measurement of pre and postprandial urine calcium to ... · identify calcium oxalate urolithiasis...
TRANSCRIPT

Measurement of Pre and Postprandial Urine Calcium to Creatinine Ratio to
Identify Calcium Oxalate Urolithiasis in Miniature Schnauzers
Susan V. Carr
Thesis submitted to the faculty of Virginia Polytechnic Institute and State
University in partial fulfillment of the requirements for the degree of
Master of Science
In
Biomedical and Veterinary Sciences
David C. Grant, Chair
Stefanie M. DeMonaco
Megan Shepherd
May 21, 2018
Blacksburg VA

Measurement of Pre and Postprandial Urine Calcium to Creatinine Ratio to
Identify Calcium Oxalate Urolithiasis in Miniature Schnauzers
Abstract:
The intent of this research is to identify a simple diagnostic test to detect abnormal calciuresis and
predict calcium oxalate (CaOx) urolith presence in Miniature Schnauzers. We investigated the impact
of postprandial time on the specificity of urine calcium:creatine (UCa/Cr) in identifying affected dogs.
The hypotheses were: 1) Significant differences exist in fasted and postprandial UCa/Cr between
urolith-forming and control schnauzers. 2) UCa/Cr increases significantly from fasted baseline at one
or more postprandial time point(s).
Urine samples were collected from Miniature Schnauzers with (urolith-formers) and without (controls)
CaOx uroliths in a fasted state and 1, 2, 4, and 8 hours after feeding a standardized diet. The change in
UCa/Cr from baseline was calculated for each postprandial time. Urolithiasis status and the time point
were assessed for impact on the UCa/Cr and change in UCa/Cr using a mixed model ANOVA.
Based on 9 urolith-forming and 15 control dogs enrolled, urolith-forming Miniature Schnauzers have
significantly higher mean UCa/Cr at 1 hour and 8 hours postprandial timepoints indicating altered
calciuresis. The change in UCa/Cr was not significant at any post-prandial time point between or
within groups.
This pilot study shows male urolith-forming Miniature Schnauzers have excessive calciuresis
throughout the day, providing insight into the mechanism behind their formation of CaOx uroliths. If
using the Ca/Cr ratio, the postprandial sampling time is not critical. This simple urine measurement
has potential as a marker of urolith presence and possibly risk of urolith formation.

Measurement of Pre and Postprandial Urine Calcium to Creatinine Ratio to
Identify Calcium Oxalate Urolithiasis in Miniature Schnauzers
Abstract (public):
Calcium oxalate urinary stones are a frequently encountered problem in Veterinary Medicine, as they
have an increased incidence amongst several popular dog breeds; the Miniature Schnauzer, Yorkshire
Terrier, Bichon Frise, Toy Poodle and Dachshund. These stones are a significant source of pain for
affected dogs and financial strain for pet owners. The causes of calcium oxalate urinary stone
formation are not fully known, but increased urinary calcium has been identified in affected dogs. We
are quantifying calcium excretion by performing a measurement called urine calcium to creatinine ratio
(UCa/Cr). The hypothesis of this research is that the UCa/Cr will be significantly greater in stone-
forming dogs than non-stone forming dogs (controls). The second hypothesis is that the difference
between the two groups will be even greater in the hours after feeding.
This findings of this study show that Miniature Schnauzers that form calcium oxalate urinary stones
have significantly higher mean UCa/Cr than control dogs at multiple points throughout the day. The
change in UCa:Ca over the day was not significant. The UCa/Cr proved to be a simply cost-effective
biomarker to identify Miniature Schnauzers who may be at risk for CaOx urinary stone formation.

Acknowledgements:
Thank you to my Masters and residency supervisor Dr. David Grant, for conceiving the idea for this
project, then supervising and supporting me throughout. I would also like to thank my committee
members Dr. Stefanie DeMonaco and Dr. Meghan Shepherd for their suggestions with study design and
advice on manuscript preparation. Dr. Werre provided valuable statistical advice and assistance. Thank
you to Mindy Quigley who creatively helped with patient recruitment and co-ordination. Finally I
gratefully acknowledge the staff and clients of the VTH who volunteered to participate and contribute to
this research. Financial support for this project was generously provided by the Morris Animal
Foundation.

iv
Table of Contents
Abstract
Acknowledgments
Table of Contents
List of Abbreviations used
Chapter 1: Literature Review
A. Calcium homeostasis …………………………………………………………………………………1
1. Intestinal absorption
A.1.1. Role of diet
2. Renal handling
A.2.1. Diseases and drugs affecting calciuresis
B. Kinetics of calcium oxalate crystal formation and growth ………………………………...………9
1. Urine supersaturation
2. Promotors and inhibitors of crystallization, aggregation and growth
B.2.1. Promotors
B.2.2. Inhibitors
B.2.2.1. Organic inhibitors
B.2.2.2. Inorganic inhibitors: Crystalloid complexors
3. The noncrystalline matrix
C. Clinical calcium oxalate urolithiasis in dogs ………………………………………...…………….13
1. Prevalence and consequences
2. Risk factors
C.2.1. Urine composition
C.2.1.1. USG
C.2.1.2. Calcium concentration
C.2.1.3. Urinary oxalate
C.2.1.4. Other urinary consistuents
C.2.2. Patient variables
C.2.2.1. Gender
C.2.2.2. Breed
C.2.2.3. Age
C.2.2.4. Body Condition
C.2.2.5. Body Size
C.2.2.6. Concurrent disease
3. Diagnosis and Treatment
4. Management and Prevention
C.4.1. Diet composition
C.4.2. Moisture content
C.4.3. pH
C.4.4. Potassium citrate

v
C.4.5. Thiazide diuretics
Chapter 2: Pre and postprandial urinary calcium to creatinine ratio to identify calcium oxalate urolithiasis
in male Miniature Schnauzers
A. Introduction …………………………………………………………………..…………………..19
B. Materials and Methods……………………………………………………………………………20
C. Results…………………………………………………………………………………………….22
D. Discussion and Conclusion……………………………………………………………………….24
References ………………………………………………………………………………………………...27
Appendices……………………………………………………………………………………………...…37
List of abbreviations
1,25-dihydroxyvitamin D3 (calcitriol)
Calcium oxalate (CaOx)
Calcium sensing receptors (CaSR)
Familial hypomagnesemia with hypercalciuria and nephrocalcinosis (FHHNC)
Odds Ratio (OR)
Parathyroid hormone (PTH)
Relative supersaturation (RSS)
Renal outer medullary potassium channel (ROMK)
Tamm-Horsfall protein (THP)
Transient Receptor potential Vanilloid Channel type 5,-6 (TRPV-5, TRPV-6)
Urinary Calcium to creatinine ratio (UCa/Cr)
Urine Specific Gravity (USG)

1
CHAPTER ONE
SECTION A: CALCIUM HOMEOSTASIS
Calcium homeostasis is tightly regulated by a number of pathways that are designed to maintain steady
serum calcium concentration. Strict control ensures sufficient calcium for neuronal signaling, muscle
contraction and many other biochemical pathways, whilst avoiding the deleterious effects of
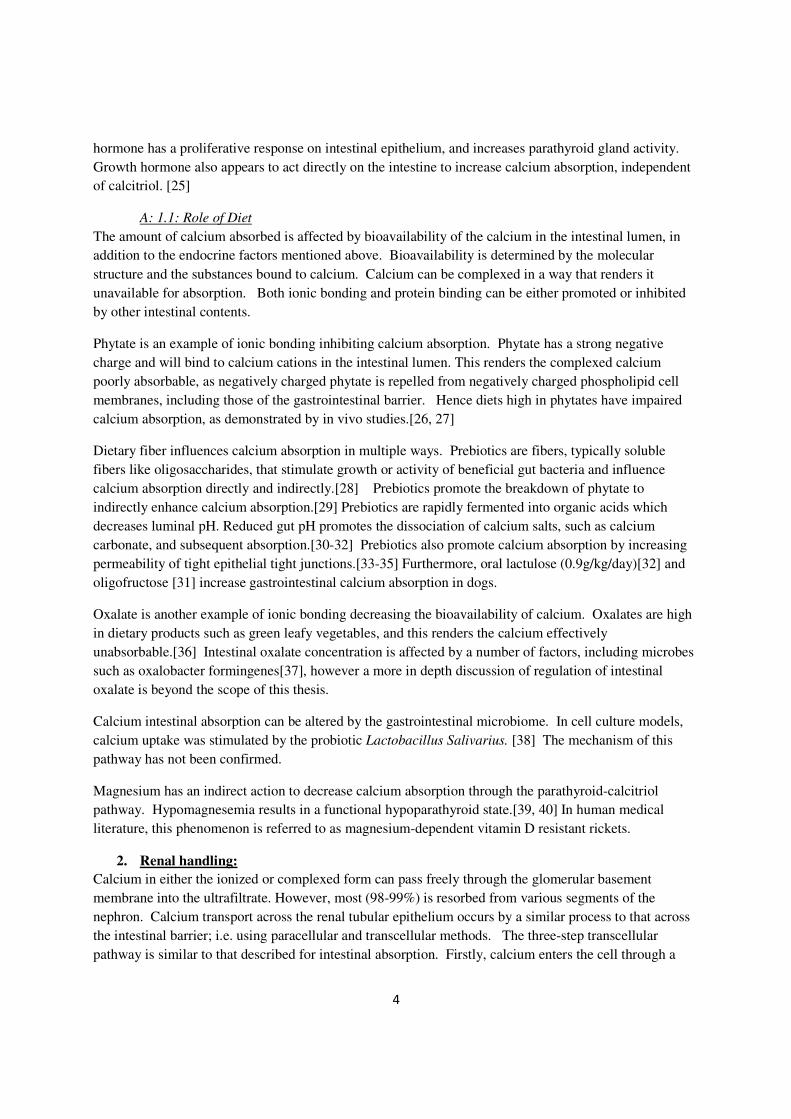
hypercalcemia such as dystrophic soft tissue mineralization. Calcium homeostasis is regulated by a
number of mechanisms (see figure 1). The sources of serum calcium are intestinal absorption and the
skeleton. This is balanced against calcium efflux, either excreted in urine or stool or stored as bone.
Although the skeleton is a vital component of calcium homeostasis as the reservoir of 99% of the body’s
calcium, this thesis will only be discussing mechanisms of control of gastrointestinal absorption and renal
elimination, reabsorption, and excretion.
Figure 1: Factors affecting calcium homeostasis
1. Gastrointestinal absorption and elimination
Although calcium is absorbed throughout the intestinal tract, it mainly occurs mainly in the duodenum,
ileum and cecum, and to a lesser extent in the proximal and distal colon. [1, 2]
There are three methods of calcium absorption across the gastrointestinal barrier: transcellular facilitated
diffusion, transcellular vesicle transport and paracellular movement through tight junctions. Transcellular
facilitated diffusion is a three step pathway through the enterocyte. In the initial step, calcium cations pass
through the channels in the apical side of the enterocyte membrane (see Figure 2), along an
electrochemical gradient. Evidence suggests that the TPRV6 channel (previously also referred to as
ECaC2 and CaT1) is involved in the step, and other proteins and channels such as Cav1.3 and TRPV5

2
(also called ECaC1 and CaT2). [3-6] The second step involves transport across the epithelial cell. The
calcium cations bind to calbindin-D9k protein, which moves calcium across the cell to the basement
membrane. The act of calcium cation removal from the apical side assists in maintaining the translumen-
epithelial concentration gradient. Finally, calcium is transported across the basal membrane by one of
two ways: either an ATP-ase pump or a Ca-Na exchange transporter.
The second mechanism of transcellular calcium movement is transcellular vesicle transport, which occurs
via endocytosis-exocytosis transport. This is less frequently described, although has been demonstrated
in chick models.[7]
The third method of calcium absorption across the intestinal barrier is paracellular movement through
tight junctions. Tight junctions are regulated by various proteins, including claudins, which control which
substances can pass through the junction. [8]
Figure 2: Pathways of gastrointestinal calcium absorption.
(A) Transcellular facilitated diffusion, which occurs by
three steps: (1) movement through calcium channel such as
TPRV6 on apical cell surface. (2) transport across cell by
calcium binding protein, calbindin-D9k. (3) extrusion from
basement membrane by either an ATPase pump or Ca-Na
co-transporter.
(B) Transcellular vesicular transport,
(C) Paracellular movement through tight junctions.
Only a limited amount of ingested dietary calcium is absorbed across the intestine and the remainder is
eliminated in feces. When serum calcium concentration is normal and there is abundant dietary calcium,
the main route of calcium absorption is by paracellular diffusion down the concentration gradient.
However, if additional calcium absorption is required, the demand is met mainly by the transcellular
pathway as it has significant scope for upregulation, unlike the paracellular pathway that is saturatable.

