mechanism of action and safety of heartburn therapies · tinct mechanism of action. most antacids...
TRANSCRIPT
PRACTICAL GASTROENTEROLOGY • APRIL 200380
INTRODUCTION
Heartburn, a substernal burning rising up from thestomach to the lower chest and neck (1), is theprimary symptom of gastroesophageal reflux dis-
ease (GERD). Heartburn is one of the most commoncomplaints of patients presenting to physicians, with
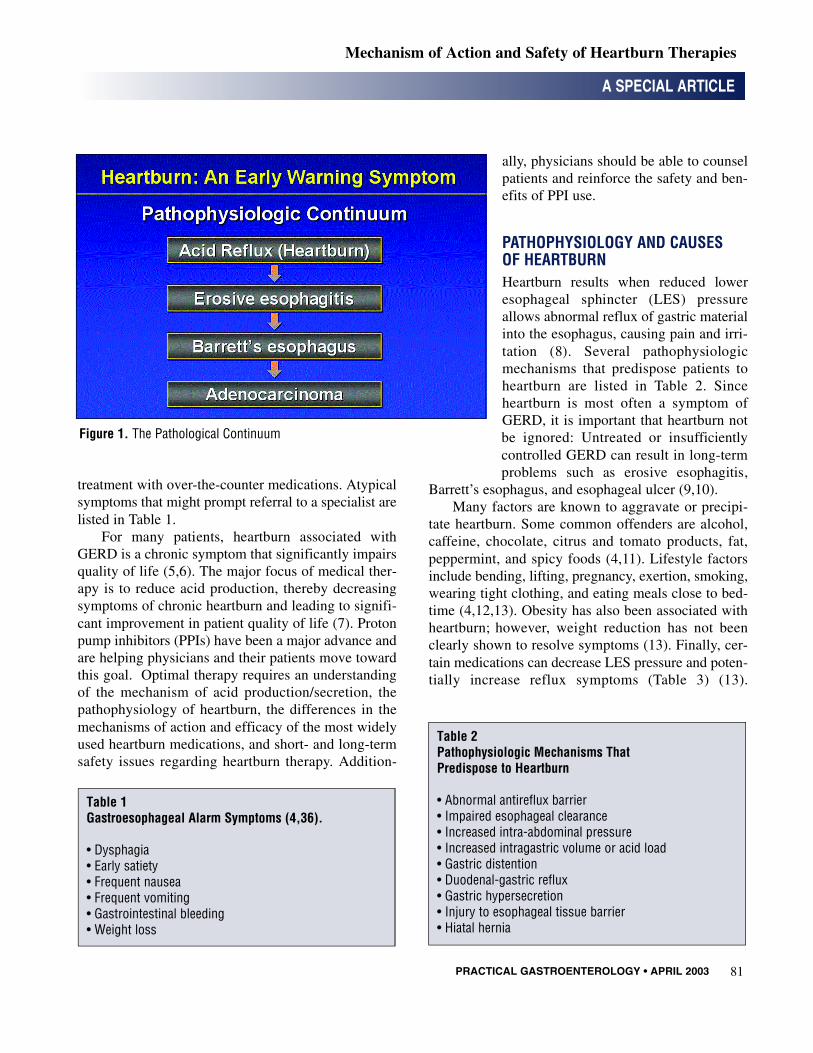
approximately 40% of the US population experiencingheartburn at least once per month and about 10% hav-ing it daily (2–4). Frequent heartburn is an early-warn-ing symptom in the pathological continuum of GERDand is a risk factor for esophageal adenocarcinoma(Figure 1). Endoscopic evaluation in some studies,however, has indicated that only about one half ofpatients with frequent heartburn have erosiveesophagitis, and less than 15% of patients with nonero-sive esophagitis experience worsening of their symp-toms over 6 months (4). Patients with heartburn, butwithout alarm symptoms, may be candidates for self-
Mechanism of Action and Safety of Heartburn Therapies
A SPECIAL ARTICLE
Philip O. Katz, M.D., Kimbel Professor and Chairman,Department of Medicine, Chief, Division of Gastroen-terology, Graduate Hospital, Philadelphia, PA. GeorgeSachs, M.D., University of California—Los Angeles,Los Angeles, CA.
