mechanism hormone disease (lec 3)
DESCRIPTION
endokrinTRANSCRIPT

1
Mechanisms of endocrine disease
• Endocrine disorders result from hormone deficiency, hormone excess or hormone resistance
• Almost without exception, hormone deficiency causes disease – One notable exception is calcitonin deficiency

2
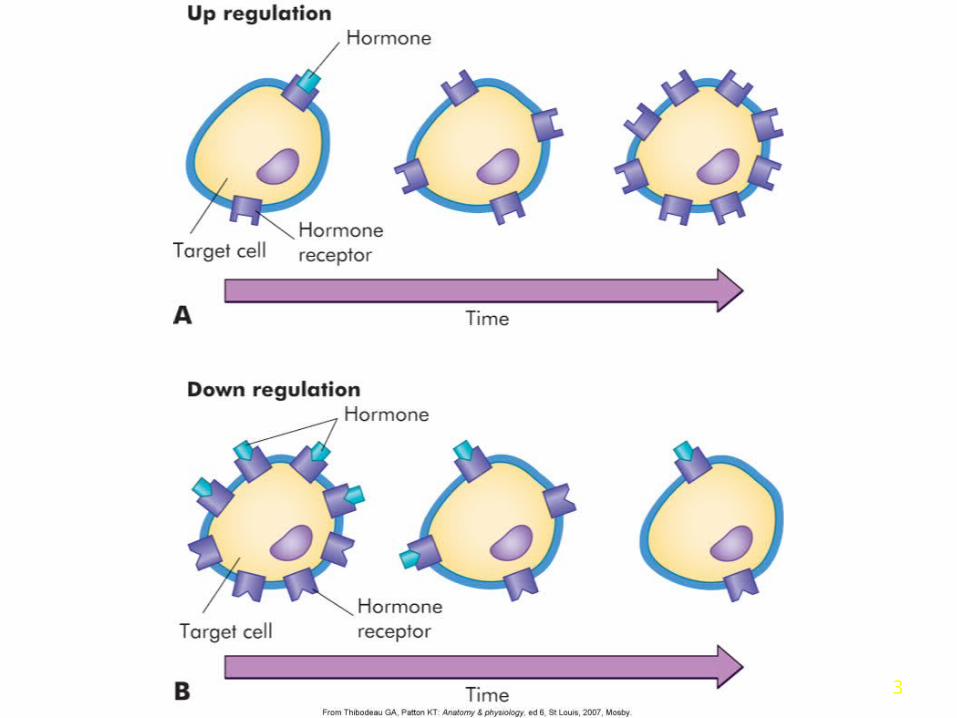
Cellular Mechanisms of Hormone Action
• Target cell – recognize, bind and initiate
• Up – regulation
• Down – regulation
• Hormone effects– Direct – stimulation– Permissive – facilitates maximum
response/function
3
4
Mechanisms of endocrine disease
• Deficiency usually is due to destructive process occurring at gland in which hormone is produced—infection, infarction, physical compression by tumor growth, autoimmune attack
Type I Diabetes

5
Mechanisms of endocrine disease
• Deficiency can also arise from genetic defects in hormone production—gene deletion or mutation, failure to cleave precursor, specific enzymatic defect (steroid or thyroid hormones)
Congenital Adrenal Hyperplasia

6
Mechanisms of endocrine disease• Inactivating mutations of receptors can
cause hormone deficiency
Testicular Feminization Syndrome
7
Mechanisms of endocrine disease
• Hormone excess usually results in disease
• Hormone may be overproduced by gland that normally secretes it, or by a tissue that is not an endocrine organ.
• Endocrine gland tumors produce hormone in an unregulated manner.
Cushing’s Syndrome

8
Mechanisms of endocrine disease• Exogenous ingestion
of hormone is the cause of hormone excess—for example, glucocorticoid excess or anabolic steroid abuse

9
Mechanisms of endocrine disease
• Activating mutations of cell surface receptors cause aberrant stimulation of hormone production by endocrine gland.– McCune-Albright syndrome usually
caused by a mutation in a gene called GNAS1 (Guanine Nucleotide binding protein, Alpha Stimulating activity polypeptide 1).

10
Mechanisms of endocrine disease
• Malignant transformation of non-endocrine tissue causes dedifferentiation and ectopic production of hormones
• Anti-receptor antibodies stimulate receptor instead of block it, as in the case of the common form of hyperthyrodism.
Grave’s Disease
11
Mechanisms of endocrine disease
• Alterations in receptor number and function result in endocrine disorders
• Most commonly, an aberrant increase in the level of a specific hormone will cause a decrease in available receptors
Type II diabetes

12
Adrenal Gland
Adrenal glands are located on the top of both kidneys.
Each gland consists of a medulla, the center of the gland, encased by a cortex.

13
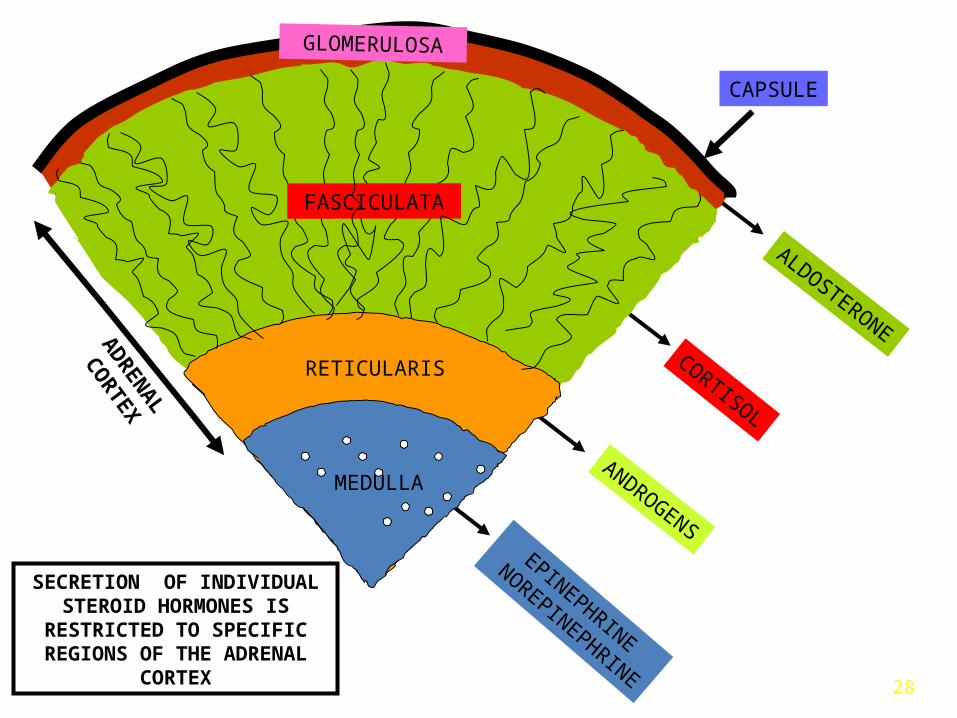
Adrenal Glands• Adrenal cortex
– 80% of an adrenal gland’s total weight– Zona glomerulosa – aldosterone 15%– Zona fasciculata – glucocorticoids 78%– Zona reticularis – androgens and estrogens
(others) – 7%
• Adrenal medulla
– Innervation by SNS

14
Adrenal Glands

15
-Inner part “medulla”: -Chromaffin cells-Source of catecholamines (Epi/NEpi),-Innervated by pre-ganglionic sympathetic fibers; forms an
extension of the sympathetic nervous system (fight/flight).
-Outer part “cortex”: -Source of steroid hormones
-Glucocorticoids, mineralocorticoids and sex steroids
Anatomy/Physiology of Adrenal Gland
16
DHBR
NADP+
NADPHfrom phe, diet, or protein breakdown
Tyrosine L-Dopa
H2OO2
Tyrosine hydroxylase(rate-determining step)
BH2BH4
1
Dopadecarboxylase
CO2
Dopamine
pyridoxalphosphate
2
Dopamine hydroxylase
ascorbateH2O
Norepinephrine
O23
NMT
SAM SAH
Epinephrine
4
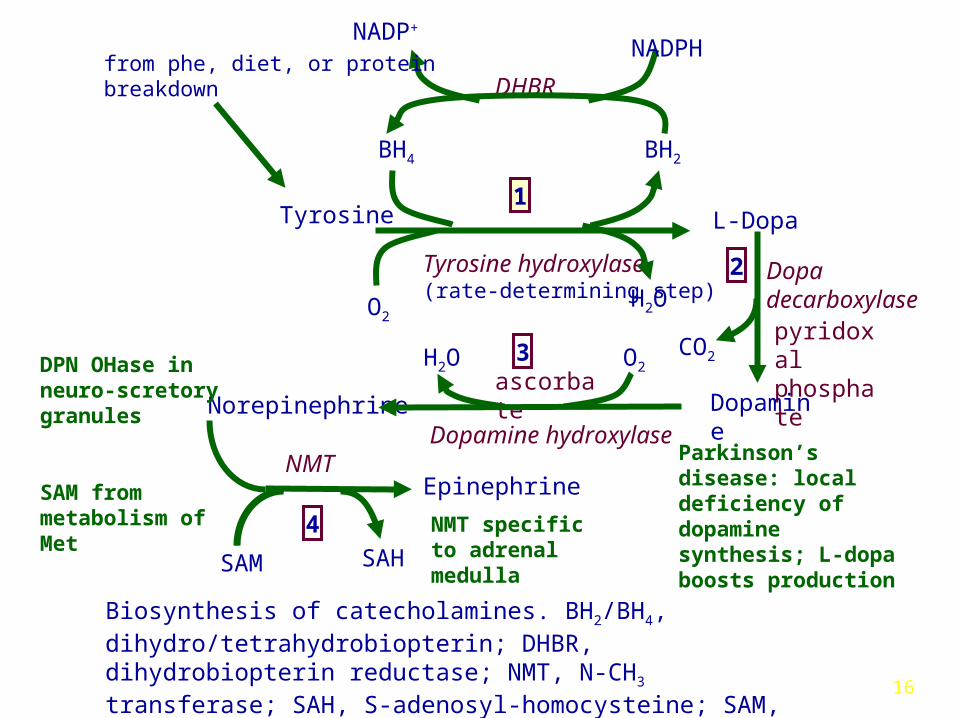
Biosynthesis of catecholamines. BH2/BH4, dihydro/tetrahydrobiopterin; DHBR, dihydrobiopterin reductase; NMT, N-CH3 transferase; SAH, S-adenosyl-homocysteine; SAM, S-adenosylmethionine
Parkinson’s disease: local deficiency of dopamine synthesis; L-dopa boosts productionNMT specific to
adrenal medulla
SAM from metabolism of Met
DPN OHase in neuro-scretory granules