3
In adult humans, it has been estimated that approximately 30% of dietary calcium is absorbed.[9]
However, this varies widely with reports of intestinal calcium absorption ranging from <10% to >60%
[10]. Fecal calcium is generally the primary means for calcium elimination as fecal calcium rises in
parallel, when dietary calcium is doubled or tripled in humans [11] and dogs [12]. Conversely, when
serum calcium is low, fractional intestinal absorption increases. This has also been demonstrated by a
number of studies in dogs, which have been summarized elsewhere[13]. This variability in fractional
absorption is regulated by various mechanisms in an attempt to keep serum calcium at a constant
concentration.
The most effective regulator of intestinal calcium absorption is the active form of vitamin D, 1,25-
dihydroxyvitamin D3 (from here-on referred to as calcitriol). In response to hypocalcemia, parathyroid
hormone (PTH) stimulates hydroxylation of the precursor 25-hydroxyvitamin D to calcitriol. Conversion
requires 1-alpha-hydroxylase, an enzyme produced primarily by the kidney. It was previously considered
that the cells of the proximal tubule were the main source of this enzyme,[14] however it has now been
demonstrated by immunohistochemistry and in situ hybridization that 1-alpha-hydroxylase is expressed,
and hence calcitriol generated, throughout all segments of the nephron.[15]
Calcitriol mainly circulates bound to a carrier protein: vitamin D binding protein. Calcitriol is lipophilic
and thus can diffuse through the target cell’s membrane. Once in the cell, they bind to intracellular
receptors in the nucleus called vitamin D receptors (VDR), and they alter gene transcription.
Although VDR are located throughout the body and have a variety of actions, only their effect on
regulating calcium balance will be discussed here. When calcitriol activates the intestinal VDR,
upregulation of the TRPV-6 gene causes increased expression of calcium epithelial channels.[16]
Activation of VDR also increases calbindin D9k production.[16] Thus calcitriol increases calcium
absorption from the intestinal tract.[1, 17, 18]
Although the most significant action of calcitriol is to upregulate transcellular calcium movement, it also
affects the paracellular absorption pathway. Calcitriol stimulates the VDR in the enterocyte to cause an
upregulation of claudins-2 and -12.[19] This increases the permeability of the tight junctions to calcium,
thus allowing increased passive transport between cells.
Another regulatory pathway involves parathyroid hormone acting directly on the intestine. Using
immunoreactive staining, some research has discovered PTH receptors located on intestinal epithelial
cells.[20] However, the specifics of this pathway have not been proven. Therefore, the main action by
which PTH affects calcium absorption is indirect ie by increasing the conversion of Vitamin D to the
active form calcitriol.
Other calcitropic hormones control absorption by causing a local effect on the intestine, or by influencing
calcitriol, or both. Thyroid hormone appears to increase calcium absorption, possibly by increasing the
Na-Ca efflux pump on the basolateral membrane, and/or increasing vesicular transport across the cell.[21]
Estrogen influences intestinal calcium absorption, and this effect is demonstrated by reduced intestinal
calcium absorption in post-menopausal women. Estrogen appears to have genomic effects on the
intestine to increase expression of TRPV5, TRPV6, calbindin-D9k and the plasma membrane calcium-
ATPase pump.[22] Prolactin has also been shown to directly increase intestinal calcium absorption, [23]
and is considered to be the principal calcitropic hormone in pregnancy and lactation.[24] Growth
4
hormone has a proliferative response on intestinal epithelium, and increases parathyroid gland activity.
Growth hormone also appears to act directly on the intestine to increase calcium absorption, independent
of calcitriol. [25]
A: 1.1: Role of Diet
The amount of calcium absorbed is affected by bioavailability of the calcium in the intestinal lumen, in
addition to the endocrine factors mentioned above. Bioavailability is determined by the molecular
structure and the substances bound to calcium. Calcium can be complexed in a way that renders it
unavailable for absorption. Both ionic bonding and protein binding can be either promoted or inhibited
by other intestinal contents.
Phytate is an example of ionic bonding inhibiting calcium absorption. Phytate has a strong negative
charge and will bind to calcium cations in the intestinal lumen. This renders the complexed calcium
poorly absorbable, as negatively charged phytate is repelled from negatively charged phospholipid cell
membranes, including those of the gastrointestinal barrier. Hence diets high in phytates have impaired
calcium absorption, as demonstrated by in vivo studies.[26, 27]
Dietary fiber influences calcium absorption in multiple ways. Prebiotics are fibers, typically soluble
fibers like oligosaccharides, that stimulate growth or activity of beneficial gut bacteria and influence
calcium absorption directly and indirectly.[28] Prebiotics promote the breakdown of phytate to
indirectly enhance calcium absorption.[29] Prebiotics are rapidly fermented into organic acids which
decreases luminal pH. Reduced gut pH promotes the dissociation of calcium salts, such as calcium
carbonate, and subsequent absorption.[30-32] Prebiotics also promote calcium absorption by increasing
permeability of tight epithelial tight junctions.[33-35] Furthermore, oral lactulose (0.9g/kg/day)[32] and
oligofructose [31] increase gastrointestinal calcium absorption in dogs.
Oxalate is another example of ionic bonding decreasing the bioavailability of calcium. Oxalates are high
in dietary products such as green leafy vegetables, and this renders the calcium effectively
unabsorbable.[36] Intestinal oxalate concentration is affected by a number of factors, including microbes
such as oxalobacter formingenes[37], however a more in depth discussion of regulation of intestinal
oxalate is beyond the scope of this thesis.
Calcium intestinal absorption can be altered by the gastrointestinal microbiome. In cell culture models,
calcium uptake was stimulated by the probiotic Lactobacillus Salivarius. [38] The mechanism of this
pathway has not been confirmed.
Magnesium has an indirect action to decrease calcium absorption through the parathyroid-calcitriol
pathway. Hypomagnesemia results in a functional hypoparathyroid state.[39, 40] In human medical
literature, this phenomenon is referred to as magnesium-dependent vitamin D resistant rickets.
2. Renal handling:
Calcium in either the ionized or complexed form can pass freely through the glomerular basement
membrane into the ultrafiltrate. However, most (98-99%) is resorbed from various segments of the
nephron. Calcium transport across the renal tubular epithelium occurs by a similar process to that across
the intestinal barrier; i.e. using paracellular and transcellular methods. The three-step transcellular
pathway is similar to that described for intestinal absorption. Firstly, calcium enters the cell through a

5
calcium channel due to the electrochemical or electrical gradient. Secondly, calcium is transported to the
basolateral membrane by a cytoplasmic binding protein, such as calbindin. Thirdly, calcium exits the cell
across the basolateral membrane by either a Ca-ATPase pump or a sodium-calcium counter
transporter.[41]
The predominate method and rate of absorption varies among the different segments of the nephron.[42]
Approximately 60-65% of calcium resorption occurs in the proximal tubule, mainly by paracellular
processes.[43] Solute drag occurs as a significant proportion of fluid passes out of the ultrafiltrate into the
interstitial space, driven mainly by a sodium concentration gradient. As calcium ions are dissolved in this
fluid, they are carried out of the tubular lumen, between the epithelial cells, and into the interstitial space.
Calcium and sodium ions are able to freely pass between cells due to cation-permeable channels formed
by claudins 16 and 19. [44] Calcium excretion in the proximal tubule is predominately determined by
filtered load; a fractional excretion study in the dog demonstrates decreased filtered calcium in volume-
depleted dogs and increased filtered calcium in saline-loaded dogs.[43]
No significant calcium transport occurs in the thin loop of Henle. The thick loop of Henle resorbs
approximately 10-30% of the reclaimed calcium, predominately through paracellular diffusion. In this
segment, paracellular diffusion is driven by the lumen positive transepithelial potential. This electrical
gradient is maintained due to the apical Na-K-2Cl cotransporter and the renal outer medullary potassium
channel (ROMK)[45] (see Figure 3). Due to the calcium ion’s positive charge, paracellular movement
out of the lumen is promoted.
Figure 3. The lumen-positive trans-epithelial gradient is driven
by the Na-K-2Cl co-transporter and the ROMK channels. This
promotes paracellular diffusion in the thick loop of Henle.
In the distal tubule and collecting duct, calcium resorption is primarily by a transcellular route. There is
some variation in the intracellular binding proteins that assist with transcellular movement. Parvalbumin
is the predominate intracytoplasmic binding protein in the early distal tubule, while calbindin-D28k is the
predominate transporter in the late distal tubule and connecting tubule, although Calbindin-D9k is also
expressed[46],[47]. This is different from transcellular intestinal transport described above; calbindin-
D9K is the only calbindin that is expressed in mammalian intestinal cells.
Calcium resorption is controlled by several homeostatic mechanisms. The requirement to adjust calcium
movement in response to demand is primarily met by adjusting the transcellular movement in the distal
nephron, although resorption in other parts can also be adjusted. PTH acts directly on the thick

6
ascending loop of Henle, distal tubule and collecting tubule to cause up-regulation of the calcium channel
TRPV 5 and increased expression of calcium binding proteins.[48]
Calcitriol increases calcium resorption, although not to the same extent as PTH. Increased calcitriol
concentrations increase expression of calbindin-D9K in the proximal tubule, loop of Henle and the distal
tubule epithelial cells.[49] Calcitriol does not change calbindin–D28k expression as this protein appears
to be vitamin D independent.[50] Calcitriol also has a weak action on increasing paracellular calcium
movement.
The thick loop of Henle has calcium sensing receptors (CaSR) in the basolateral membrane, allowing
local autocrine control. Increased activation of CaSR, for example by hypercalcemia, cause inhibition of
the TRPV5 channel on the luminal membrane and reduces transcellular resorption. CaSR also inhibit
activity of the Na-K-2Cl co-transporter and the ROMK channel, which dissipates the transepithelial
gradient driving paracellular transport.[51]
A:2.1: Drugs and diseases affecting calciuresis:
There are various drugs that incude calciuresis by inhibition of the Na-K-2Cl cotransporter, although the
physiology of the resulting calciuresis depends upon which segment of the nephron is affected.
Furosemide inhibits the Na-K-2Cl cotransporter in the thick loop of Henle. This leads to a loss of the
transluminal voltage gradient, without which there is no driving force for paracellular calcium
resorption.[52] This results in hypercalciuresis. Thiazide diuretics, such as hydrochlorothiazide, inhibit
the Na-K-2Cl cotransporter in the distal nephron. This diuretic effect in the distal tubule results in a
decreased extracellular volume. This prompts increased passive resorption of sodium through
upregulation of the sodium-hydrogen exchanger in the proximal nephron. As a result passive solute drag
is increased, resulting in increased calcium resorption.[53, 54]
Primary hyperaldosteronism causes hypercalciuria and is described as a risk factor for calcium
nephrolithiasis in humans.[55] The volume expansion from primary hyperaldosteronism decreases
sodium resorption in the proximal tubule and hence reduced calcium resorption occurs.
Hyperadrenocorticism is another disease which induces hypercalciuria[56] and is also a risk factor for the
formation of canine calcium oxalate urolithiasis.[57] The proposed mechanism is excessive cortisol
acting as a ligand for the mineralocorticoid receptor.[58] Activation of mineralocorticoid receptors cause
fluid retention and hypercalciuresis by the same aldosterone-mediated mechanism mentioned above. The
mineralocorticoid receptor in the distal tubule is also activated if local cortisol is not effectively
metabolized to cortisone.[59] This can occur due to a deficiency in 11b-hydroxysteroid dehydrogenase,
an inherited human condition named “apparent mineralocorticoid excess” or pseudohyperaldosteronism.
As result of hypercalciuresis, nephrocalcinosis is a common feature of this disease.[60]
A similar mechanism can be induced by some exogenous glucocorticoids. Corticosterone and
dexamethasone were also demonstrated to also activate mineralocorticoid receptors to varying degrees in
the canine brain.[61]
Bisphosphonates are used to alter calciuresis. Traditionally used to inhibit bone resorption for treatment
of osteoporosis, they are now being suggested for use in human patients with idiopathic hypercalciuria to
decrease mobilization of skeletal calcium, and subsequent excretion.[62]

7
Diseases causing calciuresis were first classified by Pak et al [63] based on the different predominant
underlying mechanism: absorptive hypercalciurias, resorptive hypercalciurias and renal hypercalciuras.
Absorptive hypercalciurias are due to hyperabsorption from the gastrointestinal system. In humans
absorptive hypercalciuric conditions are sometimes diagnosed by an oral calcium-loading test which
results in a great increase in urinary calcium. This type of hypercalciuria can be resolved with a low
calcium diet. A disease model of this is mice with overexpression of TRPV-6 gene developing
calciuresis.[64] Exogenous vitamin D excess or diseases causing increased endogenous calcitriol
production also result in enhanced gastrointestinal absorption. These diseases appear to be only described
in human medicine and include granulomatous disease, most notably sarcoidosis.[65] Other diseases
include infectious granulomatous disease such as histoplasmosis[66], coccidomycosis[67] and
bartonellosis[68]. Possibly granulomatous disease in animals which results in overproduction of calcitriol
may cause a similar response.
Resorptive hypercalciuria refers to conditions that stimulate increased bone resorption.
Hyperparathyroidism is the most common example of this. Hyperparathyroidism causes hypercalcemia
which results in hypercalciuria; if there is increased calcium in the serum this will translate into increased
calcium in the ultrafiltrate. Despite the direct effect of PTH on the distal tubules in upregulating calcium
resorption, hypercalciuria overwhelms the capacity for tubular resorption. The clinical result of
hypercalciuresis from hyperparathyroidism is demonstrated in a retrospective evaluation of canine
hyperparathyroid patients, 65/210 hyperparathyroid dogs had concurrent calcium based urolithiasis.[69]
Further evidence for this causal relationship is seen in post-parathyroidectomy human patients who have
resolution of the calciuresis and associated decreased likelihood of calcium nephrolithiasis after surgery.
[70]
Renal hypercalciuria is also known as renal leak hypercalciuria or diet-independent hypercalciuria.
Patients with primary renal hypercalciuria always have high urinary calcium, regardless of fasting state or
diet. Therefore, only a moderate increase in urinary calcium occurs with the calcium-loading test. A
variety of conditions affect the ability of the tubules to resorb calcium. Two conditions discussed earlier,
hyperadrenocorticism and hyperaldosteronism, are examples of renal hypercalciuria affecting veterinary
patients.
There are several additional examples of renal hypercalciuric which have been described in people, but
not in dogs. Some of the various forms of Bartter syndrome result in renal hypercalciuria. Bartter
syndrome type 1 is a genetic m
utation in the SLC12A1 gene, which causes dysfunction of the Na-K-2Cl cotransporter on the basolateral
membrane of the thick ascending loop of Henle. This causes loss of the transluminal electrochemical
gradient that is responsible for driving sodium, water and electrolyte resorption similar to furosemide’s
mechanism of action. Marked hypercalciuria, due to the loss of paracellular solute drag, generally results
in medullary nephrocalcinosis in the first few months of life.[71]
Another genetic disease is “familial hypomagnesemia with hypercalciuria and nephrocalcinosis”
(FHHNC). This mutation results in defective expression of claudins 16 and 19, which prevents
development of cation-selective paracellular channels and removes the transepithelial gradient required
for paracellular calcium resorption.[44]

8
In patients with primary renal hypercalciuria and unidentified underlying cause, the hypercalciuria is
referred to as idiopathic. This is thought to have both a genetic and environmental cause due to over-
representation in certain ethnicities and geographic areas such as amongst the Italian population.[72]
Bataille et al[73] investigated 42 hypercalciuric stone forming human patients and only identified one
with primary renal hypercalciuria. It could be suggested that primary bone resorption is more common
cause of hypercalciuria in people compared with renal hypercalciuria, but this hypothesis is limited by the
small sample size. No similar data is available in dogs. With the exception of dogs with hypercalcemia
or hyperadrenocorticism, the underlying cause of canine urolithiasis is usually not identified.

