizing events(such as action potentials and synaptic poten-tials) and cause a generalized reduction in ex-citability. In 1998, the first genes for a humanidiopathic epilepsy were identified (Charlieret al. 1998). These genes, designated KCNQ2and KCNQ3, encoded novel brain potassiumchannel subunits, Kv7.2 and Kv7.3, respectively,which are homologous to a previously identi-fied cardiac potassium channel Kv7.1, encoded
Antiseizure Drugs and the Ketogenic Diet
Cite this article as Cold Spring Harb Perspect Med 2016;6:a022780 5
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
Press on December 16, 2021 - Published by Cold Spring Harbor Laboratoryhttp://perspectivesinmedicine.cshlp.org/Downloaded from

by KCNQ1 (LQT1). These brain potassiumchannels mediate the M current, a potassiumcurrent that increases as the membrane poten-tial in neurons approaches action potentialthreshold. Kv7 channels, together with hyperpo-larization-activated cyclic nucleotide-gated po-tassium (HCN) channels and small-conduc-tance calcium-activated potassium (KCa/SK)channels, generate the medium after-hyper-polarization, which is elicited by a burst of ac-tion potentials and serves to limit further firing(Gu et al. 2005). Kv7 potassium channels alsoserve to counteract the spike after-depolariza-tion generated by recruitment of INaP, whichcan lead to bursting (Yue and Yaari 2006). Kv7potassium channels, therefore, act as a “brake”on epileptic burst firing. The Kv7 family of po-tassium channels is now known to contain fivemembers, including Kv7.1, which is expressedpredominantly in the heart and Kv7.2–Kv7.5,which are expressed exclusively in the nervoussystem (Brown and Passmore 2009). Of theseKv7 family members, Kv7.2 and Kv7.3 are high-ly expressed in neurons relevant to epilepsy,including principal (pyramidal) cells of thehippocampus and neocortex. Kv7.2 and Kv7.3compose heterotetrameric channels in whichfour subunits are arranged around a potassiumselective pore. Kv7.5 channels may also contrib-ute to M current and to neuronal after-hyper-polarization, for example, in the CA3 area of thehippocampus (Tzingounis et al. 2010).
Studies of the localization of Kv7.2 andKv7.3 potassium channels by immunohisto-chemical techniques have indicated that thechannels are present at highest density in axonsand their terminals (Vacher et al. 2008). In my-elinated fibers, they are present at nodes of Ran-vier and the channels are also expressed at axoninitial segments. In addition, the channels areexpressed at lower levels in the somata of prin-cipal neurons and in some GABAergic neurons.Physiological studies in CA1 pyramidal neuronsindicate that Kv7 channels are functionally ac-tive in the perisomatic region (Hu et al. 2007)and possibly also on distal dendrites (Yue andYaari 2006).
Ezogabine (retigabine), which is efficaciousin the treatment of focal seizures, acts as a pos-
itive modulator of the nervous system Kv7potassium channels (Kv7.2–Kv7.5), but doesnot affect the cardiac member of the family(Kv7.1) (Fig. 1). Of particular relevance to theantiseizure action of ezogabine is its action onthe M current, which is predominantly carriedby channels composed of Kv7.2 and Kv7.3,although Kv7.5 alone or in combination withKv7.3 also contributes (Rogawski 2006; Gun-thorpe et al. 2012). Ezogabine causes a hyper-polarizing shift in the activation of Kv7 channelssuch that more M current is generated near theresting potential. It also causes a change in thekinetics of single KCNQ channels to favor chan-nel opening, thus increasing the macroscopicM current; ezogabine, nevertheless, does notalter the single channel conductance of individ-ual Kv7 channels (Tatulian and Brown 2003).As noted, many Kv7 channels in the brain arebelieved to be Kv7.2/Kv7.3 heteromers, andthese are highly sensitive to ezogabine (EC50,1.6 mM) (Gunthorpe et al. 2012). Peak plasmalevels of ezogabine range from 354 to 717 ng/ml(1.2–2.4 mM) (Hermann et al. 2003), andplasma protein binding is 80% so that free plas-ma concentrations are estimated to be �0.2–0.5 mM; brain concentrations are expected to besimilar. Therefore, therapeutic concentrationslikely only modestly potentiate the most sen-sitive Kv7 channels and do not affect less sensi-tive channels. The binding site for ezogabine inKv7.2/Kv7.3 heteromers is in a pocket formedby the pore-lining S5 membrane segment ofone subunit and the pore-lining S6 membranesegment of the neighboring subunit (Wuttkeet al. 2005; Lange et al. 2009). Channel openingmay expose the pocket, permitting binding ofezogabine, which stabilizes the open channelconformation.
Several experimental approaches supportthe role of Kv7 potassium channels in the anti-seizure activity of ezogabine. Mice with a ge-netic defect in these channels show reducedsensitivity to the antiseizure effect of ezogabine(Gunthorpe et al. 2012). Furthermore, theKCNQ inhibitor, XE-991, partially blocks theantiseizure effect of ezogabine in an electricalseizure test (Gunthorpe et al. 2012). However,the precise way in which activation of Kv7 chan-
M.A. Rogawski et al.
6 Cite this article as Cold Spring Harb Perspect Med 2016;6:a022780
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
Press on December 16, 2021 - Published by Cold Spring Harbor Laboratoryhttp://perspectivesinmedicine.cshlp.org/Downloaded from

nels leads to seizure protection remains to beelucidated. Consistent with the presynaptic lo-calization of many Kv7 channels, ezogabine hasbeen found to inhibit the release of various neu-rotransmitters, including GABA and probablyalso glutamate (Martire et al. 2004). Inhibitionof glutamate release is expected to confer seizureprotection. The impairment of GABA releaseor the direct inhibition of inhibitory inter-neurons (Lawrence et al. 2006; Grigorov et al.2014) would be expected to enhance circuitexcitability. Indeed, in rodents, retigabine showsproconvulsant activity at doses (�61.9 mg/kg)that are approximately 10-fold greater thanthose associated with seizure protection (U.S.Food and Drug Administration 2010). Para-doxically, and in contrast to biochemical obser-vations, physiological studies have found thatezogabine “increases” glutamate-mediated syn-aptic transmission in the hippocampus througha presynaptic action by reducing the inactiva-tion of voltage-gated sodium channels so thatsodium-dependent action potentials are elic-ited with greater probability (Vervaeke et al.2006). This action could contribute to the pro-convulsant effects of the drug. If ezogabine doesconfer seizure protection through effects on ex-citatory neurons, postsynaptic actions to inhibitsomatic excitability likely predominate.
In addition to its effects on Kv7 potassiumchannels, ezogabine has been reported to inter-act with the GABA system. At high concen-trations (.10 mM), ezogabine was shown topotentiate GABA-mediated inhibitory trans-mission by acting as a positive allosteric mod-ulator of GABAA receptors (Rundfeldt andNetzer 2000; Otto et al. 2002). Recent evidencethat inhibitory effects of the drug on seizure-likeactivity in hippocampal neurons persist in thepresence of blockade of Kv7 channels has bol-stered the view that positive modulation ofGABAA receptors could be key to its antiseizureactivity (Treven et al. 2015). Thus, at lowerconcentrations than are required for effects onsynaptic GABAA receptors, ezogabine selective-ly enhances extrasynaptic GABAA receptors thatcontain the d-subunit (Treven et al. 2015). Ezo-gabine has also been reported to increase GABAsynthesis (Kapetanovic et al. 1995); the mecha-
nism and implications of this effect are notknown. In sum, various lines of evidence raisethe possibility that effects of ezogabine onGABA mechanisms could be of importance inits antiseizure activity.
GABA INHIBITION
GABA, the neurotransmitter of local inhibitoryinterneurons, acts through GABAA and GABAB
receptors. GABAA receptors, which are Cysloop-type ligand-gated chloride channels, rep-resent an important target for ASDs and willbe considered here. GABAB receptors, whichare heterodimeric G-protein-coupled receptorsthat activate potassium channels and inhibitcalcium channels, are distinct in structure andfunction from GABAA receptors and are not atarget of any ASD. Although only about one infive cortical neurons is GABAergic (Sahara et al.2012), these neurons play a critical role in con-trolling the firing rate and timing of principal(excitatory) neurons. In addition, they syn-chronize local neuronal ensembles and restrainthe generation of abnormal epileptic behavior.Consequently, enhancement of GABAergic in-hibition is a key mechanism of ASD action.
GABAA Receptors
GABAA receptors are heteropentameric proteincomplexes localized to the postsynaptic mem-brane of inhibitory synapses (Fig. 2) where theymediate fast neuronal inhibition on a millisec-ond timescale. They are also located extrasynap-tically where they respond to ambient GABA inthe extracellular milieu and confer tonic (long-term) inhibition. There are 19 known GABAA
receptor subunits (a1–6, b1–3, g1–3, d, 1, u,p, and r1–3) (Olsen and Sieghart 2009). How-ever, the bulk (60%) of synaptic GABAA re-ceptors are believed to have the a1b2g2 con-figuration, and a considerable fraction of theremainder (15%–20%) has a2b3g2. Amongthe receptor subtypes that contribute to tonicsignaling in brain regions relevant to epilepsyare a4bxd receptors, which are believed to me-diate the tonic current in dentate granule cellsand thalamocortical neurons, and a5-contain-
Antiseizure Drugs and the Ketogenic Diet
Cite this article as Cold Spring Harb Perspect Med 2016;6:a022780 7
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
Press on December 16, 2021 - Published by Cold Spring Harbor Laboratoryhttp://perspectivesinmedicine.cshlp.org/Downloaded from

ing GABAA receptors in CA1 pyramidal cells(Walker and Kullmann 2012).
Benzodiazepines, such a diazepam, loraze-pam, and clonazepam, and barbiturates, such asphenobarbital (Loscher and Rogawski 2012),are ASDs that act on GABAA receptors aspositive allosteric modulators (Fig. 2). At higherconcentrations, barbiturates can directly acti-vate GABAA receptors in the absence of GABA(Rho et al. 1996), whereas benzodiazepines can-not. Benzodiazepines are specific for synapticGABAA receptors containing the g2 subunitand act to allosterically modulate these recep-tors to increase the channel-opening frequency,resulting in enhanced synaptic inhibition. Thisconfers a broad-spectrum antiseizure action.In most epilepsy syndromes, the specific cellu-lar types that are involved in the antiseizureactivity of benzodiazepines are not known.However, in the case of absence epilepsy, itis believed that benzodiazepines desynchronizethe thalamocortical oscillations underlyinggeneralized spike-wave discharges by specificeffects on a3-containing GABAA receptors in
the thalamic reticular nucleus (Sohal et al.2003). Barbiturates, presumably because theyare not specific fora3-containing GABAA recep-tors, are not active in absence epilepsy and mayeven aggravate absence seizures. In contrast tobenzodiazepines, barbiturates do not appearto increase the frequency of GABA-inducedchloride channel opening, but instead increasethe channel open time. In addition to effectson GABAA receptors, barbiturates modulateother ion channel systems, including calciumand sodium channels, and these actions maycontribute to therapeutic activity (ffrench-Mul-len et al. 1993).
GAT1 GABA Transporter
The action of the neurotransmitter GABA isterminated by uptake into neurons and glialcells by membrane-bound GABA transporters,of which there are four types, termed GAT1,BGT1, GAT2, and GAT3. GAT1 (encoded bythe SLC6A1 gene), the predominant form inthe forebrain (including the neocortex and hip-
Phenobarbital
Presynaptic terminalof GABA neuron
GABA
GABA
GABA
GABA-TGABA
GABA-TSuccinicsemi-aldehyde
GAT1
Benzo-diazepines
Synapticvesicles
Tiagabine
Succinicsemi-aldehyde
Vigabatrin
Astrocyte
Postsynapticneuron
GADGlutamate
CI–CI–
SynapticGABAA receptor
ExtrasynapticGABAA receptor
Figure 2. Diverse molecular targets for antiseizure drugs (ASDs) at inhibitory g-aminobutyric acid (GABA)ergicsynapses. Seizure protection can be conferred by effects on synaptic or extrasynaptic GABAA receptors or onGABA transaminase (GABA-T) or GABA transporter 1 (GAT1). Furthermore, some ASDs (e.g., valproate) havebeen shown to increase the activity of the GABA-synthesizing enzyme glutamic acid decarboxylase (GAD),thereby increasing GABA turnover. Astrocytes contain elements, including GABA transporters, which influencethe dynamics of GABA, thereby affecting the excitability of the postsynaptic neuron.
M.A. Rogawski et al.
8 Cite this article as Cold Spring Harb Perspect Med 2016;6:a022780
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
Press on December 16, 2021 - Published by Cold Spring Harbor Laboratoryhttp://perspectivesinmedicine.cshlp.org/Downloaded from

pocampus), is localized to GABAergic termi-nals, as well as to glial processes near GABAsynapses (Fig. 2). Tiagabine is a highly selectiveinhibitor of GAT1 in neurons and glia (Schous-boe et al. 2014). Inhibition of GAT1 by tiagabinesuppresses the translocation of extracellularGABA into the intracellular compartment, thusraising extracellular GABA levels. Functionally,tiagabine prolongs GABA-mediated inhibitorysynaptic responses (Thompson and Gahwiler1992) and the marked elevation in extracellularGABA it produces may lead to activation of ex-trasynaptic GABA receptors.
GABA Transaminase
4-Aminobutyrate aminotransferase (GABAtransaminase), an enzyme that catalyzes theconversion of GABA and 2-oxoglutarate intosuccinic semialdehyde and glutamate, is respon-sible for the metabolic inactivation of GABA(Fig. 2). Inhibition of GABA transaminase withvigabatrin (g-vinyl GABA), an irreversible sui-cide inhibitor of the enzyme, leads to markedincreases in brain GABA levels (Petroff et al.1996). Although the antiseizure action of viga-batrin is believed to reflect inactivation of GABAtransaminase, how this occurs is not straight-forward and does not appear to be caused byan enhancement of inhibitory synaptic trans-mission. In contrast to the action of tiagabine,vigabatrin does not elicit larger or more pro-longed GABAA receptor-mediated synaptic re-sponses (Overstreet and Westbrook 2001; Wuet al. 2003). Rather, preincubation of brain sliceswith vigabatrin irreversibly inhibited miniatureand evoked inhibitory postsynaptic currents.Additional experiments suggested that the par-adoxical effect resulted from a reduction in theGABA content of synaptic vesicles caused byGABA transaminase inhibition. In contrast tothe effect on GABA-mediated synaptic trans-mission, vigabatrin caused an increase in tonic(nonsynaptic) GABAA receptor current. Thissteady current is believed to be mediated bythe action of GABA in the extracellular milieuacting on extrasynapic GABAA receptors. Highlevels of intracellular GABA cause a reversal ofGABA transporters, resulting in a marked ele-
vation in extracellular GABA, which is likelyresponsible for the increase in tonic GABAA re-ceptor current. It can be concluded that vigaba-trin causes divergent effects on synaptic andextrasynaptic GABA-mediated inhibition withseizure protection resulting from a predomi-nance of the extrasynaptic action. Interestingly,in the early period after administration of vig-abatrin to animals, there is a reduction in seiz-ure threshold, whereas the antiseizure actionsbecome evident only later (Loscher et al. 1989;Stuchlık et al. 2001). Thus, vigabatrin has a bi-phasic action with proconvulsant effects likelyrelated to suppression of synaptic GABAergicneurotransmission and antiseizure effects as aresult of spillover of GABA into the extracellularspace and activation of extrasynaptic GABAA
receptors. Interestingly, individuals with a raregenetic deficiency of GABA transaminase expe-rience refractory seizures, supporting the viewthat inhibition of GABA transaminase is, infact, the proconvulsant mechanism of vigaba-trin (Medina-Kauwe et al. 1999).
SYNAPTIC RELEASE MACHINERY
SV2A
Multiple lines of evidence support the conclu-sion that SV2A, a membrane glycoproteinfound in the secretory vesicles of neurons andendocrine cells and possibly immune cells, is themolecular target for levetiracetam (Kaminskiet al. 2012; Li et al. 2013). There is a strongcorrelation between the affinity of levetiracetamanalogs for binding to SV2A and the potency ofthe analogs in several animal seizure models.Moreover, seizure protection conferred by leve-tiracetam and other SV2A ligands strongly cor-relates with the degree of SV2A occupancy invivo. Finally, the antiseizure efficacy of levetir-acetam (but not valproate, which does not in-teract with SV2A) is reduced in SV2Aþ/ – micethat have one copy of SV2A disrupted by genetargeting. The precise way in which binding oflevetiracetam to SV2A leads to seizure protec-tion is not understood.
Indeed, the function of SV2A itself is ob-scure. Among the various functions proposed
Antiseizure Drugs and the Ketogenic Diet
Cite this article as Cold Spring Harb Perspect Med 2016;6:a022780 9
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
Press on December 16, 2021 - Published by Cold Spring Harbor Laboratoryhttp://perspectivesinmedicine.cshlp.org/Downloaded from

