mcn audit report - woscan.scot.nhs.uk · skin cancer . managed clinical network . audit report ....
TRANSCRIPT
West of Scotland Cancer Network Skin Cancer Managed Clinical Network
Audit Report Report of the 2012 Clinical Audit Data
Dr Girish Gupta MCN Clinical Lead Iona Scott Information Manager Tom Kane MCN Manager

West of Scotland Cancer Network Final - Published Skin Cancer MCN Audit Report 12th September 2013
2
CONTENTS
EXECUTIVE SUMMARY 3
1. INTRODUCTION 6
2. BACKGROUND 7
2.1 NATIONAL CONTEXT 7
2.2 WEST OF SCOTLAND CONTEXT 8
3. METHODOLOGY 11
4. RESULTS AND ACTION REQUIRED 12
4.1 DATA QUALITY 12
4.2 PERFORMANCE AGAINST KEY OUTCOME MEASURES 13
5. CONCLUSIONS 23
6. ACKNOWLEDGEMENTS 24
7. REFERENCES 25
8. ABBREVIATIONS 26
9. APPENDICES: NHS BOARD ACTION PLANS 27

West of Scotland Cancer Network Final - Published Skin Cancer MCN Audit Report 12th September 2013
3
Executive Summary
Introduction The purpose of this report is to present an assessment of performance of Malignant Melanoma Skin Cancer Services relating to patients diagnosed in the West of Scotland in 2012. Data are reported against Key Outcome Measures (KOMs) developed regionally by a core review group and agreed by the Skin Cancer Managed Clinical Network (MCN). The National Cancer Quality Steering Group, under the auspices of the Scottish Cancer Taskforce, is currently taking forward the development of national Quality Performance Indicators (QPIs) for all cancers. This will enable future national comparative reporting and will help to drive continuous improvement for patients. At the beginning of 2011, the West of Scotland Cancer Network (WoSCAN) initiated a process to optimise the use of available resources which would agree regional quality of care and outcome measures for those tumour networks which do not yet have QPIs implemented or do not have NHS Quality Improvement Scotland (NHS QIS) Clinical Standards. This work was aimed at focussing regional analysis on key clinical outcome measures as an interim measure prior to the introduction of QPIs. Additionally, it was anticipated that this process would support more targeted data collection and ensure more efficient use of audit resource. Background The trend in incidence of cancer in Scotland is an increasing one generally however the incidence rate of malignant melanoma of the skin has increased by approximately 58% in males and 46% in females over the last decade. Malignant melanoma is now the 5th most common cancer in Scotland, for both sexes1. While the incidence of malignant melanoma is increasing significantly, survival rates are also improving with increases in the five year relative survival from 64% to 85% in males and 82% to 92% in females1. Four NHS Boards serve the 2.4 million population of the West of Scotland (WoS). In 2012, 537 cases of malignant melanoma were reported through audit as diagnosed in the WoS. The multi disciplinary team (MDT) configuration for services in the region is detailed below: MDT Constituent Hospital(s) Ayrshire & Arran Crosshouse Hospital, Ayr Hospital Clyde Royal Alexandra Hospital, Inverclyde Royal Hospital, Vale of Leven South & East Glasgow Southern General Hospital, Glasgow Royal Infirmary North & West Glasgow Western Infirmary Forth Valley Stirling Community Hospital, Forth Valley Royal Hospital Lanarkshire Wishaw General Hospital, Monklands District General, Hairmyres
Methodology The clinical audit data presented in this report were collected by clinical audit staff in each NHS Board in accordance with an agreed dataset and definitions. Data were entered locally into the electronic Cancer Audit Support Environment (eCASE): a secure centralised web-based database. Data relating to patients diagnosed between 1st January and 31st December 2012 were downloaded from eCASE on 6th June 2013. Analysis was performed centrally by the WoSCAN Information Team and the timescales agreed took into account the patient pathway to ensure that a complete treatment record was available for each case. Initial results of the analysis were provided to local Boards to check for inaccuracies or obvious
West of Scotland Cancer Network Final - Published Skin Cancer MCN Audit Report 12th September 2013
4
gaps before final analysis was carried out. Final results were disseminated for NHS Board verification, in line with the regional audit governance process, to ensure that the data was an accurate representation of service in each area. Results Overall case ascertainment for WoSCAN is high however there is some fluctuation between areas. This may, in part, be due to the difficulty in calculating case ascertainment using previous years’ figures when the incidence of melanoma is increasing and yearly fluctuations occur in some NHS Boards. NHS Ayrshire and Arran has notably lower ascertainment than the other areas which is worthy of further investigation. Data quality is good with significant improvement over the past 3 years, particularly in the recording of pathological tumour stage data. This is data of high importance given that meaningful interpretation of numerous KOMs is dependant on tumour stage data. The completeness of excision margin data has improved considerably however some improvement is still required in NHS Greater Glasgow and Clyde and NHS Lanarkshire. Data are measured against agreed criteria including six KOMs developed by the Skin Cancer Managed Clinical Network (MCN). Below is a summary of results; figures are expressed in percentages and represent the combined WoS figure and the range across NHS Boards. Results highlight a significant improvement in performance across all KOMs since 2010.
1. All malignant melanomas should be referred urgently (74.9 [70.4-89.2] %).
2. Patients with malignant melanoma should not receive excision in Primary Care (1.5 [0-4.7] %).
3. Patients with malignant melanoma should generally1 not receive biopsy before surgical treatment (13.2 [4.8-17.1] %).
4. Breslow thickness or Clark level (if Breslow cannot be measured) should be recorded for all malignant melanoma patients (99.8 [99.7-100] %).
5. Pathological staging should be used to stage all malignant melanoma patients (99 [97.4-100] %).
6. Surgical wide excision margins should be appropriate to stage of tumour in line with SIGN guideline, as set out in page 21 of the main report (86.1 [70.0 – 91.0] %).
Conclusions and Action Required Collection of data on malignant melanoma diagnoses began in 2006 and since that time there has been significant improvement in data quality. With data quality improving and the introduction of KOMs, the MCN is moving towards robust performance assessment where audit data can highlight clinical/service issues and lead to improvement and service change. The outcome measures analysed allow assessment of service quality however there are still some minor data quality issues which require further improvement to enable consistent and comparable reporting. The MCN will actively take forward regional actions identified and NHS Boards are asked to develop local Action/Improvement Plans in response to the findings presented in the report. Progress against these plans will be monitored by the MCN Advisory Board and reported to the Regional Cancer Advisory Group (RCAG) annually by Board Lead Cancer Clinicians and MCN Clinical Leads, as part
1 In some situations it may be appropriate to biopsy a lesion before surgical treatment, e.g. due to size or location of lesion.