9
SECTION B: KINETICS OF CALCIUM OXALATE CRYSTAL FORMATION AND GROWTH
The precipitation of crystals and formation of uroliths depends upon urinary concentration of calcium
oxalate and other relevant mediators.
1. Urine supersaturation
Relative supersaturation (RSS) is widely used as an assessment of risk of a specific stone formation.
Briefly, the concentrations of calculogenic substances calcium, magnesium, sodium, potassium,
ammonium, phosphate, oxalate, citrate, sulfate, uric acid and chloride are required, and calculations are
made regarding the possible complexes that can be formed. The scale is adjusted so an RSS of 1 is equal
to a concentration at which the salt is just soluble. Hence an RSS < 1 is termed undersaturated and an
RSS >1 is said to be supersaturated. A supersaturated solution can be said to be in a precipitation or
nucleation zone when precipitation or amorphous aggregation occurs. Alternatively a supersaturated
solution may be in a metastable state, when spontaneous precipitation does not occur.
Relative supersaturation was found to be significantly higher in 17 dogs with CaOx urolithiasis when
compared to 17 control dogs.[74] The change in RSS is often used as a marker to assess the effectiveness
of intervention measures designed to reduce calcium excretion or urine supersaturation in healthy dogs.
For example, feeding healthy beagles a sodium chloride supplement, in addition to a maintenance urinary
diet, significantly decreased their urine oxalate concentration and the relative urine supersaturation.[75]
The main advantage of using RSS to estimate stone formation risk is that the measurement is rapidly
available to researchers. Measuring clinical stone formation would take years of research and be far more
cost and labor intensive.
However, there are a number of limitations in extrapolating RSS to clinical calcium oxalate (CaOx) stone
formation risk. First, RSS does not account for all components involved in urolith formation. Many
other proteins that are not included in the RSS have also been identified in CaOx uroliths. One study of
human CaOx identified 68 other proteins, including inflammatory proteins such as immunoglobulins,
complement C3a and fibrinogen were involved.[76] Second, urolith formation is influenced by more than
simple urinary mineral concentration. Other properties of urine account for the existence of a metastable
state in which the urine can hold large amounts of solutes beyond saturation level. These properties that
inhibit urolith growth will be discussed below. Third, RSS does not take into account the environment in
which CaOx uroliths may be initiated. RSS measurement is that it is typically measured on urine from a
voided sample or collected directly from the bladder. This measurement does not represent the RSS of
the ultrafiltrate in the kidney, where the initial crystallization may form.[77] Furthermore, RSS of the
ultrafiltrate varies at different sites in the nephron, due to the changing concentrations of calculogenic
substances and water.[78] If RSS in the loop of Henle causes nucleation, then this precipitation may be
responsible for further growth, regardless of the final urine RSS. Although occasional micropuncture
studies[78] overcome this limitation, the majority of studies reporting changes to RSS are possibly an
oversimplification of a more complex process.
2. Promotors and inhibitors of crystallization, aggregation and growth
Stone development is a multi-step process. In humans, this is described as (a) nucleation, (b) aggregation
and growth of crystal formation, (c) cell-crystal interaction with movement into the interstitium, (d)
crystal retention and attachment.[79]

10
In human kidneys, it is accepted that calcium oxalate crystal aggregation often occurs secondary to
formation of a nucleus of Randall’s plaque. Randall’s plaques are mineral depositions in the renal papilla,
which serve as a nidus for further crystal formation. They are divided into type I and type II by the
histological location of calcium accumulation along the nephron. Type I Randell’s plaques appear to be
more common, occur in human idiopathic-calcium-stone formers, and are likely related to
hypercalciuria.[80, 81] This process starts with calcium phosphate deposits at the basement membrane in
the thin loop of Henle. It is suggested this might occur due to increased post prandial calcium absorption
at the thick loop of Henle, which is then carried down the medulla by the vasa recta.[80] Alternatively
there may be defective calcium resorption in the proximal tubule, when results in an increased luminal
calcium load being delivered to the thick loop of Henle.[82] Regardless of the origin of the calcium, the
plaque accumulates in the interstitium, eventually penetrating the epithelium or becoming exposed when
there is other urothelial damage. It has been hypothesized that oxidative epithelial damage from
inflammatory mediators in metabolic syndrome may be responsible.[83, 84] Interestingly, calcium
oxalate nephrolithiasis is associated with metabolic syndrome, high triglyceride and high cholesterol
concentrations.[85] This leads to speculation that familial hypertriglyceridemia of Miniature Schnauzers
may have a role to play in renal tubule damage and canine nephrolith pathogensis.
Once the epithelium is eroded, the exposed calcium deposits culminates in crystal aggregation and stone
attachment at the renal papillae.[77, 80] From here there is further growth into nephroliths or inhibition
of crystal formation depending on urine constituents or the “urinary milieu” as further discussed below.
There are variations in distributions of Randall’s plaques. Type II plaques cause calcium deposits inside
the tubule lumen of collecting ducts, also known at ducts of Bellini, in obese patients receiving intestinal
bypass.[80] This type of plaque does not appear to be associated with hypercalciuria[80], so is perhaps
unlikely to be a useful model for hypercalciuric miniature schnauzers.
Urocystoliths occur rarely in humans compared to dogs. The above process of human nephrolith
formation is extrapolated to canine urolith formation, although there are inherent limitations based on the
current available literature. First, it has not been established if Randell’s plaques are involved in the
pathogenesis of canine nephroliths. Therefore, the same nucleation, aggregation, retention, attachment
model may not apply. Second, factors causing the growth of nephroliths have been extrapolated to factors
which cause clinical disease in dogs, which predominately involves urocystoliths. Although it is possible
there are differences in growth of urocystoliths compared to nephroliths, the basic concepts of urolith
growth and aggregation will be discussed.
B: 2.1 Promotors
A promotor is a substance or an environment that makes crystal formation and/or growth more likely.
Chemicals other than calcium and oxalate can promote CaOx crystal formation by increasing RSS. In
vitro addition of sodium urate [86] and cystine [87] to human urine have been shown to promote
crystallization of calcium oxalate. Although the mechanism was once considered to be due to epitaxy (a
crystalline overlayer on a crystalline substrate with a similar orientation[88]) this theory has now been
largely disproven.[87, 89] Rather, urate and cysteine action is referred to “salting out” CaOx due to
increasing RSS to a supersaturated state.[87, 89]

11
Another chemical group which can act as a promotor is calcium salts. Calcium carbonate crystals act as
promotors of calcium oxalate growth by providing a nidus for lithogenesis.[90] Further growth is
promoted by epitaxy.[90] Calcium phosphate can also act as a nidus promoting calcium oxalate growth.
A rather extreme example is a case report of ectopic bone (calcium phosphate) formation in a feline
bladder, promoting CaOx urolithiasis.[91]
Acidic urine can be a promoter of crystalline growth. This occurs by two mechanisms. First, the
solubility of calcium oxalate decreases in slightly acidic solutions. In one veterinary study, the calcium
oxalate saturation of feline urine was lower when the urine pH was above 7.2 and higher when the urine
pH was below 6.5.[92] Second, acidic urine reduces the effectiveness of both organic and inorganic
inhibitors. In human studies, research shows macromolecule inhibitors (discussed below) are less
effective in acidic conditions than at neutral or alkaline pH.[93] In addition, acidic pH increases
resorption of citrate in the proximal tubule so there is less available to form complexes with calcium.[94,
95]
B: 2.2 Inhibitors
Inhibitors are polyanionic substances that retard the development and/or growth of calcium salt crystals.
They can be inorganic or organic substances. The inorganic fraction is composed predominately of
crystalloid complexors. Organic inhibitory compounds include urinary macromolecules, crystal surface
binding substances, and components of non-crystalline stone matrix.
B: 2.2.1: Inorganic inhibitors: crystalloid complexors
Inorganic cations and anions inhibit stone formation by crystalloid complexing. Cations (primarily
magnesium) bind to oxalate and anions (mainly citrate and pyrophosphate) bind to calcium. This reduces
the urinary concentration of free calculogenic ions. This may result in an increase in the metastable limit
as was demonstrated with pyrophosphate.[96]
Citrate is sometimes referred to as a crystalloid complexor, as it forms complexes with calcium.
However, the relevant calcium chelation occurs in the gastrointestinal tract and in circulation. The main
action of urinary citrate is now thought to be direct inhibitory action on the calcium oxalate crystal
surface, rather than chelating urinary calcium.[97] Urinary citrate was demonstrated to have some
importance in inhibiting stone formation as one study has identified hypocitraturia in >50% of human
nephrolithiasis patients.[98]
B: 2.2.2: Organic inhibitors: Urinary Macromolecules and Crystal Surface Binding Substances.
Organic inhibitors include urinary macromolecules which bind to the crystal surface and the organic
matrix within the crystal. Some substances may occur both dissolved in urine and within the matrix.
Urinary macromolecule inhibitors are glycoproteins that covering the crystal surface and act as a biofilm.
The hydrophilic portion attaches to the crystal, and exposes the hydrophobic portion to surrounding urine
or ultrafiltrate. The altered hydrophobic crystal surface has only a weak electrical charge and is therefore
not an attractive binding site for urinary ions.
Nephrocalcin is an inhibitory urinary macromolecule that may have a role in protection against
urolithiasis. This glycoprotein is observed in different forms in urine of humans with and without a

12
history of CaOx urolithiasis. Nephrocalcin type A and B are strong inhibitors of crystalline growth.
Reduced quantities of these were found in some stone forming humans [99] and possibly in dogs.[100]
Rather, affected patients had greater concentrations of nephrocalcin type C and D, which act as only weak
inhibitors.
Other macromolecules include other protoglycans such as Tamm-Horsfall protein (THP) and bikunin, and
urinary prothrombin fragment 1.
Further proof of the importance of inhibitors is demonstrated by knockout mice models of two other
glycoprotein inhibitors; ostoeopontin and THP.[101] Knockout mice without ostoeopontin, TPH or
without either of these can be induced to form CaOx crystalluria when hyperoxaluria was induced. The
wild type mice with normal concentrations of ostoeopontin and THP did not form these crystals.[101]
B: 2.2.3: Organic inhibitors: the soluble stone matrix
In addition to the crystalline components of a urolith, a lattice of organic material, called the matrix, is
present. This organic matrix is difficult to quantify, as it is destroyed by quantitive stone analysis
laboratory techniques. The matrix arises from urine constituents – both those present in urine at the
beginning of stone formation and those produced by trauma from irritation and inflammation during stone
aggregation and growth. In healthy humans, heparin sulfate, the key GAG component, strongly inhibits
crystal aggregation and growth.[102] However, the role of heparin sulfate in canine urolithiasis has not
been evaluated.

13
SECTION C: CLINICAL CALCIUM OXALATE UROLITHIASIS IN DOGS
1. Introduction
CaOx urolithiasis may result in clinical disease such as infection, urinary obstruction or pain in dogs. The
consequences of urolithiasis depend, in part, upon the location within the urinary system affected. Certain
breeds have a strong predisposition to CaOx urolithiasis, which can lead to further studies into the
underlying cause. The popularity of these predisposed breeds with the American public makes research
into the pathogenesis of CaOx urolithiasis an important priority.
Laboratory submissions of CaOx uroliths removed from dogs have been increasing in frequency. In the
first year of operation in 1981, the Minnosota Urolith Center reported only 5% of canine uroliths were
CaOx based.[103] This is compared to canine urolith submissions analyzed during 2007, of which 41%
were CaOx.[103] A similar distribution and trend was noted at the Urinary Stone Analysis Laboratory
based in Davis, California.[104] A contributing factor is suspected to be a decline in struvite
submissions. One relevant point to note is that this data represents stones submitted for analysis, not the
incidence of clinical disease. The recommended treatment for suspected struvite stones is now
dissolution with dietary and anti-microbial treatments, rather than stone retrieval methods, so a decrease
in struvite uroliths submitted for analysis is expected.
2. Predisposing factors
Causal risk factors for CaOx urolithiasis are largely unknown. Epidemiological studies have identified
various dog factors listed below which are associated with an increased odds ratio of disease. However,
the mechanism or pathogenesis has not been identified. These factors do not induce disease in all dogs,
and correcting them has not been demonstrated to reverse the increased risk of disease or recurrence.
A potential limitation of a discussion on risk factors is that multiple epidemiological studies use data from
Minnesota Urolith Center, sometimes reporting from the same or overlapping time periods. This can lead
to overrepresentation of the data in the literature.
2.1. Urine factors
2.1.1. Calcium and oxalate concentration: Hypercalciuresis is a risk factors for canine calcium
oxalate urolithiasis.[105, 106] Unlike urine calcium, urinary oxalate concentration is not
considered of primary importance for calcium oxalate stone formation in dogs.[105-107]
2.1.2. Other urine constituents: Dogs with abnormal concentration of any of the crystalline
inhibitors or promoters discussed in Section B are at increased risk for calcium oxalate
urolithiasis.
2.2. Patient factors
2.2.1. Gender: An increased risk for male dogs was identified in some studies. [104, 108-110] It
is possible that calcium oxalate urolithiasis is identified more commonly in male dogs
because they more frequently develop urethral obstruction. Another suggested reason is an
estrogen-dependent increase in urinary citrate, resulting in a decrease in urinary calcium and
oxalate. This has been demonstrated in human studies involving estrogen supplementation.
[111] However the majority of female dogs which received veterinary care (and hence may
have urolithiasis diagnosed) are spayed, with little estrogen production so this mechanism
may not be as significant in veterinary patients.