are roles in calcium-dependent exocytosis, neu-rotransmitter loading/retention in synapticvesicles, and synaptic vesicle priming, as wellas transport of vesicle constituents. SV2A isone of three homologous SV2 proteins thatbelong to the major facilitator superfamily of12-transmembrane domain transporters. De-spite substantial effort, no transport functionof these proteins has yet been identified, al-though studies with protein tomography havefound that SV2A can adopt two alternate con-formations consistent with a transporter role(Lynch et al. 2008). Interestingly, however, lev-etiracetam binding does not cause a large-scaleconformational change in SV2A, or lock a spe-cific conformational state of the protein, aswould an inhibitor of transport. Apparently,the drug has a more subtle effect on the protein.Although the function of SV2A is still poorlydefined, SV2A2/ – knockout mice show a lethalseizure phenotype demonstrating that SV2A, insome way, serves to restrain seizure activity.
A series of recent studies has examined theimpact of levetiracetam on synaptic transmis-sion in brain slice recordings (Meehan et al.2011, 2012). Although the drug had no effecton synaptic physiology with low frequencyactivation, levetiracetam did reduce the synap-tic release of both excitatory (glutamate) andinhibitory (GABA) neurotransmitters duringhigh-frequency activation. The frequency de-pendence is compatible with the selective sup-pression of epileptic activity. Modulation ofsynaptic release is a common mechanism ofmany ASDs, including sodium-channel block-ers, which indirectly inhibit release at both ex-citatory and inhibitory synapses by inhibitingaction potential firing. It appears that drugsthat suppress inhibition and excitation can ef-fectively protect against seizures, and they arenot often proconvulsant. However, it is note-worthy that in some instances ASDs (notably,phenytoin) can have proconvulsant effects, par-ticularly at high doses.
With several seconds of heavy use, as likelyoccurs during epileptic activity, excitatory syn-apses undergo a form of short-term plasticitythat is dependent on the supply of new vesiclesreferred to as “supply-rate depression” (Garcıa-
Perez et al. 2008). This form of synaptic depres-sion is distinct from that mediated by depletionof the readily releasable pool of vesicles and isnot believed to come into play during ordinaryongoing activity. It may, however, limit synaptictransmission during sustained high-frequencyfiring and thus serve as an endogenous mecha-nism to restrain epileptic activity. It is, therefore,of interest that levetiracetam has been shown tocause a small acceleration of supply rate depres-sion (Garcıa-Perez et al. 2015). This effect wasobserved in experiments with mouse hippo-campal CA1 neurons activated by Schaffer col-lateral stimulation in brain slices and also inhippocampal neurons in culture, but not in cul-tured neurons from mice lacking SV2A, indicat-ing that an interaction of levetiracetam withSV2A is likely to account for the phenomenon.Thus, work in various laboratories raises thepossibility that levetiracetam confers seizureprotection through an interaction with SV2Aby reducing synaptic release in a use-dependentfashion that requires high-frequency activationfor prolonged periods.
With respect to the specificity of levetirace-tam’s effect on SV2A, it is important to note thatseveral other cellular and molecular effects ofthis ASD have been reported at therapeuticallyrelevant concentrations, including inhibitionof high-voltage–gated calcium channels, inhi-bition of calcium release from intraneuronalstores, effects on the metabolism and turnoverof GABA in discrete brain regions, reductionin the firing activity of GABAergic neurons insubstantia nigra pars reticulata in vivo, and re-versal of zinc-induced inhibition of GABAA re-ceptors in epileptic tissue (Loscher et al. 1996;Lyseng-Williamson 2011; Wakita et al. 2014).The relevance of any of these various pharma-cological actions to the antiseizure effect of lev-etiracetam remains to be defined.
a2d-1
The gabapentinoids gabapentin and pregabalinact by binding to the a2d-1 protein, which isan accessory subunit of voltage-gated calciumchannels (Dolphin 2013; Stahl et al. 2013).a2d-1 is located heterogeneously in the brain,
M.A. Rogawski et al.
10 Cite this article as Cold Spring Harb Perspect Med 2016;6:a022780
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
Press on December 16, 2021 - Published by Cold Spring Harbor Laboratoryhttp://perspectivesinmedicine.cshlp.org/Downloaded from

particularly, at presynaptic sites on excitatory(glutamatergic) neurons. Dense expression isobserved in areas relevant to epilepsy, includingin excitatory hippocampal mossy fibers and inthe neocortex and amygdala. In contrast, a2d-1has minimal expression in the thalamus and it isnoteworthy that gabapentinoids are not activein absence seizures, which, as discussed above,are dependent on this brain structure. Four a2dsubunits have been identified, but gabapenti-noids only bind to a2d-1 and a2d-2 owingto the presence of an RRR motif containinga critical arginine that is required for binding.In knock-in mutant mice bearing a mutationin this motif (RRR mutated to RRA) in a2d-1,which eliminates gabapentin and pregabalinbinding, the analgesic and anxiolytic-like activ-ity of pregabalin is eliminated (Field et al. 2006;Lotarski et al. 2011). A corresponding mutationin a2d-2, which also eliminates binding, hasno similar effect on the anxiolytic-like activityof pregabalin demonstrating thata2d-1 and nota2d-2 is relevant for its pharmacological ac-tivity; studies to determine whether bindingto a2d-1 and not a2d-2 is necessary and suffi-cient to account for the antiseizure activity ofgabapentinoids have not been reported. Inter-estingly, deletion of a2d-1 or a2d-2 in mice isassociated with absence epilepsy or enhancedseizure susceptibility (Ivanov et al. 2004; Davieset al. 2007).
The precise manner in which binding ofgabapentin and pregabalin to the a2d-1 proteinresults in its pharmacological activity, includingseizure protection, is not well understood (Ro-gawski and Bazil 2008). Although some studieshave found that the drugs inhibit calcium chan-nel currents, most have not and it is generallybelieved that calcium channel inhibition is notthe mechanism of action of gabapentinoids(Stefani et al. 1998; van Hooft et al. 2002; Brownand Randall 2005). Regardless of whether thedrugs inhibit calcium channel function, theydo seem to block the release of various neuro-transmitters, including glutamate, and thismay account for the antiseizure activity (Dooleyet al. 2007). There is some evidence thatgabapentinoids cause internalization of calci-um channels by reducing trafficking to the cell
membrane (Hendrich et al. 2008; Weissmannet al. 2013). Whether this action could accountfor the rapid antiseizure effects of gabapenti-noids in animal models is uncertain.
Gabapentin and pregabalin were initiallydeveloped as lipophilic, blood–brain barrierpermeable forms of GABA (3-alkylated GABAanalogs), but it is generally accepted that effectson GABA do not contribute to the pharma-cological action of these drugs (Taylor et al.2007). However, the gabapentinoids do activatethe GABA-synthesizing enzyme glutamic aciddecarboxylase (GAD) (Silverman et al. 1991)and elevate GABA turnover at antiseizure dosesin rats (Loscher et al. 1991) and patients withepilepsy (Petroff et al. 1996). Interestingly, theactivating effects of the gabapentinoids on GADand GABA turnover were similar to those re-ported for valproate (Loscher 1989; Silvermanet al. 1991; Taylor et al. 1992).
AMPA RECEPTORS
Of the synapses in the brain, 80%–90% areexcitatory (Hassel and Dingledine 2012). Atthese synapses, which are often between the pre-synaptic terminal of an excitatory neuron anda dendritic spine of the postsynaptic neuron,neurotransmitter glutamate released from thepresynaptic terminal acts on ionotropic (ionflux conducting) and metabotropic (nonionflux conducting, G-protein-coupled) glutamatereceptors localized to the postsynaptic density.Ionotropic glutamate receptors mediate a fast(millisecond timescale) depolarization of thepostsynaptic neuron, referred to as the excitato-ry postsynaptic potential (EPSP). AMPA recep-tors, one type of ionotropic glutamate receptor,generate the bulk of the EPSP and are there-fore the principal ion channel responsible forfast synaptic excitation. It has been long appre-ciated that cascading excitation within net-works of synaptically connected neurons is akey mechanism of epileptic synchronization,at least in the hippocampal CA3 subfield and,possibly, in other brain areas (Rogawski 2013).Epileptic activity emerges from the networkwhen GABA-mediated inhibition is deficientand, indeed, chronic alterations in inhibition
Antiseizure Drugs and the Ketogenic Diet
Cite this article as Cold Spring Harb Perspect Med 2016;6:a022780 11
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
Press on December 16, 2021 - Published by Cold Spring Harbor Laboratoryhttp://perspectivesinmedicine.cshlp.org/Downloaded from

represent a leading hypothesis to explain someforms of epilepsy (Houser 2014). AMPA recep-tors have a special role in epileptic activity asepileptic synchronization cannot occur whenAMPA receptors are blocked. In contrast, kai-nate receptors, which are ionotropic glutamatereceptors that have a similar structure to AMPAreceptors, do not have a similarly essential roleas kainate receptor knockout does not inter-fere with seizure generation (Fritsch et al.2014). NMDA receptors are thought to contrib-ute to epileptiform activity, but the blockadeof NMDA receptors is insufficient to abolishepileptiform discharges in many seizure models(Neuman et al. 1988; Loscher 1998). Moreover,NMDA blockers may exacerbate seizures inhumans (Sveinbjornsdottir et al. 1993; Kaste-leijn-Nolst Trenite et al. 2015). Pharmacologicalblockade of AMPA receptors has broad spec-trum antiseizure activity in in vitro and animalseizure and epilepsy models (Yamaguchi et al.1993; Rogawski 2011; Twele et al. 2015). In neo-cortical and hippocampal tissue removed frompatients with focal epilepsy, there is evidencethat AMPA receptor density is increased (Ma-thern et al. 1998; Zilles et al. 1999; Eid et al.2002). Thus, it has been proposed that the hy-perexcitability in focal epilepsy, in part, relatesto strengthened excitatory circuits because ofincreased expression of AMPA receptors. AMPAreceptors may therefore be a pivotal pharmaco-logical target for the control of seizures.
Perampanel, a potent noncompetitiveAMPA receptor antagonist, is the first and atpresent only antiseizure agent available for clin-ical use that selectively targets AMPA receptors(Fig. 1). Perampanel does not affect NMDA re-ceptor responses and has no known effects onother ion channels or molecular targets at ther-apeutically relevant concentrations (Hanadaet al. 2011; Chen et al. 2014). Therapeutic bloodlevels are expected to result in brain concentra-tions that would produce only low levels of in-hibition of AMPA receptors (Rogawski andHanada 2013). However, such low-level blockof AMPA receptors is apparently sufficient toexert a clinical antiseizure action. Perampanelhas a relatively low therapeutic window. Adversecentral nervous system effects, such as dizziness,
irritability, and somnolence, are common, par-ticularly at higher doses, emphasizing the im-portance of AMPA receptors in brain function.Although AMPA receptor antagonists havepowerful antiseizure effects, they are not anti-epileptogenic in animal models (Rogawski et al.2001; Twele et al. 2015).
Secondarily generalized tonic–clonic sei-zures and, probably, also primary generalizedtonic–clonic seizures engage distant regions inthe cerebral cortex, as well as subcortical struc-tures including thalamus, cerebellum, and basalganglia (Blumenfeld et al. 2009). Glutamatergicneurons are responsible for the spread of exci-tation to these structures and also for thala-mocortical projections that synchronize distantcortical sites. As is the case at glutamate synap-ses, generally, AMPA receptors generate the bulkof the excitatory current during fast synaptictransmission in these pathways (Turner andSalt 1998). The involvement of AMPA receptorsin long cortical–cortical and cortical–subcor-tical pathways, which mediate the spread of ex-citation in generalized seizures, is likely the basisfor the effectiveness of AMPA receptor antago-nists in the treatment of secondarily generalized(Steinhoff et al. 2013) and primary generalizedtonic–clonic seizures, and also in suppressingthe generalized photoparoxysmal electroen-cephalography (EEG) response in patients withphotosensitive epilepsy (Kasteleijn-Nolst Tre-nite et al. 2015).
MIXED TARGETS
Valproate
Although valproate is one of the most widelyprescribed ASDs, the mechanism by which itprotects against seizures is poorly understood.Valproate has multiple pharmacological actions(Rogawski and Porter 1990; Loscher et al. 2002).Because it has been difficult to relate any onemechanism to the drug’s broad spectrum ofclinical activity, it has been proposed that com-bined actions on several targets could accountfor its therapeutic properties. Although the ac-tions of valproate on GABA systems are notstraightforward, among the various pharmaco-logical effects that have been described, those
M.A. Rogawski et al.
12 Cite this article as Cold Spring Harb Perspect Med 2016;6:a022780
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
Press on December 16, 2021 - Published by Cold Spring Harbor Laboratoryhttp://perspectivesinmedicine.cshlp.org/Downloaded from