Philip O. Katz
Heartburn is a frequent problem for adults in the United States and is the most com-mon symptom of gastroesophageal reflux disease. This often troublesome symptom,when frequent and severe enough, has a major impact on quality of life. The primarygoal, successful management of heartburn, is achievable for most patients. The choiceof therapy is based on understanding 1) the mechanism of acid secretion/production,2) the pathophysiology of heartburn, 3) the mechanisms of action of antisecretorytherapies, and 4) the safety profiles of available agents. This review focuses on the epi-demiology and pathophysiology of heartburn as well as on treatment options. Thisinformation can help care providers increase their patients’ awareness of the benefitsand limitations of the various available therapies so that patients can successfullymanage their heartburn.
George Sachs
PRACTICAL GASTROENTEROLOGY • APRIL 2003 81
A SPECIAL ARTICLE
Mechanism of Action and Safety of Heartburn Therapies
treatment with over-the-counter medications. Atypicalsymptoms that might prompt referral to a specialist arelisted in Table 1.
For many patients, heartburn associated withGERD is a chronic symptom that significantly impairsquality of life (5,6). The major focus of medical ther-apy is to reduce acid production, thereby decreasingsymptoms of chronic heartburn and leading to signifi-cant improvement in patient quality of life (7). Protonpump inhibitors (PPIs) have been a major advance andare helping physicians and their patients move towardthis goal. Optimal therapy requires an understandingof the mechanism of acid production/secretion, thepathophysiology of heartburn, the differences in themechanisms of action and efficacy of the most widelyused heartburn medications, and short- and long-termsafety issues regarding heartburn therapy. Addition-
ally, physicians should be able to counselpatients and reinforce the safety and ben-efits of PPI use.
PATHOPHYSIOLOGY AND CAUSES OF HEARTBURNHeartburn results when reduced loweresophageal sphincter (LES) pressureallows abnormal reflux of gastric materialinto the esophagus, causing pain and irri-tation (8). Several pathophysiologicmechanisms that predispose patients toheartburn are listed in Table 2. Sinceheartburn is most often a symptom ofGERD, it is important that heartburn notbe ignored: Untreated or insufficientlycontrolled GERD can result in long-termproblems such as erosive esophagitis,
Barrett’s esophagus, and esophageal ulcer (9,10).Many factors are known to aggravate or precipi-
tate heartburn. Some common offenders are alcohol,caffeine, chocolate, citrus and tomato products, fat,peppermint, and spicy foods (4,11). Lifestyle factorsinclude bending, lifting, pregnancy, exertion, smoking,wearing tight clothing, and eating meals close to bed-time (4,12,13). Obesity has also been associated withheartburn; however, weight reduction has not beenclearly shown to resolve symptoms (13). Finally, cer-tain medications can decrease LES pressure and poten-tially increase reflux symptoms (Table 3) (13).
Table 1Gastroesophageal Alarm Symptoms (4,36).
• Dysphagia• Early satiety• Frequent nausea• Frequent vomiting• Gastrointestinal bleeding• Weight loss
Figure 1. The Pathological Continuum
Table 2Pathophysiologic Mechanisms That Predispose to Heartburn
• Abnormal antireflux barrier• Impaired esophageal clearance• Increased intra-abdominal pressure• Increased intragastric volume or acid load• Gastric distention• Duodenal-gastric reflux• Gastric hypersecretion• Injury to esophageal tissue barrier• Hiatal hernia

PRACTICAL GASTROENTEROLOGY • APRIL 200382
A SPECIAL ARTICLE
Mechanism of Action and Safety of Heartburn Therapies
Although absence of the above factors may reduce theoccurrence of heartburn, many patients find it difficultor impossible to avoid these triggers consistently.
MECHANISM OF ACID PRODUCTION AND SECRETIONThe parietal cell, located in the gastric gland of thestomach, produces and secretes gastric acid (14). Theresting parietal cell is characterized by the presence oflarge amounts of smooth surface membranes calledtubulovesicles, as well as a small infolding of the api-cal membrane known as the secretorycanaliculus, which is continuous with thelumen of the stomach (14). Within thetubulovesicular membrane, hydrogenion/potassium ion-adenosine triphosphatase(H+/K+ ATPase), or proton pump, whenactivated, transports hydrogen (H+) out ofthe parietal cell (14).