14
2.2.2. Breed: Certain breeds are significantly over-represented and summarized in the table below.
It has been suggested that some breeds may have idiopathic hypercalciuresis.[106]
Breed Odds Ratio (OR)
Standard Schnauzer 18.1[109]
Miniature Schnauzer 14.1[109]- 21.6[104]
Lhasa Apso 10.1[104]-10.9[109]
Jack Russell Terrier 9.9[109]
Papillion 9.9[109]
Bichon Frise 6.6[109]-23.6[104]
Yorkshire Terrier 6.5[104]
Keeshond 4.6[104]5.5[109]
Pomeranian 4.9[109]-7.2[104]
Samoyed 4.6[109]
Shih Zhu 4.5[109]- 10.2[104]
Chihuahua 3.9[109]
Cairn Terrier 3.7[109]-7.3[104]
Maltese 3.5[109]-5.2[104]
Miniature and Toy Poodles 3.3[109]
West Highland White Terrier 3.3[109]
Dachshund 2.7[109]
Dogs of non-urolith forming breeds, such as retrievers, greyhounds and Pitbulls, have been found
to have significantly greater colonization of Oxalobacter formigenes when compared to urolith-
forming dogs[37]. This suggests that it may be one breed-associated patient-related risk factor.
There are likely to be many other breed-related differences which have not yet been identified.
2.2.3. Age: Dogs over 4 years of age are at least 5 times more likely to form calcium oxalate
uroliths.[109] The mean age of dogs at first time stone removal was 8 years with a standard
deviation of 3 years.[108]
2.2.4. Body Condition Score: It has been suggested that obesity is associated with calcium oxalate
stone formation and/or calcium oxalate crystalluria[112], however the causal relationship
has not been proven. It has been hypothesized that obesity is likely to cause urine
acidification, however no difference in urine pH was observed between groups in the
aforementioned study.
2.2.5. Body Size: Smaller breed size is associated with corresponding increased risk of
disease[110]. One hypothesis for this increased risk is small breed dogs have a greater
surface area and have a higher energy requirement per kilogram body weight. A higher
energy requirement will translate into greater mineral intake if the diet is kept constant.
However canine athletes, such as sled dogs, who have a significantly greater calorie
requirement do not have a higher prevalence of CaOx urolithiasis, so this hypothesis is
uncertain.
2.2.6. Concurrent disease: Diseases which cause hypercalciuresis were discussed in Section A,
and these increase the patient’s risk. The two most significant diseases are likely to be
hyperadrenocorticism which increases the odds ratio by a factor of 10 [57] and primary
hyperparathyroidism.

15
3. Diagnosis and treatment
Calcium oxalate uroliths are visible on radiographs as smooth or spiky, radio-opaque, mineral dense
structures. Typically they appear as many small round stones with a diameter approximately 2-
7mm.[113] Although 2mm is often considered the smallest size calculi that are radiographically
detectable, one paper found calcium oxalate urocystoliths 1mm and smaller were only missed on 2-5% of
survery films using a simulated bladder model.[114] These characteristics can be used to help identify
CaOx uroliths from uroliths of other types. Contrast radiography tends to be less useful for CaOx
detection as calcium based urocystoliths tend to be isopaque to iodinated contrast.[114]
Ultrasound can also be used to identify uroliths. Ultrasonography was found to be superior to radiography
in detecting small human nephroliths[115], and it could be speculated that the same is true for either
canine nephroliths and possibly canine cystoliths. On a phantom bladder model with 7.5MHz transducer,
ultrasonographic assessment was slightly superior to survery radiographs, with an average sensitivity of
~97% considering all uroliths types and sizes, including <1mm.[114] Limitations of ultrasonography is
that it consistently overestimated the size of nephroliths and had low specificity.[116] These restrictions
may or may not apply to canine cystoliths. The frequency of the transducer will affect the sensitivity of
detection.[114]
The use of computer tomography to detect urolithiasis presence and identify stone type has been
uncommonly described in dogs.[117] Although this has high accuracy for identifying calcium oxalate
type stones in 93-96% simulated models, the additional cost, sedation and radiation exposure may not be
justified in the majority of dogs.
Once uroliths are observed, identification of any of the above risk factors (signalment, urine pH, calcium
oxalate crystalluria, concurrent predisposing disease or medications) can be useful to predict calcium
oxalate urolith composition. Mineral type could be predicted in approximately 70% of urocystoliths
using an algorithm based on signalment alone.[113] Ultimately, calcium oxalate urolithiasis is confirmed
by submission of a urolith for quantitative mineral analysis.
Treatment for calcium oxalate urolithiasis is removal by surgery or minimally invasive methods.
Indications for removal are the presence of clinical signs or dysfunction related to urolithiasis. In
addition, urocystoliths that are small enough to fit into the urethra and judged at risk of causing future
lower urinary tract obstruction are also good candidates for removal. These signs or dysfunction may
present as stranguria, pollakiuria or urinary obstruction from urocystoliths, urethroliths and/or
ureteroliths. Upper urinary calculi are generally asymptomatic. However they occasionally may result in
pain and/or renal dysfunction from outflow obstruction, which then warrants their removal.
In general, nephroliths are not routinely removed. The majority of the time their presence appears to be
of little clinical consequences and dogs are generally asymptomatic. ACVIM recommendations suggest
only considering removal if there are clinical signs such as urinary obstruction, persistent infection or
pain. Minimally invasive options include breakdown by extracorporal shock wave lithotripsy or
percutaneous nephrolithotomy. Other more invasive options for removal are pyelotomy or
nephrectomy.[118]
Methods for urocystolith and/or urethrolith removal are summarized below. Patient urethral size, urolith
size and number, and equipment will dictate the methods available.

16
Method Indications Limitations and potential
complications
Natural voiding Suitable for very small stones (1-2mm).
Catheter retrieval Suitable for very small stones as above. Requires the urethral lumen to
accommodate at least an 8Fr
catheter size to be effective.
Voiding
urohydropulsion
Suitable for stones up to 5-7mm
depending on size of urethra[119].
Low but present risk of bladder
rupture with over-distention,
inadequate anesthesia or
preexisting weakness.
Cystoscopic basket
removal
Suitable for very small stones (1-3mm) Suggested size limit of less than
4mm in female dogs and less
than 2-3mm in most male
dogs.[120]
Lithotripsy
Can be combined with cystoscopic basket
removal or voiding hydropulsion to
remove fragments[121].
Lithotripsy may be more time
consuming for male dogs than a
cystotomy, depending on size
and number of stones
present[122]. Risk of bladder
rupture as for voiding
hydropulsion, also damage from
cystoscope or laser fiber[122]
and transient urethral swelling
[121]. Low risk of stones
remaining after procedure
(complete stone removed in 82-
87% of cases[121-123]).
Retrograde
hydropulsion
Relocates urethroliths into the bladder for
removal by cystotomy.
Cystotomy Suitable for any number and all sizes of
stones.
Risks associated with wound
healing.
Incomplete removal of stones in
15-20% of cystotomy
cases.[124]
Percutaneous
Cystolithotomy
Suitable for any number and size of
stones.[125] May allow for more
complete removal of stones.[125]
Table 1: Different methods for calcium oxalate urocystolith and/or urethrolith removal. Based on Bartges
and Polzin, 2011[126]
4. Management and prevention
Unfortunately dogs with CaOx urolithiasis have a high risk of recurrence. One study reported a recurrence
rate of 48% within 3 years.[127] In another, Miniature Schnauzers with a history of CaOx cystoliths had
a 62% rate of recurrence.[128] Strategies to alter the urine composition combined with ongoing
monitoring are recommended. To reduce future formation the American College of Veterinary Internal
Medicine consensus recommendations include decreasing urine concentration, reducing calculogenic
minerals and avoiding urine acidification. Addressing underlying disease which may contribute to
calciuresis and discontinuing medications discussed in Section A are ideal if possible. Monitoring of

17
urine parameters and screening imaging is also recommended, as early intervention allows for less
invasive stone removal methods to be used.
The majority of prevention methods are designed to reduce calciuresis. Various studies have attempted
to assess the efficacy of prevention measures, which is often expressed as reduction in RSS and without
long term follow up data.
4.1. Diet composition Reduction of calculogenic minerals can be achieved by adjusting the
composition of the diet. Therapeutic diets which are restricted in calcium and oxalate have been
shown to reduce CaOx RSS.[129] Although the recommendation for human calcium oxalate
urolithiasis patients is moderate calcium and low oxalate, dogs had the lowest RSS when both
calcium and oxalate were reduced. Furthermore, dogs which were fed a therapeutic diet with
either moderate or a low calculogenic products (calcium, phosphorus and protein) had less
recurrence of calcium oxalate cystic calculi.[130] Lower protein diets were historically
recommended to avoid urine acidification associated with purine metabolites, however the
effectiveness of this is unproven.
4.2. Moisture content: Increasing moisture content of food can increase total water intake in some
dogs. Increased water intake will result in a reduced urine specific gravity and RSS. This has
been demonstrated in healthy Miniature Schnauzer dogs fed either dry kibble (7% moisture) or
soaked in water to achieve 73% moisture content.[131] Even though voluntary water
consumption was not accounted for, the soaked-kibble diet was associated with lower USG
values, indicating dogs from this group had higher total moisture intake. Another alternative is
to increase the sodium content of the food, to promote polydipsia. However, urinary sodium
excretion is linked to calciuresis as discussed above. Up to 1.2g/400kcal or 170-230mg/kg/day
did not significantly increase urine calcium concentration but did reduce RSS. Therefore,
increasing dietary sodium is an alternative for dogs unable to be changed onto a moist diet.[75]
4.3. pH: Urine alkalization may be required to achieve a target pH of 7.0. Strategies for this include
avoiding excessive dietary protein and the addition of potassium citrate if required. A fasted
sample should be used for assessment of pH to avoid recording the transient post-prandial
“alkaline tide”.
4.4. Potassium citrate: Although supplementary citrate alkalizes urine and decreases the CaOx RSS
in humans [94, 132], the result of supplementation on either the pH or CaOx RSS in healthy
dogs is less clear.[133] Potassium citrate is sometimes recommended as a therapy based on a
study that showed it reduced the RSS in some Miniature Schnauzers.[133] There are several
proposed mechanisms why it may have this effect. Firstly, potassium citrate induces a metabolic
alkalosis which induces tubular calcium resorption and lowers urinary calcium (see discussion in
Section B). Secondly, the metabolic alkalosis increases the urinary citrate levels, which chelates
calcium and further reduces urinary calcium (see section B). Thirdly, increased the urinary pH
increases the strength of calcium-phosphate binding and activation of other inhibitors such as
pyrophosphate (see section B). Despite these theories, human studies fail to consistently find
reduced calcium excretion with potassium citrate supplementation. It appears that we currently
do not have enough information to make a strong recommendation that potassium citrate will

18
lower stone risk. Measuring the benefit to the patient (ie reduction in calciuresis and pH after
starting therapy) may assist with making individual treatment recommendations.
4.5. Thiazide diuretics: In humans, hydrochlorothiazide has been shown to decrease calciuresis[134]
and decrease episodes of calcium oxalate urolithialsis.[135] This medication is routinely used to
treat humans with idiopathic hypercalciuria. Veterinary research shows dogs with a history of
calcium oxalate urolithiasis have decreased urine calcium excretion when treated with
hydrocholothiazide.[136] However research demonstrating reduced urolithaisis recurrence is
lacking. Chlorthalidone has also been shown to reduce calculous recurrence in people[137],
however this medication is not used routinely in dogs.
Calcium oxalate urolith prevention strategies are largely unproven; supportive veterinary literature is
minimal or absent. Most interventions are based on reduction of stone disease in humans or a reduction
of RSS. We must extrapolate this to canine patients and assume RSS closely correlates with clinical
disease. However as discussed above there are many additional elements apart from RSS that play a part
in CaOx formation, including factors which we do not yet understand. In vivo prospective studies are
vitally needed to improve our ability to help dogs with this condition.