related to GABA mechanisms are among themost likely to be relevant to valproate’s antisei-zure activity. For example, valproate increasesthe turnover of GABA in a regionally selectivemanner (Loscher 1989) and this might be asso-ciated with enhanced synaptic or extrasynapticinhibition. At high concentrations, valproate af-fects voltage-gated sodium channels, but recentstudies in brain slice recordings have failed toprovide support for sodium-channel block as arelevant mechanism to explain clinical activity(Englund et al. 2011). Similarly, despite efficacyin absence epilepsy, there is little support foreffects on T-type calcium channels. It is clearthat valproate has pharmacological actions rel-evant to its antiseizure activity that remain to beelucidated.
Felbamate
Felbamate has been shown to act both as a pos-itive modulator of GABAA receptors and also toinhibit NMDA receptors (Rho et al. 1994). Fel-bamate potentiates GABA responses via aninteraction with a site on the GABAA receptorthat is distinct from the benzodiazepine recog-nition site. This action may be of relevance tofelbamate’s clinical activity. As discussed above,NMDA receptors have not been validated asa target to treat focal or generalized seizures.Therefore, it is uncertain whether the NMDA-receptor-blocking activity of felbamate is rele-vant to its clinical antiseizure activity.
Topiramate
Topiramate shows a variety of pharmacologicalactions, but the extent to which any of the ac-tions are relevant to its broad-spectrum antisei-zure activity is uncertain. Targets potentiallyrelevant to seizure protection include voltage-gated sodium channels, GABAA receptor sub-types, AMPA or kainate receptors, and types IIand IV carbonic anhydrase isoenzymes. Unlikeother ASDs, the effects on ion channels arenot likely to occur through direct modulationof channel gating. Rather, the pharmacologi-cal actions of topiramate seem to be mediatedindirectly, possibly through effects on channelphosphorylation (Shank et al. 2008).
The effects of topiramate on sodium chan-nels occur at relatively low, therapeutically rele-vant concentrations and could be similar to theeffects of other sodium-channel-blocking ASDs(Avoli et al. 1996). In addition to effects on fastsodium currents, topiramate, like phenytoin,blocks INaP at low concentrations (Sun et al.2007). Effects of topiramate on GABAA recep-tors could contribute to the broad spectrumactivity of topiramate. Topiramate is not activein animal models, such as the pentylenetetrazol(PTZ) test, which are typically sensitive to drugsthat positively modulate GABAA receptors.Nevertheless, the drug does have activity inan absence of epilepsy models (Rigoulot et al.2003) and can affect pentylenetetrazol thresh-old, which is consistent with effects on GABAA
receptors. There is evidence that topiramatemay preferentially modulate a subset of GABAA
receptors and that drug sensitivity is dependenton the b-subunit type (Simeone et al. 2011).
Several investigators have suggested that ac-tions on fast glutamate-mediated excitatoryneurotransmission could contribute to topira-mate’s antiseizure activity. In cultured neurons,the drug has been reported to inhibit responsesto kainate, an agonist of AMPA and kainatereceptors, leading to the conclusion that topir-amate could be an antagonist of either AMPA orkainate receptors (Gibbs et al. 2000). Recently,kainate receptors have been found to be an un-likely target for an antiseizure agent (Fritschet al. 2014). Whether actions of topiramate onglutamate-mediated neurotransmission con-tribute to its antiseizure activity remains to bedetermined.
It has been assumed that the topiramate’sinhibition of carbonic anhydrase does not con-tribute to its clinical efficacy because there isno cross-tolerance to the antiseizure activity oftopiramate when tolerance occurs to the classi-cal carbonic anhydrase inhibitor acetazolamidein mice. However, a recent review left open thepossibility that carbonic anhydrase inhibitioncould, in part, play a role (Shank and Maryanoff2008).
Topiramate is well recognized to cause ad-verse cognitive effects, including impairment ofworking memory and verbal fluency. A blood-
Antiseizure Drugs and the Ketogenic Diet
Cite this article as Cold Spring Harb Perspect Med 2016;6:a022780 13
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
Press on December 16, 2021 - Published by Cold Spring Harbor Laboratoryhttp://perspectivesinmedicine.cshlp.org/Downloaded from

concentration-dependent decline in phonemicgenerative fluency has been shown, but the basisfor this effect is not understood (Ahmed et al.2015).
Zonisamide
There are some similarities between topiramateand zonisamide as they both contain a sulfuratom and both inhibit carbonic anhydrase. Inaddition, like topiramate, zonisamide may acton voltage-gated sodium channels (Biton 2007).Electrophysiological studies, however, do notsupport an action on GABAA receptors. Unliketopiramate, there are reports that zonisamidecan inhibit T-type voltage-gated calcium chan-nels (Matar et al. 2009), which as stated abovemay account for its activity in absence epilepsy.
Rufinamide
The unique spectrum of clinical activity ofrufinamide in the treatment of Lennox–Gas-taut syndrome (a highly medically intractableepileptic encephalopathy) suggests that it has adistinct mechanism of action (Rogawski 2006).However, to date, rufinamide has only beenshown to interact with voltage-gated sodiumchannels and the effects are subtle. Relevantconcentrations of the drug may, at least forsome subunit isoforms, cause a depolariza-tion in the activation voltage and slowing ofrecovery from inactivation, which would be ex-pected to reduce neuronal excitability (Gilchristet al. 2014). Clearly, the effects on sodium chan-nels cannot explain the special clinical profileof rufinamide.
Adrenocorticotrophin
The mechanism of adrenocorticotrophin(ACTH) in the treatment of infantile spasms isnot well understood (Stafstrom et al. 2011).ACTH stimulates glucocorticoid (cortisol) syn-thesis and release from the zona fasciculataof the adrenal cortex. The cortisol could pro-duce an anti-inflammatory action or have someother action in the brain to influence infantilespasms. Indeed, glucocorticoids are well recog-nized themselves and have therapeutic activity
in the treatment of infantile spasms; whetherACTH is truly superior remains to be shownconclusively. One possible additional actionof ACTH that could contribute to an enhancedaction is through stimulation of neurosteroidsynthesis. In addition to its actions with respectto glucocorticoids, ACTH also stimulates de-oxycorticosterone (DOC) release from thezona glomerulosa of the adrenal cortex. DOCis, in part, converted to the antiseizure neuro-steroid tetrahydro-DOC, which is a positive al-losteric modulator of GABAA receptors (Reddyand Rogawski 2002). It has been hypothesizedthat the tetrahydro-DOC could, at least in part,contribute to the ability of ACTH to terminateinfantile spasms.
KETOGENIC DIET
The use of dietary manipulations to treatepilepsy—in particular, controlling seizuresthrough sustained fasting—dates back to thetime of Hippocrates (Lennox and Cobb 1928;Wheless 2008). In the early 1920s, investigatorsrealized that a diet composed principally of fatscould be as effective as fasting and yield long-term suppression of seizures without severe ca-loric deprivation. Thus was born the ketogenicdiet whose hallmark feature is the productionof ketone bodies (b-hydroxybutyrate, acetoace-tate, and acetone) by the liver (Peterman 1924;Freeman and Kossoff 2010). In an era before theavailability of safe and effective ASDs, the keto-genic diet quickly became popular in large med-ical centers. However, with the advent of phe-nytoin in 1938, the ketogenic diet quickly fellout of favor mainly because the oral medicationwas simpler than the strict and exacting dietaryregimen. Beginning in the mid-1990s, there wasa resurgence of interest in the ketogenic diet as itwas increasingly recognized that the diet hasutility in the treatment of drug-resistant epilep-sy (Freeman and Kossoff 2010). Today, the ke-togenic diet is an established therapy for diffi-cult-to-treat epilepsies, particularly in children,and is increasingly being studied for therapeu-tic efficacy in a number of other neurologicaldisorders (Gasior et al. 2006; Neal et al. 2008;Stafstrom and Rho 2012).
M.A. Rogawski et al.
14 Cite this article as Cold Spring Harb Perspect Med 2016;6:a022780
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
Press on December 16, 2021 - Published by Cold Spring Harbor Laboratoryhttp://perspectivesinmedicine.cshlp.org/Downloaded from

Scientific interest in the mechanisms bywhich the ketogenic diet exerts seizure controlhas evolved rapidly in parallel with the growthin clinical use of the diet over the past 20 years(Masino and Rho 2012). Effectiveness of theketogenic diet has been amply shown in animalmodels of seizures and epilepsy. Still, at present,the basic mechanisms of ketogenic diet actionremain incompletely understood. There is sub-stantial interest in defining these mechanisms.Dietary therapy is not feasible for many pa-tients, but the insights gained from study ofthe diet may provide clues to the creation ofmore effective ASDs to address pharmacoresis-tant epilepsy. Since the 1930s, numerous mech-anistic hypotheses have been advanced to ex-plain the antiseizure effects of the ketogenicdiet; the key mechanisms are discussed belowand summarized in Table 2.
Direct Effects of Ketone Bodies
The earliest demonstration that ketone bod-ies have antiseizure properties was given inthe 1930s. Acetoacetate was shown to protectagainst thujone-induced seizures in rabbits(Keith 1933). Further, acetone was shown toexert antiseizure activity in several animal mod-els (Likhodii et al. 2003; Gasior et al. 2007).Recently, chronic administration of the majorketone, b-hydroxybutyrate, was shown to blockspontaneous seizures in epileptic mice (Kimet al. 2015). Interestingly, the in vivo evidencefor the antiseizure effects of ketone bodies hasbeen discordant with earlier in vitro studies.Application of acetoacetate or b-hydroxybuty-rate in acute hippocampal brain slices fromnormal rats failed to reveal effects on GABAA
receptors and ionotropic glutamate receptors,and on synaptic transmission (Thio et al.2000). However, more recent data indicate thatthe antiseizure activity of ketone bodies in vitromay require long-term incubation and not sim-ply acute exposure (Kim et al. 2015). Collective-ly, it appears that ketone bodies afford broadspectrum antiseizure activity in animal modelsand, hence, the possibility that these metabo-lites contribute to the therapeutic efficacy ofthe diet cannot be discounted. Although the
molecular targets through which ketone bodiesact to protect against seizures have not yet beenclearly identified, there is strong evidence tosuggest that mitochondria are critically in-volved (Masino and Rho 2012). Also, giventhat the ketogenic diet is mainly used in youngerpatients, enhanced efficacy in this populationcould reflect age-dependent changes in theexpression of monocarboxylate transporters,which import ketone bodies across the blood–brain barrier from the systemic circulation(Morris 2005; Pierre and Pellerin 2005).
Effects on GABA and Glutamate Metabolism
It has been proposed that increased synthesis orlevels of the inhibitory neurotransmitter GABAor decreased synthesis or levels of the excitatoryneurotransmitter glutamate could explain theantiseizure activity of the ketogenic diet. Theimplication of such findings is uncertain inas-much as it has not been shown that these ma-nipulations influence neural circuit excitability,either through synaptic or nonsynaptic actions.Nevertheless, we summarize the results of someof these studies to illustrate the kinds of obser-vations that have been reported.
The influence of the ketogenic on GABA hasbeen proposed to originate in changes in gluta-mate metabolism (Yudkoff et al. 2005). Gluta-mate is cleared from the synaptic space by as-trocytes, which convert glutamate to glutaminethrough the action of the glial enzyme gluta-mine synthetase. Glutamine is then exportedto neurons where it is hydrolyzed to glutamateand can then either be converted to GABA ortransaminated to aspartate in a reaction thatrequires oxaloacetate. Because the ketogenicdiet induces metabolic changes that requireavailable oxaloacetate to condense with acetyl-CoA for incorporation into the tricarboxylicacid (TCA) cycle, the production of aspartatefrom glutamate is reduced. This may resultin enhanced flux through GAD to increase thesynthesis of GABA.
Experimental support for this biochemicalhypothesis is mixed. In the study proposing thehypothesis, which used a mouse model of keto-sis, changes in levels of aspartate were found,
Antiseizure Drugs and the Ketogenic Diet
Cite this article as Cold Spring Harb Perspect Med 2016;6:a022780 15
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
Press on December 16, 2021 - Published by Cold Spring Harbor Laboratoryhttp://perspectivesinmedicine.cshlp.org/Downloaded from
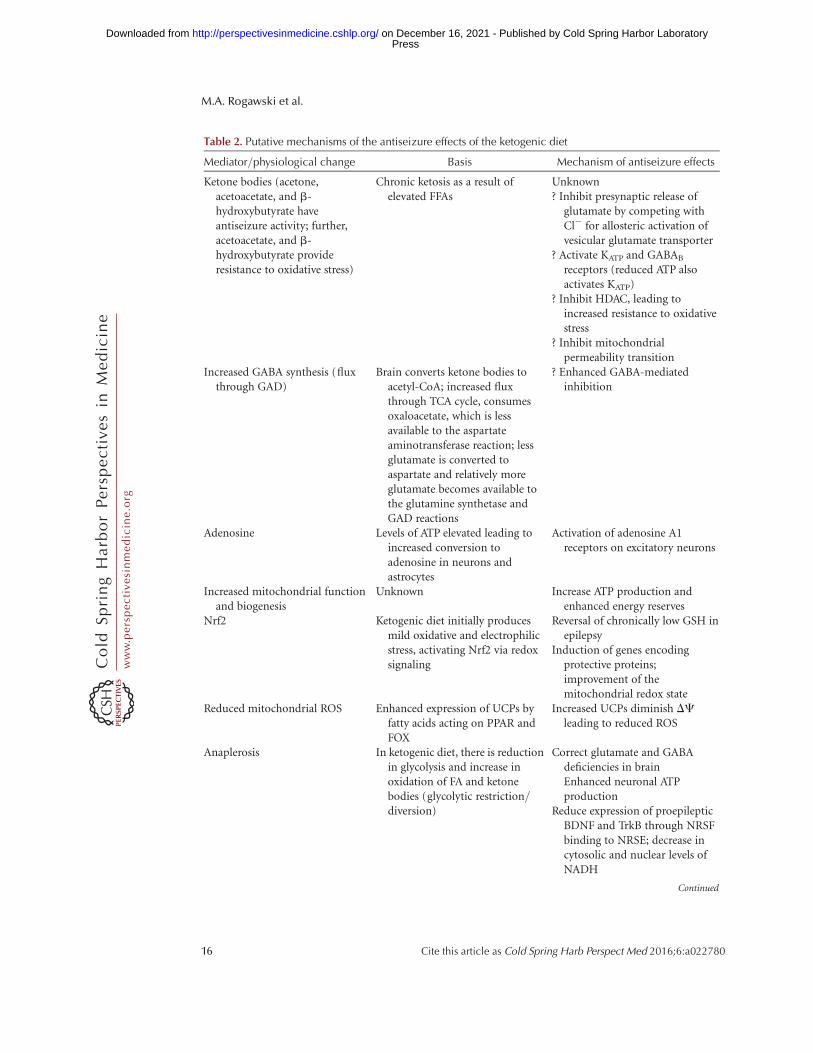
Table 2. Putative mechanisms of the antiseizure effects of the ketogenic diet
Mediator/physiological change Basis Mechanism of antiseizure effects
Ketone bodies (acetone,acetoacetate, and b-hydroxybutyrate haveantiseizure activity; further,acetoacetate, and b-hydroxybutyrate provideresistance to oxidative stress)
Chronic ketosis as a result ofelevated FFAs
Unknown? Inhibit presynaptic release of
glutamate by competing withCl2 for allosteric activation ofvesicular glutamate transporter
? Activate KATP and GABAB
receptors (reduced ATP alsoactivates KATP)
? Inhibit HDAC, leading toincreased resistance to oxidativestress
? Inhibit mitochondrialpermeability transition
Increased GABA synthesis (fluxthrough GAD)
Brain converts ketone bodies toacetyl-CoA; increased fluxthrough TCA cycle, consumesoxaloacetate, which is lessavailable to the aspartateaminotransferase reaction; lessglutamate is converted toaspartate and relatively moreglutamate becomes available tothe glutamine synthetase andGAD reactions
? Enhanced GABA-mediatedinhibition
Adenosine Levels of ATP elevated leading toincreased conversion toadenosine in neurons andastrocytes
Activation of adenosine A1receptors on excitatory neurons
Increased mitochondrial functionand biogenesis
Unknown Increase ATP production andenhanced energy reserves
Nrf2 Ketogenic diet initially producesmild oxidative and electrophilicstress, activating Nrf2 via redoxsignaling
Reversal of chronically low GSH inepilepsy
Induction of genes encodingprotective proteins;improvement of themitochondrial redox state
Reduced mitochondrial ROS Enhanced expression of UCPs byfatty acids acting on PPAR andFOX
Increased UCPs diminish DC
leading to reduced ROS
Anaplerosis In ketogenic diet, there is reductionin glycolysis and increase inoxidation of FA and ketonebodies (glycolytic restriction/diversion)
Correct glutamate and GABAdeficiencies in brainEnhanced neuronal ATPproduction
Reduce expression of proepilepticBDNF and TrkB through NRSFbinding to NRSE; decrease incytosolic and nuclear levels ofNADH
Continued
M.A. Rogawski et al.
16 Cite this article as Cold Spring Harb Perspect Med 2016;6:a022780
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
Press on December 16, 2021 - Published by Cold Spring Harbor Laboratoryhttp://perspectivesinmedicine.cshlp.org/Downloaded from