Stimulation of the parietal cell initiatesthe fusion of tubulovesicles with the secre-tory canaliculus, increasing its surface areaand volume (14). Concurrently, the protonpump translocates from the cytoplasmictubulovesicular membrane to the canalicu-lar membrane (14). H+, adenosine triphos-phate (ATP), and magnesium (Mg+) subse-quently bind to the proton pump (14).Transfer of the terminal phosphate of ATPto the proton pump produces a conforma-tional change in the enzyme that reduces the
affinity for H+ and increases the relative affinity forK+ (14). Consequently, an H+/K+ exchange occurs asH+ is released into the lumen and K+ in the gastricjuice becomes bound to the proton pump (14).Dephosphorylation of the proton pump returns theenzyme to its original conformation state, which leadsto the release of K+ into the cytoplasm (Figure 2) (14).
Certain mediators stimulate acid secretion byinteracting with one another and by binding to theirrespective receptors in the parietal cell to form intra-cellular messengers. The release of acetylcholine, theactivation of histamine-2 (H2) receptors, and the secre-tion of gastrin all stimulate H+ ion generation and pro-duction of gastric acid (15).
TREATMENT OF HEARTBURN Antacids, H2 receptor antagonists (H2RAs), and PPIsare among the pharmacologic options for treatingheartburn. Each of these therapeutic classes has a dis-tinct mechanism of action. Most antacids are availablewithout a prescription. Despite the many brands on themarket, antacids are all based on 4 active ingredients invarious strengths and combinations: magnesium
Table 3Medications That May Aggravate Heartburn
• Alpha-adrenergic blockers• Anticholinergics• Beta-adrenergic agonists• Calcium channel blockers• Diazepam, alprazolam• Narcotics• Progesterone• Theophylline
From Katzka D. Practical Gastroenterology, 2000:14–31.
Figure 2. Mechanism of Acid Secretion.
(continued on page 84)

PRACTICAL GASTROENTEROLOGY • APRIL 200384
A SPECIAL ARTICLE
Mechanism of Action and Safety of Heartburn Therapies
hydroxide, calcium carbonate, aluminum hydroxide,and sodium bicarbonate (11). Antacids neutralize gas-tric acid, which increases intragastric pH, leading tosubstantial inhibition of the formation of pepsin andacid-pepsin complex (13). They also cause a transientincrease in LES pressure. Antacids, which are taken asneeded, provide fast symptomatic relief to approxi-mately 50% of patients with mild heartburn (16,17).Although there is rapid onset of relief with antacids,heartburn may return in as little as 30 to 60 minutes,resulting in the need for frequent dosing.
H2RAs such as cimetidine, famotidine, nizatidine,and ranitidine suppress acid secretion by blocking his-tamine from binding to the H2 receptor on the parietalcell (18). H2RAs only partially inhibit acid secretionelicited by gastrin (which stimulates secretion of hist-amine by enterochromaffinlike cells) and are thereforemore effective at reducing basal acid secretion than atreducing food-stimulated acid secretion (11 , 1 5 ) .H2RAs reduce H+ concentration, gastric juice volume,and pepsin production, but they have no effect on LESpressure, gastric emptying, or pancreatic secretion(18). H2RAs provide relief to approximately 60% ofpatients (19). Symptomatic relief usually occurs within30 to 60 minutes and lasts up to 10 hours (19). Somepatients, however, may develop tolerance to H2RAswith continued use (20).