West of Scotland Cancer Network Final - Published Skin Cancer MCN Audit Report 12th September 2013
5
of the regional audit governance process to enable RCAG to review and monitor regional improvement. Action required: Service Improvement
All NHS Boards should discuss referral criteria of suspicious lesions with dermatologists and Primary Care Cancer Leads and identify means to increase numbers of appropriate urgent referrals.
MCN to advocate inclusion of melanoma in the national Detect Cancer Early Programme. This in turn may yield greater results in promoting appropriate referrals than reliance on education events.
NHS Ayrshire and Arran, NHS Greater Glasgow and Clyde and NHS Lanarkshire should review cases where excisions have been performed in Primary Care to establish reasons for the occurrences and promote referral into Secondary Care for biopsy/excision.
NHS Ayrshire and Arran and NHS Greater Glasgow and Clyde should review the cases where biopsy was performed prior to surgical treatment to assess whether practice was appropriate.
All WoS NHS Boards should monitor clinical practice to ensure that further increases in biopsy prior to surgical resection are not observed.
NHS Forth Valley should discuss and review surgical techniques to establish whether compliance with the SIGN guideline recommendation on appropriate surgical excision can be improved.
All WoS NHS Boards should review the number of patients undergoing wide local excision to determine if the relatively low numbers are due to a data recording issue or demonstrate a change in clinical practice. Results should be reviewed by the Skin Cancer MCN.
Data Quality Improvement
NHS Ayrshire and Arran should review their case ascertainment by utilising ACaDMe to compare identified malignant melanoma patients with Cancer Registry. The Board should also review the process for notification of cases from pathology department(s).
NHS Lanarkshire should review audit data collection processes to ensure complete and accurate data capture for surgical excision margins, particularly identifying a process for retrieval of surgical margin data from Plastic Surgery Department in NHS Greater Glasgow and Clyde.
NHS Greater Glasgow and Clyde and NHS Lanarkshire should review audit data collection processes to ensure complete and accurate capture of surgical excision margin data.
A summary of actions for each NHS Board has been included within the Action Plan templates in Appendices I – IV. Completed Action Plans should be returned to WoSCAN within two months of publication of this report.

West of Scotland Cancer Network Final - Published Skin Cancer MCN Audit Report 12th September 2013
6
1. Introduction The purpose of this report is to present an assessment of performance of Malignant Melanoma Skin Cancer Services relating to patients diagnosed in the region in 2012. These audit data underpin much of the regional development/service improvement work of the Managed Clinical Network (MCN) and regular reporting of activity and performance is a fundamental requirement of an MCN to assure the quality of care delivered across the region. The National Cancer Quality Steering Group, under the auspices of the Scottish Cancer Taskforce, is currently taking forward the development of national Quality Performance Indicators (QPIs) for all cancers. This will enable future national comparative reporting and will help to drive continuous quality improvement for patients. Development of Malignant Melanoma QPIs commenced in February 2013, with indicators scheduled for implementation in October 2014. Currently this disease group does not have NHS Quality Improvement Scotland (NHS QIS) Clinical Standards to report against. In 2011, the West of Scotland Cancer Network (WoSCAN) initiated a process to optimise the use of available resources regionally and locally which would assure regional quality of care and have agreement on outcome measures for specific tumour networks. This work was aimed at focussing regional analysis on key clinical outcome measures whilst also aiming to support more targeted data collection and ensure more efficient use of audit resource. Additionally, it was anticipated that this early preparatory work would help inform the development of national QPIs and in time help expedite the national process for these networks. A core review group was established to carry out the initial process of drafting key outcome measures (KOMs). Regional measurability for the KOMs was then determined before disseminating documentation for wider consultation and regional agreement. KOMs have now been analysed and reported against for 3 successive years of clinical audit data (2010 to 2012).

West of Scotland Cancer Network Final - Published Skin Cancer MCN Audit Report 12th September 2013
7
2. Background Four NHS Boards serve the 2.4 million population of the West of Scotland (WoS) where over 500 cases of malignant melanoma are diagnosed each year. Patients are referred from their general practitioner to the dermatology department with a pigmented lesion for assessment. At clinic the lesion is assessed and patients with a benign mole are generally discharged. Patients with a possible melanoma have urgent surgery (excision) to remove the lesion. Tissue taken from the excision is sent to pathology for confirmation of a malignant melanoma diagnosis. Confirmed malignant melanoma patients are discussed at the next local skin cancer multi disciplinary team (MDT) meeting which takes place on a weekly to fortnightly basis. Unlike most other cancer types, patients are generally discussed at MDTs after they have completed their primary treatment. Generally patients will go on to have a wide excision at a later stage to reduce the risk of local recurrence. The MDT configuration is shown below: MDT Constituent Hospital(s) Ayrshire & Arran Crosshouse Hospital, Ayr Hospital Clyde Royal Alexandra Hospital, Inverclyde Royal Hospital, Vale of Leven South & East Glasgow Southern General Hospital, Glasgow Royal Infirmary North & West Glasgow Western Infirmary Forth Valley Stirling Community Hospital, Forth Valley Royal Hospital Lanarkshire Wishaw General Hospital, Monklands District General, Hairmyres
2.1 National Context
The overall number of cancers diagnosed in Scotland has increased over the last 10 years although incidence of some cancers is decreasing1. Over the last decade the incidence of malignant melanoma of the skin has increased significantly by 51% (58% in men and 46% in women)1. Malignant melanoma is the now the 5th most common cancer in Scotland, for both males and females, with over 1200 cases diagnosed per annum1. This increase is, in the main, attributed to changes in sun related behaviour and increased exposure to sunlight, both natural and artificial, with the increased use of sunbeds and holidays abroad1, 4. Predictions are for more than a 70% increase in the incidence of malignant melanoma in Scotland in the two decades up to 20202. Whilst the incidence of malignant melanoma is increasing significantly survival from the disease is also improving with an increase in the five year relative survival for malignant melanoma from 64% to 85% in males, and 82% to 92% in females1. Like many other cancers malignant melanoma incidence is related to age however it has an unusual pattern in that 25% of cases in Scotland occur in people under the age of 50 and more than half are under 65 years of age3, UK-wide data shows a similar trend4. The largest overall increase in incidence is however demonstrated in males between 60 and 79 years of age4. In the UK as a whole it has been shown that there is a link between age and mortality with mortality rates being the highest in older men and women. Between 2008 and 2010 in the UK an average of 5% of deaths due to malignant melanoma were in the age group 15-39 years and an average of 62% of deaths were in those aged over 64 years of age4.