17
........
acetylcholine
Adrenal MedullaChromaffin Cell
Neuron
Acuteregulation
Tyrosine
L-Dopa DPN
DPN NE
granuleinduction
Chronicregulation
Stress
Hypothalamus
ACTH
Cortisolfrom adrenal cortex via intra-adrenal portal system
EpinephrinePNMT
NE
neuro-secretorygranules
E E ENE E
Regulation of the release of catecholamines and synthesis of epinephrine in the adrenal medulla chromaffin cell.
promotesexocytosis
................
EEEENE
E
E E
NE
E
Ca2+
18
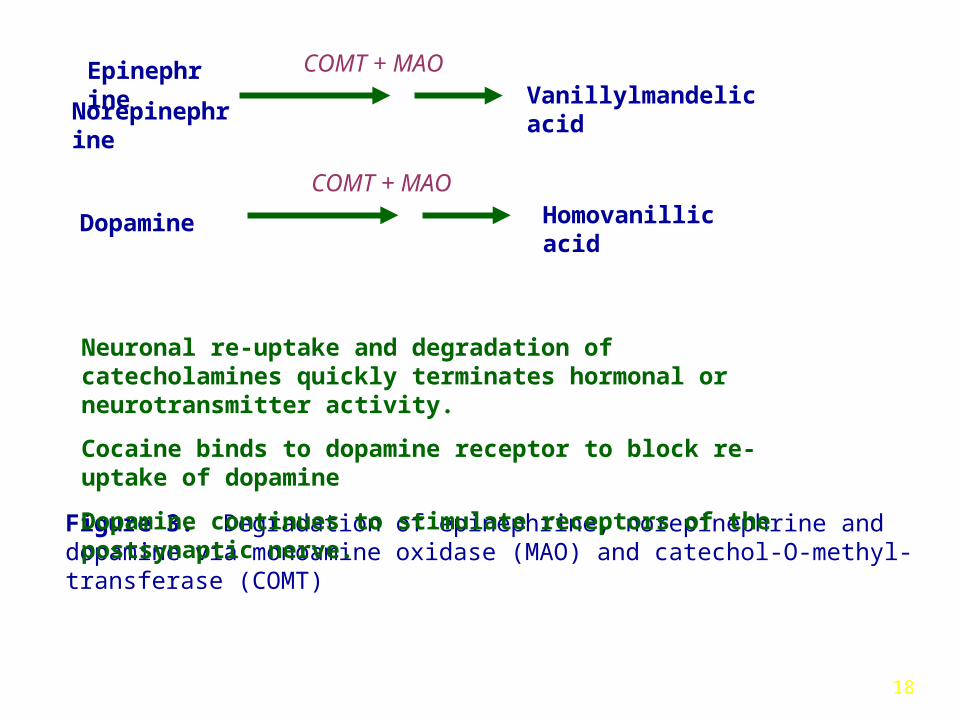
Norepinephrine
Epinephrine COMT + MAOVanillylmandelic acid
Figure 3. Degradation of epinephrine, norepinephrine and dopamine via monoamine oxidase (MAO) and catechol‑O‑methyl-transferase (COMT)
Neuronal re-uptake and degradation of catecholamines quickly terminates hormonal or neurotransmitter activity.
Cocaine binds to dopamine receptor to block re-uptake of dopamine
Dopamine continues to stimulate receptors of the postsynaptic nerve.
Dopamine Homovanillic acidCOMT + MAO

19
Classification of Adrenergic Hormone Receptors
Receptor AgonistsSecond
MessengerG protein
alpha1 (1) E>NE IP3/Ca2+; DAG Gq
alpha2 (2) NE>E cyclic AMP Gi
beta1 (1) E=NE cyclic AMP Gs
beta2 (2) E>>NE cyclic AMP Gs
E = epinephrine; NE = norepinephrine
Synthetic agonists:isoproterenol binds to beta receptorsphenylephrine binds to alpha receptors (nose spray action)
Synthetic antagonists: propranolol binds to beta receptors phentolamine binds to alpha receptors
20
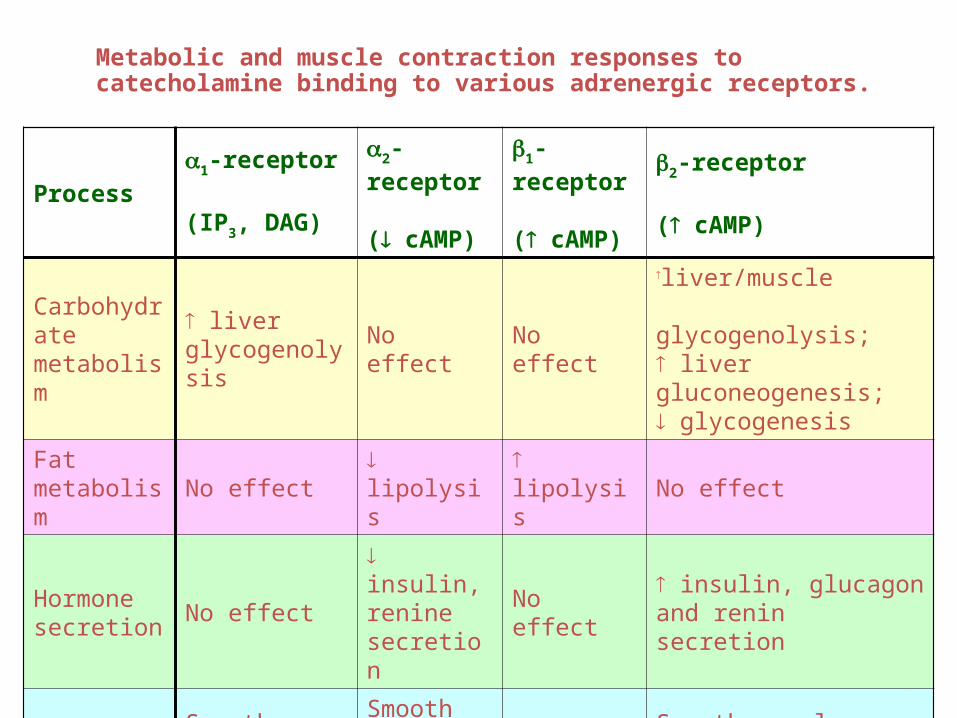
Metabolic and muscle contraction responses to catecholamine binding to various adrenergic receptors.
Process
1-receptor
(IP3, DAG)
2-receptor
( cAMP)
1-receptor
( cAMP)
2-receptor
( cAMP)
Carbohydratemetabolism
liver glycogenolysis
No effect No effect
liver/muscle glycogenolysis; liver gluconeogenesis; glycogenesis
Fatmetabolism
No effect lipolysis lipolysis No effect
Hormonesecretion
No effect insulin, renine secretion
No effect insulin, glucagon and renin secretion
Muscle contraction
Smooth muscle - blood vessels, genitourinary tract contraction
Smooth muscle - some vascular;GI tract relaxation
Myocardial - rate, force
Smooth muscle relaxation - bronchi, blood vessels, GI tract, genitourinary tract

21
1 or 2
receptor
ATP cyclic AMP
Gs
s
GTP
inactiveadenylylcyclase
GTP
ACTIVEadenylylcyclase
inactiveadenylylcyclase
2 receptor
Mechanisms of 1, 2, and 2 agonist effects on adenylyl cyclase activity
Gi
i
GTPs
GTP
i
X
22
"FIGHT OR FLIGHT" RESPONSE
epinephrine/ norepinephrine major elements in the "fight or flight" response
acute, integrated adjustment of many complex processes in organs vital to the response (e.g., brain, muscles, cardiopulmonary system, liver)
occurs at the expense of other organs less immediately involved (e.g., skin, GI).
epinephrine: rapidly mobilizes fatty acids as the primary fuel for muscle action increases muscle glycogenolysismobilizes glucose for the brain by hepatic glycogenolysis/
gluconeogenesis• preserves glucose for CNS by insulin release leading to reduced glucose
uptake by muscle/ adipose • increases cardiac output
norepinephrine elicits responses of the CV system - blood flow and insulin secretion.