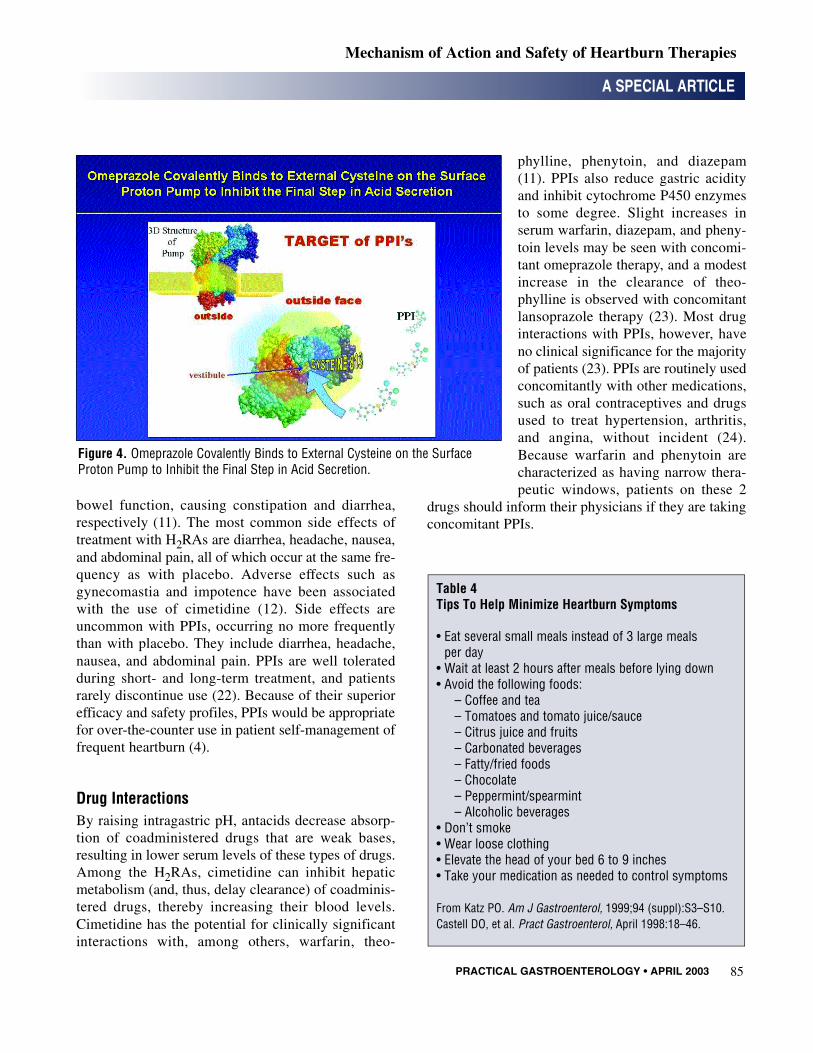
The PPIs include omeprazole, lanso-prazole, pantoprazole, esomeprazole, andrabeprazole. The mechanism of action ofthese weak base prodrugs involves 3stages: (1) PPIs selectively accumulate inthe acidic secretory canaliculus of theactive parietal cell (Figure 3) (2). At thatsite or on the surface of the ATPase in thecell membrane, they undergo H+-catalyzedconversion to an active form (3). Uponactivation, PPIs covalently bind to anexternal cysteine in the transport region ofthe proton pump. This inhibits acid secre-tion, no matter what the stimulus (Figure4) (15). PPIs accumulate, are activated,and work where needed, directly inhibitingthe acid-producing proton pump regardlessof whether acid secretion was stimulatedby food, medication, or other factors. This
unique trait of selective accumulation and action hasprompted some clinicians, including Dr. Georg eSachs, one of the authors of this article, to apply theterm “smart drugs” to PPIs.
PPIs provide symptomatic relief to up to 90% ofpatients with frequent heartburn; this is superior to theefficacy of antacids or H2RAs (15). PPIs are usuallytaken once daily, less frequently than other heartburntherapies (21). Many patients achieve symptomaticrelief after the first dose, but optimal response to PPIsoccurs after 2 to 3 days of treatment (15). Patients fre-quently remain symptom free with PPI therapy for upto 24 hours (15).
SAFETY OF ACID-REDUCING THERAPIES
Adverse EffectsSince heartburn can be a chronic problem necessitatinglong-term therapy, safety is a major concern in thechoice of treatment. There are several potential sideeffects associated with the use of antacids: 1) Sodiumbicarbonate can alter systemic pH. 2) Calcium carbon-ate can stimulate acid production through release ofgastrin and can also cause hypercalcemia. 3) Alu-minum hydroxide and magnesium hydroxide can alter
Figure 3. Accumulation of Omeprazole in the Secretory Canaliculus of theParietal Cell.
(continued from page 82)
PRACTICAL GASTROENTEROLOGY • APRIL 2003 85
A SPECIAL ARTICLE
Mechanism of Action and Safety of Heartburn Therapies
bowel function, causing constipation and diarrhea,respectively (11). The most common side effects oftreatment with H2RAs are diarrhea, headache, nausea,and abdominal pain, all of which occur at the same fre-quency as with placebo. Adverse effects such asgynecomastia and impotence have been associatedwith the use of cimetidine (12). Side effects areuncommon with PPIs, occurring no more frequentlythan with placebo. They include diarrhea, headache,nausea, and abdominal pain. PPIs are well toleratedduring short- and long-term treatment, and patientsrarely discontinue use (22). Because of their superiorefficacy and safety profiles, PPIs would be appropriatefor over-the-counter use in patient self-management offrequent heartburn (4).