2.2 West of Scotland Context
In the West of Scotland (WoS) 537 cases of malignant melanoma were reported through audit as diagnosed in 2012. In line with the trend in Scotland and the UK, over half of malignant melanomas in the WoS occur in people under 65 years of age (52%). The WoS also follows the aforementioned UK wide trend for increasing incidence in older males with an increase from 61 in 2010 to 70 in 2012. Note that cases collected through audit do not include patients under the age of 16 years. Figure 1 illustrates the number of patients diagnosed with malignant melanoma in WoS by age and sex. Figure 1: Number of patients diagnosed in WoSCAN in 2012 by age and sex
*Patients under 16 years of age are not included in the audit
0 – 19* 20 - 34 35 - 44 45 - 54 55 - 64 65 - 74 ≥ 75 Total Male 0 7 17 33 52 70 62 241 Female 2 25 36 54 53 49 77 296
The incidence of malignant melanoma continues to increase and in the West of Scotland incidence rose from 318 in 2000 to 546 in 20113. The clinical site of melanomas diagnosed in the West of Scotland in 2012 is presented in Figure 2.
West of Scotland Cancer Network Final - Published Skin Cancer MCN Audit Report 12th September 2013
8

Figure 2: Clinical site of malignant melanoma diagnosed in WoS in 2012
The distribution of cases by SIMD (Scottish Index of Multiple Deprivation) category is shown in Figure 3 for NHS Board of diagnosis. In the majority of Boards, around 45% of patients are in the two most affluent groups, with the exception of NHS Lanarkshire at 37%. Figure 3: SIMD category by NHS Board of diagnosis
0%
20%
40%
60%
80%
100%
AA FV GGC LAN WoS
NHS Board of Diagnosis
% Patients
Not found
5 ‐ least deprived
4
3
2
1 ‐ most deprived
West of Scotland Cancer Network Final - Published Skin Cancer MCN Audit Report 12th September 2013
9

Figure 4 indicates that superficial spreading melanoma is the most common type of melanoma found in WoS patients with almost two thirds of patients presenting with this type of melanoma in 2012. This is consistent with previous year’s analyses (2010 and 2011). Figure 4: Histogenic type of tumours diagnosed in WoS in 2012
Lentigo maligna melanoma is the next most common type of melanoma, however this percentage has decreased slightly from 2010 and 2011 figures (15% and 16% of patients in 2010 and 2011 respectively). These melanomas develop from very slow growing pigmented areas of skin called lentigo maligna. The lentigo maligna (also known as an ‘in-situ’ lesion) is flat and grows outwards in the surface layers of the skin. It may gradually enlarge over several years and may change shape. If it becomes a lentigo maligna melanoma, it starts to invade into the deeper layers of the skin and may form lumps (nodules). Once this happens it is described as invasive melanoma. Only invasive melanomas are collected and reported upon through the audit and consequently lentigo maligna (in-situ lesions) are not included in this report. Nodular melanoma was equally as common as lentigo meligna melanoma in 2012, with figures broadly unchanged from previous year’s analyses (11% and 14% of patients in WoS in 2010 and 2011 respectively). This type of melanoma tends to develop quickly and begins to invade deeper into the skin quite rapidly if it is not removed. There is often a raised area on the skin surface with this type of melanoma. Due to the rate of growth, thickness and local invasion this is one of the most aggressive melanomas and has a higher chance of spreading to other areas.
West of Scotland Cancer Network Final - Published Skin Cancer MCN Audit Report 12th September 2013
10

West of Scotland Cancer Network Final - Published Skin Cancer MCN Audit Report 12th September 2013
11
3. Methodology The clinical audit data presented in this report were collected by clinical audit staff in each West of Scotland NHS Board in accordance with an agreed dataset and definitions. Data were recorded manually and entered locally into the electronic Cancer Audit Support Environment (eCASE): a secure centralised web-based database. Data relating to patients diagnosed between 1st January and 31st December 2012 were downloaded from eCASE at 22:00hrs on 6th June 2013. Cancer audit is a dynamic process with patient data continually being revised and updated as more information becomes available. This means that apparently comparable reports for the same time period and cancer site may produce different figures if extracted at different times. Analysis was performed centrally for the region by the WoSCAN Information Team and the timescales agreed took into account the patient pathway to ensure that a complete treatment record was available for each case. Initial results of the analysis were provided to local Boards to check for inaccuracies, inconsistencies or obvious gaps and a subsequent download taken upon which final analysis was carried out. The final data analysis was disseminated for NHS Board verification in line with the regional audit governance process to ensure that their data were an accurate representation of service in each area.

4. Results and Action Required
4.1 Data Quality
Quality of audit data can be assessed in the first instance by estimating the proportion of expected patients that have been identified through audit. Case ascertainment is calculated by the number of patients identified as diagnosed in a NHS Board through audit as a percentage of the incidence of cancer diagnosed in that NHS Board from Cancer Registry. Cancer Registry information is available some time after the year of interest as collection and verification of data is time intensive, for this reason audit data cannot be compared directly to Cancer Registry data for the same year. The trend in incidence of malignant melanoma is an increasing one and this presents some difficulty in the assessment of case ascertainment. Cancer Registry figures used were extracted from ACaDMe (Acute Cancer Deaths and Mental Health), a system provided by Information Services Division (ISD), on 22nd April 2013 via the standard reports available. Cancer Registry figures are an average of 2009 to 2011 figures to take account of annual fluctuations in incidence within NHS Boards. Figure 5 presents the case ascertainment for each NHS Board and for WoSCAN as a whole. Figure 5: Case ascertainment of 2012 data by location of diagnosis.
AA GGC FV Lan WoSCAN
Cases from audit 64 317 44 112 537 Cases from Cancer Registry (2009-2011) 78 321 41 116 556 Case ascertainment 82.1% 98.8% 107.3% 96.6% 96.6%
NHS Ayrshire and Arran has a notably lower case ascertainment than the other NHS Boards, which is a significant decrease on 2011 case ascertainment (105.2%). Reasons for this variance should be explored. In 2011 NHS Lanarkshire completed work to address low case ascertainment figures; it would appear from 2012 data that any issues have now been resolved with an increase in case ascertainment now demonstrated (83% to 97%).
West of Scotland Cancer Network Final - Published Skin Cancer MCN Audit Report 12th September 2013
12