along with the expected increases in acetyl-CoA,but there were no changes in the levels of GABAor glutamate (Yudkoff et al. 2005). The samestudy did show increases in glutamine andGABA on infusion of the nitrogen donors ala-nine or leucine. Rats fed the ketogenic diet for3 wk showed a reduction in brain glutamatelevels, but also no change in GABA (Meloet al. 2006). However, in children fed the keto-genic diet, cerebrospinal fluid levels of GABAhave been shown to increase, but without achange in glutamate concentrations (Dahlinet al. 2005). Another study in rats fed the keto-genic diet for 3 wk found “increased” levels ofglutamate and glutamine in the hippocampus(Bough et al. 2006). Further, using both mildcaloric restriction (90% of daily energy require-ments) and an isocaloric ketogenic diet, inves-tigators found significant increases in the mes-senger RNA (mRNA) expression of bothisoforms of GAD (GAD65 and GAD67) in sev-eral brain regions that were independent of ke-togenic effects (Cheng et al. 2004); the function-al implications are unclear given that GABAlevels were not increased.
Recently, it has been proposed that the ke-togenic diet could suppress neuronal excitabil-
ity by inhibiting the presynaptic release of glu-tamate. The ketone bodies b-hydroxybutyrateand acetoacetate were shown to diminish gluta-mate release by directly competing with Cl2 forallosteric activation of vesicular glutamatetransporters (Juge et al. 2010). In the samestudy, application of the potassium channelblocker 4-aminopyridine to rat brain in vivoevoked seizures with concurrent secretion ofglutamate, and these effects were blocked byacetoacetate. The relevance of this study is fur-ther supported by the recent observation thatb-hydroxybutyrate does indeed induce antisei-zure activity (Kim et al. 2015).
KATP Channels and GABAB Receptors
It has been proposed that activation of KATP
channels and GABAB receptors could underliethe action of the ketogenic diet (Ma et al. 2007).In brain slice recordings, acetoacetate andb-hydroxybutyrate were found to reduce thespontaneous firing rate of GABAergic neuronsin the substantia nigra pars reticulata, a putativesubcortical seizure gate, and this action was de-pendent on KATP channels and GABAB recep-tors. Apart from the fact that KATP channels and
Table 2. Continued
Mediator/physiological change Basis Mechanism of antiseizure effects
PUFAs Ketogenic diet enhancesmobilization of PUFAs fromadipose tissue to liver andbrains
PUFAs directly affect ion channelsActivation of PPARa and PGC-1a
(coactivator) leads to changes intranscription of genes linked toenergy, amino acid, andneurotransmitter metabolism
Boost activity of UCPsMedium-chain triglycerides Exogenous administration of in
the medium-chain triglycerideketogenic diet
Unknown (similar action tovalproate)
FFA3 Activated by short-chain fattyacids and b-hydroxybutyrate
Inhibit N-type voltage-gatedcalcium channels, leading toreduced glutamate release atsynapses
FFAs, Free fatty acids; HDAC, histone deacetylase; GABA, g-aminobutyric acid; GAD, glutamic acid decarboxylase; Nrf2,
NF E2-related factor 2; TCA, tricarboxylic acid; GSH, glutathione; ROS, reactive oxygen species; UCPs, uncoupling proteins;
PPAR, peroxisome proliferator-activated receptor; FOX, forkhead box; FA, fatty acid; NRSF, neural restrictive
silencing factor; NRSE, neuron restrictive silencing element; PUFAs, polyunsaturated fatty acids; BDNF, brain-derived
neurotrophic factor; TrkB, tropomyosin receptor; NADH, nicotinamide adenine dinucleotide (reduced).
Antiseizure Drugs and the Ketogenic Diet
Cite this article as Cold Spring Harb Perspect Med 2016;6:a022780 17
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
Press on December 16, 2021 - Published by Cold Spring Harbor Laboratoryhttp://perspectivesinmedicine.cshlp.org/Downloaded from

GABAB receptors have been previously shownnot to be germane antiseizure targets except inspecial circumstances (Meldrum and Rogawski2007), most problematic for the hypothesis isthe fact that the ketogenic diet and ketone bod-ies actually increase ATP production, whichwould tend to close KATP channels and enhanceinstead of inhibit neuronal excitability (Masinoand Rho 2012). In any case, the same group hasshown that the open probability of KATP chan-nels in the hippocampus in vitro is enhancedin the presence of b-hydroxybutyrate (Tanneret al. 2011).
Adenosine
Recent studies have implicated the potent in-hibitory modulator adenosine, which is wellrecognized to have antiseizure activity (Dun-widdie and Masino 2001), in the action of theketogenic diet (Masino et al. 2012). Adenosineproduces antiseizure effects through activationof inhibitory adenosine A1 receptors on excit-atory neurons. Adenosine is synthesized byhydrolysis of ATP in neurons and astrocytes.Because levels of ATP are elevated by the keto-genic diet, it is plausible that adenosine syn-thesis and release could also be enhanced. Tar-geted heterozygous (A1Rþ/ – ) or homozygous(A1R2/ – ) deletion of A1 receptors or increasedexpression of adenosine kinase (Adk-Tg), anenzyme that enhances clearance of adenosine,causes spontaneous electrographic seizures inmice (Masino et al. 2011). A 3-wk treatmentwith the ketogenic led to decreased electro-graphic seizures in Adk-Tg and A1Rþ/ – mice,but not in animals entirely missing A1R recep-tors (A1R2/ – ), supporting the concept thatadenosine may be an important mediator ofthe ketogenic diet’s antiseizure effects.
Bioenergetic and Mitochondrial Changes
Pathological changes in mitochondrial energymetabolism and reactive oxygen species (ROS)production are known to occur with epilepto-genesis, and the ketogenic diet has been foundto profoundly affect these processes (Rowleyand Patel 2013). In addition to enhancing ener-
gy reserves, ATP levels, and the expression ofmany enzymes involved in mitochondrial me-tabolism, the ketogenic diet has also beenshown to increase mitochondrial biogenesis inthe hippocampus (Bough et al. 2006) and toreduce oxidative stress through multiple cellularmechanisms, including those involving mito-chondria, such as through increases in reducedglutathione (GSH). The effect on GSH is ofparticular interest because depletion of GSH isknown to occur in epilepsy (Mueller et al. 2001).Increased GSH was shown to correlate with in-creased activity of glutamate cysteine ligase(GCL), the rate-limiting enzyme in GSH bio-synthesis, and enhanced expression of the GCLcatalytic subunit, GCLC, and modulatory sub-unit, GCLM, in rats fed the ketogenic diet (Jar-rett et al. 2008).
The increase in GSH and associated changeswere subsequently shown to involve NF E2-related factor 2 (Nrf2), a redox-sensitive tran-scription factor that is activated by cellular stressand induces a diverse array of genes, includingthe GSH antioxidant pathway (Suzuki et al.2013). The ketogenic diet resulted in elevatedlevels of Nrf2 for 3 wk, and this was associatedwith increased activity of NAD(P)H:quinoneoxidoreductase, a prototypical Nrf2 target(Milder et al. 2010). Interestingly, a recent studyfound that increasing Nrf2 expression in a ratmodel of temporal lobe epilepsy decreasedspontaneous seizures (Mazzuferi et al. 2013).
Acute application of the ketone bodies b-hydroxybutyrate and acetoacetate in hippocam-pal slices enhanced catalase activity in responseH2O2 (Kim et al. 2010) and decreased oxida-tion of carboxy-20,70-dichlorodihydrofluoresceindiacetate, a dye often used as an indicator ofintracellular ROS (Maalouf and Rho 2008). Inisolated mitochondria, b-hydroxybutyrate andacetoacetate have been shown to decrease ROSlevels in response to glutamate by enhancingoxidation of NADH (Maalouf et al. 2007). Ad-ditionally, b-hydroxybutyrate and acetoacetatereduced mitochondrial ROS both basally and inresponse to the ATP synthase inhibitor oligomy-cin (Kim et al. 2007).
A possible mechanism mediating the de-crease in mitochondrial ROS production with
M.A. Rogawski et al.
18 Cite this article as Cold Spring Harb Perspect Med 2016;6:a022780
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
Press on December 16, 2021 - Published by Cold Spring Harbor Laboratoryhttp://perspectivesinmedicine.cshlp.org/Downloaded from

the ketogenic diet is enhanced expression of un-coupling proteins (UCPs). Increased activity ofUCPs can diminish the mitochondrial mem-brane potential (DC), resulting in a decreasein ROS production, and this has been associatedwith increased resistance to kainate-inducedseizures (Sullivan et al. 2003). Additionally, fat-ty acids can induce increases in UCP expressionpossibly through enhanced activity of transcrip-tion factors, such as the peroxisome prolifera-tor-activated receptor (PPAR) and the forkheadbox (FOX) family of transcription factors (Azzuand Brand 2010). In mice fed the ketogenic diet,UCP activity was enhanced and this was asso-ciated with increased levels of UCP2, UCP4,and UCP5 in the hippocampus (Sullivan et al.2004). Additionally, ROS production—assessedin the presence of oligomycin to maximizeDC—was reduced in mice fed the ketogenicdiet (Sullivan et al. 2004).
Recently, b-hydroxybutyrate was shown tobe an inhibitor of class I histone deacetylases(HDACs) in vitro and in vivo, and this activitywas associated with increased resistance to oxi-dative stress (Shimazu et al. 2013). Specifically,b-hydroxybutyrate increased acetylation of his-tone H3 lysine 9 (H3K9) and histone H3 lysine14 and enhanced transcription of genes regulat-ed by FOXO3A, including the antioxidant en-zymes manganese superoxide dismutase andcatalase. Further, b-hydroxybutyrate (adminis-tered in vivo for 24 h via an osmotic pump)decreased protein carbonylation and 4-hydrox-ynonenal and lipid peroxides in the kidney. Al-though the investigators did not report sucheffects in neuronal tissue or cells, it is possiblethat direct inhibition of HDACs and the ensuingtranscriptional changes may mediate some ofthe antioxidant effects known to occur in thebrain with the ketogenic diet.
Glycolytic Restriction/Diversion
It has been proposed that increased neuro-transmission caused by the hyperexcitability inneural networks in chronic epilepsy leads to de-pletion of TCA cycle intermediates, includinga-ketoglutarate, which is a precursor for gluta-mate and GABA (Borges and Sonnewald 2012).
Seizure susceptibility is further augmented bythe reduction in these neurotransmitters andreduced energy (ATP) production as a resultof diminished acetyl-CoA. A key feature of theketogenic diet is a relative reduction in glycoly-sis and an increase in nonglucose sources of fuelthrough the oxidation of fatty acids and ketonebodies, which ultimately feed the TCA cyclethrough a process known as anaplerosis (i.e.,the replenishing of depleted metabolic cycle in-termediates). Anaplerosis is believed to correctthe neurotransmitter (glutamate and GABA)deficiencies and enhance neuronal ATP produc-tion, which ultimately leads to a reduction inseizure susceptibility. Glycolytic restriction isthought to be an important mechanism medi-ating the antiseizure properties of the ketogenicdiet (Masino and Rho 2012). Indeed, caloricrestriction has antiseizure, and possibly antiepi-leptogenic, effects (Mantis et al. 2004). The ear-liest clinical observation supporting this notionis the rapid reversal of seizure control on inges-tion of carbohydrates or glucose in patients onthe ketogenic diet (Huttenlocher 1976). Addi-tionally, studies in animals using labeled meta-bolic precursors have shown that the ketogenicdiet reduces glycolysis (Yudkoff et al. 2005;Melo et al. 2006).
Recently, attempts have been made to mim-ic the antiseizure activity of the ketogenic dietusing glycolytic inhibitors. In vitro applicationof 2-deoxy-D-glucose (2-DG), an inhibitor ofphosphoglucose isomerase, reduced epilepti-form bursts induced in hippocampal slices bybicuculline, 4-aminopyridine, and increasedextracellular Kþ (Stafstrom et al. 2009). Addi-tionally, in vivo administration of 2-DG pro-vides protection against audiogenic and 6-Hzstimulation-induced seizures in mice and alsoproduced an antiseizure and antiepileptogeniceffect in a rat kindling model (Garriga-Canutet al. 2006; Stafstrom et al. 2009; Gasior et al.2010). The antiseizure effects of 2-DG may bepartially mediated by changes in the expressionof genes encoding brain-derived neurotrophicfactor and its receptor TrkB, both of whichare regulated by the activity of the transcriptionfactor neural restrictive silencing factor (NRSF),which represses transcription by binding to the
Antiseizure Drugs and the Ketogenic Diet
Cite this article as Cold Spring Harb Perspect Med 2016;6:a022780 19
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
Press on December 16, 2021 - Published by Cold Spring Harbor Laboratoryhttp://perspectivesinmedicine.cshlp.org/Downloaded from