Drug InteractionsBy raising intragastric pH, antacids decrease absorp-tion of coadministered drugs that are weak bases,resulting in lower serum levels of these types of drugs.Among the H2RAs, cimetidine can inhibit hepaticmetabolism (and, thus, delay clearance) of coadminis-tered drugs, thereby increasing their blood levels.Cimetidine has the potential for clinically significantinteractions with, among others, warfarin, theo-
phylline, phenytoin, and diazepam(11). PPIs also reduce gastric acidityand inhibit cytochrome P450 enzymesto some degree. Slight increases inserum warfarin, diazepam, and pheny-toin levels may be seen with concomi-tant omeprazole therapy, and a modestincrease in the clearance of theo-phylline is observed with concomitantlansoprazole therapy (23). Most druginteractions with PPIs, however, haveno clinical significance for the majorityof patients (23). PPIs are routinely usedconcomitantly with other medications,such as oral contraceptives and drugsused to treat hypertension, arthritis,and angina, without incident (24).Because warfarin and phenytoin arecharacterized as having narrow thera-peutic windows, patients on these 2
drugs should inform their physicians if they are takingconcomitant PPIs.
Figure 4. Omeprazole Covalently Binds to External Cysteine on the Surface Proton Pump to Inhibit the Final Step in Acid Secretion.
Table 4Tips To Help Minimize Heartburn Symptoms
• Eat several small meals instead of 3 large meals per day
• Wait at least 2 hours after meals before lying down• Avoid the following foods:
– Coffee and tea– Tomatoes and tomato juice/sauce– Citrus juice and fruits– Carbonated beverages– Fatty/fried foods– Chocolate– Peppermint/spearmint– Alcoholic beverages
• Don’t smoke• Wear loose clothing• Elevate the head of your bed 6 to 9 inches• Take your medication as needed to control symptoms
From Katz PO. Am J Gastroenterol, 1999;94 (suppl):S3–S10.Castell DO, et al. Pract Gastroenterol, April 1998:18–46.

PRACTICAL GASTROENTEROLOGY • APRIL 200386
LONG-TERM SAFETY OF PPIsInitial concerns about long-term use of PPIs includedatrophic gastritis; intestinal metaplasia/gastric cancer;bacterial overgrowth; and malabsorption of fats, miner-als, and essential nutrients. Since the approval of the firstPPI in the United States in 1989, the long-term use ofPPIs has been documented as safe, with no conclusiveevidence that long-term PPI therapy contributes to thedevelopment of atrophic gastritis or intestinal metapla-sia/gastric cancer (25–27). As with H2RAs, the use ofPPIs has been associated with gastric and duodenal bac-terial overgrowth, but the clinical consequence of thishas not been established (28). Additionally, the malab-sorption of fats and minerals, such as iron, calcium,phosphorus, magnesium, and zinc, does not occur withPPI therapy (24,29,30). Decreased vitamin B1 2 l e v e l swith prolonged PPI therapy have been observed in rarecases (24).
COUNSELING PATIENTS AND REINFORCING THE BENEFITS OF ADHERENCE TO THERAPYIt is widely recognized that PPIs are effective, safe,and cost-effective for controlling heartburn (22,23,31).PPIs would be the appropriate first step in an approachto self-treatment for individuals with symptoms of fre-quent heartburn typical of uncomplicated GERD(31,32). The success of such a program would dependin large part on patients’ prompt and regular use ofmedication, adoption of appropriate lifestyle modifica-tions (Table 4), and understanding of when they shouldseek medical advice.
Studies indicate that patient education and coun-seling contribute a great deal to treatment adherenceand success (33,34). Indeed, patients in clinical trialsseem to do better than the general population ofpatients because they receive counseling and take theirmedications regularly. Patients who understand theirsymptoms and treatment tend to feel empowered andinvested in success (Table 5) (21,35).
Physicians should educate their patients about thebasic mechanism of frequent heartburn (21), the factthat acid-suppressing treatment is available, the rami-fications of not treating heartburn, and the importanceof making the lifestyle adjustments listed in Table 4. It
is important that patients be aware that they shouldconsult their physicians if they do not achieve reliefwithin the allotted treatment period for the medicationthey are using or if they notice alarm symptoms (suchas those listed in Table 1) or other unusual symptomsdue to extraesophageal manifestations of GERD(Table 6) (4,19,36).