19
CHAPTER TWO
SECTION A: INTRODUCTION
Calcium oxalate (CaOx) urolithiasis can be detected in approximately 24% of older, healthy dogs of high-
risk breeds such as the Miniature Schnauzer. Recurrence occurs in 48% of cases within 3 years[127] and
may be due to a limited understanding of CaOx pathogenesis. Identifying a marker of the disease is the
first step to better assess the risk of disease or recurrence.
Urine composition from dogs with CaOx urolithiasis differs from healthy dogs. Relative supersaturation
(RSS) [74] and increased urine calcium concentration[74, 105, 106] appear to be the most consistent
differences. Of these two, measurement of urinary calcium concentration is more cost-effective and
readily available. Although urine calcium excretion (calciuresis) has traditionally been measured by
performing 24 hour urine collection, the convenience can be improved by performing a spot
measurement. To account for variations in glomerular filtration rates throughout the day, urine calcium
concentration can be indexed to concurrent urine creatinine concentration (UCa/Cr). In children, the
UCa/Cr correlates moderately well to 24 hour urinary calcium measurements.[138] Therefore, UCa/Cr
has the potential to be an attractive alternative for measuring calciuresis in dogs.
Although there is no accepted reference range for the UCa/Cr, a recent study showed a significant
difference between fasted control and fasted urolith-forming dogs.[106] Therefore, one of the goals is to
assess the UCa/Cr as a diagnostic tool to identify stone status, and determine the most accurate threshold
for healthy dogs.
Furthermore, previous data also shows that six urolith-forming dogs had abnormally increased post-
prandial calciuresis.[105] A better understanding of variation in calciuresis in regards to fasted and post-
prandial states could improve the specificity of using the UCa/Cr measurement to differentiate between
healthy and stone-forming dogs. We hypothesized that post-prandial urine calcium excretion kinetics
differ between urolith-forming and non-urolith-forming dogs, and these differences could improve the
discriminatory power of the UC/Cr.
There are a variety of other patient variables that affect renal excretion of calcium, including sex, breed,
diet, concurrent diseases and medications.[109] Any attempt to investigate the effect of postprandial
calciuresis should attempt to control for these as much as possible.
Male miniature schnauzers have the highest incidence of CaOx urolithiasis[108], therefore this
population was selected for inclusion. We wanted to avoid classifying dogs with CaOx nephroliths as
healthy controls, due to the strong association between human CaOx nephrolithiasis and hypercalciuria.
Therefore, the inclusion criteria for urolith-former was expanded to include all forms of urolithiasis
including nephroliths, urocystoliths or both.
The aims of this study were firstly to quantify differences in fasted and postprandial UCa/Cr between
urolith-forming and control Miniature Schnauzers. The second aim was to compare the UCa/Cr in the
postprandial period to a fasted baseline in both urolith-forming and control miniature schnauzers. Finally

20
we investigated if the post-prandial change is significantly different between stone-forming and control
dogs.
SECTION B: MATERIALS AND METHODS
Case selection
The study was advertised to clients of the Veterinary Teaching Hospital (VTH)at the Virginia-Maryland
College of Veterinary Medicine and to the local community. The proposed experimental protocol was
reviewed and approved by the Institutional Animal Care and Use Committee (IACUC) of Virginia Tech.
Inclusion criteria were adult (> 24 months of age), male (either neutered or intact), Miniature Schnauzer
dogs. Dogs with diseases which alter calcium excretion (e.g. hypercalcemia, hyperparathyroidism, renal
disease, diabetes mellitus, osteolytic disease, granulomatous disease and hyperadrenocorticism) were
excluded. To identify concurrent disease, the medical history was reviewed, in addition to performing a
physical exam, biochemistry profile, urinalysis, abdominal radiography and urinary tract ultrasonography.
Dogs were excluded if they were not consuming a complete and balanced commercial canine adult
maintenance food substantiated per Association of American Feed Control Officials (AAFCO) nutrient
profiles or feed test. Specifically, dogs were excluded if they were consuming a prescription urinary diet
which would be designed to alter urine constituents. A detailed diet history was collected and reviewed
by a board certified nutritionist. Dogs currently receiving medications which are known to alter calcium
excretion (glucocorticoids, furosemide, thiazide diuretics, levothyroxine, theophylline or potassium
citrate) were also excluded. Dogs were prospectively enrolled with informed owner consent. Therefore,
the study population was based on a convenience sample; all dogs that met the inclusion criteria without
any of the exclusion factors were enrolled.
Dogs were classified into two groups based on client history, medical records review and results of
abdominal radiography and urinary tract ultrasonography (kidney, ureter, bladder) performed by the
investigators. The groups were: 1) “Urolith-former” dogs being those with previously removed or
currently present calcium oxalate uroliths anywhere in their urinary system, or 2) breed-matched
“controls” with no history or current presence of uroliths.
If urolithiasis was identified through either diagnostic imaging or the medical history, the following
criteria were then applied to determine if it was reasonable to conclude that uroliths were composed of
calcium oxalate. The criteria were either: 1) confirmatory calcium oxalate urolith analysis, or 2) had
neutral or acidic urine with lack of evidence of bacterial urinary tract infection, hepatic disease, or
crystalluria of any type other than CaOx. Dogs concluded to have other types of uroliths were excluded
from the study.
Study procedures
Dogs presented to the VTH the afternoon before sample collection. The Daily Energy Requirement
(DER) was calculated using the equation 1.6 X 70 X BW0.75 where BW is the current body weight in
kilograms. All dogs were fed a standardized diet to meet the DER, divided into an evening and morning
meal, 12 hours apart. Dogs had to eat at least half the prescribed meal, either voluntarily or by syringe
feeding. Dogs urinated 3-5 hours after the evening meal, which reduced the likelihood of post-prandial
evening urine contributing significantly to the fasted morning sample. The following morning, an initial

21
urine sample was collected prior to feeding (“fasted baseline”). After the fasted baseline was collected,
dogs were fed their morning meal. Urine was collected at four post-prandial time points (referred to as the
1, 2, 4 and 8 hour post-prandial samples).
Urine was collected by free catch whenever possible, but if dogs did not voluntarily urinate, a sample was
collected by aseptic urinary catheterization or cystocentesis, whichever was least stressful for individual
dogs.
Laboratory measurements
Initial fasted blood and urine samples were submitted immediately upon collection to the VITALS
Laboratory of the VMCVM for a biochemistry profile and a urinalysis. If the urine dipstick detected 2+
or higher proteinuria, then an SSA bumin test was performed. If this was also positive then a urine
protein:creatinine ratio was calculated. If the serum total calcium was outside the laboratory reference
range, then an ionized calcium measurement was performed.
The fasted and post-prandial urine samples were submitted immediately for calcium and creatinine
measurements. Urine calcium and creatinine concentrations were measured by spectroscopy on all five
samples using a Beckman Coulter AU 480 anlayzer, by the calcium sensitive Arsenazo dye and the
modified Jaffe procedures, respectively.
Statistical analysis
The primary outcome was UCa/Cr while the primary exposure of interest was urolith status (urolith-
former vs control). Several potentially confounding variables including age, body condition, and
proteinuria were selected for further analysis. This was based on previously published associations with
CaOx formation.[106, 109, 112] Furthermore, because an association between dyslipidemias and
proteinuria in Miniature Schnauzers has been described[139], the effects of serum triglycerides and serum
cholesterol were also investigated. A initial tentative UCa/Cr reference range for Miniature Schnauzer
dogs was extrapolated from previous published literature.[106] This was based on the UCa/Cr
interquartile range from miniature schnauzers with no history of urolithiasis, and yielded 0.05 as the
upper limit of normal.
To assess for postprandial change, firstly a ∆UCa/Cr was calculated for each dog at each time point using
[UCa/Crx] – [UCa/Cr0], where UCa/Cr0 is the fasted baseline of the individual dog, and x refers to the
specific postprandial timepoint. Secondly the % ∆UCa/Cr was calculated using
([∆UCa/Cr]/[UCa/Cr0])*100.
Normal probability plots showed that UCa/Cr, ∆UCa/Cr, %∆UCa/Cr, age, and serum cholestrerol levels
followed a normal distribution while body condition score and serum triglycerides level were skewed.
Normally distributed variables were summarized as means (standard deviation) and skewed variables as
medians (range). Categorical variables were summarized as contingency tables. Associations between
urolith status and potential confounders were assessed using 2-sample t-tests (age and cholesterol),
Wilcoxon rank sum test (body condition score and triglycerides) and Fisher’s exact test (presence of
proteinuria, presence of hypercalciuresis). A mixed model ANOVA was used to assess the impact of
urolith status (urolith-former vs control) and time (fasted vs 1, 2, 4, 8hr post prandial) on the UCa/Cr,
∆UCa/Cr, and %∆UCa/Cr (separately). Each model also specified dog identification as a random effect,

22
and residuals were inspected to verify that the errors were normally distributed with a mean of zero and a
constant variance. Age, proteinuria, cholesterol, triglycerides were added to each of the models mixed
model ANOVA models but none reached statistical significance (data not shown). Statistical significance
was said to be p<0.05. All analyses were performed using SAS 9.4 (Cary, NC, USA).
ROC analysis was performed to determine the most appropriate threshold for using the UCa/Cr to identify
CaOx urolithiasis in male Miniature Schnauzers. The mean UCa/Cr for each dog was calculated. In
addition, we utilized UCa/Cr data from male miniature schnauzers from a previously published paper
[106]. A receiver operator curve was constructed using JMP to determining the ideal UCa/Cr cut-off
value with yields maximum sensitivity and specificity for differentiating stone-formers from control dogs.
SECTION C: RESULTS
Twenty-four Miniature Schnauzers were enrolled; nine urolith-fomers and fifteen healthy controls. The
urolith-formers comprised of two dogs with nephroliths only, one dog with urocystoliths only, and six
dogs with nephroliths plus either current or previous urocystoliths. Comparative data for the two groups
of dogs are seen in Table 1. Dogs had a mean age of 8 years, with a range from 2-12 years of age. The
urolith-formers were older, although this did not reach significance. Dogs were predominately neutered,
with the exception of two intact males in the control group. Both groups had a similar body weight and
body condition score (mean of 5.6/9). Proteinuria, as detected by SSA Bumin test, was identified in 20%
of control dogs and 44% of urolith-formers, although this did not reach statistical significance. Mean
protein:creatinine ratio was numerically higher in the urolith formers; however significance was not
achieved. Serum cholesterol and triglyceride concentrations were both significantly greater within the
urolith-formers compared with the controls.
Across all 120 urine samples collected, the urolith-formers had significantly higher UCa/Cr compared to
controls. Furthermore, urolith-formers had greater UCa/Cr, compared to controls, at 1 and 8 hours
postprandial (refer to Figure 1). Individual UCa/Cr values are illustrated in Appendix 1.
A significant postprandial effect on UCa/Cr was not appreciated in either group. The ∆UCa/Cr at 1 hour,
2 hours, 4 hours and 8 hours postprandial were not significantly different from zero, and the ∆UCa/Cr
was not significantly different between the groups. The %∆UCa/Cr were also not significantly different
from zero or between stone-forming and control groups (Figure 2).
Controls Urolith-formers p-value
Age (years)* 7.2 (± 3.7) 9.4 (±2.0) 0.107
Body Condition
Score (/9) # 6.0 (±1.0) 5.0 (±1.0) 1.00
Serum triglycerides
(mg/dL)# 98.0 (±147.0) 451.0 (±516.0) 0.008
Serum cholesterol
(mg/dL)* 210.1 (±39.6) 273.6 (±93.5) 0.029
Presence of
proteinuria
3/15 4/9 0.362

23
UP:C# 1.1 (±1.43) 2.5 (±0.94) 0.299
UCa/Cr* (all
timepoints)
• 0hr
• 1hr
• 2hr
• 4hr
• 8hr
0.038
0.034 (±0.018)
0.031 (±0.017)
0.039 (±0.024)
0.042 (±0.039)
0.044 (±0.017)
0.060
0.052 (±0.031)
0.063 (±0.036)
0.061 (±0.027)
0.064 (±0.035)
0.064 (±0.036)
0.020
0.129
0.010 0.068
0.078
0.001
% ∆UCa:Cr *
• 1 hour
• 2 hours
• 4 hours
• 8 hours
-2.14 (±38.8)
19.8 (±49.3)
32.9 (±80.4)
36.3 (±83.9)
42.9 (±77.1)
45.2 (±71.1)
45.9 (±65.7)
49.4 (±72.7)
0.123
0.381
0.651
0.650
Presence of
hypercalciuresis
(UCa/Cr >0.05)
2/15 6/9 0.022
Table 1: Variables of control and urolith-former dogs. Normally distributed variables are marked by an asterisk (*);
the mean values are listed and the standard deviation in parentheses. Skewed variables are marked by a pound (#) so
the median is listed, and the interquartile range in parentheses. Significant p-values are shown in bold font.
Hypercalciuresis was initially defined as UCa/Cr >0.05 based on Furrow et al, 2015.[106]
Fig 1: UCa/Cr at different postprandial time points in control (white boxes) and urolith-forming (grey boxes)
Miniature Schnauzer dogs. The box represents the median and the IQR, the whiskers represent values within
p=0.01 p=0.01

24
1.5IQR. Circles and crosses within the box represent mean values. Values outside 1.5 IQR were deemed outliers,
represented by circles and/or crosses outside the box.
Fig 2: Box plot showing % ∆UCa/Cr for control dogs (white boxes) and urolith-formers (grey boxes). The box
represents the median and the IQR. The circles and crosses within boxes represent the mean. The whiskers represent
values within 1.5 IQR. Values outside 1.5IQR are considered outliers and represented either circles or crosses
outside boxes. There are no significant changes between the groups at any time point.
Based on ROC analysis of these 24 dogs and 34 previously published dogs[106], an optimal UCa/Cr cut-
off value of 0.059 (see Appendix 2) was determined. Using this, the UCa/Cr has a sensitivity of 90% and
a sensitivity of 64% for detecting CaOx urolithiasis in male Miniature Schnauzers.
SECTION D: DISCUSSION
This study provides additional information on the UCa/Cr measurement in male Miniature Schnauzers,
and the association of the UCa/Cr with stone status. It provides further evidence that some Miniature
Schnauzers who form CaOx uroliths have abnormal calciuresis. Additionally, we did not observe
significant increases in postprandial UCa/Cr, which is contrary to observations by Lulich [105] who