23
ADRENAL “CORTEX”-DERIVED STEROIDS

24

25
Adrenal Cortex
“all hormones derived from cholesterol”• Stimulated by adrenocorticotropic hormone (ACTH)• Glucocorticoid hormones
– Direct effect on carbohydrate metabolism– Anti-inflammatory and growth suppression effects– Influences awareness and sleep habits– Inhibits bone matrix-protein matrix– Cortisol – most potent naturally occurring

26
Adrenal Cortex
• Mineralocorticoid hormones – Aldosterone– ↑ Na+ uptake in epithelial cells – distal
nephrons– ↑ Na retention with loss of K+ and H+
– Regulation by the renin-angiotensin system
• Na+ and H2O depletion
• ↑ K+ excreteion
• ↓ blood volume
27
Adrenal “Cortex”-derived Steroids
Class Major Effects
Glucocorticoids Cortisol Glucose metabolism control
Mineralocorticoids Aldosterone Na/K/H20 control
Sex steroids DHEA Androgen precursorsAndrostendione
28
SECRETION OF INDIVIDUAL STEROID HORMONES IS
RESTRICTED TO SPECIFIC REGIONS OF THE ADRENAL
CORTEX
MEDULLA
RETICULARISCORTISOL
ANDROGENS
CAPSULE
EPINEPHRINE
NOREPINEPHRINE
ALDOSTERONEAD
REN
AL
CO
RTEX
MEDULLARETICULARIS
MEDULLA
GLOMERULOSA
FASCICULATA

29
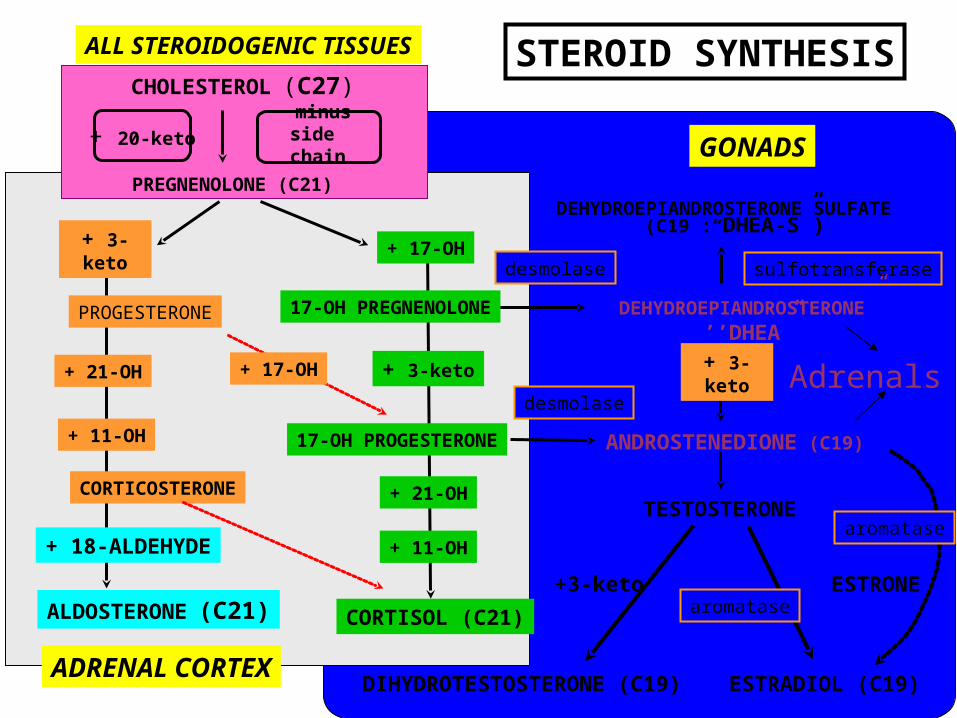
SYNTHESIS OF ADRENAL CORTEX HORMONES

30
Hypothalamus
Anterior pituitary
Adrenal cortex
Corticotropin-releasing factor (CRF)
Adrenocorticotropic hormone (ACTH)
Glucocorticoids(especially cortisol)
HypoxiaHypoglycemiaHyperthermia
ExerciseCortisol insufficiency
Stress
Diurnal rhythms
( - )
SomatostatinHypothalamic
lesions
( - )
(+)
(+)(+)
31
minus side chain
ALL STEROIDOGENIC TISSUES
CHOLESTEROL (C27)
+ 3-keto
+ 11-OH
PROGESTERONE
+3-keto
+ 21-OH
+ 3-keto
+ 11-OH
+ 21-OH
+ 17-OH
CORTISOL (C21)
CORTICOSTERONE
ALDOSTERONE (C21)
+ 20-keto
+ 17-OH
PREGNENOLONE (C21)
ANDROSTENEDIONE (C19)
+ 18-ALDEHYDE
TESTOSTERONE
ESTRADIOL (C19)
GONADS
ADRENAL CORTEX
ESTRONE
STEROID SYNTHESIS
DEHYDROEPIANDROSTERONE” ’’DHEA”
17-OH PROGESTERONE
DEHYDROEPIANDROSTERONE SULFATE (C19 :“DHEA-S”)
+ 3-keto
aromatase
17-OH PREGNENOLONE
DIHYDROTESTOSTERONE (C19)
sulfotransferasedesmolase
desmolase
aromatase
Adrenals
32
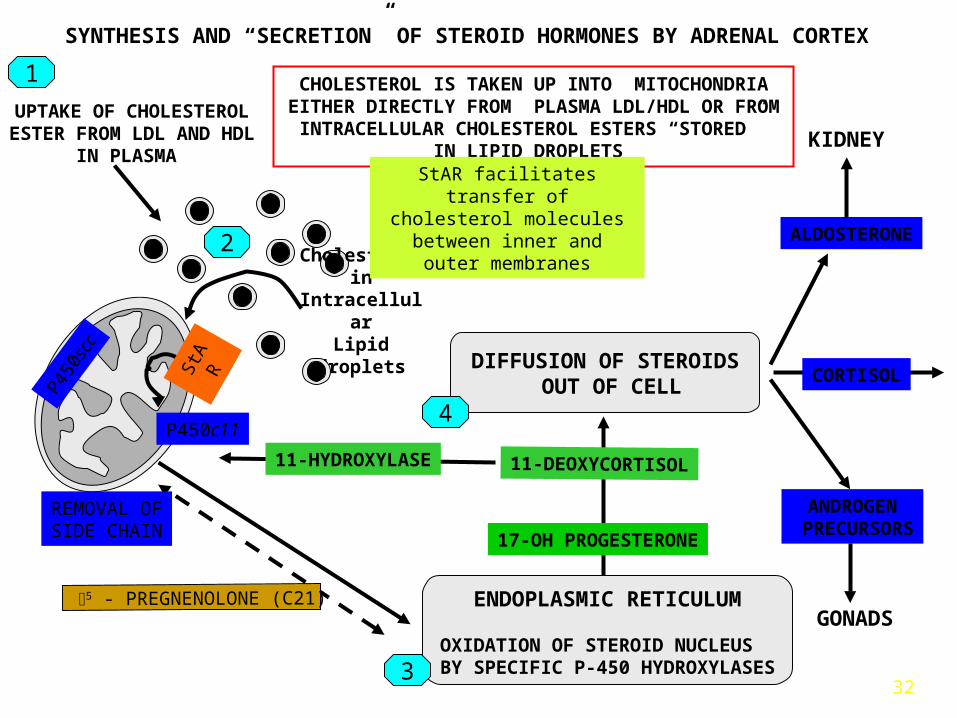
ENDOPLASMIC RETICULUM
OXIDATION OF STEROID NUCLEUS BY SPECIFIC P-450 HYDROXYLASES
5 - PREGNENOLONE (C21)
ALDOSTERONE
ANDROGEN PRECURSORS
11-DEOXYCORTISOL
SYNTHESIS AND “SECRETION” OF STEROID HORMONES BY ADRENAL CORTEX
GONADS
Cholesterol in
IntracellularLipid droplets
2
1
3
KIDNEY
DIFFUSION OF STEROIDS OUT OF CELL
CORTISOL
CHOLESTEROL IS TAKEN UP INTO MITOCHONDRIA EITHER DIRECTLY FROM PLASMA LDL/HDL OR FROM INTRACELLULAR CHOLESTEROL ESTERS “STORED”
IN LIPID DROPLETS
UPTAKE OF CHOLESTEROLESTER FROM LDL AND HDL
IN PLASMA
P450
scc
StAR facilitates transfer ofcholesterol molecules between
inner and outer membranes
4
17-OH PROGESTERONE
REMOVAL OFSIDE CHAIN
StA
R
P450c11
11-HYDROXYLASE
33
The metabolic effects of glucocorticoids
They increase glucose production by:1. Increasing the supply of amino acids to the liver2. Activating the expression of genes of gluconeogenic enzyme
Promote lipolysis in peripheral tissues by inducing enzyme synthesis
(Increase mobilization of peripheral fat)
When at very high levels can cause lipogenesis in face and trunk
When at a very high levels has catabolic effect on proteins in peripheral tissues and anabolic effect in the liver
34
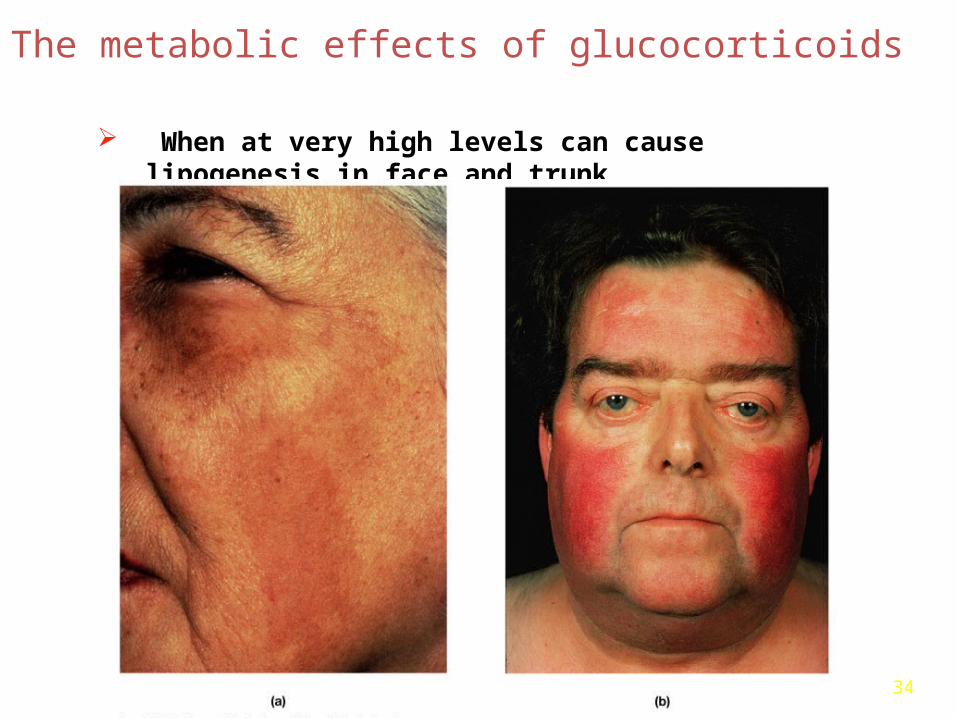
The metabolic effects of glucocorticoids
When at very high levels can cause lipogenesis in face and trunk