West of Scotland Cancer Network Final - Published Skin Cancer MCN Audit Report 12th September 2013
13
Cases of malignant melanoma are generally identified through the reporting of pathology following surgical removal of the lesion. High case ascertainment would be expected as a result as almost all patients will undergo a surgical procedure. Action required:
NHS Ayrshire and Arran should review their case ascertainment by utilising ACaDMe to compare identified malignant melanoma patients with Cancer Registry. The Board should also review the process for notification of cases from pathology department(s).
In the report of 2011 WoSCAN Skin Cancer Audit Data it was outlined that recording of pathological tumour stage (pT stage) was poor, particularly in NHS Ayrshire and Arran where over 50% of excisions did not have pathological tumour stage recorded. Considerable improvement in pT stage recording is demonstrated by data for patients diagnosed in 2012; from 11.4% not recorded in 2011 to 1% in 2012. For NHS Lanarkshire KOM 6 results are affected by the incompleteness of the surgical excision margin for patients undergoing excision by the Plastic Surgery Department in Greater Glasgow and Clyde (14.3% not recorded). In Greater Glasgow and Clyde 3.8% of patients did not have a surgical excision margin recorded, this has however decreased from over 10% in 2011. In other NHS Boards, Forth Valley and Ayrshire and Arran, surgical excision margin data have improved significantly from previous years, however it should be noted that a small number of cases in NHS Ayrshire and Arran are recorded as inapplicable, reasons for this include an inability to obtain information of surgical margins for patients undergoing excision in Greater Glasgow and Clyde. On the whole, following action by all Boards since 2010, surgical excision margin data are well recorded. There is still some room for improvement in data quality if KOM 6 is to provide robust results for all NHS Boards. Action required:
NHS Lanarkshire should review audit data collection processes to ensure complete and accurate data capture for surgical excision margins, particularly identifying a process for retrieval of surgical margin data from Plastic Surgery Department in NHS Greater Glasgow and Clyde.
4.2 Performance Against Key Outcome Measures
Results of analysis of selected performance criteria are set out in the following section. Graphs and charts have been provided where this aids interpretation and where appropriate, figures are also included to provide context. Results are presented by NHS Board of diagnosis with some criteria given as an overall WoSCAN representation. Specific Regional and NHS Board actions have been recommended to address issues highlighted through the data analysis. 4.2.1 KOM 1: All malignant melanomas should be referred urgently Scottish Intercollegiate Guidelines Network (SIGN) national guidelines for cutaneous melanoma state that “GPs should refer urgently all patients in whom melanoma is a strong possibility rather than carry out a biopsy in primary care” 5(p9). Earlier referral results in earlier treatment which may have an impact on thickness of melanoma and thus lead to improved survival.