25
identified postprandial increases in calciuresis in 24-hour collections. Our study does not necessarily
exclude differences in postprandial calciuresis, as we used the UCa/Cr as an estimator of calciuresis as
previously done by Furrow.[106] Normalizing urine calcium, or any other analyte, to urine creatinine will
only lead to a significant linear relationship to 24-hour excretion if both urine calcium and creatinine
concentrations remain steady or fluctuate in unison thoughout a 24-hour period. Studies in human
populations have shown variably significant relationships between spot UCa/Cr and 24-hour urine
calcium quantification.[140-142] Further research into the relationship between these two parameters in
dogs is needed. Twenty four hour urine collections would be impractical for the majority of pet owners
and veterinarians to collect. The goals of this study were to gain further information on a practical
measurement that can be utilized by practitioners to define calciuresis and possibly predict stone risk or
status.
However, the UCa/Cr was sensitive enough to detect a significant difference in calciuresis between the
affected dogs compared to the control dogs. Although significant differences were identified only at 1
hour and 8 hours postprandially, these specific timepoints are unlikely to reflect a clinically relevant
difference from other time points. When examining all individual dog results (see Appendix 1), many
affected Miniature Schnauzers have hypercalciuresis (initially defined as UCa/Cr > 0.05) throughout the
day. Therefore, if using the UCa/Cr to identify hypercalciuresis, the time of sample collection does not
appear to be critical. Furthermore, prolonged urine supersaturation may be one of the mechanisms behind
clinical CaOx urolithiasis in Miniature Schnauzers.
If using the UCa/Cr as an indicator of calcium oxalate stone formation, we propose a tentative upper
reference interval of 0.06. This maximum UCa/Cr value has an excellent specificity at correctly
excluding CaOx urolithiasis in 90% of healthy Miniature Schnauzers. This reference interval has only
modest sensitivity; it could be expected to correctly identify 64% of urolith-formers. One reason for the
moderate sensitivity of the UCa/Cr is that calcium oxalate urolithiasis in Miniature Schnauzers is
presumed to have a multifactorial etiology. Additional factors apart from urinary calcium concentration
contribute to CaOx urolith formation. Promotors and inhibitors of urinary crystal initiation, aggregation
and growth that are important for development of CaOx urolithiasis in humans likely also contribute to
the development of disease in dogs. One example is the urinary macromolecule nephrocalcin, a strong
inhibitor of crystalline growth. A defective isoform of this glycoprotein was the predominate phenotype
expressed in some stone forming humans [99] and possibly in dogs[100] compared to healthy controls.
The association of CaOx urolithiasis with dyslipidemias and proteinuria was an interesting finding. In this
study proteinuria was not identified as a significant factor, which is in contrast to previous findings[112]
and likely due to the limited sample size reported here. Humans with Metabolic Syndrome typically have
hypercholesterolemia and hypertriglyceridemia, and this is associated with subepithelial tubular damage,
development of Randall’s plaques, crystal formation and then nephroliths[84]. It is not known if canine
nephroliths form by the same mechanisms, although it is an attractive theory given the association of
these co-morbidities. Alternatively, dyslipidemias, proteinuria and calcium oxalate urolithiasis may be
common but unrelated conditions in the Miniature Schnauzer.
Though it would not have been appropriate to do with the small population included in this pilot study,
with larger studies, regression analysis could be applied to remove confounding variables such as age.
Another approach is to use age-matched controls to remove this variable. Unfortunately slow patient

26
recruitment and low numbers of suitable Miniature Schnauzers prevented age-matched control dog
enrollment in this study. Larger studies would also allow regression analysis to identify and quantify
contributions from other variables such as proteinuria, hypercholesterolemia and hypertriglyceridemia.
Dietary composition has been previously examined for its role in urolith formation.[128] In this study,
comparing the current or previous diets between stone status groups or calciuresis groups could not be
done due to the wide variety of diets fed and the lack of specific manufacturer’s nutritional information.
We attempted to minimize the effect of diet variation by feeding a standardized diet one meal before and
after the fasted sample.
There are several other limitations of this study. First, dogs were given ample opportunity to empty their
bladder at each timepoint, but residual urine volumes were not measured. Therefore it is possible that
some urine produced during the previous time period may have remained in the bladder and confounded
subsequent results.
Secondly, it is possible that some control dogs may develop urolithiasis in the future. The mean age of
dogs diagnosed with CaOx urolithasis is reported to be 8 years,[109] so younger control animals may be
‘latent’ stone formers. It is not known if the UCa/Cr would increase before the onset of clinical disease,
although this would be a useful finding to proactively manage high-risk dogs. Ideally control dogs could
be followed over time to identify if the UCa/Cr can identify future urolith-formers before the onset of
clinically detectable urolithiasis. In addition, following the UCa/Cr of urolith-formers over time could be
used to help identify the effectiveness of prevention measures designed to reduce calciuresis. This may be
considerably more convenient for investigators than measurement of 24 hour urine calcium excretion,
such as performed by Lulich et al to assess the impact of hydrochlorothiazide.[136]
In conclusion, hypercalciuresis is common amongst male urolith-forming Miniature Schnauzers. The
UCa/Cr proved to be a simple and cost-effective test that has potential to be used to identify dogs at risk
of CaOx urolithaisis. A tentative cut-off for UCa/Cr of male Miniature Schnauzers is 0.06, although
further studies will help establish a more widely accepted reference range for normal calcium excretion.
If using this, the sensitivity and specificity of the UCa/Cr for CaOx urolithiasis is 64% and 90%
respectively. Excessive calciuresis appears to occur throughout the day so strict timing of urine collection
is likely not required.
a Hills Science Diet Adult 1-6yr Chicken and Barley Entrée Canned Dog Food

27
1. Favus, M.J., Factors that influence absorption and secretion of calcium in the
small intestine and colon. American Journal of Physiology - Gastrointestinal
and Liver Physiology, 1985. 248(2): p. G147-G157.
2. Barger-Lux, M.J., R.P. Heaney, and R.R. Recker, Time course of calcium
absorption in humans: evidence for a colonic component. Calcif Tissue Int,
1989. 44(5): p. 308-11.
3. Hoenderop, J.G.J., et al., Molecular Identification of the Apical Ca2+Channel in
1,25-Dihydroxyvitamin D3-responsive Epithelia. Journal of Biological
Chemistry, 1999. 274(13): p. 8375-8378.
4. Peng, J.-B., et al., Molecular Cloning and Characterization of a Channel-like
Transporter Mediating Intestinal Calcium Absorption. Journal of Biological
Chemistry, 1999. 274(32): p. 22739-22746.
5. Christakos, S., C. Gabrielides, and W.B. Rhoten, Vitamin D-dependent calcium
binding proteins: chemistry, distribution, functional considerations, and
molecular biology. Endocr Rev, 1989. 10(1): p. 3-26.
6. Diaz de Barboza, G., S. Guizzardi, and N. Tolosa de Talamoni, Molecular aspects
of intestinal calcium absorption. World J Gastroenterol, 2015. 21(23): p. 7142-
54.
7. Nemere, I., V. Leathers, and A.W. Norman, 1,25-Dihydroxyvitamin D3-mediated
intestinal calcium transport. Biochemical identification of lysosomes containing
calcium and calcium-binding protein (calbindin-D28K). J Biol Chem, 1986.
261(34): p. 16106-14.
8. Christakos, S., et al., Vitamin D and intestinal calcium absorption. Molecular
and cellular endocrinology, 2011. 347(1): p. 25-29.
9. Mallette, L.E., Regulation of blood calcium in humans. Endocrinol Metab Clin
North Am, 1989. 18(3): p. 601-10.
10. Heaney, R. and R. Recker, Distribution of calcium absorption in middle-aged
women. The American journal of clinical nutrition, 1986. 43(2): p. 299-305.
11. Hoek, A.C., et al., Influence of dietary calcium:phosphorus ratio on mineral
excretion and nephrocalcinosis in female rats. J Nutr, 1988. 118(10): p. 1210-6.
12. Stockman, J., et al., Adult dogs are capable of regulating calcium balance, with
no adverse effects on health, when fed a high-calcium diet. Br J Nutr, 2017.
117(9): p. 1235-1243.
13. Council, N.R., Nutrient Requirements of Dogs and Cats. 2006, Washington, DC:
The National Academies Press. 424.
14. Brunette, M.G., et al., Site of 1, 25 (OH) 2 vitamin D3 synthesis in the kidney.
Nature, 1978. 276(5685): p. 287.
15. Zehnder, D., et al., Expression of 25-hydroxyvitamin D3-1alpha-hydroxylase in
the human kidney. J Am Soc Nephrol, 1999. 10(12): p. 2465-73.
16. Kutuzova, G.D. and H.F. DeLuca, Gene expression profiles in rat intestine
identify pathways for 1, 25-dihydroxyvitamin D 3 stimulated calcium absorption

28
and clarify its immunomodulatory properties. Archives of biochemistry and
biophysics, 2004. 432(2): p. 152-166.
17. Grinstead, W.C., C. Pak, and G.J. Krejs, Effect of 1, 25-dihydroxyvitamin D3 on
calcium absorption in the colon of healthy humans. American Journal of
Physiology-Gastrointestinal and Liver Physiology, 1984. 247(2): p. G189-
G192.
18. Haussler, M.R., et al., Molecular mechanisms of vitamin D action. Calcif Tissue
Int, 2013. 92(2): p. 77-98.
19. Fujita, H., et al., Tight junction proteins claudin-2 and-12 are critical for vitamin
D-dependent Ca2+ absorption between enterocytes. Molecular biology of the
cell, 2008. 19(5): p. 1912-1921.
20. Nemere, I. and D. Larsson, Does PTH have a direct effect on intestine? Journal
of Cellular Biochemistry, 2002. 86(1): p. 29-34.
21. Kumar, V. and R. Prasad, Thyroid hormones stimulate calcium transport
systems in rat intestine. Biochim Biophys Acta, 2003. 1639(3): p. 185-94.
22. van Abel, M., et al., Regulation of the epithelial Ca2+ channels in small intestine
as studied by quantitative mRNA detection. Am J Physiol Gastrointest Liver
Physiol, 2003. 285(1): p. G78-85.
23. Charoenphandhu, N., L. Limlomwongse, and N. Krishnamra, Prolactin directly
stimulates transcellular active calcium transport in the duodenum of female
rats. Can J Physiol Pharmacol, 2001. 79(5): p. 430-8.
24. Charoenphandhu, N., K. Wongdee, and N. Krishnamra, Is prolactin the cardinal
calciotropic maternal hormone? Trends Endocrinol Metab, 2010. 21(7): p.
395-401.
25. Fleet, J.C., et al., Growth hormone and parathyroid hormone stimulate intestinal
calcium absorption in aged female rats. Endocrinology, 1994. 134(4): p. 1755-
60.
26. Weaver, C.M., et al., Human calcium absorption from whole-wheat products. J
Nutr, 1991. 121(11): p. 1769-75.
27. Fredlund, K., et al., Absorption of zinc and retention of calcium: dose-dependent
inhibition by phytate. J Trace Elem Med Biol, 2006. 20(1): p. 49-57.
28. Roberfroid, M.B., Prebiotics and probiotics: are they functional foods? Am J Clin
Nutr, 2000. 71(6 Suppl): p. 1682S-7S; discussion 1688S-90S.
29. Coudray, C., et al., Effect of soluble or partly soluble dietary fibres
supplementation on absorption and balance of calcium, magnesium, iron and
zinc in healthy young men. Eur J Clin Nutr, 1997. 51(6): p. 375-80.
30. Heijnen, A.M.P., et al., Ileal pH and apparent absorption of magnesium in rats
fed on diets containing either lactose or lactulose. British Journal of Nutrition,
1993. 70(3): p. 747-756.
31. Beynen, A.C., et al., Faecal bacterial profile, nitrogen excretion and mineral
absorption in healthy dogs fed supplemental oligofructose. J Anim Physiol Anim
Nutr (Berl), 2002. 86(9-10): p. 298-305.

29
32. Beynen, A.C., H.J. Kappert, and S. Yu, Dietary lactulose decreases apparent
nitrogen absorption and increases apparent calcium and magnesium
absorption in healthy dogs. Journal of Animal Physiology and Animal
Nutrition, 2001. 85(3-4): p. 67-72.
33. Suzuki, T., et al., Effects of difructose anhydride III on calcium absorption in
small and large intestines of rats. Biosci Biotechnol Biochem, 1998. 62(5): p.
837-41.
34. Saito, K., et al., Effects of DFA IV in rats: calcium absorption and metabolism of
DFA IV by intestinal microorganisms. Bioscience, biotechnology, and
biochemistry, 1999. 63(4): p. 655-661.
35. Kishi, K., T. Goda, and S. Takase, Maltitol increases transepithelial diffusional
transfer of calcium in rat ileum. Life sciences, 1996. 59(14): p. 1133-1140.
36. Amalraj, A. and A. Pius, Bioavailability of calcium and its absorption inhibitors
in raw and cooked green leafy vegetables commonly consumed in India--an in
vitro study. Food Chem, 2015. 170: p. 430-6.
37. Gnanandarajah, J.S., et al., Presence of Oxalobacter formigenes in the intestinal
tract is associated with the absence of calcium oxalate urolith formation in
dogs. Urological Research, 2012. 40(5): p. 467-473.
38. Gilman, J. and K.D. Cashman, The effect of probiotic bacteria on transepithelial
calcium transport and calcium uptake in human intestinal-like Caco-2 cells.
Curr Issues Intest Microbiol, 2006. 7(1): p. 1-5.
39. Suh, S.M., et al., Pathogenesis of hypocalcemia in primary hypomagnesemia:
normal end-organ responsiveness to parathyroid hormone, impaired
parathyroid gland function. J Clin Invest, 1973. 52(1): p. 153-60.
40. Fatemi, S., et al., Effect of experimental human magnesium depletion on
parathyroid hormone secretion and 1, 25-dihydroxyvitamin D metabolism. The
Journal of Clinical Endocrinology & Metabolism, 1991. 73(5): p. 1067-1072.
41. Hall, J.E., Control of renal calcium excretion and extracellular calcium ion
concentration, in Guyton and Hall Textbook of Medical Physiology. 2015,
Elsevier Health Sciences. p. 396-397.
42. Bushinsky, D.A., Calcium, magnesium, and phosphorus: renal handling and
urinary excretion. Primer on the Metabolic Bone Diseases and Disorders of
Mineral Metabolism, 4th ed., edited by Favus MJ, Philadelphia, Lippincott
Williams & Wilkins, 1999: p. 67-74.
43. Duarte, C. and J. Watson, Calcium reabsorption in proximal tubule of the dog
nephron. American Journal of Physiology-Legacy Content, 1967. 212(6): p.
1355-1360.
44. Hou, J., et al., Claudin-16 and claudin-19 interaction is required for their
assembly into tight junctions and for renal reabsorption of magnesium. Proc
Natl Acad Sci U S A, 2009. 106(36): p. 15350-5.