35
Cortisol (hydrocortisone) and synthetic glucocorticoids (prednisone): Potent anti-inflammatory and immunosuppressive agent [topical, oral, aerosolized, injection]
Therapeutic Effects of Glucocorticoids
-used to relieve symptoms of inflammation [swelling, heat, redness, and pain];
-used in cases of insufficient synthesis (hormone replacement);
-used to treat certain forms of arthritis; skin, blood, kidney, eye, thyroid, and intestinal disorders (e.g., colitis); severe allergies; and respiratory conditions such as asthma.
-used in the treatment of certain types of cancer.
36
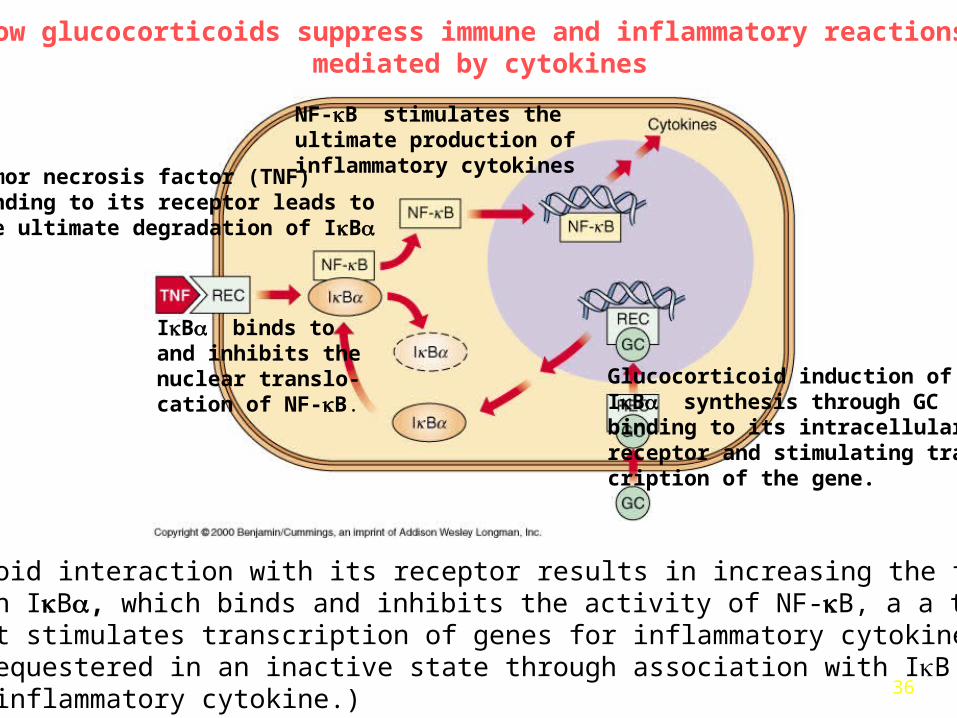
A glucocorticoid interaction with its receptor results in increasing the transcriptionof the protein IB, which binds and inhibits the activity of NF-B, a a transcriptionalactivator that stimulates transcription of genes for inflammatory cytokines. NF-Bis normally sequestered in an inactive state through association with IB proteins.(TNF is a proinflammatory cytokine.)
Glucocorticoid induction of IB synthesis through GCbinding to its intracellularreceptor and stimulating trans-cription of the gene.
IB binds toand inhibits thenuclear translo-cation of NF-B.
NF-B stimulates theultimate production ofinflammatory cytokinesTumor necrosis factor (TNF)
binding to its receptor leads tothe ultimate degradation of IB
How glucocorticoids suppress immune and inflammatory reactions mediated by cytokines

37
Adrenal Gland Steroids
Cortisol (the naturally-occurring glucocorticoid) levels are regulated by a hypothalamus-pituitary-adrenal hormone axis.
Corticotropin releasing hormone (CRH) controls adrenocortioctropic hormone (ACTH) release from the pituitary.
ACTH is a trophic hormone that stimulates:
-synthesis and secretion of cortisol and
-growth of the adrenal gland.
When cortisol levels increase, CRH and ACTH secretion/release are reduced.
38
Mineralocorticoids
Mineralocorticoids (e.g. aldosterone)-enhance renal tubular retention of Na+, HCO3- and water
and increase excretion of K+: this increases serum Na and decreases serum K
-increased blood volume and pressure
Removal of the adrenal glands leads to death within just a few days due to:
-the concentration of potassium in extracelluar fluid becomes dramatically elevated; -urinary excretion of sodium is high and concentrations of sodium in extracellular fluid decreases significantly; -volume of extracellular fluid and blood plummet; -the heart begins to function poorly, cardiac output declines and shock ensues

39
Control over aldosterone secretion is multifactorial:
-The two most significant regulators of aldosterone secretion are:
•Concentrations of K+ in extracellular fluid: Small increases in blood levels of potassium strongly stimulate aldosterone secretion.
•Angiotensin II: Activation of the renin-angiotensin system as a result of decreased renal blood flow (usually due to decreased vascular volume) results in release of angiotensin II, which stimulates aldosterone secretion
Control of Aldosterone Secretion
40
Adrenal Insufficiency (Addison’s disease, 1:100,000)
Primary Adrenal Insufficiency:
-most common cause is autoimmune-mediated destruction of the adrenal glands (>80%)
-secondary to tuberculosis, chronic fungal infections, infection by cytomegalovirus (CMV), metastasis to the glands by cancer cells (~20%)
Secondary Adrenal Insufficiency:
-Addison’s Disease caused by inadequate secretion of ACTH by the pituitary gland;
-may arise due to the prolonged or improper use of glucocorticoid hormones( temporary);
Disorders of the Adrenal Gland

41
Cushing’s Syndrome
-Cushing's Syndrome is EITHER a disease caused by an excess of cortisol production, or a disorder resulting from excessive use of glucocorticoids
Disease-related excess production of cortisol (2 types):1) Excess ACTH Production: Ex. A pituitary tumor producing too much ACTH
stimulates adrenal growth and increases cortisol (>70%); Also "ectopic" ACTH production (30%)
2) Adrenal cortex tumours: Tumours can be benign (an adenoma), or malignant (a carcinoma). Usually found on only one side.
Disorders of the Adrenal Gland
42
Hormones and stress • Stress = any condition that threatens homeostasis• GAS (General Adaptation Syndrome) is our bodies
response to stress-causing factors• Three phases to GAS
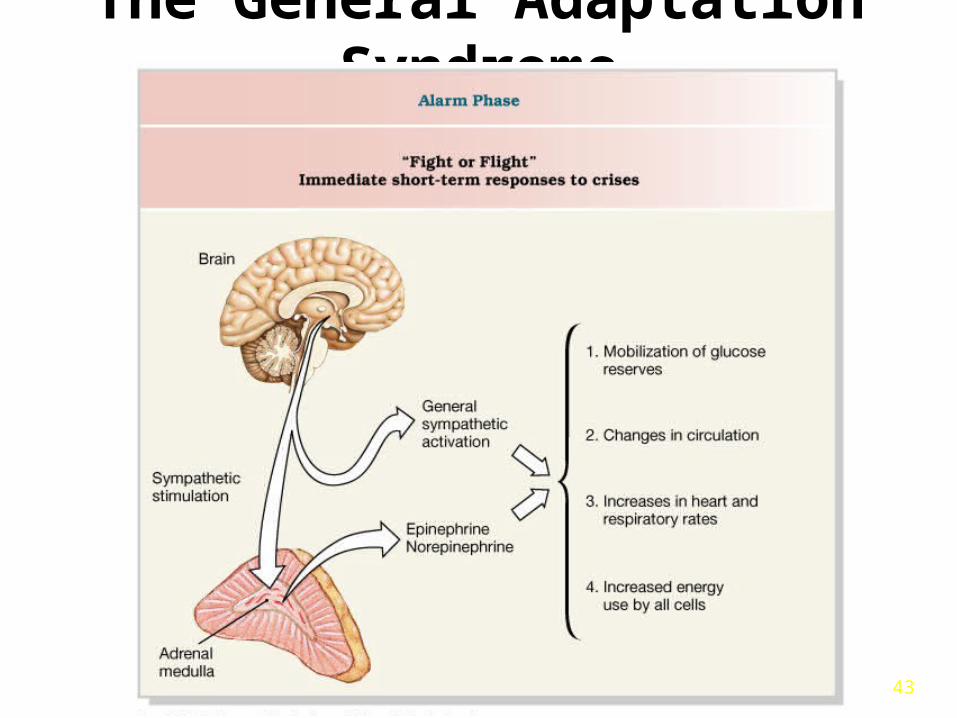
– Alarm phase (immediate, fight or flight, directed by the sympathetic nervous system and dominated by the catecholamines)
– Resistance phase (dominated by glucocorticoids)
– Exhaustion phase (breakdown of homeostatic regulation and failure of one or more organ systems)
43
The General Adaptation Syndrome