Figure 6 illustrates that the proportion of patients referred urgently has increased since 2010, from 53% in 2010 to 75% across WoS as a whole. Although short of the aspirational SIGN target of 100% of patients being referred urgently, this demonstrates a significant improvement across all WoS NHS Boards. It is however appreciated by all WoS NHS Boards that performance could still improve by enhanced relationships between Dermatology and Primary Care, specifically with education of GPs in identifying suspicious lesions. Figure 6: Proportion of patients referred urgently from 2010 and 2012 by NHS Board of diagnosis
AA FV GGC Lan 2010 2011 2012 2010 2011 2012 2010 2011 2012 2010 2011 2012
Urgent 31 41 50 35 34 33 148 141 164 80 70 72
Soon 10 0 0 1 0 0 1 0 1 0 0 0
Routine 10 28 9 6 5 3 99 103 67 19 18 23
Not Recorded 3 0 0 1 0 1 0 0 1 0 2 2
Inapplicable 11 12 0 3 6 0 82 70 0 14 8 0
Total 65 81 59 46 45 37 330 314 233 113 98 97
The measurability specification for this outcome measure has changed since 2011 audit data analysis. In previous years all patients with malignant melanoma were included. Due to their mode of referral a proportion of patients would have no urgency assigned to the referral, for example, patients referred from a review clinic or from private healthcare. To ensure more accurate assessment of the proportion of patients referred urgently these patients were excluded from the analyses in 2012. The numbers referred through these methods are however low so the effect on the proportions is not large and, ultimately, the outcome is the same i.e. that the proportion of patients referred urgently has increased.
West of Scotland Cancer Network Final - Published Skin Cancer MCN Audit Report 12th September 2013
14
Previous attempts have been made to address the low rates of urgent referrals across the region by holding educational events. Various NHS Boards have implemented a number of initiatives with the aim of increasing the proportion of patients referred urgently, including a skin referral pro-forma for
GPs. Additionally some dermatology departments across the region photo-triage all patients with suspicious lesions and upgrade their referral to urgent based upon this. Action required:
All NHS Boards should discuss referral criteria of suspicious lesions with dermatologists and Primary Care Cancer Leads and identify means to increase numbers of appropriate urgent referrals.
MCN to advocate inclusion of melanoma in the national Detect Cancer Early Programme. This in turn may yield greater results in promoting appropriate referrals than reliance on education events.
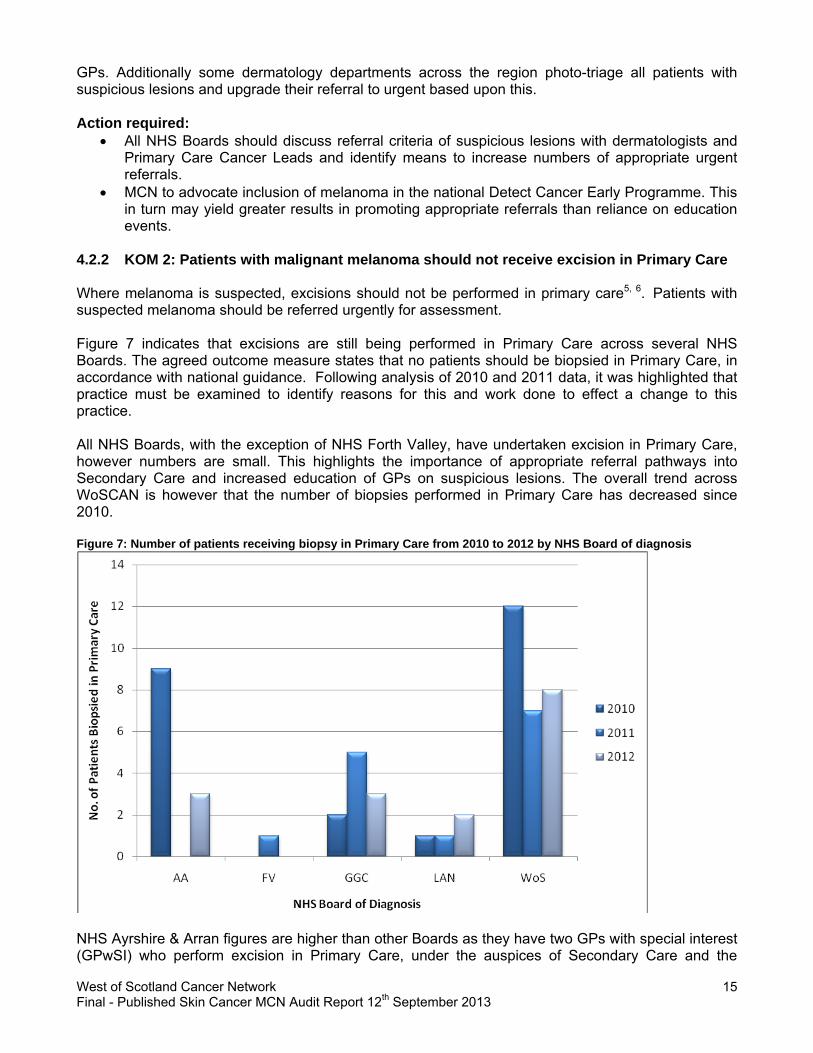
4.2.2 KOM 2: Patients with malignant melanoma should not receive excision in Primary Care Where melanoma is suspected, excisions should not be performed in primary care5, 6. Patients with suspected melanoma should be referred urgently for assessment. Figure 7 indicates that excisions are still being performed in Primary Care across several NHS Boards. The agreed outcome measure states that no patients should be biopsied in Primary Care, in accordance with national guidance. Following analysis of 2010 and 2011 data, it was highlighted that practice must be examined to identify reasons for this and work done to effect a change to this practice. All NHS Boards, with the exception of NHS Forth Valley, have undertaken excision in Primary Care, however numbers are small. This highlights the importance of appropriate referral pathways into Secondary Care and increased education of GPs on suspicious lesions. The overall trend across WoSCAN is however that the number of biopsies performed in Primary Care has decreased since 2010. Figure 7: Number of patients receiving biopsy in Primary Care from 2010 to 2012 by NHS Board of diagnosis
NHS Ayrshire & Arran figures are higher than other Boards as they have two GPs with special interest (GPwSI) who perform excision in Primary Care, under the auspices of Secondary Care and the
West of Scotland Cancer Network Final - Published Skin Cancer MCN Audit Report 12th September 2013
15

dermatological cancer MDT. These GPwSI were responsible for 3 of the 4 biopsies performed in 2012. It is recommended that, with the revision of the national minimum core dataset in 2013/14 codes are revised to account for biopsies undertaken by primary care physicians with specialist training (GPwSI). Action required:
NHS Ayrshire and Arran, NHS Greater Glasgow and Clyde and NHS Lanarkshire should review cases where excisions have been performed in Primary Care to establish reasons for the occurrences and promote referral into Secondary Care for biopsy/excision.
4.2.3. KOM 3: Patients with malignant melanoma should generally not receive biopsy before surgical treatment Biopsies should generally not be performed where a melanoma is suspected5, 6 as there is a risk of inadequate sampling. There are however situations where it is appropriate to biopsy lesions prior to surgical excision, for example due to the size of lesion or site of tumour (e.g. face or ear). Other than these specific situations, there will be a small number of cases where a biopsy is indicated prior to excision. Figure 8 displays an increase in the proportion of patients who had a biopsy prior to surgical treatment between 2010 and 2012 for the majority of Boards, with a steady increase across WoSCAN. This increase highlights that all NHS Boards should review practice to determine reasons for high, and increasing, proportions of biopsies prior to surgical treatment. Figure 8: Proportion of patients who had a biopsy prior to surgical treatment in 2010 and 2011
AA FV GGC Lan 2010 2011 2012 2010 2011 2012 2010 2011 2012 2010 2011 2012
Biopsy prior to surgical treatment 8 16 3 2 3 4 39 41 43 7 8 19
Total 64 80 63 44 44 39 325 309 309 112 97 111
West of Scotland Cancer Network Final - Published Skin Cancer MCN Audit Report 12th September 2013
16

NHS Lanarkshire and Forth Valley have now reviewed all biopsies undertaken prior to surgical treatment in 2012; results confirm that biopsy was appropriate in all of these cases due to the location of tumour or type of melanoma. In addition a number of these cases (2 cases in NHS Forth Valley) were not suspected of being malignant melanoma at time of biopsy. It is recommended that NHS Ayrshire and Arran and NHS Greater Glasgow and Clyde initiate a review of all cases. All WoS NHS Boards must monitor practice to ensure further increases do not become evident. Action required:
NHS Ayrshire and Arran and Greater Glasgow and Clyde should review the cases where biopsy was performed prior to surgical treatment to assess whether practice was appropriate.
All WoS NHS Boards should monitor clinical practice to ensure that further increases are not observed.
4.2.4. KOM 4: Breslow thickness or Clark level (if Breslow cannot be measured) should be recorded for all malignant melanoma patients There is a strong association between tumour thickness and prognosis. Breslow thickness is the single most important prognostic variable in primary cutaneous melanoma5. Where Breslow thickness is less than 1mm, Clark level should be recorded. Clark level is a measure of the depth of invasion of melanoma into the skin layers. The vast majority of patients had a Breslow thickness or Clark level recorded; 99.8% across WoSCAN, with only NHS Greater Glasgow and Clyde having less than 100% recorded (99.7%). 4.2.4.1 Breslow thickness by gender Figure 9: Breslow thickness by gender for all patients diagnosed in WoS in 2012
West of Scotland Cancer Network Final - Published Skin Cancer MCN Audit Report 12th September 2013
17