30
45. Greger, R. and E. Schlatter, Properties of the lumen membrane of the cortical
thick ascending limb of Henle's loop of rabbit kidney. Pflugers Arch, 1983.
396(4): p. 315-24.
46. Loffing, J., et al., Distribution of transcellular calcium and sodium transport
pathways along mouse distal nephron. American Journal of Physiology-Renal
Physiology, 2001. 281(6): p. F1021-F1027.
47. Christakos, S., C. Gabrielides, and W.B. Rhoten, Vitamin D-dependent calcium
binding proteins: chemistry, distribution, functional considerations, and
molecular biology. Endocrine reviews, 1989. 10(1): p. 3-26.
48. van Abel, M., et al., Coordinated control of renal Ca2+ transport proteins by
parathyroid hormone. Kidney International, 2005. 68(4): p. 1708-1721.
49. Johnson, J.A. and R. Kumar, Vitamin D and renal calcium transport. Curr Opin
Nephrol Hypertens, 1994. 3(4): p. 424-9.
50. Li, Y.C., et al., Effects of vitamin D receptor inactivation on the expression of
calbindins and calcium metabolism. Am J Physiol Endocrinol Metab, 2001.
281(3): p. E558-64.
51. Huang, C. and R.T. Miller, Novel Ca receptor signaling pathways for control of
renal ion transport. Curr Opin Nephrol Hypertens, 2010. 19(1): p. 106-12.
52. Lee, C.T., et al., Effects of furosemide on renal calcium handling. Am J Physiol
Renal Physiol, 2007. 293(4): p. F1231-7.
53. Nijenhuis, T., et al., Enhanced passive Ca2+ reabsorption and reduced Mg2+
channel abundance explains thiazide-induced hypocalciuria and
hypomagnesemia. J Clin Invest, 2005. 115(6): p. 1651-8.
54. Brickman, A.S., S.G. Massry, and J.W. Coburn, Changes in Serum and Urinary
Calcium during Treatment with Hydrochlorothiazide: Studies on Mechanisms. J
Clin Invest, 1972. 51(4): p. 945-54.
55. Tantisattamo, E. and T.B. Francis, Primary Hyperaldosteronism As A Risk
Factor For Recurrent Nephrolithiasis. Kidney Research and Clinical Practice,
2012. 31(2): p. A78.
56. Fracassi, F., et al., Urinary excretion of calcium and phosphate in dogs with
pituitary-dependent hypercortisolism: case control study in 499 dogs. Vet Rec,
2015. 177(24): p. 625.
57. Hess, R.S., P.H. Kass, and C.R. Ward, Association between hyperadrenocorticism
and development of calcium-containing uroliths in dogs with urolithiasis. J Am
Vet Med Assoc, 1998. 212(12): p. 1889-91.
58. Smets, P., et al., Cushing's syndrome, glucocorticoids and the kidney. Gen Comp
Endocrinol, 2010. 169(1): p. 1-10.
59. Ferrari, P., et al., Modulation of renal calcium handling by 11 beta-
hydroxysteroid dehydrogenase type 2. J Am Soc Nephrol, 2002. 13(10): p.
2540-6.
60. Moudgil, A., et al., Nephrocalcinosis and renal cysts associated with apparent
mineralocorticoid excess syndrome. Pediatr Nephrol, 2000. 15(1-2): p. 60-2.

31
61. Reul, J.M., et al., Binding characteristics of mineralocorticoid and glucocorticoid
receptors in dog brain and pituitary. Endocrinology, 1990. 127(2): p. 907-15.
62. Bianchi, G., et al., Bisphosphonates in the Management of Idiopathic
Hypercalciuria Associated with Osteoporosis: A New Trick from an Old Drug.
Ther Adv Musculoskelet Dis, 2010. 2(1): p. 29-35.
63. Pak, C.Y., et al., The hypercalciurias. Causes, parathyroid functions, and
diagnostic criteria. J Clin Invest, 1974. 54(2): p. 387-400.
64. Cui, M., et al., Villin promoter-mediated transgenic expression of TRPV6
increases intestinal calcium absorption in wild-type and VDR knockout mice.
Journal of bone and mineral research: the official journal of the American
Society for Bone and Mineral Research, 2012. 27(10): p. 2097.
65. Sharma, O.P., Vitamin D, calcium, and sarcoidosis. Chest, 1996. 109(2): p. 535-
9.
66. Murray, J.J. and C.R. Heim, Hypercalcemia in disseminated histoplasmosis.
Aggravation by vitamin D. Am J Med, 1985. 78(5): p. 881-4.
67. Lee, J.C., et al., Hypercalcemia in disseminated coccidioidomycosis. N Engl J Med,
1977. 297(8): p. 431-3.
68. Bosch, X., Hypercalcemia due to endogenous overproduction of active vitamin D
in identical twins with cat-scratch disease. Jama, 1998. 279(7): p. 532-4.
69. Feldman, E.C., et al., Pretreatment clinical and laboratory findings in dogs with
primary hyperparathyroidism: 210 cases (1987–2004). Journal of the American
Veterinary Medical Association, 2005. 227(5): p. 756-761.
70. Silverberg, S.J., et al., A 10-year prospective study of primary
hyperparathyroidism with or without parathyroid surgery. N Engl J Med, 1999.
341(17): p. 1249-55.
71. Waldegger, S. and M. Konrad, Bartter-, Gitelman-, and Related Syndromes, in
Pediatric Kidney Disease. 2016, Springer. p. 905-920.
72. Ramello, A., C. Vitale, and M. Marangella, Epidemiology of nephrolithiasis.
Journal of nephrology, 2001. 13: p. S45-S50.
73. Bataille, P., et al., Diet, vitamin D and vertebral mineral density in
hypercalciuric calcium stone formers. Kidney Int, 1991. 39(6): p. 1193-205.
74. Stevenson, A.E., W.G. Robertson, and P. Markwell, Risk factor analysis and
relative supersaturation as tools for identifying calcium oxalate stone-forming
dogs. J Small Anim Pract, 2003. 44(11): p. 491-6.
75. Lulich, J.P., C.A. Osborne, and S.L. Sanderson, Effects of dietary
supplementation with sodium chloride on urinary relative supersaturation with
calcium oxalate in healthy dogs. American Journal of Veterinary Research,
2005. 66(2): p. 319-324.
76. Canales, B.K., et al., Second prize: Comprehensive proteomic analysis of human
calcium oxalate monohydrate kidney stone matrix. J Endourol, 2008. 22(6): p.
1161-7.

32
77. Evan, A., et al., Randall's plaque: Pathogenesis and role in calcium oxalate
nephrolithiasis. Kidney International, 2006. 69(8): p. 1313-1318.
78. Asplin, J.R., N.S. Mandel, and F.L. Coe, Evidence of calcium phosphate
supersaturation in the loop of Henle. Am J Physiol, 1996. 270(4 Pt 2): p. F604-
13.
79. Aggarwal, K.P., et al., Nephrolithiasis: Molecular Mechanism of Renal Stone
Formation and the Critical Role Played by Modulators. Biomed Res Int, 2013.
2013.
80. Evan, A.P., et al., Randall’s plaque of patients with nephrolithiasis begins in
basement membranes of thin loops of Henle. The Journal of Clinical
Investigation, 2003. 111(5): p. 607-616.
81. Kuo, R.L., et al., Urine calcium and volume predict coverage of renal papilla by
Randall's plaque. Kidney International, 2003. 64(6): p. 2150-2154.
82. Coe, F.L., A. Evan, and E. Worcester, Pathophysiology-Based Treatment of
Idiopathic Calcium Kidney Stones. Clinical Journal of the American Society of
Nephrology, 2011. 6(8): p. 2083-2092.
83. Domingos, F. and A. Serra, Metabolic syndrome: A multifaceted risk factor for
kidney stones. Scandinavian Journal of Urology, 2014. 48(5): p. 414-419.
84. Khan, S.R., Is oxidative stress, a link between nephrolithiasis and obesity,
hypertension, diabetes, chronic kidney disease, metabolic syndrome? Urological
Research, 2012. 40(2): p. 95-112.
85. Inci, M., et al., Association between Body Mass Index, Lipid Profiles, and Types of
Urinary Stones. Renal Failure, 2012. 34(9): p. 1140-1143.
86. Grover, P.K., R.L. Ryall, and V.R. Marshall, Effect of urate on calcium oxalate
crystallization in human urine: evidence for a promotory role of
hyperuricosuria in urolithiasis. Clin Sci (Lond), 1990. 79(1): p. 9-15.
87. Martins, M.C., et al., CYSTINE: A PROMOTER OF THE GROWTH AND
AGGREGATION OF CALCIUM OXALATE CRYSTALS IN NORMAL UNDILUTED
HUMAN URINE. The Journal of Urology, 2002. 167(1): p. 317-321.
88. Lonsdale, K., Epitaxy as a Growth Factor in Urinary Calculi and Gallstones.
Nature, 1968. 217(5123): p. 56-58.
89. Grover, P.K., V.R. Marshall, and R.L. Ryall, The Promotion of Calcium Oxalate
Crystallization by Urate: Can it be that Epitaxy is Not the Cause After All?, in
Urolithiasis 2, R. Ryall, et al., Editors. 1994, Springer US: Boston, MA. p. 201-
203.
90. Geider, S., et al., Calcium carbonate crystals promote calcium oxalate
crystallization by heterogeneous or epitaxial nucleation: Possible involvement
in the control of urinary lithogenesis. Calcified Tissue International, 1996.
59(1): p. 33-37.
91. Lulich, J.P., et al., Ectopic Bone as a Nidus for Calcium Oxalate Urocystolithiasis
in a Cat. Journal of Veterinary Internal Medicine, 2017. 31(6): p. 1866-1870.

33
92. Bartges, J.W., et al., Influence of acidifying or alkalinizing diets on bone mineral
density and urine relative supersaturation with calcium oxalate and struvite in
healthy cats. Am J Vet Res, 2013. 74(10): p. 1347-52.
93. Tiselius, H.G., The effect of pH on the urinary inhibition of calcium oxalate
crystal growth. British journal of urology, 1981. 53(5): p. 470-474.
94. Rodgers, A., S. Allie-Hamdulay, and G. Jackson, Therapeutic action of citrate in
urolithiasis explained by chemical speciation: increase in pH is the determinant
factor. Nephrol Dial Transplant, 2006. 21(2): p. 361-9.
95. Vogel, E., P. Leskovar, and W. Schütz, Some acid-base balance-dependent
urinary parameters and calcium-binding anions in stone formers. European
urology, 1984. 10(4): p. 254.
96. Ryall, R.L., C.M. Hibberd, and V.R. Marshall, A method for studying inhibitory
activity in whole urine. Urological Research, 1985. 13(6): p. 285-289.
97. Basavaraj, D.R., et al., The Role of Urinary Kidney Stone Inhibitors and
Promoters in the Pathogenesis of Calcium Containing Renal Stones. EAU-EBU
Update Series, 2007. 5(3): p. 126-136.
98. Hamm, L.L. and K.S. Hering-Smith, Pathophysiology of hypocitraturic
nephrolithiasis. Endocrinol Metab Clin North Am, 2002. 31(4): p. 885-93, viii.
99. Nakagawa, Y., et al., Isolation from human calcium oxalate renal stones of
nephrocalcin, a glycoprotein inhibitor of calcium oxalate crystal growth.
Evidence that nephrocalcin from patients with calcium oxalate nephrolithiasis
is deficient in gamma-carboxyglutamic acid. J Clin Invest, 1987. 79(6): p. 1782-
7.
100. Carvalho, M., et al., Defective urinary crystallization inhibition and urinary
stone formation. Int Braz J Urol, 2006. 32(3): p. 342-8; discussion 349.
101. Mo, L., et al., Renal calcinosis and stone formation in mice lacking osteopontin,
Tamm-Horsfall protein, or both. Am J Physiol Renal Physiol, 2007. 293(6): p.
F1935-43.
102. Yamaguchi, S., et al., Heparan sulfate in the stone matrix and its inhibitory
effect on calcium oxalate crystallization. Urological research, 1993. 21(3): p.
187-192.
103. Osborne, C.A., et al., Analysis of 451,891 canine uroliths, feline uroliths, and
feline urethral plugs from 1981 to 2007: perspectives from the Minnesota
Urolith Center. Vet Clin North Am Small Anim Pract, 2009. 39(1): p. 183-97.
104. Low, W.W., et al., Evaluation of trends in urolith composition and
characteristics of dogs with urolithiasis: 25,499 cases (1985–2006). Journal of
the American Veterinary Medical Association, 2010. 236(2): p. 193-200.
105. Lulich, J.P., et al., Evaluation of urine and serum metabolites in miniature
schnauzers with calcium oxalate urolithiasis. Am J Vet Res, 1991. 52(10): p.
1583-90.