neuron restrictive silencing element (NRSE) inpromoter regions (Garriga-Canut et al. 2006).NRSF transcriptional repression was enhancedby 2-DG and this was associated with a reduc-tion in acetylation and an increase in methyla-tion of H3K9 at the NRSE promoter, epigeneticmodifications associated with suppression ofgene transcription. NRSF-mediated repressionrequired an interaction with the transcriptionalcorepressor carboxyl-terminal binding proteinthat was disrupted with increasing concentra-tions of NADH, a cofactor that is elevated onincreased glycolytic flux. This suggests that theantiseizure actions of 2-DG may be mediatedby a decrease in cytosolic and nuclear levels ofNADH and subsequent influences on histonemodifications.
Fructose-1,6-bisphosphate (FBP) also in-hibits glycolysis by diverting the metabolism ofglucose to the pentose phosphate pathway andaffords antiseizure effects in vivo. FBP was foundto protect against pilocarpine, kainate, andPTZ-induced seizures in rats (Lian et al. 2007)and also affected kindling acquisition (Dinget al. 2010). FBP had broader activity than val-proate and 2-DG, whereas the ketogenic diet wasnot active in the models. These results reinforcethe view that diversion of metabolism away fromglycolysis is a promising antiseizure strategy.
Triheptanoin, the triglyceride of the C7 fattyacid heptanoate, is an anaplerotic substrate thatrestores levels of TCA intermediates (Haderaet al. 2014). Oral administration of triheptanoinhas been shown to have antiseizure effects insome animal models, providing support forthe anaplerosis hypothesis (Willis et al. 2010;Kim et al. 2013). A recent report suggests thattriheptanoin may also have anti-ictal activity inhumans (Pascual et al. 2014).
Fatty Acid Oxidation and PolyunsaturatedFatty Acids
Intake of a high-fat diet, such as the ketogenicdiet, increases the rate of fatty acid oxidation.This leads to changes in the levels and types ofpolyunsaturated fatty acids (PUFAs) in the cir-culation, liver, and brain. In particular, it hasbeen show that there is enhanced mobilization
of PUFAs from adipose tissue to liver and brain(Taha et al. 2005). Large quantities of PUFAs arenot a typical component of the ketogenic diet,thus increases in PUFAs must be the result ofendogenous production and export into thecirculation (Fraser et al. 2003). PUFAs affectdiverse ion channels, including voltage-gatedsodium and potassium channels (Vreugdenhilet al. 1996), and it has been speculated thatactions of PUFAs on such ion channels couldmediate the antiseizure effects of the ketogenicdiet (Michael-Titus and Priestley 2013). An ad-ditional mechanism whereby PUFAs could af-fect seizure susceptibility is through activationof peroxisome proliferator-activated receptor-a(PPARa), a nuclear receptor that regulates thetranscription of numerous genes linked to en-ergy, amino acid, and neurotransmitter metab-olism. Recently, it was shown that fenofibrate,a PPARa ligand, exerts anticonvulsant activitycomparable to the ketogenic diet in adult rats(Porta et al. 2009). The specific genes relevant tothis effect remain to be determined.
In pediatric patients with epilepsy, 3–4 wkof ketogenic diet treatment led to elevations incirculating levels of b-hydroxybutyrate, corti-sol, and free fatty acids (FFAs) (Fraser et al.2003). Most PUFAs were also increased in theserum, including the triglyceride and phospho-lipid forms of linoleic acid (LA), arachidonicacid (AA) and docosahexaenoic acid (DHA),triglyceride levels of stearic acid, and palmiticacid in phospholipids. Additionally, these alter-ations in fatty acids were associated with seizurereduction in 78% of the children. Interestingly,seizure control was correlated with circulatingAA levels, but not EEG changes.
Whether PUFA ingestion can render anti-seizure effects remains controversial. Oral sup-plementation with 5 g of omega-3 PUFA for6 mo appeared to reduce the frequency and se-verity of seizures in a small observational study(Schlanger et al. 2002). However, in a 12-wkrandomized, placebo-controlled parallel groupstudy in adults with epilepsy, administration ofeicosapentaenoic acid (EPA) and DHA (1 gEPA, 0.7 g DHA daily) reduced seizure frequen-cy for the first 6 wk of treatment, but this effectdid not persist in spite of sustained increases in
M.A. Rogawski et al.
20 Cite this article as Cold Spring Harb Perspect Med 2016;6:a022780
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
Press on December 16, 2021 - Published by Cold Spring Harbor Laboratoryhttp://perspectivesinmedicine.cshlp.org/Downloaded from

DHA and EPA and decreases in AA and LA inthe plasma (Yuen et al. 2005). In an additionalrandomized, blinded trial of PUFA supplemen-tation (EPA plus DHA, 2.2 mg/d in a 3:2 ratioover 12 wk) in adults with uncontrolled epilep-sy, there was a lack of clear efficacy when com-pared with placebo (Bromfield et al. 2008).
In rats fed the ketogenic diet, there weremarked reductions of PUFA levels in plasmaand adipose tissue, but enhanced mobilizationof the PUFA AA and DHA to the liver and brain(Taha et al. 2005). This was accompanied byan initial increase in plasma levels of b-hy-droxybutyrate, followed by a reduction by day10 of the diet. Following a calorie-restrictedketogenic diet, mRNA expression of the rate-limiting enzyme for ketone body production,HMG-CoAS2, was found to increase in boththe liver and brain, in contrast to feeding withan isocaloric standard chow, which resulted inenhanced expression only in the liver (Culling-ford et al. 2002). Collectively, these and otheranimal studies suggest that diet-induced chang-es in brain content and metabolism of PUFAsmay be important contributors to antiseizureeffects of the ketogenic diet (Taha et al. 2010).
Medium-Chain Triglycerides
The medium-chain triglyceride ketogenic dietis as efficacious as the classic ketogenic diet inwhich the primary fat source is long-chain tri-glycerides (Huttenlocher et al. 1971; Neal et al.2009; Liu and Wang 2013). This diet increasesthe plasma levels of medium straight-chain fattyacids. Recently, medium-chain triglycerides ofvarious structural classes have been shown toreduce the frequency of epileptiform dischargesin in vitro slice models and to inhibit behavioraland EEG seizures in a rat status epilepticusmodel; modest activity was also reported invarious in vivo models used to screen for anti-seizure activity (Chang et al. 2012, 2013, 2015).Valproate is a short-branched-chain fatty acid.Certain structurally novel medium-chain fattyacids have been identified that have greater ac-tivity than valproate in seizure models and thatlack the HDAC activity of valproate, which hasbeen proposed as a basis for its teratogenicity.
Whether administration of a specific medium-chain triglyceride in the presence of a normaldiet could represent an epilepsy treatment ap-proach remains to be determined.
Free Fatty Acid Receptor 3
Free fatty acid receptor 3 (FFA3) is a G-proteincoupled receptor whose endogenous ligandsmay include short-chain fatty acids, such as ac-etate and propionate. A study in dissociatedsympathetic neurons recently showed that b-hydroxybutyrate is also an agonist of FFA3,causing inhibition of N-type voltage-gated cal-cium channels (Won et al. 2013). A prior studyalso found the ketone body to interact withFFA3, but in this case it was an antagonist (Ki-mura et al. 2011); the basis for the discrepancy isnot apparent. As of yet, the relevance of theseactions to brain function remains to be deter-mined.
CONCLUSION
In recent years, there have been dramatic ad-vances in our understanding of how ASDs pre-vent seizures. ASDs interact with a wide varietyof molecular targets. There are unique aspectsto the mechanism of each ASD so that it is rarelythe case that two ASDs have what could be con-sidered the same mechanisms of action (gaba-pentin and pregabalin are perhaps exceptions).Although some ASDs have a single cognate tar-get, for many of the drugs, clinical activityis likely the result of actions on several targets.This makes the definition of “mechanism ofaction” challenging, but it is perhaps not sur-prising that control of epilepsy, which is afunctional disorder of neural networks, wouldbenefit from therapeutic interventions at vari-ous points in the network.
Although ASDs provide control of seizuresfor many people with epilepsy, a disappoint-ingly large number do not achieve seizure free-dom with medications. The ketogenic diet is analternative approach that may provide seizurecontrol in cases of drug-resistant epilepsy. Thereare still many open questions regarding themechanisms of the ketogenic diet. However, as
Antiseizure Drugs and the Ketogenic Diet
Cite this article as Cold Spring Harb Perspect Med 2016;6:a022780 21
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
Press on December 16, 2021 - Published by Cold Spring Harbor Laboratoryhttp://perspectivesinmedicine.cshlp.org/Downloaded from

reviewed here, effects of the diet on intermedi-ary metabolism are likely to be central to itstherapeutic activity. These mechanisms arefundamentally different from those believed tobe relevant to ASDs. Consequently, study ofthe ketogenic diet may open avenues to the cre-ation of entirely novel treatment strategies forpharmacoresistant epilepsies. Such treatmentapproaches may improve on the efficacy ofthe diet and be more convenient and palatable.There is, therefore, strong justification for con-tinued investigation of ketogenic diet mecha-nisms.
ACKNOWLEDGMENTS
M.A.R.’s research is supported by the NationalInstitute of Neurological Disorders and Stroke(NS079202). J.M.R.’s research is supported bythe Canadian Institutes of Health Research.
REFERENCES
Ahmed GF, Marino SE, Brundage RC, Pakhomov SV, LeppikIE, Cloyd JC, Clark A, Birnbaum AK. 2015. Pharmacoki-netic-pharmacodynamic modelling of intravenous andoral topiramate and its effect on phonemic fluency inadulthealthyvolunteers.Br JClinPharmacol 79:820–830.
Alexander SPH, Benson HE, Faccenda E, Pawson AJ, Shar-man JL, Catterall WA, Spedding M, Peters JA, Harmar AJ;CGTP Collaborators. 2013. The concise guide to PHAR-MACOLOGY 2013/14: Ion channels. Br J Pharmacol170: 1607–1651.
Avoli M, Kawasaki H, Zona C. 1996. Effects induced by to-piramate on sodium electrogenesis in mammalian cen-tral neurons. Epilepsia 37: 51–52.
Avoli M, Rogawski MA, Avanzini G. 2001. Generalized ep-ileptic disorders: An update. Epilepsia 42: 445–457.
Azzu V, Brand MD. 2010. The on-off switches of the mito-chondrial uncoupling proteins. Trends Biochem Sci 35:298–307.
Berg AT, Levy SR, Testa FM, Blumenfeld H. 2014. Long-termseizure remission in childhood absence epilepsy: Mightinitial treatment matter? Epilepsia 55: 551–557.
Biton V. 2007. Clinical pharmacology and mechanism ofaction of zonisamide. Clin Neuropharmacol 30: 230–240.
Blumenfeld H, Klein JP, Schridde U, Vestal M, Rice T, KheraDS, Bashyal C, Giblin K, Paul-Laughinghouse C, Wang F,et al. 2008. Early treatment suppresses the developmentof spike-wave epilepsy in a rat model. Epilepsia 49: 400–409.
Blumenfeld H, Varghese GI, Purcaro MJ, Motelow JE, EnevM, McNally KA, Levin AR, Hirsch LJ, Tikofsky R, ZubalIG, et al. 2009. Cortical and subcortical networks in hu-
man secondarily generalized tonic-clonic seizures. Brain132: 999–1012.
Borges K, Sonnewald U. 2012. Triheptanoin—A mediumchain triglyceride with odd chain fatty acids: A new ana-plerotic anticonvulsant treatment? Epilepsy Res 100:239–244.
Bough KJ, Wetherington J, Hassel B, Pare JF, Gawryluk JW,Greene JG, Shaw R, Smith Y, Geiger JD, Dingledine RJ.2006. Mitochondrial biogenesis in the anticonvulsantmechanism of the ketogenic diet. Ann Neurol 60: 223–235.
Broicher T, Seidenbecher T, Meuth P, Munsch T, Meuth SG,Kanyshkova T, Pape HC, Budde T. 2007. T-current relatedeffects of antiepileptic drugs and a Ca2þ channel antag-onist on thalamic relay and local circuit interneurons ina rat model of absence epilepsy. Neuropharmacology 53:431–446.
Bromfield E, Dworetzky B, Hurwitz S, Eluri Z, Lane L, Re-plansky S, Mostofsky D. 2008. A randomized trial ofpolyunsaturated fatty acids for refractory epilepsy. Epilep-sy Behav 12: 187–190.
Brown DA, Passmore GM. 2009. Neural KCNQ (Kv7) chan-nels. Br J Pharmacol 156: 1185–1195.
Chang P, Orabi B, Deranieh RM, Dham M, Hoeller O, Shim-shoni JA, Yagen B, Bialer M, Greenberg ML, Walker MC,et al. 2012. The antiepileptic drug valproic acid and othermedium-chain fatty acids acutely reduce phosphoinosi-tide levels independently of inositol in Dictyostelium.Dis Model Mech 5: 115–124.
Chang P, Terbach N, Plant N, Chen PE, Walker MC, Wil-liams RS. 2013. Seizure control by ketogenic diet-associ-ated medium chain fatty acids. Neuropharmacology 69:105–114.
Chang P, Zuckermann AM, Williams S, Close AJ, Cano-Jaimez M, McEvoy JP, Spencer J, Walker MC, WilliamsRS. 2015. Seizure control by derivatives of medium chainfatty acids associated with the ketogenic diet show novelbranching-point structure for enhanced potency. J Phar-macol Exp Ther 352: 43–52.
Charlier C, Singh NA, Ryan SG, Lewis TB, Reus BE, LeachRJ, Leppert M. 1998. A pore mutation in a novel KQT-likepotassium channel gene in an idiopathic epilepsy family.Nat Genet 18: 53–55.
Chen CY, Matt L, Hell JW, Rogawski MA. 2014. Perampanelinhibition of AMPA receptor currents in cultured hippo-campal neurons. PLoS ONE 9: e108021.
Cheng CM, Wang K, Eagles DA, Bondy CA. 2004. Caloricrestriction augments brain glutamic acid decarboxylase-65 and -67 expression. J Neurosci Res 77: 270–276.
Cooper EC. 2012. Potassium channels (including KCNQ)and epilepsy. In Jasper’s basic mechanisms of the epilepsies,4th ed. (ed. Noebels JL, et al.), pp. 55–65. Oxford Uni-versity Press, New York.
Coulter DA, Huguenard JR, Prince DA. 1989. Characteriza-tion of ethosuximide reduction of low-threshold calciumcurrent in thalamic relay neurons. Ann Neurol 25: 582–593.
Crunelli V, David F, Leresche N, Lambert RC. 2014. Role forT-type Ca2þ channels in sleep waves. Pflugers Arch 466:735–745.
M.A. Rogawski et al.
22 Cite this article as Cold Spring Harb Perspect Med 2016;6:a022780
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
Press on December 16, 2021 - Published by Cold Spring Harbor Laboratoryhttp://perspectivesinmedicine.cshlp.org/Downloaded from