There is not a particularly pronounced gender difference in Breslow thickness, however it would appear that men are more likely to present with a Breslow thickness >4mm or metastatic disease (15% in men as opposed to 11% in women). 4.2.4.2 Breslow thickness by Scottish Index of Multiple Deprivation (SIMD) The Scottish Index of Multiple Deprivation (SIMD) has seven domains (income, employment, education, housing, health, crime, and geographical access) at datazone level, which have been combined into an overall index to identify area concentrations of multiple deprivation. Figure 10 demonstrates a link between Breslow thickness and deprivation with those in the most deprived areas having higher proportions of thicker melanomas. The proportion of thinner melanomas increases with deprivation score with the proportion of patients with a Breslow less than 1mm at 47% in the most deprived areas (increased from 44% in 2011) compared to 60% in the least deprived areas (decreased from 62% in 2011). This suggests that those in the most affluent areas may be more likely to present with less advanced disease, possibly due to earlier detection. Figure 10: Breslow thickness by SIMD for all patients diagnosed in WoS in 2012
West of Scotland Cancer Network Final - Published Skin Cancer MCN Audit Report 12th September 2013
18

4.2.5. KOM 5: Pathological staging should be used to stage all malignant melanoma patients Pathological staging aids in determining prognosis, treatment choice and appropriate follow up for patients. Pathological tumour stage is well recorded for patients in the WoS with only 5 patients with no pT stage recorded across the region. Figure 11 illustrates a significant improvement in the recording of pT stage across all WoS NHS Boards, with the exception of NHS Forth Valley, however this decrease represents only 1 patient who did not have pT stage recorded. Figure 11: Proportion of patients with pathological tumour stage recorded by location of diagnosis from 2010-2012
AA FV GGC Lan 2010 2011 2012 2010 2011 2012 2010 2011 2012 2010 2011 2012
pT recorded
63 37 63 44 43 38 186 286 299 109 94 111
Total 64 79 63 44 43 39 323 301 303 111 96 111
West of Scotland Cancer Network Final - Published Skin Cancer MCN Audit Report 12th September 2013
19

A breakdown of the tumour stage recorded for all patients is given in Figure 12. The majority of patients present with stage pT1 disease (early stage) which carries the best prognosis for invasive melanoma. Patients with stage pT1a disease can now be discharged after one year of follow-up7. Figures demonstrate an increase in the proportion of patients diagnosed with stage pT2 - pT4 disease, however given the significant improvement in data completeness this is likely not significant. Figure 12: Breakdown of pT stage for patients diagnosed in WoS in 2012
Various studies have identified mitotic rate, which is the speed at which tumour cells divide expressed in terms of mitoses per mm2, as an important prognostic factor in malignant melanoma5. Mitotic rate is correlated with an increase tumour thickness and a decrease in survival, whereby survival predictions decrease with a higher mitotic rate5. Figure 13 presents a breakdown of the mitotic rate for patients diagnosed in 2012. This is a new measure for 2012 audit data and therefore a comparison with previous years is not available. Figure 13: Mitotic rate for patients diagnosed in WoS in 2012
West of Scotland Cancer Network Final - Published Skin Cancer MCN Audit Report 12th September 2013
20

West of Scotland Cancer Network Final - Published Skin Cancer MCN Audit Report 12th September 2013
21
4.2.6. KOM 6: Surgical wide excision margins should be appropriate to stage of tumour in line with SIGN guidelines This outcome measure is based on the Cutaneous Melanoma SIGN Guideline (2003) and states that for wide excisions, the surgical excision margin should be appropriate to the tumour stage of the patient5. Table 1 displays the recommended surgical excision margin for each tumour stage according to the SIGN guideline. Table 1: SIGN guideline for surgical excision margins in cutaneous melanoma
Pathological tumour stage Recommended surgical excision margin pT1 (melanoma 0 to 1 mm thickness) 1 cm pT2 (melanoma 1 to 2 mm thickness) 1 to 2 cm pT3 (melanoma 2 to 4 mm thickness) 2 cm pT4 (melanoma > 4 mm thickness) 2 cm
Although it was agreed that this was an important issue and should be the subject of an outcome measure, the data currently collected does not allow exact measurement of surgical excision margins. The data for surgical margins currently collected is a categorical data item where the options do not allow for an exact match to the SIGN guideline recommendation. After discussion it was agreed that the options available were sufficient to give an indication of whether these guidelines were being adhered to. Table 2 indicates how the audit data item maps to the information in the SIGN guideline. Table 2: Mapping of WoSCAN audit data to surgical excision margins from SIGN guidelines
SIGN recommended excision margin Audit data – surgical excision margin 1 cm 1-2 cm 1 to 2 cm 1-2 cm 2 cm 2-3 cm
In the 2010 Audit Report it was highlighted as a regional action to consider a change to the dataset to collect surgical excision margins appropriate to those set out in the SIGN guidelines. The data on surgical excision margins complies with ISD National Minimum Core Data Definitions published in 2012. The MCN agreed not to make a change to the dataset, as alignment with the national minimum core dataset is preferable and allows for national comparative reporting. The National Minimum Core Dataset will be revised in 2013/14 as a component part of the QPI development process. The results of the outcome measure are presented in Figure 14 for patients diagnosed in 2012. As pathological tumour stage was poorly recorded in previous years this has affected this outcome measure, therefore data is not comparable across 3 years. In NHS Greater Glasgow and Clyde and NHS Lanarkshire approximately 4% of patients did not have a surgical excision margin recorded, as detailed in section 4.1. Figure 14 illustrates that compliance across all NHS Boards was reasonably high with the majority of cases compliant with the SIGN guideline recommendations. It should however be noted that the overall number of patients undergoing wide local excision, the population included within this KOM, appears low at 74% of patients across WoSCAN, ranging from 23% in NHS Forth Valley to 94% in NHS Lanarkshire. This is an area of some concern and cases should be reviewed by all NHS Boards to ascertain whether this is a data recording issue or represents a change in clinical practice.