44
The General Adaptation Syndrome
Figure 18.21

45
The General Adaptation Syndrome

46
Retinoid Hormones• Isoprenoid hydrophobic
hormones.• The pro-hormone, retinol, is
made in the liver.• Retinol is converted to the
hormone, retinoic acid, by many tissues.
• Retinoic acid regulates cell growth and development in most cells, but the principal targets are the cornea, skin and epithelia.
• Excess Vitamin A can cause birth defects and liver damage.
• Severe acne is treated with retinoid creams.
47
THYROID HORMONES

48
The Thyroid Gland
Figure 18.11b, c
Thyroglobulin is a protein rich in Tyr (100Tyr/1molecule)

49
Synthesis of T3 and T4
The thyroid gland: Synthesizes and secretes triiodothyronine-T3 and thyroxine-T4
-the only body tissue that can accumulate iodide
Steps of thyroid hormone synthesis-accumulation of iodide via a specific iodide pump.-iodinatition of tyrosine produces monoiodotyrosine (MIT) and
diiodotyrosine (DIT)- coupling reaction: Synthesis of MIT/DIT: -MIT +DIT produces T3 (3 iodine) -DIT+DIT, T4 (4 iodine). -MIT/DIT are complexed with thyroglobulin.-Thyroglobin proteolysis liberates T3 and T4- Released hormones are secreted: 5(T4) to 1(T3).

50
TYROSINE IODINATION
CH2CHCOOH-
NH2
HO TyrTYROSINE
CH2CHCOOH
HO
CH2CHCOOH-
NH2
HOMONOIODOTYROSINE (MIT)
DIIODOTYROSINE (DIT)
I
I
NH2
TYROSINE IODINATION
I
I
SYNTHESIS OF THYROID HORMONES: STEP 1 - IODINATION
Approximately 10% of the tyrosine residues on the 550 amino acid residue Thyroglobulin molecule may become iodinated by the enzyme - thyroid peroxidase acting on the colloid at the luminal surface of the thyroid follicle. These reactions only occur in the thyroid at specific residues in “Hormonogenic” sites located at the extreme ends of the Thyroglobulin molecule.
Tyr
Tyr
THYROGLOBULIN
THYROGLOBULIN
THYROGLOBULIN-

51
Thyroglobulin
CH2CHCOOH
Thyroglobulin
I
I
Tyr
3,5,3’5’-tetraiodothyronine
SYNTHESIS OF THYROID HORMONES: STEP- 2 COUPLING OF IODOTYROSINES
CH2CHCOOH
NH2
+HO
II
I
Tyr
NH2
T4
Thyroglobulin
I
I
Tyr CH2CHCOOH
NH2
CH2CHCOOH
I
Tyr
NH2
Thyroglobulin
Tyr
II
I
Tyr O
+
IT3
3,5,3’-Triiodothyronine
Coupling of iodotyrosine moities results in the loss of the peptide linkage to thyroglobulin allowing thyroid hormones to diffuse across the cell membrane
II
Tyr
II
I
Tyr O
I
33’
5 5’
HO
HO
HO
HO
HO
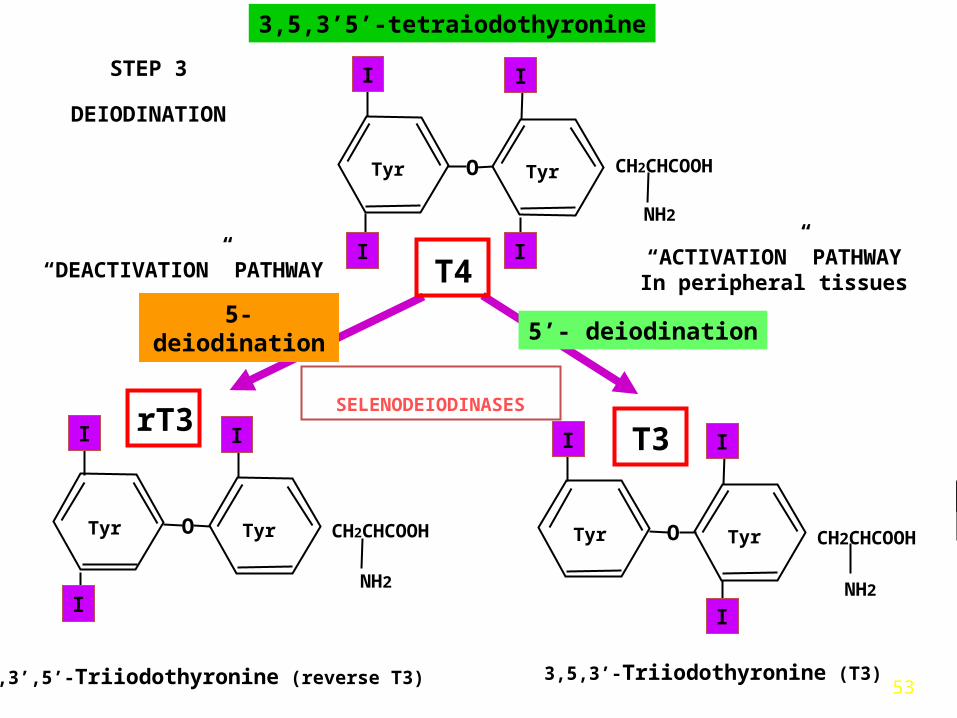
53
3,5,3’5’-tetraiodothyronine
CH2CHCOOH
NH2
CH2CHCOOH
3,3’,5’-Triiodothyronine (reverse T3)
NH2
Tyr
II I
Tyr O
rT3
I
3,5,3’-Triiodothyronine (T3)
II
Tyr
II
I
Tyr O
T4I
T3
Tyr
II I
Tyr O
I
5’- deiodination5-deiodination
CH2CHCOOH
“ACTIVATION” PATHWAYIn peripheral tissues
“DEACTIVATION” PATHWAY
NH2
STEP 3
DEIODINATION
SELENODEIODINASES
54
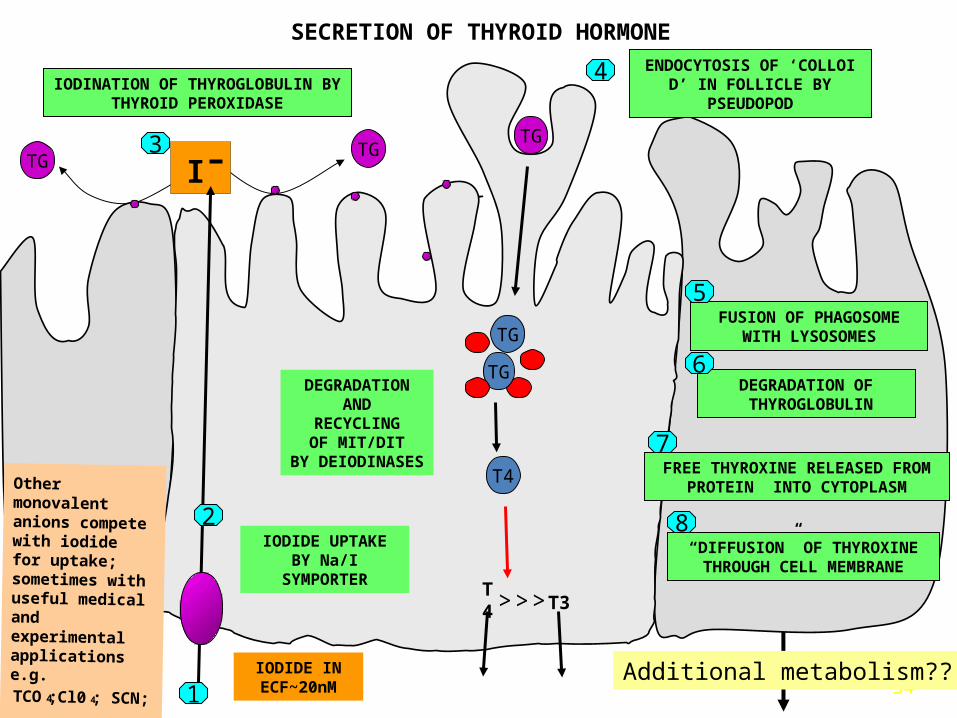
TG
SECRETION OF THYROID HORMONE
IODINATION OF THYROGLOBULIN BY THYROID PEROXIDASE
“DIFFUSION” OF THYROXINE THROUGH CELL MEMBRANE
DEGRADATION OF THYROGLOBULIN
FUSION OF PHAGOSOME WITH LYSOSOMES
ENDOCYTOSIS OF ‘COLLOID’ IN FOLLICLE BY
PSEUDOPOD
TG
TG
TG
T4
T4 T3>> >
I
IODIDE UPTAKEBY Na/I
SYMPORTER
IODIDE IN ECF~20nM
DEGRADATIONAND
RECYCLINGOF MIT/DIT
BY DEIODINASES
Other monovalent anions compete with iodide for uptake; sometimes with useful medical and experimental applications e.g.
TCO 4;Cl0 4; SCN;
FREE THYROXINE RELEASED FROM PROTEIN INTO CYTOPLASM
TG
2
1
3
4
5
6
7
8
Additional metabolism??