Cullingford TE, Eagles DA, Sato H. 2002. The ketogenic dietupregulates expression of the gene encoding the key ke-togenic enzyme mitochondrial 3-hydroxy-3-methylglu-taryl-CoA synthase in rat brain. Epilepsy Res 49: 99–107.
Dahlin M, Elfving A, Ungerstedt U, Amark P. 2005. Theketogenic diet influences the levels of excitatory and in-hibitory amino acids in the CSF in children with refrac-tory epilepsy. Epilepsy Res 64: 115–125.
Danober L, Deransart C, Depaulis A, Vergnes M, MarescauxC. 1998. Pathophysiological mechanisms of genetic ab-sence epilepsy in the rat. Prog Neurobiol 55: 27–57.
Davies A, Hendrich J, Van Minh AT, Wratten J, Douglas L,Dolphin AC. 2007. Functional biology of the a2d sub-units of voltage-gated calcium channels. Trends Pharma-col Sci 28: 220–228.
Deckers CL, Czuczwar SJ, Hekster YA, Keyser A, Kubova H,Meinardi H, Patsalos PN, Renier WO, Van Rijn CM. 2000.Selection of antiepileptic drug polytherapy based onmechanisms of action: The evidence reviewed. Epilepsia41: 1364–1374.
Dezsi G, Ozturk E, Stanic D, Powell KL, Blumenfeld H,O’Brien TJ, Jones NC. 2013. Ethosuximide reduces epi-leptogenesis and behavioral comorbidity in the GAERSmodel of genetic generalized epilepsy. Epilepsia 54:635–643.
Ding Y, Wang S, Zhang MM, Guo Y, Yang Y, Weng SQ, WuJM, Qiu X, Ding MP. 2010. Fructose-1,6-diphosphateinhibits seizure acquisition in fast hippocampal kindling.Neurosci Lett 477: 33–36.
Dodgson SJ, Shank RP, Maryanoff BE. 2000. Topiramate asan inhibitor of carbonic anhydrase isoenzymes. Epilepsia41: S35–S39.
Dolphin AC. 2013. The a2d subunits of voltage-gated calci-um channels. Biochim Biophys Acta 1828: 1541–1549.
Dunwiddie TV, Masino SA. 2001. The role and regulation ofadenosine in the central nervous system. Annu Rev Neu-rosci 24: 31–55.
Eid T, Kovacs I, Spencer DD, de Lanerolle NC. 2002. Novelexpression of AMPA-receptor subunit GluR1 on mossycells and CA3 pyramidal neurons in the human epilep-togenic hippocampus. Eur J Neurosci 15: 517–527.
Englund M, Hyllienmark L, Brismar T. 2011. Effect of val-proate, lamotrigine and levetiracetam on excitability andfiring properties of CA1 neurons in rat brain slices. CellMol Neurobiol 31: 645–652.
ffrench-Mullen JM, Barker JL, Rogawski MA. 1993. Calciumcurrent block by (–)-pentobarbital, phenobarbital, andCHEB but not (þ)-pentobarbital in acutely isolated hip-pocampal CA1 neurons: Comparison with effects onGABA-activated Cl2 current. J Neurosci 13: 3211–3221.
Field MJ, Cox PJ, Stott E, Melrose H, Offord J, Su TZ,Bramwell S, Corradini L, England S, Winks J, et al.2006. Identification of the a2-d-1 subunit of voltage-dependent calcium channels as a molecular target forpain mediating the analgesic actions of pregabalin. ProcNatl Acad Sci 103: 17537–17542.
Frahm C, Engel D, Draguhn A. 2001. Efficacy of backgroundGABA uptake in rat hippocampal slices. NeuroReport 12:1593–1596.
Fraser DD, Whiting S, Andrew RD, Macdonald EA, Musa-Veloso K, Cunnane SC. 2003. Elevated polyunsaturated
fatty acids in blood serum obtained from children on theketogenic diet. Neurology 60: 1026–1029.
Freeman JM, Kossoff EH. 2010. Ketosis and the ketogenicdiet, 2010: Advances in treating epilepsy and other dis-orders. Adv Pediatr 57: 315–329.
Fritsch B, Reis J, Gasior M, Kaminski RM, Rogawski MA.2014. Role of GluK1 kainate receptors in seizures, epilep-tic discharges, and epileptogenesis. J Neurosci 34: 5765–5775.
Garcıa-Perez E, Lo DC, Wesseling JF. 2008. Kinetic isolationof a slowly recovering component of short-term depres-sion during exhaustive use at excitatory hippocampalsynapses. J Neurophysiol 100: 781–795.
Garcıa-Perez E, Mahfooz K, Covita J, Zandueta A, WesselingJF. 2015. Levetiracetam accelerates the onset of supply ratedepression in synaptic vesicle trafficking. Epilepsia 56:535–545.
Garriga-Canut M, Schoenike B, Qazi R, Bergendahl K, Da-ley TJ, Pfender RM, Morrison JF, Ockuly J, Stafstrom C,Sutula T, et al. 2006. 2-Deoxy-D-glucose reduces epilepsyprogression by NRSF-CtBP-dependent metabolic regula-tion of chromatin structure. Nat Neurosci 9: 1382–1387.
Gasior M, Rogawski MA, Hartman AL. 2006. Neuroprotec-tive and disease-modifying effects of the ketogenic diet.Behav Pharmacol 17: 431–439.
Gasior M, French A, Joy MT, Tang RS, Hartman AL, Rogaw-ski MA. 2007. The anticonvulsant activity of acetone,the major ketone body in the ketogenic diet, is not de-pendent on its metabolites acetol, 1,2-propanediol,methylglyoxal, or pyruvic acid. Epilepsia 48: 793–800.
Gasior M, Yankura J, Hartman AL, French A, RogawskiMA. 2010. Anticonvulsant and proconvulsant actionsof 2-deoxy-D-glucose. Epilepsia 51: 1385–1394.
Gibbs JW 3rd, Sombati S, DeLorenzo RJ, Coulter DA.2000. Cellular actions of topiramate: Blockade of kai-nate-evoked inward currents in cultured hippocampalneurons. Epilepsia 41: S10–S16.
Gilchrist J, Dutton S, Diaz-Bustamante M, McPherson A,Olivares N, Kalia J, Escayg A, Bosmans F. 2014. Nav1.1modulation by a novel triazole compound attenuates ep-ileptic seizures in rodents. ACS Chem Biol 9: 1204–1212.
Gomora JC, Daud AN, Weiergraber M, Perez-Reyes E. 2001.Block of cloned human T-type calcium channels by suc-cinimide antiepileptic drugs. Mol Pharmacol 60: 1121–1132.
Goren MZ, Onat F. 2007. Ethosuximide: From bench tobedside. CNS Drug Rev 13: 224–239.
Grigorov A, Moskalyuk A, Kravchenko M, Veselovsky N,Verkhratsky A, Fedulova S. 2014. Kv7 potassium channelsubunits and M currents in cultured hippocampal inter-neurons. Pflugers Arch 466:1747–1758.
Grunnet M, Strøbæk D, Hougaard C, Christophersen P.2014. Kv7 channels as targets for anti-epileptic and psy-chiatric drug-development. Eur J Pharmacol 726: 133–137.
Gu N, Vervaeke K, Hu H, Storm JF. 2005. Kv7/KCNQ/Mand HCN/h, but not KCa2/SK channels, contribute tothe somatic medium after-hyperpolarization and excit-ability control in CA1 hippocampal pyramidal cells. JPhysiol 566: 689–715.
Antiseizure Drugs and the Ketogenic Diet
Cite this article as Cold Spring Harb Perspect Med 2016;6:a022780 23
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
Press on December 16, 2021 - Published by Cold Spring Harbor Laboratoryhttp://perspectivesinmedicine.cshlp.org/Downloaded from

Gunthorpe MJ, Large CH, Sankar R. 2012. The mechanismof action of retigabine (ezogabine), a first-in-class Kþ
channel opener for the treatment of epilepsy. Epilepsia53: 412–424.
Hadera MG, Smeland OB, McDonald TS, Tan KN, Sonne-wald U, Borges K. 2014. Triheptanoin partially restoreslevels of tricarboxylic acid cycle intermediates in themouse pilocarpine model of epilepsy. J Neurochem 129:107–119.
Hanada T, Hashizume Y, Tokuhara N, Takenaka O, Koh-mura N, Ogasawara A, Hatakeyama S, Ohgoh M, UenoM, Nishizawa Y. 2011. Perampanel: A novel, orally active,noncompetitive AMPA-receptor antagonist that reducesseizure activity in rodent models of epilepsy. Epilepsia 52:1331–1340.
Hassel B, Dingledine R. 2012. Glutamate and glutamatereceptors. In Basic neurochemistry: Principles of molecu-lar, cellular, and medical neurobiology, 8th ed. (ed. Scott T,Brady ST, Siegel GJ, et al.), pp. 343–366. Elsevier, Am-sterdam.
Hermann R, Ferron GM, Erb K, Knebel N, Ruus P, Paul J,Richards L, Cnota HP, Troy S. 2003. Effects of age and sexon the disposition of retigabine. Clin Pharmacol Ther 73:61–70.
Hoppa MB, Lana B, Margas W, Dolphin AC, Ryan TA. 2012.a2d Expression sets presynaptic calcium channel abun-dance and release probability. Nature 486: 122–125.
Houser CR. 2014. Do structural changes in GABA neuronsgive rise to the epileptic state? Adv Exp Med Biol 813:151–160.
Hu H, Vervaeke K, Storm JF. 2007. M-channels (Kv7/KCNQchannels) that regulate synaptic integration, excitability,and spike pattern of CA1 pyramidal cells are located inthe perisomatic region. J Neurosci 27: 1853–1867.
Huang CW, Kuo CC. 2015. Flow- and voltage-dependentblocking effect of ethosuximide on the inward rectifierKþ (Kir2.1) channel. Pflugers Arch 467: 1733–1746.
Hughes JR. 2009. Absence seizures: A review of recent re-ports with new concepts. Epilepsy Behav 15: 404–412.
Huguenard JR. 1996. Low-threshold calcium currents incentral nervous system neurons. Annu Rev Physiol 58:329–358.
Huguenard JR. 2002. Block of T-type Ca2þ channels is animportant action of succinimide antiabsence drugs. Ep-ilepsy Curr 2: 49–52.
Huttenlocher PR. 1976. Ketonemia and seizures: Metabolicand anticonvulsant effects of two ketogenic diets in child-hood epilepsy. Pediatr Res 10: 536–540.
Huttenlocher PR, Wilbourn AJ, Signore JM. 1971. Medium-chain triglycerides as a therapy for intractable childhoodepilepsy. Neurology 21: 1097–1103.
Jarrett SG, Milder JB, Liang LP, Patel M. 2008. The ketogenicdiet increases mitochondrial glutathione levels. J Neuro-chem 106: 1044–1051.
Juge N, Gray JA, Omote H, Miyaji T, Inoue T, Hara C, Un-eyama H, Edwards RH, Nicoll RA, Moriyama Y. 2010.Metabolic control of vesicular glutamate transport andrelease. Neuron 68: 99–112.
Kaminski RM, Gillard M, Klitgaard H. 2012. TargetingSV2A for discovery of antiepileptic drugs. In Jasper’s basic
mechanisms of the epilepsies, 4th ed. (ed. Noebels JL,et al.), pp. 974–983. Oxford University Press, New York.
Kaminski RM, Rogawski MA, Klitgaard H. 2014. The po-tential of antiseizure drugs and agents that act on novelmolecular targets as antiepileptogenic treatments. Neuro-therapeutics 11: 385–400.
Kapetanovic IM, Yonekawa WD, Kupferberg HJ. 1995. Theeffects of D-23129, a new experimental anticonvulsantdrug, on neurotransmitter amino acids in the rat hippo-campus in vitro. Epilepsy Res 22: 167–173.
Kasteleijn-Nolst Trenite D, Brandt C, Mayer T, Rosenow F,Schmidt B, Steinhoff BJ, Gardin A, Imbert G, Johns D,Sagkriotis A, et al. 2015. Dose-dependent suppression ofhuman photoparoxysmal response with the competitiveAMPA/kainate receptor antagonist BGG492: Clear PK/PD relationship. Epilepsia 56: 924–932.
Keith HM. 1933. Factors influencing experimentally pro-duced convulsions. Arch Neurol Psychiatry 29: 148–154.
Kim DY, Davis LM, Sullivan PG, Maalouf M, Simeone TA,van Brederode J, Rho JM. 2007. Ketone bodies are pro-tective against oxidative stress in neocortical neurons. JNeurochem 101: 1316–1326.
Kim DY, Vallejo J, Rho JM. 2010. Ketones prevent synapticdysfunction induced by mitochondrial respiratory com-plex inhibitors. J Neurochem 114: 130–141.
Kim TH, Borges K, Petrou S, Reid CA. 2013. Triheptanoinreduces seizure susceptibility in a syndrome-specificmouse model of generalized epilepsy. Epilepsy Res 103:101–105.
Kim DY, Simeone KA, Simeone TA, Pandya JD, Wilke JC,Ahn Y, Geddes JW, Sullivan PG, Rho JM. 2015. Ketonebodies mediate antiseizure effects through mitochondrialpermeability transition. Ann Neurol 78: 77–87.
Kimura I, Inoue D, Maeda T, Hara T, Ichimura A, MiyauchiS, Kobayashi M, Hirasawa A, Tsujimoto G. Short-chainfatty acids and ketones directly regulate sympathetic ner-vous system via G protein-coupled receptor 41 (GPR41).2011. Proc Natl Acad Sci 108: 8030–8035.
Lambert RC, Bessaıh T, Crunelli V, Leresche N. 2014. Themany faces of T-type calcium channels. Pflugers Arch 466:415–423.
Lawrence JJ, Saraga F, Churchill JF, Statland JM, Travis KE,Skinner FK, McBain CJ. 2006. Somatodendritic Kv7/KCNQ/M channels control interspike interval in hippo-campal interneurons. J Neurosci 26: 12325–12338.
Lennox WG, Cobb S. 1928. Epilepsy: From the standpoint ofphysiology and treatment. Medicine 7: 105–290.
Leppik IE, Sherwin AL. 1977. Anticonvulsant activity ofphenobarbital and phenytoin in combination. J Pharma-col Exp Ther 200: 570–575.
Li G, Nowak M, Bauer S, Schlegel K, Stei S, Allenhofer L,Waschbisch A, Tackenberg B, Hollerhage M, HoglingerGU, et al. 2013. Levetiracetam but not valproate inhibitsfunction of CD8þ T lymphocytes. Seizure 22: 462–466.
Lian XY, Khan FA, Stringer JL. 2007. Fructose-1,6-bisphos-phate has anticonvulsant activity in models of acute sei-zures in adult rats. J Neurosci 27: 12007–12011.
Likhodii SS, Serbanescu I, Cortez MA, Murphy P, Snead OCIII, Burnham WM. 2003. Anticonvulsant properties ofacetone, a brain ketone elevated by the ketogenic diet.Ann Neurol 54: 219–226.
M.A. Rogawski et al.
24 Cite this article as Cold Spring Harb Perspect Med 2016;6:a022780
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
Press on December 16, 2021 - Published by Cold Spring Harbor Laboratoryhttp://perspectivesinmedicine.cshlp.org/Downloaded from