Figure 14: Proportion of patients having wide excision who complied with SIGN guideline for surgical excision margin
AA GGC FV LAN WoSCAN Margin Appropriate 39 213 7 82 341
Margin Not Appropriate
4 10 3 8 25
Not Recorded 0 9 0 15 24
Inapplicable 4 2 0 0 6
Total 47 234 10 105 396
Action required: NHS Greater Glasgow and Clyde and NHS Lanarkshire should review audit data collection
processes to ensure complete and accurate capture of surgical excision margins. NHS Forth Valley should discuss and review surgical techniques to establish whether compliance
with the SIGN guidelines can be improved. All WoS NHS Boards should review the number of patients undergoing wide local excision to
determine if the relatively low numbers are due to a data recording issue or demonstrate a change in clinical practice. Results should be reviewed by the Skin Cancer MCN.
West of Scotland Cancer Network Final - Published Skin Cancer MCN Audit Report 12th September 2013
22

West of Scotland Cancer Network Final - Published Skin Cancer MCN Audit Report 12th September 2013
23
5. Conclusions Cancer audit data underpins much of the regional development and service improvement work of the MCN and regular reporting of activity and performance is a fundamental requirement of an MCN to assure the quality of care delivered across the region. Data collection of malignant melanoma diagnoses began in 2006 and since that time, there has been significant improvement in data quality. With data quality improving and the introduction of KOMs, the MCN is moving towards robust performance assessment where audit data can highlight clinical/service issues and lead to service change. The outcome measures analysed go some way to allowing assessment of service quality and demonstrate, across all KOMs an improvement in performance since 2010. There are still some minor data quality issues which require further improvement to enable fully robust reporting. Clinicians and audit staff must work together to improve the capture of these data if we are to make further progress in assessing quality of service. The incidence of malignant melanoma continues to rise and is it predicted that incidence will continue to increase until 2020. Nearly 50% of patients across the region present with tumours 1mm or greater, these cases have a less favourable prognosis than thinner tumours, with a much higher risk of metastasis. It is anticipated that the Scottish Government Detect Cancer Early Initiative will highlight the importance of presenting to a GP earlier and will impact on the numbers presenting with more advanced stages of disease. There are a number of actions required as a consequence of this assessment of performance against the agreed criteria, a small number of which relate to a continued commitment to data quality improvement. Additional actions relating to service provision were identified particularly in relation to biopsies prior to surgical treatment and compliance with SIGN guidelines regarding surgical excision margins.
The MCN will actively take forward regional actions identified and NHS Boards are asked to develop local Action/Improvement Plans in response to the findings presented in the report. A summary of actions for each NHS Board has been included within the Action Plan templates in Appendices I – IV. Completed Action Plans should be returned to WoSCAN within two months of publication of this report.
Progress against these plans will be monitored by the MCN Advisory Board and reported to the Regional Cancer Advisory Group (RCAG) annually by Board Lead Cancer Clinicians and MCN Clinical Leads, as part of the regional governance process to enable RCAG to review and monitor regional improvement.

West of Scotland Cancer Network Final - Published Skin Cancer MCN Audit Report 12th September 2013
24
6. Acknowledgements This report has been prepared using clinical audit data provided by each of the NHS Boards in the WoSCAN area. We would like to thank colleagues in the clinical effectiveness departments throughout the West of Scotland for gathering, submitting and verifying these data. We would also like to thank the clinicians, nurses and others involved in the management of skin cancer in the West of Scotland for their contribution.

West of Scotland Cancer Network Final - Published Skin Cancer MCN Audit Report 12th September 2013
25
7. References
1. Information Services Division (2013) Cancer Incidence in Scotland (2011) April 2013. Available from: http://www.isdscotland.org/Health-Topics/Cancer/ [Accessed on: 6th September 2013]
2. Information Services Division (2004) Cancer in Scotland: Sustaining Change. Available from:
http://www.scotland.gov.uk/Resource/Doc/30859/0012657.pdf [Accessed on: 6th September 2013]
3. Information Services Division (2013) Cancer Statistics for Malignant Melanoma of the Skin.
Available at: http://www.isdscotland.org/Health-Topics/Cancer/Cancer-Statistics/Skin/ [Accessed on: 6th September 2013]
4. Cancer Research UK (2012) Skin Cancer Mortality Statistics. Available from:
http://info.cancerresearchuk.org/cancerstats/types/skin/mortality/ [Accessed on: 6th September 2013]
5. Scottish Intercollegiate Guidelines Network (2003) Cutaneous melanoma: a national clinical
guideline. Available from: http://www.sign.ac.uk/pdf/sign72.pdf [Accessed on: 6th September 2013]
6. Marsden JR, Newton-Bishop JA, Burrows L et al. (201) Revised U.K. Guidelines for the
Management of Cutaneous Melanoma 2010. Br J Dermatol. 163 (2):238-256. Available from: http://www.bad.org.uk/Portals/_Bad/Guidelines/Clinical%20Guidelines/Melanoma%20guidelines%202010.pdf [Accessed on: 6th September 2013]

8. Abbreviations
AA Ayrshire & Arran
ACaDMe Acute Cancer Deaths and Mental Health (information system)
e-CASE Electronic Cancer Audit Support Environment
FV Forth Valley
GG&C Greater Glasgow and Clyde
GPwSI General Practitioner with Special Interest
ISD Information Services Division
KOM Key Outcome Measure
Lan Lanarkshire
MCN Managed Clinical Network
MDT Multidisciplinary Team
NHS National Health Service
NHS QIS NHS Quality Improvement Scotland
pT Tumour Stage assessed from pathological sample (according to TNM staging system)
QPI Quality Performance Indicator
RCAG Regional Cancer Advisory Group
SIGN Scottish Intercollegiate Guidelines Network
SIMD Scottish Index of Multiple Deprivation
WoS West of Scotland
WoSCAN West of Scotland Cancer Network
West of Scotland Cancer Network Final - Published Skin Cancer MCN Audit Report 12th September 2013
26