55
THYROID HORMONES
HORMONERELATIVE POTENCY
PRODUCTION t½
(µg/day)
4-8 (24)*
BOUND TO PLASMA
PROTEINS
(%)
-
99.95
(days)
80- 90 8
0.04 99.8 0.1
+ + + +
rT3
VALUES IN PARENTHESES INDICATE PERIPHERAL CONVERSION
2-3 (27) *
1-3
6-7+T4
T3
*
(µg/dL)
PLASMACONCENTRATION
0.3 99.7
56
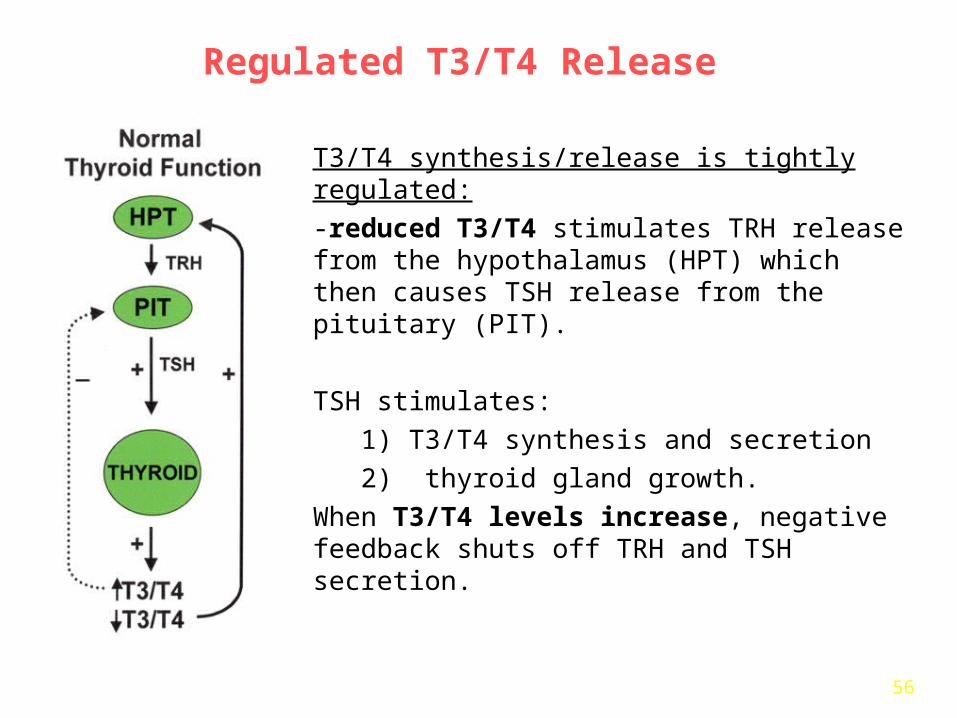
Regulated T3/T4 Release
T3/T4 synthesis/release is tightly regulated:
-reduced T3/T4 stimulates TRH release from the hypothalamus (HPT) which then causes TSH release from the pituitary (PIT).
TSH stimulates:
1) T3/T4 synthesis and secretion
2) thyroid gland growth.
When T3/T4 levels increase, negative feedback shuts off TRH and TSH secretion.
57
Physiological Actions of T3/T4
Play a Central Role in Regulating:
-growth/development of most cells,-basal metabolic rate and temperature (stimulate cellular respiration)-cardiac output by increasing rate/force of contraction,-metabolism of cholesterol to bile acids,-LDL receptor expression in hepatocytes,-TSH secretion
THYROID HORMONES ARE ESSENTIAL TO LIFE!
58
Symptoms include: fatigue/weakness, weight gain/difficulty losing weight, coarse/dry hair, dry/rough pale skin, cold intolerance, muscle cramps/muscle aches, constipation, depression, irritability, memory loss, abnormal menstrual cycles, decreased libido
-Myxedema coma: A medical emergency characterized by hypothermia, hypotension, hypoventilation and bradycardia represents the extreme expression of severe hypothyroidism
Hypothyroidism (Myxedema)Reduced circulating T3/T4 levels
59
Problems with the Thyroid Gland
Hyperthyroidism:• high metabolic rate, hyperactivity, sensitivity to heat, protruding eyes• Grave’s disease: when hyperthyroidism is due to an autoimmune problem
(TSH is mimicked by autoantibodies)
Hypothyroidism:• in the adult: myxedema- low metabolic rate, sensitivity to cold,
sluggishness, weight gain/difficulty losing weight, coarse/dry hair, dry/rough pale skin, constipation, depression, irritability, memory loss, abnormal menstrual cycles, decreased libido
• in an infant: cretinism-- stunted growth, mental retardation, abnormal bone formation
• Hashimoto’s disease: when hypothyroidism is due to an autoimmune problem (autoantibodies attack and destroy follicular cells)
• goiter no T3 and T4 can be made because not enough iodides were ingested.
60
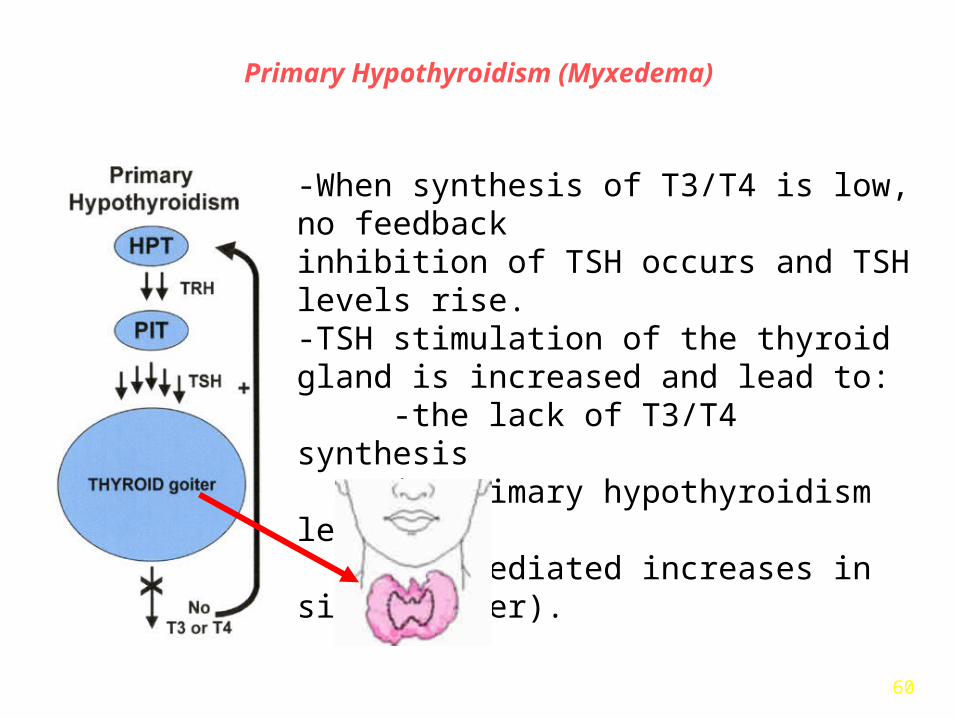
Primary Hypothyroidism (Myxedema)
-When synthesis of T3/T4 is low, no feedbackinhibition of TSH occurs and TSH levels rise.-TSH stimulation of the thyroid gland is increased and lead to:
-the lack of T3/T4 synthesisin primary hypothyroidism leads toTSH-mediated increases in size (goiter).