34
106. Furrow, E., et al., Fasting urinary calcium-to-creatinine and oxalate-to-
creatinine ratios in dogs with calcium oxalate urolithiasis and breed-matched
controls. J Vet Intern Med, 2015. 29(1): p. 113-9.
107. Dijcker, J., et al., Urinary oxalate and calcium excretion by dogs and cats
diagnosed with calcium oxalate urolithiasis. Veterinary Record, 2012: p.
vetrec-2012-101130.
108. Lulich, J.P., et al., Epidemiology of canine calcium oxalate uroliths. Identifying
risk factors. Vet Clin North Am Small Anim Pract, 1999. 29(1): p. 113-22, xi.
109. Lekcharoensuk, C., et al., Patient and environmental factors associated with
calcium oxalate urolithiasis in dogs. J Am Vet Med Assoc, 2000. 217(4): p. 515-
9.
110. Okafor, C.C., et al., Risk factors associated with calcium oxalate urolithiasis in
dogs evaluated at general care veterinary hospitals in the United States. Prev
Vet Med, 2014. 115(3-4): p. 217-28.
111. Tawashi, R., M. Cousineau, and G. Denis, Calcium oxalate crystal growth in
normal urine: Role of contraceptive hormones. Urological Research, 1984.
12(1): p. 7-9.
112. Kennedy, S.M., et al., Comparison of body condition score and urinalysis
variables between dogs with and without calcium oxalate uroliths. J Am Vet
Med Assoc, 2016. 249(11): p. 1274-1280.
113. Weichselbaum, R.C., et al., AN INTEGRATED EPIDEMIOLOGIC AND
RADIOGRAPHIC ALGORITHM FOR CANINE UROCYSTOLITH MINERAL TYPE
PREDICTION. Veterinary Radiology & Ultrasound, 2001. 42(4): p. 311-319.
114. Weichselbaum, R.C., et al., UROCYSTOLITH DETECTION: COMPARISON OF
SURVEY, CONTRAST RADIOGRAPHIC AND ULTRASONOGRAPHIC TECHNIQUES
IN AN IN VITRO BLADDER PHANTOM. Veterinary Radiology & Ultrasound,
1999. 40(4): p. 386-400.
115. Middleton, W.D., et al., Renal calculi: sensitivity for detection with US.
Radiology, 1988. 167(1): p. 239-44.
116. Ganesan, V., et al., Accuracy of ultrasonography for renal stone detection and
size determination: is it good enough for management decisions? BJU Int, 2017.
119(3): p. 464-469.
117. Pressler, B.M., et al., In vitro prediction of canine urolith mineral composition
using computed tomographic mean beam attenuation measurements.
Veterinary Radiology & Ultrasound, 2004. 45(3): p. 189-197.
118. Weisse, C.W., et al., Potential applications of interventional radiology in
veterinary medicine. J Am Vet Med Assoc, 2008. 233(10): p. 1564-74.
119. Lulich, J., et al., Nonsurgical removal of urocystoliths in dogs and cats by voiding
urohydropropulsion. Journal of the American Veterinary Medical Association,
1993. 203(5): p. 660-663.
120. Berent, A.C., Interventional urology: endourology in small animal veterinary
medicine. Vet Clin North Am Small Anim Pract, 2015. 45(4): p. 825-55.

35
121. Adams, L.G., et al., Use of laser lithotripsy for fragmentation of uroliths in dogs:
73 cases (2005-2006). J Am Vet Med Assoc, 2008. 232(11): p. 1680-7.
122. Grant, D.C., S.R. Werre, and M.L. Gevedon, Holmium: YAG laser lithotripsy for
urolithiasis in dogs. J Vet Intern Med, 2008. 22(3): p. 534-9.
123. Lulich, J., et al., Efficacy And Safety Of Laser Lithotripsy To Manage
Urocystoliths And Urethroliths In Dogs: 100 Consecutive Cases. Journal of
Veterinary Internal Medicine, 2008. 22(3): p. 732.
124. Grant, D.C., T.A. Harper, and S.R. Werre, Frequency of incomplete urolith
removal, complications, and diagnostic imaging following cystotomy for
removal of uroliths from the lower urinary tract in dogs: 128 cases (1994-
2006). J Am Vet Med Assoc, 2010. 236(7): p. 763-6.
125. Runge, J.J., et al., Transvesicular percutaneous cystolithotomy for the retrieval
of cystic and urethral calculi in dogs and cats: 27 cases (2006-2008). J Am Vet
Med Assoc, 2011. 239(3): p. 344-9.
126. Bartges, J. and D. Polzin, Nephrology and urology of small animals. 2011: John
Wiley & Sons.
127. Lulich, J., L. Perrine, and C. Osborne, Postsurgical recurrence of calcium oxalate
uroliths in dogs. J Vet Intern Med, 1992. 6: p. 119.
128. Allen, H.S., et al., Associations of diet and breed with recurrence of calcium
oxalate cystic calculi in dogs. J Am Vet Med Assoc, 2015. 246(10): p. 1098-103.
129. Stevenson, A., et al., Nutrient intake and urine composition in calcium oxalate
stone-forming dogs: comparison with healthy dogs and impact of dietary
modification. Veterinary therapeutics: research in applied veterinary
medicine, 2003. 5(3): p. 218-231.
130. Allen, H.S., et al., Associations of diet and breed with recurrence of calcium
oxalate cystic calculi in dogs. Journal of the American Veterinary Medical
Association, 2015. 246(10): p. 1098-1103.
131. Stevenson, A.E., W.K. Hynds, and P.J. Markwell, Effect of dietary moisture and
sodium content on urine composition and calcium oxalate relative
supersaturation in healthy miniature schnauzers and labrador retrievers. Res
Vet Sci, 2003. 74(2): p. 145-51.
132. Sakhaee, K., et al., Contrasting effects of potassium citrate and sodium citrate
therapies on urinary chemistries and crystallization of stone-forming salts.
Kidney Int, 1983. 24(3): p. 348-52.
133. Stevenson, A.E., et al., Effects of dietary potassium citrate supplementation on
urine pH and urinary relative supersaturation of calcium oxalate and struvite in
healthy dogs. Am J Vet Res, 2000. 61(4): p. 430-5.
134. Scholz, D., P.O. Schwille, and A. Sigel, Double-blind study with thiazide in
recurrent calcium lithiasis. J Urol, 1982. 128(5): p. 903-7.
135. Laerum, E. and S. Larsen, Thiazide prophylaxis of urolithiasis. A double-blind
study in general practice. Acta Med Scand, 1984. 215(4): p. 383-9.

36
136. Lulich, J.P., et al., Effects of hydrochlorothiazide and diet in dogs with calcium
oxalate urolithiasis. J Am Vet Med Assoc, 2001. 218(10): p. 1583-6.
137. Ettinger, B., et al., Chlorthalidone reduces calcium oxalate calculous recurrence
but magnesium hydroxide does not. J Urol, 1988. 139(4): p. 679-84.
138. Ghazali, S. and T. Barratt, Urinary excretion of calcium and magnesium in
children. Archives of disease in childhood, 1974. 49(2): p. 97-101.
139. Furrow, E., et al., Proteinuria and lipoprotein lipase activity in Miniature
Schnauzer dogs with and without hypertriglyceridemia. Vet J, 2016. 212: p. 83-
9.
140. Choi, I.S., et al., Random Urinary Calcium/Creatinine Ratio for Screening
Hypercalciuria in Children with Hematuria. Ann Lab Med, 2013. 33(6): p. 401-
5.
141. Mir, S. and E. Serdaroglu, Quantification of hypercalciuria with the urine
calcium osmolality ratio in children. Pediatr Nephrol, 2005. 20(11): p. 1562-5.
142. Jones, A.N., et al., Fasting and postprandial spot urine calcium-to-creatinine
ratios do not detect hypercalciuria. Osteoporos Int, 2012. 23(2): p. 553-62.

37
Appendix 1. UCa:Cr for control (grey triangles) and urolith-forming (black diamonds) dogs at different
timepoints
0
0.02
0.04
0.06
0.08
0.1
0.12
0.14
0.16
0.18
0.00 1.00 2.00 3.00 4.00 5.00 6.00 7.00 8.00
Uri
ne
Ca
lciu
m (
mg
/dL)
: C
rea
tin
ine
(m
g/d
L)
Postprandial time (hr)
Urolith-former 1
Control 1

38
Appendix 2: Receiver Operator Characteristic
Using Group='Stone-former' to be the positive level
AUC
0.78393
ROC Table
X Prob 1-Specificity Sensitivity Sens-(1-
Spec)
True Pos True Neg False Pos False Neg
. . 0.0000 0.0000 0.0000 0 30 0 28
0.2130000 0.9694 0.0000 0.0357 0.0357 1 30 0 27
0.1950000 0.9552 0.0333 0.0357 0.0024 1 29 1 27
0.1760000 0.9337 0.0333 0.0714 0.0381 2 29 1 26
0.1640000 0.9155 0.0333 0.1071 0.0738 3 29 1 25
0.1510000 0.8907 0.0333 0.1429 0.1095 4 29 1 24
0.1470000 0.8819 0.0333 0.1786 0.1452 5 29 1 23
0.1093941 0.7662 0.0333 0.2143 0.1810 6 29 1 22
0.1044204 0.7462 0.0667 0.2143 0.1476 6 28 2 22
0.0960000 0.7097 0.0667 0.2500 0.1833 7 28 2 21
0.0950000 0.7052 0.1000 0.2500 0.1500 7 27 3 21
0.0943105 0.7020 0.1000 0.2857 0.1857 8 27 3 20
0.0810000 0.6378 0.1000 0.3214 0.2214 9 27 3 19
0.0740210 0.6018 0.1000 0.3571 0.2571 10 27 3 18
0.0713948 0.5880 0.1000 0.3929 0.2929 11 27 3 17
0.0670000 0.5645 0.1000 0.4643 0.3643 13 27 3 15
0.0602363 0.5278 0.1000 0.5000 0.4000 14 27 3 14
0.0600000 0.5265 0.1000 0.5714 0.4714 16 27 3 12
0.0590000 0.5211 0.1000 0.6429 0.5429 * 18 27 3 10
0.00
0.10
0.20
0.30
0.40
0.50
0.60
0.70
0.80
0.90
1.00
0.00 0.10 0.20 0.30 0.40 0.50 0.60 0.70 0.80 0.90 1.00
1-Specificity
False Positive

39
X Prob 1-Specificity Sensitivity Sens-(1-
Spec)
True Pos True Neg False Pos False Neg
0.0589560 0.5208 0.1333 0.6429 0.5095 18 26 4 10
0.0504152 0.4741 0.1667 0.6429 0.4762 18 25 5 10
0.0480000 0.4610 0.2000 0.6429 0.4429 18 24 6 10
0.0474463 0.4580 0.2333 0.6429 0.4095 18 23 7 10
0.0465506 0.4531 0.2667 0.6429 0.3762 18 22 8 10
0.0448344 0.4438 0.2667 0.6786 0.4119 19 22 8 9
0.0443749 0.4413 0.3000 0.6786 0.3786 19 21 9 9
0.0430000 0.4339 0.3000 0.7143 0.4143 20 21 9 8
0.0390000 0.4126 0.3000 0.7500 0.4500 21 21 9 7
0.0368647 0.4013 0.3333 0.7500 0.4167 21 20 10 7
0.0357510 0.3954 0.3333 0.7857 0.4524 22 20 10 6
0.0330000 0.3811 0.3333 0.8214 0.4881 23 20 10 5
0.0310330 0.3710 0.3667 0.8214 0.4548 23 19 11 5
0.0310000 0.3709 0.4000 0.8214 0.4214 23 18 12 5
0.0305785 0.3687 0.4000 0.8571 0.4571 24 18 12 4
0.0289464 0.3605 0.4333 0.8571 0.4238 24 17 13 4
0.0285487 0.3585 0.4667 0.8571 0.3905 24 16 14 4
0.0270838 0.3511 0.4667 0.8929 0.4262 25 16 14 3
0.0270000 0.3507 0.5333 0.8929 0.3595 25 14 16 3
0.0230000 0.3310 0.5333 0.9286 0.3952 26 14 16 2
0.0221102 0.3267 0.5667 0.9286 0.3619 26 13 17 2
0.0220000 0.3262 0.6000 0.9286 0.3286 26 12 18 2
0.0210914 0.3219 0.6333 0.9286 0.2952 26 11 19 2
0.0210000 0.3214 0.6667 0.9286 0.2619 26 10 20 2
0.0200000 0.3167 0.7000 0.9286 0.2286 26 9 21 2
0.0190000 0.3119 0.7333 0.9286 0.1952 26 8 22 2
0.0179015 0.3068 0.7667 0.9286 0.1619 26 7 23 2
0.0177721 0.3062 0.8000 0.9286 0.1286 26 6 24 2
0.0170000 0.3026 0.8333 0.9286 0.0952 26 5 25 2
0.0140000 0.2890 0.8667 0.9643 0.0976 27 4 26 1
0.0133039 0.2858 0.9000 0.9643 0.0643 27 3 27 1
0.0100000 0.2713 0.9333 0.9643 0.0310 27 2 28 1
0.0080000 0.2627 0.9333 1.0000 0.0667 28 2 28 0
0.0070000 0.2585 1.0000 1.0000 0.0000 28 0 30 0
0.0070000 0.2585 1.0000 1.0000 0.0000 28 0 30 0