9. Appendices: NHS Board Action Plans A summary of actions for each NHS Board has been included within the Action Plan templates in Appendices I – IV. Completed Action Plans should be returned to WoSCAN within two months of publication of this report Action / Improvement Plan Health Board: NHS Ayrshire & Arran
Action Plan Lead: Date:
Timescales No. Action Required NHS Board Action Taken Start End
Lead Progress/Action Status Status (see Key)
Ensure actions mirror those detailed in Audit Report.
Detail specific actions that will be taken by the NHS Board.
Insert date
Insert date
Insert name of responsible lead for each specific action.
Provide detail of action in progress, change in practices, problems encountered or reasons why no action taken.
Insert No. from key above.
1. NHS Boards should discuss referral criteria of suspicious lesions with dermatologists and Primary Care Cancer Leads and identify means to increase numbers of appropriate urgent referrals.
2. NHS Ayrshire and Arran should review cases where excisions have been performed in Primary Care to establish reasons for the occurrences and promote referral into Secondary Care for biopsy/excision.
3. NHS Ayrshire and Arran should review the cases where biopsy was performed prior to surgical treatment to assess whether practice was appropriate.
KEY (Status) 1 Action fully implemented
2 Action agreed but not yet implemented
3 No action taken (please state reason)
West of Scotland Cancer Network Final - Published Skin Cancer MCN Audit Report 12th September 2013
27

West of Scotland Cancer Network Final - Published Skin Cancer MCN Audit Report 12th September 2013
28
Timescales No. Action Required NHS Board Action Taken Start End
Lead Progress/Action Status Status (see Key)
4. NHS Boards should monitor clinical practice to ensure that further increases in biopsy prior to surgical resection are not observed.
5. NHS Boards should review the number of patients undergoing wide local excision to determine if the relatively low numbers are due to a data recording issue or demonstrate a change in clinical practice. Results should be reviewed by the Skin Cancer MCN.
6. NHS Ayrshire and Arran should review their case ascertainment by utilising ACaDMe to compare identified malignant melanoma patients with Cancer Registry. The Board should also review the process for notification of cases from pathology department(s).

Action / Improvement Plan Health Board: NHS Forth Valley
Action Plan Lead: Date:
Timescales No. Action Required NHS Board Action Taken Start End
Lead Progress/Action Status Status (see Key)
Ensure actions mirror those detailed in Audit Report.
Detail specific actions that will be taken by the NHS Board.
Insert date
Insert date
Insert name of responsible lead for each specific action.
Provide detail of action in progress, change in practices, problems encountered or reasons why no action taken.
Insert No. from key.
1. NHS Boards should discuss referral criteria of suspicious lesions with dermatologists and Primary Care Cancer Leads and identify means to increase numbers of appropriate urgent referrals.
2. NHS Forth Valley should discuss and review surgical techniques to establish whether compliance with the SIGN guideline recommendation on appropriate surgical excision can be improved.
3. NHS Boards should monitor clinical practice to ensure that further increases in biopsy prior to surgical resection are not observed.
4. NHS Boards should review the number of patients undergoing wide local excision to determine if the relatively low numbers are due to a data recording issue or demonstrate a change in clinical practice. Results should be reviewed by the Skin Cancer MCN.
KEY (Status) 1 Action fully implemented
2 Action agreed but not yet implemented
3 No action taken (please state reason)
West of Scotland Cancer Network Final - Published Skin Cancer MCN Audit Report 12th September 2013
29

Action / Improvement Plan Health Board: NHS Greater Glasgow and Clyde
Action Plan Lead: Date:
Timescales No. Action Required NHS Board Action Taken Start End
Lead Progress/Action Status Status (see Key)
Ensure actions mirror those detailed in Audit Report.
Detail specific actions that will be taken by the NHS Board.
Insert date
Insert date
Insert name of responsible lead for each specific action.
Provide detail of action in progress, change in practices, problems encountered or reasons why no action taken.
Insert No. from key.
1. NHS Boards should discuss referral criteria of suspicious lesions with dermatologists and Primary Care Cancer Leads and identify means to increase numbers of appropriate urgent referrals.
2. NHS Greater Glasgow and Clyde should review cases where excisions have been performed in Primary Care to establish reasons for the occurrences and promote referral into Secondary Care for biopsy/excision.
3. NHS Boards should monitor clinical practice to ensure that further increases in biopsy prior to surgical resection are not observed.
4. NHS Boards should review the number of patients undergoing wide local excision to determine if the relatively low numbers are due to a data recording issue or demonstrate a change in clinical practice. Results should be reviewed by the Skin Cancer MCN.
KEY (Status) 1 Action fully implemented
2 Action agreed but not yet implemented
3 No action taken (please state reason)
West of Scotland Cancer Network Final - Published Skin Cancer MCN Audit Report 12th September 2013
30

West of Scotland Cancer Network Final - Published Skin Cancer MCN Audit Report 12th September 2013
31
Timescales No. Action Required NHS Board Action Taken Start End
Lead Progress/Action Status Status (see Key)
5. NHS Greater Glasgow and Clyde should review audit data collection processes to ensure complete and accurate capture of surgical excision margin data.

Action / Improvement Plan Health Board: NHS Lanarkshire
Action Plan Lead: Date:
Timescales No. Action Required NHS Board Action Taken Start End
Lead Progress/Action Status Status (see Key)
Ensure actions mirror those detailed in Audit Report.
Detail specific actions that will be taken by the NHS Board.
Insert date
Insert date
Insert name of responsible lead for each specific action.
Provide detail of action in progress, change in practices, problems encountered or reasons why no action taken.
Insert No. from key above.
1. NHS Boards should discuss referral criteria of suspicious lesions with dermatologists and Primary Care Cancer Leads and identify means to increase numbers of appropriate urgent referrals.
2. NHS Boards should monitor clinical practice to ensure that further increases in biopsy prior to surgical resection are not observed.
3. NHS Boards should review the number of patients undergoing wide local excision to determine if the relatively low numbers are due to a data recording issue or demonstrate a change in clinical practice. Results should be reviewed by the Skin Cancer MCN.
KEY (Status) 1 Action fully implemented
2 Action agreed but not yet implemented
3 No action taken (please state reason)
West of Scotland Cancer Network Final - Published Skin Cancer MCN Audit Report 12th September 2013
32

West of Scotland Cancer Network Final - Published Skin Cancer MCN Audit Report 12th September 2013
33
Timescales No. Action Required NHS Board Action Taken Start End
Lead Progress/Action Status Status (see Key)
4. NHS Lanarkshire should review audit data collection processes to ensure complete and accurate data capture for surgical excision margins, particularly identifying a process for retrieval of surgical margin data from Plastic Surgery Department in NHS Greater Glasgow and Clyde.
5. NHS Lanarkshire should review audit data collection processes to ensure complete and accurate capture of surgical excision margin data.