61
Secondary Hypothyroidism
When the pituitary can't make TSH there is no signal to the thyroid gland to make T3/T4. Thus secondary hypothyroidism is (i.e. pituitary- mediated) associated with decreased T3/T4 AND TSH and thyroid atrophy.
62
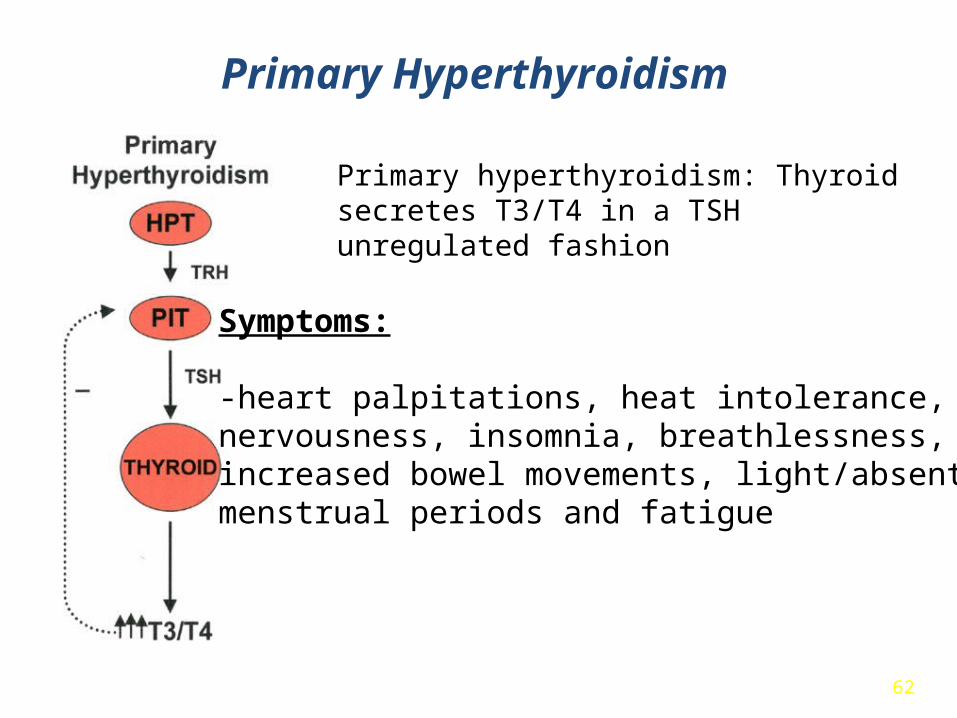
Primary hyperthyroidism: Thyroid secretes T3/T4 in a TSH unregulated fashion
Symptoms: -heart palpitations, heat intolerance, nervousness, insomnia, breathlessness,increased bowel movements, light/absentmenstrual periods and fatigue
Primary Hyperthyroidism
63
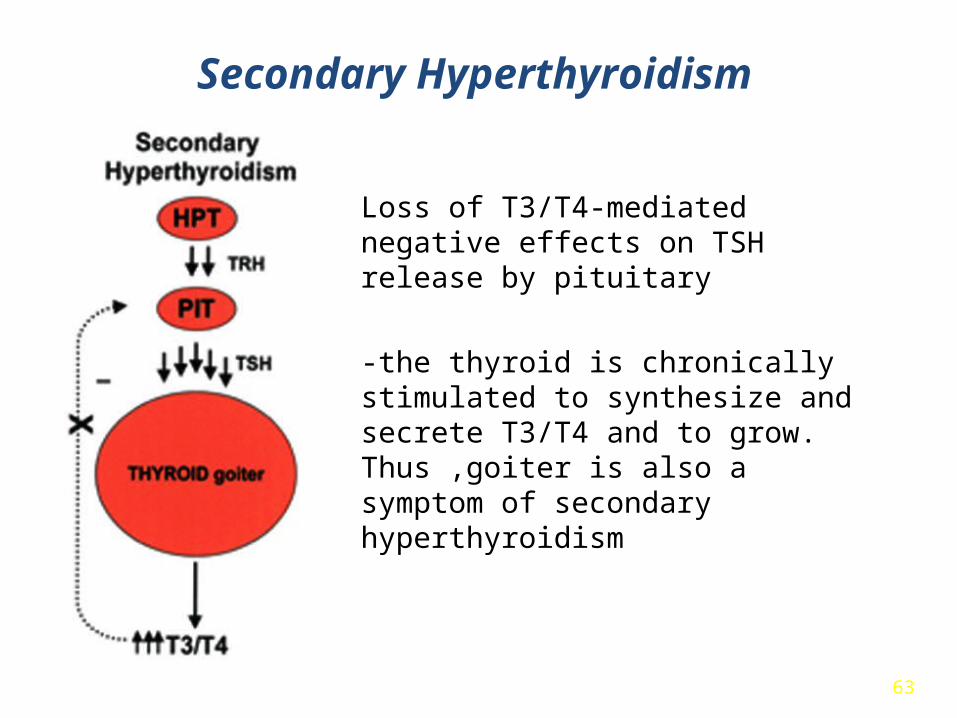
Loss of T3/T4-mediated negative effects on TSH release by pituitary
-the thyroid is chronically stimulated to synthesize and secrete T3/T4 and to grow. Thus ,goiter is also a symptom of secondary hyperthyroidism
Secondary Hyperthyroidism

64
Relief of direct symptoms: Drugs that inhibit thyroid hormone production/release (methimazole, propylthiouracil (PTU):
-Inhibit hrmone synthesis (iodine organification) -Inhibit MIT coupling
Limitations: The symptoms associated with hyperthyroidism return when the drugs are discontinued.
Hyperthyroidism-Treatments

65
Radioactive Iodine:[135I]-most widely recommended permanent treatment ofhyperthyroidism
-treatment takes advantage of the fact that only thyroid cellscan incorporate iodine
-[135I] emits gamma (γ) radiation: Directly kills thyroid cells
-There is no evidence that [135I] treatment for hyperthyroidism causes cancer of the thyroid gland or of any other tissue
Hyperthyroidism-Treatments
66
BUT IS CALCITONIN AN IMPORTANT PHYSIOLOGICAL SUBSTANCE?
The observation that calcitonin (CT) at supraphysiological doses is hypocalcemic, led to the mistaken conclusion that it was important for calcium homeostasis and this idea has persisted to this day. Despite these findings there is no apparent pathology due to CT excess or deficiency and there is no evidence that circulating CT is of substantial benefit to any mammal.
Mammalian CT at physiological doses is not essential and very likely the CT gene has survived because of the gene’s alternate mRNA pathway to produce calcitonin-gene-related peptide CGRP found in neural tissues.
HIRSCH,PF and BARUCH H, ENDOCRINE 2003, 201-208
CALCITONIN IS SECRETED FROM THE THYROID PARAFOLLICULAR CELLS

67
THE PARATHYROID HORMONE

68
Parathyroid Gland• This gland only secretes
one hormone: Parathyroid Hormone (or PTH)
• PTH function (we began learning this when we studied bone):– increases blood
calcium (Ca2+) levels and decreases blood phosphate (PO4
2-) levels
69
PTH function (continued)
• How does PTH work?– PTH causes Ca2+ & PO4
2- to be released from bone into blood (by increasing osteoclast activity)
– PTH decreases the excretion of PO42- ions
through urine– PTH increases calcitriol production, so that
more Ca2+ is absorbed during digestion• PTH is regulated by blood calcium levels-- not
by other glands!

70Figure 18.15
The Regulation of Calcium Ion Concentrations

71
THE PANCREATIC HORMONES

72
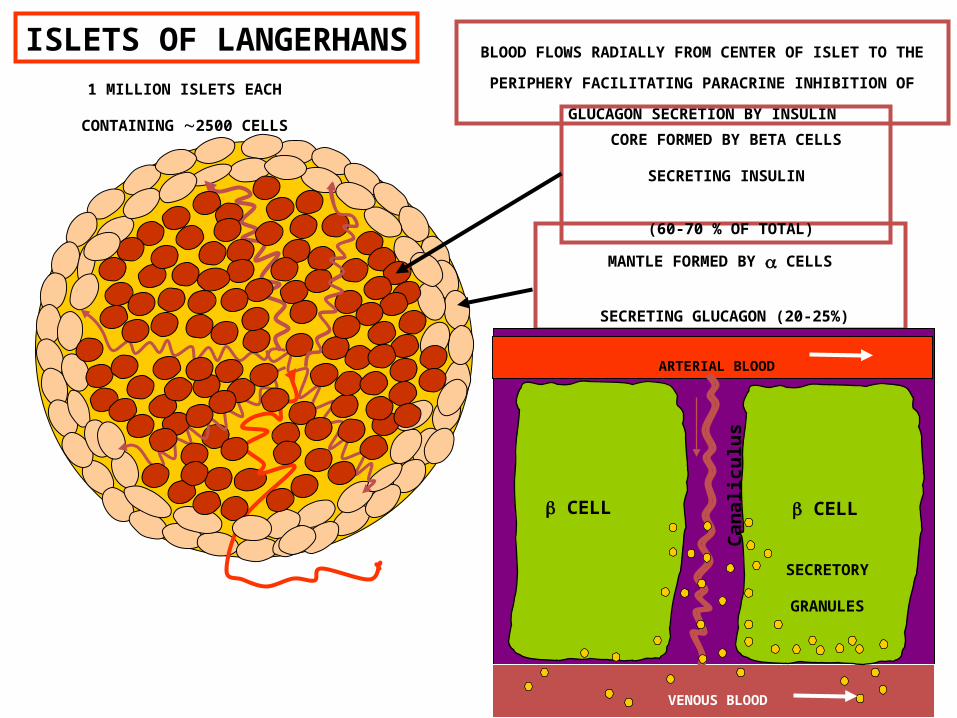
The pancreatic islets
• Clusters of endocrine cells within the pancreas called Islets of Langerhans or pancreatic islets– Alpha cells secrete glucagons– Beta cells secrete insulin– Delta cells secrete GH-IH– F cells secrete pancreatic polypeptide

73
The Endocrine Pancreas
Figure 18.18a, b
74
BLOOD FLOWS RADIALLY FROM CENTER OF ISLET TO THE
PERIPHERY FACILITATING PARACRINE INHIBITION OF
GLUCAGON SECRETION BY INSULIN
VENOUS BLOOD
ISLETS OF LANGERHANS
MANTLE FORMED BY CELLS
SECRETING GLUCAGON (20-25%)
CORE FORMED BY BETA CELLS
SECRETING INSULIN
(60-70 % OF TOTAL)
1 MILLION ISLETS EACH
CONTAINING 2500 CELLS
ARTERIAL BLOOD
VENOUS BLOOD
CELL CELL
SECRETORY
GRANULES
Ca
na
licu
lus