Liu YM, Wang HS. 2013. Medium-chain triglycerideketogenic diet, an effective treatment for drug-resistantepilepsy and a comparison with other ketogenic diets.Biomed J 36: 9–15.
Loscher W. 1989. Valproate enhances GABA turnover in thesubstantia nigra. Brain Res 501: 198–203.
Loscher W. 1998. Pharmacology of glutamate receptor an-tagonists in the kindling model. In Kindling 5 (ed. Cor-coran ME, Moshe SL), pp. 435–449. Plenum, New York.
Loscher W. 2002. Basic pharmacology of valproate: A reviewafter 35 years of clinical use for the treatment of epilepsy.CNS Drugs 16: 669–694.
Loscher W, Rogawski MA. 2012. How theories evolved con-cerning the mechanism of action of barbiturates. Epilep-sia 53: 12–25.
Loscher W, Jackel R, Muller F. 1989. Anticonvulsant andproconvulsant effects of inhibitors of GABA degradationin the amygdala-kindling model. Eur J Pharmacol 163:1–14.
Loscher W, Honack D, Taylor CP. 1991. Gabapentin increas-es aminooxyacetic acid-induced GABA accumulation inseveral regions of rat brain. Neurosci Lett 128: 150–154.
Loscher W, Honack D, Bloms-Funke P. 1996. The novelantiepileptic drug levetiracetam (ucb L059) induces al-terations in GABA metabolism and turnover in discreteareas of rat brain and reduces neuronal activity in sub-stantia nigra pars reticulata. Brain Res 735: 208–216.
Lotarski SM, Donevan S, El-Kattan A, Osgood S, Poe J,Taylor CP, Offord J. 2011. Anxiolytic-like activity of pre-gabalin in the Vogel conflict test in a2d-1 (R217A) anda2d-2 (R279A) mouse mutants. J Pharmacol Exp Ther338: 615–621.
Lynch BA, Matagne A, Brannstrom A, von Euler A, JanssonM, Hauzenberger E, Soderhall JA. 2008. Visualization ofSV2A conformations in situ by the use of protein tomog-raphy. Biochem Biophys Res Commun 375: 491–495.
Lyseng-Williamson KA. 2011. Spotlight on levetiracetam inepilepsy. CNS Drugs 25: 901–905.
Ma W, Berg J, Yellen G. 2007. Ketogenic diet metabolitesreduce firing in central neurons by opening KATP chan-nels. J Neurosci 27: 3618–3625.
Maalouf M, Rho JM. 2008. Oxidative impairment of hip-pocampal long-term potentiation involves activation ofprotein phosphatase 2A and is prevented by ketone bod-ies. J Neurosci Res 86: 3322–3330.
Maalouf M, Sullivan PG, Davis L, Kim DY, Rho JM. 2007.Ketones inhibit mitochondrial production of reactive ox-ygen species production following glutamate excitotox-icity by increasing NADH oxidation. Neuroscience 145:256–264.
Mantegazza M, Curia G, Biagini G, Ragsdale DS, Avoli M.2010. Voltage-gated sodium channels as therapeutic tar-gets in epilepsy and other neurological disorders. LancetNeurol 9: 413–424.
Mantis JG, Centeno NA, Todorova MT, McGowan R, Sey-fried TN. 2004. Management of multifactorial idiopathicepilepsy in EL mice with caloric restriction and the keto-genic diet: Role of glucose and ketone bodies. Nutr Metab(Lond) 1: 11.
Margolis JM, Chu BC, Wang ZJ, Copher R, Cavazos JE.2014. Effectiveness of antiepileptic drug combination
therapy for partial-onset seizures based on mechanismsof action. JAMA Neurol 71: 985–993.
Martire M, Castaldo P, D’Amico M, Preziosi P, AnnunziatoL, Taglialatela M. 2004. M channels containing KCNQ2subunits modulate norepinephrine, aspartate, and GABArelease from hippocampal nerve terminals. J Neurosci24: 592–597.
Masino SA, Rho JM. 2012. Mechanisms of ketogenic dietaction. In Jasper’s basic mechanisms of the epilepsies, 4thed. (ed. Noebels JL, et al.), pp. 1003–1024. OxfordUniversity Press, New York.
Masino SA, Li T, Theofilas P, Sandau US, Ruskin DN, Fred-holm BB, Geiger JD, Aronica E, Boison D. 2011. A keto-genic diet suppresses seizures in mice through adenosineA1 receptors. J Clin Invest 121: 2679–2683.
Masino SA, Kawamura M Jr, Ruskin DN, Geiger JD, BoisonD. 2012. Purines and neuronal excitability: Links to theketogenic diet. Epilepsy Res 100: 229–238.
Matar N, Jin W, Wrubel H, Hescheler J, Schneider T, Weier-graber M. 2009. Zonisamide block of cloned humanT-type voltage-gated calcium channels. Epilepsy Res 83:224–234.
Mathern GW, Pretorius JK, Mendoza D, Lozada A, Leite JP,Chimelli L, Fried I, Sakamoto AC, Assirati JA, AdelsonPD. 1998. Increased hippocampal AMPA and NMDAreceptor subunit immunoreactivity in temporal lobe ep-ilepsy patients. J Neuropathol Exp Neurol 57: 615–634.
Mazzuferi M, Kumar G, van Eyll J, Danis B, Foerch P, Ka-minski RM. 2013. Nrf2 defense pathway: Experimentalevidence for its protective role in epilepsy. Ann Neurol74: 560–568.
Medina-Kauwe LK, Tobin AJ, De Meirleir L, Jaeken J, JakobsC, Nyhan WL, Gibson KM. 1999. 4-Aminobutyrate ami-notransferase (GABA-transaminase) deficiency. J InheritMetab Dis 22: 414–427.
Meehan AL, Yang X, McAdams BD, Yuan L, Rothman SM.2011. A new mechanism for antiepileptic drug action:Vesicular entry may mediate the effects of levetiracetam.J Neurophysiol 106: 1227–1239.
Meehan AL, Yang X, Yuan LL, Rothman SM. 2012. Leveti-racetam has an activity-dependent effect on inhibitorytransmission. Epilepsia 53: 469–476.
Meldrum BS, Rogawski MA. 2007. Molecular targetsfor antiepileptic drug development. Neurotherapeutics4: 18–61.
Melo TM, Nehlig A, Sonnewald U. 2006. Neuronal-glialinteractions in rats fed a ketogenic diet. Neurochem Int48: 498–507.
Michael-Titus AT, Priestley JV. 2013. Omega-3 fatty acidsand traumatic neurological injury: From neuroprotec-tion to neuroplasticity? Trends Neurosci 37: 30–38.
Milder JB, Liang LP, Patel M. 2010. Acute oxidative stressand systemic Nrf2 activation by the ketogenic diet. Neu-robiol Dis 40: 238–244.
Morris AA. 2005. Cerebral ketone body metabolism.J Inherit Metab Dis 28: 109–121.
Mueller SG, Trabesinger AH, Boesiger P, Wieser HG. 2001.Brain glutathione levels in patients with epilepsy mea-sured by in vivo 1H-MRS. Neurology 57: 1422–1427.
Neal EG, Chaffe H, Schwartz RH, Lawson MS, Edwards N,Fitzsimmons G, Whitney A, Cross JH. 2008. The keto-
Antiseizure Drugs and the Ketogenic Diet
Cite this article as Cold Spring Harb Perspect Med 2016;6:a022780 25
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
Press on December 16, 2021 - Published by Cold Spring Harbor Laboratoryhttp://perspectivesinmedicine.cshlp.org/Downloaded from

genic diet for the treatment of childhood epilepsy: Arandomised controlled trial. Lancet Neurol 7: 500–506.
Neal EG, Chaffe H, Schwartz RH, Lawson MS, Edwards N,Fitzsimmons G, Whitney A, Cross JH. 2009. A random-ized trial of classical and medium-chain triglycerideketogenic diets in the treatment of childhood epilepsy.Epilepsia 50: 1109–1117.
Neuman R, Cherubini E, Ben-Ari Y. 1988. Epileptiformbursts elicited in CA3 hippocampal neurons by a varietyof convulsants are not blocked by N-methyl-D-aspartateantagonists. Brain Res 459: 265–274.
Oliva M, Berkovic SF, Petrou S. 2012. Sodium channels andthe neurobiology of epilepsy. Epilepsia 53: 1849–1859.
Olsen RW, Sieghart W. 2009. GABAA receptors: Subtypesprovide diversity of function and pharmacology. Neuro-pharmacology 56: 141–148.
Otto JF, Kimball MM, Wilcox KS. 2002. Effects of theanticonvulsant retigabine on cultured cortical neurons:Changes in electroresponsive properties and synaptictransmission. Mol Pharmacol 61: 921–927.
Overstreet LS, Westbrook GL. 2001. Paradoxical reductionof synaptic inhibition by vigabatrin. J Neurophysiol 86:596–603.
Pascual JM, Liu P, Mao D, Kelly DI, Hernandez A, Sheng M,Good LB, Ma Q, Marin-Valencia I, Zhang X, et al. 2014.Triheptanoin for glucose transporter type I deficiency(G1D): Modulation of human ictogenesis, cerebral met-abolic rate, and cognitive indices by a food supplement.JAMA Neurol 71: 1255–1265.
Patino GA, Isom LL. 2010. Electrophysiology and beyond:Multiple roles of Naþ channelb subunits in developmentand disease. Neurosci Lett 486: 53–59.
Peterman MG. 1924. The ketogenic diet in the treatment ofepilepsy: A preliminary report. Am J Dis Child 28: 28–33.
Petroff OAC, Behar KL, Mattson RH, Rothman DL. 1996a.Human brain g-aminobutyric acid levels and seizurecontrol following initiation of vigabatrin therapy. J Neu-rochem 67: 2399–4404.
Petroff OAC, Rothman DL, Behar KL, Lamoureux D, Matt-son RH. 1996b. The effect of gabapentin on brain g-aminobutyric acid in patients with epilepsy. Ann Neurol39: 95–99.
Pierre K, Pellerin L. 2005. Monocarboxylate transporters inthe central nervous system: Distribution, regulation andfunction. J Neurochem 94: 1–14.
Porta N, Vallee L, Lecointe C, Bouchaert E, Staels B, BordetR, Auvin S. 2009. Fenofibrate, a peroxisome proliferator-activated receptor-a agonist, exerts anticonvulsive prop-erties. Epilepsia 50: 943–948.
Powell KL, Cain SM, Snutch TP, O’Brien TJ. 2014. Lowthreshold T-type calcium channels as targets for novelepilepsy treatments. Br J Clin Pharmacol 77: 729–739.
Ragsdale DS, McPhee JC, Scheuer T, Catterall WA. 1996.Common molecular determinants of local anesthetic,antiarrhythmic, and anticonvulsant block of voltage-gated Naþ channels. Proc Natl Acad Sci 93: 9270–9275.
Reddy DS, Rogawski MA. 2002. Stress-induced deoxycorti-costerone-derived neurosteroids modulate GABAA re-ceptor function and seizure susceptibility. J Neurosci 22:3795–3805.
Rho JM, Donevan SD, Rogawski MA. 1994. Mechanism ofaction of the anticonvulsant felbamate: Opposing effectson N-methyl-D-aspartate and g-aminobutyric acidA re-ceptors. Ann Neurol 35: 229–234.
Rho JM, Donevan SD, Rogawski MA. 1996. Direct activa-tion of GABAA receptors by barbiturates in cultured rathippocampal neurons. J Physiol 497: 509–522.
Rigoulot MA, Boehrer A, Nehlig A. 2003. Effects of topir-amate in two models of genetically determined general-ized epilepsy, the GAERS and the Audiogenic Wistar AS.Epilepsia 44: 14–19.
Rogawski MA. 2006. Diverse mechanisms of antiepilepticdrugs in the development pipeline. Epilepsy Res 69: 273–294.
Rogawski MA. 2013. AMPA receptors as a molecular targetin epilepsy therapy. Acta Neurol Scand Suppl 197: 9–18.
Rogawski MA, Cavazos JE. 2015. Mechanisms of action ofantiepileptic drugs. In Wyllie’s treatment of epilepsy: Prin-ciples and practice, 6th ed. (ed. Wyllie E.), pp. 522–529.Wolters Kluwer, Philadelphia.
Rogawski MA, Hanada T. 2013. Preclinical pharmacology ofperampanel, a selective non-competitive AMPA receptorantagonist. Acta Neurol Scand 127: 19–24.
Rogawski MA, Porter RJ. 1990. Antiepileptic drugs:Pharmacological mechanisms and clinical efficacy withconsideration of promising developmental stage com-pounds. Pharmacol Rev 42: 223–286.
Rogawski MA, Kurzman PS, Yamaguchi SI, Li H. 2001. Roleof AMPA and GluR5 kainate receptors in the develop-ment and expression of amygdala kindling in the mouse.Neuropharmacology 40: 28–35.
Rogawski MA, Tofighy A, White HS, Matagne A, Wolff C.2015. Current understanding of the mechanism of actionof the antiepileptic drug lacosamide. Epilepsy Res 110:189–205.
Rowley S, Patel M. 2013. Mitochondrial involvement andoxidative stress in temporal lobe epilepsy. Free Radic BiolMed 62: 121–131.
Rundfeldt C, Netzer R. 2000. Investigations into the mech-anism of action of the new anticonvulsant retigabine.Interaction with GABAergic and glutamatergic neuro-transmission and with voltage gated ion channels. Arz-neimittelforschung 50: 1063–1070.
Sahara S, Yanagawa Y, O’Leary DD, Stevens CF. 2012. Thefraction of cortical GABAergic neurons is constant fromnear the start of cortical neurogenesis to adulthood.J Neurosci 32: 4755–4761.
Schlanger S, Shinitzky M, Yam D. 2002. Diet enriched withomega-3 fatty acids alleviates convulsion symptoms inepilepsy patients. Epilepsia 43: 103–104.
Schousboe A, Madsen KK, Barker-Haliski ML, White HS.2014. The GABA synapse as a target for antiepilepticdrugs: A historical overview focused on GABA transport-ers. Neurochem Res 39: 1980–1987.
Shank RP, Maryanoff BE. 2008. Molecular pharmacody-namics, clinical therapeutics, and pharmacokinetics oftopiramate. CNS Neurosci Ther 14: 120–142.
Shimazu T, Hirschey MD, Newman J, He W, Shirakawa K, LeMoan N, Grueter CA, Lim H, Saunders LR, Stevens RD,et al. 2013. Suppression of oxidative stress by b-hydroxy-
M.A. Rogawski et al.
26 Cite this article as Cold Spring Harb Perspect Med 2016;6:a022780
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
Press on December 16, 2021 - Published by Cold Spring Harbor Laboratoryhttp://perspectivesinmedicine.cshlp.org/Downloaded from