A SPECIAL ARTICLE
Mechanism of Action and Safety of Heartburn Therapies
Table 5Adherence Strategies for Heartburn Treatment
• Establishing effective communication– Patients do not reliably interpret the word
“heartburn”– Describing their symptoms as “a burning feeling
rising from the stomach or lower chest up towardsthe neck” has been found to be more reliable thanthe word “heartburn”
– “Are symptoms helped by antacids?”• Provide explicit directions• Explain the importance of adherence• Supply written information combined with oral
counseling– Speak in patient/consumer language
• Clarify the purpose of the medication• Repeat important points• Give consistent advice• Understand their condition
– Why is acid produced– How is acid secreted– How is acid suppressed– How do PPIs work (for example, omeprazole’s
mechanisms of action: It knows where to go andwhat to do: therefore it is a “smart, specific drug”)
Table 6Extraesophageal Manifestations of GERD (4,36)
• Chronic hoarseness• Chronic cough• Chest pain, especially radiating• Frequent wheezing• Lightheadedness, dizziness• Shortness of breath• Chronic sore throat
(continued on page 88)

PRACTICAL GASTROENTEROLOGY • APRIL 200388
A SPECIAL ARTICLE
Mechanism of Action and Safety of Heartburn Therapies
CONCLUSIONFamiliarity with the mechanism of acid production/secretion and the pathophysiology of heartburn givesphysicians the means to understand the mechanism ofaction and clinical efficacy of each treatment option.Awareness of the differences between the various acid-reducing agents enables physicians to select the besttreatment for patients suffering from heartburn. PPIsprovide superior relief of frequent heartburn symptomsand have excellent safety profiles. Counseling and rein-forcing the benefits of this therapy can improve patientadherence and, consequently, lead to successful man-agement of heartburn. ■
References1. Carlsson R, Dent J, Bolling-Sternevald E, Jonsson R, Jungha O.
The usefulness of a structures questionnaire in the Assessment ofSymptomatic Gastroesophageal Reflux Disease. Scand J Gas -troenterol, 1998;33:1023-1029.
2. Nebel OT, Fornes MF, Castell DO. Symptomatic gastroe-sophageal reflux: incidence and precipitating factors. Am J DigDis, 1976;21:953-956.
3. Heartburn Across America. Princeton, NJ: Gallup Organization;1998.
4. Katz PO. Treatment of gastroesophageal reflux disease: use ofalgorithms to aid in management. Am J Gastroenterol, 1999;94:S3-S10.
5. Dimenäs E. Methodological aspects of evaluation of Quality ofLife in upper gastrointestinal diseases. Scand J GastroenterolSuppl, 1993;199:18-21.
6. Enck P, Dubois D, Marquis P. Quality of life in patients withupper gastrointestinal symptoms: results from the Domestic/International Gastroenterology Surveillance Study (DIGEST).Scand J Gastroenterol Suppl, 1999;231:48-54.
7. Revicki DA, Crawley JA, Zodet MW, Levine DS, Joelsson BO.Complete resolution of heartburn symptoms and health-relatedquality of life in patients with gastro-oesophageal reflux disease.Aliment Pharmacol Ther, 1999;13:1621-1630.
8. Handbook of Pathophysiology. Springhouse, PA: SpringhouseCorp; 2001.
9. Bytzer P. On-demand therapy for gastro-oesophageal reflux dis-ease. Eur J Gastroenterol Hepatol, 2001;13 (suppl 1):S19-S22.
10. Richter JE, Peura D, Benjamin SB, Joelsson B, Whipple J. Effi-cacy of omeprazole for the treatment of symptomatic acid refluxdisease without esophagitis. Arch Intern Med, 2000;160:1810-1816.
11. Scott M, Gelhot AR. Gastroesophageal reflux disease: diagnosisand management. Am Fam Physician, 1999;59:1161-1169, 1199.
12. Szarka LA, Locke GR. Practical pointers for grappling withGERD. Heartburn gnaws at quality of life for many patients.Postgrad Med, 1999;105:88-90, 95-88, 103-106.
13. Katzka D. Treatment of Gerd: Lifestyle Modifications. PracticalGastroenterology, 2000:14-31.
14. Modlin I, Sachs, G. Acid Related Diseases Biology and Treat -ment: Schnetztor-Verlag GmbH D-Konstanz; 1998.
15. Wolfe MM, Sachs G. Acid suppression: optimizing therapy forgastroduodenal ulcer healing, gastroesophageal reflux disease,and stress-related erosive syndrome. Gastroenterology, 2000;118:S9-S31.