75

76
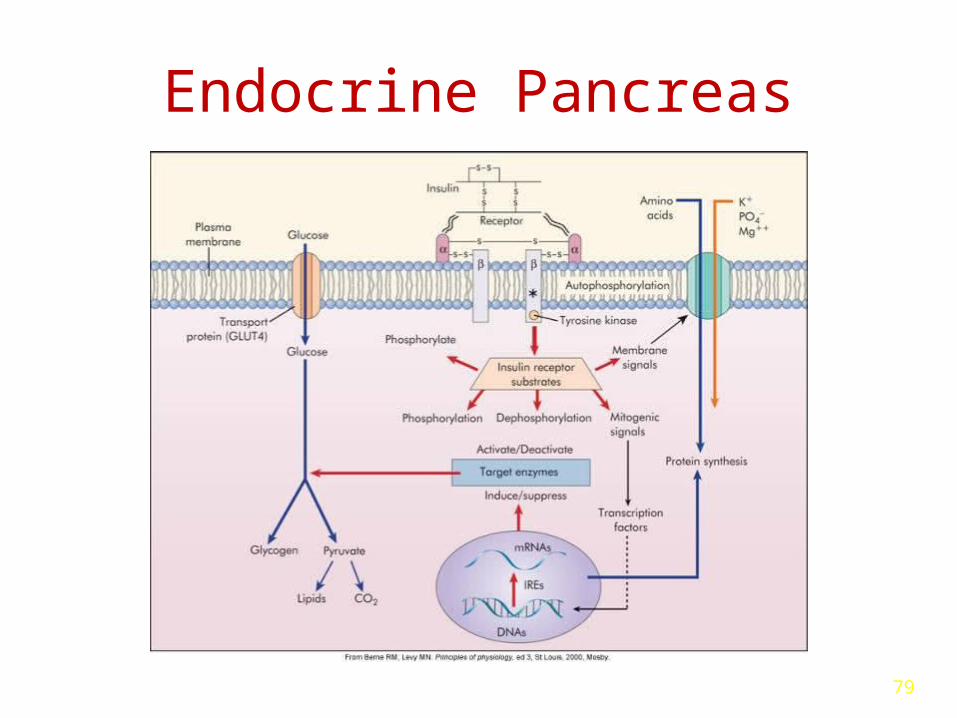
Endocrine Pancreas
• Insulin– Synthesized from proinsulin– Secretion is promoted by ↑ blood glucose– Facilitates the rate of glucose uptake into
the cells– Anabolic hormone
• Synthesis of proteins, lipids and nucleic acids
77
Endocrine Pancreas• Glucagon
– Secretion is promoted by decreased blood glucose levels
– Stimulates glycogenolysis, gluconeogenesis and lipolysis
• Somatostatin (delta cells)– Regulation alpha and beta cell secretions
78
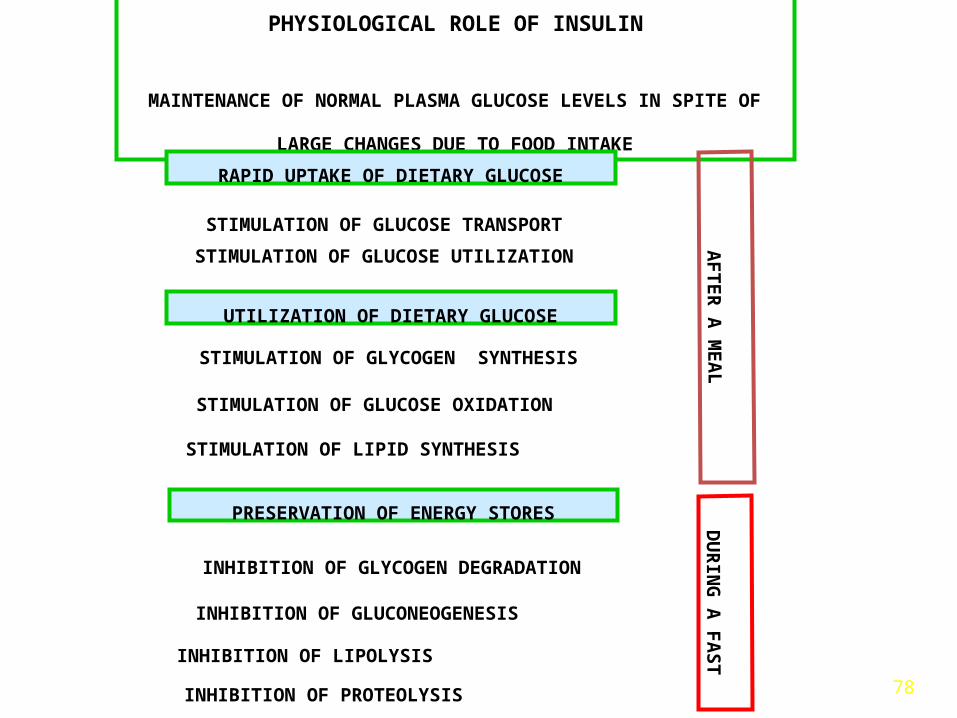
PHYSIOLOGICAL ROLE OF INSULIN
MAINTENANCE OF NORMAL PLASMA GLUCOSE LEVELS IN SPITE OF
LARGE CHANGES DUE TO FOOD INTAKE
PRESERVATION OF ENERGY STORES
STIMULATION OF GLUCOSE TRANSPORT
STIMULATION OF GLUCOSE UTILIZATION
RAPID UPTAKE OF DIETARY GLUCOSE
UTILIZATION OF DIETARY GLUCOSE
STIMULATION OF GLUCOSE OXIDATION
STIMULATION OF LIPID SYNTHESIS
STIMULATION OF GLYCOGEN SYNTHESIS
INHIBITION OF GLYCOGEN DEGRADATION
INHIBITION OF GLUCONEOGENESIS
INHIBITION OF LIPOLYSIS
INHIBITION OF PROTEOLYSIS
AF
TE
R A
ME
AL
DU
RIN
G A
FA
ST
79
Endocrine Pancreas
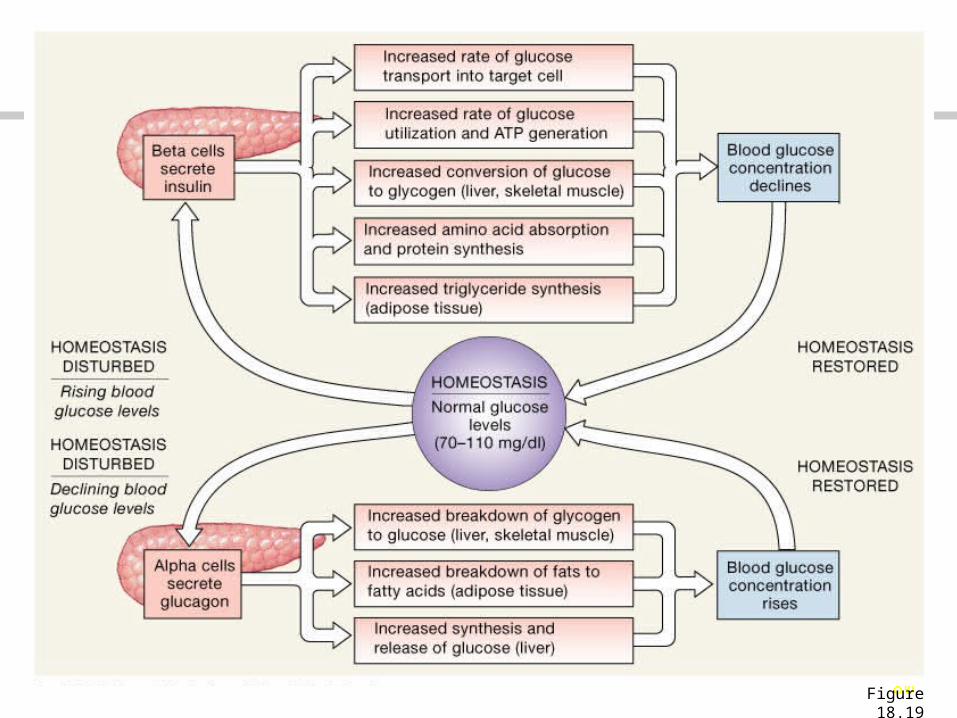
80Figure 18.19
Figure 18.19 The Regulation of Blood Glucose Concentrations

81
THE PINEAL GLAND

82
Pineal Gland
Secretes only one hormone: melatonin
- involved in your circadian rhythm (your recognition of day and night times):
– melatonin secretion decreases in the day
– melatonin secretion increases at night
Melatonin is also involved in longer rhythms, like monthly and seasonal
- inhibits reproductive function
- protects against damage by free radicals
- has anti-ageing, anti-cancer effects
83
The Endocrine Functions of Other Organs
84
The intestines
• Produce hormones important to the coordination of digestive activities

85
The kidneys
• Produce calcitriol and erythropoietin (EPO) and the enzyme rennin– Calcitriol = stimulates calcium and phosphate ion
absorption along the digestive tract– EPO stimulates red blood cell production by bone
marrow– Renin converts angiotensinogen to angiotensin I

86
Angiotensin I converted to angiotensin II in the lungs
• Stimulates adrenal production of aldosterone• Stimulates pituitary gland release of ADH• Promotes thirst• Elevates blood pressure

87
Endocrine Functions of the Kidneys

88
Endocrine Functions of the Kidneys
LUNGS

89
The heart
• Specialized muscle cells produce natriuretic peptides when blood pressure becomes excessive– Generally oppose actions of angiotensin II
90
The thymus
• Produces thymosins– help develop and maintain normal immune
defenses– are involved in white blood cell production
91
Adipose tissues secrete
• Leptin, a feedback control for appetite
• Resistin, which reduces insulin sensitivity
92
The gonads• Interstitial cells of the testes
produce testosterone– Most important sex hormone
in males• In females, oocytes develop in
follicles– Follicle cells produce
estrogens• After ovulation, the follicle cells
form a corpus luteum that releases a mixture of estrogens and progesterone
93
I fought the law, but the law won…..