butyrate, an endogenous histone deacetylase inhibitor.Science 339: 211–214.
Silverman RB, Andruszkiewicz R, Nanavati SM, Taylor CP,Vartanian MG. 1991. 3-Alkyl-4-aminobutyric acids: Thefirst class of anticonvulsant agents that activates L-glu-tamic acid decarboxylase. J Med Chem 34: 2295–2298.
Simeone TA, Wilcox KS, White HS. 2011. Topiramatemodulation ofb1- andb3-homomeric GABAA receptors.Pharmacol Res 64: 44–52.
Sohal VS, Keist R, Rudolph U, Huguenard JR. 2003. Dynam-ic GABAA receptor subtype-specific modulation of thesynchrony and duration of thalamic oscillations. J Neuro-sci 23: 3649–3657.
Stafstrom CE. 2007. Persistent sodium current and its role inepilepsy. Epilepsy Curr 7: 15–22.
Stafstrom CE, Rho JM. 2012. The ketogenic diet as a treat-ment paradigm for diverse neurological disorders. FrontPharmacol 3: 59.
Stafstrom CE, Ockuly JC, Murphree L, Valley MT, Roopra A,Sutula TP. 2009. Anticonvulsant and antiepileptic actionsof 2-deoxy-D-glucose in epilepsy models. Ann Neurol65: 435–447.
Stafstrom CE, Arnason BG, Baram TZ, Catania A, CortezMA, Glauser TA, Pranzatelli MR, Riikonen R, RogawskiMA, Shinnar S, et al. 2011. Treatment of infantile spasms:Emerging insights from clinical and basic science per-spectives. J Child Neurol 26: 1411–1421.
Stahl SM, Porreca F, Taylor CP, Cheung R, Thorpe AJ, ClairA. 2013. The diverse therapeutic actions of pregabalin: Isa single mechanism responsible for several pharmacolog-ical activities? Trends Pharmacol Sci 34: 332–339.
Steinhoff BJ, Ben-Menachem E, Ryvlin P, Shorvon S, KramerL, Satlin A, Squillacote D, Yang H, Zhu J, Laurenza A.2013. Efficacy and safety of adjunctive perampanel for thetreatment of refractory partial seizures: A pooled analysisof three phase III studies. Epilepsia 54: 1481–1499.
Stuchlık A, Kubova H, Mares P. 2001. Single systemic dose ofvigabatrin induces early proconvulsant and later anticon-vulsant effect in rats. Neurosci Lett 312: 37–40.
Sullivan PG, Dube C, Dorenbos K, Steward O, Baram TZ.2003. Mitochondrial uncoupling protein-2 protects theimmature brain from excitotoxic neuronal death. AnnNeurol 53: 711–717.
Sullivan PG, Rippy NA, Dorenbos K, Concepcion RC, Agar-wal AK, Rho JM. 2004. The ketogenic diet increases mi-tochondrial uncoupling protein levels and activity. AnnNeurol 55: 576–580.
Sun GC, Werkman TR, Battefeld A, Clare JJ, Wadman WJ.2007. Carbamazepine and topiramate modulation oftransient and persistent sodium currents studied inHEK293 cells expressing the Nav1.3 a-subunit. Epilepsia48: 774–782.
Suzuki S, Rogawski MA. 1989. T-type calcium channelsmediate the transition between tonic and phasic firingin thalamic neurons. Proc Natl Acad Sci 86: 7228–7232.
Suzuki T, Motohashi H, Yamamoto M. 2013. Toward clinicalapplication of the Keap1-Nrf2 pathway. Trends Pharma-col Sci 34: 340–346.
Sveinbjornsdottir S, Sander JW, Upton D, Thompson PJ,Patsalos PN, Hirt D, Emre M, Lowe D, Duncan JS.1993. The excitatory amino acid antagonist D-CPP-ene
(SDZ EAA-494) in patients with epilepsy. Epilepsy Res 16:165–174.
Taha AY, Ryan MA, Cunnane SC. 2005. Despite transientketosis, the classic high-fat ketogenic diet induces markedchanges in fatty acid metabolism in rats. Metabolism 54:1127–1132.
Taha AY, Burnham WM, Auvin S. 2010. Polyunsaturatedfatty acids and epilepsy. Epilepsia 51: 1348–1358.
Talley EM, Cribbs LL, Lee JH, Daud A, Perez-Reyes E, BaylissDA. 1999. Differential distribution of three members of agene family encoding low voltage-activated (T-type) cal-cium channels. J Neurosci 19: 1895–1911.
Tanner GR, Lutas A, Martinez-Francois JR, Yellen G. 2011.Single KATP channel opening in response to action po-tential firing in mouse dentate granule neurons. J Neuro-sci 31: 8689–8696.
Tatulian L, Brown DA. 2003. Effect of the KCNQ potassiumchannel opener retigabine on single KCNQ2/3 channelsexpressed in CHO cells. J Physiol 549: 57–63.
Taylor CP, Vartanian MG, Andruszkiewiewicz R, SilvermanRB. 1992. 3-Alkyl GABA and 3-alkylglutamic acid ana-logues: Two new classes of anticonvulsant agents. EpilepsyRes 11: 103–110.
Taylor CP, Angelotti T, Fauman E. 2007. Pharmacology andmechanism of action of pregabalin: The calcium channela2-d (alpha2-delta) subunit as a target for antiepilepticdrug discovery. Epilepsy Res 73: 137–150.
Thio LL, Wong M, Yamada KA. 2000. Ketone bodies do notdirectly alter excitatory or inhibitory hippocampal syn-aptic transmission. Neurology 54: 325–331.
Thompson SM, Gahwiler BH. 1992. Effects of the GABAuptake inhibitor tiagabine on inhibitory synaptic poten-tials in rat hippocampal slice cultures. J Neurophysiol67: 1698–1701.
Treven M, Koenig X, Assadpour E, Gantumur E, Meyer C,Hilber K, Boehm S, Kubista H. 2015. The anticonvulsantretigabine is a subtype selective modulator of GABAA
receptors. Epilepsia 56: 647–657.
Turner JP, Salt TE. 1998. Characterization of sensory andcorticothalamic excitatory inputs to rat thalamocorticalneurones in vitro. J Physiol 510: 829–843.
Twele F, Bankstahl M, Klein S, Romermann K, Loscher W.2015. The AMPA receptor antagonist NBQX exerts anti-seizure but not antiepileptogenic effects in the intrahip-pocampal kainate mouse model of mesial temporal lobeepilepsy. Neuropharmacology 95: 234–242.
Tzingounis AV, Heidenreich M, Kharkovets T, Spitzmaul G,Jensen HS, Nicoll RA, Jentsch TJ. 2010. The KCNQ5potassium channel mediates a component of the after-hyperpolarization current in mouse hippocampus. ProcNatl Acad Sci 107: 10232–10237.
U.S. Food and Drug Administration 2010. Ezogabine forpartial seizures in epilepsy (NDA-022345). Peripheraland Central Nervous System Drugs Advisory CommitteeBriefing Document U.S. Food and Drug Administration,Jersey City, NJ.
Vacher H, Mohapatra DP, Trimmer JS. 2008. Localizationand targeting of voltage-dependent ion channels inmammalian central neurons. Physiol Rev 88: 1407–1447.
Vervaeke K, Gu N, Agdestein C, Hu H, Storm JF. 2006. Kv7/KCNQ/M-channels in rat glutamatergic hippocampal
Antiseizure Drugs and the Ketogenic Diet
Cite this article as Cold Spring Harb Perspect Med 2016;6:a022780 27
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
Press on December 16, 2021 - Published by Cold Spring Harbor Laboratoryhttp://perspectivesinmedicine.cshlp.org/Downloaded from

axons and their role in regulation of excitability andtransmitter release. J Physiol 576.1: 235–256.
Vreugdenhil M, Bruehl C, Voskuyl RA, Kang JX, Leaf A,Wadman WJ. 1996. Polyunsaturated fatty acids modulatesodium and calcium currents in CA1 neurons. Proc NatlAcad Sci 93: 12559–12563.
Wakita M, Kotani N, Kogure K, Akaike N. 2014. Inhibitionof excitatory synaptic transmission in hippocampal neu-rons by levetiracetam involves Zn2þ-dependent GABAtype A receptor-mediated presynaptic modulation. JPharmacol Exp Ther 348: 246–259.
Waldmeier PC, Baumann PA, Wicki P, Feldtrauer JJ, StierlinC, Schmutz M. 1995. Similar potency of carbamazepine,oxcarbazepine, and lamotrigine in inhibiting the releaseof glutamate and other neurotransmitters. Neurology45: 1907–1913.
Walker MC, Kullmann DM. 2012. Tonic GABAA receptor-mediated signaling in epilepsy. In Jasper’s basic mecha-nisms of the epilepsies, 4th ed. (Noebels JL, et al., eds.),pp. 111–121. Oxford University Press, New York.
Walker MC, Williams RS. 2013. The search for better epi-lepsy treatments: From slime mould to coconuts. Bio-chem Soc Trans 41: 1625–1628.
Weissmann C, Di Guilmi MN, Urbano FJ, Uchitel OD. 2013.Acute effects of pregabalin on the function and cellulardistribution of CaV2.1 in HEK293t cells. Brain Res Bull90: 107–113.
Wheless JW. 2008. History of the ketogenic diet. Epilepsia49: 3–5.
Willis S, Stoll J, Sweetman L, Borges K. 2010. Anticonvulsanteffects of a triheptanoin diet in two mouse chronic seiz-ure models. Neurobiol Dis 40: 565–572.
Won YJ, Lu VB, Puhl HL 3rd, Ikeda SR. 2013. b-Hy-droxybutyrate modulates N-type calcium channels inrat sympathetic neurons by acting as an agonist forthe G-protein-coupled receptor FFA3. J Neurosci 33:19314–19325.
Wu Y, Wang W, Richerson GB. 2003. Vigabatrin inducestonic inhibition via GABA transporter reversal withoutincreasing vesicular GABA release. J Neurophysiol 89:2021–2034.
Yamaguchi S, Donevan SD, Rogawski MA. 1993. Anticon-vulsant activity of AMPA/kainate antagonists: Compar-ison of GYKI 52466 and NBOX in maximal electroshockand chemoconvulsant seizure models. Epilepsy Res 15:179–184.
Yu FH, Catterall WA. 2003. Overview of the voltage-gatedsodium channel family. Genome Biol 4: 207.
Yudkoff M, Daikhin Y, Nissim I, Horyn O, Lazarow A, Lu-hovyy B, Wehrli S. 2005. Response of brain amino acidmetabolism to ketosis. Neurochem Int 47: 119–128.
Yue C, Yaari Y. 2006. Axo-somatic and apical dendritic Kv7/M channels differentially regulate the intrinsic excitabil-ity of adult rat CA1 pyramidal cells. J Neurophysiol 95:3480–3495.
Yuen AW, Sander JW, Fluegel D, Patsalos PN, Bell GS, John-son T, Koepp MJ. 2005. Omega-3 fatty acid supplemen-tation in patients with chronic epilepsy: A randomizedtrial. Epilepsy Behav 7: 253–258.
Zilles K, Qu MS, Kohling R, Speckmann EJ. 1999. Iono-tropic glutamate and GABA receptors in human epilepticneocortical tissue: Quantitative in vitro receptor autora-diography. Neuroscience 94: 1051–1061.
M.A. Rogawski et al.
28 Cite this article as Cold Spring Harb Perspect Med 2016;6:a022780
ww
w.p
ersp
ecti
vesi
nm
edic
ine.
org
Press on December 16, 2021 - Published by Cold Spring Harbor Laboratoryhttp://perspectivesinmedicine.cshlp.org/Downloaded from

January 22, 20162016; doi: 10.1101/cshperspect.a022780 originally published onlineCold Spring Harb Perspect Med
Michael A. Rogawski, Wolfgang Löscher and Jong M. Rho Mechanisms of Action of Antiseizure Drugs and the Ketogenic Diet
Subject Collection Epilepsy: The Biology of a Spectrum Disorder
Research ChallengesThe Epilepsy Spectrum: Targeting Future
Gregory L. Holmes and Jeffrey L. Noebels EpilepsyEpileptogenesis and the Comorbidities of Common Mechanisms Underlying
Andrey Mazarati and Raman SankarRole of Sodium Channels in Epilepsy
David I. Kaplan, Lori L. Isom and Steven PetrouComorbiditiesImpact the Development of Epilepsy and
Epilepsy Model: How Past Events−The Diathesis
Christophe Bernard
the Ketogenic DietMechanisms of Action of Antiseizure Drugs and
M. RhoMichael A. Rogawski, Wolfgang Löscher and Jong
Potassium Channels in EpilepsyRüdiger Köhling and Jakob Wolfart
Epilepsy and AutismAshura W. Buckley and Gregory L. Holmes
GABAergic Synchronization in EpilepsyRoustem Khazipov
Immunity and Inflammation in Epilepsy
AronicaAnnamaria Vezzani, Bethan Lang and Eleonora
Status Epilepticus
ShinnarSyndi Seinfeld, Howard P. Goodkin and Shlomo
Nucleotide-Gated (HCN) Channels in EpilepsyHyperpolarization-Activated Cyclic
PoolosGary P. Brennan, Tallie Z. Baram and Nicholas P.
Genetic ModelsNeonatal and Infantile Epilepsy: Acquired and
Aristea S. Galanopoulou and Solomon L. Moshé
The Role of Calcium Channels in EpilepsySanjeev Rajakulendran and Michael G. Hanna
Epigenetics and EpilepsyDavid C. Henshall and Katja Kobow
EpilepsyInterneuron Transplantation as a Treatment for
Robert F. Hunt and Scott C. BarabanCells in Network SynchronizationMicrocircuits in Epilepsy: Heterogeneity and Hub
Anh Bui, Hannah K. Kim, Mattia Maroso, et al.
http://perspectivesinmedicine.cshlp.org/cgi/collection/ For additional articles in this collection, see
Copyright © 2016 Cold Spring Harbor Laboratory Press; all rights reserved
Press on December 16, 2021 - Published by Cold Spring Harbor Laboratoryhttp://perspectivesinmedicine.cshlp.org/Downloaded from