16. Faaij RA, Van Gerven JM, Jolivet-Landreau I, Masclee AA, Ven-drig EM, Schoemaker RC, et al. Onset of action during on-demand treatment with maalox suspension or low-dose ranitidinefor heartburn. Aliment Pharmacol Ther, 1999;13:1605-1610.
17. Lanza FL, Smith V, Page-Castell JA, Castell DO Effectiveness offoaming antacid in relieving induced heartburn. South Med J,1986;79:327-330.
18. Klinkenberg-Knol EC, Festen HP, Meuwissen SG. Pharmacolog-ical management of gastro-oesophageal reflux disease. Drugs,1995;49:695-710.
19. DeVault KR, Castell DO. Updated guidelines for the diagnosisand treatment of gastroesophageal reflux disease. The PracticeParameters Committee of the American College of Gastroen-terology. Am J Gastroenterol, 1999;94:1434-1442.
20. Tolman KG, Chandramouli J, Fang JC. Proton pump inhibitors inthe treatment of gastro-oesophageal reflux disease. Expert OpinPharmacother, 2000;1:1171-1194.
21. Castell D, Brunton S, Earnest D, al. e. GERD: Management algo-rithms for the primary care physician and the specialist. PracticalGastroenterology, 1998:18-46.
22. Wilde M, McTavish,D. Omeprazole: an update of its pharmacol-ogy and therapeutic use in acid-related disorders. Drugs, 1994;48:91-132.
23. Welage L, Berardi, RR. Evaluation of omeprazole, lansoprazole,pantoprazole, and raberpazole in the treatment of acid-related dis-eases. J Am Pharm Assoc, 2000;40:52-62.
24. Reilly JP. Safety profile of the proton-pump inhibitors. Am JHealth Syst Pharm, 1999;56:S11-S17.
25. Rubin C. Are there three types of Helicobacter pylori gastristis?Gastroenterology, 1997;112:2108-2110.
26. Pohle T, Domschke W. Results of short-and long-term medicaltreatment of gastroesophageal reflux disease (GERD). Langen-becks Arch Surg, 2000;385:317-323.
27. Lamberts R, Brunner G, Solcia E. Effects of very long (up to 10years) proton pump blockade on human gastric mucosa. Diges -tion, 2001;64:205-213.
28. Thorens J, Froehlich F, Schwizer W, Saraga E, Bille J, Gyr K, etal. Bacterial overgrowth during treatment with omeprazole com-pared with cimetidine: a prospective randomised double blindstudy. Gut, 1996;39:54-59.
29. Saltzman JR, Kowdley KV, Pedrosa MC, Sepe T, Golner B, Per-rone G, et al. Bacterial overgrowth without clinical malabsorptionin elderly hypochlorhydric subjects. Gastroenterology, 1994;106:615-623.
30. Serfaty-Lacrosniere C, Wood RJ, Voytko D, et al. Hypochlorhy-dria from short-term omeprazole treatment does not inhibitintestinal absorption of calcium, phosphorus, magnesium or zincfrom food in humans. J Am Coll Nutr, 1995;14:364-368.
31. Galmiche JP. How do we offer clinical relief to patients with gas-tro-oesophageal reflux disease? Eur J Gastroenterol Hepatol,2000;12(suppl 1):S3-S6.
32. Bardhan KD, Muller-Lissner S, Bigard MA, et al. Symptomaticgastro-oesophageal reflux disease: double blind controlled studyof intermittent treatment with omeprazole or ranitidine. TheEuropean Study Group. Brit Med J, 1999;318:502-507.
33. Lee M, Kemp JA, Canning A, Egan C, Tataronis G, Farraye FA.A randomized controlled trial of an enhanced patient complianceprogram for Helicobacter pylori therapy. Arch Intern Med,1999;159:2312-2316.
34. van Hees PAM, van Tongeren JHM. Compliance to therapy inpatients on a maintenance dose of sulfasalazine. J Clin Gastroen -terol, 1982;4:333-336.
35. Hungin AP, Rubin G, O’Flanagan H. Factors influencing compli-ance in long-term proton pump inhibitor therapy in general prac-tice. Br J Gen Pract, 1999;49:463-464.
36. Al-Sabbagh G, Wo JM. Supraesophageal manifestations of gas-troesophageal reflux disease. Semin Gastrointest Dis, 1999;10:113-119.
(continued from page 86)